")
Back to Journals » Adolescent Health, Medicine and Therapeutics » Volume 11
Exploration of Barriers to the Uptake of Nutritional Services Among Adolescent Girls from the Rural Communities of Tigray Region, Northern Ethiopia: A Qualitative Study
Authors Kahsay A , Gebregziabher H , Hadush Z , Yemane D , Hailemariam A , Mulugeta A
Received 11 August 2020
Accepted for publication 16 September 2020
Published 22 October 2020 Volume 2020:11 Pages 157—171
DOI https://doi.org/10.2147/AHMT.S276459
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Alastair Sutcliffe
Amaha Kahsay,1 Hadush Gebregziabher,1 Znabu Hadush,2 Dejen Yemane,2 Abebe Hailemariam,3 Afework Mulugeta1
1Department of Nutrition and Dietetics, School of Public Health, College of Health Sciences, Mekelle University, Mekelle, Ethiopia; 2Department of Environmental Health and Behavioral Sciences, School of Public Health, College of Health Sciences, Mekelle University, Mekelle, Ethiopia; 3UNICEF Head Office, Addis Ababa, Ethiopia
Correspondence: Amaha Kahsay
Department of Nutrition and Dietetics, School of Public Health, College of Health Sciences, Mekelle University, PO Box: 1871, Ayder, Mekelle, Tigray, Ethiopia
Tel +251 920322629
Email [email protected]
Background: Adolescence is a time of tremendous physical growth and mental development, with high nutrient requirements. Ethiopia is among the countries with a high prevalence of nutritional deficiencies among the women of reproductive age group, whilst adolescent girls from rural areas suffered disproportionately. However, there is a dearth of evidence regarding the barriers that hinder adolescent girls to utilize the available nutritional services.
Purpose: The current study aimed to qualitatively explore the range of barriers for the uptake of nutritional interventions among adolescent girls in rural communities of Tigray, Northern Ethiopia.
Methods and Participants: We employed an explorative qualitative study among purposively selected adolescent girls and school teachers from rural districts of Tigray region. We conducted 11 focused group discussions with adolescent girls, 17 in-depth interviews (seven with teachers, seven with in-school adolescent girls, and three with out-of-school adolescent girls) using a semi-structured guide. Data was audio-taped, transcribed verbatim in local language, translated into English, and imported into ATLAS.ti version 7.5 qualitative data analysis software for analysis.
Results: Adolescents perceived that stunting, anemia, and thinness are among the main nutritional problems in their community. Food insecurity, limited nutrition awareness in the community, limited access to a water source, high workload, service provider’s little attention for adolescents’ nutrition, and food taboo have emerged as barriers for the uptake of adolescent girls’ nutritional interventions. Though limited in reach, available nutritional interventions include awareness creation, nutritional supplementation, and disease prevention.
Conclusion: Food insecurity poses a strong challenge to adolescent girls’ nutrition. As access to safe drinking water continues to be a considerable bottleneck for nutritional interventions, a multi-sectoral response to integrate water, sanitation, and hygiene (WASH) services is required. Bounded by food taboo, high burden of workload among the adolescent girls, women empowerment and nutritional status seem to be the unfinished agenda in resource limited settings such as the rural areas of Tigray region.
Keywords: adolescent girls, barriers, nutritional services, rural, Tigray, Ethiopia
Background
Adolescence, which refers to the age range 10–19 years, is the period of tremendous growth and development that begins at puberty and ends in early adulthood. About 20% of final adult height, 45% of increments in bone mass, and 50% of adult weight are attained in this period,1 which requires rapid tissue expansion with special nutrient requirements, including amino acids for growth of striated muscle, as well as calcium and vitamin D to accommodate bone growth.2,3 Today, 1.2 billion individuals are in the adolescent age group, whilst nine out of ten live in the developing world with a higher likelihood to face profound nutritional challenges in their process of growth and development.4
Considerable nutritional problems attributed to an inadequate diet continue to lead to a poor health status during adolescence and sizable development challenges in developing countries. Fewer than 2% of adolescents consume adequate amounts of all the food groups, and almost 20% of females and 7% of males do not consume an adequate number of portions of any of the food groups.5 The global prevalence of underweight (thinness) among adolescents is 8.4% for girls and 12.4% for boys, which indicates that prevalence has not declined much in the past three decades.6 Nevertheless, adolescents are often not aware of the potential health risks associated with poor habits and have not thought about making dietary changes.7 On the other side, global adolescent obesity rates for both males and females were reaching 6.5% and 4.7%, respectively,8 while the prevalence for both sexes rises up to 8% in Ethiopia.9
Back to the set of socio-cultural, economic, and gender related factors, previous studies from Ethiopia show that risk of malnutrition is higher among adolescents’ girls. In Ethiopia, 22% of women aged 15–49 years are thin (with BMI less than 18.5);9 whereas, 26.5% and 58.3% adolescents in Tigray are stunted and thin, respectively.1 A recent meta-analysis from Ethiopia also shows a high pooled prevalence of stunting (20.7%) and underweight (27.5%) among adolescent girls in Ethiopia,10 whereas a school based study shows high prevalence of thinness (29%).11 Moreover, adolescents from rural settings, higher family size, with unprotected water source for drinking and food insecure household are with greater odds of the nutritional problems.10,12 As literature depicts, nutritional outcomes of adolescents have been determined by several factors like adolescent pregnancy, advertisements, watching television during mealtime, socio-economic status of parents, gender disparity, activity-related health behavior, skipping a meal, and high consumption of sweets and soft drinks containing sugar and others.13–27 In this case, nutrition-related interventions to adolescents have been undergone mainly in developed nations in response of the aforementioned and other related factors; of which, relatively successful nutrition interventions are culturally appropriate and tailored educational programs,18,–22,–28–30 using school-based health and nutrition intervention,31,32 and lifestyle (nutrition education and physical activity) and nutrient supplementation interventions.33,34 However, in most developing countries, nutrition initiatives have been focusing on children and women, thus neglecting adolescents.35 Likewise, in Ethiopia there are community-based interventions mainly to prevent malnutrition in women and children; however, there is limited effort to address malnutrition in adolescents.36
Moreover, Tigray regional state of Ethiopia is among the regions with a higher prevalence of adolescent stunting and thinness, which are 26.5% and 58.3%, respectively.1 Cognizant to the fast growth during adolescence, girls are particularly vulnerable to malnutrition as an array of socio-cultural factors restrict their food consumption, for example, as literature shows there is an association between avoiding foods for cultural beliefs, which endangers the health status and leads to nutritional deficiencies like anemia.37–39 Despite the global and national initiatives to improve the health and wellbeing of adolescent girls, they are a near miss to many of the nutritional interventions as most of the interventions are concentrated on pregnant and lactating women (PLW) and children. Understanding the available nutritional services targeted for adolescent girls (if any) residing in resource limited settings and exploring the socio-cultural barriers for the services would be worthwhile to underpin evidence-based solution. Therefore, the current study aimed at exploring the barriers for the uptake of nutritional services among adolescent girls in resource limited settings of rural Tigray Region, Northern Ethiopia.
Methods and Participants
Study Setting
The study was conducted among adolescent girls from five districts (Ofla, Seharti Samre, Laelay Maychew, and Medebay Zana) of Tigray region, Northern Ethiopia. Data was collected from November 2017 through January 2018. The details of the methodology are described elsewhere.40
Study Design
A community and institution-based exploratory qualitative study was conducted to explore barriers for nutritional services among adolescent girls in rural communities of Tigray, Ethiopia.
Sampling and Participants
First, we purposively selected five Woredas (districts) from Tigray region (Table 1) based on the districts’ food security status, as published elsewhere;40 next we took two Villages/Kebelles (smallest administrative units) from each district to select our eligible study participants. That is, we went to the respective study sites of schools and villages; and we clearly communicated with the villages’ leaders and school directors about the purpose of our study by showing them the approval and permission letters we obtained. And they gave us permission to proceed on meeting our eligible study participants.
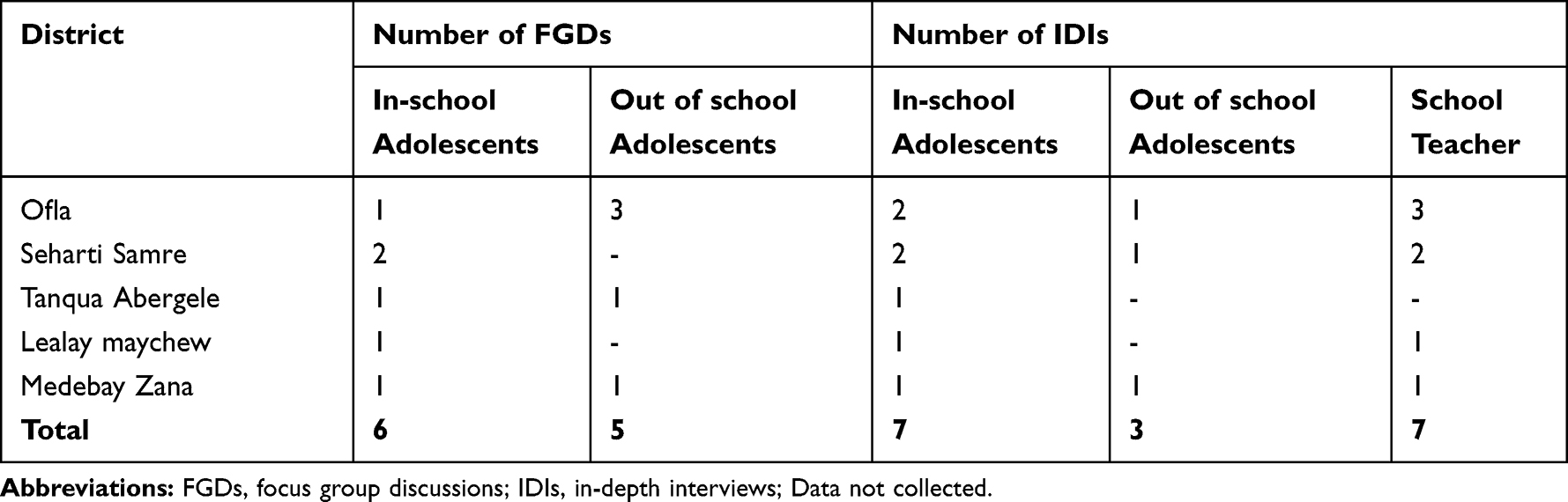 |
Table 1 Description of Groups Study Participants per District, in Rural Communities of Tigray Region, Ethiopia, 2018 |
Then after, together with the villages’ leaders, we purposively met the parents of the eligible out-of-school adolescents; and we further communicated about the purpose of our study in detail. Furthermore, the parents and adolescent girls themselves provided us their positive will about their respective daughters to be enrolled in the out-of-school adolescents’ interview. Following this, we underwent focus group discussion (FGD) and in-depth interview with purposively selected out-of-school-adolescent girls until we reached the saturation level of the qualitative data. As a result, we conducted a total of five FGDs with a total of 34 adolescent girls, which ranged from six to eight participants per each FGD, and three IDIs, that accounted for a total of 37 out-of-school adolescent girls.
In the same fashion, we purposively selected schools, and we communicated to the school directors, school teachers, and eligible school adolescent girls about the purpose of our study. And we agreed well to proceed on interviewing the eligible study participants. Finally, we undertook focus group discussion (FGD) and in-depth interviews (IDIs) with purposively selected in-school-adolescent girls until we reached the saturation level of the qualitative data; and we conducted a total of six focus group discussions (FGD) with 47 total participants ranging with six to ten participants per each FGD, and seven in-depth interviews (IDIs), which totaled 54 in-school adolescent girls, and seven in-depth interviews (IDIs) from school teachers. Overall, a total of 98 participants took part in our qualitative study (Tables 2 and 3).
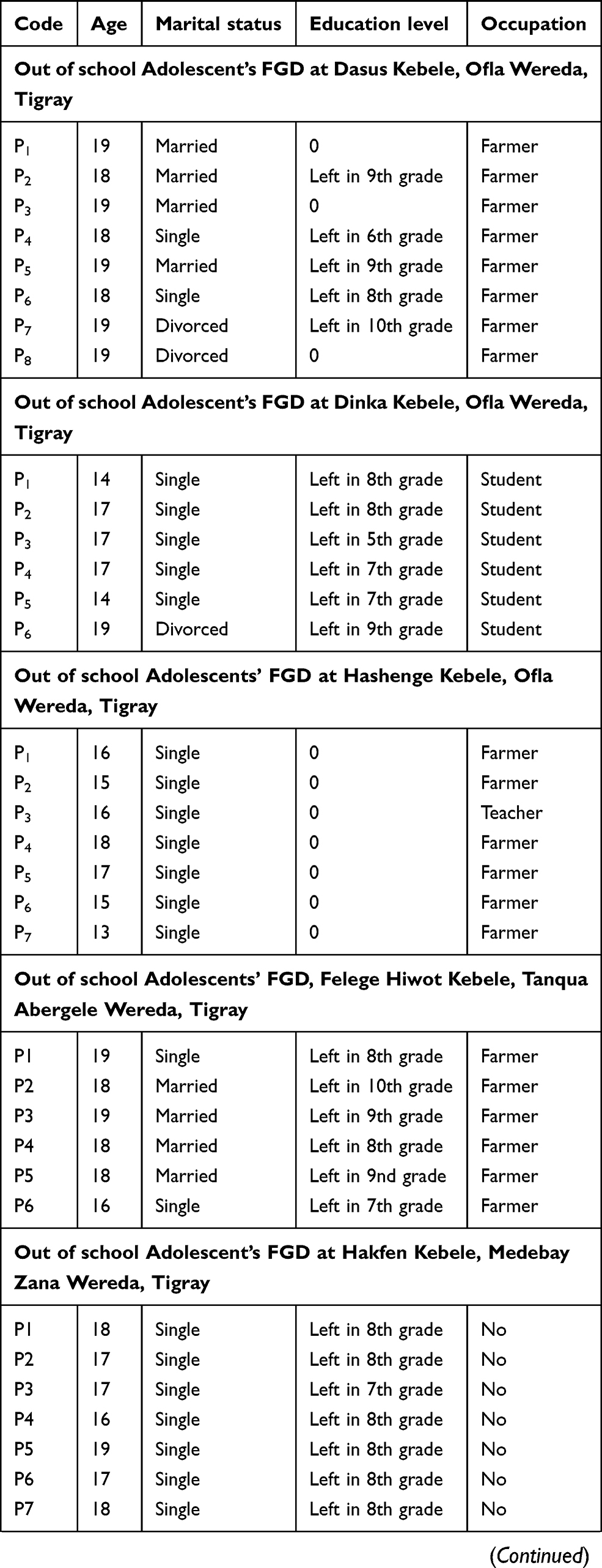 | 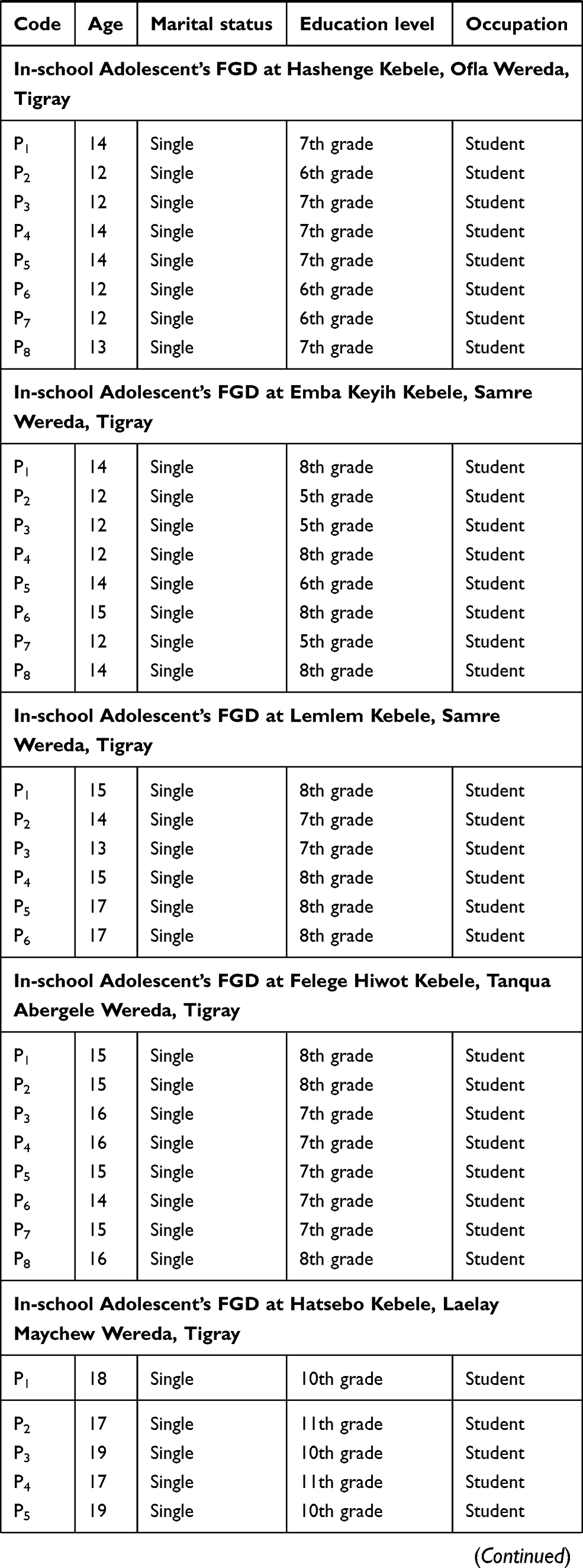 | 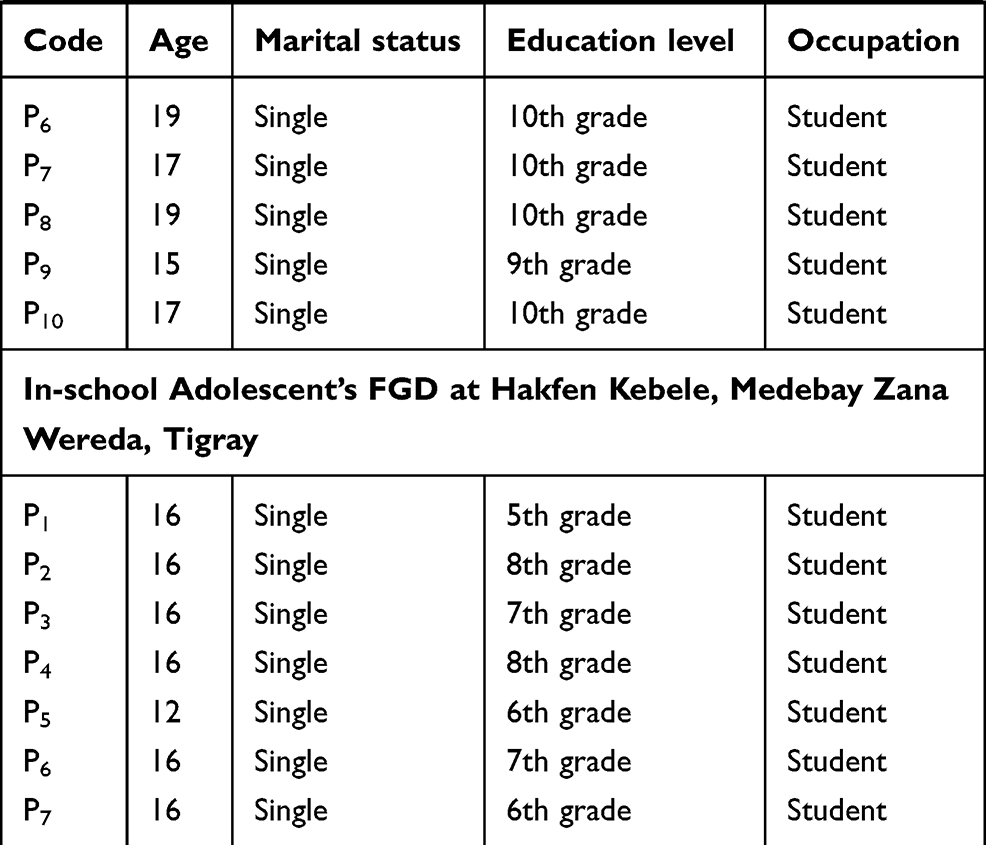 |
Table 2 Focused Group Discussions (FGDs) Participants for Barriers to Uptake Nutrition Services Among Adolescent Girls in Rural Communities of Tigray Region, Ethiopia, 2018 |
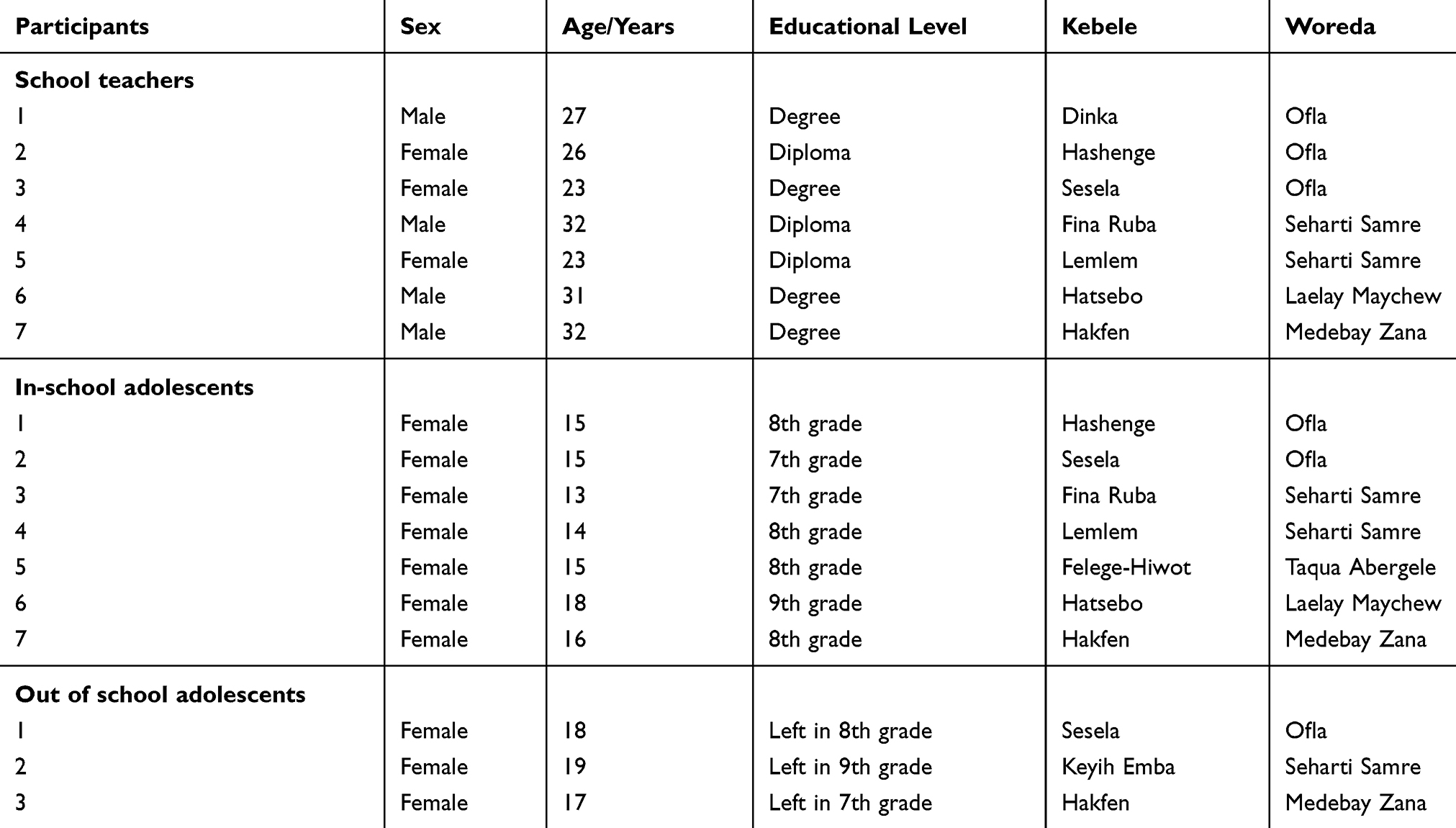 |
Table 3 In-Depth Interview (IDI) Participants for Barriers to Uptake Nutrition Services Among Adolescent Girls in Rural Communities of Tigray Region, Ethiopia, 2018 |
Data Collection Tools and Procedure
Semi-structured discussion and interview guides were developed by a team consisting of experts from multi-disciplinary areas, namely public health, agriculture, nutrition, health promotion, and food science. The guides covered existing nutrition platforms for nutrition services and barriers to the uptake of nutrition services for adolescent girls.
Then, we conducted the focus group discussions (FGDs) and in-depth interviews (IDIs) for in-school students and in-depth interviews (IDIs) for school teachers by preparing a setting where privacy is kept and recording is possible with little disturbance. Data were audio-taped, and transferred to a personal computer where access to nobody out of the investigators is denied. Audio-taped files were transcribed verbatim using the local language (Tigrigna) and translated to English. Each transcript was made ready for analysis.
Each collected data were transcribed before the next data was collected, which enabled the capture of emerging insights into the semi-structure guide. Investigators believed this helped to enhance the credibility and comprehensiveness of the insights. Peer debriefing was undertaken during the data collection and coding on a daily basis as a means of improving trustworthiness of the data. Moreover, triangulation data generated from FGDs and in-depth interviews were applied.
Data Availability Statements
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Data Analysis
Data collection and preliminary coding were conducted. Transcripts were imported into ATLAS.ti version 7.5 qualitative data analysis software. Two investigators openly coded the data independently and a daily based peer debriefing was held to assess and discuss similarities and differences in coding the transcripts. A third investigator was invited for resolution if disagreements were encountered between the coders. Similar codes were grouped into categories that link the codes. Then, categories were merged into themes in reference to the study objectives. Finally, we wrote the reports using descriptions and elaborative quotes.
Ethical Approval Procedure for the Study
Firstly, we obtained an approval letter from the Institutional Review Board (IRB) of Mekelle University (Reference number: ERC 1113/2017) and a permission letter to conduct the study from the Tigray Regional State Health Bureau. Secondly, we clearly communicated with the villages’ leaders and school directors about the purpose of our study. And they gave us their verbal informed consent to proceed on meeting our eligible study participants.
Basically, our study was non-invasive and with no risk of harm to the study participants; and it was handled using an interview-based approach. In line with this, there is evidence that supports school children and adolescents having an active involvement in deciding either to participate or refuse in such non-invasive research types.41,42 As a result, for the out-of-school adolescent girls’ interview, firstly, we communicated with the villages’ leaders and parents about the purpose of our study in detail; and they provided us their verbal informed assent to proceed with meeting the eligible adolescent girls. Next, we directly communicated with the adolescent girls about the aim of our study by raising the points that participating causes no harm to them or anyone, they have the right to withdraw at any step of the interview, to maintain the confidentiality all the information they provided us, and to omit their names and private characteristics in our resulting communication with any third-body. And we obtained their verbal approval to proceed on our interview with them. Similarly, we applied the same fashion to undergo the interview with the in-school-adolescents and school teachers. That is, after we obtained the verbal informed assent from the respective school directors for their authority and responsibility of their school adolescents;42 then next, we got a positive agreement of the school adolescent girls and a verbal informed consent from the school teachers to participate in the qualitative study.
Results
An average number of eight adolescent girls (ranging from 6 to 10) participated in each FGD. The age of participants in the focused group discussion and in-depth interviews ranged from 14–19 years. School teachers from primary schools were interviewed to complement information provided by the adolescent girls. Overall, a total of 98 participants took part in our qualitative study (Tables 2 and 3).
Perceived nutritional problems among adolescent girls, barriers to adolescent nutrition services, and possible available nutritional services for adolescent girls were explored in the current study, as depicted in detail below.
Perceived Nutritional Problems Among Adolescents Girls
Participants were asked to describe their perception regarding the nutrition related issues among adolescent girls in their community. Shortness, anemia, and thinness were the most frequently discussed nutritional problems with varieties of opinions and reflections. As an indication of the presence of stunting among adolescent girls, participants frequently mentioned that there are adolescent girls who have short stature in their locality. It is well mentioned by in-school adolescent girls:
There are adolescents their height is short as compared to their age […] [15 years, in-school, Ofla district].
Though the above opinion was predominantly reported, few adolescent girls also differently mentioned that short stature is not common in their locality. A FGD discussant adolescent girl from Hakfen village, reflected:
I have not seen stunted adolescents in this community up to date. […]. No adolescent is admitted due to malnutrition. I never encounter such case. [14 years, out of school girl]
Regarding the presence of stunting, some others also reported that the possibility of finding a short adolescent girl for age in the locality is becoming less nowadays, as dietary habits are improving. This opinion is captured in the following quotes:
When we see in adolescents, though most of them are ok, there are some that are short or small-sized. Generally speaking, it is good from the earlier times in terms of nutrition and others issues in nowadays. The situation is changed nowadays. […] However, the presence of thin and short adolescents currently may shows that there is an incidence of the problem. [17 years old, completed 8th grade, out school FGD discussant]
A school teacher also voiced a similar reflection:
As compare to the previous one, the risk of exposure to malnutrition is low now. The feeding habit of the community is extremely changed now. (23 years aged, Samre woreda)
Participants also specified their perception regarding the causes of shortness (stunting) as the result of; 1) Heredity/genetic factors from parents; 2) Mother’s inadequate feeding; 3) Adolescent girls’ inadequate feeding; 4) Disease or Illness; and 5) Carrying heavy objects in reference to their age. Extensive, strong, and repeated reflections that favor and disfavor hereditary/genetic and dietary reasons were repeatedly raised as perceived reasons of stunting. Participants reflected that if either the mother or the father or both are short stature, they may give offspring with short stature. In this view, participants considered shortness of the girls as natural, hence, acceptable and normal status. Opinions that favor dietary reasons to hereditary/genetic reasons argued that diet is the foundation of health in reference to the nutrient demanding age of adolescence (Table 4).
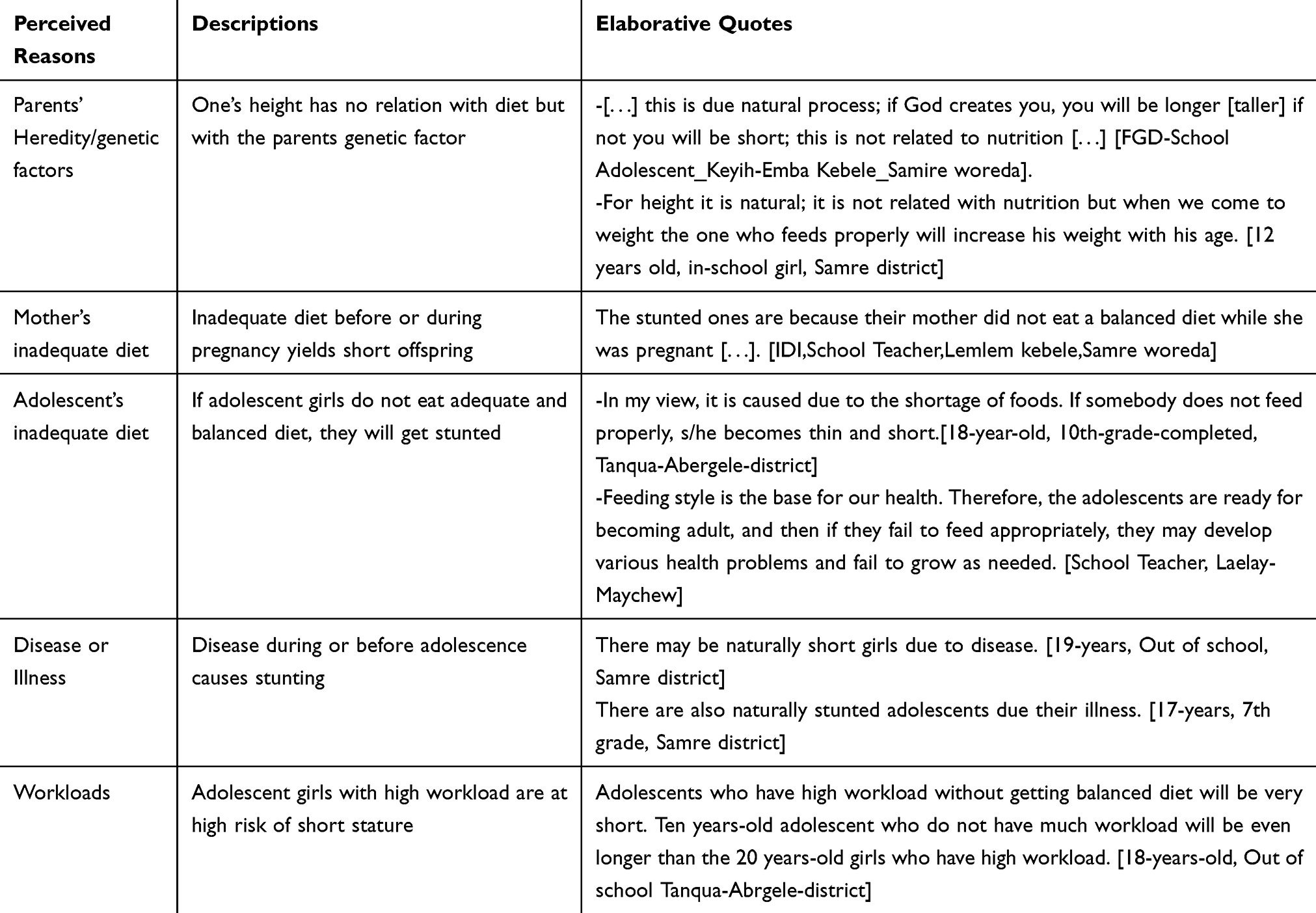 |
Table 4 Perceived Reasons and Elaborative Quotes of Stunting Among Adolescent Girls, in Rural Communities of Tigray Region, Ethiopia, 2018 |
Participants reported that anemia is evident in their locality, being adolescent girls at higher risk next to pregnant women. Although school girls claimed for irregularity and interruption, school-based folic acid supplementation was provided as nutritional intervention to prevent anemia. The following quote captured existence of anemia among adolescents,
[…] anemia is common among us (adolescents) and pregnant women […]. [14 years, in-School FGD discussant, Samire woreda]
Differently, an out-school girl and a school teacher in Medebay zana district reported that anemia is not a concern of adolescents girls.
I do not think there are adolescents with Anemia. There is education and they are eating balance diet. Therefore, there is no Anemia. [16 years, out-school, Medebay Zana district]
Before pregnancy, anemia is not that much so it is not a problem, but it becomes a problem during pregnancy [32 years old, School teacher, Medebay Zana district].
Participants repeatedly mentioned that poor balanced diet, high workload, and food shortage are the main risk factors for anemia among adolescent girls. They specified that missing breakfast, long working hours under the sun, not eating “blood substituting” vegetables including carrot and red potato, as well as cereals yields to anemia. The following quotes elaborated participants’ perceived causes of anemia,
Anemia is caused by not eating a balanced diet. [16 years-in-School, Medebay Zana woreda]
Anemia is caused as the result of high workload and poor feeding among the communities. [18 years, out-school FGD participant, Tanqua Abergele district]
Next to stunting and anemia, participants also specified the presence of thinness among adolescent girls, while only a few participants raised the presence of vitamin deficiencies and overweight in their locality among girls. Unlike in the case of stunting, almost all participants except one agreed that thinness is the result of inadequate diet. According to the participants’ opinion, adolescent girls from households with food shortages are likely to be thin. An in-school girl captured it as follows.
There are adolescents who are short compared to their age. This could be due to their nature because sometimes there are short adolescents even if they are well nourished. However, those adolescents who are very thin are due to malnutrition. [15 years, 8th grade, Ofla district]
Similarly, a FGD discussant in Samre district also uncovered this reflection.
After good feeding, people can increase their weight but not their height. [15 years, 8th grade, Samre district]
Dissimilar to the others, a FGD discussant in Medebay Zana reported that heredity is responsible for thinness as it is for shortness.
There are some who are thin and there are also some who are fat. There can be thin due to heredity and there are also hereditary for shortness. [18 years, out-school, Medebay Zana]
Participants agreed that overweight is less common and if any it is often due to heredity. Few also mentioned that overweight is less likely among adolescent girls who reside in rural areas because they lose energy in domestic work.
Barriers to Adolescent Nutrition Services
Food insecurity, limited nutrition awareness in the community, limited access to water, high workload, service providers’ little attention for adolescents’ nutrition, and food taboo among adolescent girls emerged as sub-theme barriers for nutritional services among adolescent girls (Table 5), as narrated in detail below.
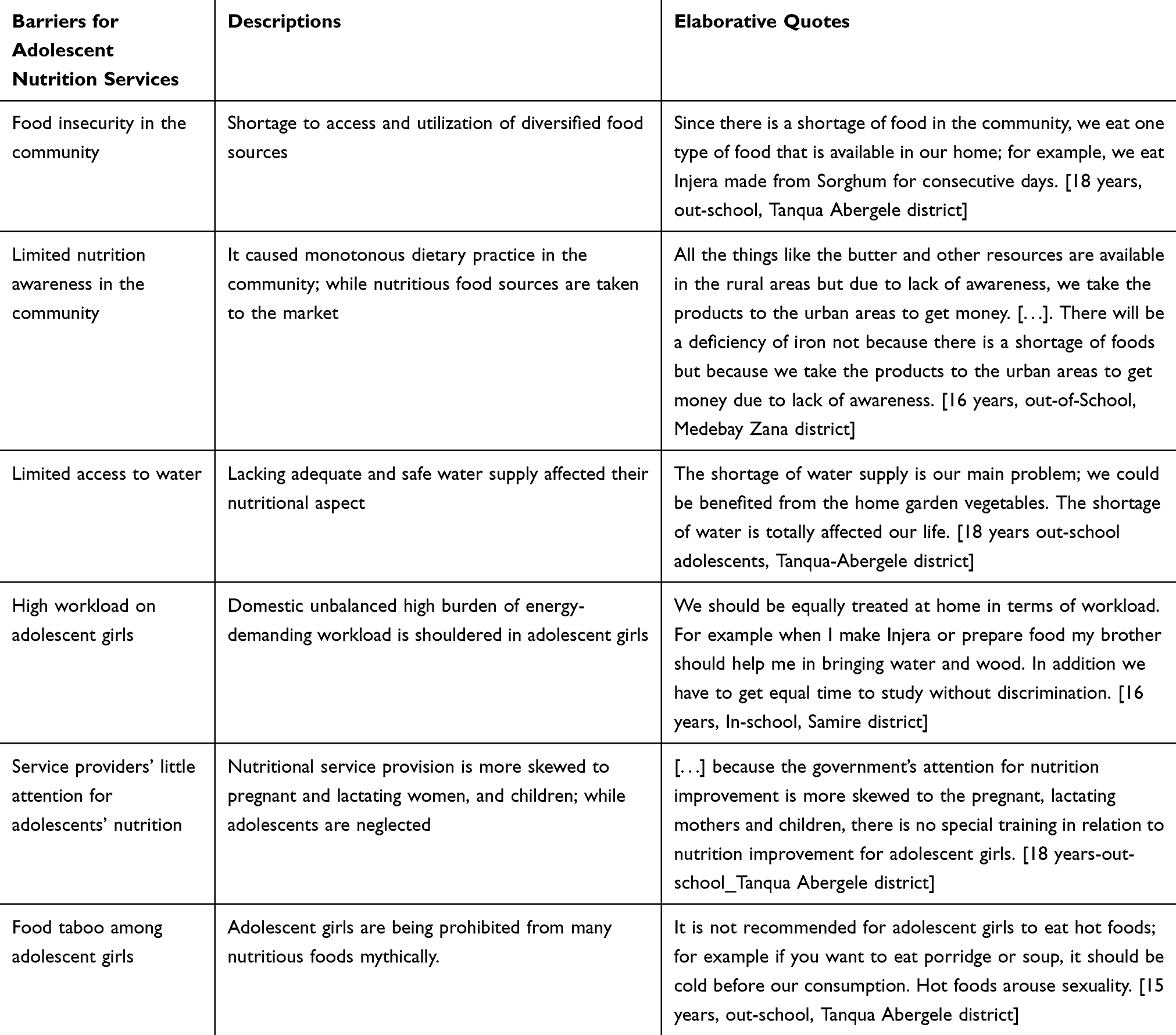 |
Table 5 Barriers for Adolescent Nutrition Services Among Adolescent Girls, in Rural Communities of Tigray Region, Ethiopia, 2018 |
Food Insecurity
Participants repeatedly mentioned that food insecurity in the community where adolescent girls live is a predominate barrier to nutritional interventions for adolescent girls. The key contributing factors specified for the food insecurity were 1) Drought and lack of rainfall; 2) Insufficient agricultural productivity; 3) Limited diversification of the agricultural products; 4) No land owned; 5) Extended family size; and 6) Households’ extravagance.
The shortage to food access in the community being attributed to an absence of rainfall was strongly discussed. FGD discussants reporting from Tanqua Abergele stated the presence of drought for the 3 consecutive years preceding the study. They stated it as,
This year, there was no rainfall and all crops were remained dry in this community; the livestock production is also affected by the drought due to the shortage of water. [18 years, out of school FGD participant, Tanqua Abergele district]
Insufficient agricultural productivity was evident. The pattern of participants response to the reasons for insufficient productivity were women’s low agricultural productivity, husband loss due to divorce or death, husband getting older, few men in the household who were able to plough, giving land to contract and crop pests. Consequently, a food shortage was reported as a common phenomenon in September and October of a year, while it could be sometimes extended from May to December. This time adolescent girls suffer from this shortage because they would be neglected to get attention. The following quotes captured this reflection,
Food shortage is common in September and October. And the problem may be extended up to December in the community until they collect their harvest. This time girls may face shortage of food. [23 years, school teacher, Samre district]
For example if there is shortage of food during summer the mother gives priority for their children, what can she do? Nothing! Because she need to feed do not her children first […]. If there is shortage of food in the family, obviously we will be affected by malnutrition. [14-years, in-school FGD participant, Samre district]
As it is said, shortage of food occurred from May–September. The produced food is may be used up to May but it would be run out starting from May. Then shortage of food happened. [16 years old, in-school, Tanqua Abergele district]
Participants also mentioned that the limited diversification of the agricultural products hinders to food diversification to realize the intention to use diversified food, out-of-school FGD discussants in Tanqua Abergele also reached a consensus that they often eat one type of diet that is available.
Since there is a shortage of food in the community, we eat one type of food that is available in our home; for example, we eat Injera made from Sorghum for consecutive days. [18 years, out-school FGD participant, Tanqua Abergele district]
A school teacher also reflected that advice on diversification is not realized because of limited products.
There are no diverse fruits and vegetables. Actually there is tomato but the other vegetable such as lettuce, Swiss chard and others are not available in the areas because the area is lowland in which diverse vegetable does not exist. [23 years, school teacher, Ofla district]
Participants also raised that households’ extravagance on marriage and other ceremonies yields to food insecurity, hence aggravates nutritional problems on household members including adolescent girls. Food insecurity was also reported in households with no man to plough themselves and those who do not own land,
It is to mean those who cannot farm their land by themselves because of death of their father are suffering from shortage of food. So that they give the land to other farmer for sharing the crop produced equally therefore the amount of crop the family gets is very minimal […]. [31 year old, school teacher, Lalay Maychew]
There is shortage of foods those that do not have farm lands such as youngsters that have recently established a household. [17 years, out school FGD participant, Medebay Zana]
As is expected, adolescent girls from households of larger family size are at higher risk of food insecurity due to high food consumption. FGD discussants uncovered this opinion,
In rural, women or mother may give 6 to 7 children this may lead to a shortage of food among our family and the mother and adolescents give priority to the young one. [15 years, in-school FGD discussant, Samire district]
Moreover, participants revealed that adolescent girls from food insecurity households are especially vulnerable for nutritional deficiencies because 1) women and adolescent girls would be left at home with insufficient food while the husband and boys could be displaced to other areas for work, 2) adolescent girls are given less priorities in the case of food shortages; 3) high workload in domestic activities; 4) women in general including adolescent girls are wrongly considered to be able to stay longer with no or limited food. The following quotes from an in-school FGD discussant in Samire woreda captured these opinions,
The female adolescents are more suffered from the food shortage because they have more workload at home than the male adolescent. The males can generate income by going out to the town but we can’t do so. [19 years, in-school FGD participant, Samre district]
Females are always at home whether they get or not and they have no option. On the other hand, males can work outside and at least they can eat for themselves. Thus, females suffer most from nutritional problems. If they get [food] they would eat; otherwise, they sleep with empty stomach. [16 years, in-school FGD participant, Tanqua Abergele district]
With the increasing burden of high workload for domestic activities, out-school adolescents girls were specified as the most vulnerable to nutritional deficiencies compared to in-school adolescent girls. This is strongly explained as:
The difference between the one that is out-school girl will only focus on the activities of food preparation for the family and no one considered her what she is eating and drinking. [Out-of-School-adolescent, FGD participant, Hakfen kebele, Medebay Zana]
Limited Nutrition Awareness in the Community
Participants also revealed that poor community’s awareness, such as of mono-diet practice, selling nutritious foods to markets, gender, and discrimination in feeding contributes to adolescent girls’ poor nutritional status. Rural residents take their animal production, high price crops, and cereals to market to buy other consumables, which makes members of the family including the adolescents at risk of under-nutrition. The following quote from a FGD participant captured this view;
All the things like the butter and other resources are available in the rural areas but due to lack of awareness, we take the products to the urban areas to get money. […]. There will be a deficiency of iron not because there is a shortage of foods but because we take the products to the urban areas to get money due to lack of awareness. [16 years, out-of-School, Medebay Zana district]
Participants also reported that there is a tendency to prioritize food for males over females in the household. Some of the participants reasoned that this is because males are involved in more energy demanding labor work than females. A FGD discussant from Samire stated this issue as,
[…] what is happening is that they have the perception to say let the girls stay and provide food to the boys. In case enough food is not ready, mothers provide the available food to their husband. [31 years, School teacher, Lalay-Maychew district]
An in-school girl FGD participant opposed the feeding discrimination as:
There should not be the practice of giving the “good” food types for boys/men and the remained for girls. We have to eat equally with our brothers. There should not be any feeding disparities like you have to eat this one, boys should to eat that one. [14 years, in-school, Ofla district]
Limited Access to Water
Lack of access to adequate and safe water was repeatedly mentioned as a barrier for adolescent nutritional services. Many respondents witnessed that adolescent girls need to walk around 3 hours on foot to fetch water, as a FGD-discussant raised:
[…] The main problem in in our community is no water availability. It takes us three hours to fetch water. [.]. We need to spend much time to fetch water. Then, we feel tired and we miss the class. [15 years, in-school FGD participant Tanqua Abergelle district]
Moreover to this, participants claimed that lack of water hindered them from practicing backyard gardening to produce nutritious foods like vegetables:
The shortage of water supply is our main problem; we could be benefited from the home garden vegetables. The shortage of water is totally affected our life. [18 years, out-school FGD participant, Tankua-Abergele district]
High Workload
Participants reported that there is a high burden of energy demanding workload to adolescent girls in domestic activities including fetching water. Adolescent girls are prone for nutritional deficiency because of frequent miss of breakfast. Thus, as a consequence they are unable to concentrate in class education, miss classes, concentrate less in class, and unable to perform well in academic results. Hence, a participant recommended that there has to be present equal sharing of labor at home.
We should be equally treated at home in terms of workload. For example when I make Injera or prepare food my brother should help me in bringing water and wood. In addition we have to get equal time to study without discrimination. [16 years, in-school, Samire district]
Summary and further detailed quotes on barriers to nutritional services among adolescent girls in rural communities are provided in Table 5.
Service Providers’ Little Attention for Adolescents’ Nutrition
Participants claimed that most nutritional interventions including counseling, awareness creation activities, nutritional supplementations, food aids, and supports are focused on pregnant, lactating women, and children. This is captured in a FGD discussion of:
[…] because the government’s attention for nutrition improvement is more skewed to the pregnant, lactating mothers and children, there is no special training in relation to nutrition improvement for adolescent girls. [18 years-out-school, FGD discussant, Tankua Abergele district]
As a result, the participants assured that nutrition related awareness creation and life skill trainings to adolescents are very limited, as supported by:
There is lack of sufficient awareness creation, and education for adolescents. There is no that much organized work to change the awareness of the adolescents. However, the education is only given by schools that may not be enough. [31 years, School Teacher, Laylay-Maychew district]
Food Taboo Among Adolescent Girls
Hot foods (hot Injera with hot stew, hot porridge, tea, and milk, hot sauces and soup) were the most frequently mentioned categories of food as tabooed for adolescent girls. Besides, cooked liver, milk, animal testicles (sheep and goat), and Ocholoni (peanut) were reported as taboo to be eaten by adolescents girls. The participants uncovered the reasons for the foods to be considered as tabooed for adolescent girls. The most frequently mentioned reason is that hot foods are relatively high in energy, which is perceived to facilitate early physical maturity, and arouse early sexual initiation. Meat, egg, and milk are also prohibited for adolescent girls for similar reasons. An FGD discussant explained it:
It is not recommended for adolescent girls to not eat heated foods; for example if you want to eat porridge or soup, it should be refrigerated before our consumption. Hot foods arouse sexuality. [15 years, out-school FGD discussant, Tankua Abergele district]
Some participants also reflected that consumption of hot foods is believed to be associated with early initiation of menses and increasing its volume. An FGD discussant in Hatsebo Kebelle captured this concept as:
Yes, our mother don’t allow us to drink hot like tea and soup since it facilitate the initiation of menses and increases the volume of the menses. But when I think of it is not true it doesn’t has any effect. [16 years, in-school, Laelay Maychew district]
Few participants also associated adolescent girls’ frequent consumption of milk with probability of having beard (facial hair) like men. Besides eating egg causes difficulties (womb narrowing) during child delivery. [14 years, in-school, Tankua-Abregele district]
The pattern analysis of adherence to food taboos showed that among adolescent girls these aregetting less strict with time. An FGD from Hatsebo captured this opinion, the adolescent girls’ disobedience to the taboo,
Previously, foods like meat, egg and milk […] were not allowed to us and our parents informed us about this issue, but now we can eat them. [19 years, in-school, Laelay-Maychew district]
Available Nutritional Services on Adolescent Girls
Awareness Creation
Few participants reported that there are interventions aimed to create awareness regarding a balanced diet and food diversification, iodized salt, andfolic acid to prevent anemia. Participants claimed that there is no nutritional screening among adolescent girls whereas it is done for children, pregnant, and lactating women. An FGD discussant at Felege-Hiwot, reported,
No, the nutrition screening is occurred among pregnant and lactating mothers and children; but no in adolescent girls. Accordingly, supplementations such as plump sup and plump nut are provided for pregnant and lactating mothers. But there is no any measurement and food supply to the adolescent girls. [18 years, out-school, Tankua-Abergele district]
Nutritional Supplementation
School-based nutritional supplementation were the commonly reported nutritional interventions such as iron folic acid, mass drug administration for trachoma, Vitamin A supplementation, deworming, and most of the nutritional interventions provided. However, the interventions were inconsistently reported across the schools. FGD discussants from Hashenege Kebele reported that iron and folic acid supplementation is provided only to pregnant women, not for adolescents, while the discussants from Hatsebo kebele mentioned that the services have been provided but are currently terminated. Despite the distribution of iodized salt, FGD discussants also raised that they do have doubt regarding its appropriate use.
Preventing Disease
On the other hand, participants frequently reported awareness creation interventions on preventing communicable diseases, mainly water borne diseases, malaria, menstrual hygiene contraceptive use to preventing pregnancy, and sexually transmitted diseases like HIV/AIDS. Optimizing the use Insecticide Treated bed Net to prevent mosquito bite was the most frequently reported intervention.
They give us [ITN] every year in the month of in May and sometimes in September. At least they give us three ITN for one household per year to prevent mosquito bite. [19 years, in-school, Lalay Maychew district]
However, participants mentioned that a long way is remains to ensure effective use of the ITN as they use the net for other purposes than the intended ones, like to carry straw, cover straw, and some of the women use it to fasten their waist (as a belt). Awareness creation activities aimed to prevent water borne diseases was also raised,
We get support and health workers regarding safe drinking water. They advised us to boil and drink the water or to drink from tap water. (14 years, in-school Tankua Abergele)
Discussion
Our study indicated that food insecurity among adolescents of the rural community of Tigray was associated with limited access and availability of food due to shortages and seasonal variation of rainfall, and lack of farmland owning by youths. Parallel to this, almost all of the participants in our study claimed that stunting and anemia were among the commonest nutritional problems in pregnant women and adolescents. These nutritional problems may have a relationship with the food insecurity in the community, as it was similarly indicated by a study in China that food insecurity is associated with poor diet quality and unfavorable health outcomes, and significantly associated with malnutrition among 6–14 years old Chinese children.10 Besides, it is indicated that food insecurity is a pervasive problem among adolescents from low-income communities and is associated with lower developmental assets.11 Consequently, it is indicated that household food insecurity has a strong linkage with adolescent school absenteeism.12 Also, food insecure adolescents have a higher conditional probability of clinically significant psychological distress. Similarly, a cross-sectional, school-based data from the Global School-based Student Health Survey from 44 countries showed that food insecurity (hunger) is a global problem and is associated with suicide attempts.37 This could be a clue that giving attention by all concerned bodies to work at addressing food security of adolescents could be the way to secure a healthy bridge between childhood and adulthood of our generation.
One of the sustainable development goals for the 2030 agenda is mentioned to be that ensuring good nutrition requires access to safe water and sanitation;38 however, as very repeatedly claimed by the respondents in our study, access to adequate and safe water is a devastating problem. Moreover, they stated that even the water they fetch, traveling for multiple hours, ois not safe and adequate to meet the need for their domestic consumption. As a consequence, it is important to bear in mind that lack of access to clean water and sanitation causes diarrhea and infectious diseases that interfere with the body´s ability to absorb nutrients. This is because unsafe water and food create a vicious cycle of diarrhea and malnutrition, threatening the nutritional status of the most vulnerable.38 And yet, the task of fetching water for households falls disproportionately to women and girls, especially in rural areas;39,43 consistent with this fact, in our study we found that adolescent girls are almost entirely involved in providing water to their households from very distant places (takeing up to 3 hours for a single trip). Most of the participants in our study claimed that stunting and anemia are common among pregnant women and adolescent girls, though they projected different notions as causes for these burdens of nutritional problems in the community. Nevertheless, it may have a relationship to the vicious cycle of inadequate and unsafe water and food, as indicated by a cross-sectional study in India which depicted that Water, Sanitation, and Hygiene (WASH) practices may affect the growth and nutritional status among adolescents.44 Besides, our study indicates that access to water for gardening is also almost absent, which hindered them from producing and consuming nutritious foods like vegetables. In support of the interest of taking nutritious foods like vegetables by the respondents of our study, a cross-sectional evaluation from the US showed that gardening experience is positively associated with F/V intake among college students.45
Furthermore, in our study almost all the participants claimed that fetching water from distant places is one indication of their heavy workload, as also supported by Saldanha et al,46 that sucks their energy; lets them feel hunger, leading to less concentration at their academic performances. This is because water is heavy to carry.43 Hence, their caloric expenditures, particularly during droughts, and other measures that affect health and quality-of-life, must be considered.47 This finding may give a clue for the need of nutritional interventions focusing on multi-sectoral response, which may better address the demand for safe drinking water.
Despite the trend that adolescents’ adherence to food taboos is getting weaker with time, avoiding eating some available foods in resource limited settings for reasons related to food taboos could significantly increase the risk of under-nutrition. Similar studies which also recognized the effect of food taboos with nutritional problems,48–50 from a qualitative study explores that parental influence on eating behaviors in the perspective of the family’s culture or religions as well as their habit, play an important role in influencing food choice of adolescents51 In settings where food shortages are evident, the presence of culturally backed food taboos among adolescent girls implies that the relatively higher nutritional deficiency can persist.
Conclusion
A range of barriers hinder adolescent girls to access nutritional services. Food insecurity poses a strong challenge to adolescent girls’ nutrition services. As access to safe drinking water continues to be a considerable bottleneck for nutritional services, a multi-sectoral response to integrate water sanitation and hygiene (WASH) services is required. Bounded by food taboo, high burden of workload and workloads among the adolescent girls, women empowerment and nutritional status seems to be the unfinished agenda in resource limited settings such as that of rural areas of Ethiopia.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval and Consent to Participate
As clearly indicated in the methods section, we obtained ethical approval from the Institutional Review Board (IRB) of Mekelle University (Reference number: ERC 1113/2017) and permission to conduct the study from the Tigray Regional State Health Bureau. Then after, for the out-of-school adolescent girls, we received verbal informed assent from their parents and the respective study villages’ leaders along with the positive will of the adolescent girls to participate in the study. In the same fashion, for the in-school-adolescent girls, we got verbal informed assent from their respective school directors along with their positive will to participate. Furthermore, we received verbal informed consent from the school teachers who participated in our qualitative study. And we utterly assured that all the responses in this study are anonymized during publication.
Consent for Publication
Not applied for this study.
Acknowledgment
Our gratitude goes to the study participants for their consent to participate and provision of invaluable information. We are also grateful to the UNICEF and Tigray Regional Health Bureau for funding this study project.
Author Contributions
All the authors (AK, HG, ZH, DY, AH, and AM) made a significant contribution to this research work, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Funding
This research work is funded by the UNICEF and Tigray Regional Health Bureau. But, these organizations had no role in the design, analysis, or writing of this article.
Disclosure
The authors declare that they have no conflict of interest.
References
1. Mulugeta A, Hagos F, Stoecker B, et al. Nutritional status of adolescent girls from rural communities of Tigray, Northern Ethiopia. Ethiopian J Health Development. 2009;23:1. doi:10.4314/ejhd.v23i1.44831
2. Das JK, Salam RA, Thornburg KL, et al. Nutrition in adolescents: physiology, metabolism, and nutritional needs. Ann N Y Acad Sci. 2017;1393(1):21–33. doi:10.1111/nyas.13330
3. Gebremariam H, Seid O, Assefa H. Assessment of nutritional status and associated factors among school going adolescents of Mekelle City, Northern Ethiopia. Int J Food Sci Nutr. 2015;4:118–124. doi:10.11648/j.ijnfs.20150401.26
4. UNICEF Staff. The State of the World’s Children 2011-Executive Summary: Adolescence an Age of Opportunity. Unicef; 2011.
5. DiMeglio G. Nutrition in adolescence. Pediatr Rev. 2000;21:32–38. doi:10.1542/pir.21-1-32
6. NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in children’s and adolescents’ body mass index, underweight, overweight and obesity, in comparison with adults, from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies with 128· 9 million participants. Lancet. 2017;390(10113):2627–2642.
7. Singla P, Sachdeva R, Kochhar A. Impact of nutrition counseling on consumption pattern of junk foods and knowledge, attitudes and practices among adolescent girls of working mothers. J Human Ecol. 2012;39(3):221–227. doi:10.1080/09709274.2012.11906514
8. Development Initiatives, 2018. 2018 Global Nutrition Report: shining a light to spur action on nutrition. Bristol, UK: Development Initiatives.
9. Central statistical agency (CSA) [Ethiopia] and ICF. Ethiopia Demographic and Health Survey. Ethiopia and Calverton, Maryland, USA: Addis Ababa; 2016.
10. Shen X, Gao X, Tang W, Mao X, Huang J, Cai W. Food insecurity and malnutrition in Chinese elementary school students. British J Nutrition. 2015;114(6):952–958. doi:10.1017/S0007114515002676
11. Shtasel-Gottlieb Z, Palakshappa D, Yang F, Goodman E. The relationship between developmental assets and food security in adolescents from a low-income community. J Adolescent Health. 2015;56(2):215–222. doi:10.1016/j.jadohealth.2014.10.001
12. Tamiru D, Argaw A, Gerbaba M, Ayana G, Nigussie A, Belachew T. Household food insecurity and its association with school absenteeism among primary school adolescents in Jimma zone, Ethiopia. BMC Public Health. 2016;16(1):802. doi:10.1186/s12889-016-3479-x
13. Kent MP, Pauzé E. The frequency and healthfulness of food and beverages advertised on adolescents’ preferred web sites in Canada. J Adolescent Health. 2018;63(1):102–107. doi:10.1016/j.jadohealth.2018.01.007
14. Tsarouhas K, Kioukia–Fougia N, Papalexis P, et al. Use of nutritional supplements contaminated with banned doping substances by recreational adolescent athletes in Athens, Greece. Food Chemical Toxicol. 2018;1(115):447–450.
15. Giray C, Ferguson GM. Say yes to “Sunday Dinner” and no to “Nyam and Scram”: family mealtimes, nutrition, and emotional health among adolescents and mothers in Jamaica. Appetite. 2018;1(128):129–137. doi:10.1016/j.appet.2018.05.132
16. Watts AW, Miller J, Larson NI, Eisenberg ME, Story MT, Neumark-Sztainer D. Multicontextual correlates of adolescent sugar-sweetened beverage intake. Eat Behav. 2018;1(30):42–48. doi:10.1016/j.eatbeh.2018.04.003
17. Pearson N, Atkin AJ, Biddle SJ, Gorely T, Edwardson C. Patterns of adolescent physical activity and dietary behaviours. Int J Behavioral Nutrition Physical Activity. 2009;6(1):45. doi:10.1186/1479-5868-6-45
18. Jongenelis MI, Scully M, Morley B, Pratt IS. Vegetable and fruit intake in Australian adolescents: trends over time and perceptions of consumption. Appetite. 2018;1(129):49–54. doi:10.1016/j.appet.2018.06.033
19. Berg T, Magala-Nyago C, Iversen PO. Nutritional status among adolescent girls in children’s homes: anthropometry and dietary patterns. Clin Nutrition. 2018;37(3):926–933. doi:10.1016/j.clnu.2017.03.020
20. Gali N, Tamiru D, Tamrat M. The emerging nutritional problems of school adolescents: overweight/obesity and associated factors in Jimma town, Ethiopia. J Pediatr Nurs. 2017;1(35):98–104. doi:10.1016/j.pedn.2017.03.002
21. Parker KE, Salmon J, Brown HL, Villanueva K, Timperio A. Typologies of adolescent activity related health behaviors. J Sci Med Sport. 2019;22(3):319–323. doi:10.1016/j.jsams.2018.08.015
22. Thomas A, Janusek L. Obesity prevention behaviors in asian indian adolescent girls: a pilot study. J Pediatr Nurs. 2018;1(42):9–15. doi:10.1016/j.pedn.2018.05.007
23. Da Silva AO, Diniz PR, Santos ME, et al. Health self‐perception and its association with physical activity and nutritional status in adolescents. Jornal De Pediatria. 2019;95(4):458–465. doi:10.1016/j.jpedp.2018.08.007
24. Lee G, Han K, Kim H. Risk of mental health problems in adolescents skipping meals: the Korean National Health and nutrition examination survey 2010 to 2012. Nurs Outlook. 2017;65(4):411–419. doi:10.1016/j.outlook.2017.01.007
25. Sormunen E, Saarinen MM, Salokangas RK, et al. Body mass index trajectories in childhood and adolescence-Risk for non-affective psychosis. Schizophr Res. 2019;1(206):313–317. doi:10.1016/j.schres.2018.10.025
26. Pereira JL, de Castro MA, Hopkins S, Gugger C, Fisberg RM, Fisberg M. Prevalence of consumption and nutritional content of breakfast meal among adolescents from the Brazilian National Dietary Survey. Jornal De Pediatria. 2018;94(6):630–641.
27. Bruckauf Z, Walsh SD. Adolescents’ multiple and individual risk behaviors: examining the link with excessive sugar consumption across 26 industrialized countries. Soc Sci Med. 2018;216:133–141. doi:10.1016/j.socscimed.2018.08.029
28. Chen JL, Guedes CM, Lung AE. Smartphone-based healthy weight management intervention for Chinese American adolescents: short-term efficacy and factors associated with decreased weight. J Adolescent Health. 2019;64(4):443–449.
29. Philippou E, Middleton N, Pistos C, Andreou E, Petrou M. The impact of nutrition education on nutrition knowledge and adherence to the Mediterranean Diet in adolescent competitive swimmers. J Sci Med Sport. 2017;20(4):328–332. doi:10.1016/j.jsams.2016.08.023
30. Koniak-Griffin D, Anderson NL, Brecht ML, Verzemnieks I, Lesser J, Kim S. Public health nursing care for adolescent mothers: impact on infant health and selected maternal outcomes at 1 year postbirth. J Adolescent Health. 2002;30(1):44–54. doi:10.1016/S1054-139X(01)00330-5
31. Tamiru D, Argaw A, Gerbaba M, Nigussie A, Ayana G, Belachew T. Improving dietary diversity of school adolescents through school based nutrition education and home gardening in Jimma Zone: quasi-experimental design. Eat Behav. 2016;1(23):180–186. doi:10.1016/j.eatbeh.2016.10.009
32. Benny L, Boyden J, Penny M. Early is best but it’s not always too late: young Lives evidence on nutrition and growth in Ethiopia, India, Peru and Vietnam, Summative report. Oxford: Young Lives, 2018.
33. Rentería-Mexía A, Vega-López S, Olson ML, et al. Effects of a lifestyle intervention on markers of cardiometabolic risk and oxidized lipoproteins among obese adolescents with prediabetes. Public Health Nutr. 2019;22(4):706–713. doi:10.1017/S1368980018003476
34. Seo YG, Lim H, Kim Y, et al. The effect of a multidisciplinary lifestyle intervention on obesity status, body composition, physical fitness, and cardiometabolic risk markers in children and adolescents with obesity. Nutrients. 2019;11(1):137. doi:10.3390/nu11010137
35. World Health Organization. Adolescent Nutrition: A Review of the Situation in Selected South-East Asian Countries. WHO Regional Office for South-East Asia; 2006.
36. Wassie MM, Gete AA, Yesuf ME, Alene GD, Belay A, Moges T. Predictors of nutritional status of Ethiopian adolescent girls: a community based cross sectional study. BMC Nutrition. 2015;1(1):20. doi:10.1186/s40795-015-0015-9
37. Koyanagi A, Stubbs B, Oh H, et al. Food insecurity (hunger) and suicide attempts among 179,771 adolescents attending school from 9 high-income, 31 middle-income, and 4 low-income countries: A cross-sectional study. J Affect Disord. 2019;248:91–98. doi:10.1016/j.jad.2019.01.033
38. World Health Organization. The state of food security and nutrition in the world 2018: building climate resilience for food security and nutrition. Food Agriculture Org. 2018;12.
39. Caruso B. Women still carry most of the world’s water: [Nov25-2019]; 2017. Available from https://theconversation.com/women-still-carry-most-of-the-worlds-water-81054.
40. Bezabih A, Wereta M, Kahsay Z, Getahun Z, Bazzano A. Demand and supply side barriers that limit the uptake of nutrition services among pregnant women from rural Ethiopia: an exploratory qualitative study. Nutrients. 2018;10(11):1687. doi:10.3390/nu10111687
41. Marsh V, Mwangome N, Jao I, Wright K, Molyneux S, Davies A. Who should decide about children’s and adolescents’ participation in health research? The views of children and adults in rural Kenya. BMC Med Ethics. 2019;20(1):
42. Alomari MA, Al-sheyab NA, Khabour OF, Alzoubi KH. Assent and consent in adolescent research: teachers’ perspectives from a developing country. Heliyon. 2020;6(1):e03116. doi:10.1016/j.heliyon.2019.e03116
43. De Moraes AF, Rocha C. Gendered waters: the participation of women in the ‘one million cisterns’ rainwater harvesting program in the Brazilian Semi-Arid region. J Clean Prod. 2013;1(60):163–169.
44. Chattopadhyay A, Sethi V, Nagargoje VP, et al. WASH practices and its association with nutritional status of adolescent girls in poverty pockets of eastern India. BMC Women’s Health. 2019;19(1):89. doi:10.1186/s12905-019-0787-1
45. Loso J, Staub D, Colby SE, et al. Gardening experience is associated with increased fruit and vegetable intake among first-year college students: A cross-sectional examination. J Acad Nutr Diet. 2018;118(2):275–283. doi:10.1016/j.jand.2017.09.005
46. Saldanha LS, Buback L, White JM, et al. Policies and program implementation experience to improve maternal nutrition in Ethiopia. Food Nutr Bull. 2012;33(2_suppl1):S2750. doi:10.1177/15648265120332S103
47. Sorenson SB, Morssink C, Campos PA. Safe access to safe water in low income countries: water fetching in current times. Soc Sci Med. 2011;72(9):1522–1526. doi:10.1016/j.socscimed.2011.03.010
48. Mohammed SH, Taye H, Larijani B, Esmaillzadeh A. Food taboo among pregnant Ethiopian women: magnitude, drivers, and association with anemia. Nutr J. 2019;18(1):19. doi:10.1186/s12937-019-0444-4
49. Getnet W, Aycheh W, Tessema T. Determinants of food taboos in the pregnant women of the awabel district, east gojjam zone, amhara regional state in Ethiopia. Adv Public Health. 2018;2018.
50. Zerfu TA, Umeta M, Baye K. Dietary habits, food taboos, and perceptions towards weight gain during pregnancy in Arsi, rural central Ethiopia: a qualitative cross-sectional study. J Health Popul Nutr. 2016;35(1):22. doi:10.1186/s41043-016-0059-8
51. Neumark-Sztainer D, Story M, Perry C, Casey MA. Factors influencing food choices of adolescents: findings from focus-group discussions with adolescents. J Am Diet Assoc. 1999;99(8):929–937. doi:10.1016/S0002-8223(99)00222-9
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.