")
Back to Journals » Journal of Inflammation Research » Volume 15
Expression of PD-1 on Memory T Lymphocytes Predicts 28-Day Mortality of Patients with Sepsis: A Prospective Observational Study
Authors Liu Q , Xue M, Song Q, Xie J, Yang Y, Liu S
Received 9 June 2022
Accepted for publication 24 August 2022
Published 1 September 2022 Volume 2022:15 Pages 5043—5052
DOI https://doi.org/10.2147/JIR.S376897
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ning Quan
Qingxiang Liu,1 Ming Xue,1 Qianwen Song,1 Jianfeng Xie,1 Yi Yang,1 Songqiao Liu1,2
1Jiangsu Provincial Key Laboratory of Critical Care Medicine, Department of Critical Care Medicine, Zhongda Hospital, School of Medicine, Southeast University, Nanjing, 210009, People’s Republic of China; 2Department of Critical Care Medicine, Nanjing Lishui People’s Hospital, Zhongda Hospital Lishui Branch, Nanjing, People’s Republic of China
Correspondence: Yi Yang; Songqiao Liu, Email [email protected]; [email protected]
Background: PD-1 is an important immune checkpoint expressed on T lymphocytes and is associated with T-cell function in sepsis. However, the role of PD-1 in naive and memory T-cell responses in sepsis is not well understood. We aimed to determine the expression of PD-1 induced on naive and memory T lymphocytes in patients with sepsis and its association with clinical outcome.
Methods: A prospective observational study was conducted at a general intensive care unit (ICU). Whole blood samples were collected from patients within 48 h after sepsis diagnosis. PD-1 expression on naive and memory T cells was measured by flow cytometry. The levels of IFN-γ, IL-2 and TNF-α released by memory T cells were also determined. All patients were followed up to 28 days, and 28-day mortality was recorded.
Results: PD-1 expression showed no difference in naive CD4+ T cells (P=0.617) or naive CD8+ T cells (P=0.079) between survivors (n = 21) and nonsurvivors (n = 9). Increased PD-1 expression on memory CD4+ T cells was found in nonsurvivors (P=0.030) and memory CD8+ T cells (P=0.006) in comparison with survivors. According to the cutoff value of the percentage of PD-1 on memory CD8+ T cells in predicting 28-day mortality of patients with sepsis, patients were divided into two groups. The 28-day mortality rates between the two groups were significantly different (P=0.009). A Kaplan Meier curve was constructed to derive a hazard ratio of 9.33 (95% CI: 2.52– 34.60) for the percentage of PD-1 on memory CD8+ T cells regarding 28-day mortality. In addition, the IFN-γ secretion of memory CD4+ T cells (P=0.046) and IL-2 secretion of memory CD8+ T cells (P=0.014) were significantly greater in survivors than nonsurvivors.
Conclusion: Flow cytometric assessment of PD-1 expression on memory CD8+ T cells identifies patients with poor outcomes during sepsis.
Keywords: PD-1, memory T cells, sepsis, outcome
Background
Sepsis, caused by a dysregulated host response to infection, is a life-threatening condition with organ dysfunction.1 Approximately 270,000 to 370,000 people die from sepsis every year in the US, making sepsis the leading cause of death for patients with critical illness.2 In China, one-fifth of patients are admitted to the intensive care unit (ICU) with sepsis and the 90-day mortality rate is as high as 35.5%.3 The treatment of sepsis remains a major challenge, and there is currently no FDA-approved therapy for sepsis.4 Even if survival from the cytokine storm improves, previously septic individuals still face a higher risk of mortality, which defines the sepsis-induced immunosuppressive state.5,6
Sepsis-induced immunosuppression is characterized by an increased sensitivity to new infections unrelated to previous encounters.6 These severe lesions were sufficient to reduce 5-year survival in the septic cohort compared to the nonseptic cohort.7 T cells play an important role in the host immune response in sepsis. Sepsis-induced immunologic impairment is typified by a transient reduction in lymphocytes and a decrease in the potency of effector lymphocytes.8,9 Specifically, lymphopenia caused by sepsis affects both naive T cells and memory T cells. Memory T cells are more susceptible than naive T cells to sepsis-induced cell loss.10,11 Additionally, memory T cells that survived the cytokine storm were less able to respond to inflammatory signals,12 suggesting that memory T cells may be a crucial factor in the pathogenic mechanism of sepsis.
The balance of coinhibitory molecules and costimulatory molecule signals that T cells receive determines the fate of T-cell activation.13 Both naive and memory T cells are effectively regulated by ligation of inhibitory receptors on the cell surface,14 which have negative immune regulation in the T-cell response during sepsis.15–17 Programmed cell death 1 (PD-1) was found to be increased on the surface of T cells in patients with sepsis, rather than T cells from nonseptic controls,18 and blocking the PD-1/PD-L1 pathway may represent a potential therapeutic strategy for the amelioration of sepsis.19 However, the role of PD-1 in naive T cells and memory T cells in sepsis is not clear. Thus, we enrolled patients with sepsis and examined the expression of PD-1 on naive and memory T cells, to elucidate the relationship between PD-1 expression on naive and memory T cells and the outcome of septic patients.
Methods
Patients
A prospective observational study was conducted by enrolling consecutive adult patients admitted to the ICU of Zhongda Hospital affiliated to Southeast University from December 2021 to March 2022. The inclusion criterion was the presence of sepsis as defined by the Sepsis-3.0 criteria.1 The exclusion criteria included the following: patients younger than 18 years; pregnancy; patients with active malignancy, or chronic viral infection, such as HIV, hepatitis B or C; autoimmune diseases, use of corticosteroid therapy (except for previous use of prednisone <10 mg or equivalent per day); and length of stay in hospital lasting for more than 1 week before ICU admission or consent could not be obtained. All patients were evaluated after admission and administered therapy according to the 2016 international guidelines for the management of sepsis.4 The study was approved by Zhongda Hospital affiliated to Southeast University Ethics Committee (Southeast University, Nanjing, China, approval ID: 2020ZDSYLL041-Y01) and was in full compliance with the Declaration of Helsinki. Written informed consent was obtained from each patient or their legal representative prior to enrollment in the study.
Data Collection and Definition
Demographic characteristics including age, sex, height and weight were recorded at admission. Clinical features, including the source of infection, acute physiology and chronic health evaluation II (APACHE II) score, sequential organ failure assessment (SOFA) score and comorbidities were recorded. Inflammatory markers such as procalcitonin (PCT) and c-reactive protein (CRP) were also recorded. Records of mechanical ventilation (MV), continuous renal replacement therapy (CRRT) and vasopressor were collected. All patients were followed up to 28 days.
Flow Cytometry
Whole blood samples were collected from patients within 48h after sepsis diagnosis. Cells were identified by forward scatter (FSC) and side scatter (SSC) properties and lymphocytes were identified with anti-CD45-Alexa Fluor®700 (clone H130, BioLegend. USA), anti-CD4-FITC (clone RPA-T4, BioLegend. USA), anti-CD8-APC-H7 (clone SK1, BD PharmingenTM. USA), anti-CD62L-Brilliant Violet 605TM (clone DREG-56, BioLegend. USA), anti-CD45RO-Brilliant Violet 650TM (clone UCHL1, BioLegend. USA), anti-PD-1-BV786 (clone EH12.1, BD HorizonTM. USA), anti-CD28-Percp-cy5.5 (clone CD28.2, BioLegend. USA), anti-CD25-PE/DazzleTM594 (clone BC96, BioLegend. USA) and anti-TIGIT-Brilliant Violet 510TM (clone A15153G, BioLegend. USA) were used for surface staining and anti-CTLA-4-Brilliant Violet 421TM (clone BNI3, BioLegend. USA) was used for intracellular staining to determine T-cell phenotype. The gating strategy is shown in Figure 1A. CD45RO−CD62L+ T cells represent naive T cells in humans. CD62L−CD45RO+ T cells and CD62L+CD45RO+ T cells represent effector memory T cells and central memory T cells, respectively. PD-1 expression on memory T cells was defined using the PD-1 fluorescence minus one (FMO) strategy.
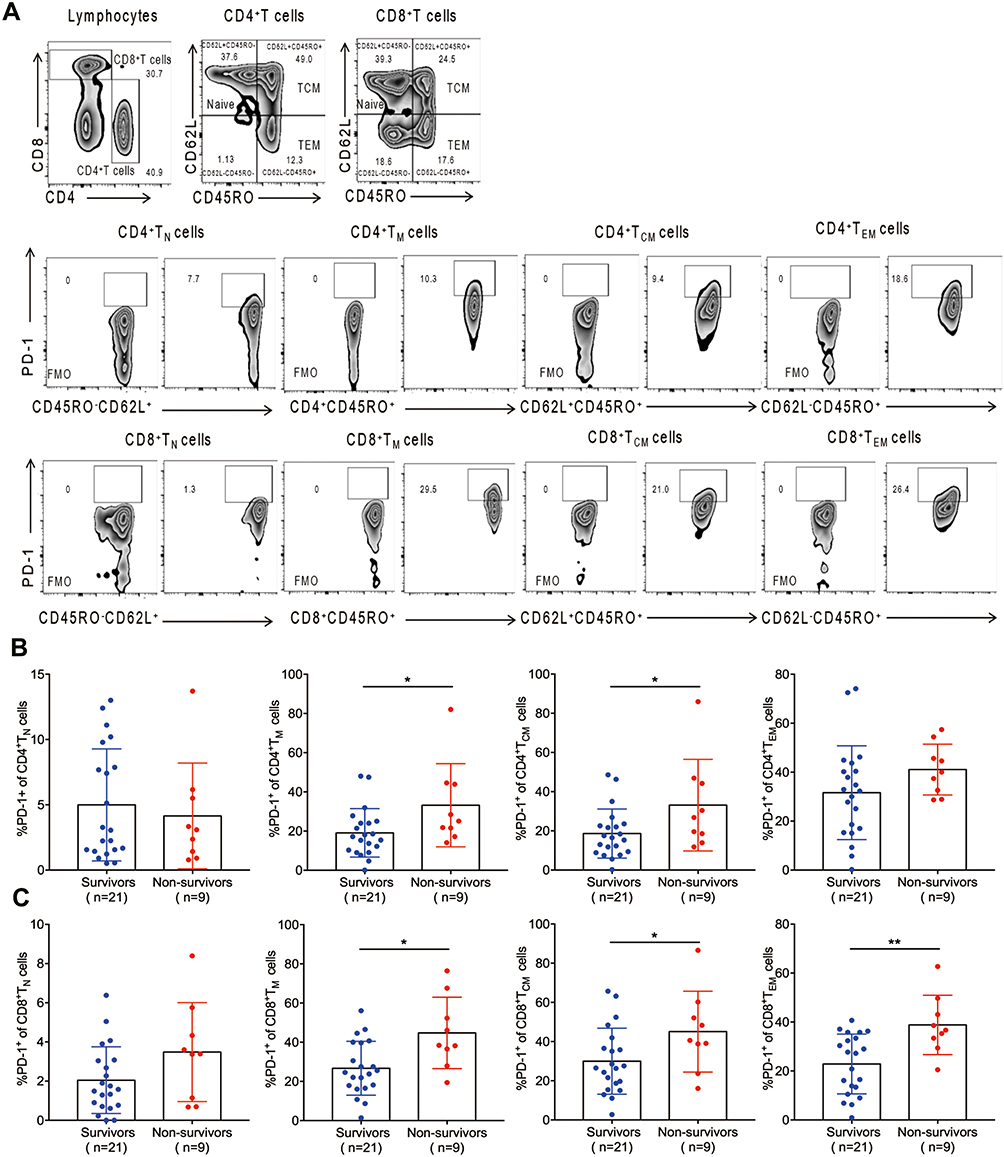 |
Figure 1 PD-1 expression on memory T cells was associated with 28-day mortality in septic patients. (A) Gating strategy used for flow cytometric analysis. (B) Percentage of PD-1 expression on naive CD4+ T cells, memory CD4+ T cells, central memory CD4+ T cells and effector memory CD4+ T cells between survivors and nonsurvivors. (C) Percentage of PD-1 expression on naive CD8+ T cells, memory CD8+ T cells, central memory CD8+ T cells and effector memory CD8+ T cells between survivors and nonsurvivors. *p < 0.05, **p < 0.01. |
For intracellular cytokine staining, 250 μL of blood was stimulated with cell activation cocktail (with brefeldin A) (eBioscience) for 5 h at 37°C. After this, the cells were stained with anti-CD45, anti-CD3-Percp-cy5.5 (clone OKT3, BioLegend. USA), anti-CD8 and anti-CD45RO, and then fixation and permeabilization solution (eBioscience) was used to permeabilize the cells. To stain intracellular cytokines, we used anti-IL-2-Brilliant Violet 510TM (clone MQ1-17H12, BioLegend. USA), anti-IFN-γ-Alexa Fluor® 488 (clone B27, BD PharmingenTM. USA) and anti-TNF-α-Brilliant Violet 421 (clone Mab11, BD PharmingenTM. USA). Samples were acquired using a BD FACSCelestaTM flow cytometer (BD Biosciences. USA). The data was analyzed using FlowJo software.
Statistical Analysis
Continuous variables with a normal distribution were presented as the mean and standard deviation (SD) and were compared with Student’s t test. Continuous variables with a skewed distribution were expressed as intermediate values within a quartile and were analyzed with the Mann–Whitney U-test. Categorical variables were expressed as frequencies and compared with the X2 test or Fisher’s exact test.
Receiver operating characteristic (ROC) curves were used to estimate the accuracy of the level of PD-1 expressed on memory T lymphocytes for 28-day mortality predictions with the area under the ROC (AuROC) curve and the cutoffs optimized using the Youden J statistic. Discrepancies in the 28-day mortality rates were analyzed with the Log rank test and expressed with Kaplan–Meier curves.
A P value <0.05 was considered as statistically significant. All statistical analyses were performed using SPSS 25 software (IBM SPSS, USA), MedCalc (version 19.6.1) and GraphPad Prism 7.0 (GraphPad Software, San Diego, USA).
Results
Patient Characteristics
A total of 66 patients with sepsis were screened and 30 patients were enrolled. One patient was pregnant. Additionally, 1 patient with hepatitis C virus infection, 8 patients with active malignancy, 1 patient with autoimmune disease, 3 patients who received the corticosteroid treatment and 22 patients who had been in the hospital for more than one week were excluded. The flow diagram of study patients is presented in Figure S1. The mean age of these patients was 64.70 ± 13.95 years and 21 (70.0%) of them were male. The most common comorbidity was hypertension (n = 15, 50.0%), followed by diabetes (n = 2, 7.0%). The leading cause of sepsis was abdominal infection (n = 14, 47.0%), followed by pulmonary infection (n = 13, 43.0%). All patients were followed up to 28 days, at which time there were 21 survivors and 9 nonsurvivors. The overall 28-day mortality was 30.0%.
The clinical characteristics of survivors and nonsurvivors are described in Table 1. There were no significant differences in age, sex, body mass index (BMI), comorbidities, source of infection, utilization rate of vasoactive drugs, mechanical ventilation and CRRT, SOFA score or APACHE II score between the survivors and nonsurvivors (P > 0.05 for each). Nonsurvivors had lower levels of PCT [ng/mL, 1.62 (0.57, 3.37) vs 8.73 (1.43, 16.96), P=0.041] (Table 1).
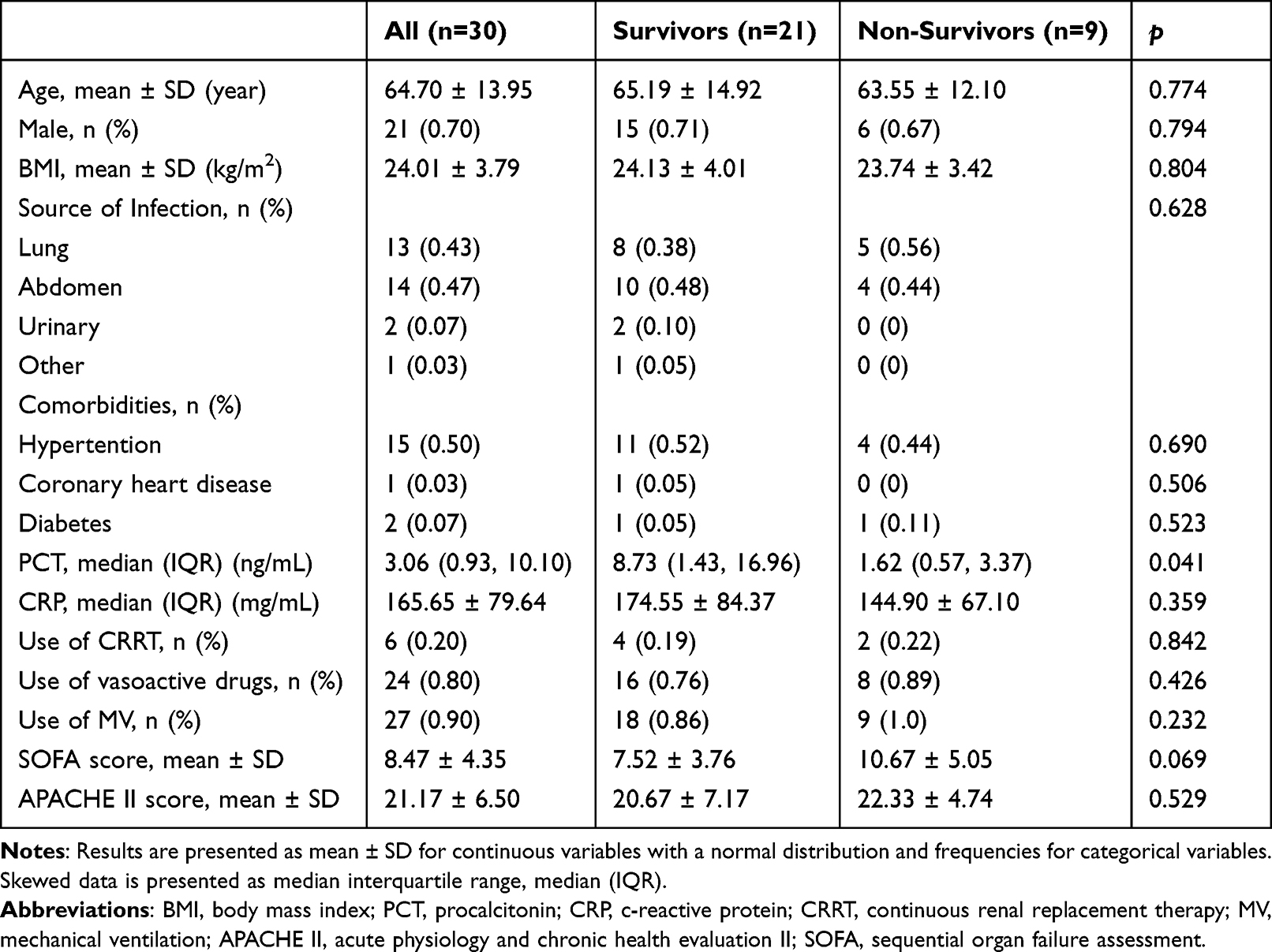 |
Table 1 Baseline Characteristics of the Patients According to 28-Day Survival |
PD-1 Expression on Memory T Cells in Surviving and Nonsurviving Patients with Sepsis
PD-1 expression on naive CD4+ T cells [%, 4.99 ± 0.94 vs 4.12 ± 1.35, P=0.617] and naive CD8+ T cells [%, 2.05 ± 0.37 vs 3.48 ± 0.84, P=0.079] showed no difference between survivors and nonsurvivors PD-1 expression on memory CD4+ T cells in the nonsurvivor group was significantly higher than that in the survivor group [%, 33.20 ± 7.08 vs 19.10 ± 2.70, P=0.030]. In particular, the percentage of PD-1 on central memory CD4+ T cells was significantly higher in nonsurvivors than survivors [%, 33.12 ± 7.79 vs 18.61 ± 2.73, P=0.034], while the percentage of PD-1 on effector memory CD4+ T cells showed no difference between two groups (P=0.177) (Figure 1B). The proportion of PD-1 on memory CD8+ T cells was significantly increased in nonsurvivors compared to survivors [%, 44.77 ± 6.08 vs 26.71 ± 3.00, P=0.006]. Both PD-1 expression on central memory CD8+ T cells [%, 45.06 ± 6.88 vs 29.97 ± 3.67, P=0.044] and effector memory CD8+ T cells [%, 38.82 ± 4.04 vs 22.86 ± 2.70, P=0.003] were increased in patients who died within 28 days after sepsis compared to survivors (Figure 1C).
The Percentage of PD-1 on Memory T Cells Was Associated with 28-Day Mortality in Sepsis
An ROC curve was subsequently used to evaluate the predictability of the percentage of PD-1 on memory CD4+ T cells on 28-day mortality in patients with sepsis, which yielded an AuROC of 0.712 (95% CI: 0.518–0.861; P=0.033). A cutoff of 21.4% was calculated using the J statistics with a sensitivity of 77.78 and a specificity of 61.90 (Figure 2A). Additionally, an ROC analysis of the percentage of PD-1 on memory CD8+ T cells on 28-day mortality yielded an AuROC of 0.757 (95% CI: 0.566–0.894; P=0.007). A cutoff of 27.5% was calculated, with a sensitivity of 88.89 and a specificity of 61.90 (Figure 2B).
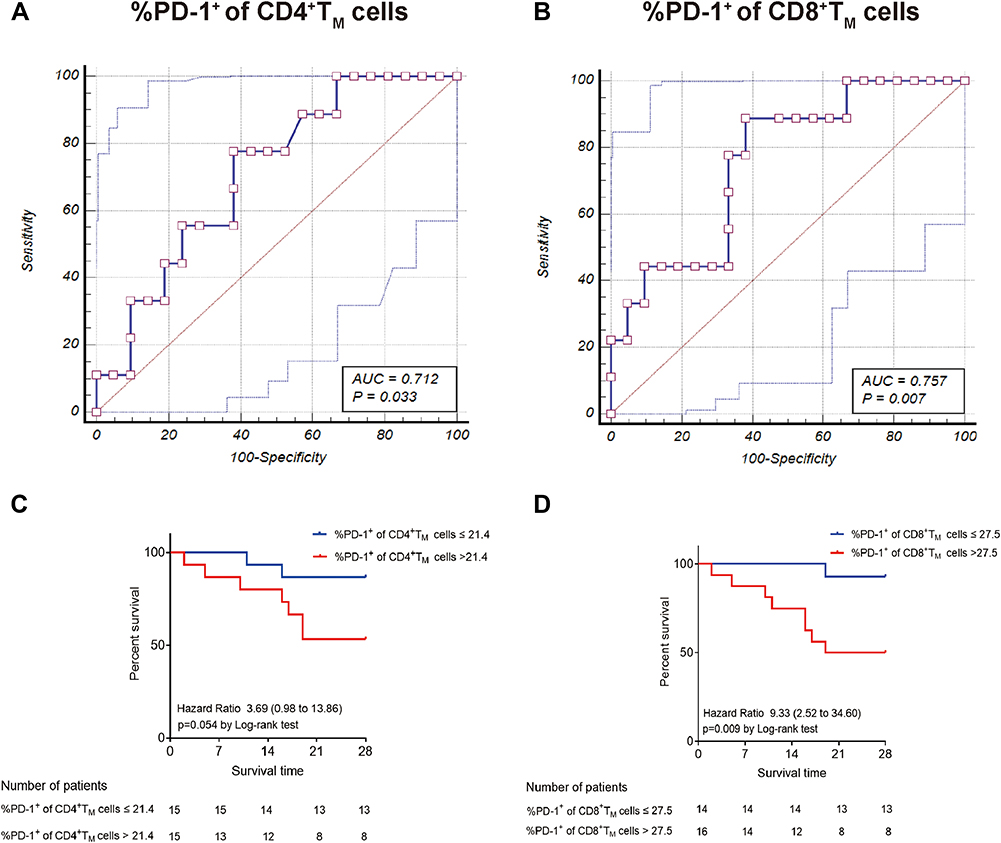 |
Figure 2 The expression of PD-1 on memory T cells predicts 28-day mortality during sepsis. (A and B) ROC analysis of the percentage of PD-1+ on memory CD4+ T cells and memory CD8+ T cells predicting 28-day mortality in septic patients. (C) Kaplan-Meier analysis of survival probability in septic patients with PD-1+ of CD4+ TM >21.4% vs ≤21.4%. (D) Kaplan-Meier analysis of survival probability in septic patients with PD-1+ of CD8+ TM >27.5% vs ≤27.5%. |
The patients were divided into “high” and “low” PD-1 expression on memory CD4+ T cells groups according to the optimized 21.4% cutoff level. According to the Log rank test, the 28-day mortality rates between the “high” and “low” groups showed no difference (P=0.054), and the Kaplan–Meier curve was elaborated to derive a hazard ratio of 3.69 (95% CI: 0.98–13.86) for percentage of PD-1 on memory CD4+ T cells regarding 28-day mortality (Figure 2C). The patients were divided into two groups according to the optimized 27.5% cutoff level of percentage of PD-1 on memory CD8+ T cells for predicting 28-day mortality in septic patients. According to the Log rank test, the 28-day mortality rates between the two groups were significantly different (P=0.009), and the Kaplan–Meier curve was also elaborated to derive a hazard ratio of 9.33 (95% CI: 2.52–34.60) for the proportion of PD-1 on memory CD8+ T cells regarding 28-day mortality (Figure 2D).
Further immunophenotyping of human PD-1+ memory CD4+ T cells revealed that these cells had a phenotype with increased CTLA-4 mean fluorescence intensity (MFI) (1551.00 ± 198.90 vs 1001.00 ± 99.58, P=0.017), and TIGIT MFI (490.80 ± 18.34 vs 371.00 ± 19.23, P<0.001) and decreased CD25 MFI (389.80 ± 58.99 vs 632.20 ± 82.48, P=0.020) compared to PD-1− memory CD4+ T cells (Figure 3A). Immunophenotyping of human PD-1+ memory CD8+ T cells revealed that these cells had a phenotype with increased TIGIT MFI (554.00 ± 15.23 vs 436.80 ± 19.74, P<0.001) and CD28 MFI (4959.00 ± 438.40 vs 3495.00 ± 431.30, P=0.021) compared to PD-1− memory CD8+ T cells (Figure 3B). Overall, these results highlighted the important role of PD-1 in memory T cells during sepsis.
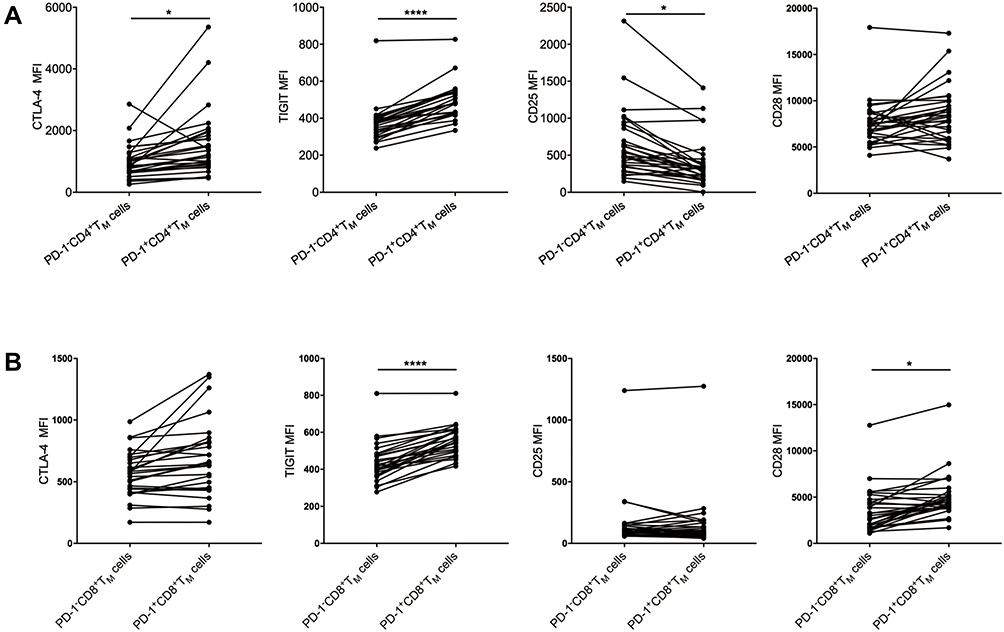 |
Figure 3 CD28, CD25, CTLA-4 and TIGIT MFI of PD-1− and PD-1+ memory T cells from septic patients. (A) CD28 MFI, CD25 MFI, CTLA-4 MFI and TIGIT MFI of PD-1−CD4+TM cells and PD-1+CD4+TM cells. (B) CD28 MFI, CD25 MFI, CTLA-4 MFI and TIGIT MFI of PD-1−CD8+ TM cells and PD-1+CD8+ TM cells. *p < 0.05, ****p < 0.0001. Abbreviation: MFI, mean fluorescence intensity. |
Cytokine Secretion of Memory T Cells in Patients with Sepsis
To determine whether memory T cells exhibit deficiency in cytokine secretion between survivor group and nonsurvivor group, we analyzed the cytokine secretion of IFN-γ, IL-2 and TNF-α from memory CD4+ T cells and memory CD8+ T cells of septic patients in our study (Figure 4A). We found that the ability of IFN-γ secretion of memory CD4+ T cells was significantly increased in 28-day survivors compared with nonsurvivors [%, 16.51 ± 1.84 vs 9.59 ± 2.69, P=0.046]. However, IL-2 and TNF-α secretion by memory CD4+ T cells showed no difference between the two groups (Figure 4B). In 28-day survivors, there was a significant increase in the ability of IL-2 secretion by memory CD8+ T cells [%, 23.83 ± 3.23 vs 10.34 ± 1.90, P=0.014], while IFN-γ and TNF-α secretion by memory CD8+ T cells showed no difference between the two groups (Figure 4C).
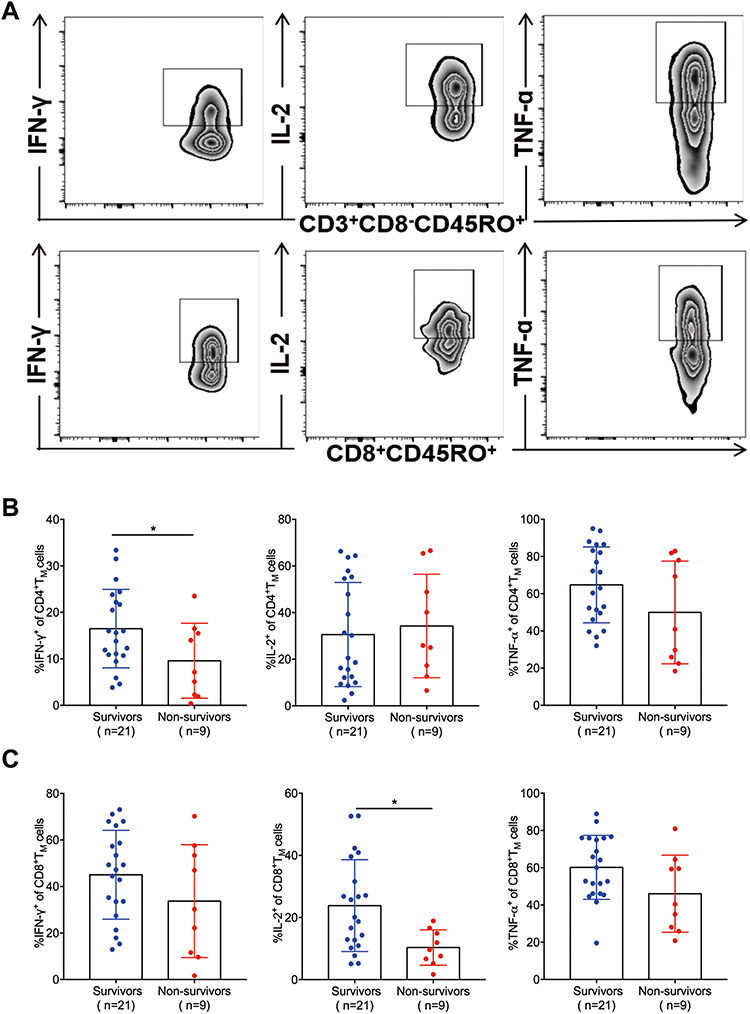 |
Figure 4 Functional characterization of memory T cells in patients with sepsis. (A) Representative levels of the cytokines IFN-γ, IL-2 and TNF-α secreted by memory CD3+CD8− T cells and memory CD8+ T cells. (B) IFN-γ, IL-2 and TNF-α secretion of memory CD3+CD8− T cells between survivors and nonsurvivors. (C) IFN-γ, IL-2 and TNF-α secretion of memory CD8+ T cells between survivors and nonsurvivors. *p < 0.05. |
Discussion
In this study, we evaluated the expression of PD-1 on naive and memory T cells in a cohort of patients with sepsis, and found that PD-1 on memory CD4+ T cells and CD8+ T cells was significantly elevated in 28-day nonsurvivors in comparison with 28-day survivors, while PD-1 expression showed no difference between survivors and nonsurvivors on naive CD4+ T cells and naive CD8+ T cells. The cytokine secretion of memory T cells was significantly decreased in nonsurvivors.
Growing evidence suggests that alterations in the T-cell repertoire can lead to dysfunction of the immune system during sepsis.20,21 Long-term immunity is provided by memory T cells, and damage to memory T cells resulting from sepsis can make patients susceptible to reinfection. In a preclinical study, Serbanescu and Xie found that there were significant reductions in memory CD4+ T-cells numbers and memory CD8+ T-cell numbers following CLP,10,22 revealing the importance of memory T cells in the pathogenesis of sepsis.
The balance of coinhibitory and costimulatory molecules is critical to determine T-cell function during infection. Numerous studies have proven that coinhibitory markers such as PD-1 are highly expressed on T cells, and are associated with T-cell apoptosis during sepsis.23–25 That anti-PD-1/PD-L1 has been shown to improve survival in cecal ligation and puncture (CLP) model mice and has entered clinical trials in patients with sepsis.26–28 Our study first reported that it is memory CD4+ T cells and memory CD8+ T cells, rather than naive CD4+ T cells and naive CD8+ T cells, that played critical role in PD-1 mediating signaling in sepsis. This was based on the following findings: the percentage of PD-1 on naive CD4+ T cells and CD8+ T cells between survivors and nonsurvivors showed no difference; however, PD-1 expression on memory CD4+ T cells and CD8+ T cells of sepsis patients who died within 28 days were significantly higher than that of patients survived. And proportion of PD-1 on memory CD8+ T cells can serve as a prognostic marker for patients with sepsis as defined by the Sepsis-3 criteria. Because the area under the ROC of PD-1+ memory CD8+ T cells on 28-day mortality of septic patients was 0.757, the 28-day mortality was higher and the survival time was shorter in patients with a higher percentage of PD-1 on memory CD8+ T lymphocytes.
Memory T cells can be further divided into central memory T cells and effector memory T cells, two subsets with different characteristics. We found that PD-1 expression was increased on central memory CD4+ T cells in nonsurvivors compared to survivors, while it showed no difference on effector memory CD4+ T cells. PD-1 expression on central memory and effector memory CD8+ T cells was different from that on CD4+ T cells, as it increased both on central memory and effector memory CD8+ T cells between the two groups. Different subsets of memory T cells play different roles, and subdivision of these cells can help us to identify the cell subpopulation that matters.
Our study first analyzed the immune phenotypes of PD-1+ memory T cells and PD-1− memory T cells. We found that human PD-1+ memory CD4+ T cells showed an exhausted phenotype with increased TIGIT MFI, CTLA-4 MFI and decreased CD25 MFI versus PD-1− memory CD4+ T cells. And PD-1+ memory CD8+ T cells exhibited increased TIGIT MFI and CD28 MFI compared to PD-1− memory CD8+ T cells. Understanding the impact of PD-1 signaling on a subset of memory T cells remains an important goal since memory T cells are more susceptible than naive T cells to sepsis induced attrition.10
Multiple cytokines, including IFN-γ, IL-2 and TNF-α, have been identified as key regulators in T-cell activation, with the ability to trigger T-cell activation response in a TCR-independent manner.29 Studies have revealed that the transcriptional profile and chromatin accessibility are altered in memory T cells from sepsis survivors, leading to decreased T-cell cytokine secretion and reduced infection control,30 which is consistent with our results. We found that the level of IL-2 released by memory CD8+ T cells and the level of IFN-γ released by memory CD4+ T cells of nonsurvivors were significantly decreased, which may abrogate the response of T cells to infection.
This clinical study also had several limitations. This was a single-center prospective and observational study, and the sample size of this study was limited, which led to false-positive results. Additionally, the proportion of PD-1 on memory T cells was measured at one time point rather than being consecutively monitored.
Conclusion
Increased expression of PD-1 on memory T cells was associated with 28-day mortality in patients with sepsis. Moreover, in nonsurvivors, the cytokine secretion of memory T cells was reduced.
Data Sharing Statement
All the data are illustrated in the figures and in the Supplementary Data.
Ethics Approval
The study was approved by the Zhongda Hospital affiliated to Southeast University Ethics Committee (Southeast University, Nanjing, China, 2020ZDSYLL041-Y01). Informed consent was obtained from each patient or their legal representative prior to enrollment in the study.
Acknowledgment
We thank the patients enrolled in this study, physicians and nurses working in the ICU in Zhongda Hospital affiliated to Southeast University.
Funding
This work was supported, in part, by grant from the National Natural Science Foundation of China (81971888; 81971885; 82072155).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Singer M, Deutschman CS, Seymour CW., et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
2. Rhee C, Dantes R, Epstein L, et al. Incidence and trends of sepsis in US hospitals using clinical vs claims data, 2009-2014. JAMA. 2017;318(13):1241–1249. doi:10.1001/jama.2017.13836
3. Xie J, Wang H, Kang Y, et al. The epidemiology of sepsis in Chinese ICUs: a national cross-sectional survey. Crit Care Med. 2020;48(3):e209–e218.
4. Rhodes A, Evans LE, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017;43(3):304–377.
5. Hotchkiss RS, Monneret G, Payen D. Sepsis-induced immunosuppression: from cellular dysfunctions to immunotherapy. Nat Rev Immunol. 2013;13(12):862–874.
6. Delano MJ, Ward PA. The immune system’s role in sepsis progression, resolution, and long-term outcome. Immunol Rev. 2016;274(1):330–353.
7. Donnelly JP, Hohmann SF, Wang HE. Unplanned readmissions after hospitalization for severe sepsis at academic medical center-affiliated hospitals. Crit Care Med. 2015;43(9):1916–1927.
8. Hotchkiss RS, Tinsley KW, Swanson PE, et al. Sepsis-induced apoptosis causes progressive profound depletion of B and CD4+ T lymphocytes in humans. J Immunol. 2001;166(11):6952–6963.
9. Jensen IJ, Sjaastad FV, Griffith TS, et al. Sepsis-induced T cell immunoparalysis: the ins and outs of impaired T cell immunity. J Immunol. 2018;200(5):1543–1553.
10. Serbanescu MA, Ramonell KM, Hadley A, et al. Attrition of memory CD8 T cells during sepsis requires LFA-1. J Leukoc Biol. 2016;100(5):1167–1180. doi:10.1189/jlb.4A1215-563RR
11. Condotta SA, Rai D, James BR, et al. Sustained and incomplete recovery of naive CD8 + T cell precursors after sepsis contributes to impaired CD8 + T cell responses to infection. J Immunol. 2013;190(5):1991–2000. doi:10.4049/jimmunol.1202379
12. Condotta SA, Khan SH, Rai D, et al. Polymicrobial sepsis increases susceptibility to chronic viral infection and exacerbates CD8 + T cell exhaustion. J Immunol. 2015;195(1):116–125. doi:10.4049/jimmunol.1402473
13. Chen L, Flies DB. Molecular mechanisms of T cell co-stimulation and co-inhibition. Nat Rev Immunol. 2013;13(4):227–242. doi:10.1038/nri3405
14. McKinney EF, Lee JC, Jayne DRW, et al. T-cell exhaustion, co-stimulation and clinical outcome in autoimmunity and infection. Nature. 2015;523(7562):612–616. doi:10.1038/nature14468
15. Parry RV, Chemnitz JM, Frauwirth KA, et al. CTLA-4 and PD-1 receptors inhibit T-cell activation by distinct mechanisms. Mol Cell Biol. 2005;25(21):9543–9553. doi:10.1128/MCB.25.21.9543-9553.2005
16. Shindo Y, Unsinger J, Burnham C, et al. Interleukin-7 and anti–programmed cell death 1 antibody have differing effects to reverse sepsis-induced immunosuppression. Shock. 2015;43(4):334–343. doi:10.1097/SHK.0000000000000317
17. Morrow KN, Liang Z, Xue M, et al. The IL-27 receptor regulates TIGIT on memory CD4+ T cells during sepsis. iScience. 2021;24(2):102093. doi:10.1016/j.isci.2021.102093
18. Niu B, Zhou F, Su Y, et al. Different Expression Characteristics of LAG3 and PD-1 in Sepsis and Their Synergistic Effect on T cell Exhaustion: A New Strategy for Immune Checkpoint Blokade. Front Immunol. 2019;10:1888. doi:10.3389/fimmu.2019.01888
19. Hotchkiss RS, Colston E, Yende S, et al. Immune checkpoint inhibition in sepsis: a Phase 1b randomized study to evaluate the safety, tolerability, pharmacokinetics, and pharmacodynamics of nivolumab. Intensive Care Medicine. 2019;45(10):1360–1371. doi:10.1007/s00134-019-05704-z
20. Ramonell KM, Zhang W, Hadley A, et al. CXCR4 blockade decreases CD4+ T cell exhaustion and improves survival in a murine model of polymicrobial sepsis. PLoS One. 2017;12(12):e188882. doi:10.1371/journal.pone.0188882
21. van der Poll T, van de Veerdonk FL, Scicluna BP, et al. The immunopathology of sepsis and potential therapeutic targets. Nat Rev Immunol. 2017;17(7):407–420.
22. Xie J, Crepeau RL, Chen CW, et al. Sepsis erodes CD8(+) memory T cell-protective immunity against an EBV homolog in a 2B4-dependent manner. J Leukoc Biol. 2019;105(3):565–575.
23. Boomer JS, Shuherk-Shaffer J, Hotchkiss RS, et al. A prospective analysis of lymphocyte phenotype and function over the course of acute sepsis. Crit Care. 2012;16(3):R112.
24. Xie J, Chen C, Sun Y, et al. Increased attrition of memory T cells during sepsis requires 2B4. JCI Insight. 2019;4(9):548.
25. Bu Y, Wang H, Ma X, et al. Untargeted metabolomic profiling of the correlation between prognosis differences and PD-1 expression in sepsis: a preliminary study. Front Immunol. 2021;12:594270.
26. Thampy LK, Remy KE, Walton AH, et al. Restoration of T cell function in multi-drug resistant bacterial sepsis after interleukin-7, anti-PD-L1, and OX-40 administration. PLoS One. 2018;13(6):e199497.
27. Hotchkiss RS, Colston E, Yende S, et al. Immune checkpoint inhibition in sepsis: a phase 1b randomized, placebo-controlled, single ascending dose study of antiprogrammed cell death-ligand 1 antibody (BMS-936559). Crit Care Med. 2019;47(5):632–642.
28. Brahmamdam P, Inoue S, Unsinger J, et al. Delayed administration of anti-PD-1 antibody reverses immune dysfunction and improves survival during sepsis. J Leukoc Biol. 2010;88(2):233–240.
29. Freeman BE, Hammarlund E, Raue HP, et al. Regulation of innate CD8+ T-cell activation mediated by cytokines. Proc Natl Acad Sci U S A. 2012;109(25):9971–9976.
30. Jensen IJ, Li X, McGonagill PW, et al. Sepsis leads to lasting changes in phenotype and function of memory CD8 T cells. Elife. 2021;1:10.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.