")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Exposure to Atmospheric Ozone Disruption and Altitude Over 3500 m.a.s.l. are Associated with a Higher Prevalence of Photodermatoses in Pediatric Population of High-Altitude in Peru
Authors Ramos W , Gutierrez EL , De La Cruz-Vargas JA , Díaz J, Hurtado J, Ronceros G, de Vries E
Received 16 May 2022
Accepted for publication 12 August 2022
Published 31 August 2022 Volume 2022:15 Pages 1779—1786
DOI https://doi.org/10.2147/CCID.S374884
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Willy Ramos,1,2 Ericson L Gutierrez,1,3 Jhony A De La Cruz-Vargas,1 Jesús Díaz,4 Jorge Hurtado,2 Gerardo Ronceros,2 Esther de Vries5
1Instituto de Investigaciones en Ciencias Biomédicas (INICIB), Universidad Ricardo Palma, Lima, Perú; 2Instituto de Investigaciones Clínicas, Universidad Nacional Mayor de San Marcos, Lima, Perú; 3Centro Nacional de Salud Pública, Instituto Nacional de Salud, Lima, Perú; 4Universidad Católica Santo Toribio de Mogrovejo, Chiclayo, Perú; 5Departamento de Epidemiologia Clínica y Bioestadística, Pontificia Universidad Javeriana, Bogotá, Colombia
Correspondence: Willy Ramos, Instituto de Investigaciones en Ciencias Biomédicas (INICIB), Universidad Ricardo Palma, Av. Alfredo Benavides 5440, Santiago de Surco, Lima, 15039, Perú, Email [email protected]
Objective: To determine if exposure to atmospheric ozone disruption and other factors are associated with photodermatoses in the high-altitude pediatric population in Peru.
Materials and Methods: A cross-sectional study based on data obtained from studies of dermatological diseases among the population exposed to mine tailings in Peru which included children under the age of 18 in 6 population centers located over 2500 meters above sea level (m.a.s.l). We evaluated the presence of photodermatoses and possible associated factors obtaining the adjusted odds ratio (aOR) and confidence intervals (CI).
Results: 594 children below the age of 18 participated in this study, 53.0% girls, the average age was 10.4 ± 4.1 years. 51.3% were exposed to a mini hole in the ozone layer, 60.1% resided at an altitude over 3500 m.a.s.l and 51.9% presented cutaneous manifestations of atopy upon physical examination. The prevalence of photodermatoses was 64.8%, of which the most frequent were actinic prurigo (49.3%), pityriasis alba (18.5%) and actinic cheilitis (4.4%). The multivariate analysis found that residing in a region exposed to the mini hole in the ozone layer (aOR = 4.23; CI 95%: 2.32– 7.72) and residing at an altitude over 3500 m.a.s.l (aOR = 2.76; CI 95%: 1.57– 4.86) were both independent associated factors to photodermatoses.
Conclusion: A high prevalence of photodermatoses exists among the pediatric population living at high-altitude in Peru. Residing in a region exposed to a mini hole in the ozone layer and residing over 3500 m.a.s.l constituted associated factors.
Keywords: ultraviolet rays, ozone depletion, high-altitude, children, adolescents
Plain Language Summary
What is Already Known on This Topic
Arequipa is a department of Peru exposed to a mini hole in the ozone layer. Several studies identified mini holes in the ozone layer from a geophysical and atmospheric standpoint; but very few linked those holes directly with human pathology.
What This Study Adds
This study shows the high prevalence of photodermatoses among children and adolescents in high-altitude populations. The exposure to the mini hole in the ozone layer and residing at an elevation over 3500 meters above sea level (m.a.s.l) are associated factors for photodermatoses.
How This Study Might Affect Research, Practice or Policy
It is important to implement educational interventions, but also to install sun protection measures, based on a budget policy and allocation that makes them sustainable, particularly in the higher risk zones.
Introduction
Exposure to ultraviolet radiation (UVR) produces direct cell damage to DNA, genetic mutations, production of reactive oxygen species (ROS), immunosuppression and inflammatory response, which play a major role in photoaging and the pathogenesis of skin cancer. Ultraviolet A (UVA: 320–360 nm) has a relatively low energy, is able to penetrate the dermis, interact with cells and stimulate melanin production. Ultraviolet B (UVB: 290–320 nm) has a much higher energy and is able to penetrate the dermis, causing most skin lesions of immediate perception, although 90% of which is filtered out by the ozone layer before reaching the Earth's surface. Ultraviolet C (UVC: 200–290 nm) has a very high energy but is completely filtered by the ozone layer and never reaches the Earth’s surface.1–3
Exposure to UVR during infancy and adolescence contributes to the risk of skin cancer (both melanoma and non-melanoma).4,5 It is estimated that 25–33% of cumulative sun exposure in one person’s lifetime occurs before the age of 18, mainly in schools and through outdoor recreational activities. Unlike adults, children have a low risk of presenting skin damage related to UV radiation; however, the most common conditions related to UVR occur within the first two decades of life, such as erythema, sunburn, photodermatoses and photosensitivity.4–6 Exposure to the sun between the hours of 10 am and 4 pm, performing outdoor activities, fair skin, high-altitude, latitude proximity to the equator and clear skies all contribute to the accumulation of UVR exposure.1,2,7,8
Arequipa is a department located approximately 1000 km south of Lima, the capital of Peru. Most of its geography is occupied by the Andes mountains, located at an altitude over 2500 m.a.s.l with a predominantly dry climate. It is estimated that Arequipa city (capital of the department of Arequipa) has an average of 300 sunny days per year and 4000 hours of sun exposure per year.9 This department is exposed to a mini hole in the ozone layer which was detectable through the satellite measures performed by the National Aeronautics and Space Administration (NASA) with the Total Ozone Mapping Spectrometer (TOMS) and the Ozone Monitoring Instrument (OMI) which allowed a daily mapping of the atmospheric ozone distribution around the planet.10–12 The areas exposed to the mini hole exhibit ozone concentrations that vary between 200 and 225 Dobson units (DU) compared to other regions of the country where the ozone concentrations vary between 225 and 275 DU due to its proximity to the equator12 (Figure 1). This mini hole constitutes a natural phenomenon characterized by the local and transient reduction in the total column ozone which produces an intermittent exposure of the population to extreme values of UVB radiation; as UVA is not filtered by the ozone layer UVA levels should not be influenced.13–17
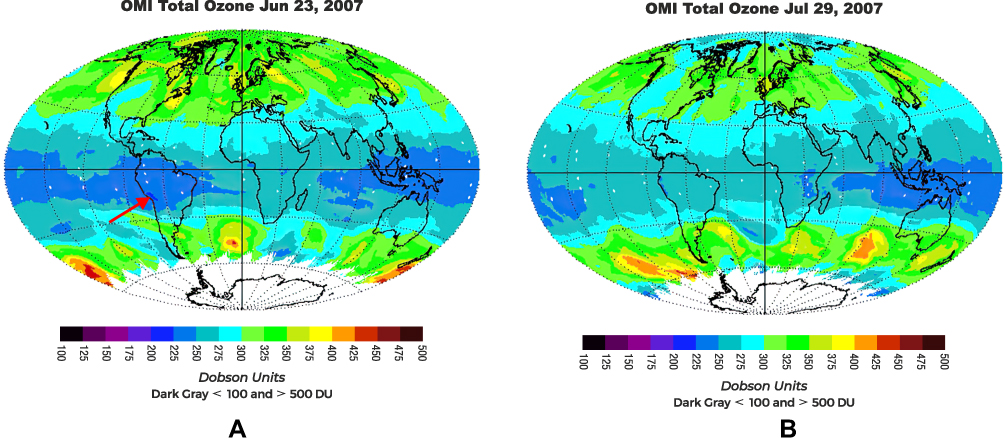 |
Figure 1 Ozone concentration satellite images. (A) Mini hole in the ozone layer which includes Arequipa (red arrow). (B) Disappearance of the mini hole days later. |
Another factor that could be relevant for the presence of photodermatoses is the altitude. Populations residing in high-altitude areas, as a large proportion of the Peruvian population along the Andes Mountains, receive higher doses of UVR: as altitude increases, the exposure to UVR, UVA as well as UVB exposures increase.18
The objective of this current study was to determine if exposure to atmospheric ozone disruption and other factors are associated to photodermatoses in the high-altitude pediatric population in Peru.
Materials and Methods
Between 2003 and 2008, several studies were conducted on skin diseases associated with chronic exposure to metals from mining environmental liabilities (mine tailings) in populations living at high-altitude (Arequipa and Lima). Participants (children, adolescents and adults) underwent a clinical dermatological exam during these studies; and photodermatoses was recorded.19,20
A cross-sectional study was conducted from the data obtained from studies on skin diseases in populations exposed and not exposed to mine tailings.19,20 For this study, we included all children and adolescents (under the age of 18), habitual residents of the population center of origin. Those who had lived away from their birth town for more than 6 months, as well as those from whom we did not obtain the parental consent nor agreement of the minor were excluded from analyses.
Patient recruitment took place in 6 population centers of high altitude (>2500 m.a.s.l) exposed to mine tailings. Home visits were performed to all dwellings in the population center, during which the study objectives were explained to parents and their children were invited to participate. Some under-aged children were not captured during the home visits; they were recruited in public educational institutions. Each participant was examined by a dermatologist for the presence of dermatological diseases and abnormalities, including photodermatoses. Prevalence of photodermatoses was calculated from these data.
For the purpose of the study, we included the immunologically mediated photodermatoses (idiopathic), drug-and-chemically induced photosensitivity, defective DNA repair disorders, and photoaggravated dermatoses within photodermatoses, according to the classification proposed by Lim and Hawk adapted by Bylaite.21
Data of factors potentially associated with photodermatoses were obtained, such as residing in an area exposed to the mini hole in the ozone layer, living at altitudes over 3500 m.a.s.l, age, sex and the presence of cutaneous manifestations of atopy. Participants were considered exposed to the mini hole in the ozone layer if they resided in the department of Arequipa where the NASA satellite images evidenced an ozone mini hole in comparison to those who lived in the department of Lima, where the satellite images did not evidence the existence of a mini hole.
Statistical analyses were conducted with the SPSS 25 program for Windows. A univariate statistic was performed based on obtaining frequencies, percentages, measures of central tendency and dispersion. Bivariate statistics were performed with Pearson’s chi-square test and Fisher’s exact test, obtaining crude odds ratios (OR) for factors potentially associated with photodermatoses. Multivariate binary logistic regression models were built with the INTRO procedure, the respective adjusted odds ratio (aOR) and confidence intervals (CI) were calculated. The calculations were performed with a confidence level of 95%.
The Ethics Committees of the Dos de Mayo National Hospital (Lima-Peru) and the Carlos Alberto Seguín Escobedo National Hospital (Arequipa-Perú) approved the original studies.19,20 This study was approved by the Ethics Committee of the Faculty of Medicine of the Ricardo Palma University, Lima-Peru (Expedited review, Code PI-002-2022). We guaranteed confidentiality of the information obtained, which was only used for the purpose of this study. The authors confirm that the guidelines outlined in the Declaration of Helsinki were followed.
Results
Of a total of 639 eligible minors under the age of 18, 28 were excluded because their parents did not give consent for their participation in the study and 17 for residing more than 6 months outside their hometown. 594 minors under the age of 18 were included, with an average age of 10.4 ± 4.1 years (median 11 years), 53% of them girls. Their characteristics are summarized in Table 1. Slightly more than half (51.3%) of the children were exposed to a mini hole in the ozone layer and 60.1% resided at an elevation greater than 3500 m.a.s.l. 51.9% showed cutaneous manifestations of atopy upon clinical examination.
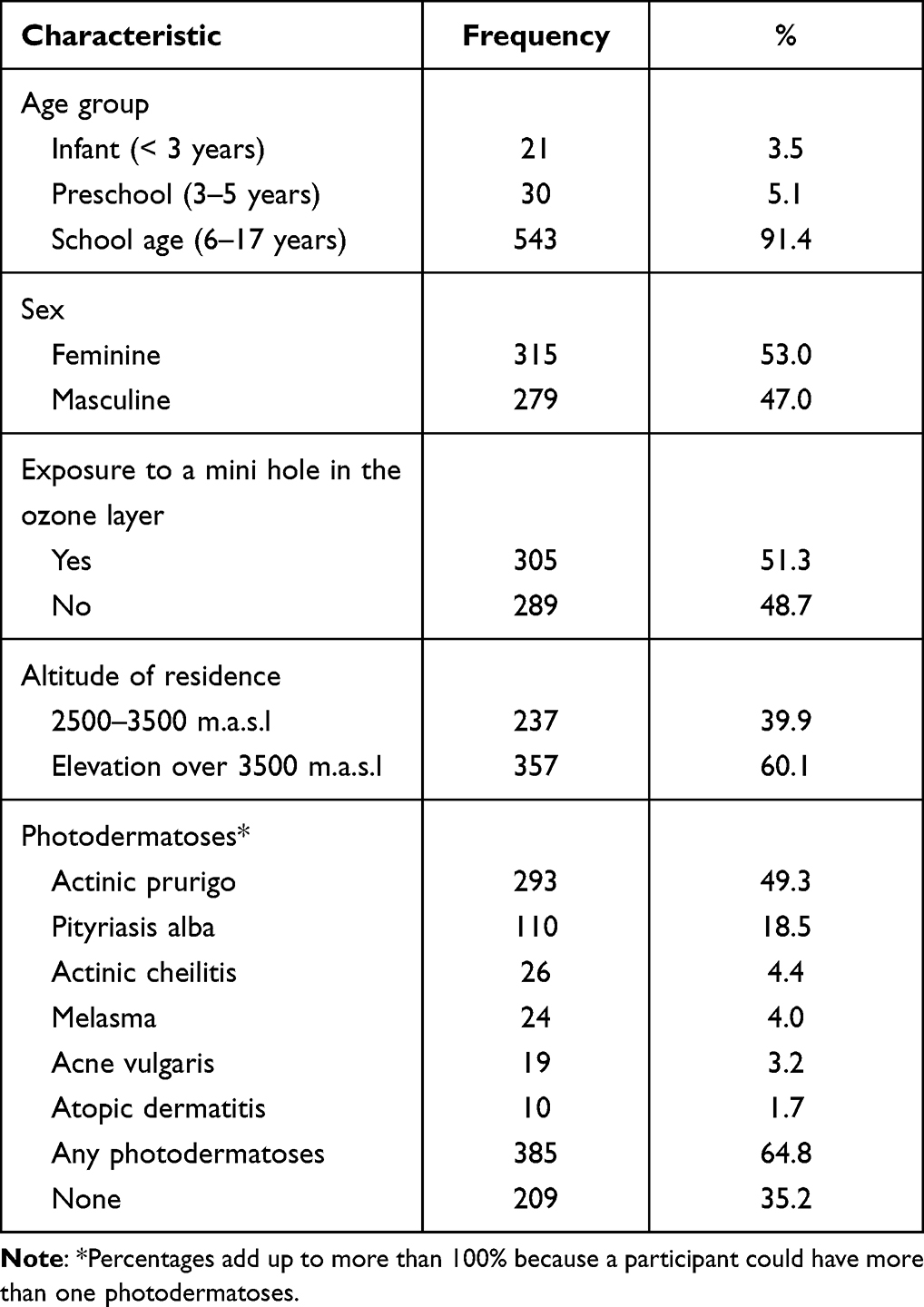 |
Table 1 Characteristics of the Pediatric Population Studied |
Prevalence of photodermatoses was 64.8%, with the main cutaneous manifestations being actinic prurigo (49.3%) and pityriasis alba (18.5%); less frequent manifestations were actinic cheilitis, melasma, acne vulgaris and atopic dermatitis (Table 1).
The photodermatoses were more frequent among girls than boys (67.3% versus 62.0%; p = 0.177) (Table 2); likewise, those exposed to the mini hole of the ozone layer had a higher prevalence of photodermatoses (74.1% versus 55.0%; p<0.001), particularly of pityriasis alba, actinic cheilitis, melasma and acne vulgaris (Table 3). Residents over 3500 meters above sea level also had a higher prevalence of photodermatoses (67.5% versus 53.2%; p<0.001), unlike those residing between 2500–3500 m.a.s.l, particularly actinic prurigo and actinic cheilitis (Table 4).
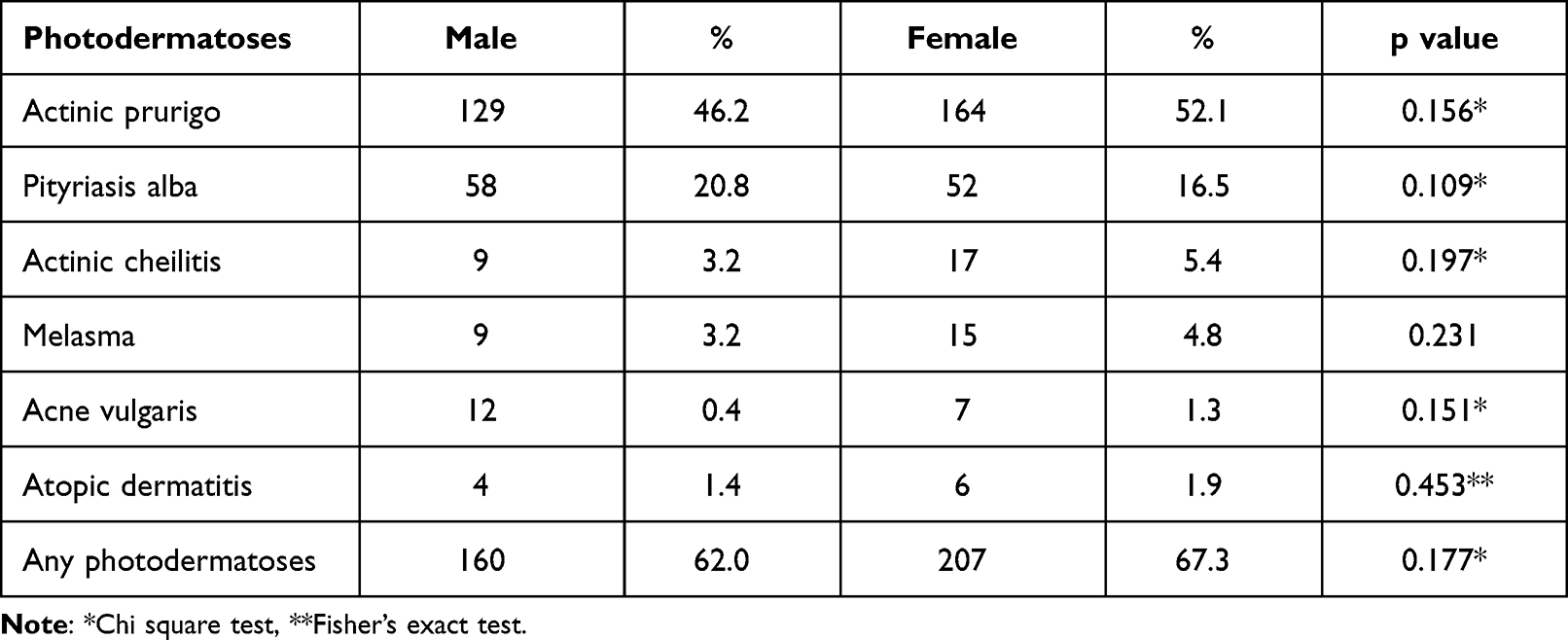 |
Table 2 Sex and Manifestations from Photodamage in the Pediatric Population of High-Altitude Population Centers |
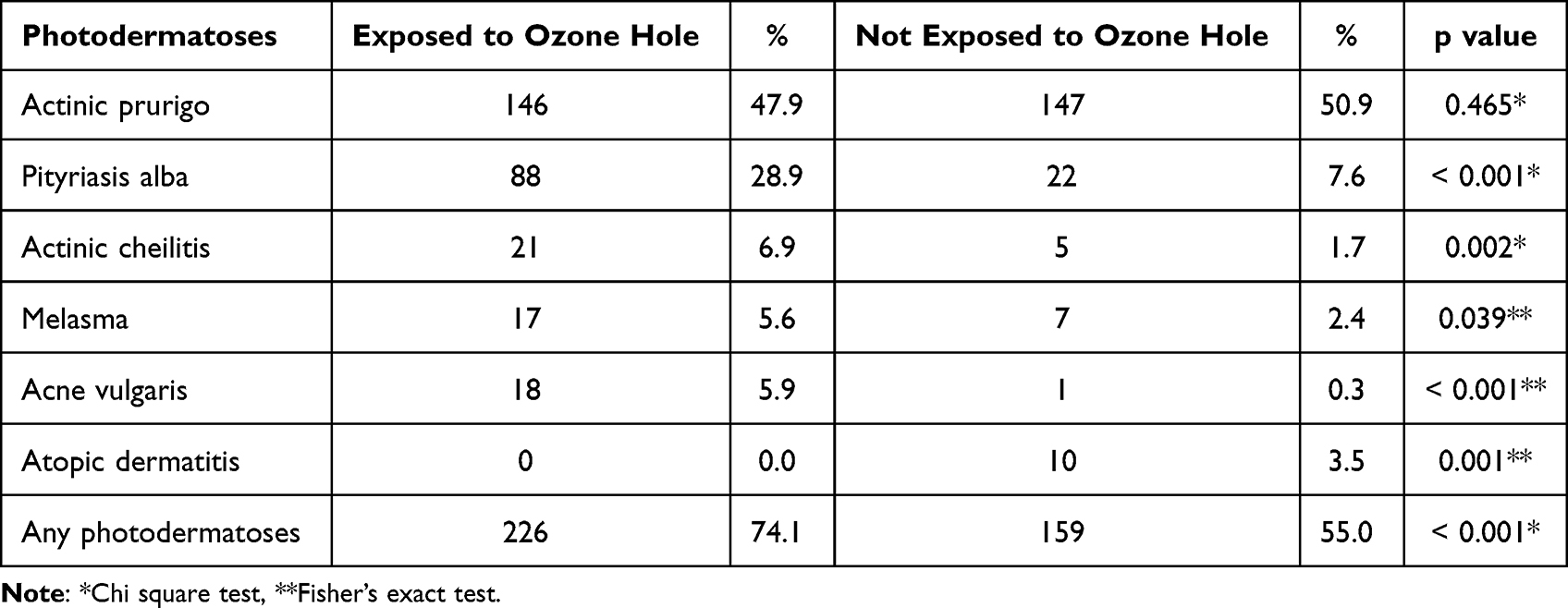 |
Table 3 Exposure to Mini Hole in the Ozone Layer and Photodermatoses in the Pediatric Population of High-Altitude Population Centers |
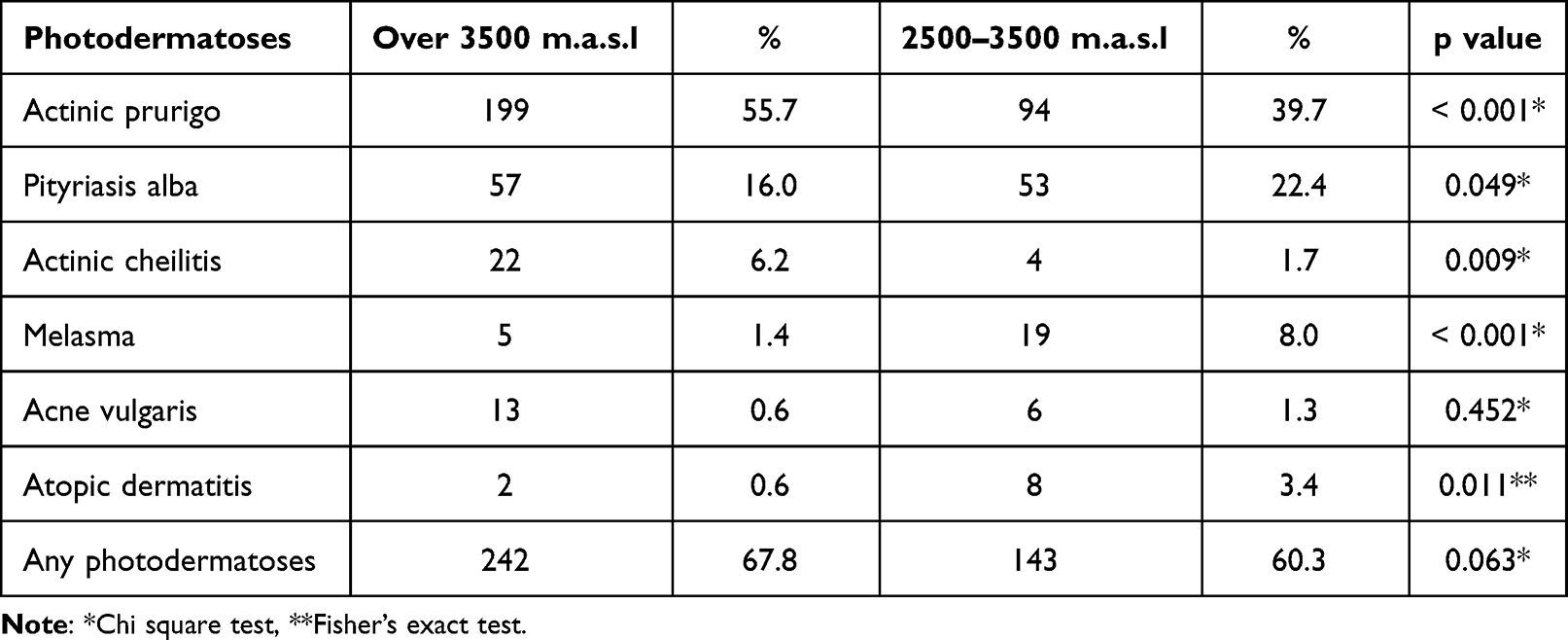 |
Table 4 Altitude and Cutaneous Manifestations from Photodermatoses in the Pediatric Population of High-Altitude Population Centers |
Multivariate analysis showed that exposure to the mini hole in the ozone layer was positively associated with photodermatoses (aOR = 4.23; CI 95%: 2.32–7.72). In addition, residing at an elevation over 3500 m.a.s.l was identified as an associated factor (aOR = 2.76; CI 95%: 1.57–4.86). No additional or potentiating effects were observed for the photodermatoses among the variables studied. The school age (of 5 or above) and female sex were not significantly associated with photodermatoses in the pediatric population studied (Table 5).
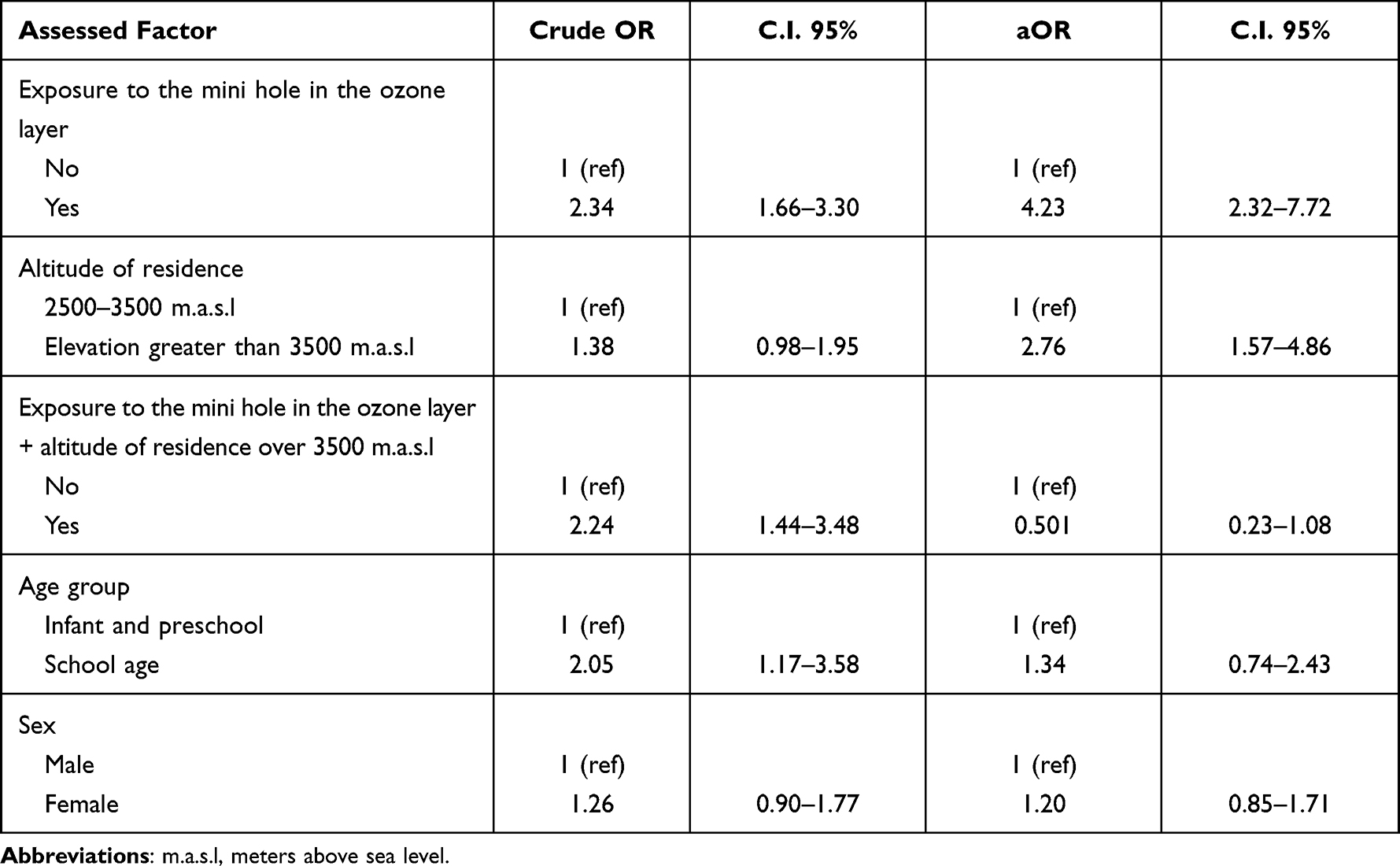 |
Table 5 Multivariate Analysis of Possible Associated Factors to Photodermatoses in the Pediatric Population of Population Centers in High Altitude |
Discussion
This study shows the high prevalence of photodermatoses among children and adolescents in high altitude populations. As expected, exposure to the mini hole in the ozone layer and residing at an elevation over 3500 m.a.s.l are associated factors for photodermatoses.
Children and adolescents living at high-altitude, where the exposure to UV radiation is intense, have a very high prevalence of photodermatoses. Besides the high UVR exposure, the damage is likely due to poor knowledge and practice of photoprotection by the population, particularly the children and adolescents.22 Determinants such as population poverty, remoteness of the population centers from capital cities and specialized health services, and the sociocultural characteristics of the population also contribute.23 There is no structured state strategy to educate the population regarding the dangers of sun exposure, sun protection measures are expensive and, besides protective clothing, usually unaffordable for most of the population. It is important to implement educational interventions throughout educational institutions and local health centers, but also to install sun protection measures (provide shadow on playgrounds, etc.), based on a budget policy and allocation that makes them sustainable, particularly in the higher risk zones.
Several studies identified mini holes in the ozone layer from a geophysical and atmospheric standpoint;14,15 but very few linked those holes directly with human pathology. For a number of years, we have observed an increment in the intensity and frequency of the mini holes in the ozone layer in Europe, underlining the need to investigate their effects.24–27 While it is accepted that the exposure to mini holes in the ozone layer is linked to skin cancer due to the increment of exposure to UV radiation,24 it is necessary to quantify the excess risk of the population exposed to these holes.
Our study shows that chronic exposure to a mini hole constitutes the main associated factor in photodermatoses so that those exposed have 4 times the chance of developing it compared to those not exposed in a population which, because of the high altitude, has a very high UVR exposure anyway. Those exposed to the mini hole of the ozone layer had a higher prevalence of pityriasis alba, actinic cheilitis and melasma, unlike those not exposed to the mini hole. This elevated prevalence indicates that despite the transient character of the mini hole, the high levels of UV radiation that are generated for short periods of time have the ability to produce photodermatoses in children and adolescents which could have implications in the future risk of developing skin cancer.
The multivariate analysis also found that residing at an elevation greater than 3500 m.a.s.l constituted associated factor for photodermatoses in children and adolescents, independent of the exposure to the ozone mini hole. This is explained, in part, by the increase in UV radiation due to high-altitude, fewer clouds and a thinner atmosphere; in this sense, the people that reside at 3500 m.a.s.l receive at least 10–12% more UV radiation compared to those at 2500 m.a.s.l at the same latitude.28 Residents over 3500 m.a.s.l had a higher prevalence of actinic prurigo and actinic cheilitis unlike those residing between 2500–3500 m.a.s.l.
With regards to the research limitations, the diagnosis of actinic prurigo were not performed using immunological tests rather based on clinical and epidemiological findings. We did not investigate the expression of HLA-DR4 (subtype DRB1*0407 or others) since these were not easily available in the country at the moment the study was carried out and their high costs where available. Despite this, we do not believe this has significantly influenced in the diagnosis because of the skills of the the dermatologists performing the diagnosis - actinic prurigo is a frequent pathology in dermatology outpatient visits in Arequipa. We did not perform hormonal studies for melasma, however, during anamnesis no participants reported receiving hormone treatment, possibly due to the distance of the populated areas to the capital city and the absence of physician specialists that could prescribe such treatment in rural Peru.
Unfortunately, in this study we did not collect data on the cutaneous phototype or the measures of photoprotection applied by children and adolescents. Similar to other reports from our populations, the majority of participants were phototype III or IV which is like other publications.29–32 During the data collection research assistants observed that the use of other measures of sun photoprotection were very limited. Most likely, most participants did not use sun protection because of its limited availability and affordability in their residential places, combined with the lack of education with respect to the importance of its use.
Conclusion
A high prevalence of photodermatoses exists among the pediatric population living at high-altitude in Peru. Residing in a region exposed to a mini hole in the ozone layer and residing at an elevation over 3500 m.a.s.l constituted associated factors. Education regarding health risks of sun exposure and ways to protect from ultraviolet information should be provided to these highly exposed populations.
Data Sharing Statement
All the data used in this review have been presented in the main text as either tables or figures. Additional requests for the data can be made electronically to the corresponding author.
Acknowledgment
We appreciated the expertise and guidance of Dr Ferdinand de Amat Loza who passed away in recent years.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Narayanan DL, Saladi RN, Fox JL. Ultraviolet radiation and skin cancer. Int J Dermatol. 2010;49(9):978–986. doi:10.1111/j.1365-4632.2010.04474.x
2. Romanhole RC, Ataide JA, Moriel P, Mazzola PG. Update on ultraviolet A and B radiation generated by the sun and artificial lamps and their effects on skin. Int J Cosmet Sci. 2015;37(4):366–370. doi:10.1111/ics.12219
3. D’Orazio J, Jarrett S, Amaro-Ortiz A, Scott T. UV radiation and the skin. Int J Mol Sci. 2013;14(6):12222–12248. doi:10.3390/ijms140612222
4. Balk SJ. Council on environmental health; section on dermatology. Ultraviolet radiation: a hazard to children and adolescents. Pediatrics. 2011;127(3):e791–817.
5. Green AC, Wallingford SC, McBride P. Childhood exposure to ultraviolet radiation and harmful skin effects: epidemiological evidence. Prog Biophys Mol Biol. 2011;107(3):349–355. doi:10.1016/j.pbiomolbio.2011.08.010
6. Godar DE, Wengraitis SP, Shreffler J, Sliney DH. UV doses of Americans. Photochem Photobiol. 2001;73(6):621–629. doi:10.1562/0031-8655(2001)073<0621:UDOA>2.0.CO;2
7. Polefka TG, Meyer TA, Agin PP, Bianchini RJ. Effects of solar radiation on the skin. J Cosmet Dermatol. 2012;11(2):134–143. doi:10.1111/j.1473-2165.2012.00614.x
8. Lucas RM, Norval M, Neale RE, et al. The consequences for human health of stratospheric ozone depletion in association with other environmental factors. Photochem Photobiol Sci. 2015;14(1):53–87. doi:10.1039/c4pp90033b
9. Medina Fernández LE, Rodríguez Zea B. Arequipa population cáncer registry. In: Incidence and Mortality 2008–2014. Arequipa: Gerencia Regional de Salud; 2018.
10. National Aeronautics and Space Administration. Total Ozone Mapping Spectrometer-Earth Probe (TOMS-EP). Washington D.C: NASA; 2013. Available from: https://eospso.nasa.gov/missions/total-ozone-mapping-spectrometer-earth-probe.
11. National Aeronautics and Space Administration. Ozone Monitoring Instrument (OMI). Washington D.C: NASA; 2007. Available from: https://www.nasa.gov/mission_pages/aura/spacecraft/omi.html.
12. Zaratti F, Forno R. La radiación ultravioleta en Bolivia. La Paz: UMSA; 2003.
13. National Aeronautics and Space Administration. What are ozone mini-holes? Goddard space flight center. NASA; 2018. Available from: https://ozonewatch.gsfc.nasa.gov/facts/miniholes_NH.html.
14. Millán LF, Manney GL. An assessment of ozone mini-hole representation in reanalyses over the Northern Hemisphere. Atmos Chem Phys. 2017;17:9277–9289. doi:10.5194/acp-17-9277-2017
15. Antón M, Cancillo LM, Serrano A, Vaquero JM, García JA. Ozone mini-hole over southwestern Spain during January 2004: influence over ultraviolet radiation. Geophys Res Let. 2007;34(10):1–5. doi:10.1029/2007GL029689
16. Liley JB, McKenzie RL Where on Earth has the highest UV? UV Radiation and its Effects; 2006:26–37. Available from: http://www.niwa.co.nz/our-services/online-services/uv-and-ozone/workshops/2006/papers.
17. Chadyšiene R, Girgždiene R, Girgždys A. Ultraviolet radiation and ground‐level ozone variation in Lithuania. J Environ Engineer Lands Manage. 2005;13(1):31–36. doi:10.3846/16486897.2005.9636843
18. Sola Y, Lorente J, Campmany E, et al. Altitude effect in UV radiation during the evaluation of the effects of elevation and aerosols on the ultraviolet radiation 2002 (VELETA-2002) field campaign, J. Geophys Res. 2008;113:D23202. doi:10.1029/2007JD009742
19. Ramos W, Galarza C, Ronceros G, et al. Noninfectious dermatological diseases associated with chronic exposure to mine tailings in a Peruvian district. Br J Dermatol. 2008;159(1):169–174. doi:10.1111/j.1365-2133.2008.08630.x
20. De Amat F, Ramos W. Enfermedades dermatológicas de tipo no infeccioso asociadas a exposición a relaves mineros en un distrito expuesto y otro no expuesto. Dermatol Peru. 2016;26(3):138–142.
21. Bylaite M, Grigaitiene J, Lapinskaite GS. Photodermatoses: classification, evaluation and management. Br J Dermatol. 2009;161(Suppl 3):61–68. doi:10.1111/j.1365-2133.2009.09451.x
22. Sejje Chambi LM, Velásquez Zeballos KP Actitud sobre efectos negativos de la radiación solar y aplicación de medidas de prevención del cáncer de piel en adolescentes. instituciones educativas públicas mixtas, Cerro Colorado, Arequipa. 2013 [Tesis]. Arequipa: Universidad Nacional de San Agustín; 2013.
23. Ramos W, Venegas D, Honorio H, Pesantes J, Arrasco J, Yagui M. Enfermedades no transmisibles: efecto de las grandes transiciones y los determinantes sociales. Rev peru epidemiol. 2014;18(S1):e06.
24. Martinez-Lozano JA, Utrillas MP, Nunez JA, et al. Ozone mini-holes over Valencia (Spain) and their influence on the UV erythemal radiation. Int J Climatol. 2011;31:1554–1566. doi:10.1002/joc.2173
25. Stebel K, Hansen GH, Edvardsen K, et al. Winter 2002/2003 above Northern Scandinavia seen by the alomar ozone dial.
26. Luk’yanova NF, Lyudchik AM. Statistics of anomalous events in the ozonosphere over Europe. Russ Meteorol Hydrol. 2008;33:491–498. doi:10.3103/S1068373908080037
27. Haluza D, Simic S, Moshammer H. Temporal and spatial melanoma trends in Austria: an ecological study. Int J Environ Res Public Health. 2014;11(1):734–748. doi:10.3390/ijerph110100734
28. World Health Organization. Ultraviolet radiation and health. Geneva: World Health Organization; 2017. Available from: https://www.who.int/uv/uv_and_health/en/.
29. Soria Solís JS Factores asociados a pitiriasis alba en pacientes del consultorio de dermatología del Hospital Goyeneche [Tesis]. Arequipa: Universidad Nacional de San Agustín; 2018.
30. Velarde H, Juan M. Conocimientos, actitudes y prácticas sobre fotoprotección infantil en madres que acuden al Servicio de Dermatología del Hospital Nacional Dos de Mayo: enero 2012 [Thesis]. Lima: Universidad Nacional Mayor de San Marcos; 2013.
31. Thomas-Gavelan E, Sáenz-Anduaga E, Ramos W, Sánchez-Saldaña L, Sialer Mdel C. Knowledge, attitudes and practices about sun exposure and photoprotection in outpatients attending dermatology clinics at four hospitals in Lima, Peru. An Bras Dermatol. 2011;86(6):1122–1128. doi:10.1590/S0365-05962011000600009
32. Ramos W, Sánchez-Saldaña L, Canales L, et al. Conocimientos, actitudes, prácticas de fotoprotección de bañistas que acuden a playas de Lima. Dermatol Peru. 2012;22(4):143–148.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.