")
Back to Journals » Patient Preference and Adherence » Volume 12
Exploring the experiences of older Chinese adults with comorbidities including diabetes: surmounting these challenges in order to live a normal life
Authors Ho HY, Chen MH, Lou MF
Received 30 July 2017
Accepted for publication 15 November 2017
Published 30 January 2018 Volume 2018:12 Pages 193—205
DOI https://doi.org/10.2147/PPA.S147756
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Hsiu-Yu Ho,1,2 Mei-Hui Chen,2,3 Meei-Fang Lou1
1School of Nursing, College of Medicine, National Taiwan University, 2Department of Nursing, Yuanpei University of Medical Technology, 3National Taipei University of Nursing and Health Sciences, Taipei, Taiwan, Republic of China
Background: Many people with diabetes have comorbidities, even multimorbidities, which have a far-reaching impact on the older adults, their family, and society. However, little is known of the experience of older adults living with comorbidities that include diabetes.
Aim: The aim of this study was to explore the experience of older adults living with comorbidities including diabetes.
Methods: A qualitative approach was employed. Data were collected from a selected field of 12 patients with diabetes mellitus in a medical center in northern Taiwan. The data were analyzed by Colaizzi’s phenomenological methodology, and four criteria of Lincoln and Guba were used to evaluate the rigor of the study.
Results: The following 5 themes and 14 subthemes were derived: 1) expecting to heal or reduce the symptoms of the disease (trying to alleviate the distress of symptoms and trusting in health practitioners combining the use of Chinese and Western medicines); 2) comparing complex medical treatments (differences in physician practices and presentation, conditionally adhering to medical treatment, and partnering with medical professionals); 3) inconsistent information (inconsistent health information and inconsistent medical advice); 4) impacting on daily life (activities are limited and hobbies cannot be maintained and psychological distress); and 5) weighing the pros and cons (taking the initiative to deal with issues, limiting activity, adjusting mental outlook and pace of life, developing strategies for individual health regimens, and seeking support). Surmounting these challenges in order to live a normal life was explored.
Conclusion: This study found that the experience of older adults living with comorbidities including diabetes was similar to that of a single disease, but the extent was greater than a single disease. The biggest difference is that the elderly think that their most serious problem is not diabetes, but rather, the comorbidities causing life limitations. Therefore, compared to the elderly suffering from a single disease of diabetes, medical professionals not only care about physiological data of the elderly but also pay attention to the impact of comorbidity on their lives.
Keywords: diabetes, comorbidity, multimorbidity, elderly, older adult, life experience
Introduction
The prevalence of diabetes increases year by year, as do the health care costs associated with the disease. In addition, diabetes patients often have comorbidities, with about 97.5% of diabetes patients having at least one comorbidity and 88.5% having two or more comorbidities.1 Comorbidities have become one of the greatest challenges of the health care system. Comorbidities not only increase the health care needs, utilization, and mortality of people with diabetes,2–4 they also increase the complexity of disease management and the burden of self-management for affected patients.5–7 Comorbidities present unique self-management challenges and more complex care needs than a single disease because of the interactions between pathologies, confusing or conflicting self-management information, and drug interaction problems.8–10 However, most clinical care guidelines are still based on single-disease studies, and limited studies have been conducted to reveal case management and clinical care for patients with multimorbidities.4,9,11,12 Health care professionals often follow their own value systems and ignore patients’ choices, priorities, and lifestyles.12 To provide a comprehensive care, a health care professional should first understand how diabetic elderly live with comorbidities in order to establish appropriate clinical care guidelines.
Most of the life experience studies of patients have focused on those with only a single disease. These studies found that the patients revealed negative psycho-social problems, saw diabetes as “a silent disease,” and would face difficulties in managing the disease. Also, they would potentially need access to various resources and services. They expressed that they could receive the support of encouragement, caring, and empathy from friends, relatives, peers, and health care professionals, and they were also able to reveal both resilience and an optimistic outlook on life, although they were full of anxiety, fear of hypo-/hyperglycemia and complications, depression, and other passive emotions.13–15 Patients with diabetes typically are motivated to engage in self-management of diabetes, because they have concerns about the anticipative effects of diabetes, wishing to “stay well,” maintaining their independence, and improving their quality of life.16 However, their comorbidities, medication management, and blood glucose monitoring could also impact their self-management.6,17 Considering the facilitators and barriers, available social resources, the diversity and capacity of social networks, these will impact on patient help-seeking behavior, and the search for and use of information. With more resources, the accumulation and use of information for these patients will become more effective. When considered in conjunction with time factors, this would allow patients to better commit themselves to self-management and work toward recovery.18–21 In the self-management process, the collective support provided by a spouse, and the friends, relatives, and peers can help a patient in maintaining and adhering to an appropriate diet and exercise regimen. However, if the patient is unaware of, or otherwise unable to avail himself or herself of, the support, disease management efforts will become less effective. While positive lifestyle changes are easy to implement at the start of a program, maintaining them over time may require additional individual support, guidance, education, and encouragement to correct knowledge gaps and sustain flagging commitment to the regimen.22–25 What patients seek from medical professionals is a feasible remedy or management program, possibly supplemented with information and practical support.26,27 Initial physician–patient relationship is established on the basis of trust, nonjudgmental acceptance, open communication, and the sincerity of both parties. However, physicians often focus on objective data and measurements such as blood pressure and HbA1C levels, while their patients typically have no understanding of these data or their implications. Conversely, collaborative decision-making can aid self-management. Hence, if the physician can provide the patients with treatment options that completely explain their own risks and benefits, allow the patients to express their concerns, values, and preferences, and ensure that the selected plan is consistent with the patients’ rights, needs, and aspirations, better disease-management results are more likely.14,28–30
Compared with the living experiences of persons with a single disease, there have been relatively few studies concerning the living experiences of elderly patients with comorbidities that include diabetes. The small numbers of studies that have been undertaken, meanwhile, show that complex treatment plans and multimorbidities may impede the motivation and confidence of patients in taking prescribed medications.31 Their comorbidities prompt emotional reactions to their health conditions, including fears of additional complications and regrets related to the future possibility of dialysis. These patients also complained about the inconsistent and incomplete information that they received, poor physician–patient communication, difficulties in balancing work and health care commitments, and the limited understanding of the multimorbidities that they had. These are all factors that will lead to difficulties in complying with complex treatment plans.10,32,33 While such patients are generally committed to avoiding the complications of diabetes, managing their comorbidities may take precedence in their daily lives, to the extent that they may even prioritize the other comorbidities over diabetes, depending on the severity of those conditions. They may, in turn, become frustrated, confused, and overwhelmed with complex or conflicting treatment recommendations, especially those relating to diet, physical activity, and medications. Compared to other burdens and distresses they face in life, some of these patients may treat diabetes as a less important problem.34,35
In Asian countries, medical pluralism, or the use of mixed medical systems, is widespread. In general, Chinese people have a preference for the combined use of conventional and traditional medicines as a means of controlling disease and promoting a state of comfort, an approach that can make the treatment and decision-making process for a given patient even more complex and multidimensional.36,37 Furthermore, while many elderly Asian people dislike Western medicine, they have generally come to rely upon it. At the same time, notions of expected family roles, cuisine culture, and a lack of reliable information sources and physician–patient communication can combine to pose challenges to patients’ self-management.38,39
Comprehensive literature found that multimorbidities have a far-reaching impact on the bodies and minds of the elderly and society as whole. Such an impact includes symptoms and psychological distress, the need for individualized self-management and complex care, inconsistent information, poor physician–patient communication, and medical pluralism. Thus, in order to design appropriate treatment programs for elderly Chinese patients with comorbidities including diabetes, it is also necessary to understand and incorporate traditional Chinese cultural considerations in the required care guidance or intervention program.
Subjects and methods
This study was performed using qualitative research methods, including semistructured, open, and in-depth one-on-one interviews, to explore the experiences of elderly persons living with comorbidities including diabetes. All the selected participants met the following criteria: age >65 years, a diagnosis of type 2 diabetes and other comorbidities, no hospitalization within the preceding 6 months, and the ability to communicate in Mandarin and Taiwanese.
Data for this study were collected by the first author (HYH) at a medical center in northern Taiwan. Written consent was obtained from each participant, and then the recorded interviews were conducted at the participant’s home at times convenient for both the interviewer and participant. The interview sessions were conducted from October 15, 2011, to June 30, 2012, with each session lasting 60–90 minutes. The semistructured interview guidelines used in the study were based on a review of the related literature and the author’s own clinical experiences, as well as on discussions with experts in this field. The following are examples of some of the prompts and questions used in the interviews: “Please describe your suffering resulting from these diseases;” “How do these diseases change your life?” and “How do you cope with these lifestyle changes?” Interview skills and techniques were used in the data collection in order to encourage the elderly participants to express themselves as openly as possible while still adhering to the topic and maximizing the amount of information provided. This study depended on the amount, integrity, and richness of the information collected and proceeded until data saturation was achieved.
Ethical considerations
This study was reviewed and approved by the Research Ethics Committee of the National Taiwan University Hospital (201108020RC). Informed consent was obtained before the start of a given interview. These participants have consented to the publication of the case details and responses. Any personal identifying information was deleted from the study and the analysis of each case number in order to protect the privacy and anonymity of the participants.
Data analysis
In this study, the data were analyzed using Colaizzi’s phenomenological approach,40 with the following steps: 1) The researchers listened carefully to the recorded interview content in order to have a complete understanding of the overall experience and then transcribed each interview verbatim as text, resulting in a faithful presentation of the original life experience data of the elderly Taiwanese participants living with comorbidities including diabetes. 2) The researchers repeatedly read, analyzed, and considered the meaningful sentences in the text. 3) The researchers extracted various meanings from the relevant sentences. 4) Keeping an open mind, the researchers carefully evaluated these meanings to formulate an interpretation of them which was consistent in terms of their common characteristics and common sense in order to, in turn, determine the context of the life experiences sought in the study. 5) The researchers reevaluated the results and tested their conclusions as a complete description. 6) Based upon the overall description, the researchers compiled the essence of the participants’ life experiences. 7) Finally, the researchers asked the elderly participants to review the study results to determine whether they accurately reflected their true experiences, and if not, to correct, clarify, and amplify the information included in the study results.
In this study, a total of 12 elderly participants with comorbidities including diabetes were selected to participate in the in-depth interviews. No new concepts resulted from the data analysis of the 11th interviewee’s interview; however, we interviewed the 12th patient to confirm that data saturation had been achieved at that point.
Credibility
The rigor of the study was governed by the Lincoln and Guba criteria for trustworthiness.41 Before each interview, the researcher established a trust relationship with the elderly participant, and then the entire interview was recorded and transcribed verbatim. The interviewer observed the nonverbal behavior of the elderly participant, as well. The first and second authors independently analyzed the verbatim transcripts of the three participants and then discussed them. After achieving consensus and consistency, the first author performed the analysis of all the verbatim transcripts. Member checking was performed at the same time. The results of the data analysis were reviewed with two of the study participants in order to confirm that the results of the study were compatible with their experiences, that is, as a way of verifying the credibility of the study. All analyses were repeatedly discussed among the research team members to increase the dependability of the study. The interview records, notes, and audio tapes were logged with respect to time and date. The process of coding, categorizing, and forming the themes for the original data allowed the reviewers to easily access and search the data. The process of deriving the original data can be clearly demonstrated and could be used to support the confirmability of this study. The researchers described the context of the data and provided a detailed description in order to explain the meaning of the phenomena experienced by or the underlying meaning of the behaviors of the elderly participants with comorbidities including diabetes through the use of phenomenological research steps. The results convey their real-life contexts and can thus provide a practical reference for medical professionals in clinical practice.
Results
A total of 12 elderly participants with comorbidities including diabetes were interviewed for this study. Their average age was 78.83 years, and the majority of the participants were female, married, living with their family, and illiterate, with an economic status described as “just getting by” (Table 1). This study found that the living experiences of these elderly participants with comorbidities including diabetes were often focused on “surmounting these challenges in order to live a normal life”. These findings were summed up in 5 themes and 14 subthemes (Table 2).
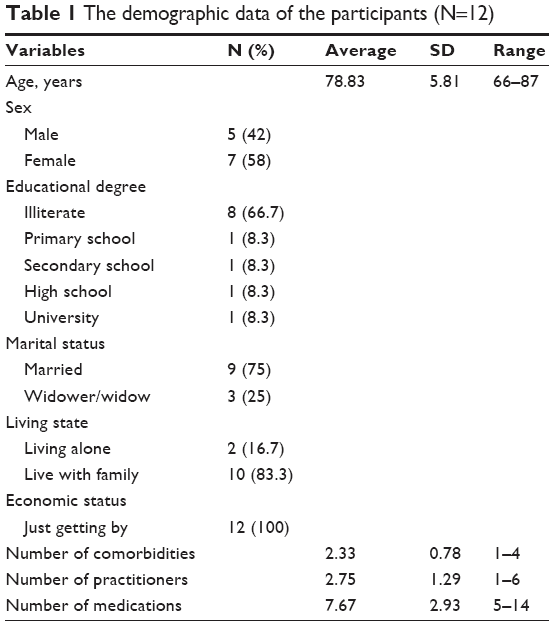 | Table 1 The demographic data of the participants (N=12) |
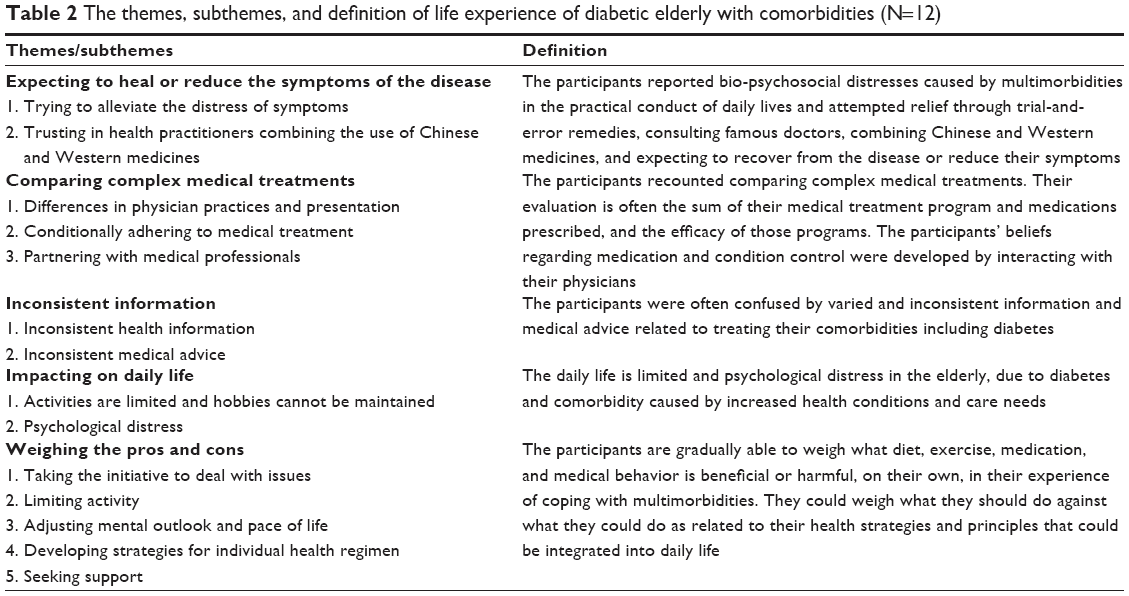 | Table 2 The themes, subthemes, and definition of life experience of diabetic elderly with comorbidities (N=12) |
Expecting to heal or reduce the symptoms of the disease
The participants reported bio-psychosocial distresses caused by multimorbidities in the practical conduct of their daily lives and indicated that they attempted to find relief through trial and error remedies, by consulting famous doctors, and by combining Chinese and Western medicines, with the expectation that they could recover from the diseases or at least reduce their symptoms.
Trying to alleviate the distress of symptoms
When the symptoms did not improve, they would continue to seek medical attention, trying different remedies (ie, trial and error) until the symptoms improved or stabilized.
Participant 11 has heart disease and hypertension and previously suffered from long-term pain (due to a pinched caudal nerve) affecting her physical and mental states, as well as her daily life.
“Oh! Steroids! If I take steroids my foot pain is relieved, but without them, my foot can be so painful. As the effect of the drug fades, the pain returns and cannot be relieved. Later I found the right doctor and underwent corrective surgery. It felt comfortable after surgery. Now I do not suffer such pain. I can eat and sleep, and have no worries!” [Participant 11]
Participant 7 has hypertension, cataracts, and hyperlipidemia and suffers from eye discomfort. She sought help from the eye clinic near her home. However, the surgical treatment was not completely effective. Therefore, she continues to seek help from many hospitals and a number of doctors.
“The clinic doctor said that my eye surgery was very successful, but I still cannot see clearly! So I went to other hospitals and to visit other doctors.…” [Participant 7]
Participant 6 is suffering from hypertension, degenerative arthritis, and Parkinson’s disease. She sought relief through complementary and alternative medicine (CAM) for her diabetes and degenerative arthritis.
“My knee was sore and painful. I had oil massages with stretching and pounding, and Qigong … I was flogging a dead horse … An advertisement claims that eating cereal can control blood sugar without the need for medicine, but my blood sugar soared (after having it).…” [Participant 6]
Trusting in health practitioners combining the use of Chinese and Western medicines
Some of the participants expressed trust in their physicians’ expertise and sought to retain that confidence, whether with regard to Western or Chinese medicine. As long as someone recommended a good doctor, they would try to visit him or her.
Participant 3 has mild heart disease, cataracts, and hypertension. In recent years, this patient has also been suffering from distress caused by the development of a trigger finger condition (stenosing tenosynovitis of the finger’s flexor tendon). After listening to a famous doctor’s speech, he sought outpatient treatment from that doctor.
“I went to listen to a doctor’s speech. I thought that this doctor is an expert. He will help me with my diabetes … and the pain and discomfort caused by my trigger finger. I keep looking for some effective treatment, whether it’s Chinese medicine, massage, or acupuncture.…” [Participant 3]
“I tried both Western and Chinese medicine. Whenever friends or relatives would recommend a prominent doctor, I would visit that doctor.” [Participant 11]
Comparing complex medical treatments
The participants recounted their own comparisons of complex medical treatments. Their evaluations often consisted of summarizing their medical treatment programs and the medications prescribed, as well as the efficacy of those programs. The participants’ beliefs regarding medication and condition control were generally developed by interacting with their physicians. It is generally accepted that the best treatment involves the least medication, but medical treatment recommendations should be adhered to in dealing with serious or complicated conditions. The participants indicated, however, that they would be more willing to adhere to their medical treatments if they could be in genuine partnerships with the medical professionals and felt genuinely cared for by them.
Differences in physician practices and presentation
One measure of comparison referred to by the participants was differences in physician practices and presentation. In this study, the elderly participants were mainly in long-term outpatient tracking programs. In the course of their treatments for multimorbidities, they would consider whether the medical professional treating them was prominent in the given field. The participants would evaluate whether the doctor truly cared for them, whether their personal well-being was a priority, whether their symptoms were being controlled, and the relevant drug efficacy, including the presence of adverse reactions. Using their own experiences with medical professionals, the participants would assess the appropriateness of the recommended treatments.
Participant 8 did not feel confident in the efficacy and individualized care received, and experienced adverse drug reactions:
“Doctors have made no progress in my blood pressure treatment, and have not adjusted my medication. They would only say, ‘Do not eat foods that are too salty, do not eat mushrooms, do not eat meat’ … after dinner medicine often causes diarrhea several times a day … after insulin injections I would have cold sweats!” [Participant 8]
Participant 3 had questioned the validity of the doctor’s treatment plan:
“I didn’t understand these drugs. The famous doctor prescribed more drugs than my original doctor did! I just took the medicines the doctor told me to take, but it resulted in itching so I stopped taking this drug … I used to be a farmer. I would not work if I did not eat rice. This doctor could only tell me to eat less rice!” [Participant 3]
Participant 6 even decided to change the physician:
“Every time he was poker-faced and silent. He didn’t speak a word!… Only instructed me to continue to take the medicine! Such a doctor … How can I communicate with him? I didn’t fully understand what he said! It’s a matter of my life! So I did replace the doctor.” [Participant 6]
Conditionally adhering to medical treatment
The interviewed participants understood the severity of their conditions and would, therefore, conditionally adhere to the medical treatment. They expected that their ailments could be controlled by drugs, but they worried that medications might harm their health or cause dependency.
“I would be worried about becoming drug dependent and harming my body … I did not want to take too much medicine. I could take it in a controlled way.” [Participant 10]
“I read books, newspapers, and magazines, on my own, to see which foods are better. Some diseases can be controlled by a good natural diet without reliance on medication. But I still take blood sugar and blood pressure medicine as prescribed.” [Participant 8]
Participant 3 thought that he only needed to comply with the prescribed treatment plan when he felt the need for his medication, although he still attended regular medical examinations. He thought that his heart disease was not serious, and so thought that it was his choice to self-regulate his medication.
“My heart is not well, but checkups show only one vessel is not smooth. The doctor prescribed medicine for me, but I did not take it for 10 or more years now. I’m good … but there are many complications of diabetes, so that I need to take medicine and regular checkups, as well.” [Participant 3
Partnering with medical professionals
The participants could form a partnership with medical professionals if they felt the medical professionals genuinely cared about them individually and personally.
“The doctors and nurses are very kind to me, like good friends. The doctors say how to take the medicine, how I should eat, and what to check. I am cooperating with them.…” [Participant 12]
Inconsistent information
In this study, the participants were often confused by varied and inconsistent information and medical advice related to treating their comorbidities including diabetes.
Inconsistent health information
Participant 8 was confused because of inconsistencies in information and recommendations:
I read a newspaper saying that blood sugar drugs should be taken at night, but this book says that it is better not to take them at night. The doctor said that it can be okay either way. It’s really ambiguous!” [Participant 8]
Inconsistent medical advice
Participant 3 went to a famous doctor’s outpatient clinic after listening to his speech, but different prescriptions from two doctors caused him frustration:
“About the drugs of the two doctors, who is correct? Who should I listen to? Whose medication did I need to take?” [Participant 3]
Participant 6 tried CAM for relief, but he returned to Western medicine treatment after the CAM failed to perform satisfactorily:
“There are a lot of folk-remedy treatments now! But we have to see a Western medicine doctor to have confidence in the treatment!” [Participant 6]
Impacting on daily life
The interviewed participants also expressed the view that their activities are limited and that their hobbies cannot be maintained due to health conditions and care needs dictated by their diabetes and comorbidities. They further indicated that psychological distress and symptoms of distress could be caused by having to rely on others.
Activities are limited and hobbies cannot be maintained
Participant 1 related that her outside activities were curtailed due to heart failure and degenerative arthritis:
“I like to go out to play, but recently I have not gone out to play!” [Participant 1]
Participant 9 deals with poor control of diabetes and replaced her former treatment plan with insulin injection so that her activities were restricted:
“I used to go on a pilgrimage, but I do not dare go now because of my insulin injections!” [Participant 9]
Psychological distress
Participant 7 has vision problems and cannot see clearly, so she had difficulty carrying out her many family responsibilities. In addition, she depended on others to do everything, and that made her feel psychological distress:
“I am a person with an independent personality, and now I have to depend on others for everything. I feel bad! I feel very bad!” [Participant 7]
“I could not sleep for a long time due to my foot pain! I could not go out! I just stayed at home, and I ate less and felt very depressed, sad.…” [Participant 11]
“My knee pain was very annoying and I was feeling very bad. I could not eat and sleep!” [Participant 6]
Participant 1, whose comorbidities restricted her activities:
“I feel very depressed!” (At this point, the participant started to cry.) [Participant 1]
Weighing the pros and cons
In their experiences of coping with multimorbidities, the participants expressed the feeling that they gradually became able to weigh on their own what diet, exercise, medication, and medical behaviors would be beneficial or harmful. They could weigh what they should do against what they could do as related to their health strategies and the principles that could be integrated into daily life. This process resulted from experiencing, thinking, comparing, and considering, as well as adjusting. And finally, they could surmount these challenges in order to live a normal life.
Taking the initiative to deal with issues
The participants would take the initiative to deal with the endless variety of conditions, or they could engage in self-management of their multimorbidities after weighing and comparing all the recognized symptoms.
“I would check my blood pressure and blood sugar. All the data would be recorded. These data are not bad.…” [Participant 8]
“There are many problems if my diabetes is not controlled well. Therefore, I would listen to a doctor’s advice.” [Participant 4]
“There would be a lot of complications of diabetes when I didn’t take my medication. I worried about my eye problems and would check my eyes every six months … My kidneys could fail, so I checked with the doctor on a regular basis, with blood tests.” [Participant 3]
“I have had low blood sugar, with dizziness and sweating, felt uncomfortable, fainting, vertigo … Now I realize I may have eaten too little in the morning. Therefore, I eat something as soon as possible when necessary.…” [Participant 9]
“I would quickly eat something after exercise because I could have low blood sugar … I would eat dry rice since eating porridge could make my blood sugar too high.” [Participant 8]
Limiting activity
The interviewed participants indicated that they would sometimes limit their behaviors according to their own multiple conditions, adjusting diet and activities as necessary.
“I am afraid of stroke. I eat very light because high blood pressure can occur without warning.…” [Participant 8]
“Sometimes I eat greedily, so I would only eat a little, bananas or apples. I would not dare to eat too much all at once, but over a period of time … my leg could cramp in pain, and feeling faint, I had to be careful. I could take a cane and umbrella to walk in the park, but I could not dare to go too far!” [Participant 9]
“I eat brown rice for three meals, and I do not eat sweet or high starch food.…” [Participant 3]
“I eat very light … I’m afraid I’ll fall when I go out, so I take a cane or stick.” [Participant 1]
“I eat less sweet food, and exercise more!” [Participant 4]
Adjusting mental outlook and pace of life
In this study, the participants reported that multiple conditions were more difficult to control when they deteriorated. When they experienced functional deterioration, they needed to consult with a professional. The participants also indicated that they could evaluate whether their condition was unstable or serious, and whether their mood was deteriorating. Relatedly, they could also initiate some self-adjustment strategies, such as adjustments of their daily activities and adjustments aimed at changing their mood.
Participant 1 has comorbidities that had gradually disabled her and led her to engage in self-care. In the past, she usually liked to go out with her husband and meet with friends, but she has lived alone after her husband’s death. Her children can only provide limited companionship because they live in different places. She has depression because of the decline in her social activities; however, she was still trying to build a relatively happy and acceptable life from her monotonous existence.
“There was no one I could rely on. I must rely on myself! Recently, my right foot got worse, so I just stayed at home … Then, I would tell myself not to think too much, but with my pain, my mood was to give up! I could watch TV to pass the time if I stayed at home, and sometimes I could talk with my old friends on the phone. I would take a cane to the park for a walk, and chat with other people if I could go out, and these helped my mood to improve. I would not be at home getting moody and angry!” [Participant 1]
Participants 4 and 5 are husband and wife:
“Our children do not have time for us! They can only visit occasionally, or bring healthy food for us to eat. We have to take good care of ourselves!” [Participants 4 and 5]
Developing strategies for individual health regimens
In order to maintain their well-being, the participants in this study also developed strategies for individual health regimens.
“I usually do exercise and massage, with acupuncture. I could think for myself, and I would plant some flowers and plants as well … People should not worry. Worrying too much makes us grow old early. People should be optimistic. The most important thing is to eat and sleep normally … to live a regular life. And now I feel life is smooth.…” [Participant 2]
Seeking support
In this study, the participants would seek support from a variety of resources, such as by speaking with relatives and friends or seeking religious solace. They would often pray and study the Bible, participate in church activities or temple worship, or engage in mission-related activities. They did all this in order to keep the body, mind, and spirit calm.
“If I am in a bad mood, I read the Bible and pray, or participate in church activities.…” [Participant 8]
“I always depend on prayer and reading the Bible, and my church sisters often come to see me at my home, and I ask them to pray for me!” [Participant 11]
“Usually I would go to the nearby temple to worship. And so my son felt free to take me on the pilgrimage … In short, I just want to go out. It would not feel good staying at home, depressed, in a bad mood!” [Participant 9]
Support from a spouse is also one of the factors that helped to sustain some of the participants living with comorbidities.
“We like to sing karaoke. We walk to the riverbank park, and remind each other to take our medicine.” [Participants 4 and 5]
“Visit a doctor, travel … we all come on our own … On Saturday and Sunday, my husband and I go hiking in the mountains behind our house.” [Participant 8]
Discussion
Diabetes is a complex chronic disease that affects multiple organ systems. The disease thus has long-term and extensive effects on the individual, family, and society. This study found that the living experiences of elderly people with comorbidities including diabetes can be summarized as “Surmounting these challenges in order to live a normal life.” These experiences can be further categorized into 5 themes. Elderly people living with comorbidities including diabetes do not only receive medical advice passively and follow that advice obediently. Rather, they also engage in trial and error regarding various behaviors, taking the initiative with respect to self-management, accepting restrictions on their lifestyles, and pursuing good outcomes while striving to avoid disaster, with multiple coping strategies. The goal of all these efforts is to build a new balance to achieve a relatively normal daily life. This is similar to what was previously reported by Martin, whose study suggested that patients would seek to establish new stability for multimorbidities.42 In this study, the elderly participants reported being able to continue, with a positive and optimistic attitude, to take the initiative in facing and dealing with their multiple conditions by incorporating the aforementioned strategies into their daily lives. These findings are similar to those of previous studies. To summarize, previous reports have indicated that although the elderly suffer from their diseases, they still, generally speaking, have a positive and resilient outlook on life.12,15,43 This conclusion is worthy of the attention of, and utilization by, medical professionals.
Compared with the life experiences of diabetes-only patients, those of the elderly patients facing multimorbidities who participated in this study were similar on many levels, although they tended to vary in degree. The elderly participants in this study also reported suffering from psychological distress and being suffused with anxiety and depression. In addition to their fear of the consequences of diabetes, such as high and low blood sugar problems and other complications, they also worried about limitations caused by their comorbidities. Most participants believed that multiple chronic conditions are quiet and silent and complained about the difficulty of managing them. However, they wanted to maintain their independence and quality of life. Also, they exhibited an optimistic outlook on life, expressed their need for access to information and resources, and expressed their need for support from family and peers. These findings are similar to those of diabetes-only studies.13–16 The elderly would have some emotional reactions, but in addition to their diabetes, they also reported being concerned about comorbidities and other problems. These results were also similar to those of previous studies.15,33–35 The distress from a variety of symptoms resulted in patients with negative emotional reactions, such as sadness due to the loss of control and due to the deterioration of their comorbid conditions. Some of the participants did not think that diabetes was a serious problem compared with the burdens and troubles that the other symptoms brought to their life. This was the biggest difference between the findings of this study and those of diabetes-only studies. This study showed that, compared with diabetes as a single disease, comorbidities make the circumstances of diabetic elderly people more complicated, such that they need more medical care and greater daily support. This is consistent with the argument posed by the findings of some previous studies. Comorbidities lead to the need for more complex medical treatments for diabetes. Elderly patients experience more burdens, receive more complex prescriptions, and are more affected by severe comorbidities, all of which may increase their burdens in self-managing their diseases.5–7 In addition to their psychological reactions, the elderly participants in this study showed more proactive self-management processes. Accordingly, the researchers were not surprised by the results of this study of elderly patients with comorbidities including diabetes. This may have been because these participants have suffered from diabetes and multiple other diseases for many years. They have been in a long-term adaptation for these diseases. Therefore, the initial impact of disease diagnosis on the elderly has been reduced.
This study found that the elderly participants discovered a variety of resources from which to receive support in dealing with their multiple diseases. Most of them reported frequently seeking comfort from family and friends, and relying on religion for inspiration. Previous studies have found that older people with diabetes rely on spiritual and/or religious resources to effectively address the difficult times because of the disease, to give them courage to accept these challenges, and to support their efforts toward self-management and healing.18 The support and encouragement from family and friends and the diversity and capacity of network relationships are very important for self-management by the elderly.19,25 Beverly and Wray found that spousal support could help patients to maintain and adhere to exercise programs that improve the quality of their life experiences22 and also found that patient motivations and responsibilities could be enhanced by strengthening spousal interdependence and the perceived support from one another, findings which are similar to the findings of this study. However, the elderly in this study often complained that their children are too busy to provide much attention so that they had to be self-reliant or that they were inconvenienced by the need to wait for their children to be available to help with their care needs. In this regard, it is worth noting that the Western concept of family differs from the Asian concept of family, which emphasizes “raising children for old age.” In the East, old people rely on filial piety. As such, when children cannot provide for the needs of their parents, the parents may experience feelings of helplessness. Therefore, medical professionals should establish a partnership with the elderly. It is recommended that formal social support, such as that provided by home nurses or social workers, could be introduced in due course to gain insight into the unique needs of the elderly, with the supportive and educational roles played by health care workers helping the elderly to strengthen their self-management abilities and assisting them in seeking and making good use of their social support networks. In short, health care professionals should provide the elderly with resources and information tailored to their self-management efforts, in addition to taking action to directly meet their care needs.
This study found that, in addition to diabetes, there are other conditions and symptoms caused by comorbidities that prompt participants to seek comparative medical advice. Therefore, the overall experiences of such participants in seeking medical treatment are diverse. While the free choice of varied medical treatments is unrestricted by the National Health Insurance system of Taiwan, there is no formal family doctor system or referral system. Relatedly, the use of CAM by diabetic patients has become a means by which these patients seek to control the condition and improve their well-being.36 The participants in this study, while generally adhering to treatment protocols, were not completely confident in their adherence due to the complexity of the prescriptions. They expected the prescribed drugs to control the disease, but also feared that the drugs would cause harm to their health, so they would sometimes adjust or interrupt their use of the drugs. Shen et al pointed out that elderly Asian diabetes patients generally distrust Western medicine, but they still rely on it.39 Relatedly, while it can quickly and effectively control blood sugar, the elderly are very reluctant to take Western medicine. They would rather take traditional Chinese medicine and healthy food, because they think that Western medicine is harmful to the body. Williams and Manias found that the motivation and confidence of patients with respect to taking prescription drugs was hampered by complex medical prescriptions and multiple illnesses31 and could even be overwhelmed by the burden of polypharmacy. In addition, such issues among Chinese patients may be associated with the Chinese preference for compound medicines. Although the elderly in this study are in long-term follow-up programs as hospital outpatients, the vast majority still reported seeking Chinese medicine and CAM treatments even while taking Western medicine. The results of this study are similar to those of the study by Nguyen, which found that Vietnamese patients with diabetes could combine Eastern and Western medical beliefs.37 Consequently, health care professionals should provide symptom management for multiple conditions of the patient, not just for diabetes. In addition, many medical institutions could consider establishing both Chinese and Western medicine departments. Relatedly, medical professionals, in addition to teaching patients about symptom management, need to understand CAM in order to facilitate active inquiry at different times, or to discuss the need for CAM with patients in order to achieve improved communication.
According to a previous study, physician–patient relationship is important to patients, “traditional” consultation styles inhibit shared decision-making, and participatory consultation styles facilitate patient control in self-management.14 This study found similar results. The elderly value effective physician–patient relationship, and they expect that medical professionals can provide them with treatment options, interpret risks and benefits, listen to them, and spend the time necessary to understand their values and preferences. The health care professionals can take care of them as a priority and make decisions together with them in order to ensure that their medical care is aligned with their rights, needs, and wishes. However, health care providers may not always discuss values and preferences with their patients,27,28,30 and vertical communication or a lack of communication between a physician and a patient is a barrier to self-management of diseases. As such, establishing trust, nonjudgmental acceptance, and open/honest communication when forming a physician–patient partnership would help the patients in their self-management efforts.30,32,39
Like some previous studies,22,27 we also found that the elderly in this study were eager to be cared for by medical professionals in good faith, expressing the desire that these professionals would provide them with practical and individualized advice and information rather than simply treating them based on test data. Relatedly, the findings of some previous studies have indicated that poor physician–patient communication could lead the patients to follow only the doctors’ advice on a conditional basis.10,12,14 Meanwhile, two-thirds of the elderly people in this study were illiterate, such that they may not know how to discuss treatment options with their physicians. As a result, some elderly people might have doubts about the given physicians’ medical disposition, resulting in conditional compliance and a missed opportunity for two-way communication.
At the same time, this study found that elderly patients tend to select what they consider right and suitable from their many sources of information. Patients often complain about inconsistent information or a lack of information.10,32,39 Their information needs are often not met, so they need concise care instructions and additional informal information.13,44 It is therefore recommended that medical professionals should establish a medical partnership with the elderly. They need to understand the educational level of the patients and observe their unique needs. When providing information, they should not only provide written information, but should also repeat their explanations or provide other audio and video materials, giving the patients the opportunity to express their thoughts about the quality of the system and their preferences regarding medical advice and information.
This study had the following limitations: 1) It was conducted exclusively in Taipei, Taiwan, at an outpatient clinic within a single medical center, with the diabetic elderly participants with comorbidities recruited solely from this single clinic. The results may thus not be generalizable to various other diseases of the elderly in Taiwan. Also, the participants were all elderly and married, even if currently widowed, so the results cannot be inferred as generalizing to the unmarried elderly. 2) The participants were interviewed only once, so we could not follow changes through different stages of their diseases and the impact of diabetes with comorbidities on their health. 3) The elderly participants in this study were seen for regular follow-ups in the outpatient clinic and their conditions were stable. Therefore, this study cannot be seen as portraying the living experiences of diabetes patients with comorbidities whose conditions are not stable, who do not go to a hospital for treatment, who are hospitalized, or who do not take Western medicines as part of their treatment. 4) Lastly, although some Asian countries have similar cultures, there are some differences between them and Taiwan. Therefore, if the results of this study are to be applied to other countries in Asia, the cultural differences between Taiwan and these countries must be carefully considered.
It is suggested that related future studies should seek to answer the following question and fulfill the following objectives: 1) What are the factors that impact the experiences of elderly patients with multimorbidities? 2) To understand the severity of different conditions and the effects of different means of treatment, such as folk medicine, Chinese medicine, and so on, on the living experiences of elderly patients. 3) To understand the changes and factors relating to different time points or stages of life experience of elderly patients. 4) To design interventions such as setting up evidence-based nursing guidance to provide a good and accurate source of information and assisting the elderly in continually adapting to living with multiple diseases.
Conclusion
In this study, we found that diabetic elderly with comorbidities were trying to surmount a lot of challenges in order to live a normal life. Their life experience could be divided into 5 themes and 14 subthemes. The overall life experience was similar to a single disease, but the extent was greater than a single disease. Compared with a single disease, the biggest difference in the impact of multimorbidities is that the elderly think that their most serious problem is not diabetes, but rather, the comorbidities causing life limitations. Therefore, compared to the elderly who suffer from just diabetes, medical professionals will manage those with comorbidities by not only monitoring their physiological data but also paying attention to the impact of comorbidities in their lives. Comorbidities lead to the need for more complex medical treatments for older patients with diabetes. These older patients have to deal with more burdens, more complex prescriptions, and a greater risk of being affected by severe comorbidities, all of which may increase their burdens with respect to the self-management of their multimorbidities. However, they were more proactive in carrying out the self-management processes. Social support could effectively address the difficult problems caused by multimorbidities by giving older patients the courage to accept these challenges. Their overall experiences in seeking medical treatment are diverse. The establishment of a physician–patient relationship would help them in their self-management efforts. Although these older patients practice a high degree of medication adherence, they still harbor mixed feelings about the prescription. Many inconsistencies in terms of information have confused them. Most participants were illiterate, such that they may not know how to discuss treatment options with their physicians. Medical professionals need to observe their individual needs. When providing information, medical professionals should give their patients the opportunity to express their thoughts about the quality of the system and their preferences regarding medical advice and information. This study was undertaken to help medical professionals achieve an in-depth understanding of the life experience of the diabetes afflicted elderly living with comorbidities and as a reference for future design of intervention measures.
Acknowledgments
We would like to thank all the participants in this study for providing valuable experience and information. The Taiwan Nurses Association provided financial support for this research project (TWNA-1012059).
Disclosure
The authors report no conflicts of interest in this work.
References
Iglay K, Hannachi H, Howie PJ, et al. Prevalence and co-prevalence of comorbidities among patients with type 2 diabetes mellitus. Curr Med Res Opin. 2016;32(7):1243–1252. | ||
Egede LE, Gebregziabher M, Yumin Z, et al. Differential impact of mental health multimorbidity on healthcare costs in diabetes. Am J Manag Care. 2015;21(8):535–544. | ||
Garin N, Koyanagi A, Chatterji S, et al. Global multimorbidity patterns: a cross-sectional, population-based, multi-country study. J Gerontol A Biol Sci Med Sci. 2016;71(2):205–214. | ||
Lynch CP, Gebregziabher M, Zhao Y, Hunt KJ, Egede LE. Impact of medical and psychiatric multi-morbidity on mortality in diabetes: emerging evidence. BMC Endocr Disord. 2014;14(68):1–8. | ||
Malik S, Billimek J, Greenfield S, Sorkin DH, Ngo-Metzger Q, Kaplan SH. Patient complexity and risk factor control among multimorbid patients with type 2 diabetes: results from the R2D2C2 Study. Med Care. 2013;51(2):180–185. | ||
Nugent LE, Carson M, Zammitt NN, Smith GD, Wallston KA. Health value & perceived control over health: behavioural constructs to support type 2 diabetes self-management in clinical practice. J Clin Nurs. 2015;24(15/16):2201–2210. | ||
Teljeur C, Smith SM, Paul G, Kelly A, O’Dowd T. Multimorbidity in a cohort of patients with type 2 diabetes. Eur J Gen Pract. 2013;19(1):17–22. | ||
Fix GM, Cohn ES, Solomon JL, et al. The role of comorbidities in patients’ hypertension self-management. Chronic Illn. 2014;10(2):81–92. | ||
Fraccaro P, Casteleiro MA, Ainsworth J, Buchan I. Adoption of clinical decision support in multimorbidity: a systematic review. JMIR Med Inform. 2015;3(1):e4p.1–e4p.18. | ||
McKinlay E, Graham S, Horrill P. Culturally and linguistically diverse patients’ views of multimorbidity and general practice care. J Prim Health Care. 2015;7(3):228–235. | ||
Hughes LD, McMurdo MET, Guthrie B. Guidelines for people not for diseases: the challenges of applying UK clinical guidelines to people with multimorbidity. Age Ageing. 2013;42(1):62–69. | ||
Zhang H, Shan W, Jiang A. The meaning of life and health experience for the Chinese elderly with chronic illness: a qualitative study from positive health philosophy. Int J Nurs Pract. 2014;20(5):530–539. | ||
Carolan M, Holman J, Ferrari M. Experiences of diabetes self-management: a focus group study among Australians with type 2 diabetes. J Clin Nurs. 2015;24(7/8):1011–1023. | ||
Rose VK, Harris MF. Experiences of self-management support from GPs among Australian ethnically diverse diabetes patients: qualitative study. Psychol Health Med. 2015;20(1):114–120. | ||
Stuckey HL, Mullan-Jensen CB, Reach G, et al. Personal accounts of the negative and adaptive psychosocial experiences of people with diabetes in the second diabetes attitudes, wishes and needs (DAWN2) study. Diabetes Care. 2014;37(9):2466–2474. | ||
Newton P, Asimakopoulou K, Scambler S. A qualitative exploration of motivation to self-manage and styles of self-management amongst people living with type 2 diabetes. J Diabetes Res. 2015;2015:1–9. | ||
Laranjo L, Neves AL, Costa A, Ribeiro RT, Couto L, Sá AB. Facilitators, barriers and expectations in the self-management of type 2 diabetes – a qualitative study from Portugal. Eur J Gen Pract. 2015;21(2):103–110. | ||
Casarez RL, Engebretson JC, Ostwald SK. Spiritual practices in self-management of diabetes in African Americans. Holist Nurs Pract. 2010;24(4):227–237. | ||
Kennedy A, Rogers A, Vassilev I, et al. Dynamics and nature of support in the personal networks of people with type 2 diabetes living in Europe: qualitative analysis of network properties. Health Expect. 2015;18(6):3172–3185. | ||
Low LL, Tong SF, Low WY. Social influences of help-seeking behaviour among patients with type 2 diabetes mellitus in Malaysia. Asia Pac J Public Health. 2016;28(1 Suppl):17S–25S. | ||
Newton P, Asimakopoulou K, Scambler S. Information seeking and use amongst people living with type 2 diabetes: an information continuum. Int J Health Promot Educ. 2012;50(2):92–99. | ||
Beverly EA, Wray LA. The role of collective efficacy in exercise adherence: a qualitative study of spousal support and type 2 diabetes management. Health Educ Res. 2010;25(2):211–223. | ||
Jones L, Crabb S, Turnbull D, Oxlad M. Barriers and facilitators to effective type 2 diabetes management in a rural context: a qualitative study with diabetic patients and health professionals. J Health Psychol. 2014;19(3):441–453. | ||
Murrock CJ, Taylor E, Marino D. Dietary challenges of managing type 2 diabetes in African-American women. Women Health. 2013;53(2):173–184. | ||
Oftedal B. Perceived support from family and friends among adults with type 2 diabetes. Eur Diabetes Nurs. 2014;11(2):43–48. | ||
Joo JY, Lee H. Barriers to and facilitators of diabetes self-management with elderly Korean-American immigrants. Int Nurs Rev. 2016;63(2):277–284. | ||
Oftedal B, Karlsen B, Bru E. Perceived support from healthcare practitioners among adults with type 2 diabetes. J Adv Nurs. 2010;66(7):1500–1509. | ||
Beverly EA, Wray LA, LaCoe CL. Listening to older adults’ values and preferences for type 2 diabetes care: a qualitative study. Diabetes Spectr. 2014;27(1):44–49. | ||
Kruse RL, Olsberg JE, Shigaki CL, et al. Communication during patient-provider encounters regarding diabetes self-management. Fam Med. 2013;45(7):475–483. | ||
Ritholz MD, Beverly EA, Brooks KM, Abrahamson MJ, Weinger K. Barriers and facilitators to self-care communication during medical appointments in the United States for adults with type 2 diabetes. Chronic Illn. 2014;10(4):303–313. | ||
Williams A, Manias E. Exploring motivation and confidence in taking prescribed medicines in coexisting diseases: a qualitative study. J Clin Nurs. 2014;23(3–4):471–481. | ||
Fort MP, Alvarado-Molina N, Peña L, Montano CM, Murrillo S, Martínez H. Barriers and facilitating factors for disease self-management: a qualitative analysis of perceptions of patients receiving care for type 2 diabetes and/or hypertension in San José, Costa Rica and Tuxtla Gutiérrez, Mexico. BMC Fam Pract. 2013;14:131. | ||
Shirazian S, Park J, Mattana J, et al. The self-management experience of patients with type 2 diabetes and chronic kidney disease: a qualitative study. Chronic Illn. 2016;12(1):18–28. | ||
Ågård A, Ranjbar V, Strang S. Diabetes in the shadow of daily life: factors that make diabetes a marginal problem. Prac Diabetes. 2016;33(2):49–53. | ||
Beverly EA, Wray LA, Chiu CJ, Weinger K. Perceived challenges and priorities in co-morbidity management of older patients with type 2 diabetes. Diabet Med. 2011;28(7):781–784. | ||
Chang HY, Wallis M, Tiralongo E, Wang HL. Decision-making related to complementary and alternative medicine use by people with type 2 diabetes: a qualitative study. J Clin Nurs. 2012;21(21–22):3205–3215. | ||
Nguyen AT. Self-management of type 2 diabetes: perspectives of Vietnamese Americans. J Transcult Nurs. 2014;25(4):357–363. | ||
Hunt LM, Kreiner M, Brody H. The changing face of chronic illness management in primary care: a qualitative study of underlying influences and unintended outcomes. Ann Fam Med. 2012;10(5):452–460. | ||
Shen H, Edwards H, Courtney M, McDowell J, Wei J. Barriers and facilitators to diabetes self-management: perspectives of older community dwellers and health professionals in China. Int J Nurs Pract. 2013;19(6):627–635. | ||
Colaizzi PF. Psychological research as the phenomenologist views it. In: Valle RS, King M. editors. Existential-Phenomenological Alternatives for Psychology. New York: Oxford University; 1978:48–71. | ||
Lincoln YS, Guba EG. Naturalistic Inquiry. Newbury Park, CA: Sage; 1985. | ||
Martin CM. What matters in “multimorbidity”? Arguably resilience and personal health experience are central to quality of life and optimizing survival. J Eval Clin Pract. Epub Sep 21, 2016 | ||
Ho HY, Lee YL, Hu WY. Elder resilience: a concept analysis. J Nurs. 2012;59(2):88–92. | ||
Frost J, Garside R, Cooper C, Britten N. A qualitative synthesis of diabetes self-management strategies for long term medical outcomes and quality of life in the UK. BMC Health Serv Res. 2014;14:348. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.