")
Back to Journals » Risk Management and Healthcare Policy » Volume 13
Exploring the Factors Affecting Bitter Melon Peptide Intake Behavior: A Health Belief Model Perspective
Authors Pan F , Hsu PK, Chang WH
Received 10 August 2020
Accepted for publication 28 September 2020
Published 20 October 2020 Volume 2020:13 Pages 2219—2226
DOI https://doi.org/10.2147/RMHP.S274154
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Frank Pan,1 Pang-Kuei Hsu,2 Wei-Hsiu Chang3
1Department of Hospitality, Pharmacy, Tajen University, Pingtung, Taiwan; 2Greenyn Biotechnology Co., Ltd, Taichung, Taiwan; 3Chang Wei Hsiu Pharmacy Co., Yunlin, Taiwan
Correspondence: Frank Pan
Department of Hospitality, Pharmacy, Tajen University, 20, Weixin Road, Yanpu, Pingtung 907, Taiwan
Tel +886 8 762 4002
Fax +886 8 762 3924
Email [email protected]
Pang-Kuei Hsu
Greenyn Biotechnology Co., Ltd., 5F, No. 43, Keya Road, Daya District, Taichung City, Taiwan
Tel +886-4-2238-2860
Fax +886-4-2238-9677
Email [email protected]
Purpose: Diabetes mellitus (DM) patients need to control their blood sugar level in order to achieve a good quality of life. This study was conducted using the health belief model (HBM), to explore the factors behind the bitter melon peptide (BMP) intake behavior and the role of self-efficacy in the model.
Materials and Methods: The subjects were type 2 diabetes mellitus patients in Taiwan. A structured questionnaire was adopted from the theory of health belief model and modified specifically for this study as an instrument to survey 292 DM patients, of whom 51.03% were female, 75.68% were married, and 49.32% were aged 40 to 64 years old. The data were analyzed using t-tests, one-way ANOVA and regression.
Results: Perceived susceptibility was the most sensitive in the response to the various demographic factors, whereas perceived barrier was the least sensitive. The HBM explained 38.0% of BMP intake behavior. Perceived benefits (β= 0.357) and perceived susceptibility (β= 0.348) were the major predictors. Self-efficacy mediated the relationship between perceived benefits and BMP intake behavior, as well as increased the variance explained to 51.30%.
Conclusion: The perceived benefits of taking BMP and perceived susceptibility to DM complications were the two major drivers acting on BMP intake behavior. The power of perceived benefits was mediated by self-efficacy in driving DM patients to take BMP regularly. Several ways of affecting perceived susceptibility and perceived benefits were suggested.
Keywords: mcIRBP-19, bitter melon, bitter gourd, Momordica charantia, perceived susceptibility, perceived benefits, self-efficacy
Introduction
Diabetes mellitus (DM) jeopardizes the human quality of life with a plethora of complications and is a major cause of mortality.1 This is indeed a major risk to human health. Despite the comprehensive diabetes education provided to DM patients, the death toll caused by DM in Taiwan remains high, and the expenditures attributed to DM complications have accounted for a large portion of the National Health Insurance (NHI) reimbursements in recent decades.2
Medical discipline generally agreed and advised DM patients to combine medications, physical activities and healthy diet (e.g. to take foods with lower glycemic index) in order to prevent and control DM and its complications. Despite the fact that the expenses for DM medications are covered by the NHI in Taiwan, the number of DM patients remains high.2 Thus, a plethora of alternative medicines and nutraceuticals were adopted in the Taiwan market, among which the herbal-based nutraceutical such as cinnamon and bitter melon are the most wanted.
Bitter melon (also called bitter gourd, Momordica charantia) is one of the common daily foods in Taiwan and has long been widely perceived by the indigenous populations in Asia, South America, India and East Africa, as a healthy vegetable that helps in regulating the human internal organs. 3 Although the effects of bitter melon in lowering blood sugar have not yet received consensus,3 some evidences had shown the significant effects of bitter melon.3–6
Bitter melon peptide (BMP) is one of the products that is recently developed and has received wide attention. 4–9 BMP with mcIRBP-19 (named as Insumate®) was developed and launched to the Taiwan market as a nutraceutical, it has been proven to be effective in regulating DM patient blood glucose levels. 9 Other than prescribed medications, taking this particular BMP as an aid to regulate blood sugar has become common in Taiwan since its introduction. The phenomenon of the wide acceptance and sharp growth of this captioned product in the nutraceutical market triggered this research interest in exploring a scientific method. The purpose of the current research is to explore the possible factors behind BMP intake behavior.
As suggested by the literature of health belief model (HBM), perceived threats drive people to seek prevention measures, and the perceived utility of an instrument or measure supporting targeted health goals enables patients to adopt the instrument subject in order to gain accessibility (or barriers) to such an instrument.10 Under the same logic, DM patients who are exposed to the threats of complications would be driven to take preventive actions.11
Other than conventional medical treatment (e.g. metformin), regular exercise and healthy diet, DM patients may take BMP as long as they believe that such nutraceutical may provide protection in the battle against DM complications subjected to accessibility (or barriers) to BMP.
Based on the HBM, three hypotheses were proposed. H1: The stronger the perceived threat of DM complications and the stronger the perceived benefits of BMP in preventing DM complications, the more likely DM patients would take BMP. H2: The more barriers to accessing BMP the patients perceive, the less likely they would take BMP. Rosenstock et al added a concept of self-efficacy 12 to the original HBM 13,14 in order to increase its predictive power. Since self-efficacy appears to have extraordinary power over constructs in many studies, self-efficacy may override other predictors of HBM.15,16
Unlike previous studies, this study proposed that a patient’s self-efficacy would be activated by perceiving the benefits BMP may bring in order to improve glycemic control. This means that a patient’s self-efficacy will mediate the association between perceived benefits and BMP intake intention. Thus, a DM patient’s self-efficacy positively mediates the relationship between perceived benefits and BMP intake. H3: The relationship between perceived benefit and BMP intake behavior will be positively mediated by self-efficacy.
Materials and Methods
Subjects
Prior to approaching prospective subjects, the study was approved by the Institutional Review Board (IRB) of Pingtung Christian Hospital (PCH; Pingtung City, Taiwan) with approval number IRB552B. The subjects were recruited on a volunteer basis when they refilled their medication for chronic diabetes from designated pharmacies. A total of 292 valid responses were included in this study, all respondents were over 20 years old and were diagnosed by qualified physicians as T2DM patients with at least 126 mg/dL of fasting blood glucose (FG) level, or at least 7.0% (equivalent to 53 mmol/mol) glycated hemoglobin (HbA1c). Respondents that failed to complete the life style survey, or significantly violated the physician’s advice, or missed major parts of the questionnaire were deleted.
Research Instrument
A structured questionnaire was developed based on the HBM9 and revised with a pre-test with 50 subjects with good levels of reliability and validity. A 5-point scale was applied to measure the responses of each construct to the items. The questionnaire which includes a survey on respondent’s demographic data contained four main constructs of the HBM, that is, perceived susceptibility and severity of DM complications, perceived benefits and barriers to taking BMP in addition to other medication and self-efficacy.
The questionnaire was accompanied by a life style survey and items to ensure that the respondents remained under regular DM management, such as medication, adhering to the doctor’s advice, physical exercise, healthy diet, etc. Cases that obviously violated the doctor’s advice were excluded from the survey.
Constructs
The construct consists of items on perceived susceptibility that inquired into the subject’s perception toward the possibility of specific health problems, including diseases affecting the cardiovascular system, kidney, eyes, feet and sexual function. As a part of the perceived threat of health problems, the perceived severity construct inquired into how worried the respondents were, regarding the consequences of these health problems. In dealing with such health problems, the perceived benefits and barriers were used to inquire how the subject would foresee the results and obstacles with regard to this BMP capsule. Perceived benefit was used as a construct to measure how the respondents believed BMP intake could be helpful in regulating glycemic levels and consequently help to retard or avoid complicated disease. Perceived barrier was used as a predictor to reflect how difficult the respondents perceived taking BMP in terms of cost, accessibility, and other possible barriers. The self-efficacy construct inquired how confident the subjects were in taking this specific nutraceutical.
Reliability and Validity
The questionnaire had an acceptable reliability in both the pre-test and actual test. Construct validities were at acceptable levels with convergent validity between 0.760 and 0.921 and discriminant validity between 0.727 and 0.887, as shown in Table 1.
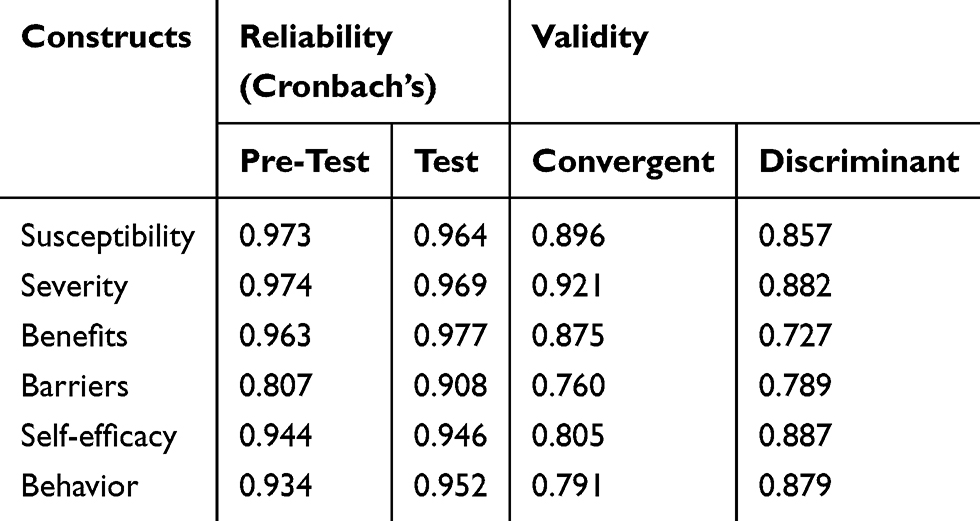 |
Table 1 Reliability and Validity of Constructs |
Measurement
Capsule of bitter melon peptide (BMP), which contains mcIRBP-19 as the active ingredient, is a nutraceutical product of BMP offered by Greenyn Biotechnology Co., Ltd. (Taichung, Taiwan). It has been claimed to regulate blood sugar and this BMP capsule was used as an alternative solution for regulating blood sugar level other than the conventional treatment. Participants were asked to complete the survey voluntarily and to provide written informed consent with a signature prior to the investigation process. Participants were also requested to read the document of product description regarding the information on test results9 of the captioned BMP nutraceutical as well as dose information and the selling price before entering the answering process.
Data were analyzed using SPSS 20.0 (Armonk, NY: IBM Corp. Sourced from TriStar, Kaohsiung City, Taiwan). Statistical analysis techniques applied in the study include descriptive statistics to examine the demographic distribution of the subjects, as well as independent t-tests and one-way ANOVA to examine whether the average difference was significant between groups with two and three categories, respectively, in terms of the major constructs of the study.
Additionally, multiple regression analysis was performed to reveal the effects of each independent variable on the dependent variable. All significance levels were set at p ≦ 0.05.
Results
Description of Samples and Variables
The demographic distribution of subjects included in the study is shown in Table 2. In general, there were slightly more female subjects than male subjects, most subjects were married, more than 70% of subjects were at least 40 years old, roughly 65% of respondents were at least junior educated, around 40% of them were retired or jobless, and the majority of respondents earned no more than NTD 30,000 per month (1000 USD equivalent).
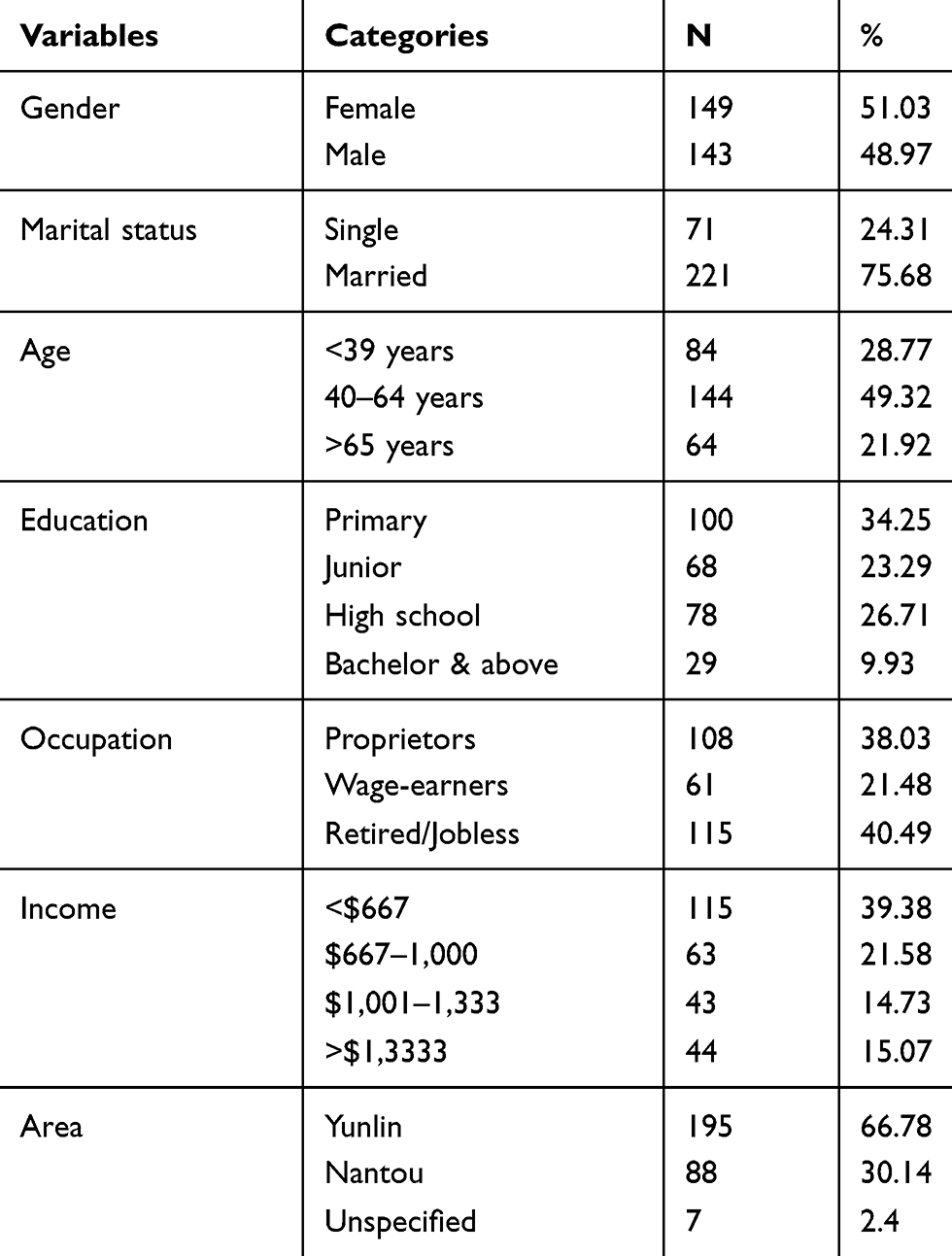 |
Table 2 Demographic Distribution of Samples |
Health Beliefs and Demographic Factors
Mean values were calculated to reveal the comparative weights among independent variables, which were then used to determine whether the values of these variables varied along with demographic factors. Demographic factors include gender, marital status, age, education, income, and residence area; marital status did not make any significant difference. Male respondents perceived higher susceptibility than female subjects (male = 4.15, female = 3.91), but not in other variables (Table 3 and Table a1 in supplementary).
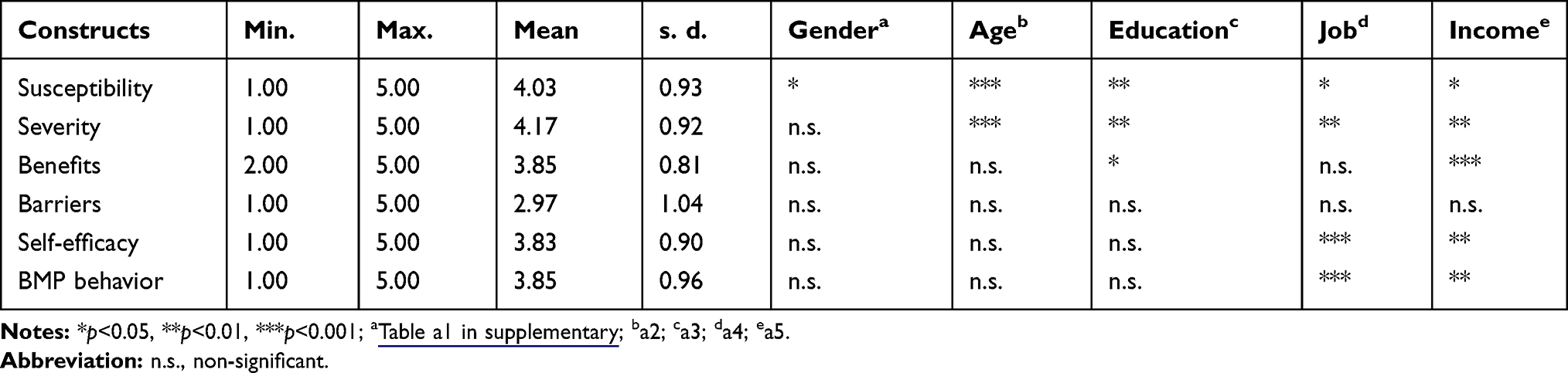 |
Table 3 Mean Scores, t-Test, and One-Way ANOVA of Variables |
The group over the age of 65 years perceived higher susceptibility (F = 4.07, p = 0.02) and severity (F = 5.41, p = 0.00) than those in the group aged below 39 years old (Table 3 and Table a2 in supplementary). The average scores of susceptibility and severity increased with age.
Regarding educational levels, respondents with high school education perceived higher health threat levels (F = 3.90, p = 0.01; F = 4.72, p = 0.01) than those with elementary and lower education. Those with other educational levels showed no significant difference from those with a high school education for almost all variables (Table 3 and Table a3 in supplementary).
Compared to other occupational types, respondents who were self-employed or owned a personal business perceived higher threat levels (susceptibility, F= 3.43, p = 0.03; severity, F = 4.49, p = 0.01) regarding DM complications. However, these subjects were more confident (F = 6.38, p = 0.00) and more willing to take BMP (F = 5.85, p = 0.00) (Table 3 and Table a4 in supplementary).
As far as the personal income is concerned, the results show that respondents with a higher income were more concerned about the threat of DM complications (susceptibility, F = 2.75, p = 0.04; severity, F = 4.29, p = 0.01) and the benefits of BMP on glycemic control (F = 4.56; p = 0.00). A higher income made DM patients more confident (F = 3.65, p = 0.01) and willing to take BMP (F = 3.93, p = 0.01) (Table 3 and Table a5 in supplementary).
Predicting BMP Intake Behavior
The regression analysis results show that the model 1 explained 38.0% of variance in BMP intake behavior, of which perceived benefits of BMP acted as the major predictor (β=0.357), followed by perceived susceptibility of diabetic complications (β=0.348), the other two predictors of perceived severity and barriers were not significant (M1 in Table 4).
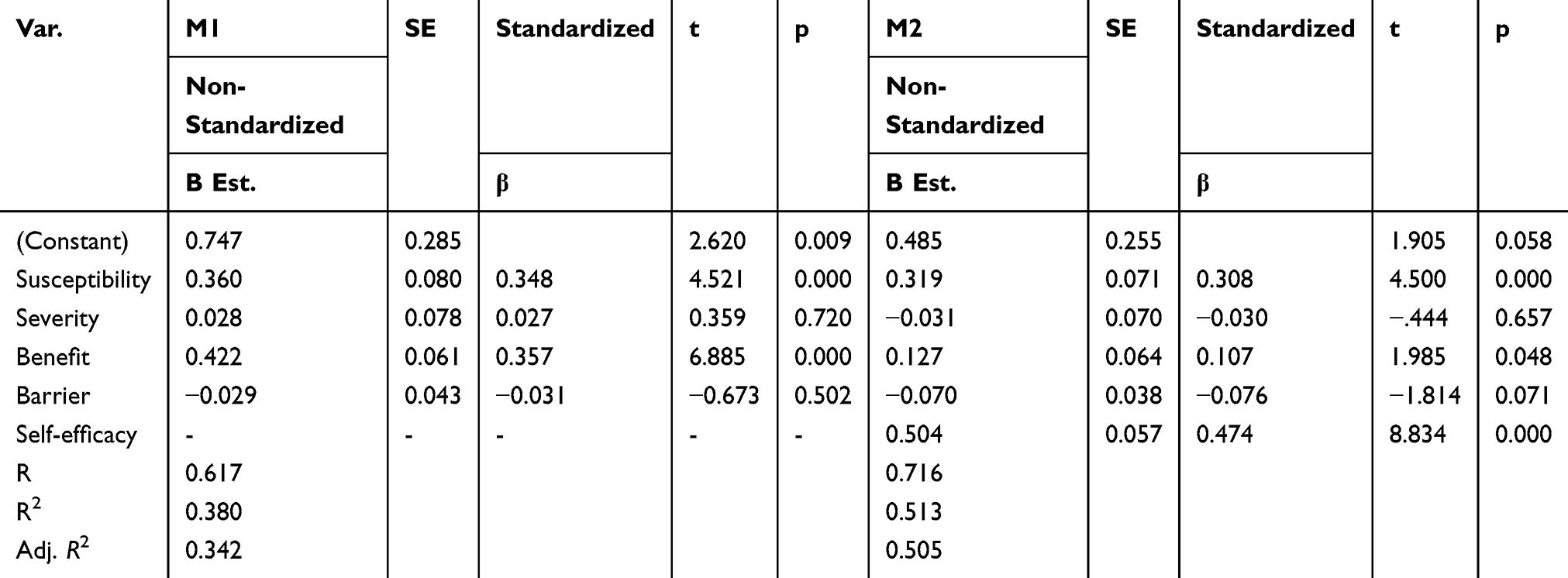 |
Table 4 Health Beliefs, Self-Efficacy, and BMP Intake Behavior |
The Role of Patient Self-Efficacy
Self-efficacy in this study referred to a patient’s confidence in his/her ability to take BMP in order to prevent the progress of DM complications.12,15,16 Although the literature generally accepts that self-efficacy could positively enhance the prediction power of the original HBM independent variables, previous research has found a negative association between DM patient self-efficacy and HbA1c levels.15 In addition, self-efficacy appears to be the sole important factor that supersedes other HBM predictors. However, to conclude that an individual’s self-confidence dominates everything did not make sense. This study argues that an individual’s self-efficacy could be strengthened by believing in the benefits of BMP, which positively enhances an individual’s intention to take BMP. In other words, self-efficacy is not a predictor, but rather a mediator affected by the perceived benefits of BMP, which then affects BMP intake behavior.
As shown in the M2 of Table 4, self-efficacy is added as new variable. The variance explained for BMP intake behavior increased from 38.0% (R2=0.380) to 51.30% (R2=0.513), self-efficacy was strongly affected by perceived benefit (β = 0.610) and became a major predictor (β = 0.474) of BMP intake behavior, and the direct power of perceived benefit reduced from 0.357 to 0.107. This denotes that a DM patient’s perceived benefit is partially mediated by self-efficacy when activating the BMP intake behavior (Figure 1). Perceived susceptibility still acts as a significant predictor with lower effects (β = 0.308), and perceived severity, as well as barrier, remains non-significant.
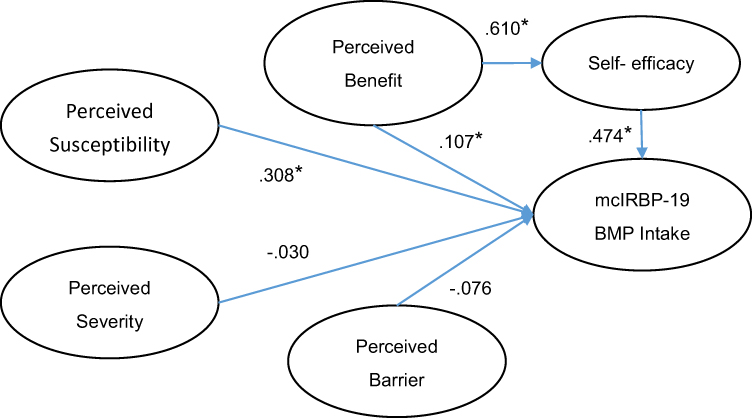 |
Figure 1 DM patient’s mcIRBP-19 BMP intake behavior model. *denotes a significant level at p<0.05. |
Discussion
Perceived Threats, Benefits, and Barriers
Compared to other variables, perceived susceptibility had the highest average values, followed by perceived severity. This means that DM patients pay more attention to the disease than the associated solutions or treatments, and are most concerned about the consequences of DM complications. DM complications issues could gain better readership than those of other solutions. As the fear appeal theory advocates that a threatening communication containing frightening material could be very effective,17 DM patients could be altered (or shocked) by possible DM complications and associated consequences prior to becoming aware of possible solutions. This understanding of consumer’s perception toward complication can be helpful for health educators and nutraceutical businesses when developing communication campaigns.
Many studies have shown susceptibility as the major threatening factor on health behavior, whereas others have shown this regarding severity. The literature suggests that varied perceptions of a health risk may be critical to differentiating levels of perceived susceptibility and perceived severity.18 The fact that perceived susceptibility is the main predictor of health threats in the current research denotes that the risk perception of DM complications may come from the result of an increase in perceived susceptibility. 18,19
The literature suggests that health risk may not adequately predict preventive behavior and should include outcome expectancy.19 Based on the theory of the HBM, the construct of perceived benefit in the current study could be viewed as an alternative to outcome expectancy.
The study included major DM complications such as kidney diseases, neurological, circulatory, oral, ophthalmic and skin complications, and other specified diabetic conditions as outlined by The International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10) in the questionnaire to inquire into the respondent’s perceptions of susceptibility and severity. The perceived benefit of BMP was measured to reflect the respondent’s trust and confidence in the function of BMP.
Demographic Variables
Male subjects were more concerned about the possibility of suffering from DM complications than female subjects, but gender was not associated with significant differences in other HBM variables. Since susceptibility is a stronger predictor than severity, communication with male DM patients should particularly focus on susceptibility rather than on severity.
Although the incidence of type 2 diabetes in youth is increasing, older age is typically a risk factor for DM. Nearly 72% of subjects who came to the pharmacy for their refill prescription were at least 40 years old, and only 28% were 39 years old or younger. DM patients who were at least 65 years old perceived significantly stronger threats from DM complications. This group of sufferers had a longer history of DM and may have been exposed to more comprehensive and intensive information regarding DM and the associated complications than younger DM patients. However, other predictors and BMP intake behavior were not significantly different according to age.
High school was the most significant level than the other educational backgrounds in the average tests of all health belief variables as well as BMP intake behavior. This group of respondents perceived more urgent health threats, more useful BMP benefits, and accordingly comparatively stronger BMP intake behavior. Health literacy/knowledge and its actions on health, such as diet and regular physical exercise, are essential to maintaining a good level of blood sugar, and a high school education seems to be a critical level for this purpose.
Although the National Health Insurance (NHI) of Taiwan provides DM patients comprehensive care for most DM complications with fractional costs as personal burden, other expenses that are not covered by insurance, such as personal preferences for inpatient services and medical supplies, are relatively high for most wage earners. Compared to the general wage earners and retired persons, business owners are generally richer and more concerned about the risks of DM complications. Rich persons generally have better opportunities to practice their will to gain whatever benefits there are for their health, for example, to regularly take BMP in addition to treatments that are covered by the NHI.
The Roles of Self-Efficacy
Other than health risk and outcome expectancy of the solution in the HBM, self-efficacy is another significant factor in shaping one’s health behaviors,19 including glycemic control in DM patients.15,16 Previous studies tended to argue for a direct association 15,16 in lowering a patient’s HbA1c levels. In studies informed by HBM theory, the power of self-efficacy was frequently found to override other predictors in the HBM. It seems from these studies that self-efficacy is the sole factor predicting a DM patient’s disease control behavior. In other words, the perceived threats of DM complications and the perceived benefits of particular disease alternatives are useless in a DM patient’s health decision-making process. This is incorrect in the real world and may mislead decisions for health educators and entrepreneurs.
Self-efficacy apparently has strong effects on leading a health promotion decision. However, the role of self-efficacy in affecting a DM patient’s health decision remains questionable. Previous studies mostly included self-efficacy as an independent predictor in HBM, only a few indicated that self-efficacy had only an indirect effect on glycemic control.20 The current study proposed and tested the notion that self-efficacy is a mediator of perceived benefit and intake behavior in the model. This means that the major predictors of DM patient’s BMP intake behavior are perceived threats of DM complications and perceived benefits of BMP, and perceived benefits influence behavior through self-efficacy.
In other words, self-efficacy is an important factor that links a patient’s perceived benefit and the targeted solution of health problems. This means that DM patients first perceive the benefit of BMP in preventing DM complications, and then this perception activates the respondent’s self-efficacy. Accordingly, perceived benefit and self-efficacy can jointly predict BMP intake behavior with a better explanation of variance than a single factor.
Limitations of the Study
The first limitation of the study is the DM patients as the study subjects. These subjects were recruited from Yunlin and Nantou in Taiwan. Although these are the top two counties regarding the DM occurrence rate, subjects included in this study may not sufficiently represent the entire population of DM patients in Taiwan.
Taking the difference of cultural practice into account, the current study was conducted in an area that grows and eats bitter melon as a daily vegetable. Research results may not be generalizable to other food cultures.
Action cue was theorized as a part of the original HBM to measure the effects of the respondent’s social network. Since the main purpose of the current study was to explore the impacts of major health belief constructs of the HBM with a special focus on the roles of self-efficacy on the respondent BMP intake behavior, the current study did not include the effects of action cues. Interpretation of the test results should be made with caution.
Outcome expectancy of particular health problems has been proposed in the literature as a supplementary to complete a health behavior prediction.14 The current study showed that the perceived benefits of the HBM theory could be used as a substitute for outcome expectancy. However, the authors did not test the difference and provide evidence accordingly for this argument.
Conclusion
The major risks to the T2DM patients are those severe DM complications. To manage this health risk, BMP with mcIRBP (specifically named as Insumate®) has been widely introduced through multiple media and sales channels as a reliable nutraceutical that helps regulate a diabetic patient’s blood glucose level in addition to the conventional medication treatment.2–4
Perceived susceptibility but not the severity of DM complications and perceived benefits of BMP are significantly active in predicting a patient’s BMP intake behavior in the original HBM theory. By adding DM patient’s self-efficacy in the new model, as hypothesized in this study, it acts as a mediator between perceived benefit and intake behavior, and consequently explains the DM patient’s behavior better than the original model.
Communication of DM patients with the fear of DM complications susceptibility is suggested to be more effective than the fear of severity. DM patient’s perceived benefit and associated self-efficacy are central to educating BMP intake behavior.
Worthy for further research is how to assess patient’s perceived susceptibility of DM complications and perceived benefits of BMP. At this stage, the health and healthcare-related professional or healthcare institute is suggested to develop a list of physical symptoms and outcomes of such complications, and continuously dispatch widely to the DM patients and the public as a reminder of DM management. Risk of DM complication could be managed and prevented. Health professionals may further develop educational material including slogan in plain and easy-understanding words to educate DM patients, especially those who are in poor health literacy, the mechanism BMP help regulating blood glucose.
Acknowledgments
The study was supported by the research project numbered JH-106019 of Tajen University, Taiwan. The authors are grateful to the anonymous reviewers’ valuable and constructive comments which have sharply improved the quality of the manuscript, we are also indebted to the editor’s corrections and suggestions on some errors in the original version. All possible errors remain our sole responsibility.
Disclosure
Pang-Kuei Hsu is an employee of Greenyn Biotechnology Co., Ltd. Taichung, Taiwan; Wei-Hsiu Chang is an employee of Chang Wei Hsiu Pharmacy Co., Yunlin, Taiwan and reports grants from Chang Wei Hsiu Pharmacy Co., during the conduct of the study. The authors report no other potential conflicts of interest in this work.
References
1. Egede LE, Ellis C. Diabetes and depression: global perspectives. Diabetes Res Clin Pr. 2010;87(3):302–312. doi:10.1016/j.diabres.2010.01.024
2. Health Promotion Administration. Ministry of Health and Welfare. Statistics of Health Promotion; 2018. Available from: http: Users/user/Downloads/Statistics+of+Health+Promotion+2018%20(1).pdf.
3. Joseph B, Jini D. Antidiabetic effects of Momordica charantia (bitter melon) and its medicinal potency. Asian Pac J Trop Dis. 2013;3(2):93–102. doi:10.1016/S2222-1808(13)60052-3
4. Lo HY, Ho TY, Lin C, Li CC, Hsiang CY. Momordica charantia and its novel polypeptide regulate glucose homeostasis in mice via binding to insulin receptor. J Agric Food Chem. 2013;61:2461–2468. doi:10.1021/jf3042402
5. Lo HY, Ho TY, Li CC, Chen JC, Liu JJ, Hsiang CY. A novel insulin receptor-binding protein from Momordica charantia enhances glucose uptake and glucose clearance in vitro and in vivo through triggering insulin receptor signaling pathway. J Agric Food Chem. 2014;62:8952–8961. doi:10.1021/jf5002099
6. Lo HY, Li CC, Ho TY, Hsiang CY. Identification of the bioactive and consensus peptide motif from Momordica charantia insulin receptor-binding protein. Food Chem. 2016;204:298–305. doi:10.1016/j.foodchem.2016.02.135
7. Garau C, Cummings EF, Phoenix DA, Singh J. Beneficial effect and mechanism of action of Momordica charantia in the treatment of diabetes mellitus: a mini review. Int J Diabetes Metab. 2003;11:46–55.
8. Bhushan MS, Rao CHV, Ojha SK, et al. An analytical review of plants for anti-diabetic activity with their phyto constituent and mechanism of action. Int J Pharm Sci Res. 2010;1:29–46.
9. Hsu PK, Pan FF, Hsieh CS. mcIRBP-19 of bitter melon peptide effectively regulates diabetes mellitus (DM) patients’ blood sugar levels. Nutrients. 2020;12(5):1252. doi:10.3390/nu12051252
10. Carpenter CJ. A meta-analysis of the effectiveness of health belief model variables in predicting behavior. Health Commun. 2010;25(8):661–669. doi:10.1080/10410236.2010.521906
11. Nathan DM. Long-term complications of diabetes mellitus. N Engl J Med. 1993;328:1676–1685.
12. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215. doi:10.1037/0033-295X.84.2.191
13. Rosenstock IM, Strecher VJ, Becker M. Social learning theory and the health belief model. Health Educ Q. 1988;15(2):175–183. doi:10.1177/109019818801500203
14. Janz NK, Becker MH. The health belief model: a decade later. Health Educ Q. 1984;11(1):1–47. doi:10.1177/109019818401100101
15. Al-Khawaldeh OA, Al-Hassan MA, Froelicher ES. Self-efficacy, self-management, and glycemic control in adults with type 2 diabetes mellitus. J Diabetes Complicat. 2012;26(1):10–16. doi:10.1016/j.jdiacomp.2011.11.002
16. Chih AH, Jan CF, Shu SG et al. Self-efficacy affects blood sugar control among adolescents with type I diabetes mellitus. J Formos Med Assoc. 2010;109(7):503–510.
17. Peters GJY, Ruiter RA, Kok G. Threatening communication: a critical re-analysis and a revised meta-analytic test of fear appeal theory. Health Psycho Rev. 2013;7:S8–S31. doi:10.1080/17437199.2012.703527
18. El-Toukhy S. Parsing susceptibility and severity dimensions of health risk perceptions. J Health Commun. 2015;20(5):499–511. doi:10.1080/10810730.2014.989342
19. Seyde E, Taal E, Wiegman O. Risk-appraisal, outcome and self-efficacy expectancies: cognitive factors in preventive behaviour related to cancer. Psycho Health. 1990;4:99–109. doi:10.1080/08870449008408144
20. Lin K, Park C, Li M, et al. Effects of depression, diabetes distress, diabetes self-efficacy, and diabetes self-management on glycemic control among Chinese population with type 2 diabetes mellitus. Diabetes Res Clin Pr. 2017;131:179–186. doi:10.1016/j.diabres.2017.03.013
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.