")
Back to Journals » Open Access Emergency Medicine » Volume 13
Exploring the Prevalence and Patterns of Use of Sleep Aids and Stimulants Among Emergency Physicians and EMS Providers in Saudi Arabia
Authors Kentab OY, Ibrahim AAAl , Soliman KR , Aljahany M , Alresseeni AI, Algarni AS
Received 11 March 2021
Accepted for publication 19 July 2021
Published 28 July 2021 Volume 2021:13 Pages 343—353
DOI https://doi.org/10.2147/OAEM.S310324
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hans-Christoph Pape
Osama Y Kentab,1 Ahmad AAl Ibrahim,1 Khaled R Soliman,1 Muna Aljahany,2 Abdulaziz I Alresseeni,1 Abdulaziz S Algarni1
1Emergency Department, King Abdullah Bin Abdulaziz University Hospital, Princess Nourah Bint Abdulrahman University, Riyadh, Saudi Arabia; 2Clinical Sciences Department, College of Medicine, Princess Nourah Bint Abdulrahman University, Riyadh, Saudi Arabia
Correspondence: Muna Aljahany
Department of Clinical Sciences, College of Medicine at Princess Nourah Bint Abdulrahman University, P.O. Box 84428, Riyadh, Saudi Arabia
Tel +966 118233711
Email [email protected]
Purpose: This study explores the prevalence and patterns of the use of pharmacologic sleep aids and stimulants among Saudi Arabia’s emergency physicians (EPs) and emergency medical services (EMS) providers.
Patients and Methods: We adopted a descriptive, cross-sectional design. To collect data on the types and frequencies of sleep aids and stimulants used, we distributed a semi-structured, anonymous, web-based questionnaire to registered EPs, paramedics, and emergency medicine technicians (EMTs) in the Saudi Commission for Health Specialties. An internal consistency analysis showed good reliability (Cronbach’s alpha=0.667) of the questionnaire. A subscale analysis confirmed the results—alpha values were 0.720 and 0.618 for the use of sleep aids and stimulants, respectively.
Results: Males and females represented 81.8% and 18.2%, respectively, of the valid sample of 669 participants. Respondents aged 25– 34, 35– 44, and 45– 55 years represented 51.9%, 32.7%, and 10.2% of the sample, respectively. Results showed that a majority of the respondents (67.1%) used stimulants. Caffeine was the most common stimulant; caffeine and energy drinks were used by 65.9% and 17.2% of the respondents, respectively. Caffeine, energy drinks, nicotine, and ephedrine were used by 65.9%, 17.2%, 18.5%, and 17.3% of the respondents, respectively. The respondents who used at least one sleeping aid and those using only one and two sleeping aids accounted for 36.6%, 15.6%, and 9.7%, respectively. The most common sleeping aids antihistamines and marijuana were used on most days by 13.4% and 13.3% of the respondents, respectively. The average monthly number of night shifts (P = 0.025) significantly influenced sleep aid use. Respondents working in night shifts for 3– 5 months or more than 7 days were more likely to use sleeping aids.
Conclusion: Future research should enhance health workers’ knowledge of the efficacy and safety of these medications and guide strategies to organize and reduce night shift work.
Keywords: sleep disruption, shift work, circadian rhythm, night shift
Introduction
Working in emergency departments (EDs) represents a unique challenge to physicians, owing to the department’s continuous operations. Therefore, it is important to create work schedules that ensure the availability of qualified staff around the clock. This involves deputing staff with an ability to work overnight and in rotating shifts. This nature of job leads to changing sleep patterns and requires the staff to compensate for their sleep debt with daytime sleep. In Saudi Arabia and several other countries, ED physicians work eight hours per shift, and they constantly rotate shifts. These clinical schedules cause the staff to experience detrimental effects, including fatigue, decreased alertness, irritability, burnout, decreased memory, and communication problems.1,2 In organizations, these effects are reflected through increased rates of absenteeism, accidents, and medical errors.3,4
It has been well-established that the aforementioned negative effects of shift work are attributable to disrupting the circadian rhythms and reducing the daytime recovery sleep of the ED staff.5 As per a study in the United States, the night-shift ED residents experienced a higher frequency of difficulties in sleeping, shorter sleep duration, and decreased performance than that of their peers working in other shifts.5 Similarly, in Saudi Arabia, the ED physicians who worked in shifts experienced a poorer sleep quality and higher Epworth sleepiness scale scores than that of their non-shift work healthcare professionals.6 Other investigations concerning nurses have demonstrated increased risks of reduced periods of sleep, insomnia, and excessive daytime sleepiness and fatigue when doing shift work,7 working night shifts,8,9 and working a three-shift pattern,10 respectively.
Given their nature of work, the ED staff should to take suitable measures to combat sleep deprivation, circadian rhythm variation, and the possible consequences to their health. Given the lack of notable changes in the medical residents’ education system and no reduction in work hours or an abandonment of shift work, there are few solutions to the sleep-related problems. Hence, there is a need to implement strategies facilitating administrative and behavioral changes. In addition to the aforementioned issues, the use of pharmacologic sleep aids has been a cause for significant concern for several years. Although the use of sleep aids is prevalent among the ED staff and may help them counteract the problems associated with their fluctuating and highly demanding schedules, the use of these medications may not be a benign solution. Along with sleep aids, there may be a high likelihood of the on-shift use of stimulants by a considerable proportion of the ED staff.
Studies assessing the use of sleep aids and stimulants among the ED staff are limited by poor response rates11,12 or to a single institution’s ED.13 It must be noted that, to the best of our knowledge, the prevalence of the use of such medication has not yet been investigated in Saudi Arabia. The outcomes of this study will provide significant insights into the current status of sleep patterns and the effect of such medications on the alertness levels. Having said that, the future research can increase the awareness and knowledge of ED staff on the use of such medications.
We assessed the prevalence and patterns of using sleep aids among ED physicians and EMS providers via a nationwide, web-based survey in the Kingdom of Saudi Arabia. As secondary outcomes, we investigated their use of stimulants and it’s effect in promoting alertness.
Materials and Methods
Study Design and Setting
Based on the guidelines of the strengthening the reporting of observational studies in epidemiology (STROBE) checklist for cross-sectional studies,14 we conducted a descriptive, prospective cross-sectional study among all the registered EPs, paramedics, and EMTs in the Saudi Commission for Health Specialties (SCFHS) in Saudi Arabia. Study conducted between February 2020 to March 2021. We invited them to participate in an online, semi-structured questionnaire designed to collect data on their use of sleep aids and stimulants. We excluded the non-ED physicians from the analysis. The study protocol was approved by the Institutional Review Board of the Princess Nourah bint Abdulrahman University.
Study’s Tool
The online questionnaire was adapted from a recent survey-based study in Canada.13 We obtained an email approval from the authors to use the survey tool. The survey had five main domains comprising 19 items: 1) sociodemographic data (4 items)—age, gender, marital status, and current living situation; 2) practice information (4 items)—work position and experience, work location, and the average number of night shifts in EDs (defined as finishing work after midnight); 3) the perceived effects of working in EDs on sleep (5 items)—the perceived effects of shift work on the ability to sleep, the subjective perceptions of the factors contributing to sleeping difficulties, and the personal perceptions of having insomnia or chronic insomnia; 4) the use of sleep aids (4 items)—the prior and current use of sleep aids, the prescriber of these medications, the reasons attributing to the use of sleeps aids; and 5) the use of stimulants (2 items)—the prior and current use of stimulants to maintain wakefulness/alertness during work.
Selection of Participants
The sample comprised all the registered EPs, paramedics, and EMTs in the SCFHS in Saudi Arabia. The sample size was estimated using the n4Studies application.15 Using a standard proportion of 0.5, standard error (d) = 0.05, Alpha (α) = 0.05, and Z (0.975) = 1.959964, the sample size was estimated to be 341. With a 20% invalid responding rate, the final sample size was determined to be 376.
The questionnaire was uploaded to SurveyMonkey® (www.surveymonkey.com)—a platform that collects participants’ responses via customized questionnaires. Participation was entirely voluntary; the participants were informed about the purpose of the study and they provided consent to participate upon the survey’s completion, and the study was conducted in accordance with the Declaration of Helsinki. While we did not collect personal information, individual data for each response was coded for subsequent analysis using Microsoft Excel 2016.
Outcome Measures
The primary outcomes represent the proportion of ED staff who had used or were using sleep aids. We also explored the types and frequency of using such medications. The secondary outcomes include the sociodemographic and practice characteristics and the use of stimulants to overcome fatigue during work. We defined insomnia as a condition wherein a person experiences difficulty with the initiation, maintenance, or quality of sleep, despite normal sleep opportunities and times, which eventually leads to daytime functional/cognitive impairment.16 Chronic insomnia was classified as having insomnia for more than one month.17 The use of sleep aids/stimulants for more than 6 times per month was defined as frequent use.
Primary Data Analysis
Using a Cronbach’s alpha test, we tested the internal consistency of the whole questionnaire and the specific items related to the use of sleep aids and stimulants. The descriptive analysis included frequencies and percentages of all the categorical variables along with their respective 95% confidence intervals (95% CIs). We used the multi-response analysis to analyze items related to the domains of using sleep aids and stimulants (domains 4 and 5). Statistical analysis was performed using the Statistical Package for Social Sciences version 26.0 (SPSS Inc., Chicago, IL, USA).
Internal Consistency of the Questionnaire
An analysis of the internal consistency of all the questionnaire items showed good reliability (Cronbach’s alpha=0.667). A subscale analysis showed similar results, where alpha values were 0.720 and 0.618 for the domains of the use of sleep aids and stimulants, respectively.
Statistical Analysis
Statistical analysis was performed using R 3.6.3. Counts and percentages were used to summarize the distribution of categorical variables, and the mean ± standard deviation (SD) was used to summarize the distribution of continuous variables. The chi-square test of independence was used to assess the relationship between categorical variables. Hypothesis testing was performed at a 5% level of significance.
Results
Of the 777 respondents, we excluded 30 responses from nurses and administrators. Subsequently, we excluded 78 responses owing to missing data (information limited to the work location). Of the excluded participants, the number of personnel working in and outside the Kingdom of Saudi Arabia accounted for 48 (61.5%) and 30 (38.5%), respectively. Thus, the final sample consisted of 669 respondents working in the Kingdom of Saudi Arabia. The overall response rate was 26%. Males and females represented 81.8% and 18.2% of the study sample, respectively. Respondents aged 25–24 years old represented 51.9% of the study sample. Respondents aged 35–404 years and 45–55 years represented 32.7% and 10.2% of the study sample, respectively. Most of them perceived shift work as negatively affecting their ability to sleep effectively (n = 560, 85%).
The percentage of respondents working >7 nights/month, on an average, exceeded more than a quarter of the sample, while 27.7% and 22.6% worked 5–7 nights/month and 5–7 night shifts/month, respectively. We did not observe any statistically significant relationship between the average number of night shifts/month (ordinal) and the number of sleeping aids used (r = 0.04, p = 0.42) (Table 1).
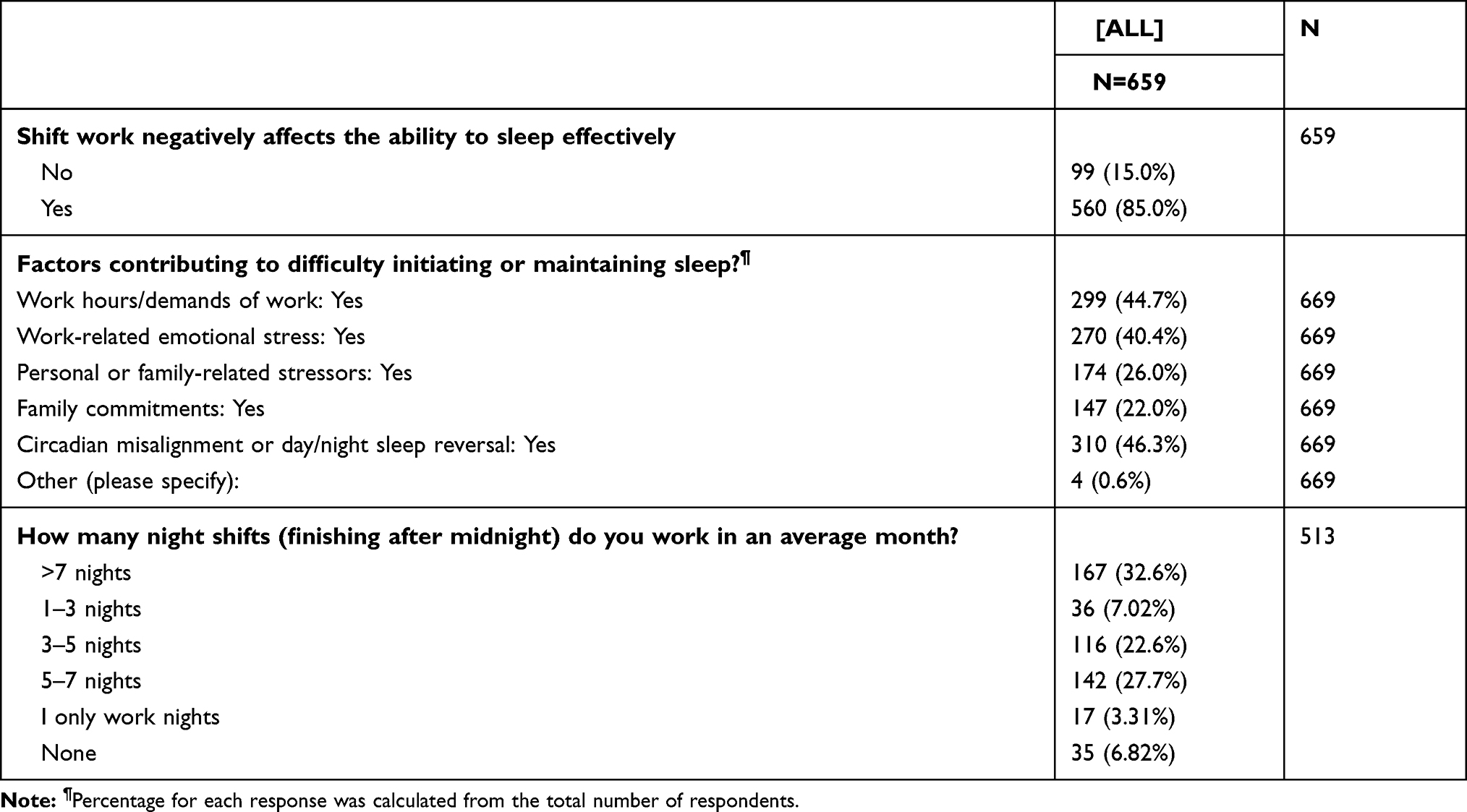 |
Table 1 Factors Contributing to Difficulty in Initiating or Maintaining Sleep |
Results showed that 63.4% (n = 424) of the respondents did not use any of the sleeping aids mentioned in the questionnaire. Thus, the number of respondents using at least one, only one, and two sleeping aids accounted for 245 (36.6%), 104 (15.6%), and 65 (9.7%), respectively (Figure 1). Melatonin and antihistamines were used by 16.1% (n=108) and 22.4% (n = 150) respondents, respectively. Barbiturates (n = 13, 1.9%) and marijuana (n = 17, 2.5%) were the least used sleeping aids (Figure 2). Based on the available data, the most commonly used sleeping aids antihistamines and marijuana were used on most days of the week by 13.4% and 13.3% of the respondents, respectively. The least commonly used sleep aid was benzodiazepine, which was used less than once/month, as per 50% of the respondents.
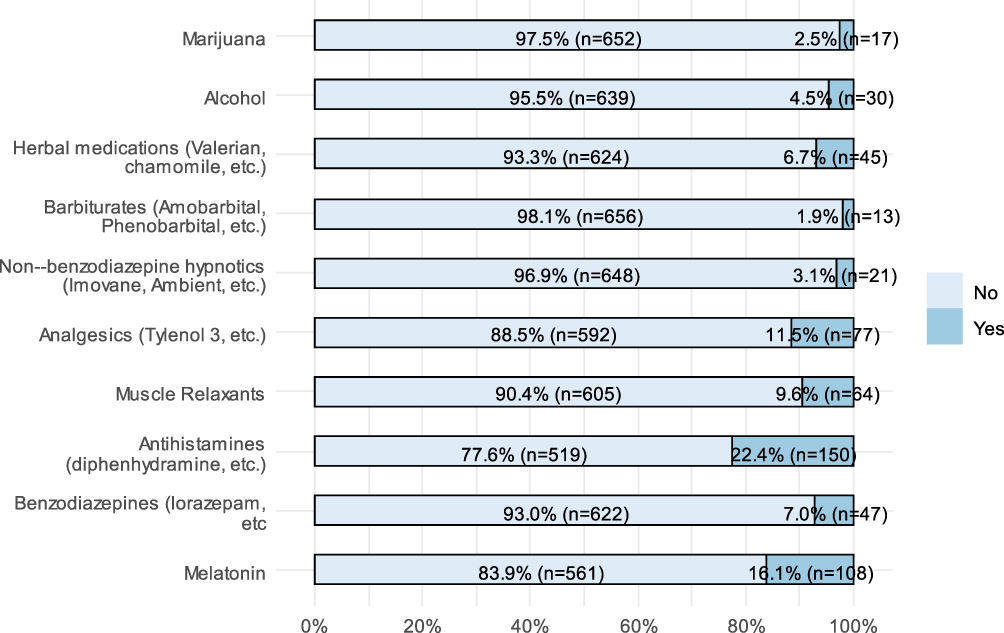 |
Figure 1 Sleeping aids used by the respondents. |
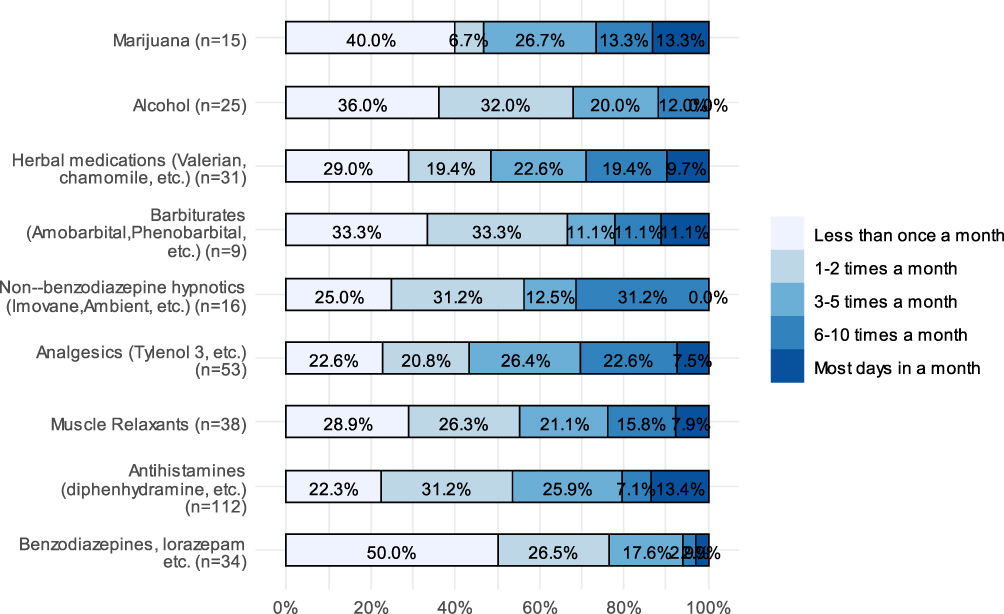 |
Figure 2 Frequency of using sleeping aids. |
Table 2 showed a statistically significant relationship between gender and the use of sleeping aids (P = 0.041). Females were more likely to use sleeping aids (45.1%) than that of males (34.7%). We did not find a statistically significant relationship between age and the use of sleeping aids, but between work area and the use of sleeping aids. The post-hoc comparisons showed that respondents from the Southern province were less likely to use sleeping aids than those from Riyadh (P = 0.043). We did not find any statistically significant relationship between the marital status and ED-work duration and the use of sleeping aids, but between the average monthly number of midnight shifts and the use of sleeping aids (P = 0.025).
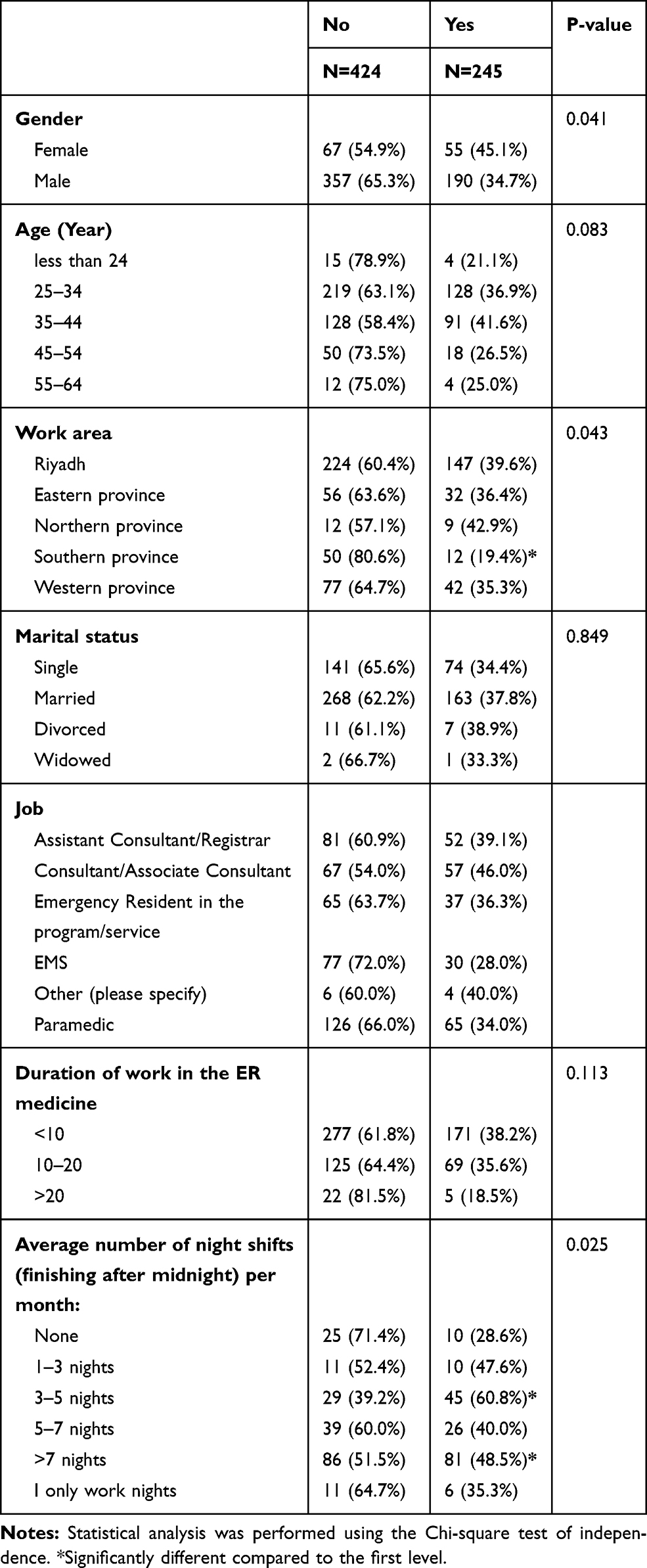 |
Table 2 Factors Associated with Using at Least One Sleeping Aid |
The post-hoc comparisons showed that respondents who worked for 3–5 months or > 7 days in night shifts were more likely to use sleeping aids. There was no statistically significant relationship between work and the use of sleeping aids.
In Table 3, 217 respondents reported the reasons for using pharmacological sleeping aids. The main reason was attributed to the need to reset the circadian rhythms or natural sleep cycle (n = 66, 30.4%). Other reasons included sleeping after (n = 48, 22.1%) and before a night shift (n = 39, 18%) and regardless of the shifts worked (n = 47, 21.7%). The proportion of respondents using OTC medications accounted for less than one-half of the sample (n = 90, 42.7%), and the proportion that self-prescribed medications accounted for one-quarter of the sample (n = 56, 26.5%). Results showed that only 32.6% of the respondents did not use any stimulants (n = 218); the respondents using only one and two stimulants represented 43.8% (less than one-half of the respondents) and 16.9% of the sample, respectively.
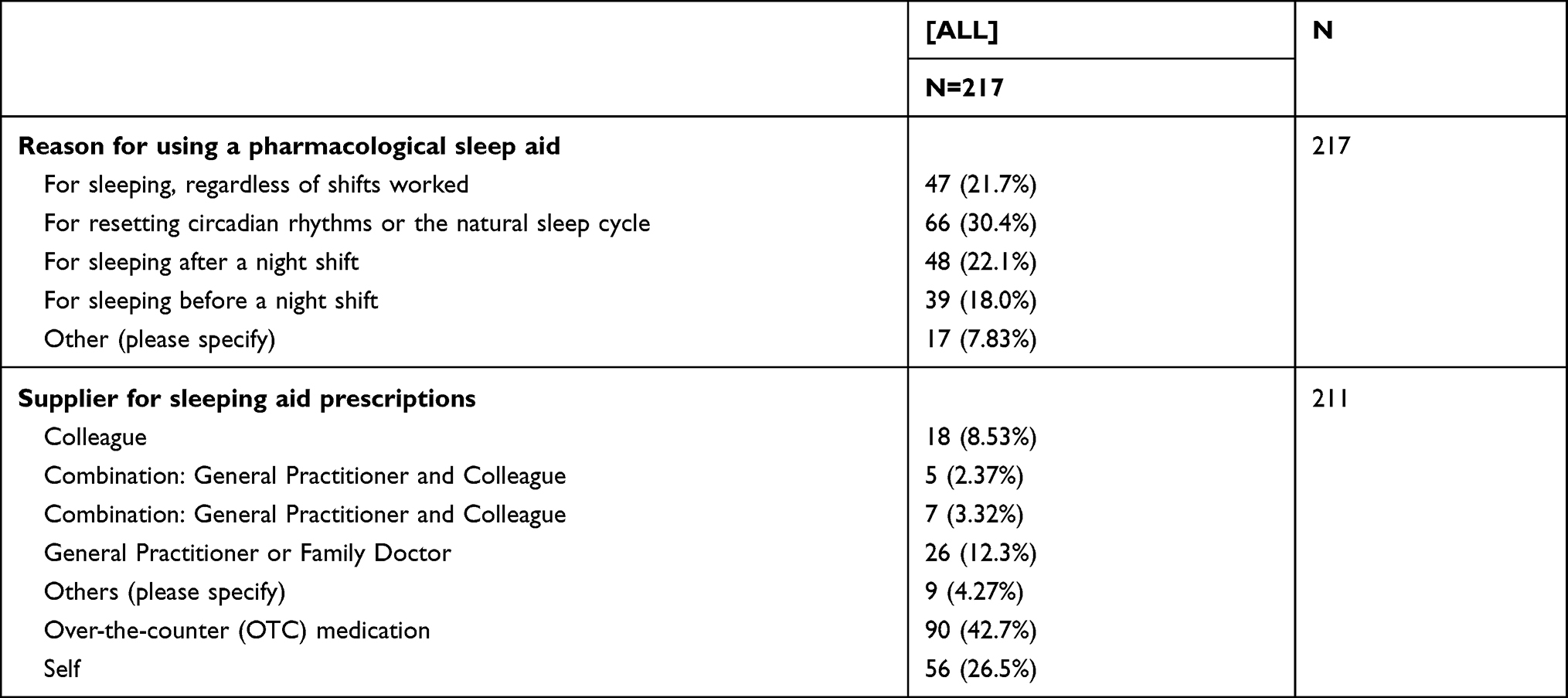 |
Table 3 Reasons for Using Sleep Aids and Supply Sources |
Results showed that caffeine and energy drinks were used by 65.9% (n = 441) and 17.2% (n = 115), respectively, of the respondents. Nicotine and ephedrine were used by 18.5% (n = 124) and 17.3% (n = 116) of the respondents, respectively. Amphetamines, modafinil, and herbals were the least used stimulants, as per the respondents (Figure 3).
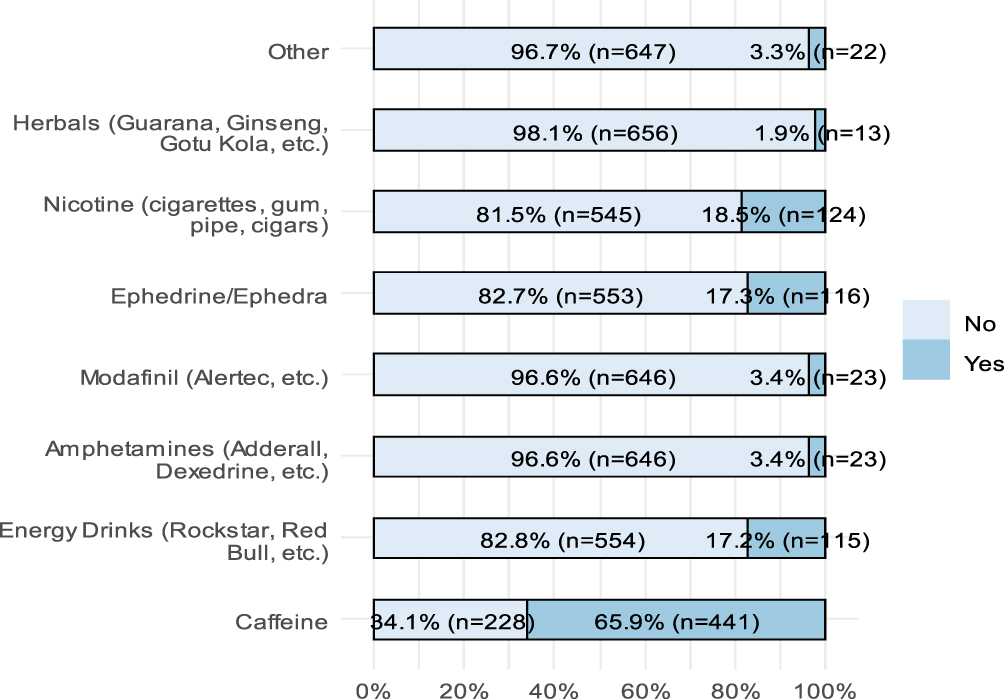 |
Figure 3 Stimulants used by the respondents. |
As per Table 4, 82.69% (n = 86) of the respondents reported that energy drinks were used once/shift. The proportion of respondents using modafinil once and twice/shift represented 61.9% (more than half of the respondents) and 13.64% of the sample, respectively. Half of the respondents used nicotine at least five times/shift.
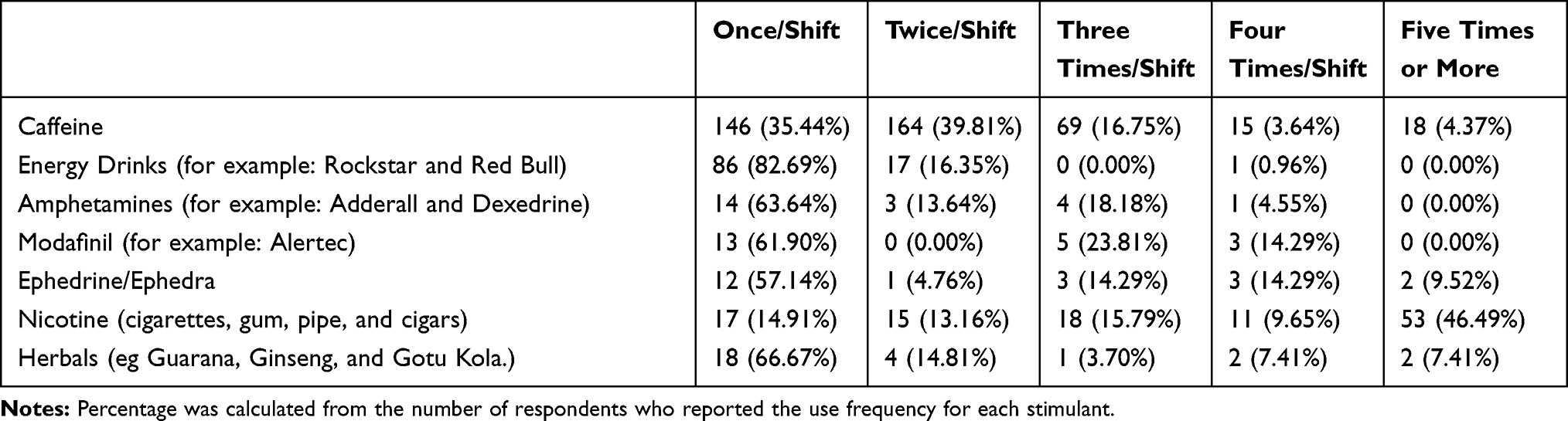 |
Table 4 Frequency of Stimulant Use |
Table 5 did not show a statistically significant relationship between the gender and age and the use of stimulants (P > 0.05 for both comparisons). We found a statistically significant relationship between the work and the use of stimulants (P < 0.05).
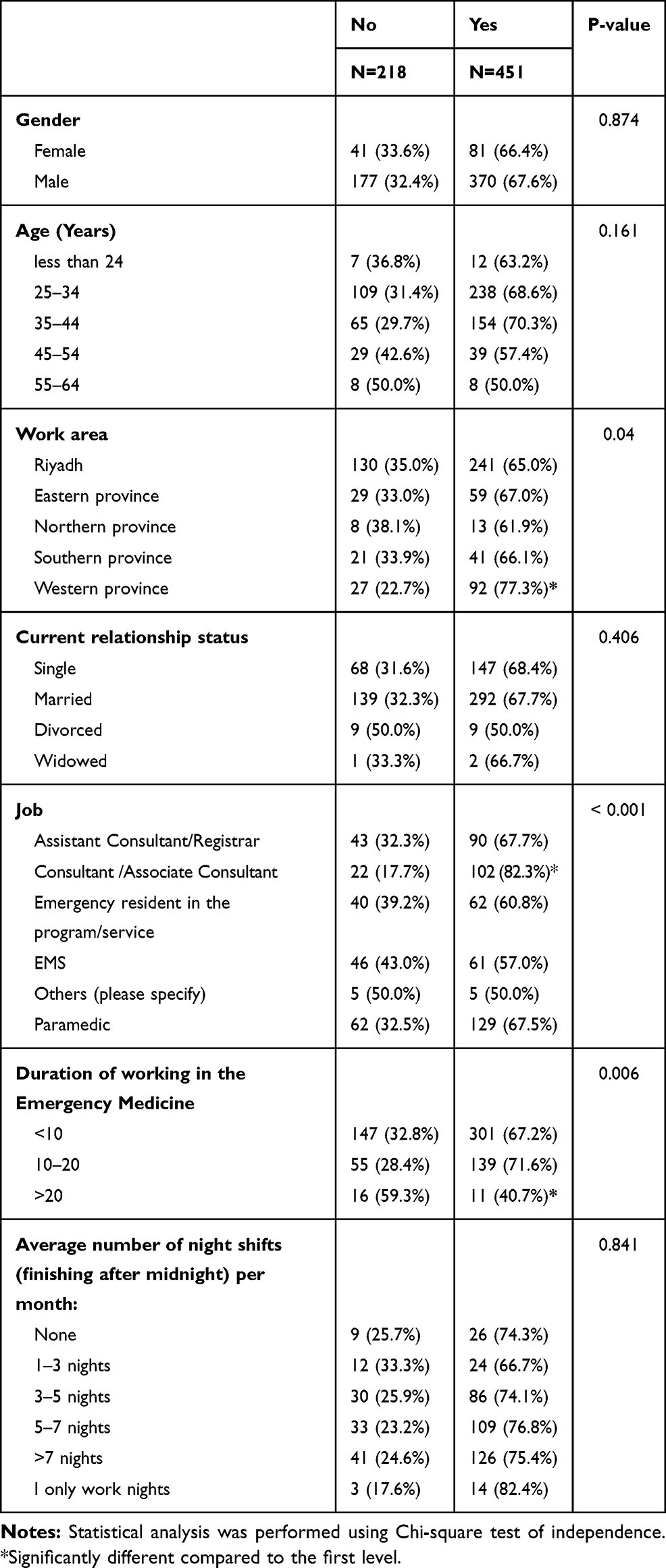 |
Table 5 Factors Associated with the Use of at Least One Stimulant |
The post-hoc comparisons showed that respondents from the Western province were more likely to use stimulants than those from Riyadh (P < 0.05). We did not find a statistically significant relationship between the marital status and the use of stimulants.
The results showed a statistically significant relationship between the current job and the use of stimulants, with consultants/associate consultants reporting a higher use of stimulants than that of the associated consultants. We found a relationship between the ED-work duration and the stimulant use (P < 0.05), with respondents who worked for > 20 years reporting less stimulant use than those who worked for < 10 years.
Discussion
Sleep deprivation resulting from ED shift schedules negatively impacts the clinical and cognitive performance of physicians and non-physicians.18,19 Several strategies can be applied to prevent sleep deprivation, such as the appropriate scheduling and sequence of shifts and napping for short periods.20 However, instead of considering these administrative aspects, at an individual level, there has been a prevalence in the use of pharmacologic aids to modulate sleep and wakefulness.
In a recent national wide study, about 15% of the general population of the employee sample reported taking sleep medications in the preceding month, where 10.8% had taken medication only infrequently compared to 36.6% who reported use from our study participants.21 In this study, 67.4% had reported use of stimulants at some point of their career. Most of them believed that shift work could have influenced their normal sleep pattern; the most significantly perceived factors of sleep disruption were circadian misalignment, increased work hours, and work-related emotional stress.
The aforementioned results mimic those reported in other studies in the literature. In Canada, the rates of the previous and current use of sleep aids were estimated at 67% and 56%, respectively, among ED physicians.13 Similarly, 55.7% of the ED staff reported the use of sleep aids in an early web-based survey in the United States.12 Concerning their routine use, a study among the staff of a local ED center in the United States revealed that about 38% of the ED residents and nurses have been using pharmacologic sleep aids.22 This reflects the urgent need to reduce the disruptive effects of shift work on the circadian rhythm, which is dependent on the internal clock controlled by the hypothalamic suprachiasmatic nucleus.23 In essence, ED shift workers deprived of nighttime sleep cannot get the same amount of rest from the daytime sleep as that from the nighttime sleep. The repeated or continuous work during night shifts disrupts sleep patterns, which cause a dyssynchronization between chronological and biological clocks and, in turn, makes it difficult for sleep-deprived individuals to recover effectively from sleep deprivation. Therefore, pharmacological solutions are usually considered by shift workers as an option, including those working in the EDs.
In this analysis, antihistamines, melatonin, marijuana and analgesics were used sleep aids as past or present routine medications. Likewise, Handel et al12 demonstrated that antihistamines, primarily diphenhydramine, were used frequently by ED residents. Nonetheless, other studies have shown a relative prevalence of other medications. Nonbenzodiazepine hypnotics were the most popular among ED physicians in Canada13 and the ED residents of the national American Board of Emergency Medicine.24 Recently, Richards et al22 found marked discrepancies between past and current uses; they showed that the ED staff used diphenhydramine, melatonin, and alcohol in the past, whereas melatonin, diphenhydramine, and doxylamine were routinely used by the participants.
There is a lack of clinical evidence regarding the efficacy and safety of the use of antihistamines among shift work-staff, as indicated by a recent systematic review.25 Antihistamines induce tolerance with repeated use, and they can be associated with adverse events such as dizziness, xerostomia, and post-awakening sedation. However, after night shifts, it has been shown that melatonin improves the length of sleep, but no other sleep quality parameters.26 Other randomized clinical trials have found no significant effects of melatonin on sleep quality, cognitive functions, or night alertness in ED physicians; these studies are also outdated.27,28 These inconsistent outcomes indicate the lack of high-quality studies, which necessitates conducting prospective clinical investigations involving different sleep aid medications used by shift work-ED staff.
Concerning stimulants, we found that the sampled participants predominantly used caffeine-based stimulants. This was in agreement with other studies on nightshift workers in healthcare settings.11,22,29 This observation was unsurprising since caffeine is the most commonly used psychoactive substance worldwide.30 It increases arousal in a dose-dependent manner, with more significant effects in fatigued than rested individuals.31 The non-sleep-deprived and sleep-deprived individuals experience performance benefits, owing to increased alertness, after consuming 30–300 mg and 200–600 mg of caffeine, respectively.32,33 Notwithstanding the low-quality evidence, caffeine combined with naps can significantly reduce sleepiness during night shifts, as revealed by a Cochrane systematic review published in 2014.26 Among nightshift workers, the caffeine use is usually associated with improved cognitive performance, mood, and enhanced wakefulness; however, its use may induce tolerance in a significant proportion of individuals.34 We could not assess the effects of caffeine on work performance among ED staff; this could be best assessed by assessing fatigue during shifts.
Limitations
As with any observational study, we could not infer causation owing to the self-reported nature of data. The subjective reporting of data might have also led to underreporting of the prevalence of the use of sleep aids and stimulants. In other words, social desirability bias in the responses of the participants might have resulted in dishonest responses. A recall bias is also evident, where the respondents might have inadvertently under- or over-reported their personal perceptions and uses of medications/active substances. It must be noted that sleep disruption was assessed on the basis of the responses of the participants, instead of the scores of sleep quality and daytime sleepiness. Additionally, work-related stress was not assessed using reliable tools. Finally, although the study’s tool was based on another study, and it showed good values of the parameters of the internal consistency, our questionnaire was not validated for use among ED workers, particularly in the national context.
Conclusion
In line with the aforementioned findings and limitations, this study provides recommendations for future investigations. The future research should consider a prospective, randomized design to collect real-time data from cohort groups using different types of sleep aids, in order to assess the efficacy and safety of their use among ED workers, including those working shifts. This will help in identifying robust causal associations of the possible factors that could influence the performance of these medications. The study also recommends formulating administrative strategies that can facilitate a smooth shift transition and reduce the burden of sleep disruption among healthcare professionals. On the basis of clinical, instead of subjective and self-reported, investigations, the future studies should assess the effects of such strategies on the parameters of sleep quality and daytime sleepiness. Finally, in the context of Saudi Arabia, in order to ensure the prudent use of these medications, the future research should promote the awareness and knowledge of ED physicians and nurses regarding the lack of evidence on and the possible side effects of antihistamines. In this context, it must be noted that the ED staff in Saudi Arabia attributed the negative effects of shift work on the sleep quality to circadian misalignment and increased work demands. To offset these effects, 36.6% of the respondents used or have been routinely using sleep aid medications, including antihistamines and melatonin. This use is prevalent, despite the lack of robust clinical evidence on the relationship between the routing use of these medications and their safety and efficacy in promoting sleep. Most of the participants (67.4%) had also used stimulants, mostly caffeine. Future studies should be implemented, at a national level, to assess the clinical significance of sleep aids/stimulants for shift workers. These studies should explore alternative strategies formulated by decision-makers to reduce and organize shift work, mainly the night shifts, and should test the quality of sleep using reliable and effective tools.
Abbreviations
ED, emergency department; EMT, emergency medical technicians; SCFHS, Saudi Commission for Health Specialties.
Funding
This research was funded by the Deanship of Scientific Research at Princess Nourah Bint Abdulrahman University, Riyadh, Saudi Arabia, through the Fast-track Research Funding Program.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Costa C, Mondello S, Micali E, et al. Night shift work in resident physicians: does it affect mood states and cognitive levels? J Affect Disord. 2020;272:289–294. doi:10.1016/j.jad.2020.03.139
2. Castro EAS, de Almondes KM. Sleep pattern and decision–making in physicians from mobile emergency care service with 12–h work schedules. Int J Neurosci. 2018;128:530–539. doi:10.1080/00207454.2017.1400970
3. Izadpanah F, Nikfar S, Bakhshi Imcheh F, Amini M, Zargaran M. Assessment of frequency and causes of medication errors in pediatrics and emergency wards of teaching hospitals Affiliated to Tehran University of medical sciences (24 hospitals). J Med Life. 2018;11:299–305.
4. O’Shea J, Vu S, Siegelman J, Heron S, Lall M. “Breaking” the emergency department: does the culture of emergency medicine present a barrier to self–care? West J Emerg Med. 2020;21:313–321. doi:10.5811/westjem.2019.10.44584
5. Harrison EM, Walbeek TJ, Maggio DG, Herring AA, Gorman MR. Circadian profile of an emergency medicine department: scheduling practices and their effects on sleep and performance. J Emerg Med. 2020;58:130–140. doi:10.1016/j.jemermed.2019.10.007
6. Alshahrani SM, Baqays AA, Alenazi AA, AlAngari AM, AlHadi AN. Impact of shift work on sleep and daytime performance among health care professionals. Saudi Med J. 2017;38:846–851. doi:10.15537/smj.2017.8.19025
7. Epstein M, Soderstrom M, Jirwe M, Tucker P, Dahlgren A. Sleep and fatigue in newly graduated nurses–Experiences and strategies for handling shiftwork. J Clin Nurs. 2020;29:184–194. doi:10.1111/jocn.15076
8. Garde AH, Hansen AM, Hansen J. Sleep length and quality, sleepiness and urinary melatonin among healthy Danish nurses with shift work during work and leisure time. Int Arch Occup Environ Health. 2009;82:1219–1228. doi:10.1007/s00420-009-0419-4
9. Bazrafshan MR, Moravveji F, Soleymaninejad N, et al. Prevalence and effects of sleep disorders among shift–working nurse. Ann Trop Med Public Health. 2018;11:13. doi:10.4103/ATMPH.ATMPH_504_17
10. Eldevik MF, Flo E, Moen BE, Pallesen S, Bjorvatn B. Insomnia, excessive sleepiness, excessive fatigue, anxiety, depression and shift work disorder in nurses having less than 11 hours in–between shifts. PLoS One. 2013;8(8):e70882. doi:10.1371/journal.pone.0070882
11. Shy BD, Portelli I, Nelson LS. Emergency medicine residents’ use of psychostimulants and sedatives to aid in shift work. Am J Emerg Med. 2011;29(9):1034–1036.e1031. doi:10.1016/j.ajem.2010.06.004
12. Handel DA, Raja A, Lindsell CJ. The use of sleep aids among emergency medicine residents: a web-based survey. BMC Health Serv Res. 2006;6:136. doi:10.1186/1472-6963-6-136
13. Francis MN, Wishart IM, Williamson T, Iverach R. Use of pharmacologic sleep aids and stimulants among emergency medicine staff physicians in a Canadian Tertiary care setting: a web–based survey. Ann Emerg Med. 2019;73:325–329. doi:10.1016/j.annemergmed.2018.07.006
14. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Prev Med. 2007;45(4):247–251. doi:10.1016/j.ypmed.2007.08.012
15. Ngamjarus C, Chongsuvivatwong V, McNeil E. n4Studies: sample size calculation for an epidemiological study on a smart device. Siriraj Med J. 2016;68:160–170.
16. Thomas SJ, Calhoun D. Sleep, insomnia, and hypertension: current findings and future directions. J Am Soc Hypertens. 2017;11(2):122–129. doi:10.1016/j.jash.2016.11.008
17. Schutte–Rodin S, Broch L, Buysse D, Dorsey C, Sateia M. Clinical guideline for the evaluation and management of chronic insomnia in adults. J Clin Sleep Med. 2008;4(05):487–504. doi:10.5664/jcsm.27286
18. Persico N, Maltese F, Ferrigno C, et al. Influence of shift duration on cognitive performance of emergency physicians: a Prospective Cross–Sectional Study. Ann Emerg Med. 2018;72(2):171–180. doi:10.1016/j.annemergmed.2017.10.005
19. Wolf LA, Perhats C, Delao A, Martinovich Z. The effect of reported sleep, perceived fatigue, and sleepiness on cognitive performance in a sample of emergency nurses. J Nurs Adm. 2017;47(1):41–49. doi:10.1097/NNA.0000000000000435
20. Halm M. Night shift naps improve patient and workforce safety. Am J Crit Care. 2018;27:157–160. doi:10.4037/ajcc2018861
21. AlShareef SM. Occupational outcomes associated with sleep quality and excessive daytime sleepiness: results from a National Survey. Nat Sci Sleep. 2020;12:875–882. doi:10.2147/NSS.S271154
22. Richards JR, Stayton TL, Wells JA, Parikh AK, Laurin EG. Night shift preparation, performance, and perception: are there differences between emergency medicine nurses, residents, and faculty? Clin Exp Emerg Med. 2018;5:240–248. doi:10.15441/ceem.17.270
23. Grimberg A, Kutikov JK. 142 – hypothalamus: neuroendometabolic center. In: Polin RA, Abman SH, Rowitch DH, Benitz WE, Fox WW, editors. Fetal and Neonatal Physiology (Fifth Edition). Elsevier; 2017:1451–1461.e1452.
24. McBeth BD, McNamara RM, Ankel FK, et al. Modafinil and zolpidem use by emergency medicine residents. Acad Emerg Med. 2009;16(12):1311–1317. doi:10.1111/j.1553-2712.2009.00586.x
25. Culpepper L, Wingertzahn MA. Over–the–counter agents for the treatment of occasional disturbed sleep or transient insomnia: a Systematic Review of Efficacy and Safety. Prim Care Companion CNS Disord. 2015;17. doi:10.4088/PCC.4015r01798
26. Liira J, Verbeek JH, Costa G, et al. Pharmacological interventions for sleepiness and sleep disturbances caused by shift work. Cochrane Database Syst Rev. 2014;12(8):Cd009776.
27. Jorgensen KM, Witting MD. Does exogenous melatonin improve day sleep or night alertness in emergency physicians working night shifts? Ann Emerg Med. 1998;31:699–704. doi:10.1016/S0196-0644(98)70227-6
28. Wright SW, Lawrence LM, Wrenn KD, Haynes ML, Welch LW, Schlack HM. Randomized clinical trial of melatonin after night–shift work: efficacy and neuropsychologic effects. Ann Emerg Med. 1998;32:334–340. doi:10.1016/S0196-0644(98)70010-1
29. Franke AG, Bagusat C, McFarlane C, Tassone–Steiger T, Kneist W, Lieb K. The use of caffeinated substances by surgeons for cognitive enhancement. Ann Surg. 2015;261:1091–1095. doi:10.1097/SLA.0000000000000830
30. Temple JL, Bernard C, Lipshultz SE, Czachor JD, Westphal JA, Mestre MA. The safety of ingested caffeine: a comprehensive review. Front Psychiatry. 2017;8:80. doi:10.3389/fpsyt.2017.00080
31. Lieberman HR, Agarwal S, Caldwell JA, Fulgoni VL. Demographics, sleep, and daily patterns of caffeine intake of shift workers in a nationally representative sample of the US adult population. Sleep. 2020;43(3):zsz240. doi:10.1093/sleep/zsz240
32. Carvey CE, Thompson LA, Mahoney CR, Liberman HR. Caffeine: mechanism of action, genetics, and behavioral studies conducted in task simulators and the field. In: Wesensten N, editor. Sleep Deprivation, Stimulant Medications, and Cognition. Cambridge, UK: Cambridge University Press; 2012:93–107.
33. Bonnet MH, Arand DL. Studies of fatigue and human performance in the laboratory. In: Sharafkhaneh A, Hirshkowitz M, editors. Fatigue Management: Principles and Practices for Improving Workplace Safety. New York: Springer New York; 2018:13–27.
34. Williams GW, Shankar B, Klier EM, et al. Sensorimotor and executive function slowing in anesthesiology residents after overnight shifts. J Clin Anesth. 2017;40:110–116. doi:10.1016/j.jclinane.2017.04.002
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.