")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 15
Explorative analysis of gender-specific characteristics in patients with heart failure in an Italian hospital
Authors Perrone V, Veronesi C, Nica M, Colombo D , Degli Esposti L , Castello R
Received 26 January 2019
Accepted for publication 6 June 2019
Published 8 July 2019 Volume 2019:15 Pages 847—850
DOI https://doi.org/10.2147/TCRM.S203011
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
V Perrone,1 C Veronesi,1 M Nica,2 D Colombo,2 L Degli Esposti,1 R Castello3
1Clicon S.R.L. Health, Economics and Outcomes Research, Ravenna, Italy; 2Novartis Pharma, Origgio, VA, Italy; 3Division of General Medicine, University Hospital of Verona, Verona, Italy
Abstract: Sex-related differences have been shown to deeply affect health-related aspects of patients. However, the lack of gender-specific analysis makes it difficult to advance personalized medicine in terms of a gender-based approach. The aim of the present study was to describe gender-specific features of patients diagnosed with heart failure (HF), with a focus on the clinical presentation. Data were collected from a properly designed database and referred to an Italian hospital. Patients aged ≥18 years with a primary or secondary diagnosis of HF between 1 January 2012 and 31 December 2016 were included, and their demographic and clinical characteristics were analyzed according to gender. Of the 719 HF patients included, 317 (44.1%) were male and 402 (55.9%) were female. Women tended to be older compared to men (82.4±8.8 years and 77.1±10.6 years, respectively). As for clinical presentation, 62.1% of female and 38.3% of male patients had preserved ejection fraction, and 56.1% of men and 58.2% of women suffered from atrial fibrillation. The left atrium was partially compromised in 62.4% of male and 63% of female patients, while right atrium dysfunction tended to be more frequent in male patients compared to female patients (29.1% and 25.5%, respectively). In conclusion, gender-specific features of a cohort of HF patients from a clinical setting were accurately described.
Keywords: gender, specific characteristics, heart failure, clinical setting
Sex-related differences have been shown to deeply affect health-related aspects of patients; for that reason, in recent years the approach to diagnosis, treatment, and prevention of diseases is becoming even more gender-specific.1 Regarding the National Healthcare System, the attention on sex-related differences aims at increasing the appropriateness of prevention, diagnosis, and treatment as well as rehabilitation of patients, particularly for those diseases with major epidemiologic impact, such as cardiovascular diseases.1,2 As also mentioned in a recent document released by the WHO entitled “Health 2020: European Policy for Health and Well-being”,3 gender is identified as a crucial and fundamental issue as it affects health status, well-being and its perception, disease onset and progression, and pharmacological treatment approaches and their efficacy. However, the lack of gender-specific analysis makes it difficult to advance personalized medicine in terms of a gender-based approach.4
To this end, here we present an observational retrospective study whose aim was to describe gender-specific features of patients diagnosed with heart failure (HF), with a focus on the clinical presentation. The study was based on a designed database in which the selected data were previously extracted from medical records and hospitalization and laboratory test databases of the General Medicine Unit of the University Hospital of Verona (Italy); we included all patients aged ≥18 years with primary or secondary diagnosis of HF at hospital discharge (International Classification of Diseases, 9th Revision, Clinical Modification ICD-9-CM code 428) between 1 January 2012 and 31 December 2016. For all included patients we identified the index date (ID) as the date they met the inclusion criteria. As regards the presence of comorbidities, patients were classified as: a) HF only (ICD-9-CM code 428); and b) HF and diabetes mellitus (DM, ICD-9-CM codes 428 and 250). Demographic and clinical characteristics of patients at the ID were analyzed according to gender. We also analyzed the length of stay and costs related to the hospitalization index. All results were produced in an aggregate way. According to the Italian Guidelines regarding the conduction of observational studies,5 this study has been notified to the competent local Ethics Committee (University Hospital of Verona). Informed consent was not required, since it is not required when using encrypted retrospective information for research purposes.
A total of 719 HF patients were included and, except for the cohort of HF patients with DM, the percentage of female patients was higher compared to male patients (Table 1). According to the mean age at the ID, women tended to be older compared to men (82.4±8.8 years and 77.1±10.6 years, respectively; Table 1). Concerning the clinical presentation of patients at the time of HF diagnosis, a higher percentage of female patients had preserved ejection fraction compared to male patients (62.1% vs 38.3%, respectively), not only in the total study population but also when the single cohorts were considered (Table 1). 56.1% of men and 58.2% of women in the total study population of HF patients suffered from atrial fibrillation; this percentage is lower in both genders for the cohort of HF patients with DM compared to HF only patients (Table 1). The proportion of patients with NT-proBNP ≥2,000 pg/mL was higher in women compared to men in the HF cohort (70.6% and 60.8%, respectively), with this proportion inverted in the HF with DM cohort (53.1% and 76.1%, respectively; Table 1). The left atrium was mainly described as partially compromised except for female patients in the HF with DM cohort (Table 1). Right atrium dysfunction at the ID tended to be more frequent in male patients compared to female patients (29.1% and 25.5%, respectively; Table 1).
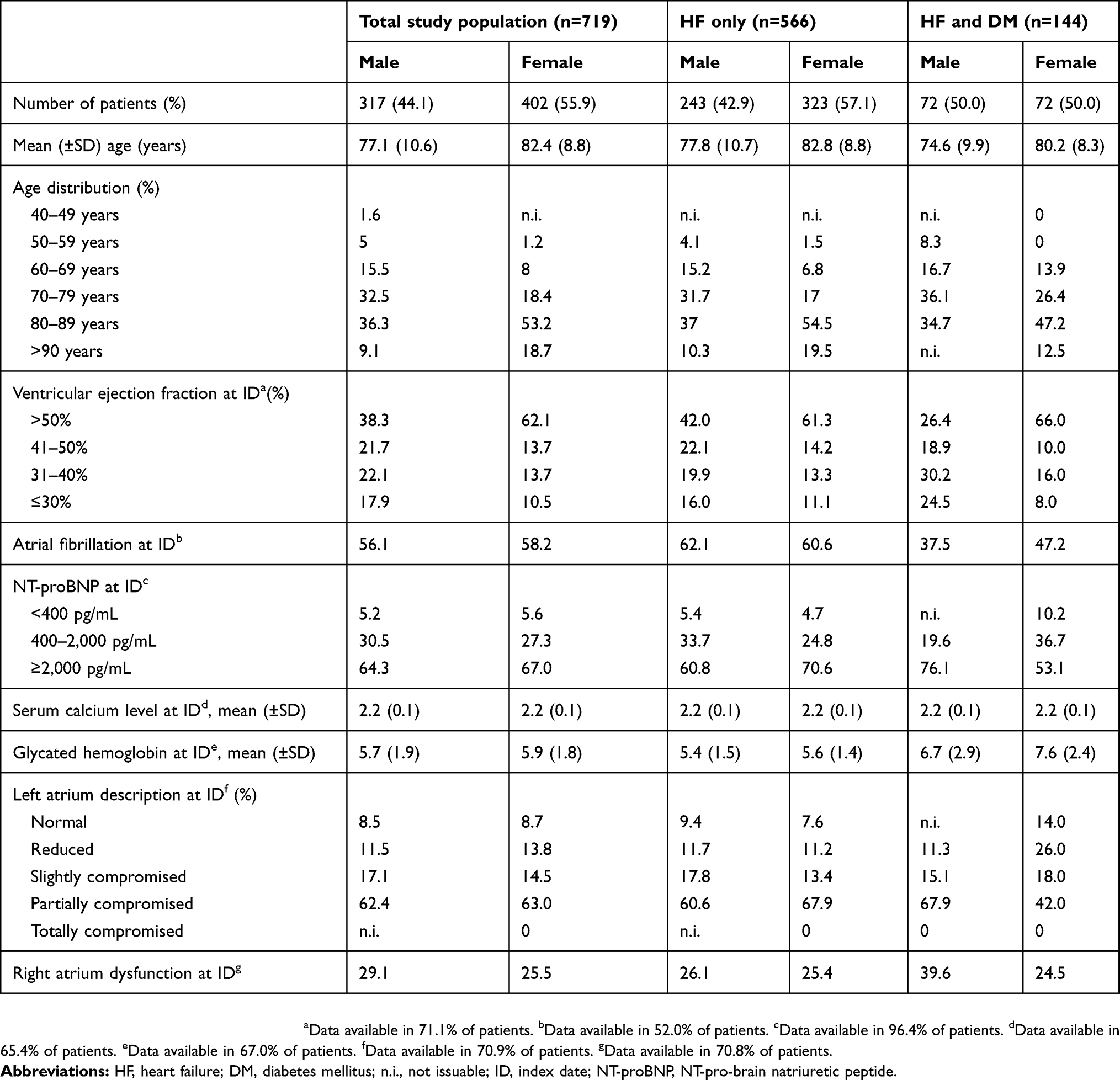 |
Table 1 Gender-specific demographic and clinical characteristics of HF patients |
The length of hospital stay for the hospitalization index was also analyzed; female patients stayed on average 6.9±5.7 days and male patients 7.0±6.5 days (Table 2). The percentage of male patients with subsequent HF-related hospitalization tended to be higher compared to female patients (89.0% and 92.5% of patients had no further hospitalization for HF, respectively; Table 2). Costs related to the hospitalization index were €3,374.27 for male and €3,386.12 for female patients (Table 2).
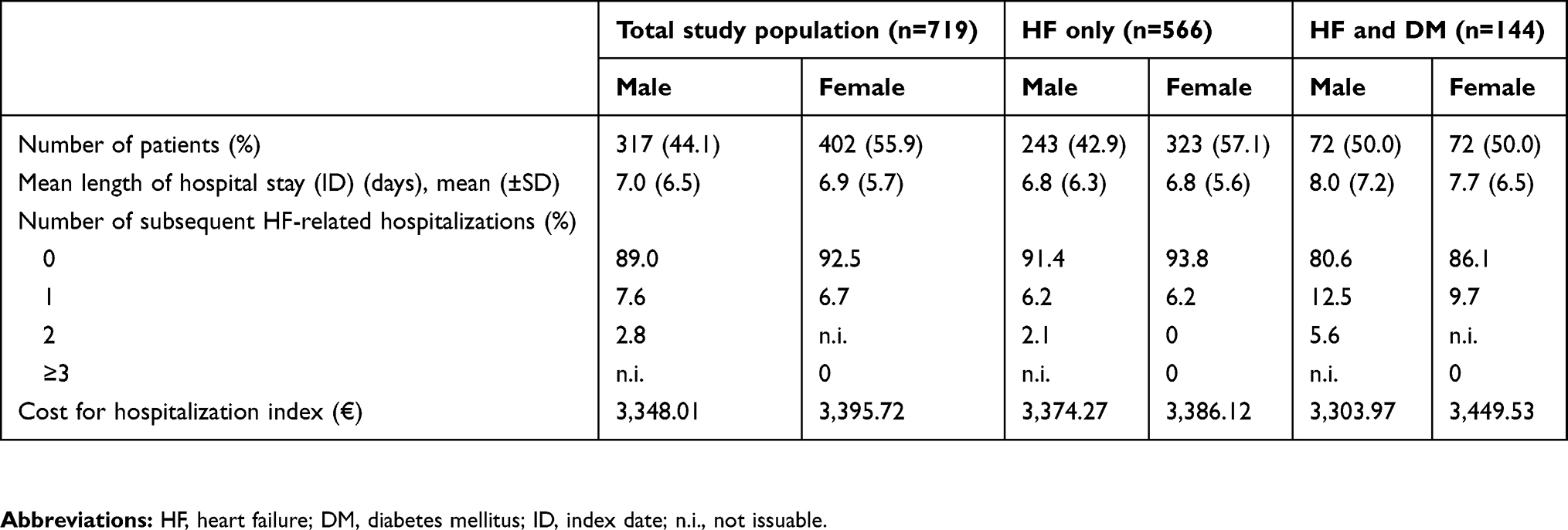 |
Table 2 Gender-specific characteristics of length of hospital stay, subsequent HF-related hospitalization and costs |
In the present study, gender-specific features of a cohort of HF patients from a clinical setting were accurately described. According to mean age, we found that women were older than men in all study populations and in all cohorts considered, consistent with a study reported in the literature.6 Razzolini and Lin7 reported that later-in-life HF is more prevalent in women than in men. In our study, age distribution analysis showed that the percentage of men was higher among age ranges up to 79 years, while this trend reverted after the age of 80 years. The higher percentage of preserved ejection fraction among women was in line with findings reported by Buonanno,8,9 who pioneered the study of sex differences in the pathophysiology of HF, and is now widely observed in the literature.10 To date, HF guidelines do not take into account gender-specific differences due also to the underrepresentation of women in clinical trials,11 therefore analysis of data from the clinical setting can play an important role in improving the knowledge of gender-specific differences in the clinical presentation of HF. Similarly to data reported by Galvao et al's12 and Stein et al's13 studies, no differences were observed among genders for length of hospital stay.
Our cohort of patients reflected real clinical practice, and the results must be interpreted taking into account limitations mainly due to the observational nature of the study. Data were collected from a database properly designed for the study, in which only the variables herein described were reported. Moreover, patients diagnosed and managed by a general practitioner were not included, as the cohort consisted of patients discharged from hospital. The results and conclusions of this study are limited to the population analyzed; furthermore, studies with larger cohorts of HF patients are needed to confirm our results and to permit the application of relevant statistical methods.
Disclosure
The study was funded by Novartis. The authors report no other conflicts of interest in this work.
References
1. Ministero della Salute. [Il genere come determinante della salute. Lo sviluppo della medicina di genere per garantire equità e appropriatezza della cura]. Quaderni Del Ministero Della Salute. 2016;26. Available from: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2490_allegato.pdf.
2. Lorenzin B. [L’attenzione al genere: una scelta strategica per l’appropriatezza]. Ital J Gender-Specific Med. 2015;1(2):41–42.
3. World Health Organization. Health 2020: the European policy for health and well-being; 2012. Available from: http://www.euro.who.int/en/health-topics/health-policy/health-2020-the-european-policy-for-health-and-well-being.
4. Regitz-Zagrosek V, Oertelt-Prigione S, Prescott E, et al.; EUGenMed Cardiovascular Clinical Study Group. Gender in cardiovascular diseases: impact on clinical manifestations, management, and outcomes. Eur Heart J. 2016;37(1):24–34. doi:10.1093/eurheartj/ehv598.
5. AIFA guideline for the classification and conduction of the observational studies on medicines. Available from: https://www.agenziafarmaco.gov.it/ricclin/sites/default/files/files_wysiwyg/files/CIRCULARS/Circular%2031st%20May%202010.pdf.
6. Savarese G, D’Amario D. Sex differences in heart failure. In: Kerkhof PLM, Miller VM, editors. Sex-Specific Analysis of Cardiovascular Function. Vol. 1065. Cham: Springer International Publishing; 2018: 529–544. doi:10.1007/978-3-319-77932-4_32.
7. Razzolini R, Lin CD. Gender differences in heart failure. Ital J Gender-Specific Med. 2015;1:15–20.
8. Buonanno C, Arbustini E, Rossi L, et al. Left ventricular function in men and women. Another difference between sexes. Eur Heart J. 1982;3(6):525–528. doi:10.1093/oxfordjournals.eurheartj.a061347
9. Buonanno C. The female left ventricle: a pathophysiological entity? Int J Cardiol. 1983;4(3):382–386.
10. Dunlay SM, Roger VL. Gender differences in the pathophysiology, clinical presentation, and outcomes of ischemic heart failure. Curr Heart Fail Rep. 2012;9(4):267–276. doi:10.1007/s11897-012-0107-7
11. Mentzer G, Hsich EM. Heart failure with reduced ejection fraction in women. Heart Fail Clin. 2019;15(1):19–27. doi:10.1016/j.hfc.2018.08.003
12. Galvao M, Kalman J, Demarco T, et al. gender differences in in-hospital management and outcomes in patients with decompensated heart failure: analysis from the Acute Decompensated Heart Failure National Registry (ADHERE). J Card Fail. 2006;12(2):100–107. doi:10.1016/j.cardfail.2005.09.005
13. Stein GY, Ben-Gal T, Kremer A, et al. Gender-related differences in hospitalized heart failure patients. Eur J Heart Fail. 2013;15(7):734–741. doi:10.1093/eurjhf/hft024
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.