")
Back to Journals » OncoTargets and Therapy » Volume 7
External iliac vein – transplant ureteral fistula combined with renal cell carcinoma: an unusual case of hematuria
Authors Luo J, Liu B, Wang P, Zhou F, Xu X, Li S, Cai S, Wang Y
Received 23 March 2014
Accepted for publication 9 June 2014
Published 23 July 2014 Volume 2014:7 Pages 1339—1342
DOI https://doi.org/10.2147/OTT.S64685
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Jin-dan Luo, Ben Liu, Ping Wang, Feng Zhou, Xiang-lai Xu, Shi-qi Li, Song-liang Cai, Yi-min Wang
Department of Urology, the First Affiliated Hospital, School of Medicine, Zhejiang University, Zhejiang, People's Republic of China
Abstract: Iliac vein-ureteral fistula is a rare cause of hematuria. The diagnosis of an iliac vein-ureteral fistula can be elusive even with the use of multiple methods. With regards to the treatment, there appears to be a shift in management from primarily open surgical to primarily angiographic management. We present a unique case of an external iliac vein – transplant ureteral fistula. A 48 year-old female complained of recurrent gross hematuria. She underwent transplant nephrectomy and radical left nephrectomy because of rejection of transplanted kidney and cystic renal cell carcinoma when the hematuria arose for the first time. Ten months later, the hematuria recurred again, and cystoscopy showed bleeding from the right transplant ureteral orifice. Open exploration confirmed the diagnosis of external iliac vein – transplant ureteral fistula. Diagnostic difficulties and treatment dilemma of such a rare cause of hematuria are also discussed.
Keywords: iliac vein, ureteral fistula, renal transplantation, hematuria
Introduction
Iliac vein-ureteral fistula (IVUF) is a direct fistulous communication between an iliac vein and a ureter that results in gross hematuria. It is an uncommon condition but one that can have serious consequences when not properly diagnosed and managed. As reported by literature, the most common fistula of vascular genesis is iliac artery-ureteral fistula (IAUF).1 Though not as life-threatening as IAUF, gross intermittent hematuria and pain caused by IVUF is still a matter of urgency. A number of underlying conditions are known to be predisposing factors in the development of an IVUF. Secondary vein-ureteral fistula is more common. The etiology of such a fistula is mostly iatrogenic, including pelvic malignancy, previous vascular or pelvic surgery, radiotherapy, ureterolithiasis, diverting urinary conduit construction, infection, and indwelling ureteral stents.2 Primary uretero-iliac fistula caused by aortoiliac aneurysm and arteriovenous malformation only constitutes 15% of all such fistulas.3 We describe a dramatic case with recurrent hematuria even after undergoing transplant nephrectomy and radical nephrectomy because of renal allograft rejection with combined renal cell carcinoma (RCC), which finally turned out to be an external iliac vein – transplant ureteral fistula.
Case report
The patient was a 48 year-old female who underwent renal transplantation in another institution because of uremia in 1998. After the surgery, the patient was on an immunosuppressive regimen including mycophenolate mofetil, cyclosporin A, and methylprednisolone. Although the serum creatinine levels fluctuated at the upper limit of the normal range in the first few years postoperatively, it increased gradually and arrived at a climax of 570 μmol/L in 2007. At the same time, the patient’s highest blood pressure reading was 180/105 mmHg, subsequently, the patient received hemodialysis therapy five times every 2 weeks, with nifedipine and benazepril hydrochloride to control her blood pressure. In 2011, the patient was admitted in a local hospital for intermittent gross hematuria with right lower abdominal pain. There were no symptoms such as frequent urination, urodynia or lumbago. Serum creatinine level was 839 μmol/L. The diagnosis of rejection of transplanted kidney was made, and the patient received transplant nephrectomy. Histological examination confirmed the diagnosis of chronic renal allograft rejection. However, gross hematuria persisted after the surgery. Further examination by computed tomography (CT) showed a suspicious lesion with a diameter of 1.0 cm in the upper pole of the left kidney, so the patient received radical left nephrectomy and postoperative pathological results confirmed the diagnosis of cystic RCC. The symptom of hematuria disappeared after the surgery for 10 months, but then the patient was referred to our institution with a complaint of gross hematuria again. Serum creatinine level was 1,393 μmol/L. Urinalysis showed hematuria and proteinuria (3+). The cystoscopy examination showed bleeding from the right transplant ureteral orifice, with clots in the bladder. Open exploration was subsequently performed through a Gibson incision in the lower right abdomen. Transplant ureteral stump was located near the right wall of the bladder and had adhered to the external iliac vein tightly (Figure 1). It was difficult to separate the transplant ureteral stump from the external iliac vein, so we decided to remove the transplant ureteral stump including part of the wall of the external iliac vein. The patient recovered with no complication postoperatively. Pathological analysis showed a fistula between the transplant ureteral stump and the external iliac vein (Figure 2). At present, 20 months after the operation, the patient is free of hematuria. There are also no signs of recurrence of RCC.
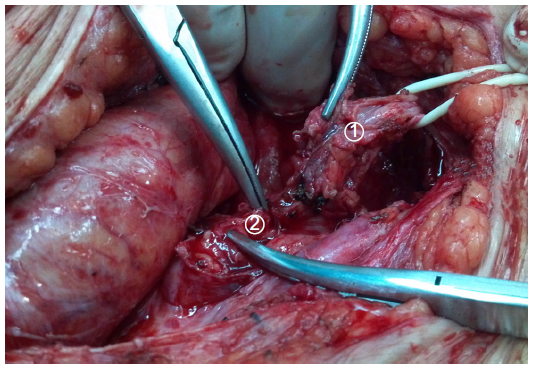 | Figure 1 Transplant ureteral stump tightly adhered to the external iliac vein. |
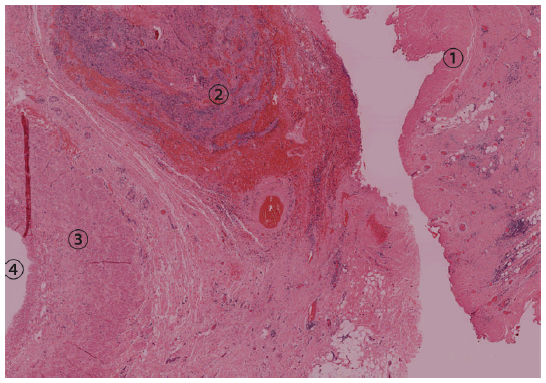 | Figure 2 A fistula between the transplant ureteral stump and the external iliac vein. |
Discussion
Ureteroiliac fistula is a rare cause of gross hematuria. However, it is appearing more frequently due to trends of more aggressive surgical resection of pelvic malignancy along with pelvic radiotherapy coupled with the increased use of indwelling ureteral stents.4 IAUF is more common than IVUF. The pathophysiology behind the development of IVUF remains poorly understood; many factors have a potential role. Surgery, radiation therapy, and urine leaks are all probably responsible for the intense fibrotic, inflammatory response that causes the ureter to attach itself to the vein. The liberal use of indwelling ureteral stents is also thought to be a contributor because very few ureteroiliac fistulas were reported prior to the development of indwelling ureteral catheters in 1978.5 The fistula may form once fibrosis from prior surgery causes the transplant ureteral stump to become attached to the external iliac vein where the two intersect and cross. The vein is then more susceptible to rupture, erosion, and necrosis.6
IVUF caused by transplant ureter has seldom been reported. In our patient, the gross hematuria was considered to be caused by renal allograft dysfunction when it appeared for the first time. However, hematuria persisted after transplant nephrectomy. More interestingly, a tumor was found located in the left kidney and the patient underwent radical nephrectomy. Hematuria had ceased for 10 months until it recurred because of external iliac vein – transplant ureteral fistula, which was likely due to transplant nephrectomy.
Hematuria, hydronephrosis, and obstruction are the most frequently presenting symptoms.7 Flank pain and pyelonephritis are also concomitant symptoms. However, all these symptoms are not specific. The diagnosis of IVUF requires a high degree of suspicion. In a series of IAUF, the mortality rate of patients who were explored without the correct preoperative diagnosis was 58%. Conversely, when the correct diagnosis was made before surgery, the mortality rate declined to 8%.2 Although torrential hemorrhage due to IVUF is not as common as IAUF, the importance of obtaining the correct preoperative diagnosis cannot be overemphasized. No single test can diagnose all cases of IVUF, and most cases require the use of multiple imaging methods.
Three-dimensional CT or multiplanar reconstruction CT should be performed first,8 but finding the definite source of bleeding can be challenging because hemorrhage often occurs intermittently. Cystoscopy and retrograde pyelography are still options, though the greatest sensitivity is between 45% and 60%.9 In our case, cystoscopy was the crucial method of diagnosis. The use of ureteroscopy should be approached with caution because it can tear the fistula or dislodge a tamponading clot, leading to massive hemorrhage. Identification of a fistulous communication is sometimes difficult during endoscopic procedures unless there is active bleeding, as blood clots may occlude the fistulous tract. Standard angiography has demonstrated a sensitivity of 23% to 41% for detecting uretero-iliac fistulas.9 Provocative angiography can improve the sensitivity through manipulating the indwelling ureteral stent and angiographic catheter with a contrast agent positioned directly over the suspected fistula site until bleeding is seen. However, provocative angiographic maneuvers should only be attempted after appropriate preparation to manage the bleeding.
Multiple options are available for the treatment of IVUF. Both the specific situation and the individual patient’s overall clinical status should be considered during the treatment. The vascular defect can be repaired by open reconstruction, embolization with extra-anatomic vascular reconstruction, or endovascular stenting. The ureter can be managed by ureteral stenting, nephrectomy with ureteral ligation or nephroureterectomy, ureteral reconstruction or nephrostomy tube placement. Some surgeons prefer nephrectomy with ureteral ligation or nephroureterectomy for patients with normal renal function.9 Even though open reconstruction has yielded excellent results, many surgeons are reluctant to do so because of the hostile surgical field resulting from earlier surgery, prior radiation treatment, and the potential presence of residual malignancy. Embolization was one of the first endovascular approaches used to control the hemorrhage,10 but embolization may not be possible in the absence of active bleeding. Endovascular stenting has now become an appealing option superior to open surgical reconstruction as it is minimally invasive, and effective in controlling bleeding. However, to identify the fistula site during an angiogram in IVUF still remains challenging because the pressure of the vein is not as high as the artery and the bleeding is intermittent. Using an endovascular stent is also associated with the risk of graft occlusion or persistent bleeding. In our case, we chose open exploration because cystoscopy examination showed bleeding from the right transplant ureteral orifice. Since the patient had already undergone transplant nephrectomy, the diagnosis of transplant ureteral fistula seemed like a reasonable explanation. Embolization and endovascular stenting may not have been as effective as open surgery was in this case.
In summary, the rarity of IVUF may result in a diagnostic and treatment dilemma. The prompt and accurate diagnosis of these entities remains a challenge. Methods utilized to treat this condition have evolved over the last decade. We present an interesting case of recurrent hematuria caused by external iliac vein – transplant ureteral fistula, which was also combined with RCC. Although treatment with endovascular stenting appears to be a minimally invasive and effective option, open exploration and resection of external iliac vein – transplant ureteral fistula is also a definitive treatment for such an unusual condition.
Acknowledgments
This work was supported by grants from the Scientific Research Fund of Zhejiang Provincial Education Department (grant No Y201120149), the Scientific Research Fund of the Health Bureau of Zhejiang Province (grant No 2013KYB099) and the National Key Clinical Specialty Construction Project of China.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
Bergqvist D, Parsson H, Sherif A. Arterio-ureteral Fistula – a Systematic Review. European Journal of Vascular and Endovascular Surgery. 2001;22(3):191–196. | |
Kerns DB, Darcy MD, Baumann DS, Allen BT. Autologous vein-covered stent for the endovascular management of an iliac artery-ureteral fistula: case report and review of the literature. J Vasc Surg. 1996;24(4):680–686. | |
Khong TL, Winstanley V, Lee G, Christmas T, Ramsay J. Primary uretero-iliac fistula: the unusual source of haematuria. Int Urol Nephrol. 2007;39(3):751–753. | |
Vandersteen DR, Saxon RR, Fuchs E, Keller FS, Taylor LM Jr, Barry JM. Diagnosis and management of ureteroiliac artery fistula: value of provocative arteriography followed by common iliac artery embolization and extraanatomic arterial bypass grafting. J Urol. 1997;158(3 Pt 1):754–758. | |
Finney RP. Experience with new double J ureteral catheter stent. J Urol. 1978;120(6):678–681. | |
Puppo P, Perachino M, Ricciotti G, Zinicola N, Patrone PE. Ureteroarterial fistula: a case report. J Urol. 1992;148(3):863–864. | |
McCullough MC, Oh EE, Lucci JA 3rd, Alvarez EA. Ureteroarterial fistula. J Obstet Gynaecol. 2012;32(7):617–620. | |
Araki T, Nagata M, Araki T, Takihana Y, Takeda M. Endovascular treatment of ureteroarterial fistulas with stent-grafts. Radiat Med. 2008;26(6):372–375. | |
Krambeck AE, DiMarco DS, Gettman MT, Segura JW. Ureteroiliac artery fistula: diagnosis and treatment algorithm. Urology. 2005;66(5):990–994. | |
Darcy M. Uretro-arterial fistulas. Tech Vasc Interv Radiol. 2009;12(3):216–221. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.