")
Back to Journals » International Journal of Women's Health » Volume 12
Exploration of Lifestyle Choices, Reproductive Health Knowledge, and Polycystic Ovary Syndrome (PCOS) Awareness Among Female Emirati University Students
Authors Pramodh S
Received 24 July 2020
Accepted for publication 25 September 2020
Published 28 October 2020 Volume 2020:12 Pages 927—938
DOI https://doi.org/10.2147/IJWH.S272867
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Sreepoorna Pramodh
College of Natural and Health Sciences, Zayed University, Dubai, United Arab Emirates
Correspondence: Sreepoorna Pramodh
Zayed University, C-L1-41, Dubai Campus, Academic City, Dubai 19282, United Arab Emirates
Tel +97144021736
Fax +97144021008
Email [email protected]
Objective: Healthy lifestyle and adequate reproductive health knowledge are prerequisites for maintenance of physical and mental well-being of women across the world. With increasing prevalence of metabolic disorders such as polycystic ovary syndrome (PCOS), it is important that sufficient awareness of these issues is generated, especially in conservative communities in Arab regions. The main objective of this study is to assess reproductive health (RH) knowledge and awareness of PCOS among female Emirati students and also to explore their lifestyle choices.
Materials and Methods: A total of 493 Emirati students were recruited based on convenience sampling and completed a survey containing questions related to demography, lifestyle preferences, RH knowledge, and PCOS awareness.
Results: Of the students, 13% self-reported being diagnosed with PCOS, with 3.5% also taking medication for the same, 6% reported having high androgen levels, 30.7% reported polymenorrhea, and 3.5% reported oligomenorrhea for frequency of menstrual cycle. Also, 12.4% students experienced abnormal bleeding (heavy/none) during menstruation and 24% reported excessive body hair. It was found that 4.3% of students were taking medication for hyperglycemia and 75% of students reported a family history of diabetes. Students displayed low reproductive health knowledge and poor awareness of PCOS. Lifestyle preferences indicated low physical activity and high indulgence in fast food.
Conclusion: Lifestyle choices adopted by Emirati University students may predispose them to disorders such as PCOS. Early detection and management of PCOS coupled with a dynamic awareness campaign for RH can help in improving fertility rates of Emirati women. The study identifies major gaps in knowledge and awareness of RH and PCOS in Emirati women that need to be addressed by creating a culturally congruent heathcare policy with emphasis on education and health promotion. Mandatory PA programs and increasing availability of healthy eating options in campus should be considered by all universities, particularly in Arab regions, for improving lifestyle and preventing metabolic disorders in young students.
Keywords: PCOS, reproductive health, lifestyle choices, infertility, menstrual disorder, Emirati, UAE, health policy
Introduction
Polycystic ovary syndrome (PCOS) is a common endocrinological condition afflicting 4–10% women worldwide and may extend to 15–21% based on Rotterdam diagnostic criteria.1,2 It is emerging as a major public health concern with a huge impact on reproductive, metabolic, and psychological health of women worldwide.2 Needless to say, it adds to the economic burden of a country as treatment for infertility and management of other metabolic symptoms is expensive. The most adverse aspect of the disease is its manifestation across the lifespan, predisposing its victims to increased risk of cardiovascular disease (CVD), type 2 diabetes, infertility, and poor quality-of-life due to depression and anxiety.1 CVD is already the leading cause of death among women in UAE;3 conditions such as PCOS will only aggravate this situation.
PCOS begins during adolescence and gradually transitions to adulthood and its effects persist even post-menopause. Clinical features of PCOS can be grouped into three categories – reproductive, metabolic, and psychological – and these features may appear to different extents based on the PCOS phenotype diagnosed. Reproductive features include ovulatory and menstrual dysfunction, infertility, hyperandrogenism, hirsutism, miscarriage, and increased risk of gestational diabetes.1 More than 50% of women with PCOS seek treatment for infertility, and 70–80% of them have oligomenorrhea or amenorrhea.4 Metabolic features comprise increased risk of dyslipidemia, insulin resistance, type 2 diabetes, metabolic syndrome, and CVD. Psychological implications are negative body image, depression, anxiety, and poor quality-of-life.5 Poor lifestyle choices like frequent consumption of fat-laden fast food, sugar-containing drinks, sedentary lifestyle, and lack of adequate exercise can hasten the progress of the disease. The manifestation of this condition is also influenced by ethnicity, genotype, and environmental factors.2 A proper study addressing this disorder among Emirati women in UAE has been lacking.
PCOS is usually diagnosed when patients report to the physician with menstrual irregularity, an inability to conceive naturally, or due to metabolic issues such as dyslipidemia or insulin resistance. Diagnosis was initially based on the National Institute for Health (NIH) criteria of oligomenorrhoea/amenorrhoea and clinical or biochemical hyperandrogenism, but was later modified to include polycystic ovaries at ultrasound as a key diagnostic criterion as recommended by ESHRE/ASRM.6 Usually more than 12 cysts of 8 mm or above are found in the ovary during ultrasound. This Rotterdam Criteria, which is now the accepted diagnostic criteria worldwide, requires diagnosis of two out of three conditions – PCO (P), hyperandrogenism (H), or anovulation (O). In 2006, the Androgen Excess and PCOS (AE-PCOS) recommended that clinical or biochemical hyperandrogenism should be essential for diagnosis, along with oligo-anovulation or PCO.7 The Rotterdam criteria further identifies four phenotypes of PCOS- (i) O+P, (ii) O+H, (iii) H+P, and (iv) O+P+H. Endocrine, metabolic, and psychological features may be present to varying extents in each of these phenotypes.8
Since PCOS is a multifactorial disease, there is no single approach or treatment for managing this condition. However, its symptoms and severity can be managed by proper intervention such as educating young women about the symptoms and implications of this disease, advocating healthy lifestyle, providing counselling for psychological distress, and pharmacological treatment as needed.
In many conservative communities across the world, especially in Arab regions, women hesitate in communicating about reproductive issues such as menstrual irregularity, excess body hair, or low libido. Conventional education systems in these regions also do not emphasize the relevance of knowing basic anatomy and physiology. Science/biology courses are omitted in many schools, resulting in poor physiology knowledge in students.9 Consequently, awareness about infertility and disorders such as PCOS may be low among Arab teenagers.10 Studies conducted in Iran, Saudi Arabia, Oman, and Kuwait have reported PCOS prevalence rate of 6–9%.11 However, no conclusive study indicating its prevalence or awareness of such a condition among Emirati women of UAE has been reported.
United Arab Emirates (UAE) is one of the fastest developing nations of the Arab world. The country is strongly encouraging its national population, especially women, to contribute to its growth by providing ample educational and employment opportunities.12 This has resulted in more young women seeking higher education, pursuing active careers, and consequently advancing the age of marriage and delaying childbearing.13,14 As a result, the fertility rate amongst local Emirati women has dropped.15 This poses a concern as the local Emirati population only constitutes less than 12% of the total population and the government has been actively providing many health programs to address this issue.16–18
Poor lifestyle choices, such as fast food preference, sedentary lifestyle, and unhealthy habits like smoking and drinking among Arab youth, have only exacerbated this fertility issue.19 The purpose of this study was to assess if young Emirati female university students were consciously making life-style choices related to fast food, smoking, or physical exercise, and their awareness of basic terms pertaining to their reproductive health. In this regard, their awareness of PCOS and its symptoms were also evaluated, as it is a rising health concern amongst most reproductively active women in UAE.20,21 This cohort was selected due to their ease in accessibility and also as they represent women in the active reproductive age group in whom early detection and management of PCOS is of utmost importance. The results of this study may be indicative of the knowledge/awareness of other young Arab women in this region and may help formulate suitable public health awareness campaigns. Such interventions are necessary to empower young women in making healthy, conscious choices that may have far reaching effects on their long-term health.
Materials and Methods
Study Design and Sample Recruitment
In total, 512 Female Emirati students taking undergraduate and graduate courses at Zayed University, Dubai campus in the age group of 18–25 years participated in the study. Convenience based sampling was performed and students were administered a questionnaire after obtaining written informed consent. Incomplete questionnaires and those from non-local participants were excluded, thus reducing the sample size to 493. Inclusion criteria was female, Emirati women in the age group of 18–25 with formal school education. Men and non-Emirati women were excluded from the study.
Data Collection Instrument and Procedure
The questionnaire was designed in consultation with a gynecologist, statistician, and student counsellor. The questionnaire included questions pertaining to personal information (age, height, weight, marital status, location of residence, college), lifestyle choices (smoking, fast food preference, soft drinks preference and consumption frequency, physical activity frequency in a week), Knowledge of basic reproductive biology (familiarity with terms such as ovary, uterus, hormones, menstrual periods, etc.), knowledge about PCOS, symptoms of PCOS, frequency of menstrual cycle, diagnosis of PCOS, and Medical history (diabetes, androgen test, ultrasound). Students who answered the question, “Have you been diagnosed with PCOS by a Physician?” in affirmative were considered to be categorized as having PCOS. Key terms in the survey were translated into Arabic and rechecked by a native Arabic speaker (Supplementary text). The survey was initially piloted in a small group of 15 students and their recommendations were considered. Instructors from different colleges in the University were contacted by e-mail and requested for participation in the survey. Eighteen instructors obliged and provided 30 minutes of their class time for administering hard copies of the survey instrument. Students in each class were provided a brief introduction about the purpose of the study and explained that participation was voluntary. Interested students signed the informed consent document and completed the questionnaire. The study was approved by the Research Ethics Committee at Zayed University (ZU16_038_F) and was conducted in accordance with the Declaration of Helsinki.
Data Analysis
Data was entered into an Excel spreadsheet by research assistant and cross-checked by another student assistant. It was coded and entered into SPSS by an investigator. Data obtained were statistically analyzed using Statistical Package for the Social Science (SPSS: SPSS Inc., Chicago, IL, USA) software version 17. Demographic and medical history variables were expressed in frequencies and percentages. Significance of difference in the variables between participants with or without PCOS was determined using student’s t-test. Previous diagnoses of PCOS, self-reported by students, were compared to different symptoms, frequency of menstrual cycles, high androgen, fast food consumption frequency, and duration of physical activity using the Pearson Chi square test of independence. The levels of awareness of reproductive biology terms and PCOS were compared to education level using the same test. A P-value of less than 0.05 was considered to be statistically significant.
Data Availability
All data supporting the findings of this study are available from the corresponding author upon reasonable request.
Results
Demographics
Of the 493 students who participated in the study, the majority were from Dubai (66.3%), followed by Sharjah (17.9%), and the remaining from other emirates. Exposure to peers, academic content, and other experiences in a university may impact awareness levels of students. To evaluate this, we studied the student distribution across different academic levels. Students appeared to be divided in their academic level at the university, with 53% being in their 1st–2nd year and 43.8% in their 3rd–4th year of undergraduate study; 3.1% were in their first year pursuing an entry level program (Figure 1A); 13% of the respondents were pursuing a science related major. The level of study did not appear to impact their knowledge of reproductive health significantly post-analysis with independent samples t-test (P=0.06/0.07). The majority of respondents were between 19–21 years of age (52%), 34% were between 17–19 years of age, and 12% were above 21 years. Of the students experiencing PCOS, 66.6% belonged to the age group 19–21 years (Figure 1B). This association was statistically significant (P=0.034) according to Pearson chi-square test. However, age did not appear to influence knowledge of reproductive health or PCOS awareness.
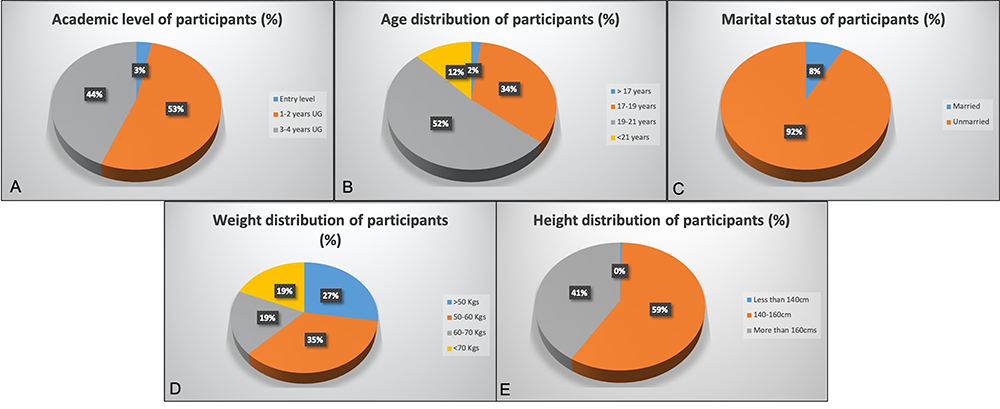 |
Figure 1 Demographic information of all study participants. (A) Academic level, (B) Age distribution, (C) Marital status, (D) Weight range, and (E) Height range of participants. |
The majority (92%) of students were unmarried and 8% were married, of which 3% had children and half of them (1.5%) needed some medical intervention for getting pregnant (Figure 1C). It was observed that 35% of participating students weighed between 50–60 kgs and 19% weighed between 60–70 kgs, 18.5% of students weighed above 70 kgs, and 27.5% weighed less than 50 kgs (Figure 1D). Students who reported being diagnosed with PCOS were distributed through all the weight ranges and weight did not seem to correlate with the condition (Table 1). The majority of students (59%) reported that they were more than 160 cm in height and none were below 140 cm (Figure 1E).
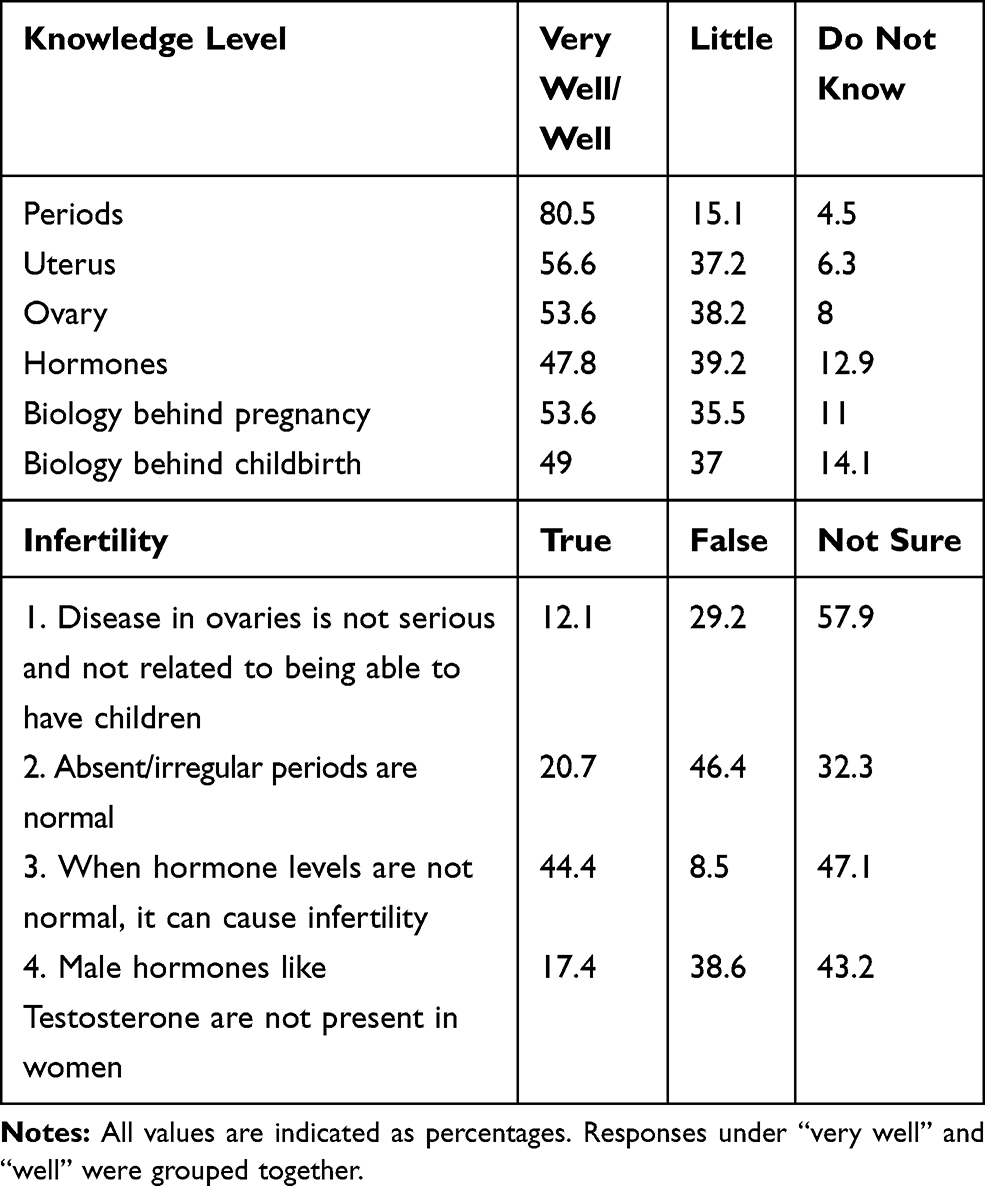 |
Table 1 Reproductive Health and Infertility Knowledge Levels of Study Participants |
Lifestyle Preferences
The majority of students (98%) were nonsmokers (Figure 2A). In total, 64.5% students responded saying that they performed 5 hours or less of physical activity per week and only 3.2% reported doing more than 10 hours/week (Figure 2B). Students reported that walking (77%) and shopping in malls (42.5%) were their favorite physical activity, whereas cycling (11.6%) and doing household chores (16.7%) were their least favored preference (Figure 2C). There was no significant association between physical activity and PCOS diagnosis. Also, 85.4% of students reported consuming fast food less than 5 times a week, 12% at least 5–10 times a week, and 1.2% more than 10 times a week (Figure 2D); 39.4% of students consumed 1–3 soft drinks per week and 3% more than 5 drinks a week (Figure 2E).
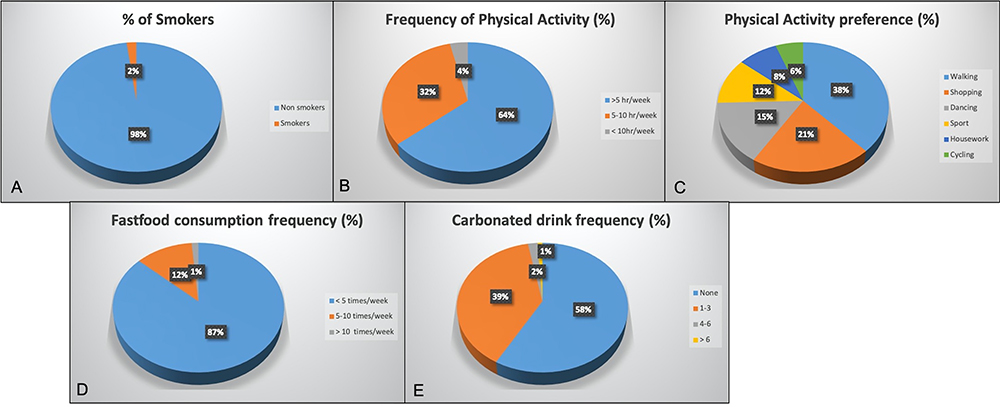 |
Figure 2 Lifestyle choices of participants. (A) Percentage of smokers, (B) Frequency of physical activity, (C) Physical activity preference, (D) Fast food consumption frequency, and (E) Carbonated drink consumption frequency. |
Knowledge About Female Reproductive Biology Terms
In total, 80% of Emirati students were fairly aware of the term “periods”, 56.8% were aware of “uterus”, and 54% students were aware what “ovary” meant. Awareness levels for “hormones” seemed to be less than the other terms, as only 48% knew well about it. Also, 62.5% of participants knew about pregnancy, and only 48.7% knew about the biology of childbirth (Table 1).
Knowledge About Infertility
Students were assessed for their knowledge about infertility by presenting four true/false statements: 57.9% of respondents correctly identified that disease in ovaries was serious and could lead to issues related to conception; 20.7% of students believed that absent/irregular periods were normal, and only 46.7% were sure that this was not true; 44.4% of students were aware that abnormal hormonal levels could lead to infertility, whereas 47.1% were not sure about this fact; 17.4% students were not aware that male hormones like Testosterone could be present in females, while 43.2% were not sure about it (Table 1). These results are indicative that female students were not clear about many important concepts related to infertility.
Awareness About PCOS and Its Symptoms
The term PCOS was explained as a disease afflicting the ovary and described as “growth/cyst or liquid filled bubbles” in Arabic. Only 38.3% had heard about PCOS (Figure 3A). Students were asked if they experienced four major symptoms of PCOS – absent/excess bleeding during menstruation, excessive hair growth, acne, and patches of thick dark skin. In response, 12.4% of students reported experiencing heavy/absent bleeding, 24% reported excessive hair growth on unusual locations such as the face, chest, abdomen, or upper thighs, 40.6% reported oily skin with acne, and 13.5% reported persistent occurrence of patches of thick dark skin. The responses under “always” and “many times” were grouped together (Figure 4). There was a strong correlation of PCOS occurrence with symptoms reported-absent/frequent periods (P=0), hirsutism (P=0), acne (P=0.02), and patches of thick skin (P=0.04).
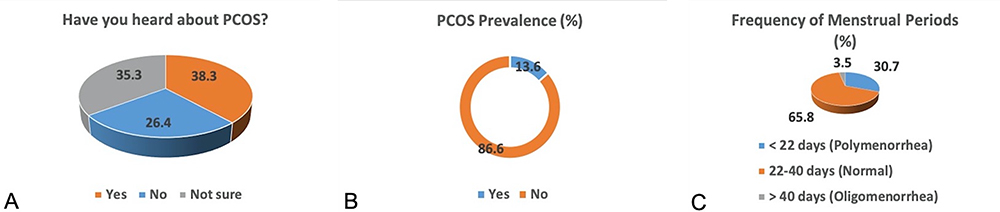 |
Figure 3 PCOS awareness and prevalence in Emirati students and positive correlation with frequency of periods. (A) Percentage of students who were aware about PCOS. (B) Percentage of students who self-reported PCOS after being diagnosed by a physician. (C) Frequency of periods reported by students. |
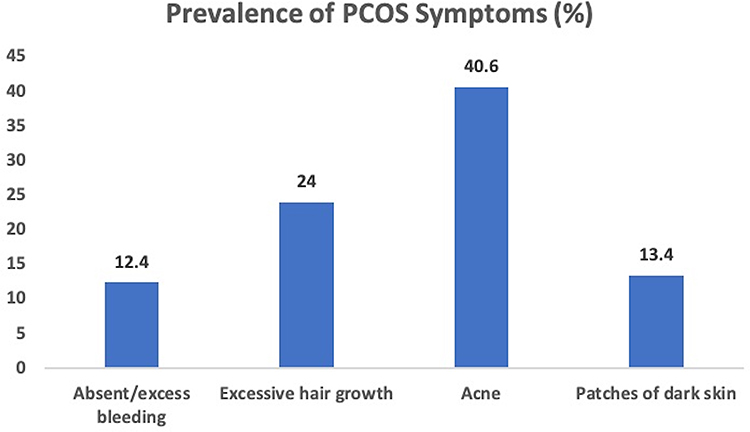 |
Figure 4 Prevalence of different symptoms commonly associated with PCOS in the study subjects. |
Of the respondents, 30.7% students reported poly menorrhea with cycles with intervals of 22 days or less, and 3.5% reported oligomenorrhea (Figure 3C). There was a positive association of detection of PCOS and duration of menstrual cycle (P=0.02). Also, 22.3% of students recollected having their hormone levels tested, of which 6% reported being tested with high androgen levels, and 18.3% of the girls said that they had undergone an ultrasound scan of the uterus or ovaries (Table 2). Since the presence of symptoms, high androgen levels, and scan of ovaries is indicative of PCOS, students were asked if any had been diagnosed with this condition. In reply, 13.4% of students self-reported being detected with PCOS by a physician and 3.5% were also taking medication for the same (Figure 3B). There was also a strong association between PCOS reported responses and those taking medication for it (P=0.02), those who reported high androgen levels (P=0), and those who took an ultrasound (P=0).
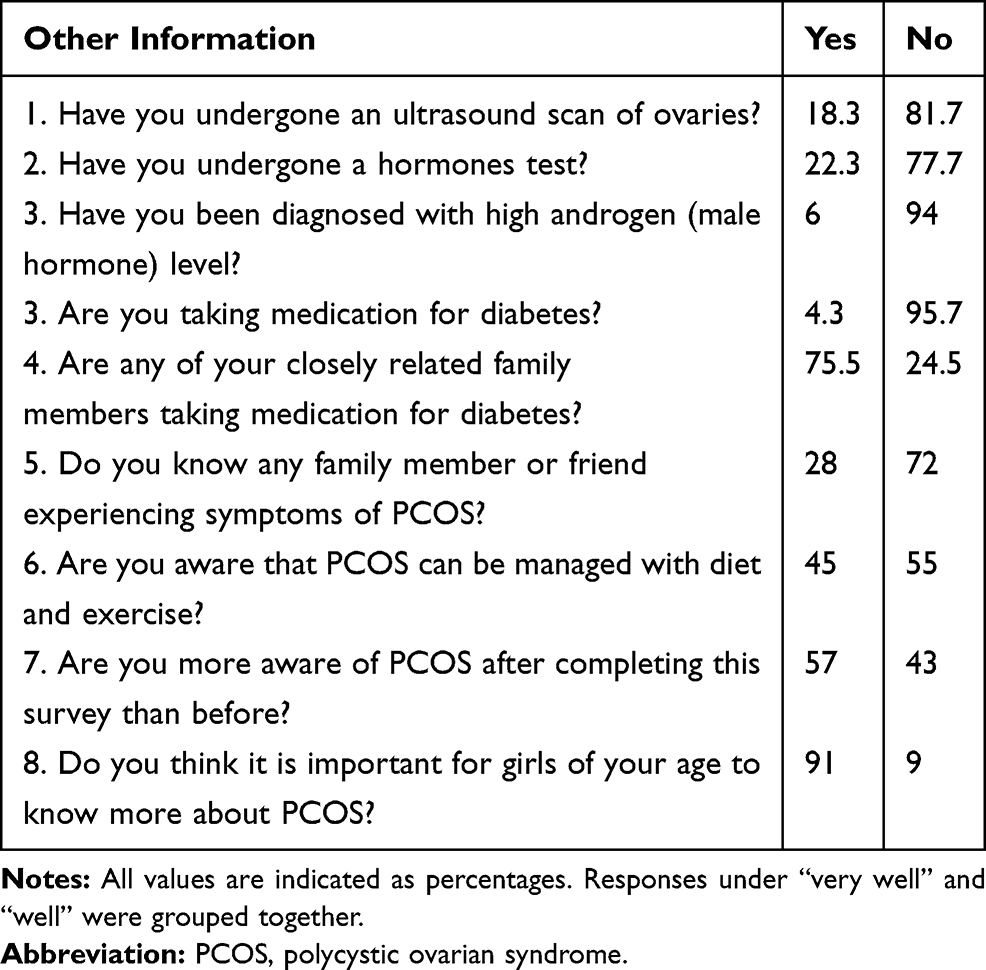 |
Table 2 Medical History and PCOS Related Information Awareness of Study Participants |
It was reported that 4.3% of participants were taking medication for hyperglycemia and a substantial 75.5% had a close family member taking medication for high blood sugar. While 28% students knew friends or family who were experiencing symptoms of PCOS, 45% of total respondents were aware that PCOS could be managed with proper diet, exercise, and medication (Table 2).
Of the 493 students that participated in the survey, 57% agreed that they were more aware about PCOS after completing the survey. A clear majority of 91% girls felt that it was very important for girls of their age to know more about this disease, and 62% expressed that they would prefer to get more information about PCOS from a health center or health professional (doctor, nurse), 29.5% from schools or teachers, 21.5% from the internet, and 16% from media (Figure 5).
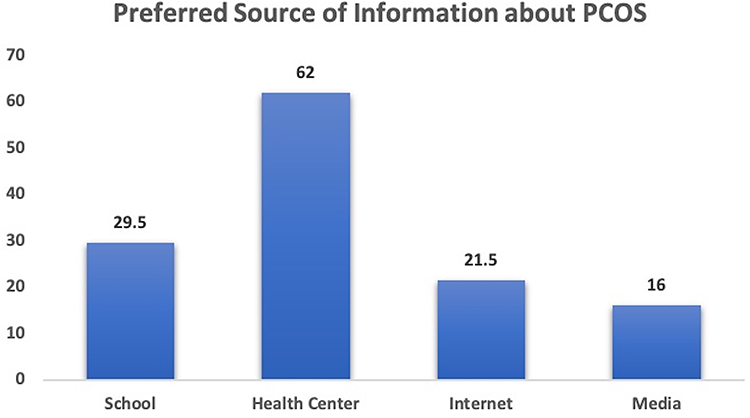 |
Figure 5 Participant’s preferred source for obtaining PCOS related information. |
Discussion
The Arab world is undergoing a renaissance in growth and development. But true progress can be achieved only when women in these nations are empowered with knowledge that will help them make life altering health choices. In most of the Middle East countries, reproductive health (RH) is a culturally sensitive issue that is not well discussed. As a result, adolescents do not have access to sufficient RH information, leading to misconceptions and lack of awareness.9 PCOS is a disorder affecting RH with far reaching effects on metabolism and mental health all through the lifespan of women. A key factor that limits PCOS treatment is that a very high percentage of individuals remain undiagnosed until the disease has progressed and warrants medication. Unhealthy lifestyle and poor awareness accelerate the early onset of the disorder. Early diagnosis and management can help many young women lead health lives and achieve normal pregnancy.
In this context, UAE is a country that has witnessed tremendous transformations in the past decades. The population of the country has risen to 9.7 million in 2019.22 However, Emiratis or local citizens constitute only 11–12% of the total populations. While the Government is aiming to balance the demographic mix between Emiratis and expatriates by 2021, a major deterrent is that the fertility rates (TFR) of women here have been decreasing. Emirati women are actively and efficiently playing effective roles in developing the society and building the country. As a result, more and more career-oriented women are delaying marriage and childbirth. Rising levels of PCOS have been reported in local media and this adds to the infertility burden. This study was undertaken to evaluate the awareness levels pertaining to reproductive health, PCOS, and lifestyle choices of young Emirati university students. Since early detection and management is key to alleviation of PCOS symptoms, the study also intended to generate awareness so that afflicted students could seek medical help.
Demography and Lifestyle
Of the participants, 66.3% belonged to the Emirate of Dubai, and the remaining population was from adjoining emirates. Dubai and Abu Dhabi are considered to be the hubs of employment in UAE. Since the University campus was based at Dubai, most participants were from the emirate. The majority (92%) of these students were unmarried, which is a far contrast from the scenario a few years ago. Emirati women are married early as per local tradition, but our data confirms the changing trend in society, as more local women seem to be delaying marriage.23,24 Years spent at university or their college experience did not seem to impact student awareness levels of female physiology or PCOS. Students are typically in the age range of 17–21 years at the university, with few beyond 21 years of age, as the Federal University is very supportive of student life, permitting breaks for pregnancy and other personal issues. Results indicate that age did not affect student awareness levels of RH or PCOS. However, nearly 66% of PCOS afflicted participants were in the 19–21 age group, and this was statistically significant. This is a reminder that such important basic information has to be imparted early on and reiterates the need for awareness campaigns for early detection and deterring progress of PCOS.
Most metabolic issues, including PCOS, are aggravated by poor lifestyle choices such as frequent consumption of fast food, juices, and low physical activity (PA). These increase risk factors such as obesity, CVD, and type 2 diabetes, and escalate severity of symptoms. Only 2% of participating students reported smoking, although smoking and Sheesha cafes are quite popular amongst college students in the Arab region.25 Low PA and high frequency of fast food consumption associated with high BMI lead to obesity, another risk factor associated with PCOS. Earlier studies had reported that females performed less PA compared to males and that the prevalence of PA among young population in UAE was very low.26–28 Of the Emirati female students in our study, 64.5% performed 5 hours or less of physical activity per week. The high incidence of childhood obesity and low levels of PA observed among children in the UAE have prompted local health bodies to recommend at least 60 minutes per day. However, this is not a guideline. Similar levels of PA (62%) in a mixed population of female UAE students was reported by another study.29 Other studies in the region such as in KSA and Qatar have reported 58% and 65% PA inactivity in students.27,30 The type of PA preferred also varies between regions and communities. Our data indicates that Emirati students preferred walking (77%) and shopping in malls (42.5%), whereas cycling (11.6%) and doing household chores (16.7%) were their least preference. Qatari students preferred going to the gym and walking, while another study conducted in a mixed population in Ajman in UAE indicated that students preferred brisk walking and doing household chores.30,31 The low PA levels were further supplemented with unhealthy eating choices.
Easy access to fast food with food delivery Apps, Instagram ratings, and the availability of a multitude of cuisines have made fast food popular among youth. A study of student’s food preferences revealed that nearly 12% consumed fast food 5–10 times a week and 85% at least 1–5 times a week. This is slightly higher than other studies that have reported 35% of UAE students consumed fast food at least once a week, 22.5% of Bahrani females consumed fast food 4 days per week, and 47.1% female KSA students reported eating fast food two or more times per week.29,32,33 Also, 39.4% of participants reported that they consumed one-to-three soft drinks per week and 3% more than five drinks a week. These results are indicative that these students had consciously selected an unhealthy lifestyle with high calorie food, supported by a low PA regime. This calls for more effective intervention strategies. Student and health groups in universities should ensure that health food choices, with accurate food labels, are provided in cafeterias and other outlets. Student events should focus on activities involving sport or physical activity rather than encouraging food trucks or other unhealthy, popular choices.
Reproductive Health Knowledge
A “puberty class” for girls is usually conducted in most schools across the world, to educate young girls about menstruation, pregnancy, and basic female physiology. This is essential as it equips them with knowledge of the working of their body, but more importantly also alerts them when something is amiss like irregular bleeding, appearance of dark patches of skin, or excessive body hair. It helps them seek timely medical guidance, thereby circumventing potential disorders. Students attending university are expected to know this information. However, sexual and reproductive health are considered to be socially sensitive issues in the Gulf regions.10 A study in Saudi Arabia reported that only 54.3% of female adolescents had correct knowledge about female reproductive organs. Reproductive health (RH) knowledge was unsatisfactory, as 66.3% of the participants had incorrect knowledge.10 Our study showed similar results as awareness levels of common terms such as ovary (54%), uterus (57%), hormones (48%), periods (80%) were lower than expected. The biology behind pregnancy (62.5%) and childbirth (48.7%) was also not clear to many students, but this could be attributed to the conservative attitude of the participants, with many being shy to divulge that they were aware about the process of childbirth and pregnancy. Concepts related to fertility such as importance of ovary for childbirth (58%), impact of hormonal fluctuations (44%) and presence of male hormones in females (22%) were not accurate. These students may not be capable of identifying issues related to RH and may thus delay detection of fertility-impacting disorders such as PCOS. An earlier study had reported that Emirati women perceived themselves as not having enough general health education and education related to marriage, childbearing, and child rearing.24 This calls for development of a reproductive health policy framework to address sexual and reproductive health issues among young women in Arab regions, specifically in UAE.
Awareness of PCOS, Symptoms, and Management
PCOS is being described as a major health issue, on the rise in UAE by many local media reports.20,21 However, a scientific exploration focusing on PCOS in Emirati women has been lacking. In general, there is a lack of awareness about this disease, as many women are hesitant to discuss intimate details associated with it. Only 38% of our study population had heard about PCOS before the survey, and this study was able to increase this awareness level to 57% by the end of the survey. Having completed the survey, the majority (91%) agreed that information on PCOS was important for girls of their age group and they would prefer to receive this knowledge through a healthcare center or family physician (62%). This observation highlights the important role played by these agencies (private clinics, primary healthcare centers, family physicians) in disseminating such vital health information. It is ideal that healthcare professionals counsel young patients and their parents about menstruation related disorders, future scope of manifestation, and their management through diet, exercise, and medication. They must also emphasize the importance of following a healthy lifestyle and its impact on reproductive health.
PCOS is linked to menstrual disorders like poly and oligomenorrhea (observed in 28% of Iranian women, 31% of Qatari women, and 19% of Indian adolescents) and other symptoms such as hirsutism, acne, and elevated androgen levels.34,35 Our participants also reported irregularities such as poly menorrhea (30.7%) and oligomenorrhea (3.5%), and there was a positive association of detection of PCOS and duration of menstrual cycle (P=0.02). This differs from other studies that have reported higher incidence of oligomenorrhea compared to polymenorrhea. Oligomenorrhea was found in 23% of women from the US, 14.6% of women from Greece, and 16% of students in Sharjah University, while polymenorrhea was observed in 4% of students from Sharjah University.36–38 In addition, 12.4% of participating students in our study also reported experiencing heavy/absent bleeding, indicating that they could be predisposed to PCOS. The incidence of hirsutism varies in different parts of the world based on diagnostic criteria used. While 24% of students in this study self-reported excessive hair growth at unusual locations, this was not verified clinically, but appears similar to other studies that have reported occurrence of hirsutism as 7% in Spanish women, 21% in Australian women, 31.7% in Qatari women, and 13% in Iranian women.34,35,39,40
Acne, another indicator of PCOS, was reported by 40.6% of our students, although this may be more of a cosmetic observation than a clinical one. Acne was present in 26% of Iranian women, 31% of Qatari women, and a prevalence rate of 50–80% was reported in Turkey and Palestine.34,35,41,42 While persistent occurrence of patches of thick dark skin was reported by 13.5% of students in our study, 23% of Indian adolescents had also reported the same in a previous study.43 These results indicated the presence of a highly PCOS predisposed cohort in our study population that was confirmed when 13.4% of students self-reported being detected with PCOS by a physician, with 3.5% also taking medication for the same. There was a strong correlation of PCOS occurrence with symptoms reported-absent/frequent periods (P=0), hirsutism (P=0), acne (P=0.02), and patches of thick skin (P=0.04). This finding strengthens the validity of our results as most data is self-reported and not tested clinically. This is the first report of PCOS prevalence in Emirati students in UAE and is evidence of its role in impacting fertility in this population. The reported prevalence of PCOS worldwide based on NIH, Rotterdam, and AES is between 7–12%, but this prevalence could vary based on geographical regions and race/ethnic factor.44,45 This is confirmed by the variable prevalence rates between 6% and 9% documented across different countries (UK, Spain, Greece, Australia, Asia, Qatar, Iran, Palestine). Of the participants in this study, 6% also reported having been diagnosed with high androgen levels, another clinical feature commonly associated with PCOS.35 Similarly, since diabetes Type 2 and PCOS are comorbidities, it was not surprising to find that 4.3% of participants were taking medication for hyperglycemia and 75% had some family history of diabetes, similar to another study that reported 76% family history of diabetes in Qatar.35 CVD and Diabetes are among the top chronic diseases in UAE, and our finding supports this trend. Having understood that symptoms highlighted in the survey are indicative of PCOS, 28% of students said they knew friends or family who could be having PCOS. A previous study had indicated that family history of PCOS could be a risk factor for PCOS, indicating that these students may be predisposed to PCOS themselves.46 The survey was successful in increasing awareness of participating students, and this was one of the intended goals of the study.
This study provides evidence about the growing prevalence of PCOS and its symptoms in the Emirati community. This is compounded by the lack of basic RH awareness and adoption of unhealthy lifestyle choices by these young women. Intervention at different levels may be required to tackle this issue. A culturally congruent policy should be created that accounts for provision of RH knowledge to female students of all curriculum in a comfortable, gender-specific environment. This should be supplemented with a comprehensive and integrated women-centered, healthcare setting with a focus on health promotion that addresses the diverse health needs of national women. Since most students preferred to receive healthcare information from medical practitioners, they should be trained to provide RH education and encourage increased parental involvement in the same. Primary health centers can be advised to provide counseling for young PCOS patients and their parents to make them aware of future health implications of the disease and how it can be managed early on. It may also be pertinent to consider implementing a mandatory PA program with credits in universities, to encourage students to incorporate more PA in their daily lives. Campus-wide dynamic women’s health campaigns, provision of healthy eating alternatives with accurate labeling, and inclusion of extracurricular activities supporting sport are strategies that may curtail the invasion of lifestyle metabolic disorders such as PCOS.
The main limitation of this study is the lack of clinical evidence to support the survey results. Ultrasound scan, hormonal evaluation, or FG scoring for hirsutism were not possible within the scope of this study, respecting the conservative values of the target population. Nevertheless, it may be noted that all symptoms correlated positively with PCOS diagnosis on statistical analysis, adding credibility to the self-reported data. Another limitation is that students provided approximate weight and height measurements by selecting a range. Hence, BMI calculations could not be performed. Moreover, the homogeneity of our sample population lends strength to our data pointing towards a pattern, as this is the first report of PCOS awareness and prevalence within young women in the Emirati community.
Conclusion
Emirati students self-reported a PCOS prevalence rate of 13% along with other symptoms such as menstrual irregularities, hirsutism, elevated androgens, and acne. The study provides insight into the many unhealthy lifestyle choices adopted by these students and their low awareness of RH and disorders such as PCOS. The study survey was successful in increasing PCOS awareness among students. These results may also be representative of young women of a similar age group in other rapidly developing Arab countries, and it is hoped that it will assist healthcare administrators in resource allocation and developing new health programs that are better suited for Emirati women in the rapidly developing country.
Ethics Approval
This study was reviewed and approved by the Research Ethics Committee (REC) of Zayed University (Application No- ZU16_038_F). Student identifiers were anonymized and completed surveys were stored in a locked cabinet.
Acknowledgments
This study was supported by a Start Up Grant provided by Zayed University. The author appreciates and acknowledges the efforts of Dr. Qasim Shboul towards statistical analysis of data.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Teede H, Deeks A, Moran L. Polycystic ovary syndrome: a complex condition with psychological, reproductive and metabolic manifestations that impacts on health across the lifespan. BMC Med. 2010;8(1):41. doi:10.1186/1741-7015-8-41
2. Bozdag G, Mumusoglu S, Zengin D, Karabulut E, Yildiz BO. The prevalence and phenotypic features of polycystic ovary syndrome: a systematic review and meta-analysis. Hum Reprod. 2016;31(12):2841–2855. doi:10.1093/humrep/dew218
3. Al-Shamsi S, Regmi D, Govender RD. Incidence of cardiovascular disease and its associated risk factors in at-risk men and women in the United Arab Emirates: a 9-year retrospective cohort study. BMC Cardiovasc Disord. 2019;19(1):148. doi:10.1186/s12872-019-1131-2
4. Strowitzki T, Capp E, von Eye Corleta H. The degree of cycle irregularity correlates with the grade of endocrine and metabolic disorders in PCOS patients. Eur J Obstet Gynecol Reprod Biol. 2010;149(2):178–181. doi:10.1016/j.ejogrb.2009.12.024
5. Himelein MJ, Thatcher SS. Polycystic ovary syndrome and mental health: a review. Obstet Gynecol Surv. 2006;61(11):723–732. doi:10.1097/01.ogx.0000243772.33357.84
6. Eshre TR, ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil Steril. 2004;81(1):19–25.
7. Azziz R, Carmina E, Dewailly D, et al. Criteria for defining polycystic ovary syndrome as a predominantly hyperandrogenic syndrome: an androgen excess society guideline. J Clin Endocrinol Metab. 2006;91(11):4237–4245. doi:10.1210/jc.2006-0178
8. Orio F, Palomba S. Reproductive endocrinology: new guidelines for the diagnosis and treatment of PCOS. Nat Rev Endocrinol. 2014;10(3):130. doi:10.1038/nrendo.2013.248
9. Alquaiz AM, Almuneef MA, Minhas HR. Knowledge, attitudes, and resources of sex education among female adolescents in public and private schools in Central Saudi Arabia. Saudi Med J. 2012;33(9):1001–1009.
10. Gaferi SM, Al-Harbi MF, Yakout SM, Soliman AT. Knowledge, attitude and practice related to reproductive health among female adolescents. J Nurs Educ Pract. 2018;8(8):53. doi:10.5430/jnep.v8n8p53
11. Azziz R, Dumesic DA, Goodarzi MO. Polycystic ovary syndrome: an ancient disorder? Fertil Steril. 2011;95(5):1544–1548. doi:10.1016/j.fertnstert.2010.09.032
12. Hijazi R, Zoubeidi T, Alfaki I, Al-Waqfi M, Harb NA. Study of the UAE higher education sector in light of Dubai’s strategic objectives. J Econ Admi Sci. 2008;24(1):68–81. doi:10.1108/10264116200800004
13. Abdulla F, Ridge N. Where are All the Men? Gender, Participation and Higher Education in the United Arab Emirates. Vol. 11. Dubai School of Government Working Paper Series; 2011.
14. Aswad NG, Vidican G, Samulewicz D. Creating a knowledge-based economy in the United Arab Emirates: realising the unfulfilled potential of women in the science, technology and engineering fields. Eur J Eng Educ. 2011;36(6):559–570. doi:10.1080/03043797.2011.624174
15. Blair I, Sharif AA. Population structure and the burden of disease in the United Arab Emirates. J Epidemiol Glob Health. 2012;2(2):61–71. doi:10.1016/j.jegh.2012.04.002
16. United Arab Emirates - country profile - 2019 [internet]. Indexmundi.com. 2020 [cited July 19, 2020]. Available from: https://www.indexmundi.com/united_arab_emirates/.
17. Times K. Emirati couples to get free fertility treatment in Dubai. [Internet]. 2017 [cited July 19, 2020]:1. Available from: https://www.khaleejtimes.com/news/uae-health/emirati-couples-to-get-free-fertility-treatment-in-dubai.
18. Shaer S. Challenges and opportunities for sustainable population growth in the Emirate of Dubai. 서울행정학회 학술대회 발표논문집. 2018;215–226.
19. Sharara E, Akik C, Ghattas H, Obermeyer CM. Physical inactivity, gender and culture in Arab countries: a systematic assessment of the literature. BMC Public Health. 2018;18(1):639.
20. Reporter S Polycystic ovarian syndrome on ‘staggering’ rise in UAE. Khaleej Times [Internet]. 2015 [cited July 19, 2020]:1. Available from: https://www.khaleejtimes.com/nation/uae-health/polycystic-ovarian-syndrome-on-staggering-rise-in-uae.
21. Hofmann-Werther D, WooCommerce B Polycystic Ovarian Syndrome (PCOS): a lifestyle-related problem? | Middle East Medical Portal [Internet] Middle East Medical Portal. 2020 [cited July 19, 2020]. Available from: https://www.middleeastmedicalportal.com/polycystic-ovarian-syndrome-pcos-a-lifestyle-related-problem/.
22. United Arab Emirates | Data [Internet]. Data.worldbank.org. 2020 [cited July 19, 2020]. Available from: https://data.worldbank.org/country/united-arab-emirates?view=chart.
23. Kulwicki A, Ballout S. People of Arab heritage. In: Transcultural Health Care: A Culturally Competent Approach. 2nd ed, Philadelphia, PA: F. A Davis, Vol. 3. 2003:113–128.
24. Winslow WW, Honein G. Bridges and barriers to health: her story—Emirati women’s health needs. Health Care Women Int. 2007;28(3):285–308. doi:10.1080/07399330601180206
25. Kheirallah KA, Alsulaiman JW, Al-Sakran Mohammad H, Alzyoud S, Veeranki SP, Ward KD. Waterpipe tobacco smoking among Arab youth; a cross-country study. Ethn Dis. 2016;26(1):107. doi:10.18865/ed.26.1.107
26. Buckworth J, Nigg C. Physical activity, exercise, and sedentary behavior in college students. J Am Coll Health. 2004;53(1):28–34. doi:10.3200/JACH.53.1.28-34
27. Al-Nuaim AA, Al-Nakeeb Y, Lyons M, et al. The prevalence of physical activity and sedentary behaviours relative to obesity among adolescents from Al-Ahsa, Saudi Arabia: rural versus urban variations. J Nutr Metab. 2012;2012:1–9. doi:10.1155/2012/417589
28. Yammine K. The prevalence of physical activity among the young population of UAE: a meta-analysis. Perspect Public Health. 2017;137(5):275–280. doi:10.1177/1757913916675388
29. Kerkadi A. Evaluation of nutritional status of United Arab Emirates University female students. Emir J Food Agric. 2003;15(2):42–50. doi:10.9755/ejfa.v15i2.5005
30. Al-Nakeeb Y, Lyons M, Dodd LJ, Al-Nuaim A. An investigation into the lifestyle, health habits and risk factors of young adults. Int J Environ Res Public Health. 2015;12(4):4380–4394. doi:10.3390/ijerph120404380
31. Gomathi K, Shaafie I, Mummigatti K, Shahid S, Sreedharan J. Biochemical parameters in women with polycystic ovary syndrome in Ajman, UAE. Nepal J Obstet Gynecol. 2012;6(2):7–10. doi:10.3126/njog.v6i2.6748
32. Musaiger AO, Awadhalla MS, Al-Mannai M, AlSawad M, Asokan GV. Dietary habits and sedentary behaviors among health science university students in Bahrain. Int J Adolesc Med Health. 2017;29(2). doi:10.1515/ijamh-2015-0038
33. Al-Otaibi HH, Basuny AM. Fast food consumption associated with obesity/overweight risk among university female student in Saudi Arabia. Pak J Nutr. 2015;14(8):511. doi:10.3923/pjn.2015.511.516
34. Jalilian A, Kiani F, Sayehmiri F, Sayehmiri K, Khodaee Z, Akbari M. Prevalence of polycystic ovary syndrome and its associated complications in Iranian women: a meta-analysis. Iran J Reprod Med. 2015;13(10):591.
35. Sharif E, Rahman S, Zia Y, Rizk NM. The frequency of polycystic ovary syndrome in young reproductive females in Qatar. Int J Womens Health. 2017;9:1.
36. Knochenhauer ES, Key TJ, Kahsar-Miller M, Waggoner W, Boots LR, Azziz R. Prevalence of the polycystic ovary syndrome in unselected black and white women of the southeastern UnitedStates: a prospective study. J Clin Endocrinol Metab. 1998;83(9):3078–3082.
37. Diamanti-Kandarakis E, Kouli CR, Bergiele AT, et al. A survey of the polycystic ovary syndrome in the Greek island of Lesbos: hormonal and metabolic profile. JClinEndocrinolMetab. 1999;84:4006–4011.
38. Attlee A, Nusralla A, Eqbal R, Said H, Hashim M, Obaid RS. Polycystic ovary syndrome in university students: occurrence and associated factors. Int J Fertil Steril. 2014;8(3):261.
39. Asuncion M, Calvo RM, San Millan JL, Sancho J, Avila S, Escobar- Morreale HF. A prospective study of the prevalence of the polycystic ovary syndrome in unselected caucasian women from Spain. J Clin Endocrinol Metab. 2000;85(7):2434–2438.
40. Lowe P, Kovacs G, Howlett D. Incidence of polycystic ovaries and polycystic ovary syndrome amongst women in Melbourne, Australia. Aust N Z J Obstet Gynaecol. 2005;45(1):17–19. doi:10.1111/j.1479-828X.2005.00334.x
41. Chang WY, Knochenhauer ES, Bartolucci AA, Azziz R. Phenotypic spectrum of polycystic ovary syndrome: clinical and biochemical characterization of the three major clinical subgroups. Fertil Steril. 2005;83(6):1717–1723. doi:10.1016/j.fertnstert.2005.01.096
42. Musmar S, Afaneh A, Mo’alla H. Epidemiology of polycystic ovary syndrome: a cross sectional study of university students at An-Najah National university-Palestine. Reprod Biol Endocrinol. 2013;11(1):47. doi:10.1186/1477-7827-11-47
43. Balaji S, Amadi C, Prasad S, et al. Urban rural comparisons of polycystic ovary syndrome burden among adolescent girls in a hospital setting in India. Biomed Res Int. 2015;2015:1–10. doi:10.1155/2015/158951
44. Skiba MA, Islam RM, Bell RJ, Davis SR. Understanding variation in prevalence estimates of polycystic ovary syndrome: a systematic review and meta-analysis. Hum Reprod Update. 2018;24(6):694–709. doi:10.1093/humupd/dmy022
45. Wolf WM, Wattick RA, Kinkade ON, Olfert MD. Geographical prevalence of polycystic ovary syndrome as determined by region and race/ethnicity. Int J Environ Res Public Health. 2018;15(11):2589. doi:10.3390/ijerph15112589
46. Azziz R, Kashar-Miller MD. Family history as a risk factor for the polycystic ovary syndrome. J Pediatr Endocrinol Metab. 2000;13(suppl 5):1303–1306.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.