")
Back to Journals » Hepatic Medicine: Evidence and Research » Volume 10
Expert opinion on the management of hepatitis C infection in Kuwait
Authors Saad MF, Alenezi S, Asker H
Received 22 October 2017
Accepted for publication 15 May 2018
Published 28 September 2018 Volume 2018:10 Pages 117—132
DOI https://doi.org/10.2147/HMER.S154842
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gerry Lake-Bakaar
Video abstract presented by Motaz F Saad.
Views: 1057
Motaz Fathy Saad,1 Saleh Alenezi,2 Haifaa Asker3
On behalf of the Kuwait Hepatology Club
1Haya Al-Habib Gastroenterology and Hepatology Center, Mubarak Alkabir Hospital, Hawaly, Kuwait; 2Unit of Gastroenterology and Hepatology, Department of Medicine, Farwaniya Hospital, Kuwait City, Kuwait; 3Thunayan Al-Ghanim Gastroenterology and Hepatology Center, Al-Amiri Hospital, Kuwait City, Kuwait
Abstract: Chronic hepatitis C virus (HCV) infection is a leading cause of death, especially in immunocompromised patients. The lack of clear prevalence data in the Middle East makes it difficult to estimate the true morbidity and mortality burden of HCV. In Kuwait, estimating the burden of disease is complicated by the constant flow of expatriates, many of whom are from HCV-endemic areas. The development of new and revolutionary treatments for HCV necessitates the standardization of clinical practice across all healthcare institutions. While international guidelines from the American Association for the Study of Liver Diseases (AASLD) and European Association for the Study of the Liver (EASL) do address this evolving treatment landscape, the cost-driven treatment prioritization of patients by these guidelines and unique HCV genotype presentation in the Kuwaiti population prompted the development of a more tailored approach. The predominant HCV genotypes prevalent in Kuwait are genotypes 4 and 1. The Kuwait Hepatology Club (KHC), comprising hepatologists across all major institutions in Kuwait, conducted several consensus meetings to develop the scoring criteria, evaluate all current evidence, and propose screening, diagnosis, and treatment suggestions for the management of HCV in this population. While these treatment suggestions were largely consistent with the 2016 AASLD and 2015 EASL guidelines, they also addressed gaps in the unmet needs of the Kuwaiti population with HCV.
Keywords: hepatitis C, diagnosis, treatment, management, Kuwait
Introduction
The prevalence of hepatitis C virus (HCV) infection was recently estimated as 2.8% worldwide, amounting to >185 million people,1 and has rapidly become a leading cause of death, especially in HIV-positive patients.2 In the Middle East, where countries have varying degrees of health service infrastructure, there is a distinct lack of clear epidemiology data. Most epidemiological studies have been conducted by independent scientists and are based on the seroprevalence of HCV in specific groups.3 Many foreign workers in Kuwait are coming from regions that are considered HCV endemic. HCV prevalence in Kuwait is estimated to be around 0.8% in Kuwaiti nationals and 5.4% in expatriates.4 The prevailing genotypes are genotypes 1 and 4, with genotype 4 as the most common.5
Historically, options for HCV treatment have been limited. Interferon (IFN)-α and ribavirin (RBV), the main options, had inadequate efficacy results and severe adverse effects. However, in recent years, dramatic improvements in the therapeutic landscape have vastly improved the outcomes for the patients with chronic HCV. This quickly multiplying new generation of direct-acting antiviral agents (DAAs) poses a unique challenge to healthcare governing bodies who must keep up with the rapid pace of therapy development. International guidelines created by the American Association for the Study of Liver Diseases (AASLD)6 and the European Association for the Study of the Liver (EASL)7 are regularly updated with general recommendations for the management of patients with HCV. DAAs have introduced a promising new era of shortened HCV therapy, free of adverse events associated with previous standard therapies like IFNs. However, the genetic diversity of HCV in different regions and the lagging approval pace of new therapies mean that these recommendations must be tailored to the local population.
There are no recommendations yet for the management of HCV infection in Kuwait. The purpose of this article is to assist hepatologists and other healthcare professionals in the optimum management of patients with chronic HCV within the current national regulatory and therapeutic landscape in Kuwait.
Methods
The Kuwait Hepatology Club (KHC) includes representatives from the following six major hospitals that treat HCV infections in Kuwait: Mubarak Alkabir Hospital, Al-Amiri Hospital, Al-Jahraa Hospital, Al-Adan Hospital, Al-Sabah Hospital, and Farwaniya Hospital. From September 14, 2015, the KHC conducted three consensus meetings to draft an expert opinion on hepatitis C treatment in Kuwait. During these meetings, evidence from published literature and international guidelines (ie, from AASLD and EASL) was combined with real-world experience from the KHC’s expert panel to tailor the international recommendations to the local Kuwaiti clinical practice. Therefore, these statements should be viewed as the preferred approaches to care of the expert panel, rather than guidelines. The robustness of evidence was assessed for its quality and its relevance to Kuwaiti clinical practice patterns. Scoring criteria were adapted from AASLD6 and EASL7 guidelines (Table 1).
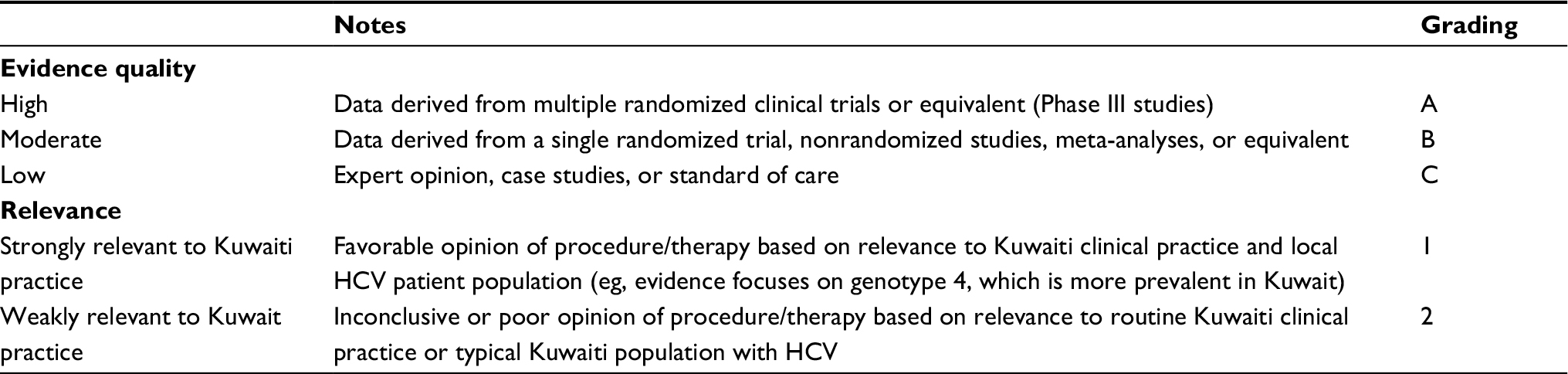 | Table 1 Scoring criteria developed by the KHC Abbreviations: KHC, Kuwait Hepatology Club; HCV, hepatitis C virus. |
Diagnosis of acute and chronic HCV
The diagnosis of HCV infection is accomplished by immunoserologic assays and nucleic acid tests.8 The most commonly used immunoserologic test is the third-generation ELISA. It is easy to perform and inexpensive, making it a suitable initial test for diagnosing HCV infection. However, this antibody test has several limitations.9 For instance, in acute infection, it may take 8 weeks for seroconversion to take place.10 Moreover, in immunocompromised settings (ie, in organ transplant recipients, hemodialysis, and HIV patients), seroconversion may be hampered, limiting the use of anti-HCV assays in the initial diagnosis.11 Therefore, a nonreactive anti-HCV test will not definitively rule out infection in these patients. The detection of antibodies indicates one of the following: 1) current infection; 2) past infection that has resolved; and 3) false positivity.12 Nucleic acid testing, using a highly sensitive polymerase chain reaction (PCR) assay for detecting HCV RNA, is more expensive and more technically demanding than the immunoserologic tests. Detecting HCV RNA indicates current infection.11 Therefore, the KHC’s expert panel suggested repeatedly testing after 3 months to rule out current infection.
The KHC’s expert panel also suggested anti-HCV antibody assay as a first-line test in patients suspected of acute HCV (Table 2). If negative, the test should be repeated after 6–12 weeks to rule out seroconversion. Alternatively, if the initial antibody test is negative, testing for HCV RNA by PCR can be performed immediately and repeated after 12 weeks. In immunocompromised individuals, both anti-HCV and PCR should be performed as first-line tests and should be repeated 12 weeks later. In cases where chronic infection is suspected, the KHC’s expert panel suggested starting with the antibody test. All reactive tests should be confirmed by PCR to diagnose current infection definitively. If HCV RNA is negative, PCR should be repeated after 12 weeks.
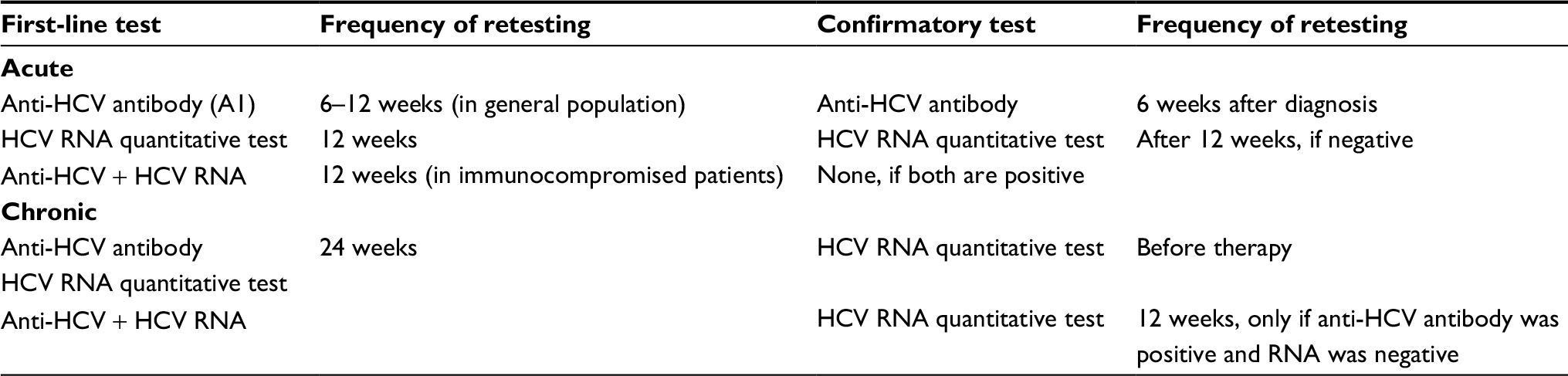 | Table 2 Workshop: Kuwait standard of practice for diagnostics tests Abbreviation: HCV, hepatitis C virus. |
Screening for hepatitis C infection
The AASLD guidelines suggest screening select high, such as individuals who inject drugs, hemodialysis patients, healthcare workers, children born to HCV-infected women, HIV-infected individuals, individuals who received blood or blood products before 1992, and those born between 1945 and 1965.6 The AASLD and Centers for Disease Control and Prevention (CDC) do not recommend testing average-risk individuals.6,10–12
While endorsing the AASLD and CDC screening guidelines, the KHC’s expert panel took into consideration data suggesting that targeted screening may miss a significant proportion of infected individuals and expanding screening practices to the general population may be cost-effective.13 Currently, the Ministry of Health in Kuwait includes testing for HCV infection in the mandatory premarital and preemployment medical screening protocols, the practice that the KHC members find meritorious. For screening purposes, the panel suggested using the antibody test initially. If positive, current infection should be confirmed by PCR using another blood sample. A negative antibody test does not warrant further testing (Table 2).
Pretherapeutic assessments
It is important to determine comorbid conditions and disease severity for the implementation of corrective actions and to tailor therapy. Noninvasive tests and liver function tests are important to determine the fibrotic damage to the liver.6 The KHC voted that routine liver stiffness measurements and liver function tests are necessary to assess disease severity. It is also important to determine at-risk behaviors, alcohol consumption, underlying comorbidities, and hepatitis B virus, or HIV co-infection to differentially assess patient disease severity. However, liver biopsies or histology examinations are rarely performed and testing for IL-28 genotypes was deemed unnecessary.
Goals and endpoints of HCV therapy
The ultimate goal of HCV therapy, as defined by AASLD, is to cure HCV infection and to prevent hepatic cirrhosis, decompensation of cirrhosis, hepatocellular carcinoma, severe extra-hepatic manifestations, and death.6 Achieving a sustained virologic response (SVR), as a therapeutic endpoint, in HCV-infected patients will reduce all-cause mortality and the consequences of liver-related disease, including end-stage liver disease and hepatocellular carcinoma.
Treatment of HCV
Therapeutic landscape
The HCV uses the nonstructural (NS) 3 protease and NS5A and NS5B polymerase enzymes for posttranslational processing and replication. These enzymes have become prime targets for HCV therapy. Protease inhibition interrupts posttranslational processing by blocking the catalytic site. In contrast, RBV monophosphate mimics inosine 5′-monophosphate and is a competitive inhibitor of inosine 5′-monophosphate dehydrogenase, an enzyme involved in the de novo synthesis of guanine nucleotides. Table 3 lists the therapeutic regimens currently approved and applied in Kuwaiti clinical practice.
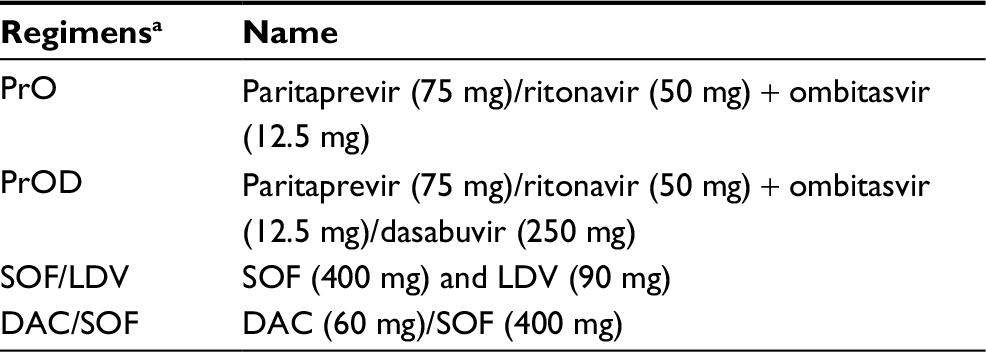 | Table 3 Therapies currently available in Kuwait Note: aThese regimens may be administered with or without ribavirin depending on prior therapy experience, genotype status, or underlying demographic characteristics and comorbidities. Abbreviations: DAC, daclatasvir; LDV, ledipasvir; PrO, paritaprevir/ritonavir-ombitasvir; PrOD, PrO and dasabuvir; SOF, sofosbuvir. |
Expert opinion on genotype-specific therapy
The most common genotypes are genotypes 4 and 1.5 Treatment options for both are summarized in Table 4, with 12 weeks being the most popular duration for most regimens. Consistent with the AASLD 2016 updated guidelines, the KHC suggested moving away from 24-week regimens unless a case is difficult to treat.
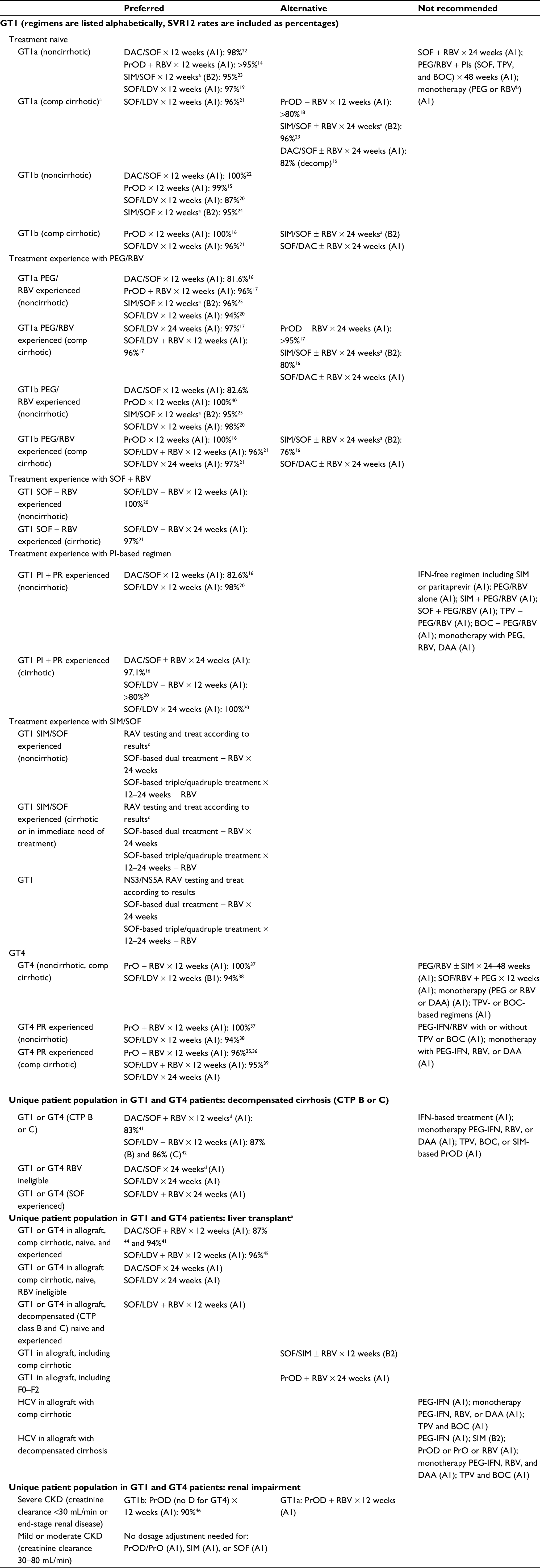 | Table 4 Summary of KHC treatment suggestions for GT1, GT4, and special populations Notes: aFor cirrhotic patients, some regimens are classified as alternative regimens because they have longer duration, potentially reduced efficacy, and/or limited supporting data compared with the preferred regimens. bLow-dose RBV (600–800 mg) can be used with patients who have an initial hemoglobin value of <11 g/dL (evidence rating: C1). cThe KHC voted that there was no need to defer treatment in GT1 SIM/SOF-experienced noncirrhotic patients. SOF/LDV may be given. The KHC was divided on whether to wait for FibroScan results before SOF/LDV could be administered. dDose-adjust cytochrome P450 3A/4 inducers. eThe KHC stated that not enough postliver transplant patients are seen in Kuwait. Abbreviations: BOC, boceprevir; DAA, direct-acting antiviral agent; DAC, daclatasvir; GT, genotype; HCV, hepatitis C virus; IFN, interferon; KHC, Kuwait Hepatology Club; LDV, ledipasvir; NS, nonstructural; CKD, chronic kidney disease; CTP, Child–Turcotte–Pugh; PEG, PEGylated; PIs, protease inhibitors; PR, PEG-IFN and RBV; PrO, paritaprevir/ritonavir-ombitasvir; PrOD, PrO and dasabuvir; RAV, resistance-associated variants; RBV, ribavirin; SIM, simeprevir; SOF, sofosbuvir; SVR, sustained virologic response; TPV, telaprevir. |
High evidence grading (A1) was given to the AASLD-approved regimens for treatment-naive and treatment-experienced patients, with some caveats. Grazoprevir/elbasvir, although approved by the European Medical Agency (EMA), is not yet available in Kuwait so is not mentioned in this expert opinion. The simeprevir (SIM)/sofosbuvir (SOF) regimen has been deprioritized because the Q80K screening test is not available in Kuwait, making it difficult to predict a positive outcome for these noncirrhotic patients.
Genotype 1
Paritaprevir/ritonavir-ombitasvir and dasabuvir (PrOD) in treatment-naive patients
Paritaprevir is a protease inhibitor (PI) that is administered with ritonavir, ombitasvir is an NS5a inhibitor, and dasabuvir is a nonnucleoside analog polymerase inhibitor. This regimen is approved in Kuwait for the treatment of genotype 1 patients and is frequently combined with RBV, except for genotype 1b cirrhotic and noncirrhotic patients. Based on the updated 2016 AASLD guidelines and the following pivotal clinical trials, the KHC suggested PrOD plus RBV for 12 weeks in treatment-naive compensated cirrhotic genotype 1a patients with an evidence rating of A1 (Table 4).
The SAPPHIRE-I trial demonstrated 96% of SVR rates in treatment-naive noncirrhotic patients treated with PrOD plus RBV for 12 weeks.14 These results were consistent with genotype 1a (95% of SVR) and genotype 1b (98% of SVR). Genotype 1b treatment-naive noncirrhotic patients achieved 99% of SVR rate in PrOD regimens with and without RBV.15 Genotype 1a treatment-naive noncirrhotic patients achieved 90% of SVR with PrOD + RBV and 97% of SVR with PrOD–RBV. Another trial in cirrhotic patients, TURQUOISE-II, investigated the combination of PrOD and RBV for 12 and 24 weeks.16 Consistent with the previous trial, 95% of treatment-naive patients achieved SVR in both groups. A subanalysis of genotypes 1a and 1b revealed 100% of SVR rates for genotype 1b in both arms, whereas genotype 1a achieved 92% at 12 weeks and 93% at 24 weeks.
PrOD in treatment-experienced patients
The KHC suggested the PrOD plus RBV regimen for 12 weeks in treatment-experienced noncirrhotic genotypes 1a and 1b patients, with an evidence rating of A1 based on the evidence from the SAPPHIRE II and TURQOISE II trials. However, in genotype 1a cirrhotic patients, PrOD plus RBV can be reserved as alternative therapy.
In the SAPPHIRE II trial, noncirrhotic patients previously treated with PEGylated IFN (PEG-IFN) and RBV (PEG/RBV) achieved >95% of SVR in genotypes 1a and 1b on PrOD plus RBV treatment for 12 weeks.17 The TURQUOISE-II trial revealed that genotype 1b cirrhotic patients who had failed prior treatments achieved 100% of SVR rates, irrespective of their previous treatment response, when treated with PrOD for 12 or 24 weeks.16 Genotype 1a patients with an inadequate previous treatment response, however, did not achieve as significant an SVR rate (>80%).18
SOF/ledipasvir (LDV) in treatment-naive patients
SOF is a nucleotide analog polymerase inhibitor and LDV is an NS5A inhibitor. In the ION-1 trial, treatment-naive patients achieved 97% of SVR at 12 weeks and 100% at 24 weeks. The ION-3 trial explored an 8-week regimen with SOF/LDV in combination with RBV.19 With the exception of those patients with a low HCV viral load, more relapse cases were seen in the 8-week regimen and, thus, the KHC voted against this shortened duration of treatment.
SOF/LDV in treatment-experienced patients
Consistent with AASLD, the KHC suggested the use of SOF/LDV in genotype 1 treatment-naive and treatment-experienced patients, with an evidence rating of A1. In the ION-2 trial, SOF/LDV demonstrated significant SVR rates at both 12 (94%) and 24 (99%) weeks in treatment-experienced genotype 1 patients.20 An integrated efficacy and safety analysis of >500 pooled Phases II and III cirrhotic treatment-naive and treatment-experienced patients revealed significant response rates (96%) on a 12-week regimen of SOF/LDV with and without RBV despite previous therapy failure.21
Daclatasvir (DAC) and SOF in treatment-naive and treatment-experienced patients
DAC is another NS5A inhibitor. The KHC suggested this regimen based on the following evidence, with a rating of A1. Sulkowski et al22 conducted a trial of DAC/SOF in previously treated and untreated chronic HCV patients. Treatment-naive noncirrhotic patients achieved a high sustained viral response of undetectable HCV by 12 weeks (SVR12) of 98% with or without RBV. The ALLY-1 trial revealed that 82% of patients who had decompensated cirrhosis treated with DAC/SOF plus RBV for 12 weeks achieved SVR12.16
SIM and SOF in treatment-naive patients
SIM is a PI. Based on the following evidence, the KHC suggested deprioritizing this regimen in treatment-naive, noncirrhotic patients, given that evidence published in favor of SIM/SOF was not conclusive enough to out value the existing alternative therapies (evidence rating: B2). SIM/SOF in combination with RBV was investigated in the COSMOS trial for 12 and 24 weeks.23 In treatment-naive patients, ~95% achieved SVR12 rates at 12 and 24 weeks. In a diverse, longitudinal, observational cohort, HCV-TARGET 2.0, 89% of patients achieved significant SVR4 rates after 12 weeks on SIM/SOF with or without RBV.24 Genotype 1b patients had better SVR rates (95%) than genotype 1a patients (89%). Kwo et al25 demonstrated in the OPTIMIST-1 trial that SIM/SOF-treated, treatment-naive, noncirrhotic patients achieved a high rate of SVR12 (97%), whereas cirrhotic patients achieved a lower SVR (85%). No difference was observed in Q80k resistance in these noncirrhotic types.25 A TRIO cohort analysis also revealed that SIM/SOF-treated cirrhotic patients who were treatment naive achieved 88% of SVR when treated for 12 weeks with or without RBV.16 Lawitz et al26 discovered that genotype 1a patients with Q80K polymorphism achieved lower SVR (74%) than genotype 1a patients without the mutation (92%). The test for Q80K polymorphism is not currently available in Kuwait.
SIM and SOF in treatment-experienced patients
Similar to the treatment suggestions for treatment-naive patient for SIM/SOF, the KHC suggested deprioritizing this regimen in treatment-experienced patients based on the following evidence (evidence rating: B2). In the COSMOS trial, treatment-experienced patients achieved 91% of SVR rates when treated for 12 and 24 weeks.15 The OPTIMIST-1 trial also demonstrated high SVR rates (95%) in treatment-experienced, noncirrhotic patients.25 However, cirrhotic patients who had failed previous treatments only managed 77% of SVR. The TRIO cohort analysis revealed that SIM/SOF-treated patients who were treatment experienced achieved 87% of SVR rates in noncirrhotic patients and 76% of SVR rates in cirrhotic patients.16 The rate of SVR12 in PI failures was 82 and 80% in patients with the previous failure of PEG-IFN and RBV (PR) therapy.16
Not recommended for genotype 1
Based on current evidence, other regimens such as SIM + PEG/RBV,27–29 SOF + PEG/RBV,30,31 telaprevir (TPV) + PEG/RBV,32 and boceprevir (BOC) + PEG/RBV33,34 are not more effective than the above regimens in duration or efficacy. Pending more robust data supporting the efficacy of these regimens, the KHC prioritized them as not recommended therapies (evidence rating: A1) (Table 4).
Regimens with PEG-IFN with RBV or with TPV or BOC are not recommended in patients with genotype 1.6 In patients with decompensated cirrhosis with moderate-to-severe hepatic impairment (Child–Turcotte–Pugh [CTP] class B or C), IFN-based therapy and monotherapy with PEG/RBV-, DAA-, TPV-, BOC-, SIM-, or PrOD-based regimens are not recommended (Table 4).6
Genotype 4
Paritaprevir/ritonavir-ombitasvir (PrO) and RBV
Consistent with AASLD and EASL, the KHC suggested the use of the PrO + RBV regimen for the treatment of genotype 4 patients, based on its strong evidence rating of A1. The AGATE I trial revealed that the PRO + RBV regimen achieved 97% of SVR rates in genotype 4 patients with cirrhosis.35 The AGATE II trial focused on Egyptian patients with HCV who had cirrhosis.36 Sensitivity analysis showed that PrO + RBV demonstrated the SVR12 rates of 97% (30/31) at 12 weeks and 96% (27/28) at 24 weeks in these patients excluding those who discontinue study drug prematurely with no on-treatment failure or those with missing follow-up data in the SVR12 window.36 The PEARL-1 trial demonstrated that PrO + RBV was highly successful in achieving an SVR12 rate of 100% in treatment-naive and treatment-experienced, genotype 4 noncirrhotic patients.37
SOF/LDV
In a proof-of-concept study, the SOF/LDV combination demonstrated 95% of SVR in 21 genotype 4 patients.38 Another study in 44 patients with genotype 4 confirmed the SVR12 rate of 93%.39 This regimen is preferred by the KHC for the treatment of genotype 4 patients (evidence rating: B1).
Not recommended for genotype 4
Regimens with PEG-IFN with RBV or with TPV or BOC are not recommended in patients with genotype 4 with or without cirrhosis based on the results from the PEARL-II and TURQOISE-III trials, respectively (evidence rating: A1).40,41
Special populations in genotype 1 and genotype 4
Patients with decompensated cirrhosis
DAC and SOF
Based on the following evidence, the KHC suggested DAC/SOF for the treatment of decompensated cirrhosis in patients with genotype 1 HCV infection (evidence rating: A1). The ALLY-1 study demonstrated that a 12-week regimen of DAC/SOF successfully treated genotype 1 patients with advanced cirrhosis (CTP class B and C; n=60) achieved the SVR rates of 83%.42
SOF and LDV
Based on the following evidence, the KHC suggested SOF/LDV for the treatment of patients with genotypes 1 or 4 HCV infection and decompensated cirrhosis (evidence rating: A1). In a large, multicenter, randomized controlled trial, SOLAR-1, 108 patients with HCV genotype 1 or 4 infection and who had decompensated cirrhosis (CTP class B or C) achieved the SVR rates of 87% (CTP B) and 86% (CTP C) when treated for 12 weeks. These rates were slightly improved when CTP B (89%) patients and CTP C patients (87%) received 24 weeks of SOF/LDV therapy.43 Similar results were seen in a multicenter randomized controlled trial, SOLAR-2, of 108 patients with HCV genotypes 1 and 4 who had decompensated cirrhosis and achieved 87% of SVR after 12 weeks of treatment with SOF/LDV and 89% of SVR after 24 weeks.44
Patients who have received liver transplants
SAC and SOF
Based on the following evidence, the KHC suggested DAC/SOF for the treatment of postliver transplant patients with genotype 1 or 4 HCV infection (evidence rating: A1). The ALLY-1 study demonstrated that a 12-week regimen of DAC/SOF-helped genotype 1 patients with recurrent HCV infection posttransplant achieved 94% of SVR12.42 In another trial of 64 liver transplant recipients with HCV genotype 1 infection, patients treated with DAC/SOF achieved an SVR12 rate of 87%.45
SOF and LDV
Based on the following evidence, the KHC suggested DAC/SOF for the treatment of postliver transplant patients with genotype 1 or 4 HCV infection (evidence rating: A1). In the SOLAR-1 study, 223 liver transplant recipients with genotype 1 or 4 HCV infection achieved an SVR rate of 96% when treated with SOF/LDV for 12 or 24 weeks.46
Patients with renal impairment
PrOD
Based on the following evidence, the KHC suggested the PrOD regimen for the treatment of patients with renal impairment, with the caveat that PrOD should be avoided in patients with CTP B or C (evidence rating: A1).
In a Phase II study of 20 patients with genotype 1 and stage 4 or 5 (estimated glomerular filtration rate <30 mL/min/1.73 m2) CKD without cirrhosis, a PrOD combination regimen was administered with or without RBV.47 All patients achieved SVR4. Regimens containing ofosbuvir48 and SIM49 have been found to be effective in mild CKD.
Genotypes 2, 3, 5, and 6
Genotypes 2, 3, 5, and 6 are very rare in Kuwait. KHC refers to the AASLD guidelines should patients present with any of these genotypes, with caveats for local availability of recommended therapy or testing options, as shown in Table 5.
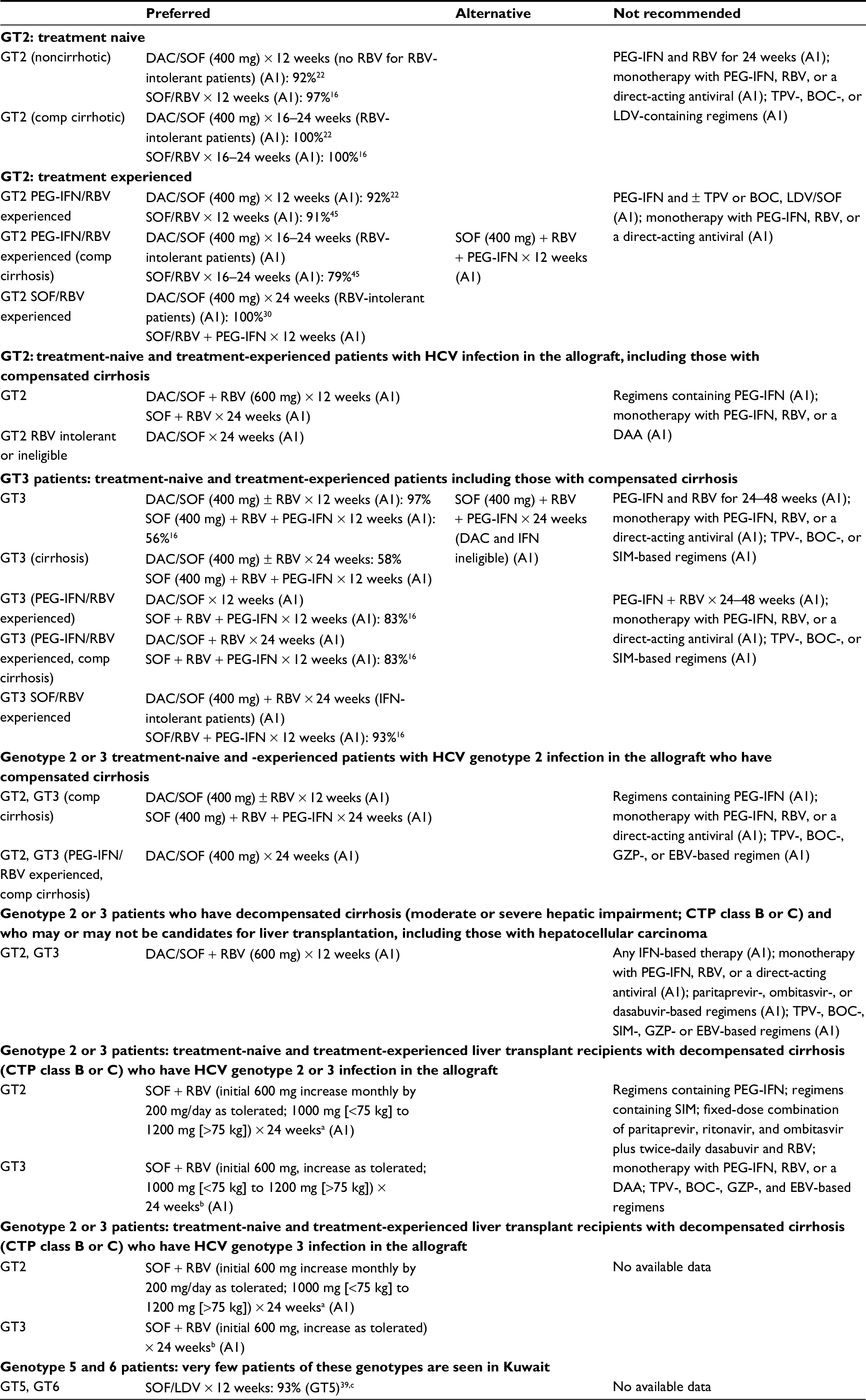 | Table 5 Summary of KHC treatment suggestions for genotypes 2, 3, 5, and 6 Notes: aWith consideration of the patient’s creatinine clearance rate and hemoglobin level for up to 48 weeks. bNo dose adjustment is required for tacrolimus or cyclosporine with SOF–RBV, SOF–LDV, or SOF–DAC. Because of high plasma concentrations of SIM, the concomitant use of SIM and cyclosporine A is not recommended in liver transplant recipients. No SIM dose changes are required with tacrolimus and sirolimus, but the patient’s blood concentrations should be monitored regularly. When using the combination of ritonavir-boosted paritaprevir, ombitasvir, and dasabuvir, the tacrolimus dose must be adjusted to 0.5 mg once weekly or to 0.2 mg every 3 days, whereas the cyclosporine A dose must be adjusted to one-fifth of the daily dose given prior to HCV treatment once daily; prednisone use at doses ≤5 mg/day is permitted, but mTOR inhibitors are not recommended. cThe KHC generally agreed with AASLD recommendation for the treatment of these patients. Currently, SOF/LDV is the only option available in Kuwait. Other AASLD-approved treatments are not approved yet. Abbreviations: AASLD, American Association for the Study of Liver Diseases; BOC, boceprevir; CTP, Child–Turcotte–Pugh; DAC, daclatasvir; EBV, elbasvir; GT, genotype; GZP, grazoprevir; HCV, hepatitis C virus; IFN, interferon; KHC, Kuwait Hepatology Club; LDV, ledipasvir; PEG, PEGylated; RBV, ribavirin; SIM, simeprevir; SOF, sofosbuvir; TPV, telaprevir. |
General suggestions for the management of HCV
Although the KHC’s expert panel suggestions were mostly consistent with AASLD, there were a few caveats.
Assessments prior to starting antiviral therapy
The AASLD recommends noninvasive testing and, in some cases, liver biopsies prior to starting antiviral therapy,6 whereas in clinical practice, the KHC does not routinely include these tests. Instead, a “treat all” strategy is used to manage HCV infections (evidence rating: C1).50
Assessments during antiviral therapy
The AASLD recommends discontinuing RBV therapy in patients with a history of cardiovascular disease whose hemoglobin levels drop <8.5 g/dL.6 The KHC suggests that severe anemia needs not to be an indication to discontinue therapy (evidence rating: C1).51
Suggested testing for diagnosing acute HCV infection
The KHC identified the preferred criteria for the diagnosis of acute HCV infection as
- Positive anti-HCV IgG and a documented negative anti-HCV IgG in the previous 12 months, or
- Positive serum HCV RNA test and a documented negative serum HCV RNA and negative anti-HCV IgG in previous 12 months, or
- Positive serum HCV RNA test with an acute rise of alanine transaminase >5 times the upper limit of normal, or 3.5 times the high baseline alanine transaminase level with an absence of other causes of acute hepatitis.
Suggestions for medical management and monitoring in acute HCV infection
The KHC agreed with most of the AASLD recommendations for the medical management and monitoring of acute HCV infections, with one exception. Treatment of acute HCV infection after 24 weeks of presentation is not preferred except in special situations such as patients with CKD in whom spontaneous viral clearance is very uncommon.
Acute HCV infection in patients with CKD can progress very rapidly to cirrhosis. Treatment of acute HCV infection can be considered earlier in occupationally infected healthcare workers to prevent ongoing transmission events.
Follow-up for patients who achieve an SVR
The KHC suggested that patients with advanced liver fibrosis (stages F3–F4) should be monitored by FibroScan and other noninvasive methods (evidence rating: B1).52 Patients with known or suspected bridging fibrosis and cirrhosis are at increased risk of developing complications of advanced liver disease and may require more frequent follow-up and surveillance by ultrasound.
Monitoring during chemotherapy and immunosuppression
The KHC determined that the major cause of death for patients with hepatocellular carcinoma is liver failure. Life expectancy may be compromised by underlying comorbidities. Functional improvement is important. Monitoring of HCV RNA is routinely practiced during chemotherapy (evidence rating: C1).
Suggestions for managing patients with risk factors (eg, obesity and alcoholism)
The KHC’s expert panel stated that multidisciplinary support involving diabetologists and dieticians is needed to manage these patients (evidence rating: A2).53
Suggestions for monitoring quality of life (eg, patient-reported outcomes and work productivity)
The KHC’s expert panel observed that although an integrated care infrastructure is important to optimally manage patients with HCV, parameters for assessing the quality of life are not routinely measured due to the lack of adequate ancillary support (evidence rating: A2).54
Suggestions for elderly patients
The KHC stated that the exclusion of elderly persons from HCV screening policy should be avoided. All people living with HCV infection should be considered for therapy, except those with a short-life expectancy (<6 months) due to nonliver-related or non-HCV-related comorbidities (evidence rating: B1).55
Elderly patients should be a major topic in HCV epidemiology research, awareness campaigns, and targeted screening (evidence rating: C1).56
In contrast to the AASLD guidelines, the KHC stated that HCV screening in elderly persons may be added to the screening colonoscopy program and may decrease viral transmission by colonoscopy. Use of shorter regimen courses, and avoidance of use of RBV because it has more adverse effects in elderly patients, is suggested (evidence rating: B2).57 For people aged >50 years who are prescribed RBV-containing regimens, it is important to consider the complications of anemia and screen those who have a history of cardiovascular disease and who have had an electrocardiogram (ECG). For people with cardiovascular disease, a regimen that does not involve RBV may be most suitable (evidence rating: B2).57
Suggestions for monitoring for pregnancy-related issues prior to and during antiviral therapy that includes RBV
In contrast to the AASLD, the KHC stated that antepartum HCV screening to decrease vertical transmission is preferred and may be cost-effective (evidence rating: C1).58–60 Delaying pregnancy until HCV antiviral therapy is completed should be considered, as treatment courses with DAAs are short in duration (evidence rating: A1).61,62 The KHC suggested two contraceptive measures. Patients treated with RBV should be counseled about the risk of teratogenicity, and patients of child-bearing age should be advised not to become pregnant during, and for 6 months after, therapy (evidence rating: A1).63,64
As the safety of DAAs during lactation has not yet been established, treating women who are breastfeeding is not recommended (evidence rating: A1).61,62
Suggestions for incarcerated individuals
Universal screening of incarcerated individuals is suggested (evidence rating: B1).65 In fact, jails may be an ideal setting for identifying individuals with HCV infection (evidence rating: C2).66,67
In contrast to the AASLD, the KHC suggested a smooth transition process from HCV treatment within the prison to treatment in the community by official referral to regional hospitals without a lapse in treatment. Education on the importance of HCV screening and treatment in HCV high-prevalence community settings (ie, the jail population) is crucial to containing the spread of HCV. Incarceration presents a unique opportunity for HCV therapy, due to controlled access to healthcare and stable accommodation (evidence rating: C1).68
Suggestions for persons who inject drugs (PWIDs)
Initial HCV RNA testing in PWIDs is suggested because an anti-HCV test is expected to be positive because of reinfection after spontaneous or treatment-related viral clearance (evidence rating: A1).69–71 In contrast to the AASLD, the KHC suggested that PWIDs can be successfully treated for HCV infection even with ongoing injection drug use (evidence rating: C2).72 Suitable settings, specific models of care, and a multidisciplinary team approach have an important role in HCV treatment acceptance in PWIDs.73–78
Persons identified as abusing alcohol and as having alcohol dependence require treatment and consideration for referral to an addiction specialist (evidence rating: C2).79 Integration of HCV therapy with addiction therapy in opioid substitution therapy centers is suggested to enhance HCV treatment uptake (evidence rating: C2).74 Education and training of clinical staff at opioid substitution therapy centers to integrate HCV treatment with addiction treatment are suggested (evidence rating: B2).6,7
Body piercing procedures such as tattooing and Hijama should be monitored. Authorities should consider a needle-exchange program (evidence rating: B2).
Suggestions for emerging therapies
A difference in patient treatment patterns noted by the KHC is that the non-Kuwaiti population is mostly treated with generics rather than new direct-acting agents.
Common barriers to HCV
Despite advancements in the therapeutic landscape, barriers to achieving treatment goals, which are unique to HCV, exist locally. The KHC proposed the strategies listed in Table 6 to overcome these barriers.
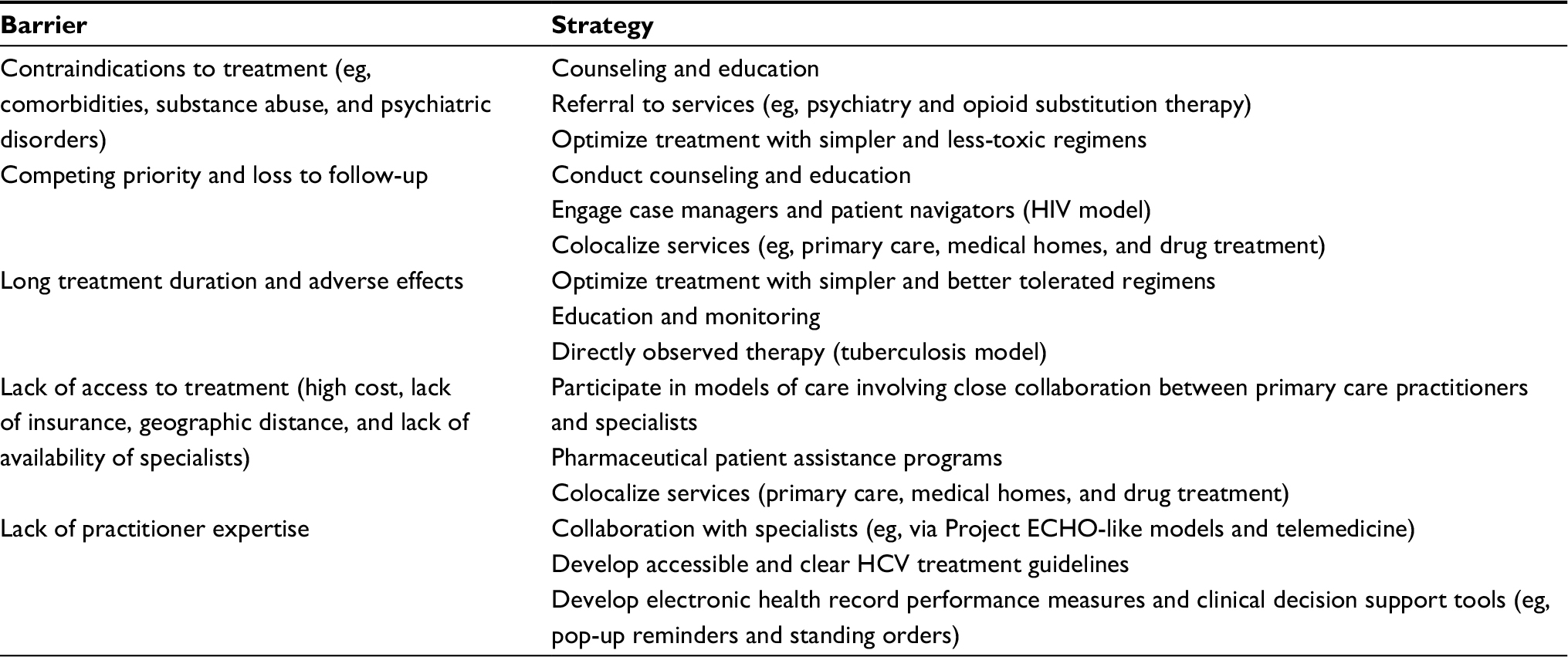 | Table 6 Common barriers to HCV treatment and potential strategies to address these barriers Abbreviations: ECHO, Extension for Community Health Outcomes; HCV, hepatitis C virus. |
HCV carries a strong negative connotation as a sexually transmitted disease. The KHC’s expert panel highlighted the need for the education of healthcare providers and patients to counter the stigma associated with the disease. The need to create an expert group to influence government policy on HCV treatment was also suggested.
Patients may fear diagnosis because of misleading information about HCV being incurable. Another barrier is the cost and access to therapy. The club highlighted the immediate need to build a national registry to capture current and long-term detailed information on Kuwaiti patients with HCV. Collection of these data will help shape HCV management strategies. Additional measures discussed by the KHC to prevent the transmission of HCV are listed in Figure 1.
 | Figure 1 Proposed initiatives to contain the transmission of HCV. Abbreviations: HCV, hepatitis C virus; STD, sexually transmitted diseases; PWIDS, people who inject drugs. |
Conclusion
HCV remains a pressing public health issue in Kuwait, but this expert opinion marks the first step in standardizing HCV treatment practices and maximizing patient benefit. The approval of new oral HCV therapies has expanded the possibilities of achieving unprecedented control of HCV infections. With this changing landscape, new challenges arise that require all healthcare and regulatory sectors to collaborate and design strategies to seamlessly and safely integrate these new therapies into existing treatment algorithms and improve patient access to these medications.
Acknowledgments
The following members of the Kuwait Hepatology Club (listed alphabetically by last name) contributed significantly to the writing and review of the article: Ali Abdulhamid (Gastroenterology and Hepatology Unit, Al-Sabah Hospital), Bader Alenezi (Gastroenterology and Hepatology Unit, Al-Jahra Hospital), Wafaa Alhashash (Gastroenterology and Hepatology unit, Al-Sabah Hospital), Raed Alzafiri (Gastroenterology and Hepatology Unit, Al-Jahra Hospital), Ramadan Hassan Eldamarawy (Gastroenterology and Hepatology Unit, Al-Adan Hospital), Ahmed Elfadhly (Haya Al-Habib Gastroenterology and Hepatology Center, Mubarak Alkabir Hospital), Hasan Elgarem (Gastroenterology and Hepatology Unit, Al-Sabah Hospital), Amal Gad (Thunayan Al-Ghanim Gastroenterology and Hepatology Center, Al-Amiri Hospital), Amr Hamed (Gastroenterology and Hepatology Unit, Al-Jahra Hospital), Fuad Hassan (Haya Alhabib Gastroenterology and Hepatology Center, Mubarak Alkabir Hospital, Faculty of Medicine, Kuwait University), Jafer Ismael (Gastroenterology and Hepatology Unit, Al-Adan Hospital), Ali A Ismaiel (Gastroenterology and Hepatology Unit, Farwaniya Hospital, Kuwait), Tamer Mansour (Thunayan Al-Ghanim Gastroenterology and Hepatology Center, Al-Amiri Hospital), Sherif Saeed Mehrem (Gastroenterology and Hepatology Unit, Al-Sabah Hospital), Samuel Sobhy Shaker (Gastroenterology and Hepatology Unit, Al-Adan Hospital), and Heba Zaki (Thunayan Al-Ghanim Gastroenterology and Hepatology Center, Al-Amiri Hospital). We acknowledge Aarati Rai, PhD, MBA, OPEN Health Dubai, for providing medical writing support for this article. Medical writing support was funded by Abbvie. Abbvie had no contribution to the content of the article.
Disclosure
The authors report no conflicts of interest in this work.
References
Mohd Hanafiah K, Groeger J, Flaxman AD, Wiersma ST. Global epidemiology of hepatitis C virus infection: new estimates of age-specific antibody to HCV seroprevalence. Hepatology. 2013;57(4):1333–1342. | ||
Antiretroviral Therapy Cohort Colllaboration. Causes of death in HIV-1-infected patients treated with antiretroviral therapy, 1996–2006: collaborative analysis of 13 HIV cohort studies. Clin Infect Dis. 2010;50(10):1387–1396. | ||
Daw MA, Dau AA. Hepatitis C virus in Arab world: a state of concern. ScientificWorldJournal. 2012;2012:719494. | ||
Ameen R, Sanad N, Al-Shemmari S, et al. Prevalence of viral markers among first-time Arab blood donors in Kuwait. Transfusion. 2005;45(12):1973–1980. | ||
Pacsa AS, Al-Mufti S, Chugh TD, et al. Genotypes of hepatitis C virus in Kuwait. Med Princ Pract. 2001;10:55–67. | ||
AASLD/IDSA HCV Guidance Panel. Hepatitis C guidance: AASLD-IDSA recommendations for testing, managing, and treating adults infected with hepatitis C virus. Hepatology. 2015;62(3):932–954. | ||
European Association for Study of Liver. EASL recommendations on treatment of hepatitis C 2015. J Hepatol. 2015;63(1):199–236. | ||
European Association for Study of Liver, Asociacion Latinoamericana para el Estudio del H. EASL-ALEH Clinical Practice Guidelines: non-invasive tests for evaluation of liver disease severity and prognosis. J Hepatol. 2015;63(1):237–264. | ||
Chou R, Clark EC, Helfand M; U.S. Preventive Services Task Force. Screening for hepatitis C virus infection: a review of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med. 2004;140(6):465–479. | ||
Workowski KA, Bolan GA; Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64(RR-03):1–137. | ||
Alter MJ, Kuhnert WL, Finelli L; Centers for Disease Control and Prevention. Guidelines for laboratory testing and result reporting of antibody to hepatitis C virus. Centers for Disease Control and Prevention. MMWR Recomm Rep. 2003;52(RR-3):CE11–CE14. | ||
Centers for Disease Control and Prevention. Testing for HCV infection: an update of guidance for clinicians and laboratorians. MMWR Morb Mortal Wkly Rep. 2013;62(18):362–365. | ||
Coffin PO, Scott JD, Golden MR, Sullivan SD. Cost-effectiveness and population outcomes of general population screening for hepatitis C. Clin Infect Dis. 2012;54(9):1259–1271. | ||
Feld JJ, Kowdley KV, Coakley E, et al. Treatment of HCV with ABT-450/r-ombitasvir and dasabuvir with ribavirin. N Engl J Med. 2014;370(17):1594–1603. | ||
Ferenci P, Bernstein D, Lalezari J, et al. ABT-450/r-ombitasvir and dasabuvir with or without ribavirin for HCV. N Engl J Med. 2014;370(21):1983–1992. | ||
A special meeting review edition: highlights in the treatment of hepatitis C virus from the 2014 liver meeting: a review of selected presentations. From the 2014 Liver Meeting November 7–11, 2014. Gastroenterol Hepatol (N Y). 2014;10(12 Suppl 6):1–19. | ||
Zeuzem S, Jacobson IM, Baykal T, et al. Retreatment of HCV with ABT-450/r-ombitasvir and dasabuvir with ribavirin. N Engl J Med. 2014;370(17):1604–1614. | ||
Poordad F, Hezode C, Trinh R, et al. ABT-450/r-ombitasvir and dasabuvir with ribavirin for hepatitis C with cirrhosis. N Engl J Med. 2014;370(21):1973–1982. | ||
Kowdley KV, Gordon SC, Reddy KR, et al. Ledipasvir and sofosbuvir for 8 or 12 weeks for chronic HCV without cirrhosis. N Engl J Med. 2014;370(20):1879–1888. | ||
Afdhal N, Reddy KR, Nelson DR, et al. Ledipasvir and sofosbuvir for previously treated HCV genotype 1 infection. N Engl J Med. 2014;370(16):1483–1493. | ||
Reddy KR, Bourliere M, Sulkowski M, et al. Ledipasvir and sofosbuvir in patients with genotype 1 hepatitis C virus infection and compensated cirrhosis: an integrated safety and efficacy analysis. Hepatology. 2015;62(1):79–86. | ||
Sulkowski MS, Gardiner DF, Rodriguez-Torres M, et al. Daclatasvir plus sofosbuvir for previously treated or untreated chronic HCV infection. N Engl J Med. 2014;370(3):211–221. | ||
Lawitz E, Sulkowski MS, Ghalib R, et al. Simeprevir plus sofosbuvir, with or without ribavirin, to treat chronic infection with hepatitis C virus genotype 1 in non-responders to PEGylated interferon and ribavirin and treatment-naive patients: the COSMOS randomised study. Lancet. 2014;384(9956):1756–1765. | ||
Sulkowski MS, Vargas HE, Di Bisceglie AM, et al. Effectiveness of simeprevir plus sofosbuvir, with or without ribavirin, in real-world patients with HCV genotype 1 infection. Gastroenterology. 2016;150(2):419–429. | ||
Kwo P, Gitlin N, Nahass R, et al. Simeprevir plus sofosbuvir (12 and 8 weeks) in HCV genotype 1-infected patients without cirrhosis: OPTIMIST-1, a phase 3, randomized study. Hepatology. 2016;64(2):370–380. | ||
Lawitz E, Matusow G, DeJesus E, et al. Simeprevir plus sofosbuvir in patients with chronic hepatitis C virus genotype 1 infection and cirrhosis: a Phase 3 study (OPTIMIST-2). Hepatology. 2016;64(2):360–369. | ||
Jacobson IM, Dore GJ, Foster GR, et al. Simeprevir with PEGylated interferon alfa 2a plus ribavirin in treatment-naive patients with chronic hepatitis C virus genotype 1 infection (QUEST-1): a phase 3, randomised, double-blind, placebo-controlled trial. Lancet. 2014;384(9941):403–413. | ||
Manns M, Marcellin P, Poordad F, et al. Simeprevir with PEGylated interferon alfa 2a or 2b plus ribavirin in treatment-naive patients with chronic hepatitis C virus genotype 1 infection (QUEST-2): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet. 2014;384(9941):414–426. | ||
Reddy KR, Zeuzem S, Zoulim F, et al. Simeprevir versus telaprevir with PEGinterferon and ribavirin in previous null or partial responders with chronic hepatitis C virus genotype 1 infection (ATTAIN): a randomised, double-blind, non-inferiority phase 3 trial. Lancet Infect Dis. 2015;15(1):27–35. | ||
Lawitz E, Mangia A, Wyles D, et al. Sofosbuvir for previously untreated chronic hepatitis C infection. N Engl J Med. 2013;368(20):1878–1887. | ||
Pearlman BL, Ehleben C, Perrys M. The combination of simeprevir and sofosbuvir is more effective than that of PEGinterferon, ribavirin, and sofosbuvir for patients with hepatitis C-related Child’s class A cirrhosis. Gastroenterology. 2015;148(4):762–770.e2; quiz.e11–2. | ||
Zeuzem S, Andreone P, Pol S, et al. Telaprevir for retreatment of HCV infection. N Engl J Med. 2011;364(25):2417–2428. | ||
Poordad F, McCone J Jr, Bacon BR, et al. Boceprevir for untreated chronic HCV genotype 1 infection. N Engl J Med. 2011;364(13):1195–1206. | ||
Bacon BR, Gordon SC, Lawitz E, et al. Boceprevir for previously treated chronic HCV genotype 1 infection. N Engl J Med. 2011;364(13):1207–1217. | ||
Asselah T. AGATE-I Study – Part I: OBV/PTV/r + RBV in genotype 4 with cirrhosis. Presented at EASL 2016. J Hepatol. 2016;64(Abs. SAT-278):S827. | ||
Waked I. AGATE-II Study: OBV/PTV/r + RBV in genotype 4 Egyptian patients without or with cirrhosis. Presented at EASL 2016. J Hepatol. 2016;64(Abs. SAT-166):S772. | ||
Hezode C, Asselah T, Reddy KR, et al. Ombitasvir plus paritaprevir plus ritonavir with or without ribavirin in treatment-naive and treatment-experienced patients with genotype 4 chronic hepatitis C virus infection (PEARL-I): a randomised, open-label trial. Lancet. 2015;385(9986):2502–2509. | ||
Kohli A, Kapoor R, Sims Z, et al. Ledipasvir and sofosbuvir for hepatitis C genotype 4: a proof-of-concept, single-centre, open-label phase 2a cohort study. Lancet Infect Dis. 2015;15(9):1049–1054. | ||
Abergel A, Metivier S, Samuel D, et al. Ledipasvir plus sofosbuvir for 12 weeks in patients with hepatitis C genotype 4 infection. Hepatology. 2016;64(4):1049–1056. | ||
Feld JJ, Moreno C, Trinh R, et al. Sustained virologic response of 100% in HCV genotype 1b patients with cirrhosis receiving ombitasvir/paritaprevir/r and dasabuvir for 12weeks. J Hepatol. 2016;64(2):301–307. | ||
Andreone P, Colombo MG, Enejosa JV, et al. ABT-450, ritonavir, ombitasvir, and dasabuvir achieves 97% and 100% sustained virologic response with or without ribavirin in treatment-experienced patients with HCV genotype 1b infection. Gastroenterology. 2014;147(2):359–365.e1. doi: 10.3851/IMP3037. | ||
Poordad F, Schiff ER, Vierling JM, et al. Daclatasvir with sofosbuvir and ribavirin for hepatitis C virus infection with advanced cirrhosis or post-liver transplantation recurrence. Hepatology. 2016;63(5):1493–1505. | ||
Charlton M, Everson GT, Flamm SL, et al. Ledipasvir and sofosbuvir plus ribavirin for treatment of HCV infection in patients with advanced liver disease. Gastroenterology. 2015;149(3):649–659. | ||
Manns M, Samuel D, Gane EJ, et al. Ledipasvir and sofosbuvir plus ribavirin in patients with genotype 1 or 4 hepatitis C virus infection and advanced liver disease: a multicentre, open-label, randomised, phase 2 trial. Lancet Infect Dis. 2016;16(6):685–697. | ||
Fontana RJ, Brown RS Jr, Moreno-Zamora A, et al. Daclatasvir combined with sofosbuvir or simeprevir in liver transplant recipients with severe recurrent hepatitis C infection. Liver Transpl. 2016;22(4):446–458. | ||
Welzel TM, Reddy KR, Flamm SL, et al. On-treatment HCV RNA in patients with varying degrees of fibrosis and cirrhosis in the SOLAR-1 trial. Antivir Ther. 2016;21(6):541–546. | ||
Pockros PJ, Reddy KR, Mantry PS, et al. Efficacy of direct-acting antiviral combination for patients with hepatitis C virus genotype 1 infection and severe renal impairment or end-stage renal disease. Gastroenterology. 2016;150(7):1590–1598. | ||
Saxena V, Koraishy FM, Sise ME, et al. Safety and efficacy of sofosbuvir-containing regimens in hepatitis C infected patients with impaired renal function. Liver Int. 2016;36(6):807–816. | ||
Nazario HE, Ndungu M, Modi AA. Sofosbuvir and simeprevir in hepatitis C genotype 1- patients with end-stage renal disease on hemodialysis or GFR <30mL/min. Liver Int. 2016;36(6):798–801. | ||
Castera L, Sebastiani G, Le Bail B, de Ledinghen V, Couzigou P, Alberti A. Prospective comparison of two algorithms combining non-invasive methods for staging liver fibrosis in chronic hepatitis C. J Hepatol. 2010;52(2):191–198. | ||
Coppola N, De Pascalis S, Pisaturo M, et al. Sustained virological response to antiviral treatment in chronic hepatitis C patients may be predictable by HCV-RNA clearance in peripheral blood mononuclear cells. J Clin Virol. 2013;58(4):748–750. | ||
Afdhal NH, Bacon BR, Patel K, et al. Accuracy of FibroScan, compared with histology, in analysis of liver fibrosis in patients with hepatitis B or C: a United States multicenter study. Clin Gastroenterol Hepatol. 2015;13(4):772–779.e1–3. | ||
Ortiz V, Berenguer M, Rayon JM, Carrasco D, Berenguer J. Contribution of obesity to hepatitis C-related fibrosis progression. Am J Gastroenterol. 2002;97(9):2408–2414. | ||
Ho SB, Brau N, Cheung R, et al. Integrated care increases treatment and improves outcomes of patients with chronic hepatitis C virus infection and psychiatric illness or substance abuse. Clin Gastroenterol Hepatol. 2015;13(11):2005–2014. | ||
Vespasiani-Gentilucci U, Galati G, Gallo P, De Vincentis A, Riva E, Picardi A. Hepatitis C treatment in the elderly: new possibilities and controversies towards interferon-free regimens. World J Gastroenterol. 2015;21(24):7412–7426. | ||
Cainelli F. Hepatitis C virus infection in the elderly: epidemiology, natural history and management. Drugs Aging. 2008;25(1):9–18. | ||
Younossi ZM, Stepanova M, Nader F, Henry L. Patient-reported outcomes of elderly adults with chronic hepatitis C treated with interferon- and ribavirin-free regimens. J Am Geriatr Soc. 2016;64(2):386–393. | ||
Elrazek AE, Amer M, Hawary B, et al. Prediction of HCV vertical transmission: what are factors should be optimized using data mining computational analysis. Liver Int. 2017;37(4):529–533. | ||
Tovo PA, Calitri C, Scolfaro C, Gabiano C, Garazzino S. Vertically acquired hepatitis C virus infection: correlates of transmission and disease progression. World J Gastroenterol. 2016;22(4):1382–1392. | ||
Poliquin V, Yudin MH, Murphy KE, Okun N. Antepartum screening for maternal infection and immune status: is it time to broaden our routine? J Obstet Gynaecol Can. 2015;37(12):1118–1121. | ||
Spera AM, Eldin TK, Tosone G, Orlando R. Antiviral therapy for hepatitis C: has anything changed for pregnant/lactating women? World J Hepatol. 2016;8(12):557–565. | ||
Granot E, Sokal EM. Hepatitis C virus in children: deferring treatment in expectation of direct-acting antiviral agents. Isr Med Assoc J. 2015;17(11):707–711. | ||
Jain S, Goharkhay N, Saade G, Hankins GD, Anderson GD. Hepatitis C in pregnancy. Am J Perinatol. 2007;24(4):251–256. | ||
Floreani A. Hepatitis C and pregnancy. World J Gastroenterol. 2013;19(40):6714–6720. | ||
Spaulding AC, Weinbaum CM, Lau DT, et al. A framework for management of hepatitis C in prisons. Ann Intern Med. 2006;144(10):762–769. | ||
Larney S, Kopinski H, Beckwith CG, et al. Incidence and prevalence of hepatitis C in prisons and other closed settings: results of a systematic review and meta-analysis. Hepatology. 2013;58(4):1215–1224. | ||
Bate JP, Colman AJ, Frost PJ, Shaw DR, Harley HA. High prevalence of late relapse and reinfection in prisoners treated for chronic hepatitis C. J Gastroenterol Hepatol. 2010;25(7):1276–1280. | ||
Kim AY, Nagami EH, Birch CE, Bowen MJ, Lauer GM, McGovern BH. A simple strategy to identify acute hepatitis C virus infection among newly incarcerated injection drug users. Hepatology. 2013;57(3):944–952. | ||
Hofer H, Watkins-Riedel T, Janata O, et al. Spontaneous viral clearance in patients with acute hepatitis C can be predicted by repeated measurements of serum viral load. Hepatology. 2003;37(1):60–64. | ||
Dore GJ, Hellard M, Matthews GV, et al. Effective treatment of injecting drug users with recently acquired hepatitis C virus infection. Gastroenterology. 2010;138(1):123–135. | ||
Grebely J, Matthews GV, Petoumenos K, Dore GJ. Spontaneous clearance and the beneficial impact of treatment on clearance during recent hepatitis C virus infection. J Viral Hepat. 2010;17(12):896. | ||
Martin NK, Vickerman P, Grebely J, et al. Hepatitis C virus treatment for prevention among people who inject drugs: modeling treatment scale-up in the age of direct-acting antivirals. Hepatology. 2013;58(5):1598–1609. | ||
Aspinall EJ, Corson S, Doyle JS, et al. Treatment of hepatitis C virus infection among people who are actively injecting drugs: a systematic review and meta-analysis. Clin Infect Dis. 2013;57(Suppl 2):S80–S89. | ||
Fragomeli V, Weltman M. Addressing viral hepatitis in the opiate substitution setting: an integrated nursing model of care. J Gastroenterol Hepatol. 2015;30(Suppl 2):6–11. | ||
Arora S, Thornton K, Murata G, et al. Outcomes of treatment for hepatitis C virus infection by primary care providers. N Engl J Med. 2011;364(23):2199–2207. | ||
Baker D, Alavi M, Erratt A, et al. Delivery of treatment for hepatitis C virus infection in the primary care setting. Eur J Gastroenterol Hepatol. 2014;26(9):1003–1009. | ||
Wade AJ, Macdonald DM, Doyle JS, et al. The cascade of care for an Australian community-based hepatitis C treatment service. PLoS One. 2015;10(11):e0142770. | ||
Ho SB, Bräu N, Cheung R, et al. Integrated care increases treatment and improves outcomes of patients with chronic hepatitis C virus infection and psychiatric illness or substance abuse. Clin Gastroenterol Hepatol. 2015;13(11):2005–2014.e1–3. | ||
National Health and Medical Research Council (NHMRC). Australian Guidelines to Reduce Health Risks from Drinking Alcohol. 2009. Available from: http://www.nhmrc.gov.au/_files_nhmrc/publications/attachments/ds10-alcohol.pdf. Accessed February 2016. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.