")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Exploring Factors Contributing to Chronic Obstructive Pulmonary Disease (COPD) Guideline Non-Adherence and Potential Solutions in the Emergency Department: Interdisciplinary Staff Perspective
Authors Issac H , Taylor M , Moloney C, Lea J
Received 12 December 2020
Accepted for publication 4 February 2021
Published 6 April 2021 Volume 2021:14 Pages 767—785
DOI https://doi.org/10.2147/JMDH.S276702
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Hancy Issac, Melissa Taylor, Clint Moloney, Jackie Lea
School of Nursing and Midwifery, University of Southern Queensland, Toowoomba, Australia
Correspondence: Hancy Issac Email [email protected]
Purpose: Acute exacerbations of chronic obstructive pulmonary disease (COPD) have a significant and prolonged impact on health-related quality of life, patient outcomes, and escalation of pulmonary function decline. COPD-X guidelines published in 2003 subsist to facilitate a shift from the emphasis on pharmacological treatment to a more holistic multi-disciplinary interventions approach. Despite the existing comprehensive recommendations, readmission rates have increased in the last decade. Evidence to date has reported sub-optimal COPD guidelines adherence in emergency departments. This qualitative study explored contributing factors to interdisciplinary staff non-adherence and utilisation of COPD-X guidelines in a major Southern Queensland Emergency Department.
Methods: Semi-structured qualitative interviews with interdisciplinary staff were conducted in an emergency department. A purposive sample of doctors, nurses, physiotherapists, pharmacist and a social worker were recruited. Interviews were digitally recorded, de-identified and transcribed verbatim. Data analysis followed a coding process against the Theoretical Domains Framework (TDF) to examine implementation barriers and potential solutions. Identified factors affecting non-adherence and underutilisation of guidelines were then mapped to the capability, opportunity, motivation, behaviour model (COM-B) and behaviour change wheel (BCW) to inform future implementation recommendations.
Results: Prominent barriers influencing the clinical uptake of COPD guidelines were identified using TDF analysis and included knowledge, professional role clarity, clinical behaviour regulation, memory, attention, and decision process, beliefs about departmental capabilities, environmental context and resources. Potential interventions included education, training, staffing, funding and time-efficient digitalised referrals and systems management reminders to prevent COPD readmissions, remissions and improve patient health-related quality of life.
Conclusion: Implementation strategies such as electronic interdisciplinary COPD proforma that facilitates a multimodal approach with appropriate patient/staff resources and referrals prior to discharge from an ED require further exploration. Greater clarity around which components of the COPD X guidelines must be applied in ED settings needs to stem from future research.
Keywords: AECOPD management, COPD guidelines adherence, theoretical domains framework, multidisciplinary, COM-B, behaviour change wheel, behaviour change techniques taxonomy
Introduction
COPD guideline non-adherence in clinical practice is a significant problem well recognised and reported in national and international literature.1–3 Chronic obstructive pulmonary disease (COPD) kills more than 3 million people worldwide every year and affects around 174 million people globally.4 The World Health Organization predicts COPD to become the third leading cause of death by 2030 considering its increase in prevalence and morbidity. Complex chronic disease management processes need to be examined further to meet unmet patient and carer needs in the community with a focus on health-related quality of life. Non-pharmacological programmes inclusive of pulmonary rehabilitation, smoking cessation programmes, increasing physical activity, and early detection and treatment of comorbidities are reiterated as key components to reduce the burden of the disease.4,5 Current holistic national guidelines originally published in 2003 in Australia known as COPD-X Plan are not adhered to consistently by doctors, nurses and interdisciplinary health professionals.3 Pharmacological interventions are well explored and reported compared to non-pharmacological interventions in relation to adherence rates.3 National guidelines (COPD-X plan) and international guidelines (Global initiative for chronic obstructive lung disease [GOLD]) have consistently pointed towards the importance of non-pharmacological interventions to assist patients with self-management and community management to prevent readmissions and acute exacerbations.5,6 In 2008, estimated costs for COPD care in Australia were AUD $8.8 billion in primary and tertiary hospitals, with AUD $89 billion spent on COPD-related disability and premature death.7,8 The Australian National Morbidity Database reveals that in 2017–2018, there were 77,660 hospitalisations of people above 45 and over, and the rate of hospitalisation was 732 per 100,000 population.8,9
A significant variation in clinical practice was reported through a cohort study conducted in 46 EDs in Australia, New Zealand, Singapore, Hong Kong and Malaysia that aimed to explore epidemiology, clinical features, treatment outcomes, hospital length of stay and in-hospital mortality.10 The findings revealed that most acute exacerbations of chronic obstructive pulmonary disease (AECOPD) patients arriving in EDs by ambulance had increased hospitalisation and significant in-hospital mortality.10 A planned sub-study of Australia, Asia, New Zealand dyspnoea in emergency departments (AANZDEM) concluded compliance with COPD evidence-based guidelines is suboptimal in EDs and suggested further research to improve compliance with guidelines and consideration for implementation strategies.3 Economic research data in three Southern Queensland Hospitals reveal a total health service cost of AUD $ 42, 142, 474 for COPD ED presentations across all 3 sites where 41.1% of presentations were assessed as emergency triage category 3 or 4 in the EDs and were transferred home on the same day.11,12 The Australian triage scale outlines five categories from Category-1, an immediately life-threatening condition involving prompt assessment and treatment to Category-5, a chronic or minor condition to be assessed and treated within 2 hours.13 The estimated cost savings of reduced COPD-related admission is around AUD $533 per patient in these ED’s. These economic research data further report that 50% of COPD presentations were discharged within 4 hours without a targeted referral. Implications of this practice often lead to repetitive readmissions of COPD exacerbations, increased economic burden, and poor optimisation of patient lung function and overall health.11,12,14,15
Sub-optimal dissemination and implementation of guidelines can significantly impede adoption into daily practice.16 Local, national, and international respiratory societies are seeking better implementation strategies for the uptake of COPD guidelines,5 particularly since pharmacological interventions and invasive ventilation support practices have drifted from evidence-based guidelines.3,17,18 A Canadian retrospective study of COPD readmissions discharged from ED reported a significantly higher risk of readmission due to variability in treatment.19,20 The findings indicate less than 50% of COPD patients presenting to the ED received recommended COPD therapy.19 A COCHRANE systematic review on integrated disease management programs reported improved disease-related quality of life, increased exercise capacity, reduced hospital admissions and hospital days per person.20 Future implementation research should consider barriers and facilitators to inform change management and compliance indicators among hospital stakeholders.
COPD-X plan entails advances in the management of COPD that are updated quarterly in the national COPD guidelines (COPD-X plan) by Lung Foundation Australia in conjunction with the Thoracic Society of Australia and New Zealand.5 This guideline comprises evidence-based recommendations to interdisciplinary health care professionals to assist with case identification and diagnosis, optimise patient function, prevent deterioration, develop support network and self-management plan to avoid future exacerbations.5 COPD guideline non-adherence is a well-studied and reported phenomenon albeit no studies have to date explored barriers and potential solutions from an interdisciplinary staff perspective. This study aimed to investigate the barriers and enablers that influence the uptake of COPD-X plan guidelines amongst interdisciplinary staff in the emergency department. The premise of the study was to determine elements of the COPD guidelines that are adhered to by interdisciplinary health professionals and explore potential solutions to mitigate guideline non-adherence.
The Theoretical Domains Framework (TDF) has been utilised in this research as an overarching framework that integrates a range of behaviour change theories. In similar research designs, it has been used to examine barriers and uptake of evidence in a variety of clinical settings.21 The framework includes 14 domains: 1) knowledge, 2) skills, 3) beliefs about capabilities, 4) memory, attention, and decision processes, 5) behavioural regulation, 6) environmental context and resources, 7) social influences, 8) intentions, 9) social/professional role and identity, 10) beliefs about consequences, 11), reinforcement, 12) emotion, 13) optimism, and 14) goals.21 Capability, opportunity, motivation and behaviour model (COM-B) recognises behaviour as part of an interacting interconnected system where planned interventions need to address one or all of them to achieve optimum implementation.22 Behaviour change wheel (BCW) originally developed from a systematic review analysing 19 frameworks of behaviour change methods consists of three layers.22 Central hub incorporates sources of behaviour to assist with the diagnosis of implementation barriers (capability [physical, psychological], opportunity [physical, reflective], motivation [psychological, automatic]), whereas the middle layer comprehends choices of nine intervention functions compatible to COM-B diagnosis of barriers (Education, Persuasion, incentivisation, coercion, training, enablement, modelling, environmental restructuring and restrictions).22 The outer layer of the wheel identifies seven policy categories to support the implementation of the chosen interventions (Guidelines, Environmental/social planning, Communication/Marketing, Legislation, Service provision, Regulation, Fiscal measures).22 This approach provides a means to prioritise implementation strategies and target determinants of individual, professional or organisational behaviour and practice.
Methods
A qualitative interpretive study design employing semi-structured individual interviews with questions stemming from a preliminary literature review was used to explore enablers and barriers that influence COPD management in interdisciplinary teams in the ED. In addition, reflexive thematic analysis was applied with the TDF and COM-B model to assist in the development of potential intervention strategies to improve COPD guideline adherence.
Setting, Sample, and Recruitment
Eight participants (2 doctors, 2 nurses, 2 physiotherapists, 1 pharmacist, and 1 social worker) were recruited from a metropolitan, tertiary hospital in Queensland, Australia. The participants were derived from a convenience sample of interdisciplinary staff (doctors, nurses, allied health) that were invited to participate via email. The research was advertised via flyers placed in the local ED. Written and signed informed consent was sought from individuals participating in the research. Ethics approval was obtained, prior to commencement, from the Hospital Human Research Ethics Committee (HREC EC00168/55098), and administrative approval was gained from the University Human Research Ethics Committee (H19REA308).
Data Collection
Individual semi-structured interviews of 20–50 minutes duration were conducted in the ED in a quiet room to ensure privacy. Questions included participant’s experience, perceptions and solutions to current perceived barriers towards COPD-X guidelines non-adherence in the ED (see Table 1). Data saturation was assessed once no new information emerged at which point data collection ceased. Digitally recorded interviews were later de-identified and transcribed verbatim. Demographic data, including position, gender and, years of experience, were collected as part of the interview process.
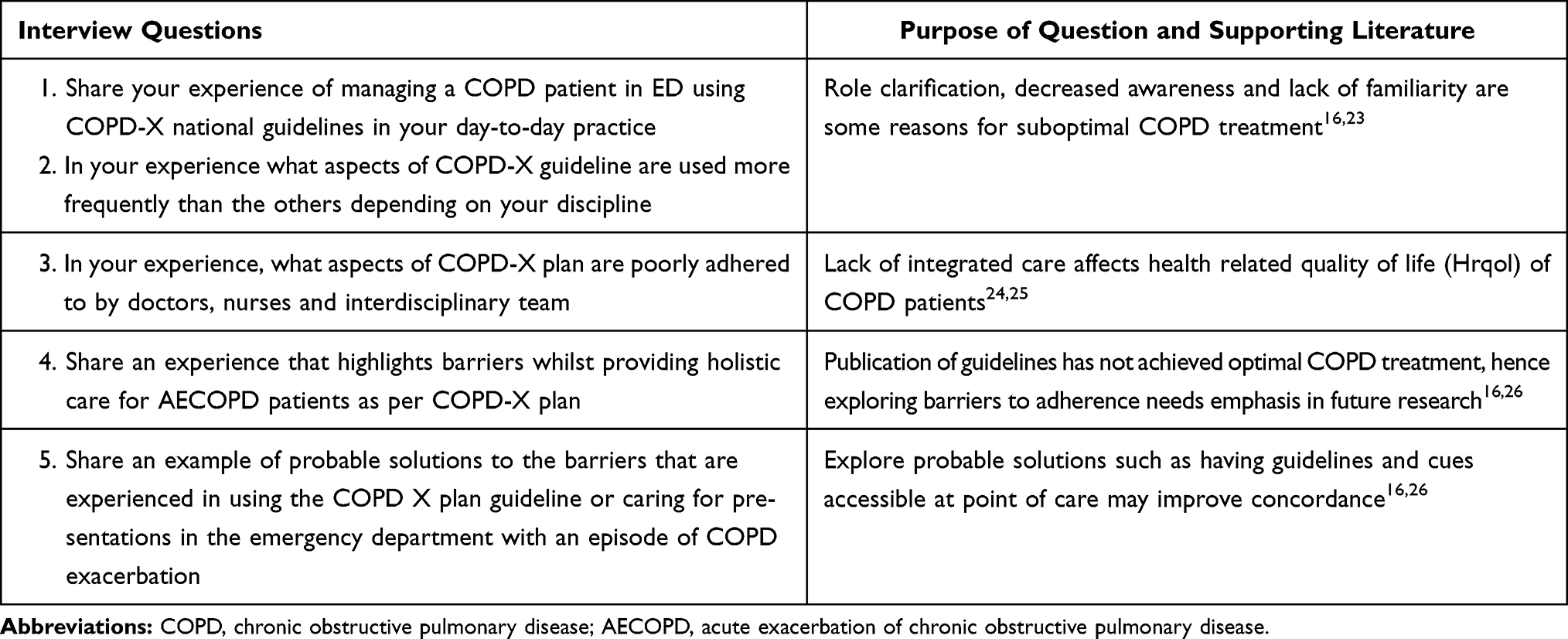 |
Table 1 Interview Questions Designed to Create Discussion and Share Experiences |
Data Analysis
The TDF, as part of the Behaviour Change Wheel (BCW), has previously guided a process for developing interventions and policy that specifically target deficits in three identified essential behaviour change conditions: capability, opportunity, and motivation (referred to as the COM-B system).21 Researchers have utilised the BCW to develop potential interventions to improve the utilisation and implementation of health guidelines. This taxonomy has been proven and applied to inform the development of interventions and policies to improve the delivery of healthcare in a variety of clinical settings including stroke and perioperative clinical guidelines adherence.27–29 The TDF and COM-B model assisted this research team in providing a systematic approach to data analysis that enabled the team to prioritise and develop implementation strategies that specifically target clinician-identified deficits and address barriers and enablers that influence the uptake of the clinical guidelines.
Six steps of reflexive thematic analysis as outlined by Braun & Clark (2006) were mapped against 14 domains of the Theoretical Domains Framework (TDF). Phase 1 included familiarisation of data and Phase 2 had two independent members of team review the data. The final stage of Phase 2 included the identification of initial codes. Phase 3, 4, 5 of thematic analysis was utilized to generate belief statements across the domains analysed, categorised and the textual data were assigned into the 14 TDF domains (see Figure 1). The coding strategy was reviewed and the consensus was established in the research team before applying the same principles to the remaining data. Disagreements between reviewers were resolved through discussion in the research team. Identified domains affecting clinical behaviour and non-adherence to guidelines were mapped to the capability (C), opportunity (O), and motivation (M) components, which form the behaviour change wheel. Sub-components of COM-B were merged with individual BCT techniques and participant implementation suggestions for their department to achieve better adherence.
 |
Figure 1 Data analysis graphic representation. Notes: Research design stages utilising reflexive thematic analysis (data from Braune & Clarke37) merged with theoretical domains framework (TDF) and Capability, Opportunity, Motivation- behaviour change wheel (COM-B, BCW) (data from Michie et al38). |
Results
Results are depicted in tables under each domain with participant quotes linking the 14 TDF domains to identified barriers in the use of the COPD X guideline. All illustrative quotes were matched with COM-B behaviour change wheel components and participants' implementation suggestions for better uptake of guidelines. Frequency scores were given to each domain to understand the prominence of the barriers and frequency of beliefs among participants.21,30 The reflexive thematic analysis identified seven theoretical domains as most relevant (frequency score 4 and above) to the clinical uptake for COPD X guidelines in the emergency department. Improving adherence to the guidelines was highly dependent on the identified domains and recommended interventions and implementation strategies from participants. Each of the most relevant domains identified is represented in the analysis. Eight domains emerged with the most prominent themes including knowledge, skills, beliefs about capabilities, memory/attention/decision process, behaviour regulation, environmental context and resources, social/professional role/identity and emotion. This was in parallel to six less relevant meta-themes representing beliefs about consequences, optimism, reinforcement, intentions, goals and social influences.
Domain 1 (Knowledge)
Lack of awareness of guidelines and a lack of focussed respiratory management pre-eminently associated with COPD management were identified as a major barrier to the formation of knowledge and subsequent utilisation of the guidelines. Participants expressed a lack of awareness of the guidelines and declared they had never accessed them. Clinicians expressed their awareness of international guidelines and the need to utilise them, however, existence, awareness and utilisation of Australian National COPD-X guidelines in the clinical area existed to be a source of confusion for some clinicians. Participants stated if they were aware of community services or how and where to refer, they would action these referrals. Lack of education and in-services on the guidelines and management of COPD patients were expressed as a cause of non-adherence by most participants in the emergency department. Several participants noted that it was difficult to grow knowledge around COPD guidelines as the systems access or online availability of resources was quite poor. Participants believed continuing education with respiratory focus, through in-service and awareness programmes to point towards existing community services would augment staff awareness, utilisation and adherence. A complete summary of staff perspectives and the recommended evidenced based implementation strategies from BCT and participants for the TDF domain 1, knowledge is identified in Table 2.
 |
Table 2 Identified Barriers Mapped to COM-B Model and Recommended Implementation Strategies from BCW and Participants for TDF Domain 1: Knowledge |
Domain 2 (Skills)
Emergency department staff consult diverse disease conditions and as a result upskilling according to all specialities can be challenging. Participants reported lacking skills and experience in respiratory management and patient education skills that have affected their capacity to implement the guidelines in clinical practice. Current in-service educational sessions for the Emergency Department staff are not targeted to training particularly with respiratory disease management skills. It was noted that some staff bring years of expertise working in different clinical areas prior to working in ED. Physiotherapists who had more experience working in the ED stated that their skills and knowledge are mostly in musculoskeletal therapy and there is no staff from their department who are focussed on respiratory conditions in the ED. Nurses noted that they are often teaching patients on inhaler technique however are not trained themselves on the best techniques or specific detail outlined in the COPD-X guidelines. Clinicians who had more knowledge of disease condition and preventative measures of COPD had acquired skills during their undergraduate medical training, conferences, or working in respiratory wards previous to commencing in the ED. Three participants reported ongoing educational sessions on COPD management, preventative and restorative health and appropriate referrals are inevitable as they have multiple specialities to accommodate when working in an ED. A comprehensive summary of participant perspectives on lack of respiratory management skills is provided in Table 3.
 |
Table 3 Identified Barriers Mapped to COM-B Model and Recommended Implementation Strategies from BCW and Participants for TDF Domain 2: Skills |
Domain 3 (Beliefs About Capabilities)
Reality or validity regarding the ability to adhere to COPD-X guidelines in the emergency department is explored in this domain. Table 4 outlines the beliefs about the capabilities of the participants interviewed. Interdisciplinary staff disclosed a lack of confidence in managing and discharging COPD patients. Most participants expressed that due to the nature, busy pace and time constraints in EDs are not feasible to provide care more than the acute emergent needs of the patient. National emergency access target (4 hours in ED) rule emphasise the requirement of discharging a patient from ED to make space available for upcoming acute patients which results in a higher turnover of patients, increased pressure and demand on staff. Participants believed the challenging and unprecedented nature of the emergency department with high acuity patients, and life-threatening conditions diminish their capability to provide care more than acute emergent needs of the patient. The participants revealed that time constraints and the volume of patients impact the capabilities of staff to provide accurate discharge planning or referrals as per guideline recommendations, such as vaccination, smoking cessation and other non-acute guideline-recommended interventions. Participants are certain that time-efficient assessment and referral processes could prevent fragmented care and COPD remissions or related readmissions. Although participants agreed on a current lack of capacity to provide discharge planning and referrals, it was evident from their responses that easily accessible patient information for packages for smoking cessation and easier electronic referrals to the community from ED could prevent COPD readmissions.
 |
Table 4 Identified Barriers Mapped to COM-B Model and Recommended Implementation Strategies from BCW and Participants for TDF Domain 3: Beliefs and Capabilities |
Domain 4 (Memory Attention and Decision Process)
Ability to retain information from guidelines is compromised periodically as participants are required to deal with a multitude of life-threatening conditions from different specialities of medicine at any point in time within a single shift. Thus, participants discussed that recalling all management, recommendations and treatment modalities from COPD guidelines can be difficult. It was clear that participants preferred speciality based review from a respiratory clinical nurse consultant in the first instance to facilitate appropriate care prior to discharge from ED. Multiple staff reiterated the need for point of care clinical cues, prompts, checklist and easier access to resources including patient information as a probable solution to better adherence to COPD guidelines. A sense of optimism existed between staff as they expressed that if they had the resources and timely access to utilise knowledge with accurate digital instructions, then guideline adherence is likely to improve. Table 5 shares quotes and implementation strategies relating to memory attention and decision processes by staff caring for COPD patients in the ED.
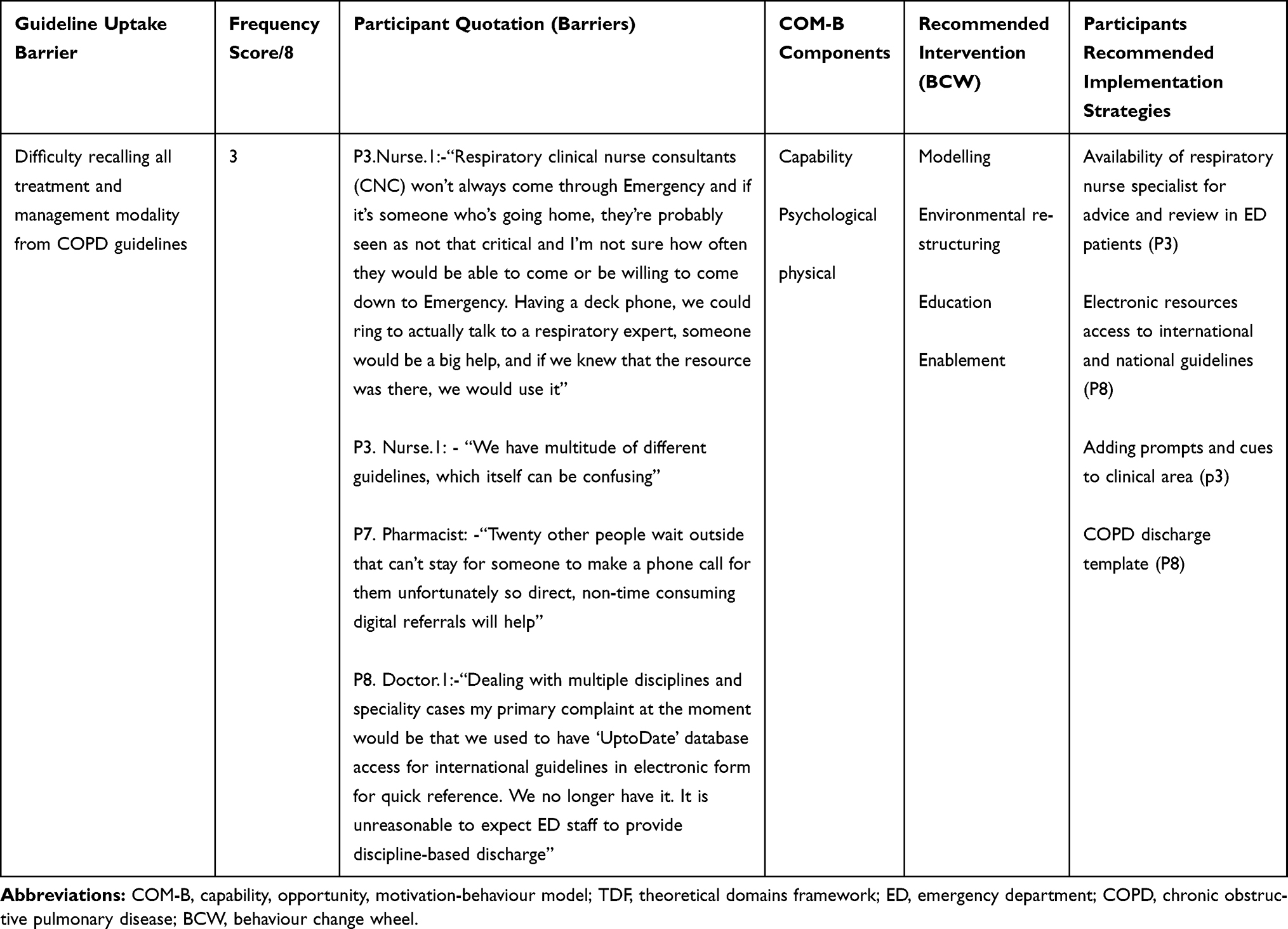 |
Table 5 Identified Barriers Mapped to COM-B Model and Recommended Implementation Strategies from BCW and Participants for TDF Domain 4: Memory Attention and Decision Process |
Domain 5 (Behavioural Regulation)
Clinical behaviour measured objectively that is capable of affecting COPD-X plan guideline adherence is discussed in this domain. Participants indicated that interdisciplinary staff often fail to abide by the current corporate governance, services and management. Common themes emerged through the experience of participants for areas of quality improvement including: anxiety, smoking cessation, palliative care, opportunistic vaccination, inhaler compliance and pulmonary rehabilitation referrals. Participants expressed that each of these areas could be improved and the social worker indicated that they are hardly involved in the emergency department patient referral process prior to discharge. To a certain degree, all staff agreed with better systems and change management with appropriate implementation strategies this may be rectified. The participants expressed areas where improvements could occur. These areas supported by the experiences of participants suggested having ED respiratory change champions, better technology to provide ED to community referrals and COPD discharge templates that could be utilised to assist staff to screen and refer in the ED as per the COPD guidelines. The specific quotes and implementation strategies are outlined in Table 6.
 |
Table 6 Identified Barriers Mapped to COM-B Model and Recommended Implementation Strategies from BCW and Participants for TDF Domain 5: Behavioural Regulation |
Domain 6 (Environmental Context and Resources)
The environmental context and resources domain confer circumstances and situations that discourage guideline adherence. This domain had the highest frequency of themes comprising funding, staffing, inability to communicate, lack of equipment and lack of appropriate referral systems. Participants outlined the need for more resources during the winter months. Throughout this time frame participants identified periods that required more respiratory staffing and funding allocated to meet the higher patient demands in respiratory presentations. Participants repeatedly stated if psychology team and occupational therapist are employed to an ED team, they would be able to assist with better management of COPD patients in terms of anxiety and acopia management strategies. Participants commented that equipment such as spirometry and other pulmonary function tests are not readily available and are dismissed as the job of respiratory specialty rather than ED staff. In addition, it was evident from participant statements that care requirements including vaccinations, smoking cessation and pulmonary rehabilitation referrals were not provided to patients on discharge. Participants outlined that current barriers hindering appropriate interdisciplinary referrals included the lack of environmental resources such as technology being unavailable to enable direct referrals to respiratory outpatient clinics or directly to community services. Three participants expressed restructuring of care processes with direct respiratory clinic referral processes, a respiratory nurse review in ED and electronic concise interdisciplinary COPD guidelines for ED management will assist better utilisation of guidelines. Participants identified that these initiatives could assist in the promotion of COPD guideline adherence in the ED. The barriers and implementation strategies recommended by participants are outlined in Table 7.
 |
Table 7 Identified Barriers Mapped to COM-B Model and Recommended Implementation Strategies from BCW and Participants for TDF Domain 6: Environmental Context and Resources |
Domain 7 (Social Professional Role Identity)
Coherent set of clinical behaviours influenced by the social and professional role identity of interdisciplinary staff is elucidated in this domain (Table 8). Participants identified their professional standing in the interviews and each expressed a clear understanding of their role and scope of practice in the ED. They identified professional boundaries and lack of role clarification in managing COPD patients and lack of communication amongst staff had affected the uptake of guideline adherence. Participants stated they were confused regarding referrals for COPD patients particularly in regard to needing more clarity, access or guidance around interdisciplinary professional roles relating to the COPD guidelines. In addition, they felt that these areas inevitably contributed to guideline adherence in the ED. Role clarification and lack of systems referral processes remain a barrier to provide appropriate care to COPD patients in the ED.
 |
Table 8 Identified Barriers Mapped to COM-B Model and Recommended Evidenced Based Implementation Strategies from BCT and Participants for TDF Domain 7: Social Professional Role Identity |
Domain 8 (Emotion)
Personal belief, attitude and nihilistic views of treating staff towards guideline adherence and related quality initiative, acting as a barrier towards ED COPD holistic management will be construed in this domain. A layer of confusion existed as participants expressed concerns about referrals of COPD patients in the ED. Participants expressed a general perception or attitude with staff viewing non-acute care patients to be beyond their responsibility. Non-acute patients tended to be discharged from ED without appropriate follow-up and participants disclosed concern that for some patients presenting to the ED, this results in increasing COPD remissions and readmissions. In addition, participants repeatedly stated due to different professions and specialities involved in the Emergency Department in terms of setting and treating patients this perception leads to poor interdisciplinary communication with referrals and patient management. Participants outlined that the primary care team specialising in patients within the realm of Chronic Obstructive Airways Disease should be held responsible for non-adherence. Table 9 identifies the emotional barriers to adherence and the strategies identified by participants of this study to improve practice and compliance with COPD guidelines by staff in the ED. These strategies included better communication, delegation and planning between specialty departments interdisciplinary staff may assist in mitigating this attitude amongst staff.
 |
Table 9 Identified Barriers Mapped to COM-B Model and Recommended Implementation Strategies from BCW and Participants for TDF Domain 8: Emotion |
Less Relevant Domains
Six Domains were considered less relevant due to their lower frequency scores of below 3 which included domains surrounding beliefs about consequences, reinforcement, optimism, intention, social influences and goals (see Table 10). Two participants expressed the consequences of performing multidisciplinary care in ED is the verity that other patients may be compromised with acute emergent care needs (beliefs of consequences). Several participants thought automation and technological advancement with clinical cues and prompts in the ED could be beneficial to COPD guideline usage and compliance. Participants recommended utilising an interdisciplinary checklist, e-resources and patient community services information packages to assist with reinforcing interdisciplinary staff behaviour to enable COPD guideline adherence (Reinforcement). Multiple participants revealed having resource champions in the respiratory area and interested senior staff engagement in evaluation methods and leadership is anticipated and proven to increase interdisciplinary guideline adherence (Reinforcement). Participants believed that time-efficient systems for clinicians and interdisciplinary staff knowledge enhancement practices will improve guideline adherence (optimism). Participants felt positive in involving community services as it was deemed a usual referral in the prevention of COPD-related remissions and readmissions to ED (optimism). Participants stated they intend to provide guidance to the primary care physician with discharge letters to ensure appropriate services are facilitated in the community to assist COPD patients with better health-related quality of life (Intention). Further, they identified that communication between staff is pivotal to reduce inpatient admission, timely discharges, prevent remissions and readmissions to ED (social influences). Participants have not identified any barriers with their goals (domain.14) towards guideline adherence in this study.
 |
Table 10 Identified Barriers Mapped to COM-B Model and Recommended Implementation Strategies from BCW and Participants for Domains 9,10, 11,12,13 (Beliefs About Consequences, Reinforcement, Optimism, Intention, Social Influences) |
Discussion
This research study is the first of its kind exploring modifiable factors to improve uptake of COPD guidelines from an interdisciplinary ED staff perspective. Knowledge, skills, behaviour and environmental context and resources have impacted the implementation and uptake of guidelines in clinical practice.1 Utilising the theoretical domains framework and behaviour change techniques provides a novel, contemporary approach that is adopted here to share the experience of the interdisciplinary teams and explore views on future implementation strategies that could be adopted within emergency departments. Emerging themes from the interviews consolidate that improving adherence to clinical guidelines was highly dependent on knowledge; skills; beliefs about capabilities; memory attention, decision process; behavioural regulation; environmental context and resources; social/professional role identity; reinforcement; beliefs about consequences and emotions. These domains applied into the COM-B, behaviour change wheel enlightened the research team with selection and recommendation of intervention strategies suggested by participants, validated through substantiated implementation frameworks and clinical practice behaviour change science. Adoption and implementation of improved strategies will have the potential to improve guideline adherence, patient outcomes and reduce COPD remissions and ED readmissions.17,26,31
Relevant key impediments to guideline adherence remain with a lack of knowledge of the existence of guidelines and the significance of timely or existing referrals (for example, referrals to a pulmonary rehabilitation program) services from the ED. Significance of time-efficient referral processes and identification of education and ongoing assistance with referral processes is vital in the ED to assist staff, patients and to meet the national targets of creating bed space for new patients within 4 hours of admission. Literature reviews and other adherence papers support this research interpretation as education initiatives and ongoing training is essential to influence staff to comply with COPD guidelines.1,16,19,20,26 Environmental hindrances such as patient acuity, resources and staffing during peak hours and in the winter timeframe in the department were identified as sources of concern. Strategies were identified to assist with the prioritisation of implementation of strategies that specifically focused on improving the uptake of COPD guidelines in practice. Interventions to be considered to augment this uptake of COPD guidelines include educational training (self-directed or department focussed), clinical reminders with easier access to concise guidelines, change champions in the departments, direct referrals to the community with the inclusion of pharmacist home medicine reviews, COPD discharge templates, time-efficient digital referrals from the ED and digital enablement of interdisciplinary communication pathways. Digital reminder or systems access for information of COPD guidelines would assist with easier utilisation of referrals and guidelines in practice in an unprecedented and challenging ED environment.3,16,18,32–34
The strategies likely to improve the implementation of COPD guideline adherence identified after mapping to the evidence-based framework to design behaviour change techniques according to the COM-B model are educational in-services, ED change champions steering the knowledge dissemination, digital referral and access to COPD resources for staff and patients. Interdisciplinary staff clinical behaviour change is integral to increase and sustain guideline adherence. Digitalizing and delegation with appropriate referrals will also provide time-efficient care in the Emergency departments (See Tables 4, 6, 7, 9 and 10). Preliminary findings of a systematic literature review and scoping review protocols (should you reference yourself up) exploring modifiable barriers to enhance COPD guideline adherence and referrals in the hospitals support the findings of the recommendations arising from this current study to promote uptake of COPD guidelines35,36 Targeted behaviours and recommended selection of 93 behaviour change techniques (BCT) recommended by the taxonomy and deducted from data analysis are categorised into capabilities, opportunities and motivation strategies.29 Capability components are demonstrated by specific skills and knowledge of guidelines and management of COPD patients, whereas opportunity components evaluate and instil social and environmental factors external to interdisciplinary clinicians to assist facilitation of change. Motivation components involve reflective or emotional processes that encourage uptake and clinical practice of guidelines.
The capability component in this model is explained as the physical and psychological ability to engage, comprehend and reason with the barriers. Problem behaviours acting as a barrier in this category are recommended to be approached with modelling and enablement. Identified interventions such as in-services training, provision of resources including self-directed study, time efficient and readily access, ED champions to lead new implementation, COPD ED discharge templates, and direct referrals by admin staff would assist to enhance uptake of guidelines (see Tables 2, 3, 5 and 6). Opportunity components in this model construe physical and social opportunities affordable by the staff in their clinical environment. Recommended approaches by the framework are restriction, environmental restructuring and enablement. Recommendations were made for more funding, increased staffing, dedicated administration staff to do referrals, digital platforms to promote quicker and clearer interdisciplinary communication and restructuring clinical processes to a time-efficient clinician-friendly manner to adapt to the bustling nature of the emergency departments (see Tables 4, 9 and 10). Motivation components comprise reflective and automatic motivation to address staff clinical behaviour, emotional responses, beliefs and intention towards utilising COPD clinical guidelines. Reflective motivation focuses on education, persuasion, incentivisation and coercion, whereas automatic motivation includes all mentioned strategies in addition to environmental restructuring, modelling and enablement. Recommendations from this study include time-efficient electronic referrals, automated electronic staff/patient information resources and discharge templates with respiratory department consultation and consensus to complement COPD guidelines adherence and management (see Tables 7, 8 and 10).
COPD is a multimodal disease that requires a multidisciplinary involvement of a comprehensive health care team that is skilled, knowledgeable and has the capacity to implement best practice strategies in line with national COPD guidelines. To enable clinicians, it is recommended that the roles within multidisciplinary teams are clear within and across disciplines and through implementation strategies. The contribution of all clinicians towards the preferential implementation of COPD guidelines in practice is indispensable to prevent readmission of patients within the ED. Future interventions and implementation strategies should adopt educational training, assistance and resource provision appealable to multidisciplinary teams and in an environment where online resources are readily available and accessible.
Conclusion
Barriers and potential solutions to improve COPD-X plan guideline adherence in the emergency department were explored through this study. Utilisation of a framework (TDF) and associated behaviour change technique application in conjunction with participants' recommendations suggest multiple intervention strategies to acquire guideline uptake in the emergency department. Education, training and provision of resources notably in easily accessible electronic formats and time-efficient software platforms are prominent and preferred implementation strategy to improve guideline adherence.
Strengths and Limitations
The multidisciplinary approach to this study assisted with capturing the experiences of clinicians from a range of health-related disciplines. However, this study was conducted in one acute care ED setting and hence generalizability will be limited. This facility did not employ a psychologist in the ED setting thus no inclusion of this area of allied health engagement could be captured. The inclusion of a psychological team member may have further assisted in providing emotional and anxiety-related strategies to patients in the ED. A limitation of the study was that the department did not employ respiratory physiotherapists or respiratory clinical nurses in the ED and a study that was inclusive of these clinicians may have contributed to different perspectives and findings.
Abbreviations
COPD, chronic obstructive pulmonary disease; BCT, Behaviour Change Taxonomy; BCW, Behaviour Change Wheel; HREC, Human Research Ethics Committee; ED, Emergency department; TDF, Theoretical Domains Framework.
Data Sharing Statement
To protect the rights and confidentiality of participant details raw data will only be available to members of the research team. No data will be shared externally or in any public forum. Only de-identified data summaries will be shared publicly.
Ethical Approval and Informed Consent
Ethics approval was obtained prior to commencement from the Metro North Hospital Human Research Ethics Committee (HREC EC00168/55098). A site-specific ethics/administrative approval including a research agreement between Metro North hospital (The Prince Charles hospital) and the University of Southern Queensland was acquired. Ethics approval was also gained from the University of Southern Queensland, Human Research Ethics Committee (H19REA308). The ethics was categorised as low risk. Signed participant consent was obtained and a participation information sheet was provided to each participant prior to interviews. Research collaboration agreement for publication was obtained between southern Queensland and Metro north hospital. Participants' information sheet included the publication of anonymised responses and this study was conducted in accordance with the Declaration of Helsinki. Data management adhered to the Metro North hospital and University of Southern Queensland research data management policy. De-identified hard copy data will be stored by the Principal investigator in a locked filing cabinet with digital transcribed copies of the interviews stored in password-protected University research cloud drive.
Acknowledgments
We acknowledge input from Professor Ian Yang, Thoracic Physician at The Prince Charles Hospital and The University of Queensland, who provided comment on this study from a respiratory medicine point of view. We acknowledge all efforts, support and facilitation provided in the emergency department by Dr. Frances Kinnear, Dr. Alastair Newton and Dr. Polash Adhikari. We express deep gratitude to all research participants for providing us with their valuable time for the prospects of improving patient care.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Lodewijckx C, Sermeus W, Vanhaecht K, et al. Inhospital management of COPD exacerbations: a systematic review of the literature with regard to adherence to international guidelines. J Eval Clin Pract. 2009;15(6):1101–1110. doi:10.1111/j.1365-2753.2009.01305.x
2. Seys D, Bruyneel L, Decramer M, et al. An international study of adherence to guidelines for patients hospitalised with a COPD exacerbation. COPD: J Chronic Obstr Pulm Dis. 2017;14(2):156–163. doi:10.1080/15412555.2016.1257599
3. Kelly A-MA-M, Van Meer O, Keijzers G, et al. Get with the guidelines: management of chronic obstructive pulmonary disease in emergency departments in Europe and Australasia is sub-optimal. Intern Med J. 2020;50(2):200–208. doi:10.1111/imj.14323
4. Lewis A, Axson EL, Potts J, et al. Protocol for a systematic literature review and network meta-analysis of the clinical benefit of inhaled maintenance therapies in chronic obstructive pulmonary disease. BMJ Open. 2019;9(2):e025048. doi:10.1136/bmjopen-2018-025048
5. Yang IA, George J, Jenkins S, et al. The COPD-X plan: Australian and New Zealand Guidelines for the management of chronic obstructive pulmonary disease 2018. 2018.
6. Gold PM. The 2007 GOLD Guidelines: a comprehensive care framework. Respir Care. 2009;54(8):1040–1049.
7. Crawford G, Brooksbank MA, Brown M, et al. Unmet needs of people with end‐stage chronic obstructive pulmonary disease: recommendations for change in Australia. Intern Med J. 2013;43(2):183–190. doi:10.1111/j.1445-5994.2012.02791.x
8. welfare, A.I.o.h.a. Chronic obstructive pulmonary disease (COPD). H.a. welfare, Editor. web report; 2017.
9. Australian Institute of health and Welfare. Chronic obstructive pulmonary disease. H.a. welfare, Editor. 2017.
10. Kelly AM, Holdgate A, Keijzers G, et al. Epidemiology, treatment, disposition and outcome of patients with acute exacerbation of COPD presenting to emergency departments in Australia and South East Asia: an AANZDEM study. Respirology. 2018;23(7):681–686. doi:10.1111/resp.13259
11. Moloney C. Reducing avoidable COPD emergency room presentations: an integrated cross-health service utilisation scoping initiative in South Queensland. Respirology. 2020;25(S1):143.
12. Rana R, Gow J, Moloney C, et al. Does distance to hospital affect emergency department presentations and hospital length of stay among COPD patients? Intern Med J. 2020. doi:10.1111/imj.15014
13. Australasian College For Emergency Medicine. Triage. 2020 [cited 2021]; Available from: https://acem.org.au/Content-Sources/Advancing-Emergency-Medicine/Better-Outcomes-for-Patients/Triage.
14. Harrison SL, Goldstein R, Desveaux L, et al. Optimizing nonpharmacological management following an acute exacerbation of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2014;9:1197. doi:10.2147/COPD.S41938
15. Corrado A, Rossi A. How far is real life from COPD therapy guidelines? An Italian observational study. Respir Med. 2012;106(7):989–997. doi:10.1016/j.rmed.2012.03.008
16. Overington JD, Huang YC, Abramson MJ, et al. Implementing clinical guidelines for chronic obstructive pulmonary disease: barriers and solutions. J Thorac Dis. 2014;6(11):1586–1596. doi:10.3978/j.issn.2072-1439.2014.11.25
17. Considine J, Botti M, Thomas S. Emergency department management of chronic obstructive pulmonary disease: Audit of compliance with evidence based guideline. Intern Med J.2011;41(1a):48–54. doi:10.1111/j.14455994.2009.02065.x.PMID:19811556
18. Sha J, Worsnop CJ, Leaver BA, et al. Hospitalised exacerbations of chronic obstructive pulmonary disease: adherence to guideline recommendations in an Australian teaching hospital. Intern Med J. 2020;50(4):453–459. doi:10.1111/imj.14378
19. Bartels W, Adamson S, Leung L, Sin DD, Van Eeden SF. Emergency department management of acute exacerbations of chronic obstructive pulmonary disease: factors predicting readmission. Int J Chron Obstruct Pulmon Dis. 2018;Volume 13:1647–1654. doi:10.2147/COPD.S163250
20. Kruis AL, Smidt N, Assendelft WJ, et al. Integrated disease management interventions for patients with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2013;10.
21. Atkins L, Francis J, Islam R, et al. A guide to using the Theoretical Domains Framework of behaviour change to investigate implementation problems. Implement Sci. 2017;12(1):77. doi:10.1186/s13012-017-0605-9
22. Michie S, Atkins L, West R. The Behaviour Change Wheel. A Guide to Designing Interventions.
23. Alsubaiei M, Frith PA, Cafarella PA, et al. COPD care in Saudi Arabia: physicians’ awareness and knowledge of guidelines and barriers to implementation. Int J Tuberc Lung Dis. 2017;21(5):592–595. doi:10.5588/ijtld.16.0656
24. Pothirat C, Liwsrisakun C, Bumroongkit C, et al. Comparative study on health care utilization and hospital outcomes of severe acute exacerbation of chronic obstructive pulmonary disease managed by pulmonologists vs internists. Int J Chron Obstruct Pulmon Dis. 2015;10:759. doi:10.2147/COPD.S81267
25. Kitchlu A, Abdelshaheed T, Tullis E, et al. Gaps in the inpatient management of chronic obstructive pulmonary disease exacerbation and impact of an evidence-based order set. Can Respir J. 2015;22(3):157–162. doi:10.1155/2015/587026
26. Kelly AM, Van Meer O, Keijzers G, et al. Get with the guidelines – management of COPD in emergency departments in Europe and Australasia is sub-optimal. Intern Med J. 2020;50:200–208.
27. Craig LE, McInnes E, Taylor N, et al. Identifying the barriers and enablers for a triage, treatment, and transfer clinical intervention to manage acute stroke patients in the emergency department: a systematic review using the theoretical domains framework (TDF). Implement Sci. 2016;11(1):157. doi:10.1186/s13012-016-0524-1
28. Munday J, Delaforce A, Forbes G, et al. Barriers and enablers to the implementation of perioperative hypothermia prevention practices from the perspectives of the multidisciplinary team: a qualitative study using the Theoretical Domains Framework. J Multidiscip Healthc. 2019;12:395. doi:10.2147/JMDH.S209687
29. Michie S, Richardson M, Johnston M, et al. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behav Med. 2013;46(1):81–95. doi:10.1007/s12160-013-9486-6
30. Patey AM, Islam R, Francis JJ, et al. Anesthesiologists’ and surgeons’ perceptions about routine pre-operative testing in low-risk patients: application of the Theoretical Domains Framework (TDF) to identify factors that influence physicians’ decisions to order pre-operative tests. Implement Sci. 2012;7(1):52. doi:10.1186/1748-5908-7-52
31. Gerber A, Moynihan C, Klim S, et al. Compliance with a COPD bundle of care in an Australian emergency department: a cohort study. Clin Respir J. 2018;12(2):706–711. doi:10.1111/crj.12583
32. Cousins JL, Wark PA, McDonald VM. Acute oxygen therapy: a review of prescribing and delivery practices. Int J Chron Obstruct Pulmon Dis. 2016;11:1067.
33. Harrison A, Borg B, Thompson B, et al. Inappropriate inhaled corticosteroid prescribing in chronic obstructive pulmonary disease patients. Intern Med J. 2017;47(11):1310–1313. doi:10.1111/imj.13611
34. Markun S, Franzen DP, Dalla Lana K, et al. Acute exacerbated COPD: room for improvement in key elements of care. Int J Chron Obstruct Pulmon Dis. 2017;12:2969. doi:10.2147/COPD.S145496
35. Moloney C, Sneath E, Phillips T, et al. Recommendations and practices for holistic (COPD) assessment and optimal referral patterns in emergency department presentations: a scoping review protocol study. BMJ Open. 2019;9(8):1–5. doi:10.1136/bmjopen-2019-030358
36. Issac H, Moloney C, Taylor M, et al. Mapping of modifiable barriers and facilitators with interdisciplinary chronic obstructive pulmonary disease (COPD) guidelines concordance within hospitals to the Theoretical Domains Framework: a mixed methods systematic review protocol. BMJ Open. 2020;10(7):e036060. doi:10.1136/bmjopen-2019-036060
37. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
38. Michie S, Atkins L, West R. The behaviour change wheel. A guide to designing interventions. 1st ed. Great Britain. Silverback Publishing. 2014;10:03–1010.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.