")
Back to Journals » Psychology Research and Behavior Management » Volume 15
Experiences of Work-Related Stress Among Female Healthcare Workers During the COVID-19 Public Health Emergency: A Qualitative Study in the United Arab of Emirates
Authors Hijazi H , Baniissa W , Al Abdi R , Al-Yateem N, Almarzouqi A , Rahman S, Alshammari R, Alameddine M
Received 24 July 2022
Accepted for publication 7 September 2022
Published 21 September 2022 Volume 2022:15 Pages 2701—2715
DOI https://doi.org/10.2147/PRBM.S381177
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Heba Hijazi,1,2 Wegdan Baniissa,3 Rabah Al Abdi,4 Nabeel Al-Yateem,3 Amina Almarzouqi,1 Syed Rahman,1 Rayya Alshammari,1 Mohamad Alameddine1
1Department of Health Services Administration, College of Health Sciences, University of Sharjah, Sharjah, United Arab Emirates; 2Department of Health Management and Policy, Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan; 3Nursing Department, College of Health Sciences, University of Sharjah, Sharjah, United Arab Emirates; 4Department of Biomedical Engineering, Faculty of Engineering, Jordan University of Science and Technology, Irbid, Jordan
Correspondence: Heba Hijazi, Department of Health Services Administration, College of Health Sciences, University of Sharjah, Sharjah, United Arab Emirates, Email [email protected]
Objective: Frontline healthcare workers experienced high levels of psychological distress and emotional turmoil due to the changes necessitated by the COVID-19 public health emergency. Given that workplace stress can negatively influence both quality of work, and job performance, this study sought to explore the lived experiences of work-related stress among female healthcare workers in United Arab of Emirates during the COVID-19 pandemic.
Methods: A qualitative phenomenological investigation was performed using a purposive sampling approach. A total of 26 semi-structured interviews were conducted with female healthcare workers who worked directly with COVID-19 patients. Using Giorgi’s descriptive method, the data were analyzed to identify the main themes.
Results: Three main themes emerged from the data analysis, with nine categories under these themes. The first theme was “sources of work-related stress.” The participants reported a high workload, fear of being infected and transmitting the virus to others, and uncertainty and lack of knowledge regarding COVID-19 to be the main sources of their work-related stress. The second theme was “challenges of working during the pandemic.” The participants related being challenged by changes in the organization of care, the need to use personal protective equipment, a work-life imbalance, and witnessing patients’ suffering. The third theme was “coping strategies.” The participants perceived having sources of social support and using self-adjustment skills to be helpful strategies in terms of coping with the stressful situations they experienced.
Conclusion: The findings suggest a number of strategies and interventions that could be used at the individual and institutional levels to promote the preparedness and efficacy of healthcare workers during future crises and public health emergencies.
Keywords: work-related stress, female healthcare workers, qualitative research, work experiences, healthcare professionals, COVID-19 pandemic, public health emergency
Introduction
The novel coronavirus disease 2019 (COVID-19), which was declared a global pandemic by the World Health Organization (WHO) in March 2020, placed a significant additional burden on healthcare systems worldwide, particularly on the health workforce.1 During the pandemic, healthcare workers (HCWs) were recognized to be among the groups considered most susceptible to infection with the virus due to their greater risk of occupational exposure to biological hazards, which caused increased levels of psychological distress, emotional turmoil, and depression among members of this group.2 According to a systematic review of 12 cross-sectional studies conducted in several countries during the pandemic, the pooled prevalence of depression and anxiety among HCWs were 22.8% and 23.2%, respectively.3
Based on the definition provided by the WHO, work-related stress is a response that workers may experience when the demands and responsibilities of their job do not match with their level of knowledge and capabilities, meaning that they feel overwhelmed or unable to cope.4 Research has shown that facing unmanageable pressures or demands in the workplace contributes to lower productivity, lower quality, increased errors, and reduced organizational effectiveness.5 It has been widely acknowledged that the types and sources of stress differ among individuals. For instance, females have been found to suffer more from the symptoms of stress than males.6,7 However, females appear to manage their stress better than males, and they are less likely to experience major depression brought on by work-related stress.6 Moreover, responses to increased work-related demands and stressful situations vary in terms of their intensity based on the individual’s age, marital status, occupation, and personal, social, and professional circumstances.8,9 While working in a professional environment has been found to play a vital role in enhancing an individual’s sense of financial and social stability, working in a demanding or challenging environment can also lead to certain complications, including difficulty concentrating, lack of motivation, interpersonal conflict, and other behavioral and psychological conditions.10
Stress is known to occur in a wide range of workplaces; however, the healthcare sector is considered to be among the most demanding work environments, even during non-pandemic times. In fact, the findings of recent studies have indicated that HCWs, especially females, face a higher risk of excessive stress and burnout, not only due to the likelihood of work overload, but also due the imbalance between professional and personal life commonly experienced by people in the healthcare sector.11,12
Until May 2022, systematic searches for qualitative research focusing on work-related stress among HCWs were conducted using PubMed, Scopus, EMBASE, and Web of Science. To facilitate literature review, three compartments of PICO framework (population, intervention, comparison, and outcome) were considered in the search strategy process.13 According to the PICO compartments, P denotes HCWs as the study population, I represent COVID-19 pandemic, and O represents stress. C, or the comparison group, was not investigated because there was no comparison group. Firstly, the search string was created for the PubMed database and then adapted for other interested databases. Our search findings showed that qualitative studies concerning the impact of the COVID-19 pandemic on HCWs’ experience of stress in the United Arab Emirates (UAE) has been limited. In view of that, the present study sought to fill the knowledge gap regarding how HCWs cope effectively with work-related stress and challenges taking into attempt the local context.
Given that workplace stress can negatively influence both quality of work and job performance, it is vital to strengthen the health system’s resilience to it, which can be informed by analyzing HCWs’ experiences during times of crisis. Several prior studies have emphasized the importance of identifying effective strategies for mitigating the feeling of stress among frontline HCWs due to COVID-19,14,15 and this study represents an attempt to provide health managers and policymakers with implications concerning interventions intended to promote the preparedness and efficacy of the healthcare workforce when it comes to crisis management. In the UAE, 64% of the healthcare workforce is female, which indicates the significant contribution made by women to the country’s healthcare industry.16 In light of this, the present study conducted an in-depth exploration of the lived experiences of work-related stress among female HCWs in the UAE during the COVID-19 pandemic.
Current Status of the COVID-19 Pandemic in the UAE
The UAE became the first country in the Middle East to announce a confirmed case of COVID-19 on 29 January 2020.17 Since then, the government of the UAE has worked to identify gaps and priorities in terms of the healthcare workforce, facilities, and availability of both medical devices and personal protective equipment (PPE) as a response to the global crisis. As of July 21, 2022, a total of 978,966 cases of COVID-19 have been confirmed in the UAE, with 2329 corresponding deaths. The country has administered at least 24,922,054 doses of different COVID-19 vaccines, meaning that 98% of the population is now fully vaccinated.18
Following the onset of the pandemic, the UAE’s Ministry of Health and Prevention (MoHAP) has established a coronavirus helpline, as well as a hotline offering mental health counselling, in an effort to respond to people’s psychological concerns and anxieties.19 Moreover, all licensing processes and procedures for healthcare settings, frontline workers, medical equipment, and technology have been amended to adapt to the ongoing crisis.20 In addition, local health authorities in the UAE have introduced mandatory weekly or bi-weekly COVID-19 testing for all HCWs.
Methods
Study Design
A qualitative research design with a phenomenological approach was applied in this study to better understand the participants’ experiences of work-related stress within its real-life context. The chosen methodology was not intended to provide generalized results; rather, the aim was to explore the phenomenon of interest in depth by encouraging the participants to freely describe their lived experiences during the first year of the COVID-19 pandemic.
Data Collection and Sampling Techniques
Using the semi-structured interview approach, qualitative data were collected from female HCWs who worked directly with confirmed COVID-19 cases. Each participant was telephoned to arrange an appointment for an online interview at a time that was convenient for them. To promote experience diversity, participants from different healthcare professions and hospitals in the Emirate of Sharjah were chosen to participate in the study, including nurses, physicians, radiologists, and medical laboratory technicians (MLTs). With a population of 1.2 million, Sharjah represents the third largest Emirate in terms of size, population, and numbers of healthcare facilities and HCWs in the UAE after Abu Dhabi and Dubai.16
The participating HCWs were identified using a purposive snowball sampling technique. This involved identifying and selecting HCWs who were particularly experienced in relation to the phenomenon of interest. Only adult HCWs who had a full-time job, provided direct care for COVID-19 patients, and had worked in the same institution for the last two years were eligible to participate. The latter inclusion criterion was applied to ensure that the HCWs had worked at the same hospital both before and during the pandemic. The involvement of the different HCWs in patient care included being in a direct contact with positive cases through treating, injecting, taking blood samples, and performing radiological examinations with regard to COVID-19 patients.
To facilitate the data collection process, a well-trained female interviewer contacted all the potential participants, all of whom agreed to participate in the study. Prior to the interviews, verbal consent was obtained from all the participants, with an emphasis on the voluntary nature of participation. All the participants were also informed that the online interviews would be recorded and that they had the right to skip any of the interviewer’s questions or to withdraw from the study at any time without penalty. During the interviews, which lasted for approximately 45–60 minutes, no script was used and only open-ended questions were asked. A total of 26 female HCWs were successfully interviewed during the period from March to August, 2021. This sample size was determined on a progressive basis until no new themes emerged and data saturation was reached.
The interview outline was developed and refined through a collaborative effort involving all the research team members (two clinical nursing experts and two psychologists). The following general question was first asked to all the participants: Please tell me about your experiences of taking care of COVID-19 patients during 2020. Next, the following additional open-ended questions were asked to obtain detailed descriptions of the phenomenon of interest: What differences were there between providing care before and during the pandemic? What caused you the most stress? Can you provide some examples of stressful situations you faced? What were some of the complications of stress you experienced? What challenges did you encounter? How did you handle those challenges? What external support have you received? What other support do feel that you still require? Moreover, probing questions were also used to enhance the depth of discussion, including the following: Can you explain further? What is your biggest fear regarding this issue? How would you describe the challenge you are facing? Information regarding each participant’s individual characteristics was also collected (ie, age, marital status, current profession, and years of experience).
Data Analysis
All the interviews were transcribed verbatim and stored electronically on a hard drive. The data analysis was performed based on Giorgi’s four-step phenomenological method.21 These four steps were as follows. First, getting to know the data by reading the entire transcript repeatedly to familiarize oneself with the data and understand the meanings conveyed. Second, identifying the units of meaning by breaking down the whole transcript into its constituent elements. Here, a unit of meaning consists of “those words, phrases, non-verbal or para-linguistic communication which express a unique and coherent meaning.”22 Third, transforming the units of meaning into descriptive expressions relative to the phenomenon of interest. Fourth, synthesizing and integrating the units of meaning that could be taken as true in most cases into a final general description. While each participant related unique and distinctive experiences, combining all the common perspectives together in a particular context helped to link the identified units of meaning and explore the differences and similarities among the constituents of meaning.
To generate an in-depth understanding of the HCWs’ lived experiences, all the transcribed interviews were read several times to ensure their completeness, which was followed by a sentence-by-sentence analysis. The coding of the interview data began once all the data were fully transcribed. These data were independently coded by two researchers (H.H. and R.A.). To ensure the intercoder reliability, Cohen’s kappa was computed, which indicated substantial agreement between the two coders (κ = 0.79).23 Once the coding was completed, the whole research team was involved in interpreting the data, identifying the emerging themes and categories, and highlighting any similarities and differences among the data. The themes and categories were developed using a combination of a hand coding procedure and a software package (NVivo version 10; QSR International Pty Ltd., Melbourne, Australia). All the authors agreed on the final thematic structure.
Ethical Approval
The data collection process commenced after approval to conduct the study was obtained from the Research Ethics Committee of the University of Sharjah (Reference number: REC-21-03-03-07-S). Participant informed consent was obtained before enrolment in this study, and analysis was performed on de-identified data. Confidentiality and anonymity of data are maintained as this study was conducted in accordance with the Declaration of Helsinki.
Results
The study sample consisted of eight nurses, seven physicians, six radiologists, and five MLTs. As shown in Table 1, the ages of the participating HCWs ranged from 25–48 years (median: 33 years). The participants’ length of work experience at their respective healthcare facilities ranged from 3–21 years (median: 7.5 years).
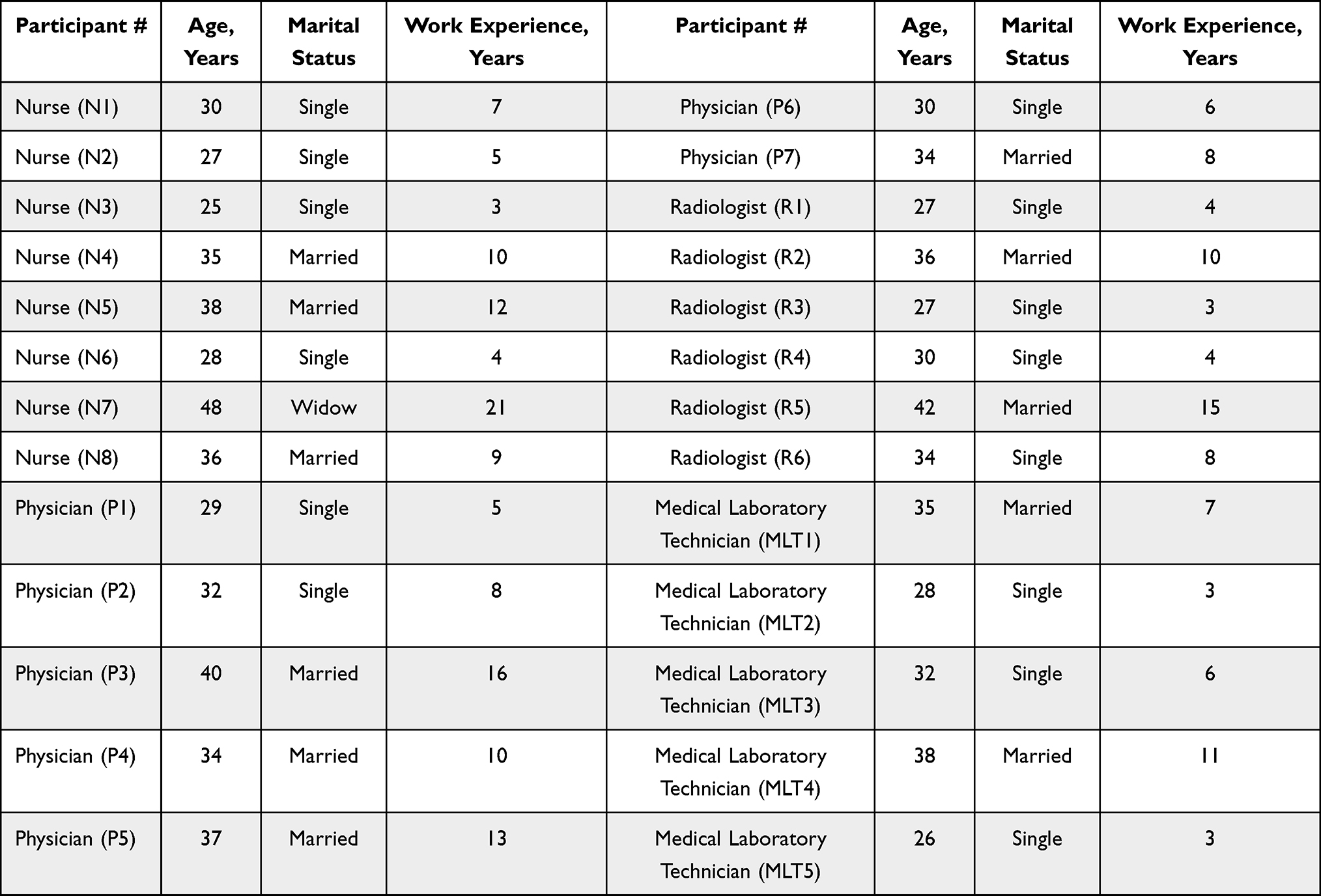 |
Table 1 Characteristics of Participants |
The analysis revealed three major themes that captured the participants’ experiences of work-related stress during the COVID-19 public health emergency: “sources of work-related stress”, “challenges of working during the pandemic”, and “coping strategies.” Table 2 presents the main themes, categories, and codes that emerged from the analysis. Representative quotations from the participants were used to verify and validate the study’s findings.
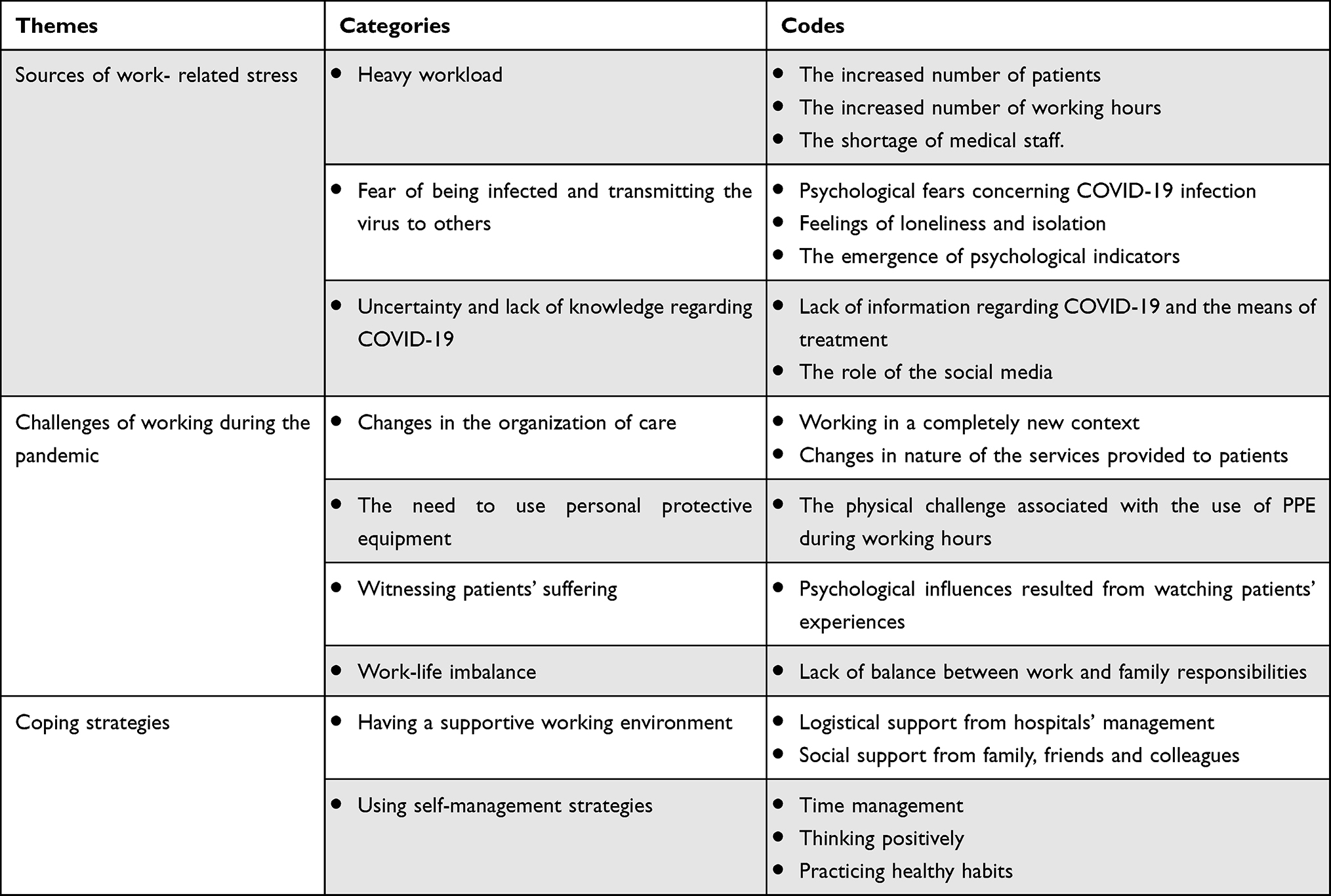 |
Table 2 The Main Themes, Categories, and Codes |
Theme 1: Sources of Work-Related Stress
In terms of this theme, three categories emerged: “heavy workload”, “fear of being infected and transmitting the virus to others”, and “uncertainty and lack of knowledge regarding COVID-19.”
Heavy Workload
All the participants reported that working during the pandemic was associated with high-intensity demands and a heavy workload due to a number of reasons, including the increase in the number of patients, the need to work long hours, and the shortage of medical staff.
Usually, the hospital occupancy rate is around 70%; however, during 2020, it reached 100%. All the beds in the ICU were fully occupied. (P2)
I was always overloaded and it negatively affected my way of doing things. I was doing multiple tasks at the same time. This caused me to make some mistakes and to have to repeat the tests again, which was really stressful. (MLT2)
The participants also indicated that they usually had one or two days off each week, although due to the increase in the number of positive and critical cases during the pandemic, their number of working days had increased, along with the number of working hours per shift.
At the beginning of the outbreak, there was an increase in our working days due to the constant increase in the number of critically ill COVID-19 patients who required continuous care and monitoring. (P1)
During the peak of the pandemic, the number of working hours increased from eight hours to twelve hours due to the increased number of patients. Sometimes, we couldn’t even find time to eat. (N2)
The participants further mentioned that the staffing levels of several departments declined during the pandemic, which resulted in an excessive workload for those who remained.
The workload actually doubled because the number of workers decreased due to their infection. In some shifts, I had to work until the next day to fill the work gap. In cases of infection, staff members needed to stay quarantined until they received a negative result. (MLT4)
As per the hospital’s new precautionary measures, the number of medical staff was reduced to limit crowding. For example, from March to July 2020, only two radiologists were allowed to work simultaneously in the department. (R1)
Fear of Being Infected and Transmitting the Virus to Others
This category comprised the HCWs’ psychological fears concerning COVID-19 infection. The participants expressed how being in close contact with positive cases was one of the main workplace stressors, because it placed them at higher risk of getting infected and, therefore, at higher risk of passing on the virus to others (ie, partners, parents, children, and colleagues).
I am a widow and I have three kids who are totally dependent on me physically, emotionally, and economically. I was always thinking about what would happen to my kids if I was infected and died. Thinking about the possibility that I may leave them alone in this world was quite stressful. (N7)
All the HCWs, especially those who lived with elderly parents or sick children, reported a strong commitment to consistently maintaining a social distance from their family members in an effort to reduce the potential risk of infecting them. Furthermore, the participants stated that many of their friends had started to avoid them during the pandemic, which triggered feelings of loneliness and isolation.
I didn’t care about myself, but I was worried about my son who has low immunity. If he had become infected, I would have blamed myself for not protecting him. (N4)
My mother was seventy-four years old and she had cancer, so every time I got home I felt stressed. I was always taking all precautions to stay away from her. Being physically apart from my mom was really rough. (P5)
With the onset of the pandemic, people started to stay away from me. For example, most of my close friends and relatives maintained a social distance when they communicated with me, and they refrained from visiting my house. Feeling a sense of social alienation was hard. (R3)
Interestingly, the participants also reported that after they started to come into direct contact with COVID-19 patients, a number of psychological indicators emerged, including obsessive thoughts regarding contamination, compulsive washing, insomnia, irritability, and mood changes.
I started biting my nails after the outbreak. What made me even more nervous was the presence of the virus. For example, every time I realized what I was doing, I spent two to three days waiting for the appearance of infection symptoms. (R4)
I experienced frequent and prolonged nocturnal awakenings during the first six months of the pandemic. (N6)
I became moody and sensitive with others. I have to admit that I sometimes overthought things, but most people didn’t understand that the stress stemming from dealing with positive cases was double or even triple. (P7)
Uncertainty and Lack of Knowledge Regarding COVID-19
The participants repeatedly pointed out that one of the major workplace stressors was the lack of information about how to treat patients with the new disease. The level of risk, the modes of transmission, and the means of treatment were all ambiguous at the start of the pandemic. However, this kind of uncertainty declined to some extent over time.
As you know, we had never heard of or studied COVID-19, so a lack of confidence about how to treat COVID-19 patients and prevent the spread of the virus placed us under extra strain. (N1)
Some of the symptoms that we saw in patients were really new. I had personally never seen similar compilations before, which created a feeling of fear about this ambiguous disease. (P6)
According to the participants, the rapid spread of news about the disease via the social media and the high numbers of reported deaths both further elevated their stress levels during the pandemic.
The rumors regarding COVID-19 and its modes of transmission increased dramatically on television and social media during the first year of the pandemic. Furthermore, there was a lack of sufficient medical information and scientific research about the virus. (P7)
Theme 2: Challenges of Working During the Pandemic
The second theme comprised four categories. The participants mentioned that they had to cope with different physical and psychological challenges during the first year of the pandemic, including changes in the organization of care, the need to use PPE, witnessing patients’ suffering, and a work-life imbalance.
Changes in the Organization of Care
Working in a completely new context exacerbated the feelings of stress and pressure among the HCWs. All the participating physicians and nurses reported that their working environment was progressively changed to prevent the transmission of the virus and reduce mortality. For example, the hospital wards and emergency room (ER) were restructured, additional preventive measures were introduced, and access to those involved in care was restricted.
Our hospital specified isolation wards for confirmed positive cases, so it was not allowed for staff involved in the care of COVID-19 patients to work in other departments. It was real isolation, not only for the patients, but also for us. (N3)
As per the hospital’s new restrictions, medical staff who entered the contaminated areas had to be provided with the highest level of protection. No one could enter those areas without using additional PPE. All these changes put us under additional stress. (P4)
Due to the increased number of positive cases, many regular wards were transformed into isolation wards within a short period of time. The real challenge was that some of the new wards were not well equipped or adequately prepared to treat COVID-19 patients. (P2)
The participants mentioned that the nature of the services provided also changed as a result of the pandemic. For example, many critically ill patients required non-routine procedures and interventions; however, the performance of such procedures and interventions was beyond the HCWs’ level of expertise. Moreover, the participants added that they played a crucial role in assisting patients with their daily living activities, including eating, dressing, using the toilet, and moving around.
The majority of patients were not accompanied by their families, which meant that we had to provide them with additional physical and emotional support. No matter how busy I was, I tried my best to help them with anything they asked for. (N2)
All the patients on ventilators needed extra care and monitoring, because sometimes the ventilator’s parameters needed to be adjusted based on the patient’s status. I had to learn how to master these new procedures within a short time. (P3)
The Need to Use PPE
The participating HCWs repeatedly mentioned that the need to use PPE represented a major physical challenge during working hours. Using PPE involved wearing protective clothing, helmets, goggles, respirators, or other garments. The most common problems associated with using PPE were excessive sweating, the fogging of goggles, breathlessness, nasal pain, fatigue, headache, pain at the root of the pinna, and skin allergy or dermatitis. Some participants further expressed how wearing a full protective ensemble increased the sense of disconnection from other patients and staff and also led to ineffective communication due to a lack of speech clarity.
Wearing the protective clothing posed a significant challenge to building a rapport with patients. It was really difficult to hear what the patients were saying. (N5)
I could not tolerate wearing the full protective ensemble for several hours. It was really uncomfortable and increased my temperature, leaving my clothes drenched in sweat. (MLT1)
My protective goggles became blurred if I wore them with the mask. This made my work harder and more complicated. For example, I couldn’t see well while giving patients their medications. (N8)
Wearing the protective helmet, mask, or face shield meant that we could not eat or drink easily. Sometimes, we spent half of the day without eating anything. I lost seven kilograms last year. (R5)
I have asthma and wearing the face mask made me feel that I couldn’t breathe adequately. It was really challenging to put it on for a long time. (R3)
Witnessing Patients’ Suffering
Unsurprisingly, the HCWs were affected psychologically by their patients’ conditions. The physicians and nurses expressed how they felt happy, relaxed, and proud when a patient’s health status improved. However, if they witnessed the rapid deterioration and sudden death of a patient, they felt disappointed, depressed, and powerlessness.
When patients showed improvements, I felt relief that I was able to provide them with the required treatments. However, the death of any of them made me feel sad and depressed, especially if I was supervising the patient for a long time. (P1)
One of the hardest moments I have ever faced was a young lady who lost both of her parents in two days. She cried heartily beside her mother’s bed. Both of her parents were quite young and healthy before catching COVID. It was extremely painful; I cried. (N4)
Work-Life Imbalance
All the participants revealed how the pandemic had negatively influenced their personal and social lives. The married participants were more likely to have faced additional difficulties in terms of striking a balance between their work and family responsibilities, especially those with minor children.
All the schools closed in March 2020. My kids, who were in the first and second grades, had to stay at home and study online. They didn’t even know how to use the computer, so it was a challenge to find someone to stay with them. (N5)
I was overwhelmed most of the time. I didn’t have time even for myself. Besides my housework and childcare responsibilities, I had to be nice and smiley with others all the time. No one understood how challenging it was. I am a human and I have my limits. (P3)
In addition to my job, I was studying for a master’s degree in radiology. Also, as a mother of six children, I was responsible for their well-being, safety, nutrition, and education. It was really challenging to be a full-time employee, a mother, a wife, and a student all at the same time. (R5)
Theme 3: Coping Strategies
The third theme consisted of two categories: “having a supportive work environment” and “using self-management strategies.”
Having a Supportive Work Environment
The participants repeatedly identified the presence of logistical support from their hospitals’ management, as well as encouragement and emotional support from their colleagues, as contributing to enhancing their sense of safety and well-being. Family support was also reported to be an essential means of reducing feelings of stress and maintaining a balanced life.
I have a supportive husband who understood very well the stress associated with being a physician during the pandemic. It was really important to have someone who was willing to listen. Talking to close friends and colleagues and sharing with them some work experiences was also helpful in terms of feeling relief. (P5)
One lesson I learned from the pandemic is how family gatherings are important. The outbreak made me appreciate the value of being with my parents, brother, and sisters. Their presence in my life is a really good stress reliever. (MLT2)
The hospital management took all precautions to ensure a safe working environment for us. They also provided us with adequate training to deal with COVID-19 patients and all the necessary protective equipment. (R6)
Using Self-Management Strategies
All the participants reported making use of certain self-management strategies to cope with workplace stressors and challenges, including time management (ie, preparing to-do lists, planning ahead, and prioritizing tasks), thinking positively (ie, positive self-talking and avoiding negative thinking), and practicing healthy habits (ie, doing exercise, praying and reading the holy book, eating a healthy diet, and listening to music).
I suffered from a panic attack while I was wearing a hazmat suit. One of my colleagues advised me to start taking medication. I know medications have side effects so instead I decided to start thinking positively and avoid tracking the numbers of COVID-19 cases and deaths. (N7)
I purchased a treadmill and started exercising. It really helped to reduce my negative energy. (R2)
I used several strategies to mitigate daily stress, such as having deadlines for all tasks, taking mini-breaks, and setting goals and priorities. (MLT1)
The pandemic brought me closer to God and strengthened my spiritual and religious belief that God takes care of everyone in this life and that there is a reason for everything, including traumatic events. (P6)
Leaving work-related issues behind in the workplace and not bringing them into the home was an effective way of achieving a healthy balance between work and leisure. When we think about health, we should also consider our own health to be a priority. (MLT3)
Discussion
This study sought to explore the lived experiences of stress among female HCWs during the COVID-19 public health emergency in the Emirate of Sharjah. The results showed that frontline female HCWs experienced a high workload to be one of their main workplace stressors due to several reasons, including the increased working hours, the shortage of medical staff, and the increased number of patients. This finding is consistent with the results of other studies, where an excessive workload was also found to be a risk factor for increased mental stress among healthcare professionals during the pandemic.24–26 According to a recent quantitative study conducted in the UAE (n = 1290), around 26% and 53% of participating HCWs reported feelings of anxiety and burnout, respectively, while working during the COVID-19 pandemic.17 The same study found that the burnout and anxiety scores differed significantly based on the numbers of working hours per night shift, indicating that the increase in HCWs’ workload may have negatively impacted their mental health.17
This study’s findings further revealed that the participants were afraid of unintentional occupational exposure to COVID-19 due to the nature of their contact with patients (eg, treating and injecting positive cases, taking blood samples, touching patients’ personal belongings, etc.). According to a qualitative study conducted in 2020, the fear of becoming infected with COVID-19 was identified among all the participating caregivers, and it was determined to cause additional psychological effects and extreme stress among them.27 One possible interpretation of this finding that is women generally tend to be overly concerned about life events, leading them to anticipate more negative impacts of the disease on their own health and the health of their significant others.7,28,29 In this context, a recent study found that alleviating the fears associated with COVID-19 infection would positively contribute to increasing positivity and reducing feelings of depression, anxiety, and stress.6
This study also showed that the uncertainty and lack of knowledge regarding COVID-19 acted as stressors during the pandemic. According to the participants, the spreading of rumors about COVID-19 through social networking platforms contributed to an increased feeling of stress. This finding is in line with the results of a Chinese study, wherein greater exposure to news concerning the pandemic via social media was found to be associated with having more mental health problems.30 Another Chinese study investigated gender differences in terms of experiences of depression and anxiety among social media users and found that female users experienced more severe stress and anxiety symptoms than males.31 One possible explanation for this is that people perceive COVID-19 to be a threat and, therefore, use social media as a means of mitigating uncertainty. While doing so may help individuals to obtain more information about the virus and the associated risks, the increased use of social media may also expose them to additional rumors, which could greatly exacerbate their negative emotions and heighten their risk of mental health disorders.30 In light of this, the findings of the present study suggest that HCWs need to minimize their search for information to only reliable news sources during public health emergencies.
Although HCWs are commonly exposed to different types and levels of patient care, the nature of the health services they provided changed during the pandemic. For instance, additional preventive measures and restrictions were introduced in healthcare settings, while many COVID-19 patients were found to require non-routine procedures and interventions. As a consequence, providing HCWs with specialized training on how to deal with patients during major outbreaks seems essential to adapting to sudden and significant work-related changes and helping HCWs to improve their ability to work under stress. This includes offering HCWs sufficient training on technical issues such as ventilator operation, the use of PPE and N95 masks, taking test samples using nasopharyngeal swabs, and handling the bodies of deceased COVID-19 patients.24 A study by Feroz et al illustrated how adequate training should be given to all medical personnel across the hospital in order to prepare a central backup plan.32 Such a plan would allow HCWs to effectively respond to staff shortages due to infection and quarantine and, therefore, reduce their work-related stress. A similar finding was reported in another study.33 As the priority during a public health emergency is to address the acute needs of patients, healthcare leaders and managers should routinely provide training to HCWs and ensure emergency preparedness before they are faced with such an emergency. Additional virtual training programs could also be offered during an emergency, depending on how the situation unfolds.
Due to the severity of the COVID-19 pandemic increasing, the WHO recommended the use of PPE as an essential strategy for reducing the airborne transmission of the virus and saving lives.34 This recommendation seems to have created controversy among workers in many professions, including HCWs. There appears to be a consensus in recent studies that the use of PPE is perceived as uncomfortable, cumbersome, a nuisance, or inconvenient.34,35 For example, a cross-sectional study conducted in a Moroccan hospital reported that the increased use of PPE, especially high-filtrating masks, was responsible for causing headaches among frontline HCWs during the pandemic.36 The HCWs also reported reduced concentration and lower performance when compared with working without PPE. In a study conducted by Ong et al in Singapore, the prevalence of de novo PPE-associated headache was found to be 81% among frontline HCWs when using N95 masks and protective eyewear.37 The authors mentioned that other important factors could potentially have worsened the HCWs’ pre-existing headaches, including sleep deprivation, physical and emotional stress, irregular meal times, and inadequate hydration.37 In the same context, studies have found that covering the face can cause a great deal of stress or even panic, and it may cause negative feelings about identity or body image due to changing the way a person looks.38
Another challenge that emerged in this study concerned the work-life imbalance during the pandemic, especially among the married HCWs. In the context in which the present study was conducted, women are typically the predominant caregivers for their families, meaning that they are expected to carry out most of the tasks related to childrearing and household labor.39 Previous studies have found that women with a greater caregiver burden face greater mental and physical strain, in addition to higher levels of stress.40 During the pandemic, the closure of schools and daycare centers resulted in an additional burden for working mothers, particularly those with minor children and partners who had the same working pattern. The findings of a recent study demonstrated that the pandemic negatively impacted women’s ability to strike a balance between their personal and professional lives.41 Many women experienced feelings of guilt due to the conflict between their tasks in the public and private spheres, leaving them feeling more stressed and frustrated and less satisfied with their life.41 Drawing on prior research, some women were also found to make an extra effort to hide their feelings of stress and anxiety from their children and partners in order to ease the atmosphere in the home and keep the family calm. This invisible mental work could represent a major source of stress that may affect women’s mental and physical health.41–43 Healthcare system stakeholders and institutional leaders in the Emirate of Sharjah must commit to the systematic assessment of workers’ work-life balance, especially female HCWs, and they must offer evidence-based support programs and interventions to help restore the balance and prevent both burnout and turnover.
In the current study, a number of HCWs also felt challenged by witnessing the worsening situation of the COVID-19 patients they were treating. Indeed, watching the rapid deterioration and sudden death of patients increased the HCWs’ feeling of helplessness, as they were unable to improve the health outcomes of these patients. Such a feeling of powerless might also increase the HCWs’ sense of guilt, leading some of them to experience psychological distress. Various studies have found witnessing patients’ experiences to be difficult for both nurses and physicians.24,44–46 Furthermore, becoming stressed and feeling helpless are dependent not only on personal characteristics, but also on the presence of situational factors that surround the death event.47 Accordingly, healthcare managers should provide HCWs, especially females, with professional psychological counseling and guidance as a routine, rather than offering such services only when HCWs are seen to be mentally struggling.
To further improve the work-related experiences of HCWs during times of crises, this study sought to develop some recommendations with regard to facing work-related challenges and stressors. The analysis indicated that the use of certain self-regulation strategies was helpful for the HCWs in terms of coping with the stressful situations experienced, including practicing healthy habits, time management, and thinking positively.6 Such stress-relieving activities also included making time for reading, watching movies, taking a shower, eating good food, or having quiet time.48 Moreover, the analysis revealed that positive thinking was one of the coping strategies used by the participants to manage their work-related stress. Aside from the belief that maintaining healthy thinking patterns is important when it comes to achieving happiness, prior studies have demonstrated that thinking positively helped HCWs to cope with their daily work-related stress during the pandemic.1 One potential explanation for these findings is that the use of self-adjustment skills can help build individuals’ resilience to challenges, which may contribute to maintaining a good mood and, therefore, serve to relieve feelings of pressure and stress. This argument is supported by the results of a recent study, which found developing resilience to be an effective stress management behavior among nurses in the UAE.49
The results of this study also illustrated how the participating HCWs appreciated the presence of many sources of support during the pandemic. Similarly, previous research has shown that when hospital management has ensured a supportive environment for HCWs, feelings of negative emotions and challenges have been minimized and the ability to effectively deal with stressful situations has been improved.32 Receiving familial support and having regular conversations with colleagues were reported to be additional essential coping mechanisms that provided the HCWs with a sense of mental strength and allowed them to stay positive during the crisis.24 Undoubtedly, the intensive work could drain HCWs both physically and mentally, which indicates that the provision of institutional support should be a key strategy for safeguarding their well-being and enhancing their ability to manage during difficult times.
Implications for Interventions
Below are some suggested implications of the findings, within the context of the UAE in general and Sharjah in particular, for HCWs, healthcare managers, and decision makers seeking to enhance preparedness and responses to possible future COVID-19 waves or other outbreaks.
Supportive Institutional Environment
Given that the pandemic proved frightening for HCWs due to its complex nature, it is essential to find ways to foster a sense of calm and safety among the healthcare workforce. The UAE’s health authorities need to develop and implement mental health intervention programs to protect the psychological well-being of HCWs and help them overcome the consequences of the COVID-19 pandemic. Accordingly, HCWs’ mental health should be continuously monitored, and professional psychological counselling must be provided when necessary.
Healthcare managers should also ask their workers about the obstacles they have encountered while working during the pandemic. Based on the HCWs’ responses, plans for the future can be developed to form a protective strategy capable of meeting HCWs’ needs and expectations. This may include recruiting more HCWs, introducing more reasonable work schedules, increasing the availability of necessary medical equipment, developing a strong system of information sharing at the organizational level, and providing HCWs with appropriate training on the use of such equipment.
Social Engagement and Support
It has been widely acknowledged that receiving social support can increase individuals’ emotional and cognitive capacities, which indicates that maintaining constant channels of communication with significant others is beneficial when it comes to reducing the feeling of stress. The use of technology (ie, telephone calls or video conferencing) could be a good means of staying in touch with others during times of crisis. Small gatherings after work during which problems can be shared, as well as participating in other recreational activities and spending quality time socializing, can all play an important role in reducing the feeling of work-related stress. Introducing various practices intended to strengthen HCWs’ work-life balance, such as flexible work arrangements, alternative work times, and child/elder care facilities, could be an effective strategy for making their life more comfortable.
Positive Thinking and Hope
Encouraging healthy thinking patterns could be a useful strategy for ensuring a feeling of calmness and helping HCWs adapt to changes. To achieve such goals, HCWs may need to limit how much they think about negative events (eg, virus infection). They may also need to train their minds and emotions so that they can think positively and calm themselves when feeling stressed or anxious. Some other strategies for increasing the emotional and cognitive capacities of HCWs include doing regular physical exercise and participating in a mindfulness-based stress reduction program. Practicing spiritual and religious traditions such as strong faith, commitment to prayers, and reading can also contribute to increasing individuals’ hope and reducing their stress.
Moreover, HCWs need to find meaning in their experiences and to feel proud of themselves for being able to save patients’ lives when facing risks and danger. Enhancing HCWs’ sense of achievement, self-esteem, and confidence could be an effective strategy for helping them overcome the difficulties associated with working under stress. Constantly looking for positives should enable HCWs to continuously improve their self-regulation skills while remaining focused and motivated.
Strengths and Limitations
A key strength of this study is the fact that to the best of the researchers’ knowledge, it is the first qualitative study conducted in Sharjah (UAE) to explore female HCWs’ lived experiences of work-related stress during the early stages of the COVID-19 pandemic. Another strength is its targeting of different healthcare professions, rather than focusing solely on nurses and physicians as most prior research on COVID-19 has done. Yet, this study also had some limitations. First, the participants were limited to HCWs in the Emirate of Sharjah, which means that the results may not be generalizable to HCWs in other UAE Emirates or other countries. Moreover, to minimize the risk of infection during the pandemic, the data were collected via telephone interviews, which means that the researchers did not have a real chance to build a rapport with the participants. Despite the use of a purposive snowball sampling technique for the data collection, it is still possible that the sample belongs to a particular subgroup of HCWs who were interested in participating in the study, which means that the representativeness of the sample is not guaranteed. Nevertheless, the study sample was substantially larger than the samples of several previous qualitative studies that explored the perceptions of HCWs.24,27,45,46 As with all qualitative research, the findings of this study may be subject to research bias; however, the entire data coding procedure was reviewed and finalized with the consent of all the authors.
Future studies could perform a comparative analysis of the levels of stress among HCWs during the COVID-19 public health emergency and after the pandemic conditions eased. Exploring male experiences of stress should also be considered to provide more detailed information about gender differences in terms of stress responses during crises.
Conclusion
Although the COVID-19 pandemic has had adverse consequences for HCWs’ mental and physical health, as well as for their lives more generally, many other aspects related to their mental health need to be considered. HCWs in other roles are also exposed to various sources of stress, which means that the findings of this study provide an initial evidence of HCWs’ lived experiences of stress and highlight some of the work-related challenges encountered by them during the pandemic. Addressing the main workplace stressors and challenges should help reduce the psychological hazards that HCWs may face while working under pressure, thereby potentially having a positive impact on the quality of the services provided to patients in healthcare settings. The use of multiple support systems and self-adjustment skills could play an important role in mitigating HCWs’ work-related stress. In light of all this, the findings of the present study suggest a number of strategies and interventions that could be used at the individual and institutional levels to promote preparedness and efficacy in relation to crisis management.
Abbreviations
COVID-19, Coronavirus Disease 2019; ER, Emergency Room; HCWs, Healthcare Workers; MLTs, Medical Laboratory Technicians; MoHAP, Ministry of Health and Prevention; PPE, Personal Protective Equipment; PICO, Population, Intervention, Comparison, and Outcome; UAE, United Arab Emirates; WHO, World health Organization.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Acknowledgment
The authors would like to sincerely thank all healthcare workers for their willingness to participate in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. All the authors dedicated their additional working hours to develop this paper.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. McFadden P, Ross J, Moriarty J, et al. The role of coping in the wellbeing and work-related quality of life of UK health and social care workers during COVID-19. IJERPH. 2021;18(2):815. doi:10.3390/ijerph18020815
2. Xiong J, Lipsitz O, Nasri F, et al. Impact of COVID-19 pandemic on mental health in the general population: a systematic review. J Affect Disord. 2020;277:55–64. doi:10.1016/j.jad.2020.08.001
3. Pappa S, Ntella V, Giannakas T, Giannakoulis VG, Papoutsi E, Katsaounou P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: a systematic review and meta-analysis. Brain Behav Immun. 2020;88:901–907. doi:10.1016/j.bbi.2020.05.026
4. World Health Organization. Occupational health: stress at the workplace; 2020. Available from: https://www.who.int/news-room/q-A-detail/ccupational-health-stress-at-The-workplace.
5. Jacobs CM. Ineffective-Leader-Induced Occupational Stress. SAGE Open. 2019;9(2):215824401985585. doi:10.1177/2158244019855858
6. Bakioğlu F, Korkmaz O, Ercan H. Fear of COVID-19 and positivity: mediating role of intolerance of uncertainty, depression, anxiety, and stress. Int J Ment Health Addiction. 2021;19(6):2369–2382. doi:10.1007/s11469-020-00331-y
7. Alsalman A, Mubarak H, Aljabal M, et al. The psychological impact of COVID-19 pandemic on the population of Bahrain. SSRN J. 2020. doi:10.2139/ssrn.3660648
8. Liu CH, Doan SN. Psychosocial stress contagion in children and families during the COVID-19 pandemic. Clin Pediatr. 2020;59(9–10):853–855. doi:10.1177/0009922820927044
9. Ojha J, Bhandari T, Karki R. Job stress and its associated factors among working women in Pokhara Metropolitan, Nepal. J Sci Soc. 2020;47(2):105. doi:10.4103/jss.JSS_50_20
10. Overton A, Lowry A. Conflict management: difficult conversations with difficult people. Clin Colon Rectal Surg. 2013;26(04):259–264. doi:10.1055/s-0033-1356728
11. De Hert S. Burnout in healthcare workers: prevalence, impact and preventative strategies. LRA. 2020;13:171–183. doi:10.2147/LRA.S240564
12. Baniissa W, Al Nusair H, AlTamimi A, et al. Posttraumatic stress disorders and influencing factors during the COVID-19 pandemic: across-sectional study of frontline nurses. Int Nurs Rev. 2022;69:285–293. doi:10.1111/inr.12734
13. Ghahramani S, Lankarani KB, Yousefi M, Heydari K, Shahabi S, Azmand S. A systematic review and meta-analysis of burnout among healthcare workers during COVID-19. Front Psychiatry. 2021;12:758849. doi:10.3389/fpsyt.2021.758849
14. Albott CS, Wozniak JR, McGlinch BP, Wall MH, Gold BS, Vinogradov S. Battle buddies: rapid deployment of a psychological resilience intervention for health care workers during the COVID-19 pandemic. Anesth Analg. 2020;131(1):43–54. doi:10.1213/ANE.0000000000004912
15. Blake H, Bermingham F, Johnson G, Tabner A. Mitigating the Psychological Impact of COVID-19 on healthcare workers: a digital learning package. Int J Environ Res Public Health. 2020;17(9):E2997. doi:10.3390/ijerph17092997
16. MOHAP. UAE National Health Workforce Account (NHWA); 2019. Available from: https://mohap.gov.ae/en/open-data/mohap-open-data.
17. Ajab S, Ádam B, Al Hammadi M, et al. Occupational health of frontline healthcare workers in the United Arab Emirates during the COVID-19 Pandemic: a Snapshot of Summer 2020. IJERPH. 2021;18(21):11410. doi:10.3390/ijerph182111410
18. Ministry of Health and Prevention (MOHaP). Recent COVID-19 Information and Updates. Available from: https://mohap.gov.ae/en/covid-19.
19. Hosani FA, Aden B, Memari SA, et al. Epidemiology of asymptomatic and symptomatic coronavirus disease 2019 confirmed cases in the Emirate of Abu Dhabi, United Arab Emirates: observational study. Medicine. 2021;100(12):e25219. doi:10.1097/MD.0000000000025219
20. Department of Health—Abu Dhabi. Abu Dhabi’s health workforce management system. Available from: https://www.doh.gov.ae/en/.
21. Giorgi A. The Descriptive Phenomenological Method in Psychology: A Modified Husserlian Approach. Duquesne University Press; 2009:xiv, 233.
22. Hycner RH. Some guidelines for the phenomenological analysis of interview data. Hum Stud. 1985;8(3):279–303. doi:10.1007/BF00142995
23. McHugh ML. Interrater reliability: the kappa statistic. Biochem Med. 2012;22(3):276–282. doi:10.11613/BM.2012.031
24. Razu SR, Yasmin T, Arif TB, et al. Challenges faced by healthcare professionals during the COVID-19 pandemic: a qualitative inquiry from Bangladesh. Front Public Health. 2021;9:647315. doi:10.3389/fpubh.2021.647315
25. Xiao C, Novel A. Approach of consultation on 2019 novel coronavirus (COVID-19)-related psychological and mental problems: structured letter therapy. Psychiatry Investig. 2020;17(2):175–176. doi:10.30773/pi.2020.0047
26. Wang C, Pan R, Wan X, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) Epidemic among the General Population in China. IJERPH. 2020;17(5):1729. doi:10.3390/ijerph17051729
27. Sun N, Wei L, Shi S, et al. A qualitative study on the psychological experience of caregivers of COVID-19 patients. Am J Infect Control. 2020;48(6):592–598. doi:10.1016/j.ajic.2020.03.018
28. Broche-Pérez Y, Fernández-Fleites Z, Jiménez-Puig E, Fernández-Castillo E, Rodríguez-Martin BC. Correction to: gender and Fear of COVID-19 in a Cuban Population Sample. Int J Ment Health Addiction. 2020. doi:10.1007/s11469-020-00377-y
29. Sriharan A, Ratnapalan S, Tricco AC, et al. Occupational stress, burnout, and depression in women in healthcare during COVID-19 pandemic: rapid scoping review. Front Glob Womens Health. 2020;1:596690. doi:10.3389/fgwh.2020.596690
30. Zhao N, Zhou G. Social media use and mental health during the COVID‐19 pandemic: moderator role of disaster stressor and mediator role of negative affect. Appl Psychol Health Well-Being. 2020;12(4):1019–1038. doi:10.1111/aphw.12226
31. Hou F, Bi F, Jiao R, Luo D, Song K. Gender differences of depression and anxiety among social media users during the COVID-19 outbreak in China: across-sectional study. BMC Public Health. 2020;20(1):1648. doi:10.1186/s12889-020-09738-7
32. Feroz AS, Pradhan NA, Hussain Ahmed Z, et al. Perceptions and experiences of healthcare providers during COVID-19 pandemic in Karachi, Pakistan: an exploratory qualitative study. BMJ Open. 2021;11(8):e048984. doi:10.1136/bmjopen-2021-048984
33. Vera san juan N, Clark SE, Camilleri M, et al. Training and redeployment of healthcare workers to intensive care units (ICUs) during the COVID-19 pandemic: a systematic review. BMJ Open. 2022;12(1):e050038. doi:10.1136/bmjopen-2021-050038
34. Scheid JL, Lupien SP, Ford GS, West SL. Commentary: physiological and psychological impact of face mask usage during the COVID-19 Pandemic. IJERPH. 2020;17(18):6655. doi:10.3390/ijerph17186655
35. Rebmann T, Carrico R, Wang J. Physiologic and other effects and compliance with long-term respirator use among medical intensive care unit nurses. Am J Infect Control. 2013;41(12):1218–1223. doi:10.1016/j.ajic.2013.02.017
36. Hajjij A, Aasfara J, Khalis M, Ouhabi H, Benariba F, El Kettani C. Personal protective equipment and headaches: cross-sectional study among Moroccan healthcare workers during COVID-19 pandemic. Cureus. 2020. doi:10.7759/cureus.12047
37. Ong JJY, Bharatendu C, Goh Y, et al. Headaches associated with personal protective equipment – a cross‐sectional study among frontline healthcare workers during COVID‐19. Headache. 2020;60(5):864–877. doi:10.1111/head.13811
38. Howard MC. Gender, face mask perceptions, and face mask wearing: are men being dangerous during the COVID-19 pandemic? Pers Individ Dif. 2021;170:110417. doi:10.1016/j.paid.2020.110417
39. Mittal M, Bhakar SS. Examining the impact of role overload on job stress, job satisfaction and job performance-A study among married working women in banking sector. IJMS. 2018:01. doi:10.18843/ijms/v5i2(7)/01
40. Sharma N, Chakrabarti S, Grover S. Gender differences in caregiving among family - caregivers of people with mental illnesses. WJP. 2016;6(1):7. doi:10.5498/wjp.v6.i1.7
41. Hjálmsdóttir A, Bjarnadóttir VS. “I have turned into a foreman here at home”: families and work–life balance in times of COVID‐19 in a gender equality paradise. Gender Work Organ. 2021;28(1):268–283. doi:10.1111/gwao.12552
42. Craig L, Churchill B. Dual‐earner parent couples’ work and care during COVID‐19. Gender Work Organ. 2021;28(S1):66–79. doi:10.1111/gwao.12497
43. Del Boca D, Oggero N, Profeta P, Rossi M. Women’s and men’s work, housework and childcare, before and during COVID-19. Rev Econ Household. 2020;18(4):1001–1017. doi:10.1007/s11150-020-09502-1
44. Chemali S, Mari-Sáez A, El Bcheraoui C, Weishaar H. Health care workers’ experiences during the COVID-19 pandemic: a scoping review. Hum Resour Health. 2022;20(1):27. doi:10.1186/s12960-022-00724-1
45. Liu Q, Luo D, Haase JE, et al. The experiences of health-care providers during the COVID-19 crisis in China: a qualitative study. Lancet Glob Health. 2020;8(6):e790–e798. doi:10.1016/S2214-109X(20)30204-7
46. Gao X, Jiang L, Hu Y, Li L, Hou L. Nurses’ experiences regarding shift patterns in isolation wards during the COVID‐19 pandemic in China: a qualitative study. J Creat Behav. 2020;29(21–22):4270–4280. doi:10.1111/jocn.15464
47. Eftekhar Ardebili M, Naserbakht M, Bernstein C, Alazmani-Noodeh F, Hakimi H, Ranjbar H. Healthcare providers experience of working during the COVID-19 pandemic: a qualitative study. Am J Infect Control. 2021;49(5):547–554. doi:10.1016/j.ajic.2020.10.001
48. Wang H, Zhou X, Jia X, et al. Emotional exhaustion in front-line healthcare workers during the COVID-19 pandemic in Wuhan, China: the effects of time pressure, social sharing and cognitive appraisal. BMC Public Health. 2021;21(1):829. doi:10.1186/s12889-021-10891-w
49. Dabou EAR, Ilesanmi RE, Mathias CA, Hanson VF. Work-related stress management behaviors of nurses during COVID-19 Pandemic in the United Arab Emirates. SAGE Open Nurs. 2022;8:237796082210849. doi:10.1177/23779608221084972
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.