")
Back to Journals » International Journal of Women's Health » Volume 14
Exclusive Breastfeeding Experiences of Thai Mothers in Metropolitan Bangkok
Authors Topothai C , Topothai T , Suphanchaimat R , Waleewong O, Putthasri W, Patcharanarumol W, Tangcharoensathien V
Received 15 October 2021
Accepted for publication 12 January 2022
Published 9 February 2022 Volume 2022:14 Pages 155—166
DOI https://doi.org/10.2147/IJWH.S344389
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Chompoonut Topothai,1,2 Thitikorn Topothai,1,2 Rapeepong Suphanchaimat,1,3 Orratai Waleewong,1 Weerasak Putthasri,4 Walaiporn Patcharanarumol,1 Viroj Tangcharoensathien1
1International Health Policy Program, Ministry of Public Health, Nonthaburi, 11000, Thailand; 2Department of Health, Ministry of Public Health, Nonthaburi, 11000, Thailand; 3Department of Disease Control, Ministry of Public Health, Nonthaburi, 11000, Thailand; 4National Health Commission Office, Ministry of Public Health, Nonthaburi, 11000, Thailand
Correspondence: Chompoonut Topothai, Tel +66 2590-2380
, Email [email protected]
Introduction: In 2019, only 14% of mothers in Thailand performed six-month exclusive breastfeeding. This study sought to understand the pathways that mothers in Bangkok Metropolitan took to achieve successful six-month exclusive breastfeeding.
Methods: A total of 50 mothers living in Bangkok with children aged 6– 12 months, who achieved and not achieved 6-month exclusive breastfeeding, were recruited for in-depth interviews during February to July 2020. Inductive thematic analysis of participants’ viewpoints was applied for data analysis and interpretation.
Results: Four themes that contributed to six-month exclusive breastfeeding were i) maternal breastfeeding self-efficacy; ii) support provided by family members; iii) engagement with and support from healthcare professionals; and iv) employers’ support and workplace environments. Mothers with strong breastfeeding intentions and “perceived capability” to succeed at breastfeeding tended to prioritize breastfeeding and overcome and cope well with unforeseen breastfeeding challenges. Supportive family members, who were convinced of the benefits of breastfeeding, engaged in maternal decision-making, and provided optimal support, contributed to successful exclusive breastfeeding. Health professionals were key in supporting mothers throughout pregnancy until the postpartum period. Lactating-mother-friendly working conditions, flexible working hours and enabling workplace environments, including the provision of breastfeeding breaks and a dedicate space for breast milk expression, were enabling factors for successful exclusive breastfeeding among working mothers.
Conclusion: We recommend that all mothers and their family members are fully informed and convinced of the benefit from breastfeeding and trained with practical skill during their visit to antenatal care clinics. These interventions aim to develop mothers’ self-efficacy for breastfeeding and to prepare them to manage common breastfeeding challenges. Health professionals should provide regular follow-up and counseling sessions on breastfeeding practices to mothers and families throughout the lactating period, especially working mothers for breastfeeding continuation after resume to work. Enhanced societal collective actions such as breastfeeding-friendly policy in workplace, including breastfeeding break-time and corner, can create enabling environments for successful exclusive breastfeeding.
Keywords: breastfeeding, maternal-self efficacy, qualitative study, urban, Bangkok
Introduction
The World Health Organization (WHO) and the United Nation Children’s Fund (UNICEF) recommend that infants should be initially breastfed within one hour after birth, exclusively breastfed during the first six months, and continue to be breastfed with appropriate complementary feeding for two years or beyond.1 This recommendation is based on evidence confirming that breast-milk brings incomparable benefits to health and socio-economic outcomes for both mothers and children.2 Breastfeeding protects babies from infection-related mortality such as pneumonia and diarrhea, reduces the risk of obesity and type-2 diabetes, and promotes cognitive development. Also, a longer duration of breastfeeding reduces incidence of breast and ovarian cancers and supports natural birth control.3 The positive health impact for children and mothers results in a high return on investments in breastfeeding: approximately US$35 in return for every dollar of investment.4
However, globally only 44% of infants younger than six months of age are currently exclusively breastfed.5 This is despite the global breastfeeding target aiming to achieve a minimum of 50% exclusive breastfeeding (EBF) in the first six months by 2025 and 70% by 2030.4 Among Southeast Asian countries,5 Thailand performed poorly with the lowest rates of EBF of infants under 6 months old, at 14% in 2019.6
Evidence confirms that the decision to breastfeed is complex and influenced by several personal and environmental determinants.7–11 At a personal level, study shows that self-efficacy has positive correlation with successful EBF and is found to be a strong predictor of breastfeeding duration in first-time Australian and Chinese mothers;12,13 self-efficacy refers to the confidence of a person in their capacity to undertake behaviors which lead to desired outcomes.14 Other personal-level factors are maternal age, education, income, breastfeeding intention, past experience of EBF, and the mother-infant relationship. Environmental factors also play an important role; these are family and community support, supports and advice from health professionals. Besides, work and workplace environment, marketing by formula milk companies and certain cultural beliefs can hamper breastfeeding efforts.7,9,15–20
Prior studies have identified multiple determinants of breastfeeding among Thai mothers. Mothers with higher socioeconomic status, higher breastfeeding knowledge and intention to breastfeed and prior experiences of successful EBF are more likely to achieve EBF than mothers without these attributes. Moreover, mothers who receive adequate support from family members, advice and support from health professional seem to achieve better EBF outcomes. In contrast, working conditions, and advertisements and active marketing by formula industries have been identified as barriers for initiation and continuation of breastfeeding.21–25
Although prior studies identify the enablers of and barriers to breastfeeding practice, they have yet to examine how these determinants interlink and how these links influence EBF. The qualitative evidence on the pathways that mothers take to achieve EBF is still lacking. Thus, this study sought to understand how Thai mothers in urban metropolitan areas initiate and sustain EBF for six months and how breastfeeding challenges are addressed. We chose Bangkok as a study site as it has consistently low EBF rates26–28 and high urbanization, and most mothers engage in labor force which adds more difficulties and stress on lactating mothers.29 Findings from this study not only fill the knowledge gap in the Thai literature, but also support EBF for mothers living in Metropolitan areas in other low- and middle-income countries (LMICs).
Materials and Methods
Setting and Study Design
This study employed a qualitative primary data collection. We selected Bangkok, with a high population density, as the study site.30
Participant Selection and Recruitment
Participants were healthy mothers, living in Bangkok, having the last child aged 6–12 months; selected in order to assess maternal experiences and the outcomes of EBF.
The plan was to recruit 40 participants, half who were successful at 6-month EBF, and the other half with EBF of less than 6 months, with an equal balance between working and non-working mothers. Participants were recruited when they took their babies for health check-ups and routine immunizations at the well-child clinic of the Metropolitan Health and Wellness Institution in Bangkok. The research team approached the mothers while they were waiting at the clinic reception. We briefly informed them about the project, methods of data collection, and the confidentiality of information. After agreeing to participate in the study, an interview session was appointed.
Data Collection
Data collection was conducted between February and July 2020. The first author (C.T.) conducted an in-depth interview to capture breastfeeding practices and experiences by each participant, while the second author (T.T.) attended the interview sessions to take audio recording. Information from in-depth interview such as birth weight and child’s growth were triangulated using maternal and child health records. Though the initial plan aimed for 40 participants, we recruited 50 participants; 32 participated in the face-to-face interview on site immediately after they had finished their child’s health check-up in a private room in the well-child clinic. The remaining 18 participants chose for a telephone interview, which was arranged at their convenience.
Each interview lasted for an average of 60 minutes. At the beginning of each interview, written consent was obtained. The telephone interview took longer than the face-to-face interview due to an extensive introduction of the project, objectives, and confirmation of the participant’s privacy.
The researchers developed the semi-structured interview guide based on a review of literature, the interview guide was assessed by three independent Thai breastfeeding experts as part of the validity check. The interview questions were conducted in Thai. These included: 1) What do you think about breastfeeding?; 2) During pregnancy, did you have any concerns or plans about breastfeeding?; 3) After delivery, how did you initiate breastfeeding? How did you breastfeed your child?; 4) Have you ever faced breastfeeding difficulties?; 5) How do you manage breastfeeding problems or difficulties?; and 6) For working mothers, how do you deal with breastfeeding when returning to work? Is there any support at your workplace?
Participants were interviewed according to the interview guide, and were allowed to spend more time talking about topics they perceived to be important such as topics related to breastfeeding and parenthood, experiences of being a “working women”, or the beliefs and culture of their families. Compensation of US$17 was offered to each participant at the end of the interview. The interview’s records were transcribed verbatim for analysis. Field notes and observations were also collected by researchers.
Data Analysis
Inductive thematic analysis was applied as it allows researchers to understand the viewpoints and experiences of mothers without trying to fit any preconceived frames. Two researchers (C.T. and T.T.) began the analysis by thorough reading and familiarization of the verbatim transcription, and cross-checked the transcripts with field notes for accuracy and consistency. Then, they made notes on key points that emerged from the reading and independently generated initial codes from the transcribed text without specific focus. Then, all relevant codes were collated and clustered into initial themes. Subsequently, researchers had a discussion to review and refine the initial themes, to clarify the meaning of each theme, and to avoid duplication across themes.31 Finally, four themes emerged from this study.
Results
Of the total 50 mothers who participated in this study, 62% had their first baby and first breastfeeding experiences, 74% had at least a high-school degree, 66% achieved 6-month EBF, and 34% practiced for a shorter duration. Around 74% of participants were employed with an average monthly income of 15,000 THB (around US$ 500 at an exchange rate 30 THB) see Table 1.
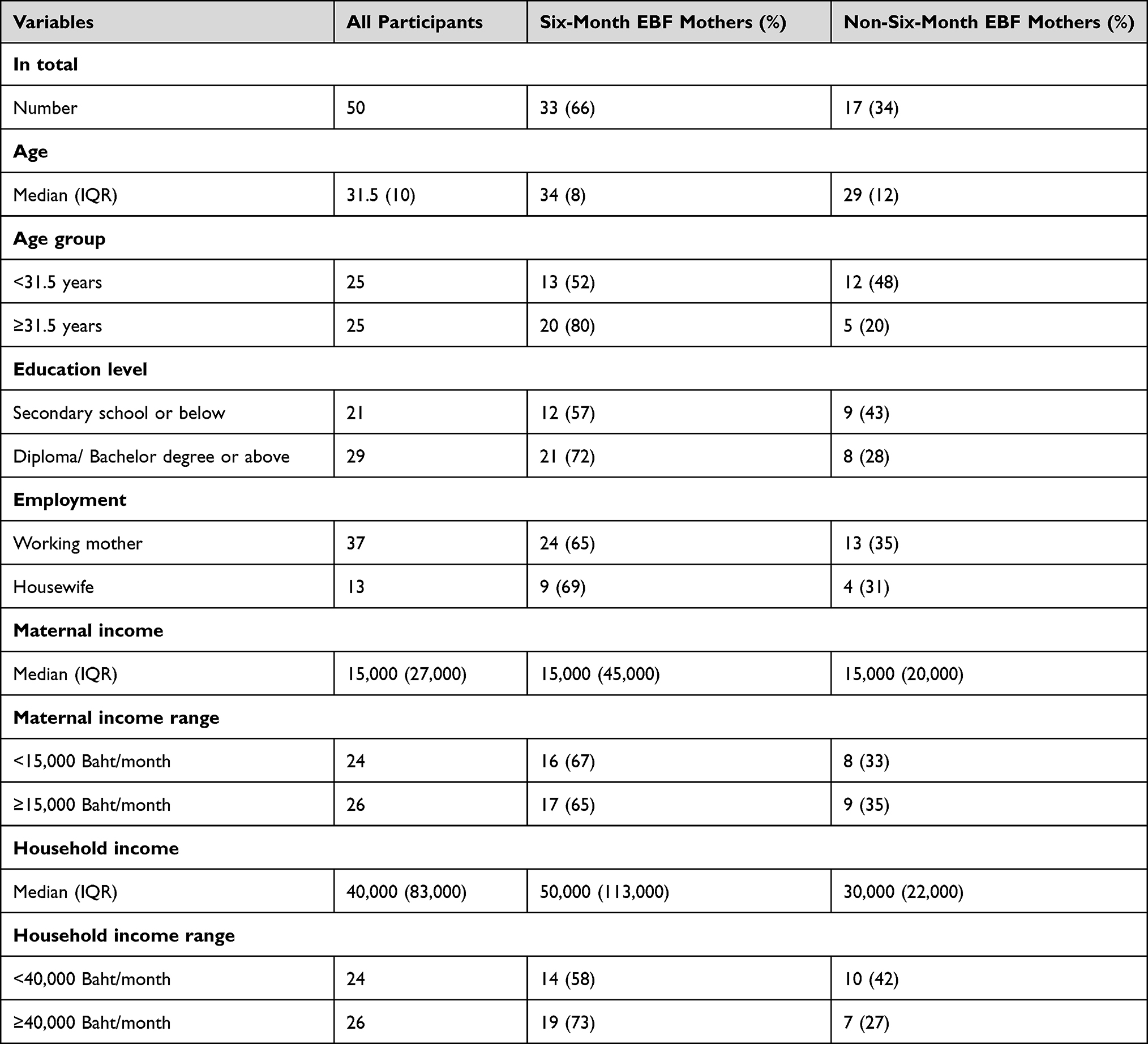 |
Table 1 Participants’ Socio-Demographic Profiles by 6-Month EBF Outcome |
Four major themes emerged from the study; i) maternal breastfeeding self-efficacy; ii) support provided by family members, iii) engagement with and support from healthcare professionals and iv) employers’ support and workplace environments especially for working mothers, see Table 2.
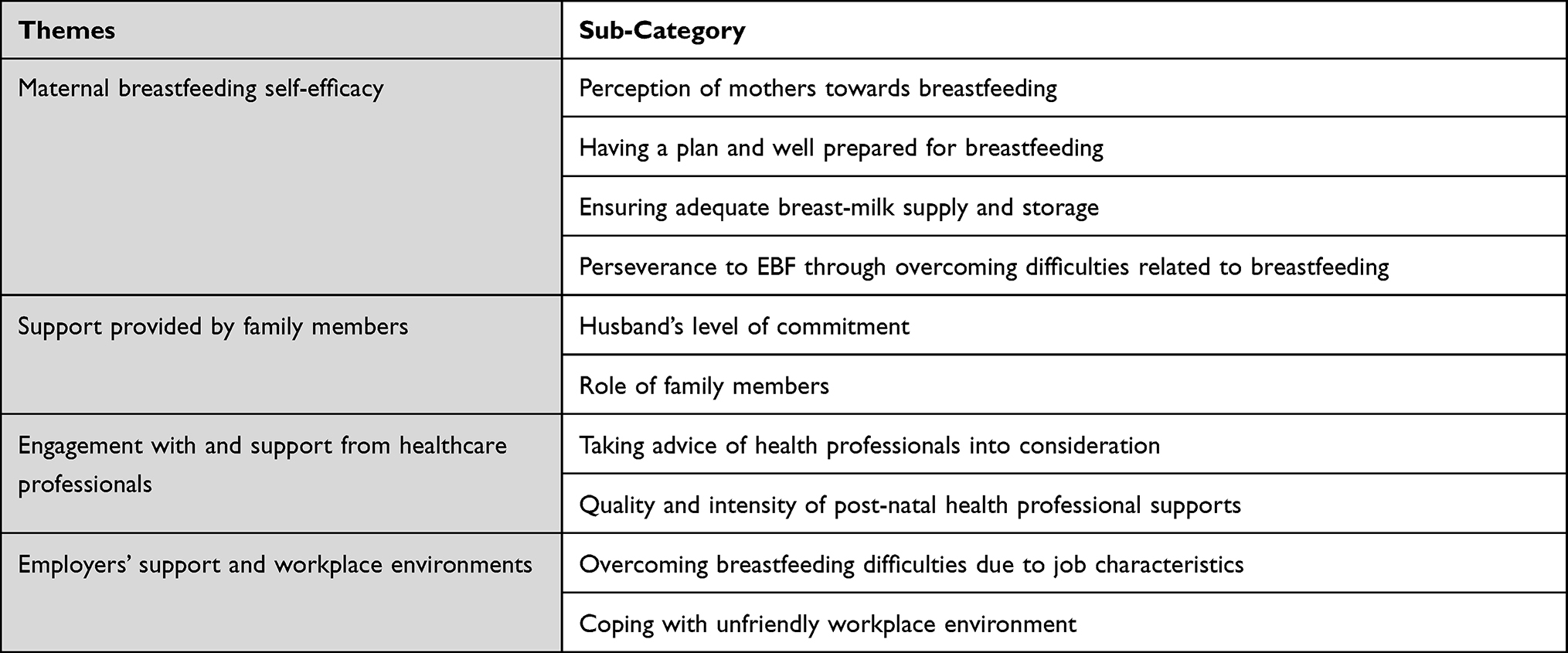 |
Table 2 Four Themes and Subcategory |
Theme 1: Maternal Breastfeeding Self-Efficacy
All mothers, regardless of the breastfeeding outcomes, had positive perceptions towards breastfeeding and intended to breastfeed their babies for some duration. This was reflected in a series of actions, such as planning and preparation for breastfeeding, ensuring adequate breast-milk supply and storage, and solving breastfeeding difficulties. This theme is demonstrated below.
Perception of Mothers Towards Breastfeeding
Most participants perceived breastfeeding as the best nutrition for their babies. During pregnancy, almost all mothers developed their intention to breastfeed for a certain duration, ranging from six months to as long as possible, although some mothers (7 out of 50) had concerns and low confidence about breastfeeding due to breast problems.
I intended to continue breastfeeding to two years or as long as possible. I did not want him (my baby) to be fed by formula milk because I know well that breast-milk is the best. - 35 years old, private sector employee, 6-month EBF mother.
The intention to complete EBF however changed in accordance with real breastfeeding experiences. Mothers who were able to breastfeed properly or overcome all breastfeeding problems, such as poor latching or inadequate breastmilk supply, gained more confidence and committed to sustain EBF up to 6 months or longer. Furthermore, mothers who regarded breastfeeding as a top priority over personal convenience and always spared adequate time for breastfeeding were likely to sustain EBF for a longer period.
My office is very strict with breastfeeding break-time. I was allowed to do breast-milk pumping only at 9.30, 12.30, and 15.30. So, I kept having lunch in the office every day in order to have time for pumping. My friend who previously did breast-milk pumping decided to stopped pumping and go out for lunch.- 36 years old, private sector employee, 6-month EBF mother.
In contrast, mothers who were unable to solve their breastfeeding problems, tended to feel uncomfortable with continuing EBF, and decided to wean sooner than expected. Those who were overwhelmed by work or earning stopped EBF earlier than expected.
I myself take care of him [her son], do housework, do everything and I cannot do it [breastfeeding] in parallel. I must choose what I can do. I always think that breastfeeding is time-consuming and takes much of my time especially when I wish to finish my job and complete all the bakery orders. I earn a living from this work.- 29 years old, self-employed, non- 6-month EBF mother.
Having a Plan and Well Prepared for Breastfeeding
Common practices included searching for information, visiting lactation clinics and attending breastfeeding counseling. Planning in advance helps mothers to better understand, have essential breastfeeding skills and know where to seek breastfeeding support after delivery. First-time mothers who prepared breastfeeding in advance had more confidence in their breastfeeding capability. Most working mothers began to plan for EBF during the first month after delivery.
With my first child, I reviewed many books and (internet) pages about breastfeeding, I read details into all the topics as I have no experience.- 33 years old, public sector employee, 6-month EBF mother.
Around 15 days before I resumed work, I set a schedule for breast-milk expression at home as if I were back at work with all the equipment prepared. I bought a new set of dresses, all of them were nursing dresses.- 33 years old, public sector employee, 6-month EBF mother.
Ensuring Adequate Breast-Milk Supply and Storage
Mothers’ perceived sufficient breast-milk supply is a critical factor for EBF. Successful six-month EBF mothers revealed that they breastfed the baby as early as possible immediately after birth and had less concern about their breast-milk supply. The majority of respondents judged breast-milk adequacy by good and long sleeping hours and enough monthly weight gain of babies. Effective latch-on is an important skill that enabled mothers to provide feeding at the breast and foster their confidence that their babies were sufficiently breastfed. In contrast, mothers who failed to feed at the breast had to do breast-milk pumping around the clock; this tiring situation pushed them to reconsider EBF goals.
While non-working mothers continued to feed at the breast, most working mothers began to express breast-milk using either a manual or electric pump during maternity leave and cumulated a large stock of breast-milk for the baby. Some working mothers who started breastmilk pumping and breast-milk-bottle-feeding as early as less than one month due to a shorter period of maternity leave faced several negative consequences, such as breast refusal, duct obstruction, and insufficient breastmilk supply. Mothers who took a full three-months or longer maternity leave were more likely to delay breast-milk-pumping and they subsequently continued breastfeeding with fewer problems.
I started pumping breast-milk seriously when my child reached 2 months old because I had to go to work when he turned 3 months. Previously, I only breastfed him. I just wanted to make sure that I had enough breast-milk stock for him- 24 years old, private sector employee, 6-month EBF mother.
Perseverance to EBF Through Overcoming Difficulties Related to Breastfeeding
Almost all mothers had experienced some breastfeeding difficulties, ranging from very mild to severe, either due to physical or mental causes. Difficulties arose at early postpartum and after returning to work. Common physical problems such as poor latching, nipple confusion, and perceived insufficient milk supply were coped by “trial and error” solutions, seeking information from internet and peer support from friends or health care workers. Unresolved physical or psychological stresses resulted in shorter than six months EBF. Perseverance fosters self-efficacy; as mothers with successful six-month EBF tried multiple solutions without distorting the original EBF intention, even though they had to trade off with other benefits.
I could not get my child to latch on since the first day, so he cried a lot and refused to be fed at the breast, this was so stressful. I tried to solve it by practicing and practicing and practicing latch-on while giving the baby a bottle feed in parallel. After one day, I could do it – 38 years old, private sector employee, 6-month EBF mother.
Theme 2: Support Provided by Family Members
Husband’s Level of Commitment
All mothers who achieved six-month EBF regarded their husbands as important primary supporters. Husbands gained knowledge from counseling sessions at antenatal or lactation clinics. Recognizing the importance of breastfeeding, husbands supported every critical step and protected the infants from early introduction of complementary food or breast-milk substitutes, which were attempted mostly by grandparents. Below are two EBF examples: one successful and one unsuccessful.
After delivery, my son was in the nursery for 6 hours. My husband was the one who kept asking the nurse to bring my son to me to initiate breastfeeding … otherwise I would have had to wait longer. He highly supports breastfeeding, I would say.- 35 years old, private sector employee, 6-month EBF mother.
I was not supported by my family at all. Everyone wanted me to feed my child with formula. My husband told me that there was no problem if I had no milk, we could feed her with formula. He did not want me to feel stress because of breastfeeding, but he did not know that this kind of response made me get worse and experience more stress because I had a strong intention to breastfeed my child.- 30 years old, public sector employee, non-6-month EBF mother.
Role of Family Members
Family members can be encouraging and discouraging and the latter experienced needs to be well managed. Common EBF support provided by family members was giving mental support or taking care of the baby while the mother took a rest or had another duty to fulfil. Mothers who received criticism from family members, such as receiving questions as to why breast-fed babies gained less weight, lost confidence and discontinued EBF earlier than expected.
My brother was my main support. When I was pregnant, my mother and my sister told me that our families inherited no-milk production genes and I would have no breast-milk, but my brother disagreed with this idea. He kept cheering me up and told me that even my-sister-in-law who was very slim, had enough breast-milk so I would have breast-milk as well… - 45 years old, self-employed, 6-month EBF mother.
My mother-in-law told me to feed my kid with formula milk in parallel with breast-milk when he was two months old. I did not want to feed him with formula but I could not convince her. When my baby reached four months old, my mother-in-law again fed him with banana despite my request for EBF to six months.- 22 years old, unemployed, non-6-month EBF mother.
Theme 3: Engagement with and Support from Healthcare Professionals
Taking Advice of Health Professionals into Consideration
Free parental classes for pregnant women, husbands and family members during antenatal care played a pivotal role in empowering self-efficacy, confidence and intention for six-month EBF.
I was not confident about breastfeeding because I was an older mother who had a high-risk pregnancy. I believed I could not exclusively breastfeed my child for a long duration; as the first and second child were breastfed for very short period. However, after attending parental class here, I received useful advice from the nurses and doctors. They motivated me to try my best … They inspired me to continue breastfeeding.- 42 years old, private sector employee, 6-month EBF mother.
Quality and Intensity of Post-Natal Health Professional Support
Mothers who accessed quality professional support such as face-to-face training on latching and positioning, observing baby’s hunger cue, breastmilk-production stimulation technique, and screening for tongue-tie were able to initiate breastfeeding and continue EBF confidently.
The nurse brought me my daughter soon after delivery to initiate breastfeeding, about 1.5 hours … Every time the nurses came to my room, they taught and advised me on breastfeeding, and sometimes the nurses shared their experiences of breastfeeding. … The doctor was also very keen on breastfeeding promotion. She brought many breastfeeding teaching-materials into my room to teach me and my husband.- 35 years old, self-employed, 6-month EBF mother.
My first child had tongue-tie so he could not latch on properly. Luckily, my admission was extended to seven days and I was trained by lactation nurses. I learnt how to practice breastfeeding correctly there, the lactation nurse shared many useful tips that were tailored to my problems- 36 years old, public sector employee, 6-month EBF mother.
My father-in-law believes that breast-milk is not useful for the baby aged over six months. I solved this problem by taking both my father- and mother-in-law to see the doctor at the well-child clinic when my kid went for vaccination at six months. I pretended to ask the doctor for how long should I continue breastfeeding? Is breast-milk still useful from now on? And the doctor said yes, of course I should continue breastfeeding as long as possible. This tactic worked very well.- 33 years old, public sector employee, 6-month EBF mother.
Theme 4: Employers’ Support and Workplace Environments
Most working mothers felt some sense of inconvenience for being lactating mothers while being back at work. This perception was influenced by particular job characteristics and unsupportive workplace environments. The coping strategies were to ensure adequate time and to seek proper space for breastmilk pumping and storage.
Overcoming Breastfeeding Difficulties Due to Job Characteristics
Maternal working conditions, job characteristics, and positions were raised by the participants as major factors contributing to their EBF continuation. Mothers working in office-based settings with flexible working hours could better design their breastfeeding break times than those working in service-based settings or on factory production-lines. Working mothers holding a high position can manage their working hours and have access to private spaces for breastmilk pumping. Self-efficacy, perseverance and adaptation are key factors for successful six-month EBF among working mothers.
When I resumed work as a street food vendor, there was no one to raise my kid at home, I bought the baby with me, and stop working every time he felt hungry. I found corners on the street and fed him at breast. It was not convenient but I had to do it.- 28 years old, self-employed, 6-month EBF mother.
Coping with Unfriendly Workplace Environment
Coping mechanisms by working mothers in unsupportive workplace environments include adjusting lifestyles, ignoring poor attitudes of co-workers and managers, or even changing their jobs in order to sustain six-month EBF. Mothers needed to prepare their own personal gadgets, nursing covers, ice packs and cool boxes for breastmilk storage. Some working mothers, who were criticized by their bosses and co-workers for breastfeeding as this meant they could not fulfil job duties as a result, decided to express breastmilk while working at their desks or workstation. Only mothers with strong self-efficacy and adequate breastmilk supply could sustain EBF to 6 months or beyond.
It was not convenient at my workplace for pumping breast milk because it was a furniture outlet located in a department store. There was no refrigerator and no private space in the office. I had to bring my own icepack every single day to freeze the expressed breast milk. Although there was a parent room (in the department store), it was too far away.- 36 years old, private sector employee, 6-month EBF mother.
My new office gave me a higher salary but they were so strict and I had no break time to do breast-milk pumping. It was not convenient to express breast-milk so I stopped breastfeeding four months after delivery- 20 years old, private sector employee, non-6-month EBF mother.
Discussion
The inductive synthesis of the findings is summarized in Figure 1. Though maternal self-efficacy is a primary contributing factor to successful EBF, healthcare professionals, family members, employers and the workplace environment also play important enabling secondary factors. This study confirms findings from prior a global review,7 international studies,7,32,33 and Thai literature.23,25
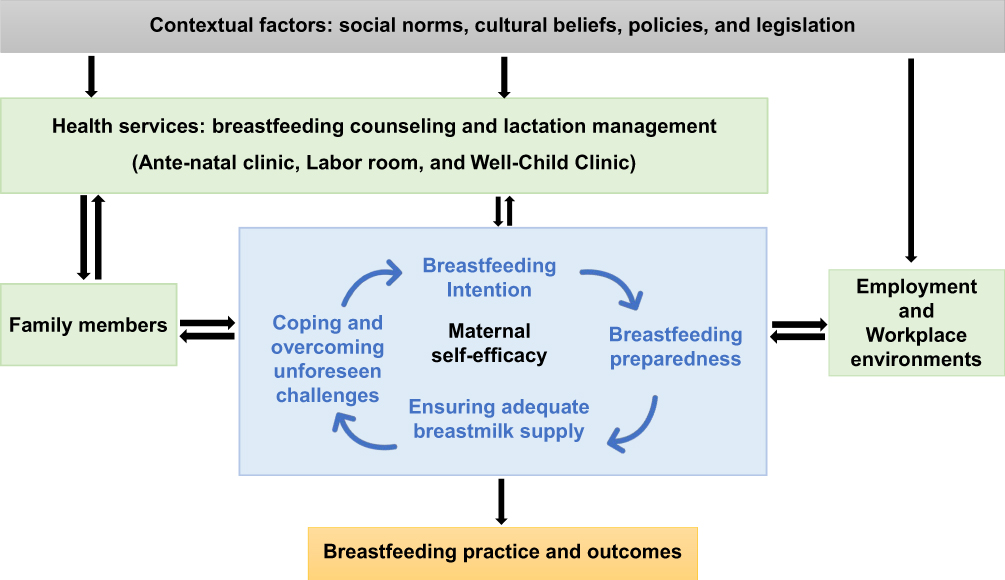 |
Figure 1 Context, actors, maternal self-efficacy and breastfeeding outcomes. |
When mothers realize breastfeeding as their ultimate responsibility, they feel empowered and determined. The Theory of Planned Behavior suggests that mothers who have positive attitudes towards breastfeeding and positive norms which value EBF are more likely to develop strong intentions to breastfeed. Due to these strong intentions, mothers prioritize breastfeeding over other activities and find ways to overcome all foreseeable and unforeseen difficulties.34,35 Successful coping experiences not only help mothers to discover their ability to breastfeeding which is a key attribute of breastfeeding self-efficacy; it in turn fosters self-determination towards a successful EBF.36–39 Therefore, empowering mothers to develop breastfeeding intentions and self-efficacy and equip them with necessary technical skills such as latching and the positioning of the baby are critical for successful EBF.7,24,40
This study confirms the critical role of health professionals in providing support at all stages, from pregnancy to delivery and post-partum and beyond. Healthcare professionals should aim to strengthen mothers’ intrinsic motivation towards EBF from early pregnancy onwards, while intrinsic motivation includes desire for self-control, concerns about baby’s health and concerns about mother’s health.41 After delivery, self-efficacy should be equipped by technical skill provided by healthcare professionals such as immediate breastfeeding initiation, correct latching and positioning, and assessment of baby’s hunger cue and breastmilk supply. Evidence shows that poor-latching and insufficient breastmilk supplies are common reasons for EBF discontinuation.23,25,40,42
Despite health professionals’ critical roles, existing breastfeeding support for Thai mothers, particularly during the early post-partum period, is still inadequate and needs significant reform;43,44 only 7.7% of infants in Thailand were put to the mother’s breast after birth and only 34% were initially breastfed within an hour after birth in 2019.6 Inadequate breastfeeding follow-up is a result of a shortage of lactation counselors and other competing responsibilities.44,45 Health professionals in all hospitals including those taking part in the Baby-Friendly-Hospital-Initiative should have adequate training on breastfeeding counseling and problem-solving skills.45–47 The village health volunteers should be trained on basic breastfeeding counseling and engage in the community-based breastfeeding supporting system.48 Other skills beyond clinical skills have yet to improve especially empowering mothers and strengthening mothers’ intrinsic motivation; both of which lead to breastfeeding self-efficacy and successful EBF. Healthcare professionals can be empowered through trainings such as goal setting, action planning, and enhanced self-awareness and confidence.49 Their internalized experiences of “empowerment” can be used to empower pregnant women.
Sustained breastfeeding either at the breast or breast-milk pumping requires time commitment and effort. Mothers with no or little support might not be able to sustain breastfeeding, especially single- or working- mothers. Hence, family members are great supporters in several ways. In contrast, family members can be an obstacle for EBF, for example some grandparents feed water and complementary food to infants prior to six months old.23,25 For cultural reasons, decisions made by other family members are sometimes beyond the mother power of negotiation. Thus, family members should be educated on the benefits of breastfeeding and the supportive role they play.22 Policy makers should also advocate positive societal attitudes towards breastfeeding and promote six-month EBF.50
There is still a limited political window of opportunity for maternity leave extension from the current three months to six months, which would facilitate successful six-month EBF. Extending maternity leave to six months is non-palatable for employers and create worry among mothers for economic and job security reasons.51 Therefore, breastfeeding-friendly workplaces can be a practical solution from both employers’ and employees’ perspectives. These low cost interventions include provisions of adequate breastfeeding break time, a lactation corner and refrigerator for breast-milk expression.52
This study has some limitations. First, there was selection bias as the participants were recruited from the Metropolitan Health and Wellness Institution. Participants in this study, having been exposed to health facilities that promote breastfeeding, can have positive bias in favor of breastfeeding. Also, there was no recruitment of mothers who are not able to attend the public health facilities (most of them are the less well-off) or mothers who visited private facilities (mostly wealthy mothers).
Second, there may be social desirability bias as mothers who failed to complete six-month EBF may refrain from detailing their negative views or unsuccessful experiences. This bias was managed by building rapport and holding initial interviews with general open-ended questions, seeking descriptions of experiences from the prenatal, natal and post-natal period.
Third, although literature suggests that market promotion of infant formula creates negative attitude towards breastfeeding practices;7,25,53 only very few of the 17 participants who did not achieve six-month EBF refer to this issue. Therefore, this issue was not included in the findings.
Lastly, to prevent researchers’ confirmation bias, the researchers triangulated the interviewed data with other sources of information such as the records in the maternal and child health handbook.
Conclusion and Recommendations
This is the first study that examines the practical experiences and coping strategies in successful six-month EBF among mothers living in Bangkok. Self-efficacy and coping skills contribute to successful EBF. However, support from family members, health professionals, employers as well as societal collective actions are also key enabling factors.
We recommend that during prenatal period, health professionals should assess the attitudes towards breastfeeding of pregnant women and their family members, encourage them to determine and set breastfeeding goals, and prepare them with necessary skills; all of which aims to create or strengthen mothers’ self-efficacy for breastfeeding. During post-natal period, regular follow-up and counseling session on breastfeeding practice, and problem-solving techniques is strongly recommended for health professional working in all well-child clinics. Policy makers should monitor and evaluate the performance of health facilities to ensure compliance with the ten steps to successful breastfeeding. Breastfeeding-friendly policy in workplaces, such as breastfeeding room and break-time, should be further promoted with appealing incentives to employers. This is especially important as Thai women have high level of labor force participation, 45% of total labor force in 2019.54 Further implementation research on practical interventions that empowers self-efficacy and boost confidence among first-time and working mothers are encouraged. Such understanding may pave the way to improve six-month EBF coverage in Thailand.
Abbreviation
EBF, exclusive breastfeeding.
Ethics Approval and Informed Consent
All respondents signed informed consent prior to participation in the study. The informed consent included publication of anonymous responses. This study received ethics approval from the Institute for Development of Human Research Protection in Thailand (IHRP letterhead: 127/2563) which is a recognized agency that conform to the Declaration of Helsinki, Belmont Report, CIOMS Guidelines and ICH-GCP Guidelines.
Acknowledgments
We acknowledge staff members at the Metropolitan Health and Wellness Institution who facilitated the recruitment of sample mothers and provided a quiet room for in-depth interviews. We thank all participants for sharing their practical experiences in managing EBF. Joint funding support from (1) the Thai Health Promotion Foundation through the Food and Nutrition Policy for Health Promotion, International Health Policy Foundation (Contract No. 62-00-0144); (2) Thailand Science Research and Innovation (TSRI) for the Senior Research Scholar on Health Policy and System Research (Contract No. RTA6280007); and (3) the Capacity Building on Health Policy and Systems Research program (HPSR Fellowship) under cooperation between Bank for Agriculture and Agricultural Co-operatives (BAAC), National Health Security Office (NHSO) and International Health Policy Program Foundation (IHPF) are highly appreciated.
Author Contributions
All authors made a significant contribution to the work, ranging from the conception, study design, execution, acquisition of data, analysis and interpretation. All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization, United Nation Children’s Fund. Global Strategy for Infant and Young Child Feeding. Geneva: World Health Organization; 2003.
2. United Nation Children’s Fund. Breastfeeding: a smart investment. UNICEF; 2020. Available from: https://www.unicef.org/breastfeeding/.
3. Victora CG, Bahl R, Barros AJ, et al. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet. 2016;387(10017):475–490. doi:10.1016/S0140-6736(15)01024-7
4. World Health Organization, United Nation Children’s Fund. Global Breastfeeding Scorecard, 2019 Increasing Commitment to Breastfeeding Through Funding and Improved Policies and Programs. Geneva: World Health Organization, United Nation Children’s Fund; 2019.
5. United Nation Children’s Fund. UNICEF data: exclusive breastfeeding (<6 months); 2021. Available from: https://data.unicef.org/topic/nutrition/breastfeeding/.
6. National statistical Office, United Nation Children’s Fund. Thailand Multiple Indicator Cluster Survey in 2019: The Summary of Key Indicators. Bangkok: National Statistical Office; 2020.
7. Rollins NC, Bhandari N, Hajeebhoy N, et al. Why invest, and what it will take to improve breastfeeding practices? Lancet. 2016;387(10017):491–504. doi:10.1016/S0140-6736(15)01044-2
8. Li J, Nguyen TT, Wang X, Mathisen R, Fang J. Breastfeeding practices and associated factors at the individual, family, health facility and environmental levels in China. Matern Child Nutr. 2020;16(S2):e13002. doi:10.1111/mcn.13002
9. Sasaki Y, Ali M, Kakimoto K, Saroeun O, Kanal K, Kuroiwa C. Predictors of exclusive breast-feeding in early infancy: a survey report from Phnom Penh, Cambodia. J Pediatr Nurs. 2010;25(6):463–469. doi:10.1016/j.pedn.2009.04.010
10. Tan KL. Factors associated with exclusive breastfeeding among infants under six months of age in peninsular Malaysia. Int Breastfeed J. 2011;6(1):2. doi:10.1186/1746-4358-6-2
11. Hasan M, Hassan MN, Khan MSI, Tareq MA, Afroj MS. Prevalence, knowledge, attitudes and factors associated with exclusive breastfeeding among mothers in Dhaka, Bangladesh: a cross-sectional study. Popul Med. 2021;3:1–7. doi:10.18332/popmed/140132
12. Baghurst P, Pincombe J, Peat B, Henderson A, Reddin E, Antoniou G. Breast feeding self-efficacy and other determinants of the duration of breast feeding in a cohort of first-time mothers in Adelaide, Australia. Midwifery. 2007;23(4):382–391. doi:10.1016/j.midw.2006.05.004
13. Wu DS, Hu J, McCoy TP, Efird JT. The effects of a breastfeeding self-efficacy intervention on short-term breastfeeding outcomes among primiparous mothers in Wuhan, China. J Adv Nurs. 2014;70(8):1867–1879. doi:10.1111/jan.12349
14. Bandura A. Perceived self-efficacy in cognitive development and functioning. Educ Psychol. 1993;28(2):117–148. doi:10.1207/s15326985ep2802_3
15. Nassar MF, Abdel-Kader AM, Al-Refaee FA, et al. Breastfeeding practice in Kuwait: determinants of success and reasons for failure. East Mediterr Health J. 2014;20(7):409–415. doi:10.26719/2014.20.7.409
16. Johnston ML, Esposito N. Barriers and facilitators for breastfeeding among working women in the United States. J Obstet Gynecol Neonatal Nurs. 2007;36(1):9–20. doi:10.1111/j.1552-6909.2006.00109.x
17. Mundagowa PT, Chadambuka EM, Chimberengwa PT, Mukora-Mutseyekwa F. Determinants of exclusive breastfeeding among mothers of infants aged 6 to 12 months in Gwanda District, Zimbabwe. Int Breastfeed J. 2019;14(1):30. doi:10.1186/s13006-019-0225-x
18. Balogun OO, Dagvadorj A, Anigo KM, Ota E, Sasaki S. Factors influencing breastfeeding exclusivity during the first 6 months of life in developing countries: a quantitative and qualitative systematic review. Matern Child Nutr. 2015;11(4):433–451. doi:10.1111/mcn.12180
19. Neifert M, Bunik M. Overcoming clinical barriers to exclusive breastfeeding. Pediatr Clin North Am. 2013;60(1):115–145. doi:10.1016/j.pcl.2012.10.001
20. Mgongo M, Hussein TH, Stray-Pedersen B, Vangen S, Msuya SE, Wandel M. Facilitators and barriers to breastfeeding and exclusive breastfeeding in Kilimanjaro Region, Tanzania: a qualitative study. Int J Pediatr. 2019;2019:8651010. doi:10.1155/2019/8651010
21. Barnes SB, Perngparn U. Exclusive breastfeeding experiences among mothers in Bangkok, Thailand: findings from a mixed-methods study. J Health Res. 2013;27(1):19–25.
22. Kaewsarn P, Moyle W. Breastfeeding duration of Thai women. Aust Coll Midwives Inc J. 2000;13(1):21–26. doi:10.1016/S1031-170X(00)80038-0
23. Thepha T, Marais D, Bell J, Muangpin S. Facilitators and barriers to exclusive breastfeeding in Thailand: a narrative review. J Comm Public Health Nurs. 2017;3(1):1–9
24. Thepha T, Marais D, Bell J, Muangpin S. Perceptions of northeast Thai breastfeeding mothers regarding facilitators and barriers to six-month exclusive breastfeeding: focus group discussions. Int Breastfeed J. 2018;13(14):14. doi:10.1186/s13006-018-0148-y
25. Winichagoon P, Damrongwongsiri O. Breastfeeding situation, facilitators and obstacles, policy and program to promote breastfeeding in Thailand. J Nutr Assoc Thai. 2020;55(1):66–81.
26. National Statistical Office, United Nation Children’s Fund. Final Report: The Multiple Indicator Cluster Survey (MICS); December 2005–February 2006. Bangkok: National Statistical Office; 2006.
27. National Statistical Office, United Nation Children’s Fund, Ministry of Publich Health, National Health Security Office, Thai Health Promotion Foundation, International Health Policy Program. Monitoring the Situation of Children and Women: Multiple Indicator Cluster Survey 2012. Bangkok; 2012.
28. National Statistical Office, United Nation Children’s Fund. Thailand Multiple Indicator Cluster Survey 2015–2016, Final Report. Bangkok: National Statistical Office, United Nation Children’s Fund; 2016.
29. Laisiriruangrai P, Wiriyasirivaj B, Phaloprakarn C, Manusirivithaya S. Prevalence of exclusive breastfeeding at 3, 4 and 6 months in Bangkok Metropolitan Administration Medical College and Vajira Hospital. J Med Assoc Thai. 2008;91(7):962–967.
30. Strategy and Planning Division, Office of the Permanent Secretary, Ministry of Publich Health. Public Health Statistics A.D. 2019. Nonthaburi: Ministry of Public Health; 2019.
31. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
32. Kohan S, Keshvari M, Mohammadi F, Heidari Z. Designing and evaluating an empowering program for breastfeeding: a mixed-methods study. Arch Iran Med. 2019;22(8):443–452.
33. Heidari Z, Kohan S, Keshvari M. Empowerment in breastfeeding as viewed by women: a qualitative study. J Educ Health Promot. 2017;6:33. doi:10.4103/jehp.jehp_34_16
34. Lau CYK, Lok KYW, Tarrant M. Breastfeeding duration and the theory of planned behavior and breastfeeding self-efficacy framework: a systematic review of observational studies. Matern Child Health J. 2018;22(3):327–342. doi:10.1007/s10995-018-2453-x
35. Linares AM, Rayens MK, Gomez ML, Gokun Y, Dignan MB. Intention to breastfeed as a predictor of initiation of exclusive breastfeeding in Hispanic women. J Immigr Minor Health. 2015;17(4):1192–1198. doi:10.1007/s10903-014-0049-0
36. Brockway M, Benzies K, Hayden KA. Interventions to improve breastfeeding self-efficacy and resultant breastfeeding rates: a systematic review and meta-analysis. J Hum Lact. 2017;33(3):486–499. doi:10.1177/0890334417707957
37. Blyth R, Creedy DK, Dennis C-L, Moyle W, Pratt J, De Vries SM. Effect of maternal confidence on breastfeeding duration: an application of breastfeeding self-efficacy theory. Birth. 2002;29(4):278–284. doi:10.1046/j.1523-536X.2002.00202.x
38. Guo JL, Wang TF, Liao JY, Huang CM. Efficacy of the theory of planned behavior in predicting breastfeeding: meta-analysis and structural equation modeling. Appl Nurs Res. 2016;29:37–42. doi:10.1016/j.apnr.2015.03.016
39. Dennis CL. Theoretical underpinnings of breastfeeding confidence: a self-efficacy framework. J Hum Lact. 1999;15(3):195–201. doi:10.1177/089033449901500303
40. Topothai C, Topothai T, Suphanchaimat R, et al. Breastfeeding practice and association between characteristics and experiences of mothers living in Bangkok. Int J Environ Res Public Health. 2021;18(15):7889. doi:10.3390/ijerph18157889
41. Sardo D. Intrinsic and extrinsic motivation to breastfeed scale: adaptation and validation for Portuguese population. Procedia Soc Behav Sci. 2016;217:1133–1141. doi:10.1016/j.sbspro.2016.02.128
42. Cetthkrikul N, Topothai C, Topothai T, et al. Situation of breastfeeding among mothers receiving services in public hospitals in Thailand. J Health Res. 2017;25(4):657–663.
43. Topothai C, Tangcharoensathien V. Achieving global targets on breastfeeding in Thailand: gap analysis and solutions. Int Breastfeed J. 2021;16(1):38. doi:10.1186/s13006-021-00386-0
44. Topothai C, Cetthakrikul N. The service provision of lactation clinic in health facilities in Thailand. Thai J Health Promot Environ Health. 2018;41(4):87–100.
45. Cetthakrikul N, Topothai C. Study of lactation consultant’s services in health facilities in Thailand. J Health Syst Res. 2019;13(4):368–382.
46. World Health Organization, United Nation Children’s Fund. Protecting, Promoting, and Supporting Breastfeeding in Facilities Providing Maternity and Newborn Services: The Revised Baby-Friendly Hospital Initiative 2018: Implementation Guidance. Geneva; 2018.
47. World health Organization. National Implementation of the Baby-Friendly Hospital Initiative 2017. Geneva: World health Organization; 2017.
48. World Health Organization. Guideline: Counselling of Women to Improve Breastfeeding Practices. Geneva: World Health Organization; 2018.
49. Majee W, Anakwe A, Johnson L, Rhoda A, Frantz J, Schopp L. A self-management training intervention: perceptions and practices of community health workers in South Africa. Health Promot Pract. 2020;21(6):983–992. doi:10.1177/1524839918820038
50. World health Organization. Viet Nam breastfeeding campaign normalizes practice, improves rates. World Health Organization; 2016 [updated August 2, 2016]. Available from: https://www.who.int/news-room/feature-stories/detail/viet-nam-breastfeeding-campaign-normalizes-practice-improves-rates.
51. Cetthkrikul N, Thaichinda C, Topothai T, et al. Feasibility of the extension of paid maternity leave from 90 days to 180 days in Thailand. J Health Res. 2017;24(4):720–726.
52. World Health Organization, United Nations Children’s Fund. Advocacy Brief: Breastfeeding and Family-Friendly Policies; Global Breastfeeding Collective. Geneva; 2019.
53. Piwoz GE, Huffman SL. The impact of marketing of breast-milk substitutes on WHO-recommended breastfeeding practices. Food Nutr Bull. 2015;36(4):373–386. doi:10.1177/0379572115602174
54. Labor force participation rate, female (% of total labor force). World Bank Open Data, The World Bank Group; 2021. Available from: https://data.worldbank.org/indicator/SL.TLF.TOTL.FE.ZS?locations=TH&view=chart.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.