")
Back to Journals » Infection and Drug Resistance » Volume 15
Expression of Serum Cytokines Profile in Neonatal Sepsis
Authors Chen S, Kuang M, Qu Y , Huang S, Gong B, Lin S, Wang H, Wang G, Tao H, Yu J, Yang Z, Jiang M, Xie Q
Received 12 April 2022
Accepted for publication 23 June 2022
Published 30 June 2022 Volume 2022:15 Pages 3437—3445
DOI https://doi.org/10.2147/IDR.S368772
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Suipeng Chen,1,* Mengjiao Kuang,1,* Ying Qu,1,2 Shirui Huang,1 Binbin Gong,1 Suzhen Lin,1 Huiyan Wang,1 Guiye Wang,1 Hongqun Tao,1 Jian Yu,1 Zuqin Yang,3 Minghua Jiang,1 Qipeng Xie1
1Department of Laboratory Medicine, The Second Affiliated Hospital & Yuying Children’s Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, 325035, People’s Republic of China; 2Department of Clinical Laboratory, Wenzhou People’s Hospital, The Third Affiliated Hospital of Shanghai University, The Third Clinical Institute Affiliated to Wenzhou Medical University, Wenzhou, Zhejiang, 325035, People’s Republic of China; 3Newborn Department of Pediatrics, The Second Affiliated Hospital & Yuying Children’s Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, 325035, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qipeng Xie, Department of Laboratory Medicine, The Second Affiliated Hospital & Yuying Children’s Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, 325035, People’s Republic of China, Tel +86 15157787159, Email [email protected]
Objective: Sepsis remains a major cause of neonatal death. To better characterize the inflammatory response during neonatal sepsis, we compared the differences in serum cytokines and chemokines between full-term neonates with sepsis and without infection.
Methods: We enrolled 40 full-term neonates with sepsis and 26 full-term neonates without infection as controls between October 2016 and June 2018. Forty cytokines /chemokines in serum were analyzed using the Luminex Bead Immunoassay System.
Results: Our results showed that serum IL-6, IL-8, TNF-α, IL-1β, MIF, CXCL13, CXCL1, CXCL2, CXCL5, CXCL6, CXCL16, CCL27, CCL2, CCL8, CCL3, CCL20, CCL23, and CX3CL1 levels were significantly increased in neonates with sepsis compared to those in the control group (all p< 0.05). The levels of serum CCL20, and IL-17 were higher in late-onset sepsis (LOS) than those in early-onset sepsis (EOS) (all p< 0.05). Conversely, serum CXCL16 was lower in LOS than that in EOS (p< 0.05).
Conclusion: Our findings revealed that excessive pro-inflammatory cytokines might be involved in neonatal sepsis. In addition, chemokines significantly increased the recruitment of immune cells after infection to participate in the anti-infection defense of neonates, but this could lead to damage.
Keywords: neonatal sepsis, cytokines, chemokines
Plain Language Summary
“What is already known on this topic”
The clinical features of neonatal sepsis include systemic inflammatory response syndrome. Previous studies have shown that serum TNF-α, IL-1β, IL-6, IL-8, CXCL10, CXCR4 and CXCL12 levels rapidly and significantly increase in neonatal sepsis. These cytokines can be used as biomarkers of neonatal sepsis.
“What this study adds”
Research on the cytokine/chemokine difference between early-onset sepsis (EOS) and late-onset sepsis (LOS) is limited. In addition, there is little work to assess the significant changes in innate immunity and adaptive immunity during neonatal sepsis. Our results found that while the recruited immune cells participate in the anti-infection defense in neonates, they might also cause damage.
Introduction
Neonatal sepsis is a systemic infection, which is characterized by life-threatening organ dysfunction.1 Despite advances in the management of neonates and the new generation of antibiotics, sepsis is still the leading cause of neonatal deaths with more than one million deaths worldwide each year.2–4
After infection, pathogen-associated molecular patterns are recognized by sentinel immune cells through several classes of pathogen recognition receptors (eg, toll-like receptors).5–7 Activation of these receptors can stimulate the release of inflammatory mediators, including cytokines and chemokines. Therefore, the clinical features of neonatal sepsis include systemic inflammatory response syndrome. Several studies had demonstrated that serum pro-inflammatory TNF-α, IL-1β, IL-6, and IL-8 levels are rapidly and strikingly elevated in neonatal sepsis.8–10 Moreover, in previous studies, the levels of serum CXCR4 and CXCL12 in neonatal sepsis were found to be significantly higher than those in controls.11,12 Another study showed that the level of CXCL10 was increased in the blood and peritoneum in a murine model of neonatal polymicrobial sepsis.13 Furthermore, these cytokines served as valuable biomarkers for the diagnosis of neonatal sepsis.8–12 However, studies on the cytokines/chemokines differences between early-onset sepsis (EOS) and late-onset sepsis (LOS) were limited. Moreover, little work had been done to assess the dramatic changes in innate immunity and adaptive immunity during neonatal sepsis. Therefore, in the present study, to better characterize the inflammatory response during neonatal sepsis, we systematically analyzed cytokine/chemokine profiles in neonatal sepsis.
Materials and Methods
Subjects and Ethics Statement
Full-term neonates who were hospitalized for sepsis at the neonatal intensive care unit of the Second Affiliated Hospital of Wenzhou Medical University, between October 2016 and June 2018, were eligible to participate in this study. Neonates with congenital malformations, those who had treatment prior to sample collection, and those who had undergone surgery were excluded. In addition, full-term neonates without signs or laboratory evidence of inflammatory disease were included as controls. The study was approved by the Ethical Committee of the Second Affiliated Hospital of Wenzhou Medical University (Registration code: LCKY2018-65) and was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from the parents or legal guardians.
The Diagnostic Criteria of Neonatal Sepsis
The diagnosis of neonatal sepsis was according to the International Pediatric Sepsis Consensus.14 Confirmed neonatal sepsis was defined as a positive blood culture accompanied by the presenting signs and symptoms. Suspected neonatal sepsis was defined as the presence of laboratory findings suggestive of infection (neutrophilia/neutropenia, thrombocytopenia, elevated C-reactive protein (CRP), and erythrocyte sedimentation rate (ESR)) in combination with at least three of the following symptoms and signs without other causes: temperature instability (core temperature ≥ 38.5 or ≤ 36°C); respiratory symptoms (apnea, tachypnea with respiratory rate > 60 per minute, cyanosis, need for high ventilator settings or oxygen); cardiovascular symptoms including hypotension (blood pressure < fifth percentile for age), tachycardia (heart rate > 160 beats per minute), bradycardia (heart rate < 80 beats per minute), or poor perfusion; neurological symptoms (hypotonia, hyporeflexia, irritability, lethargy, and seizures); gastrointestinal symptoms (poor feeding, abdominal distension, green or bloody residuals, and vomiting). EOS was defined as onset in the first 72 hours after birth, and LOS was defined as onset after the first 72 hours of life.
Sample Collection
A total of 2 mL of venous blood was collected from all participants prior to treatment and was centrifuged at 3000 rpm for 15 min. In addition, sera were collected from 15 neonatal sepsis after treatment (3 EOS and 12 LOS). The sera were stored at −70 °C until analysis.
Quantification of Serum Cytokines and Chemokines
Forty cytokines and chemokines, including CCL21, CXCL13, CCL27, CXCL5, CCL11, CCL24, CCL26, CX3CL1, CXCL6, GM-CSF, CXCL1, CXCL2, CCL1, IFN-γ, IL-1β, IL-2, IL-4, IL-6, IL-8, IL-10, IL-16, CXCL10, CXCL11, CCL2, CCL8, CCL7, CCL13, CCL22, MIF, CXCL9, CCL3, CCL15, CCL20, CCL19, CCL23, CXCL16, CXCL12, CCL17, CCL25, and TNF-α, were analyzed using the Luminex Bead Immunoassay System (Bio-Rad Laboratories, Hercules, CA) following the manufacturer’s instructions. Serum IL-17 level was measured using human IL-17 Quantikine ELISA kits (eBioscience, San Diego, CA) according to the manufacturer’s instructions.
Statistical Analysis
Statistical analyses were performed using SPSS 23.0 (SPSS Inc., Chicago, IL). Categorical variables were expressed as frequencies and percentages. Continuous variables were presented as the median and interquartile range (IQR). The data were not normal distribution and were from a small sample size, the nonparametric tests were chosen. The Mann–Whitney U-test was used to compare the differences in the serum cytokine and chemokine levels, age, temperature, blood WBC counts, neutrophil counts, etc. between controls and neonatal sepsis. The serum cytokine and chemokine levels in the blood culture-positive group and blood culture-negative group were compared using the Mann–Whitney U-test. We used the Kruskal–Wallis H-test (including Dunn-Bonferroni post hoc correction) to compare the serum cytokine and chemokine levels in controls, EOS, and LOS. The differences in serum cytokine and chemokine in neonates with sepsis before and after treatment were analyzed using the Wilcoxon test. For correlation analysis between the levels of serum cytokines/chemokines and age in neonatal sepsis, Spearman correlation coefficients were calculated. We considered p<0.05 with two-tailed tests to be statistically significant.
Results
Clinical Characteristics of the Enrolled Neonates
A total of 40 full-term neonates with sepsis (10 EOS and 30 LOS) and 26 controls were enrolled in this study. The body temperature was 38.1℃ (IQR 37.13℃–38.65℃) and 36.8℃ (IQR 36.5℃–37.2℃) in neonates with sepsis and those in the control group, respectively (p<0.0001). In 13 neonates with positive blood culture, the following pathogens were isolated: Escherichia coli (seven cases), Streptococcus lactis (four cases), Klebsiella (one case), and Enterococcus faecium (one case). The levels of serum C reactive protein (CRP) and serum amyloid protein A (SAA) in neonates with sepsis were 9.11 mg/mL (IQR 6.54 mg/mL-10.13 mg/mL) and 29.38 mg/mL (IQR 4.83 mg/mL-36.24 mg/mL), respectively, which were significantly higher than those in the control group (both p<0.0001). The neutrophil counts of the neonates with sepsis and those in the control group were 9.06x109/L (IQR 5.34 x109/L-14.84 x109/L) and 6.14x109/L (IQR 4.29 x109/L-7.76 x109/L) (p=0.018), respectively. There were no significant differences in the monocyte, lymphocyte, and platelet counts between the two groups (all p>0.05). Detailed information of the clinical characteristics was shown in Table 1.
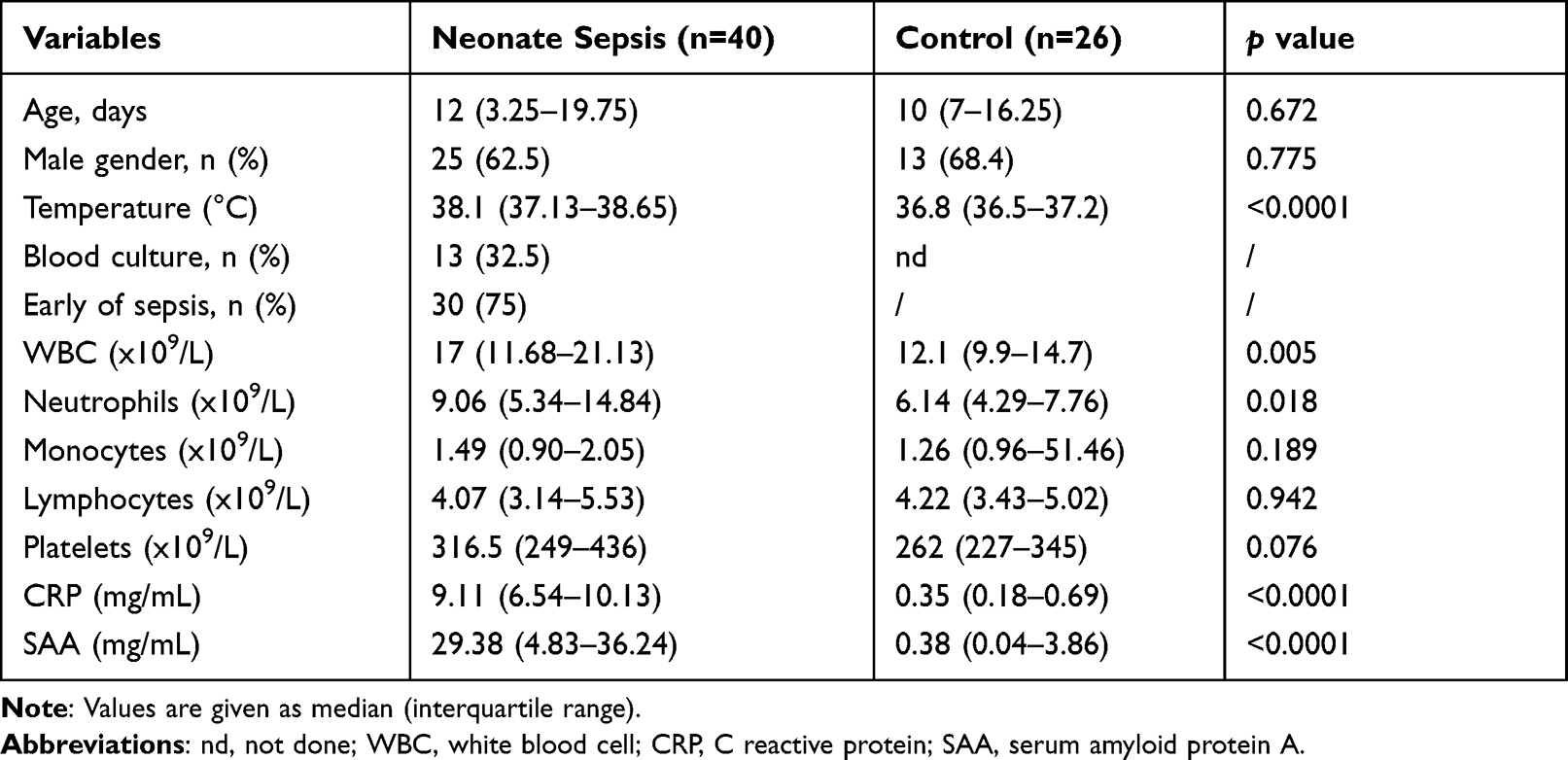 |
Table 1 The Clinical Characteristics of the Enrolled Neonates |
Levels of Serum Cytokines and Chemokines in Neonatal Sepsis
We compared serum cytokine and chemokine levels between neonates with sepsis and those in the control group. Since the level of CCL15 was not in the quantitative range of the assay and exceeded the highest calculated concentration, we did not analyze it further. As shown in Figure 1, the levels of the pro-inflammatory cytokines, IL-6, IL-8, TNF-α, and IL-1β, were significantly higher in neonates with sepsis than those in the control group (all p<0.05). There was no difference in the levels of IL-4, IFN-γ, IL-17, IL-2, IL-10, GM-CSF, and IL-16 between the two groups (all p>0.05) (Figure S1). Serum MIF level was remarkably increased in neonates with sepsis, and was 6270 pg/mL (IQR 4615 pg/mL-11,820 pg/mL) and 4947 pg/mL (IQR 3204 pg/mL-6767 pg/mL) in the sepsis and control groups, respectively (p=0.0223). Serum CXCL13, CXCL1, CXCL2, CXCL5, CXCL6, CXCL16, CCL2, CCL8, CCL3, CCL20, CCL23, CCL27, and CX3CL1 levels were significantly increased in neonates with sepsis compared to those in the control group (all p<0.05) (Figure 1). Interestingly, the levels of serum CXCL5, IL-2 and IL-4 in female were higher than those in male (Table S1).
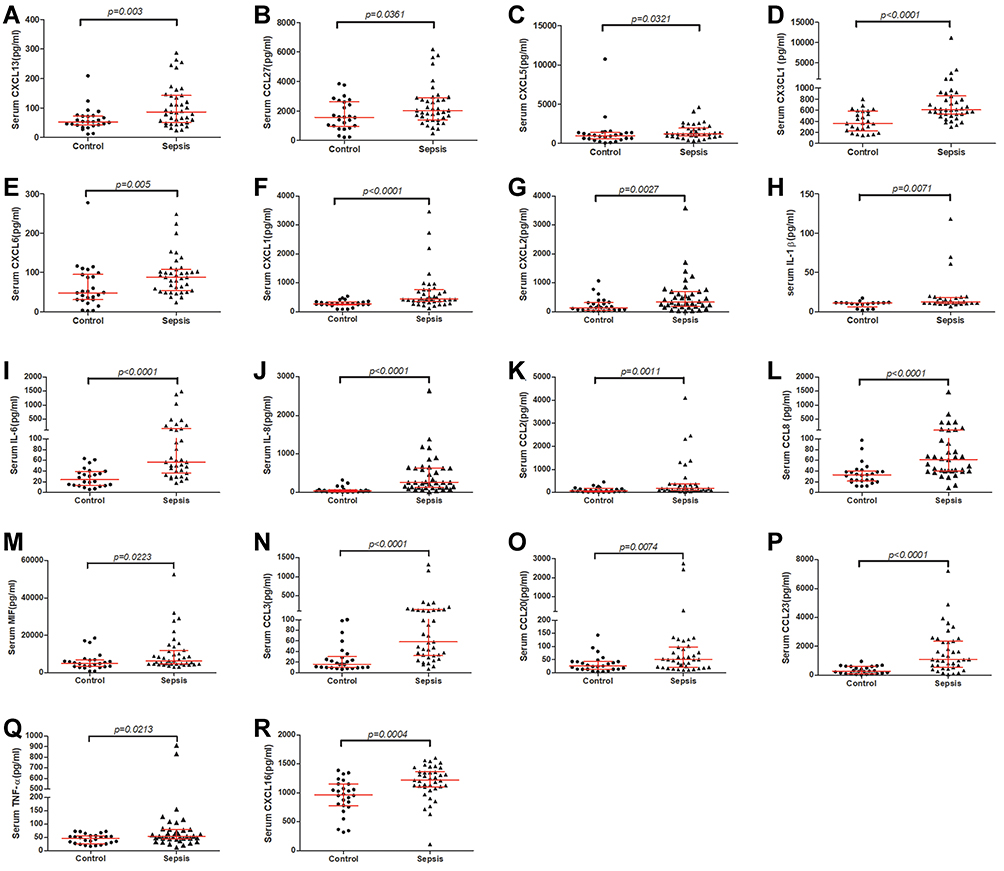 |
Figure 1 The chemokines and cytokines were significantly different between controls and neonatal sepsis. The levels of CXCL13 (A), CCL27 (B), CXCL5 (C), CX3CL1 (D), CXCL6 (E), CXCL1 (F), CXCL2 (G), IL-1β (H), IL-6 (I), IL-8 (J), CCL2 (K), CCL8 (L), MIF (M), CCL3 (N), CCL20 (O), CCL23 (P), TNF-α (Q), and CXCL16 (R) in serum from controls (n=26) and neonatal sepsis (n=40). The red horizontal lines show the medians and interquartile range. The difference between control and neonatal sepsis was assessed using the Mann–Whitney U-test. |
Subsequently, we further analyzed the differences in these cytokines and chemokines between the EOS and LOS groups. There were 10 EOS and 30 LOS. The ages of EOS and LOS were 2 days (IQR, 1day-3days) and 17days (IQR, 11.75days-21.25days), respectively (p<0.001). The body temperature was 37.15°C (IQR, 36.63°C-37.5°C) and 38.45°C (IQR, 38°C-38.73°C) in EOS and LOS, respectively (p=0.0006). All cases who were blood culture positive were LOS (Table 2). As shown in Figure 2, the levels of serum CCL20 and IL-17 were higher in LOS than those in EOS (both p<0.05). Conversely, serum IL-16 was lower in LOS than that in EOS (p<0.05).
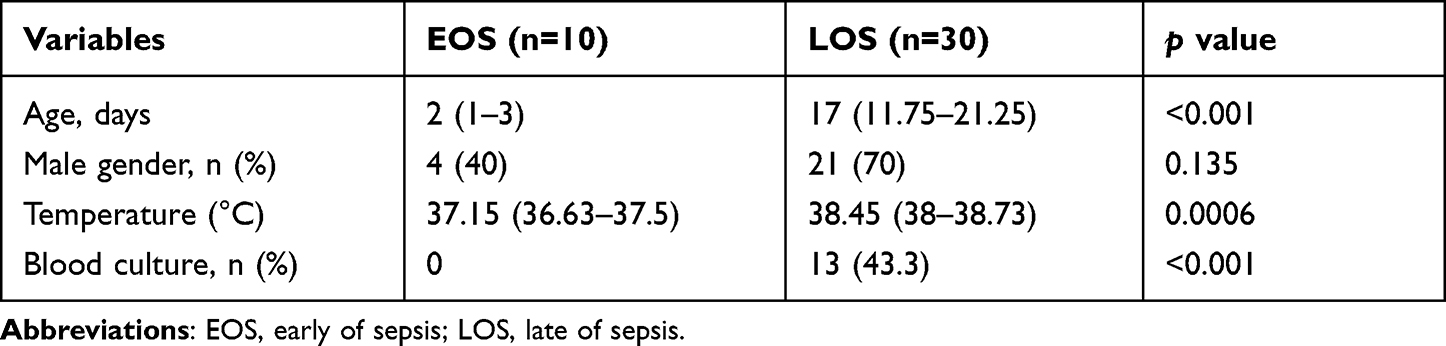 |
Table 2 The Clinical Characteristics of EOS and LOS |
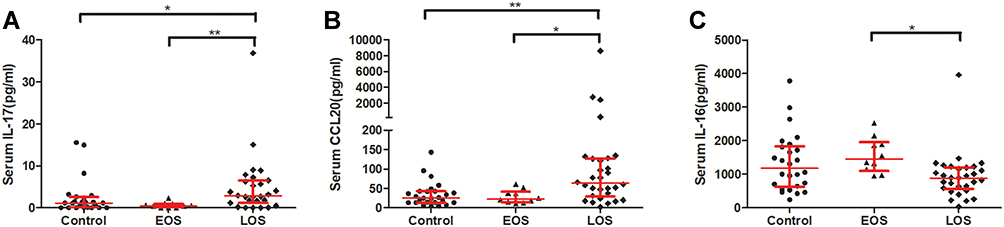 |
Figure 2 The levels of IL-17 (A), CCL20 (B), and IL-16 (C) in serum from control(n=26, EOS (n=10) and LOS (n=30). The red horizontal lines show the medians and interquartile range. The difference between control and neonatal sepsis was assessed using the Kruskal–Wallis H-test. *P < 0.05; **P < 0. 01. |
Among the 40 neonates with sepsis, there were 13 neonates with positive blood culture and 27 neonates with negative blood culture. We compared the levels of serum cytokines and chemokines between neonates with positive and negative blood cultures. The levels of CXCL6, CCL8, and CCL23 in neonates with positive blood culture were significantly higher than those with negative blood culture (all p<0.05) (Table S2). There was no difference in the levels of other cytokines and chemokines between the two groups (data not shown).
The Association Between the Levels of Serum Cytokines/Chemokines and Age in Neonatal Sepsis
We further analyzed the association between the levels of cytokines/chemokines and age among neonatal sepsis. As shown in Table S3, the levels of CCL21, CCL27, CCL22, CCL19, CXCL16, CCL17, IL-10, and IL-16 were negative correlation with their ages, and IL-17 was positively correlated with ages (all p<0.05).
Levels of Cytokines and Chemokines After Treatment
Of 15 neonatal sepsis (3 EOS and 12 LOS) were treated with antibacterial therapy. The sera of the 15 neonates with sepsis were collected after treatment. The point-in-time of collection was 5.5days (IQR, 2days-7.25days) after treatment. A total of 41 cytokines and chemokines were measured. As shown in Figure 3, IL-6, IL-8, TNF-α, IL-1β, CXCL13, CXCL16, CCL27, CCL3, CCL23, and CX3CL1 were significantly decreased after treatment (all p<0.005).
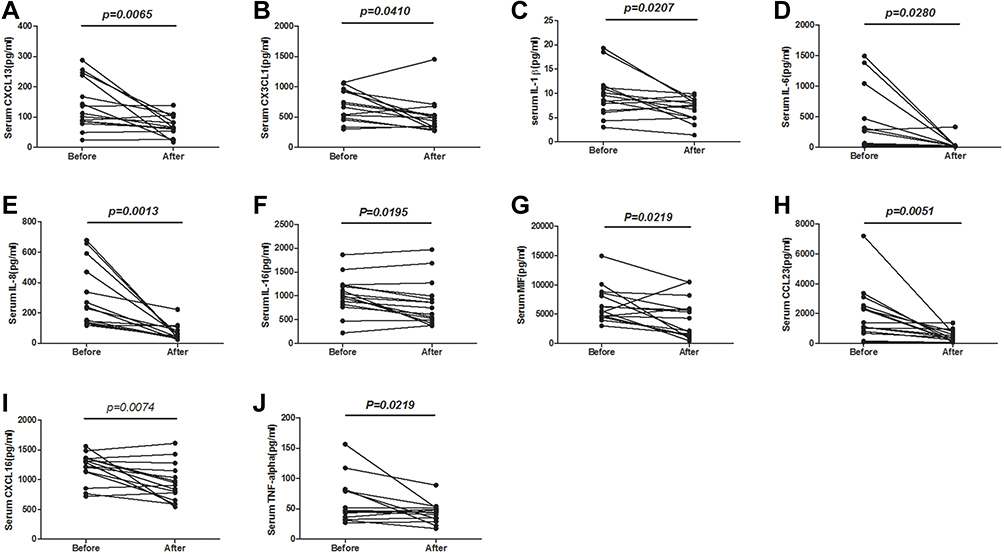 |
Figure 3 Levels of cytokines and chemokines before and after treatment in 15 neonates with sepsis. The levels of CXCL13 (A), CX3CL1 (B), IL-1β (C), IL-6 (D), IL-8 (E), IL-16 (F), MIF (G), CCL23 (H), CXCL16 (I), and TNF-alpha (J) in serum from sepsis neonates (n=15) before and after treatment. Differences before and after treatment were analyzed using the Wilcoxon test. |
Discussion
Neonatal sepsis is a major risk factor for neonatal mortality.15 Furthermore, the underlying pathological mechanisms remain unclear. In the present study, we systematically investigated the dynamic changes in cytokine and chemokine profiles in neonatal sepsis. In accordance with previous studies,8–10 the levels of the pro-inflammatory cytokines IL-6, IL-8, TNF-α, and IL-1β were significantly increased in neonates with sepsis. A moderate increase in cytokines plays a protective role and promotes antimicrobial immune responses, whereas excessive upregulation of pro-inflammatory cytokines is commonly associated with a severe and often fatal outcome due to multiple organ failure.16
Chemokines are a family of cytokines that have the capacity to recruit leukocytes to pathogen invasion sites, which is essential for the host to defend against infections.17 Our results showed that serum CXCL13, CXCL1, CXCL2, CXCL5, CXCL6, CXCL8, CXCL16, CCL27, CCL2, CCL8, CCL3, CCL20, CCL23, CCL27, and CX3CL1 levels were significantly increased in neonates with sepsis compared to those in the control group. Manoura et al also found that the levels of serum CXCL1 and CXCL5 were higher in neonates with sepsis.18 Among these chemokines, CXCL1, CXCL2, CXCL5, CXCL6, and CXCL8 are potent chemoattractants for neutrophils. Neutrophils are the most abundant cells of innate immunity and play an important role in responding to bacterial, viral, and fungal infections.19 Previous studies have shown that elastase and nitric oxide are upregulated in neonates with sepsis.20,21 In our study, neutrophil counts in neonates with sepsis were higher than those in controls. These results suggested that neutrophil-related chemokines were immediately synthesized and released after infection, which might have subsequently led to the recruitment of neutrophils as a defense mechanism against infections in the neonates.
The defense system in neonates is initially dependent on their innate immune system because adaptive immunity develops later in life.22 Interestingly, in our study, the levels of Th17 cell-related cytokine/chemokines, IL-17 and CCL20 were significantly higher in LOS than those in EOS. The level of IL-17 was positively correlated with ages. The ages of LOS were higher than those of EOS. Taken together, our results indicated that the pro-inflammatory cytokines were initially released in neonates at the onset of infection, but adaptive immunity gradually developed in the later stage of infection.
The serum MIF level in neonatal sepsis was significantly higher than that in the control group. After treatment, MIF significantly decreased. The MIF of newborns is 10-fold higher than that of children and adults. E. coli and Group B Streptococcus induce MIF secretion by neonatal monocytes.23 MIF plays an important role in promoting the production of inflammatory cytokines by monocytes.24 Previous studies have indicated that MIF is correlated with the expression of pro-inflammatory markers and the dysregulation of pituitary and adrenal function, severity scores, and disease outcomes.25–28 Therefore, MIF might play a critical role in the immune regulation of neonatal sepsis.
In our study, serum CX3CL1 levels were increased in neonates with sepsis. A previous study reported that the level of plasma CX3CL1 was elevated in a mouse model of CLP-induced sepsis.29 The level of CX3CL1 in adult sepsis patients increased with the severity and number of organ dysfunction.30 Non-survivors had sustained elevated CX3CL1 levels compared to survivors.30 Taken together, these data suggest that CX3CL1 is a risk factor for sepsis outcomes. CX3CL1 acts through the CX3CR1 receptor and is a unique member of the CX3C chemokine family. CX3CR1 is mainly expressed on CD14++CD16+ and CD14+CD16++ monocytes, which represent an activated and a more mature “macrophage-like” subset. Furthermore, the cell population is greatly expanded in various infectious and inflammatory diseases and can be more than 50% of total monocytes during sepsis.31 These data suggest that CX3CL1 recruits activated monocytes and can be involved in neonatal sepsis damage. However, the roles of CX3CL1 in neonatal sepsis need to be further studied.
Our study has some limitations. First, the subjects enrolled were relatively few; therefore, our findings need to be proven in future studies with a larger cohort. Second, gestational age is an essential factor for these cytokines and chemokines, whereas we only enrolled full-term neonates in our study. Third, although blood culture is known as the most reliable means for the definite diagnosis of neonatal sepsis, the positive rate of blood culture was low. There were only 13 neonates with blood culture positive. To be sure that the neonates were real sepsis when the blood culture was negative, the combination of laboratory examination and clinical symptoms of systemic inflammatory response syndrome indirectly verified systemic infection, at the same time, and distinguished from neonatal hepatitis, diseases of digestive or respiratory, etc.
In conclusion, our study suggested that excessive inflammation in neonatal sepsis might be involved in the damage associated with neonatal sepsis. Neutrophils, monocytes, and lymphocyte-associated chemokines increased significantly after infection. To summarize, while the recruited immune cells participate in the anti-infection defense in neonates, they might also cause damage.
Abbreviations
EOS, early-onset sepsis; LOS, late-onset sepsis; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; SAA, serum amyloid protein; CCL21, chemokine (CC-motif) ligand 21; CXCL13, chemokine (C-X-C motif) ligand 13; CCL27, chemokine (CC-motif) ligand 27; CXCL5, chemokine (C-X-C motif) ligand 5; CCL11, chemokine (CC-motif) ligand 11; CCL24, chemokine (CC-motif) ligand 24; CCL26, chemokine (CC-motif) ligand 26; CX3CL1, chemokine (C-X3-C motif) ligand 1; CXCL6, chemokine (C-X-C motif) ligand 6; GM-CSF, Granulocyte-Macrophage Colony Stimulating Factor; CXCL1, chemokine (C-X-C motif) ligand 1; CXCL2, chemokine (C-X-C motif) ligand 2; CCL1, chemokine (CC-motif) ligand 1; IFN-γ, Interferon-gamma; IL-1β, Interleukin-1beta; IL-2, Interleukin-2; IL-4, Interleukin-4; IL-6, Interleukin-6; IL-8, Interleukin-8; IL-10, Interleukin-10; IL-16, Interleukin-16; CXCL10, chemokine (C-X-C motif) ligand 10; CXCL11, chemokine (C-X-C motif) ligand 11; CCL2, chemokine (CC-motif) ligand 2; CCL8, chemokine (CC-motif) ligand 8; CCL7, chemokine (CC-motif) ligand 7; CCL13, chemokine (CC-motif) ligand 13; CCL22, chemokine (CC-motif) ligand 22; MIF, macrophage migration inhibitory factor; CXCL9, chemokine (C-X-C motif) ligand 9; CCL3, chemokine (CC-motif) ligand 3; CCL15, chemokine (CC-motif) ligand 15; CCL20, chemokine (CC-motif) ligand 20; CCL19, chemokine (CC-motif) ligand 19; CCL23, chemokine (CC-motif) ligand 23; CXCL16, chemokine (C-X-C motif) ligand 16; CXCL12, chemokine (C-X-C motif) ligand 12; CCL17, chemokine (CC-motif) ligand 17; CCL25, chemokine (CC-motif) ligand 25; TNF-α, Tumor necrosis factor alpha.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
All methods were performed in accordance with the relevant guidelines and regulations. Written informed consents have been obtained from the parents of subjects under 16 years of age for this study, and has got ethics approval and consent by Research Ethics Committee of the Second Affiliated Hospital of Wenzhou Medical University. The Ethical Approval Number was LCKY2018-65.
Acknowledgments
We thank all the children and their families for participating in this study. Neither this paper nor any similar paper has been or will be submitted to or published in any other scientific journal.
Funding
This work was partially supported by grants from by the Natural Science Foundation of China (NSFC81601849), Zhejiang Provincial Medicine and Health Technology Project (2019RC217), Wenzhou Science and Technology Bureau (Y20180109, Y20180254).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Shane AL, Sanchez PJ, Stoll BJ. Neonatal sepsis. Lancet. 2017;390(10104):1770–1780. doi:10.1016/S0140-6736(17)31002-4
2. Popescu CR, Cavanagh MMM, Tembo B, et al. Neonatal sepsis in low-income countries: epidemiology, diagnosis and prevention. Expert Rev Anti Infect Ther. 2020;18(5):443–452. doi:10.1080/14787210.2020.1732818
3. Heron M. Deaths: leading Causes for 2017. Natl Vital Stat Rep. 2019;68(6):1–77.
4. Moni SC, Mollah AH, Banerjee M, Khan TH, Sejuti A, Morshed SS. Neonatal sepsis: clinical characteristics, epidemiology and antibiotic sensitivity pattern of the bacterial pathogens in neonatal intensive care unit of a tertiary care hospital. Mymensingh Med J. 2020;29(2):366–375.
5. Carty M, Guy C, Bowie AG. Detection of viral infections by innate immunity. Biochem Pharmacol. 2021;183:114316. doi:10.1016/j.bcp.2020.114316
6. Kogut MH, Lee A, Santin E. Microbiome and pathogen interaction with the immune system. Poult Sci. 2020;99(4):1906–1913. doi:10.1016/j.psj.2019.12.011
7. Kumar V. Toll-like receptors in sepsis-associated cytokine storm and their endogenous negative regulators as future immunomodulatory targets. Int Immunopharmacol. 2020;89(Pt B):107087. doi:10.1016/j.intimp.2020.107087
8. Kurt AN, Aygun AD, Godekmerdan A, Kurt A, Dogan Y, Yilmaz E. Serum IL-1beta, IL-6, IL-8, and TNF-alpha levels in early diagnosis and management of neonatal sepsis. Mediators Inflamm. 2007;2007:31397. doi:10.1155/2007/31397
9. Leal YA, Álvarez-Nemegyei J, Lavadores-May AI, Girón-Carrillo JL, Cedillo-Rivera R, Velazquez JR. Cytokine profile as diagnostic and prognostic factor in neonatal sepsis. J Matern Fetal Neonatal Med. 2019;32(17):2830–2836. doi:10.1080/14767058.2018.1449828
10. Wu YQ, Shen J, Zhou QL, Zhao HW, Liu LR, Liu X. Interleukin-6 and interleukin-8 in diagnosing neonatal septicemia. J Biol Regul Homeost Agents. 2016;30(4):1107–1113.
11. Badr HS, El-Gendy FM, Helwa MA. Serum stromal-derived-factor-1 (CXCL12) and its alpha chemokine receptor (CXCR4) as biomarkers in neonatal sepsis. J Matern Fetal Neonatal Med. 2018;31(16):2209–2215. doi:10.1080/14767058.2017.1336760
12. Tunc T, Cekmez F, Cetinkaya M, et al. Diagnostic value of elevated CXCR4 and CXCL12 in neonatal sepsis. J Matern Fetal Neonatal Med. 2015;28(3):356–361. doi:10.3109/14767058.2014.916683
13. Cuenca AG, Wynn JL, Kelly-Scumpia KM, et al. Critical role for CXC ligand 10/CXC receptor 3 signaling in the murine neonatal response to sepsis. Infect Immun. 2011;79(7):2746–2754. doi:10.1128/IAI.01291-10
14. Goldstein B, Giroir B, Randolph A. International pediatric sepsis consensus conference: definitions for sepsis and organ dysfunction in pediatrics. Pediatr Crit Care Med. 2005;6(1):2–8. doi:10.1097/01.PCC.0000149131.72248.E6
15. Dong Y, Basmaci R, Titomanlio L, Sun B, Mercier JC. Neonatal sepsis: within and beyond China. Chin Med J. 2020;133(18):2219–2228. doi:10.1097/CM9.0000000000000935
16. Machado JR, Soave DF, da Silva MV, de Menezes LB, Etchebehere RM, Monteiro ML. dos Reis MA, Correa RR, Celes MR: neonatal sepsis and inflammatory mediators. Mediators Inflamm. 2014;2014:269681. doi:10.1155/2014/269681
17. Stone MJ, Hayward JA, Huang C, Sanchez J, Sanchez J. Mechanisms of regulation of the chemokine-receptor network. Int J Mol Sci. 2017;18(2):342. doi:10.3390/ijms18020342
18. Manoura A, Gourgiotis D, Galanakis E, et al. Circulating concentrations of alpha- and beta-chemokines in neonatal sepsis. Int J Infect Dis. 2010;14(9):e806–809. doi:10.1016/j.ijid.2010.03.015
19. Liew PX, Kubes P. The neutrophil’s role during health and disease. Physiol Rev. 2019;99(2):1223–1248. doi:10.1152/physrev.00012.2018
20. Ohlsson K, Olsson AS. Immunoreactive granulocyte elastase in human serum. Hoppe Seylers Z Physiol Chem. 1978;359(11):1531–1539. doi:10.1515/bchm2.1978.359.2.1531
21. Shi Y, Li HQ, Shen CK, et al. Plasma nitric oxide levels in newborn infants with sepsis. J Pediatr. 1993;123(3):435–438. doi:10.1016/S0022-3476(05)81753-6
22. Wilson C, Kollmann T. Induction of antigen-specific immunity in human neonates and infants. In: The Window of Opportunity: Pre-Pregnancy to 24 Months of Age. Vol. 61. Karger Publishers; 2008:183–195.
23. Roger T, Schneider A, Weier M, et al. High expression levels of macrophage migration inhibitory factor sustain the innate immune responses of neonates. Proc Natl Acad Sci U S A. 2016;113(8):E997–E1005. doi:10.1073/pnas.1514018113
24. Kang I, Bucala R. The immunobiology of MIF: function, genetics and prospects for precision medicine. Nat Rev Rheumatol. 2019;15(7):427–437. doi:10.1038/s41584-019-0238-2
25. Sparkes A, De Baetselier P, Brys L, et al. Novel half-life extended anti-MIF nanobodies protect against endotoxic shock. FASEB J. 2018;32(6):3411–3422. doi:10.1096/fj.201701189R
26. Li T, Sun H, Li Y, et al. Downregulation of macrophage migration inhibitory factor attenuates NLRP3 inflammasome mediated pyroptosis in sepsis-induced AKI. Cell Death Discov. 2022;8(1):61. doi:10.1038/s41420-022-00859-z
27. Bozza FA, Gomes RN, Japiassu AM, et al. Macrophage migration inhibitory factor levels correlate with fatal outcome in sepsis. Shock. 2004;22(4):309–313. doi:10.1097/01.shk.0000140305.01641.c8
28. Emonts M, Sweep FC, Grebenchtchikov N, et al. Association between high levels of blood macrophage migration inhibitory factor, inappropriate adrenal response, and early death in patients with severe sepsis. Clin Infect Dis. 2007;44(10):1321–1328. doi:10.1086/514344
29. He M, Moochhala SM, Adhikari S, Bhatia M. Administration of exogenous fractalkine, a CX3C chemokine, is capable of modulating inflammatory response in cecal ligation and puncture-induced sepsis. Shock. 2009;31(1):33–39. doi:10.1097/SHK.0b013e31817789da
30. Hoogendijk AJ, Wiewel MA, van Vught LA, et al. Plasma fractalkine is a sustained marker of disease severity and outcome in sepsis patients. Crit Care. 2015;19(1):412. doi:10.1186/s13054-015-1125-0
31. Ancuta P, Rao R, Moses A, et al. Fractalkine preferentially mediates arrest and migration of CD16+ monocytes. J Exp Med. 2003;197(12):1701–1707. doi:10.1084/jem.20022156
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.