")
Back to Journals » Pharmacogenomics and Personalized Medicine » Volume 15
Examining an Association of Single Nucleotide Polymorphisms with Hyperuricemia in Chinese Flight Attendants
Authors Ye J, Zeng Z, Chen Y, Wu Z, Yang Q, Sun T
Received 28 February 2022
Accepted for publication 23 May 2022
Published 8 June 2022 Volume 2022:15 Pages 589—602
DOI https://doi.org/10.2147/PGPM.S364206
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Martin H Bluth
Jianpin Ye,1,* Zhiwei Zeng,2,* Yuxian Chen,3 Zhenkun Wu,3 Qingwei Yang,4 Tao Sun2
1Outpatient Department Laboratory, Xiamen Aviation, Xiamen, Fujian, People’s Republic of China; 2Center for Precision Medicine, School of Medicine and School of Biomedical Sciences, Huaqiao University, Xiamen, Fujian, People’s Republic of China; 3Taokang Institute of Neuro Medicine, Xiamen, Fujian, People’s Republic of China; 4Department of Neurology, Zhongshan Hospital, School of Medicine, Xiamen University, Xiamen, Fujian, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Tao Sun, Center for Precision Medicine, School of Medicine and School of Biomedical Sciences, Huaqiao University, Xiamen, Fujian, People’s Republic of China, Email [email protected]
Background: Both genetic and environmental factors strongly affect serum uric acid (SUA) concentrations. The incidence of hyperuricemia tends to be younger in the Chinese population. In particular, we have found a high prevalence of hyperuricemia among Chinese flight attendants, aged from 20 to 40, in our survey. This study aims to evaluate whether there is an association between gene polymorphisms and hyperuricemia among Chinese flight attendants.
Methods: A total of 532 flight attendants with high and normal serum uric acid levels were recruited. Allele-specific polymerase chain reaction (AS-PCR) was performed using blood samples of enrolled subjects.
Results: Previous studies have reported single nucleotide polymorphisms (SNPs) that are tightly associated with uric acid levels. Among them, six SNPs that are strongly associated with SUA or gout in Asians, for instance ABCG2 (rs2231142, rs72552713 and rs2231137), GCKR (rs780094), SLC2A9 (rs1014290) and SLC17A1 (rs1183201), were selected for AS-PCR analyses. We found that SNPs such as ABCG2 rs2231142, GCKR rs780094 and SLC2A9 rs1014290 are strongly associated with hyperuricemia in male flight attendants, and SLC2A9 rs1014290 among female flight attendants.
Conclusion: Our study provides evidences of an association between SNPs and hyperuricemia in the Chinese flight attendants, and highlights the significance of improving diagnostics and prevention of disease development in uric acid metabolism disorders and gout using these SNPs.
Keywords: serum uric acid, hyperuricemia, single nucleotide polymorphisms, flight attendants
Introduction
Hyperuricemia is mainly caused by elevated purine metabolism or abnormal uric acid excretion, which is related to diet, environment and heredity.1,2 Uric acid (UA) is the final product of purine metabolism. Hyperuricemia is usually diagnosed when the concentration of serum uric acid (SUA) is higher than 420 µmol/L (7.0 mg/dL) in men and 360 µmol/L (6.0 mg/dL) in premenopausal women.3,4 Hyperuricemia has been considered closely related to the development of gout, kidney disease, cardiovascular disease, diabetes and other disorders.1,3–8 Gout is a chronic disease characterized by acute arthritis symptoms such as pain, swelling, heat, redness in the affected joint, which can cause difficulty of walking and other activities.9 Moreover, renal underexcretion of urate is a major contributor to hyperuricemia.10 In mainland China, the prevalence of hyperuricemia is about 13.3%, with a significantly higher prevalence in men (19.4%) than that in women (7.9%).11
In recent years, precision medicine has drawn a significant attention. Precision medicine is the practice of providing tailored and efficient diagnostics and treatments for patients based on individual genetic characteristics, including single-nucleotide polymorphisms (SNPs).12,13 Studies have shown that the genetic effect on uric acid levels is estimated to account for 40–70%.14 Genetic variations such as SNPs can lead to differential uric acid excretion through altering the functions of urate transporters.2,15 Some dysfunctional SNP variants increase the risk of hyperuricemia and gout, affect the age of onset of hyperuricemia/gout, and are highly associated with a familial hyperuricemia/gout history.16
In particular, studies have indicated that the SUA concentration is affected by gene-environmental interactions, and the genetic effect on uric acid levels is different in different regions of the population.2,17–19 For instance, a genome-wide association study identified two genetic loci (SLC2A9 and ABCG2) affecting SUA concentrations in the Chinese population.19 GCKR (P = 5.12×10−6) and SLC17A1 (P = 1.73×10−3) genetic variants associated with serum uric acid levels were detected in a genome-wide association study in the Japanese population.20 A case-control study replicated and confirmed that GCKR and SLC17A1 are associated with SUA and gout in Chinese.21 In particular, the most common dysfunction variant ABCG2 rs2231142 increases the risk of gout and hyperuricemia in different regions including Asia.22–26 ABCG2 rs72552713 has been widely studied in Asian populations, and 1–2 alleles (A) of rs72552713 have been proved to be associated with an increased risk of hyperuricemia and gout in Asian populations.4,26–28 The ABCG2 rs2231137 variant is identified as a protective effect from gout with high probability29 and reduces the risk of gout by approximately 36–57% in Asians.26 The protective effect of GCKR rs780094 polymorphism on SUA concentration and hyperuricemia was first found in a GWAS of European ancestry30 and was subsequently confirmed in Japanese and Chinese populations.19,20 The SNP rs1014290 G allele of SLC2A9 has been reported to protect against gout and hyperuricemia in Asian populations,31–33 and homozygous loss-of-function mutations in SLC2A9 cause massive renal hypouricemia via total loss of uric acid absorption.34 In a GWAS and a case-control study, SLC17A1 rs1183201 polymorphism was confirmed to be associated with SUA concentrations in Japanese population and Han Chinese.20,21 Therefore, revealing SNPs associated with serum uric acid levels in a specific population will help better understanding the prevalence of hyperuricemia and gout.
Noticeably, recent studies have shown that the incidence of hyperuricemia tends to be younger in the Chinese population.35,36 Interestingly, we have found a high prevalence of hyperuricemia among Chinese flight attendants, aged from 20 to 40, in our survey. The demanding tasks and unique working environment such as exposing in cosmic radiation, poor cabin air quality, hypoxia and vibrations make flight attendants become more prone to poor health conditions, for instance fatigue, musculoskeletal disorders, cancer, heart disease, depression and sleep disorders.37–42 Thus, we questioned whether it is a coincidence or there is a genetic reasoning of high prevalence of hyperuricemia in Chinese flight attendants.
In this study, to investigate the association of genetic variants with the risk of hyperuricemia among Chinese flight attendants, we selected and examined variants of six SNPs in ABCG2, GCKR, SLC2A9 and SLC17A1 genes, which have been reported to be strongly associated with SUA or gout in Asians. We have found that SNPs such as ABCG2 rs2231142, GCKR rs780094 and SLC2A9 rs1014290 are associated with hyperuricemia in male flight attendants. Our study has highlighted potential genetic variants that may help early prevention of hyperuricemia and gout, in particular among flight attendants.
Materials and Methods
Participants
We recruited 4114 Chinese flight attendants, including 867 males and 3247 females, for basic physical examinations from the Xiamen Aviation, Xiamen, Fujian, China from May 2020 to September 2021. Serum uric acid (SUA) levels of the participants under normal purine diet were measured after fasting. Hyperuricemia was determined when the concentration of SUA is higher than 420 µmol/L (7.0 mg/dL) in males and higher than 360 µmol/L (6.0 mg/dL) in females. Demographic characteristics and medical history of the participants were collected by questionnaires.
To explore the association of gene polymorphisms with hyperuricemia, 532 subjects were selected from the 4114 flight attendants for genotyping analyses. Among the 532 subjects, 276 subjects with high SUA levels, including 160 males and 116 females, were grouped as a hyperuricemia group. 256 subjects with normal SUA levels, including 138 males and 118 females, were randomly selected and grouped as a control group. These subjects were selected according to the following inclusion criteria: (1) no history of gout or acute onset of gouty arthritis. (2) no history of significant liver or renal dysfunction. (3) no history of cardiovascular disease, hypertension, diabetes and active malignancy. (4) no treatment with an anti-hyperuricemia agent or diuretics within 4 weeks before the start of the study (Table 1). Physical conditions of enrolled subjects, including age, body mass index (BMI), uric acid, fasting serum glucose, ratio of aspartate aminotransferase/alanine aminotransferase (AST/ALT), direct bilirubin (DBIL), albumin, cholesterol, blood urea nitrogen (BUN) and lactate dehydrogenase (LDH) were examined.
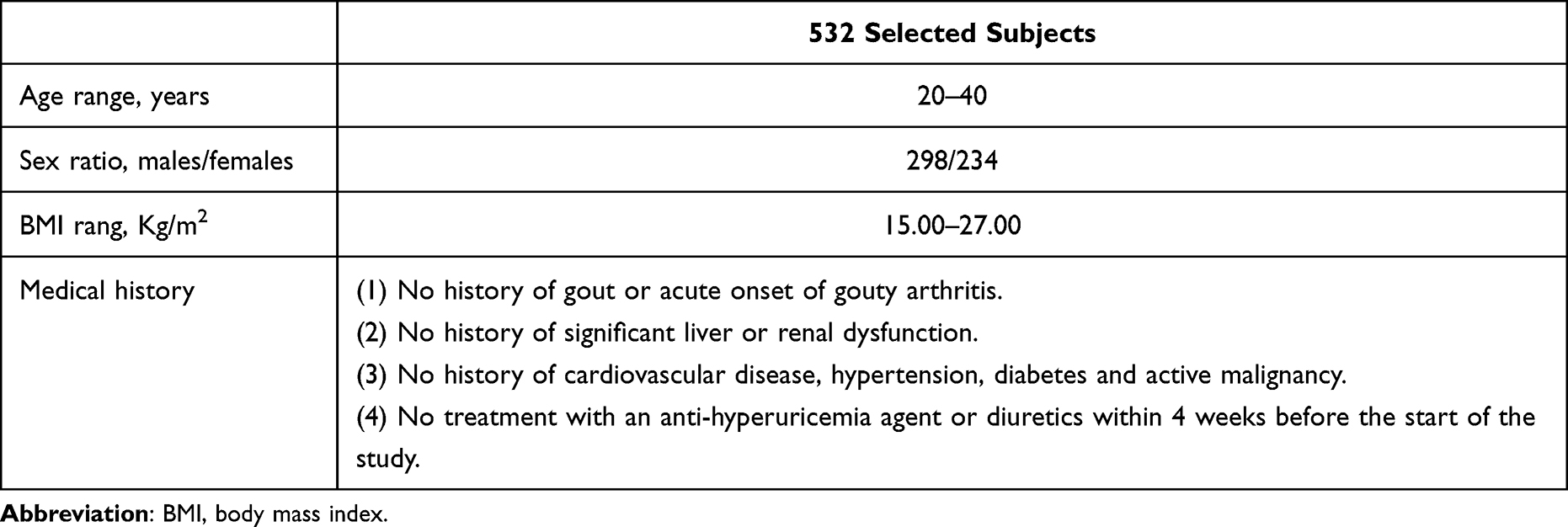 |
Table 1 Information of 532 Selected Subjects |
The study was in accordance with the principles of the Declaration of Helsinki. The study was approved by the Ethical Committee of the Xiamen Aviation and the Quanzhou First Hospital (20162016). Each subject provided written informed consent before participating.
Processes
Peripheral blood samples were collected from 532 enrolled subjects. Physical examinations were conducted and plasma samples were used for standard biochemical tests.
Blood sample DNA was extracted using the blood genomic DNA Midi kit (Jiangsu Conway Century Biotechnology Co., Ltd., China), according to the manufacturer’s instructions. Polymorphisms of the six SNPs including ABCG2 (rs2231142, rs72552713 and rs2231137), GCKR (rs780094), SLC2A9 (rs1014290) and SLC17A1 (rs1183201) were examined using allele-specific polymerase chain reaction (AS-PCR). The Primer Premier 5 software was used, and specific wild-type (W) and mutant (M) primers were designed according to the principles of base complementary pairing and mismatch (Table 2).
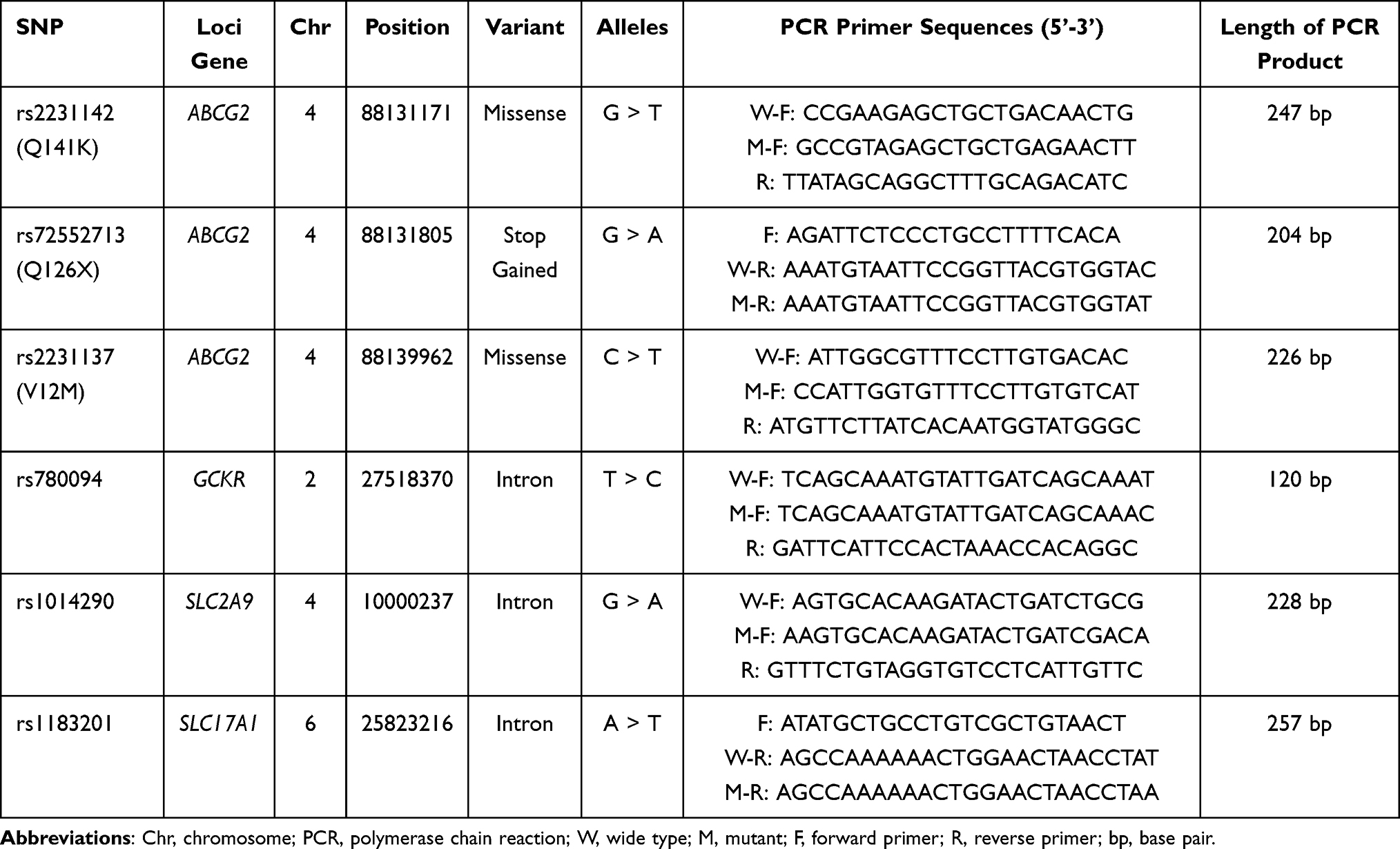 |
Table 2 Six SNPs and Primer Sequences for PCR Analyses |
PCR amplification was performed in a 20µL volume reaction, containing 10 µL 2 × STBR Green PCR Master Mix (Beijing Biterbo Biotechnology Co., Ltd., Beijing, China), 7.6 µL DNase-free water, 0.4 µL ROX Reference, 0.5 µL primers and 50 ng DNA. DNA was denatured at 95°C for 30s, followed by 40 cycles of denaturation at 95°C for 5s, annealing and extension at 60°C for 30s, running in an Applied Biosystems Quant Studio 6 (Applied Biosystems, USA). The results were analyzed using the QuantStudio 6 Flex Real-Time PCR system (Applied Biosystems, USA). The genotypes were interpreted according to ΔCt calculation and analysis. Some genotypes were further verified using the Sanger sequencing.
Statistical Analysis
The SPSS version 17.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. The biochemical baseline characteristics of the two groups were analyzed using Student’s t-test. A one-way analysis of variance (ANOVA) was used to evaluate differences in SUA levels within each genotype. Data were presented as mean ± standard deviation (SD). Categorical variables, including Hardy-Weinberg equilibrium (HWE), differences in single gene frequency and genotype distribution between two groups were estimated by Chi-Square test. Moreover, the HWE, odds ratio (OR) values, 95% confidence intervals (95% CI) and differences of genotypes and allele frequency between the two groups were analyzed to verify SNPs by using the SHEsis platform (http://analysis.bio-x.cn/myAnalysis.php).43 Logistic regression analysis was applied to adjust for covariates differentially distributed in case-control cohorts. P value <0.05 was considered to be statistically significant (double tail).
Results
Prevalence of Hyperuricemia Among Recruited Flight Attendants
To investigate whether there is an association of genetic variants with the risk of hyperuricemia among Chinese flight attendants, we recruited 4114 flight attendants, including 867 males and 3247 females, for basic physical examinations. The average age of the participants was 27.14 ± 4.85 years old (26.60 ± 4.33 years old in males, 27.29 ± 4.98 in females). The mean levels of serum uric acid (SUA) were 322.12 ± 81.97 µmol/L (424.99 ± 79.18 µmol/L in males, 294.69 ± 57.15 µmol/L in females), equivalent to 5.42 ± 1.38 mg/dL (7.15 ± 1.33 mg/dL in males, 4.96 ± 0.96 mg/dL in females).
The ages and SUA levels showed significant sex differences. Among 867 male flight attendants, 427 (49.25%) had higher SUA levels (above 420 µmol/L (7.0 mg/dL)), and among 3247 female flight attendants, 381 (11.73%) displayed higher SUA levels (above 360 µmol/L (6.0 mg/dL)) (Table 3). Our study indicates that among recruited flight attendants, male flight attendants show an elevated prevalence of hyperuricemia than females. Interestingly, both male and female flight attendants display greatly higher prevalence of hyperuricemia than the overall Chinese population, which is 19.4% in men and 7.9% in women11 (Table 3).
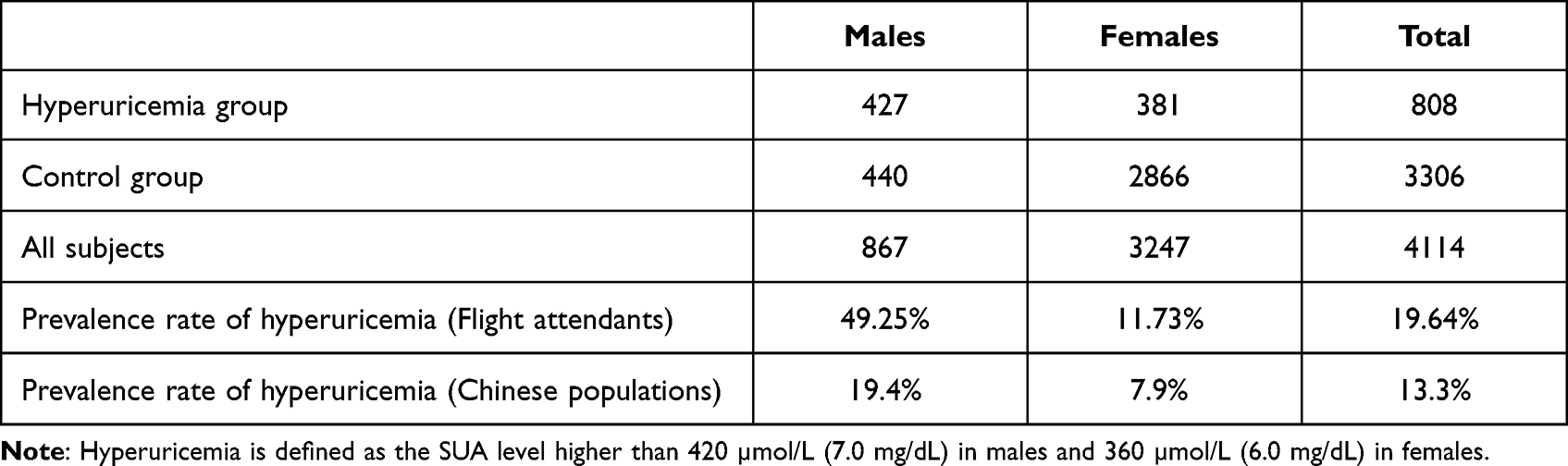 |
Table 3 Numbers of Hyperuricemia and Control Groups Among Recruited Flight Attendants |
Physical Examinations of Recruited Flight Attendants
We further selected 276 subjects with high SUA levels as a hyperuricemia group. 256 subjects with normal SUA levels as a control group according to the inclusion criteria (Table 1).
Basic physical examinations were performed among selected 532 subjects (Table 4). In all subjects, individuals in the hyperuricemia group were younger in the age, had higher levels of cholesterol and lactate dehydrogenase (LDH), compared to the control group (Table 4). There was no significant difference in body mass index (BMI), in levels of fasting serum glucose, aspartate aminotransferase/alanine aminotransferase (AST/ALT), direct bilirubin (DBIL), albumin and blood urea nitrogen (BUN) between the two groups. Subjects in the male hyperuricemia group were younger in the age, and displayed a lower ratio of AST/ALT and a higher level of LDH, while those in the female group also were younger, and showed a higher ratio of AST/ALT and the level of cholesterol, compared to their respective controls (P <0.05). These data suggest that flight attendants with hyperuricemia are overall in normal physical conditions.
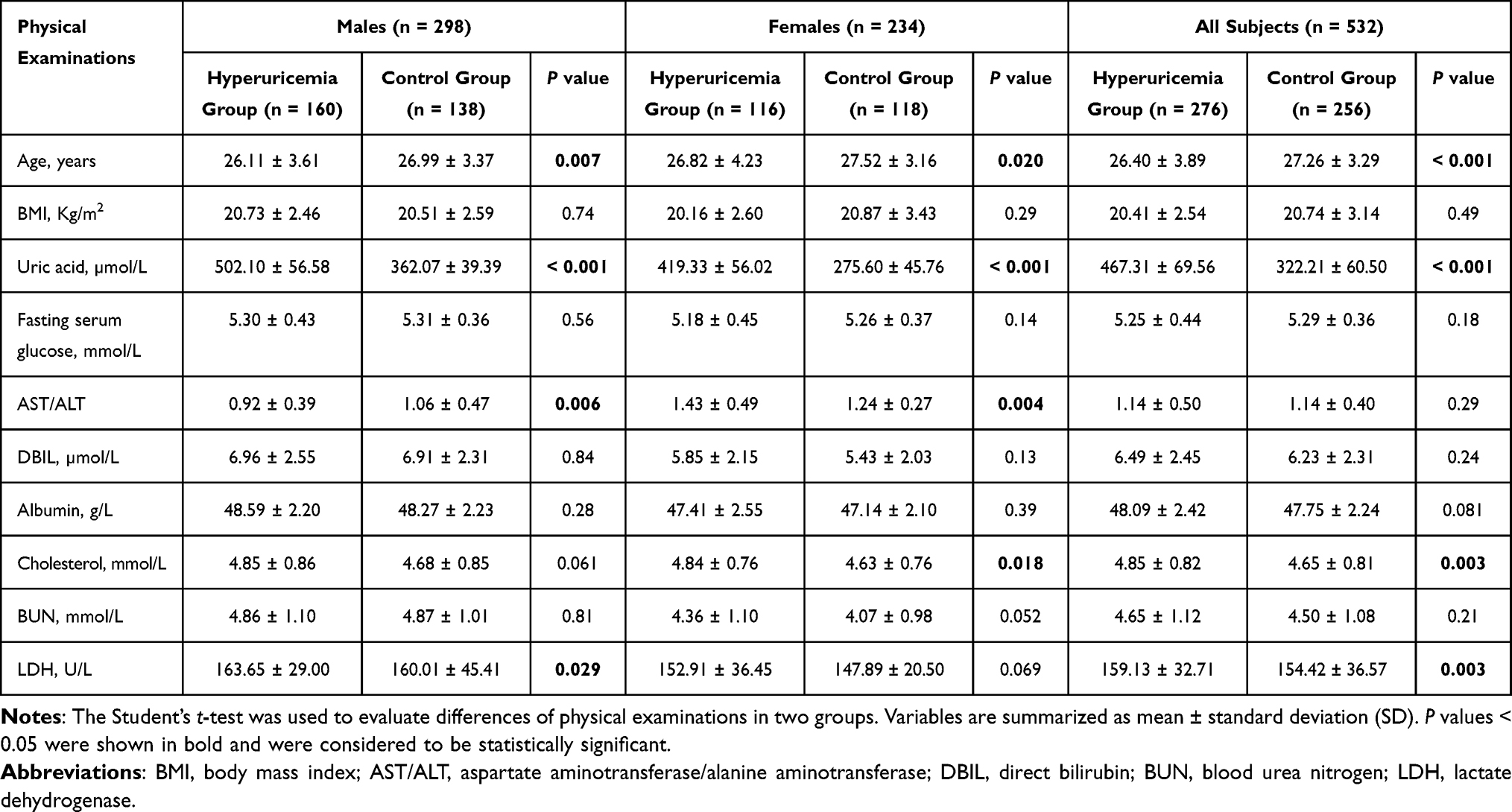 |
Table 4 Physical Examinations of Hyperuricemia and Control Groups |
Association of Genetic Variants with Hyperuricemia in Male Flight Attendants
Because male flight attendants showed a higher prevalence of elevated SUA than males of the Chinese population (Table 3), we examined whether there is a link of genetic variants with hyperuricemia in recruited male hyperuricemia and control groups. Previous studies have reported that polymorphisms of ABCG2, rs2231142 (Q141K), rs72552713 (Q126X) and rs2231137 (V12M); GCKR, rs780094; SLC2A9, rs1014290 and SLC17A1, rs1183201 might be associated with hyperuricemia,21,26,44,45 we thus decided to analyze these six SNPs among studied subjects by performing AS-PCR (Table 2). Except the SNP rs2231137 of ABCG2 (P < 0.05 in controls), genotype distributions of other SNPs in the two groups were in accordance with the Hardy-Weinberg equilibrium (HWE) test (P > 0.05).27 Therefore, we conducted SNP analyses only on the congruent 5 gene loci (Table 5).
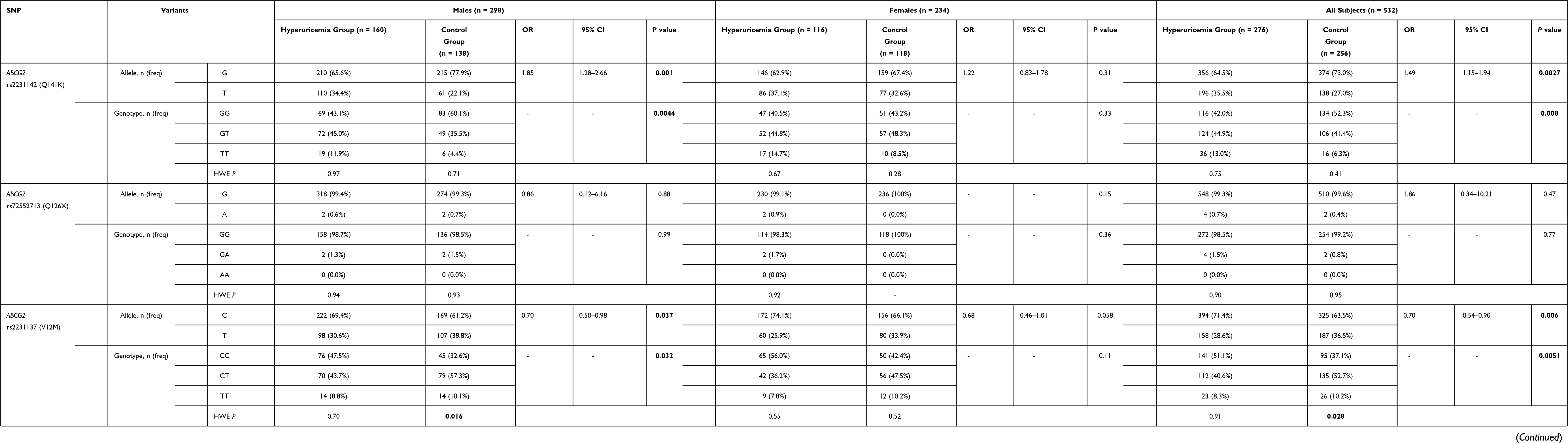 |
Table 5 Allele Frequencies and Genotype Distributions of Six SNPs Among Flight Attendants |
Among male flight attendants, the frequency of the minor T allele of the ABCG2 rs2231142 (Q141K) variant reached 34.4% in the hyperuricemia group and 22.1% in the control. The genotype frequencies of the SNP rs2231142 were 43.1% for GG, 45.0% for GT, and 11.9% for TT in the hyperuricemia group, and were 60.1% for GG, 35.5% for GT, and 4.4% for TT in the control (Table 5). Genotyping results of ABCG2 rs2231142 were further verified using Sanger sequencing (Figure 1). Moreover, the frequency of the minor A allele in the rs72552713 (Q126X) of ABCG2 was 0.6% in the hyperuricemia group and 0.7% in controls. No significant difference in the distribution of genotypes and allele in rs72552713 (P > 0.05) was observed between the two groups. These results indicate that the T allele, GT and TT genotypes in rs2231142 of ABCG2 have a significantly higher frequency in the male hyperuricemia group than in the male control.
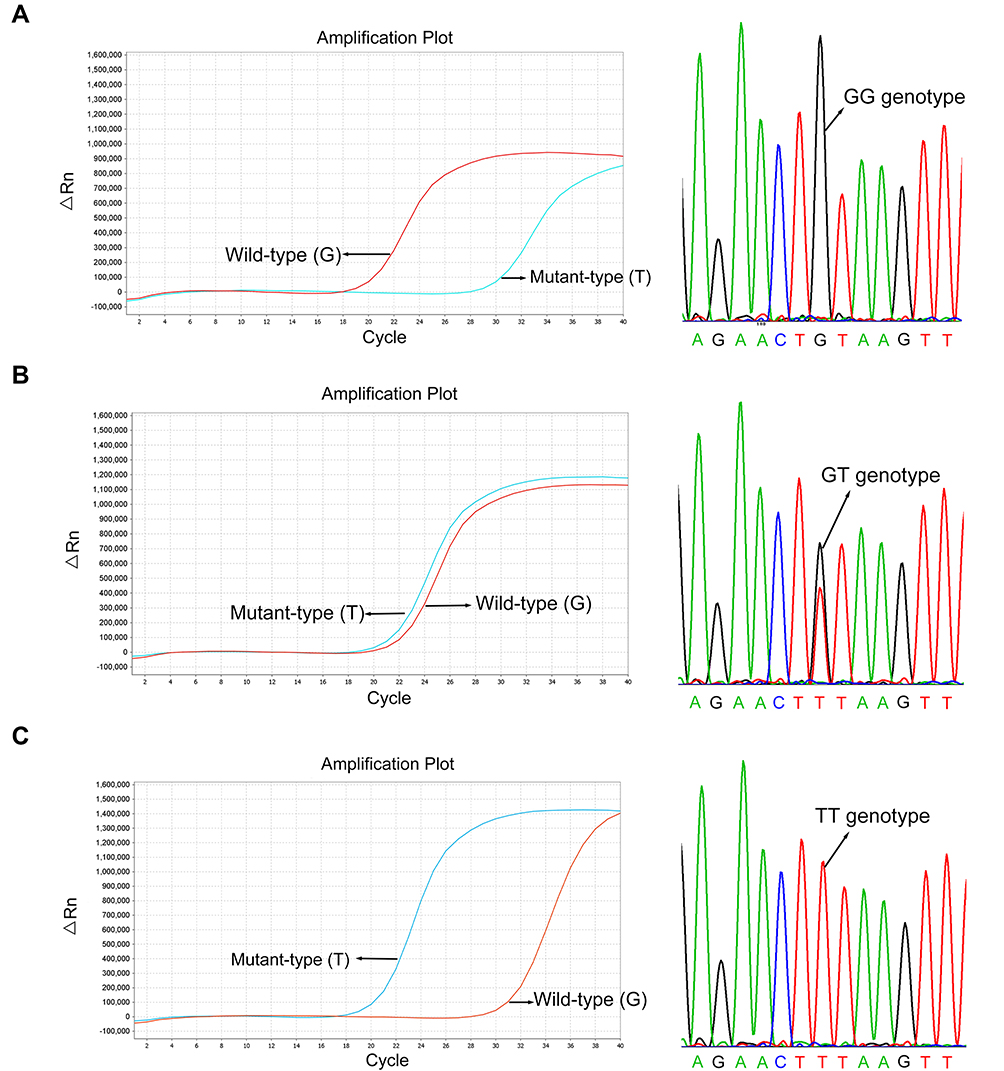 |
Figure 1 Detection of variants of the ABCG2 rs2231142 using allele-specific polymerase chain reaction (AS-PCR) and sanger sequencing (right panel). Real-time PCR amplification plots (left panel) and genotype verifications using sequencing were presented in GG genotype (A), GT genotype (B) and TT genotype (C) of the rs2231142. The same set of DNA samples were used for AS-PCR and DNA sequencing. |
Furthermore, a logistic regression analysis was performed using variants of ABCG2 rs2231142 and each of the confounding factors associated with the hyperuricemia in males (Table 6). After adjustments for ages, AST/ALT and LDH, we found that the T allele of ABCG2 rs2231142 increases the risk of hyperuricemia, and the GT and TT genotypes have significantly higher probability of suffering from hyperuricemia than the ones with GG genotype. These analyses further suggest that carrying the T allele in rs2231142 of ABCG2 could be a risk factor of hyperuricemia among male flight attendants (Figure 2A).
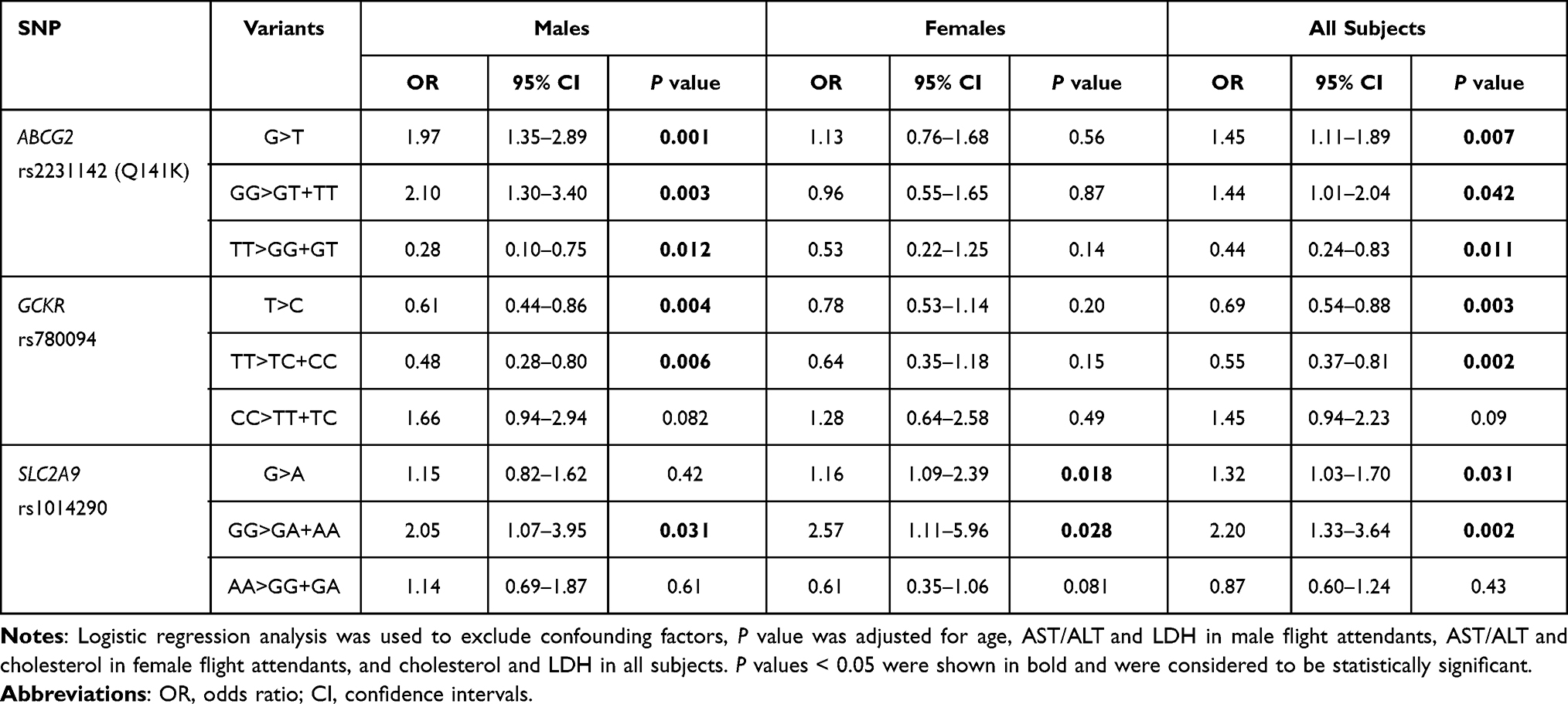 |
Table 6 Associations Between the Variants of Three SNPs and Hyperuricemia After Exclusion of Confounders |
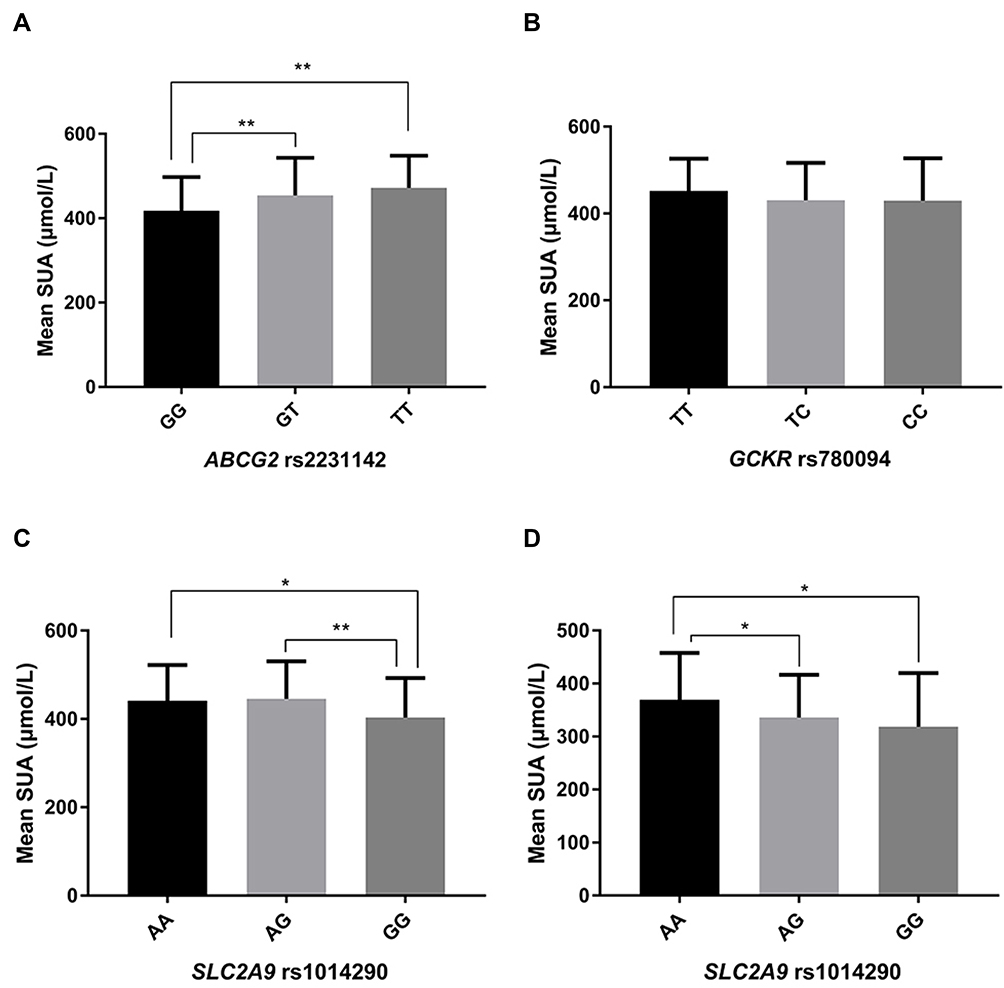 |
Figure 2 Average levels of serum uric acid (SUA) among different genotypes of SNPs, including ABCG2 rs2231142 (A), GCKR rs780094 (B), and SLC2A9 rs1014290 (C) in male flight attendants, and SLC2A9 rs1014290 (D) in female flight attendants. Statistical differences between groups were determined by a one‑way analysis of variance. P < 0.05 was considered to be statistically significant. *P < 0.05 and **P < 0.01. |
For the GCKR gene, the frequency of the C allele of GCKR rs780094 exhibited 40.3% in the hyperuricemia group and 51.4% in the control group (Table 5). The genotype frequencies were 38.7% for TT, 41.9% for TC, and 19.4% for CC in the hyperuricemia group, and were 23.2% for TT, 50.7% for TC, and 26.1% for CC in controls. These data indicate that the C allele, TC and CC genotypes of rs2231142 have a higher frequency in the male control than in the male hyperuricemia group. After adjustments for ages, AST/ALT and LDH, we found that the C allele in rs780094 is likely a protective factor for hyperuricemia development, the TC and CC genotypes exhibit a lower tendency toward hyperuricemia compared to those with the TT genotype (Table 6). However, SUA levels did not show significant differences among the three genotyping groups (Figure 2B). These results suggest that the C allele of GCKR rs780094 might have a protective effect on developing hyperuricemia among male flight attendants.
For the SNP SLC2A9 rs1014290, the frequency of the G allele showed 38.1% in the hyperuricemia group and 42.8% in the control group. The allele distribution of SLC2A9 rs1014290 did not show a significant difference between the two groups (P = 0.25). Genotype frequencies were 35.0% for AA, 53.8% for AG, and 11.2% for GG in the hyperuricemia group, and were 36.2% for AA, 42.0% for AG, and 21.7% for GG in controls (Table 5). After adjustments for ages, AST/ALT and LDH, we showed that the GA and AA genotypes have a higher tendency toward hyperuricemia compared to those with the GG genotype (Table 6). Because subjects with the GG genotype of SLC2A9 rs1014290 had lower uric acid concentration than those with AA or AG genotypes (Figure 2C), our results suggest that the GG genotype of SLC2A9 rs1014290 might play a protective role in hyperuricemia development among male flight attendants.
Moreover, for the SNP site of SLC17A1 rs1183201, the frequency of the T allele showed 83.4% and 81.2% in the hyperuricemia and control group, respectively (Table 5). The frequency distributions of alleles and genotypes did not show statistic differences between the two groups in male flight attendants, suggesting a subtle link of the SLC17A1 rs1183201 with hyperuricemia.
In summary, our analyses indicate that SNPs such as ABCG2 rs2231142, GCKR rs780094 and SLC2A9 rs1014290 are likely associated with hyperuricemia in male flight attendants.
Association of Genetic Variants with Hyperuricemia in Female Flight Attendants
We next analyzed whether the above genetic variants are as well associated with hyperuricemia among female flight attendants. We found that for the ABCG2 gene, the frequencies of the allele and genotypes of SNPs rs2231142 and rs72552713 do not show significant differences between the hyperuricemia and control groups among female flight attendants (Table 5). Similarly, the frequencies of the allele and genotypes of GCKR rs780094 and SLC17A1 rs1183201 did not exhibit significant differences in female flight attendants. These analyses indicate that the genetic variants of ABCG2, GCKR and SLC17A1 are unlikely linked with hyperuricemia among female flight attendants.
Noticeably, for the SNP SLC2A9 rs1014290, the frequencies of A allele showed 68.1% and 57.6% in the hyperuricemia and control groups, respectively (Table 5). Genotype frequencies were 44.8% for AA, 46.6% for AG, and 8.6% for GG in the hyperuricemia group, and were 33.9% for AA, 47.5% for AG, and 18.6% for GG in controls, indicating that distributions of allele and genotypes of rs1014290 are significantly different in female hyperuricemia and control groups (Table 5). After adjustments for ages, AST/ALT and cholesterol, we found that the A allele of SLC2A9 rs1014290 increases the risk of hyperuricemia, the AA and AG genotypes are associated with an increased risk of hyperuricemia compared to those with the GG genotype (Table 6). Furthermore, subjects with the AA genotype of SLC2A9 rs1014290 showed a significantly higher SUA concentration than those carrying AG or GG genotypes (Figure 2D), suggesting that the AA genotype in SLC2A9 rs1014290 might be a risk factor of hyperuricemia among female flight attendants.
Discussion
Accumulating studies have reported SNPs associated with serum uric acid levels in a specific population. In this study we have detected a higher prevalence rate of hyperuricemia in Chinese flight attendants, and examined variants in six SNPs including ABCG2 (rs2231142, rs72552713 and rs2231137), GCKR (rs780094), SLC2A9 (rs1014290) and SLC17A1 (rs1183201). We have provided genetic support of associations between SNPs and the occurrence of hyperuricemia in Chinese flight attendants. Our work should help develop potential SNPs for early diagnostics and prevention of diseases related to specific occupations such as flight attendants.
ABCG2, located on human chromosome 4q22, encodes an ATP-binding cassette transporter, which is responsible for transport and excretion of uric acid in the kidney and intestine.46,47 GWAS and meta-analyses have shown the association of ABCG2 polymorphisms with SUA and hyperuricemia.14,17,24,26,30 The link between ABCG2 variants and hyperuricemia has been shown in populations of different ethnic backgrounds including Asians, Europeans, African Americans, and American Indians.48–50 Among common variants of the ABCG2 gene, rs2231142 (Q141K), rs72552713 (Q126X) and rs2231137 (V12M) are in the uric-acid-related loci. While variants Q141K and Q126X were reported as risk factors that are associated with hyperuricemia and gout, V12M also was identified as a protective variant with high probability in different ethnic groups.29 In particular, the ABCG2 Q141K minor allele (T) was confirmed to increase the risk of hyperuricemia and promote development of gout.22–26 Knock-in mouse model of the human Q141K variant of ABCG2 showed significant hyperuricemia, which further supports the important role of ABCG2 in urate excretion.47 The minor allele (T) of ABCG2 rs2231142 had a weaker effect on uric acid level in females.30 In a GWAS study of the Chinese population, the T allele of rs2231142 in ABCG2 displayed a gender difference with its higher effect on serum uric acid level in males than in females.19 Moreover, the dysfunctional variants of Q141K and Q126X of ABCG2 increase the risk of gout and hyperuricemia.44,51,52
In agreement with previous studies, we have found that the variant (carrying minor allele T) of rs2231142 (Q141K) in the ABCG2 gene is significantly correlated with hyperuricemia among male flight attendants, indicating rs2231142 (Q141K) a risk factor of hyperuricemia among flight attendants. However, the significant association was not found among females. Causal mechanisms of sex-specific differences with the effect of ABCG2 variants on hyperuricemia or gout are unclear.23 Studies have suggested that intervene of some hormones (oestrogen and progesterone) might contribute to differences in the regulation of SUA balance between males and females.53,54 Moreover, studies have shown that carrying 1–2 minor-allele-genotypes and allele C of rs72552713 (Q126X), and carrying rs2231137 (V12M) are associated with increased risk of hyperuricemia and gout in Asians.4,26–28 However, we have not detected significant differences in the distributions of genotypes and allele of these two SNPs between the hyperuricemia and control groups among both male and female flight attendants in this study. This different finding might be caused by the relatively small sample size.
Moreover, the GCKR gene, located on chromosome 2p23.2–3, encodes a glucokinase regulatory protein that is involved in regulating glucose metabolism and balance.55 Studies have reported that while the frequency of C (G) allele of GCKR rs780094 is high in normal controls, the variant of GCKR rs780094 is significantly associated with the development of gout in the male Han and Uygur Chinese populations and in Caucasians.21,45,56–58 In consistence with previous studies, we have found that the C allele of rs780094 is highly detected in the control group than the hyperuricemia group in male flight attendants, which hints a protective effect of CT and CC genotypes from developing hyperuricemia. Functional experiments are required to explore mechanisms of the protective role of the C allele of rs780094 in hyperuricemia and gout in the future.21
In addition, the SLC2A9 gene (4p16.1) is expressed in renal epithelial cells and encodes Glucose transporter 9 (GLUT9), which is a protein of the facilitative glucose transporter family and a transporter for both fructose and urate.32 The SNP rs1014290 of the SLC2A9 gene has been reported to protect subjects from the development of gout and hyperuricemia.31,32 Individuals with rs1014290 GG (CC) genotypes had the lowest uric acid levels among the Han Chinese population.33 Similarly, we here have found that the rs1014290 GG genotype has a lower uric acid level among both male and female flight attendants, suggesting a protective role of polymorphisms of SLC2A9 in hyperuricemia development. Moreover, SLC17A1 encodes sodium phosphate transport protein 1 (NPT1) and mediates sodium and inorganic phosphate co-transport. The SNP rs1183201 in SLC17A1 has been shown to be associated with gout arthritis and uric acid concentrations in New Zealand Caucasians and Han Chinese.21,59 However, we did not detect a significant link of rs1183201 variants with hyperuricemia among Chinese flight attendants in this study.
Conclusion
In summary, our study has identified a higher prevalence of hyperuricemia in Chinese flight attendants, in particular in males. We have provided evidence of a strong association of three SNPs including ABCG2 rs2231142, GCKR rs780094 and SLC2A9 rs1014290, with hyperuricemia in Chinese flight attendants. We also have noticed the gender difference of genetic variations in hyperuricemia, with a higher prevalence and stronger genetic association in men than in women, which has as well been observed in previous studies. Identifying SNPs associated with diseases can help diagnose and prevent disease development such as uric acid metabolism disorders and gout. Evaluating health issues of flight attendants can help improve the quality of passenger service and the safety of aviation operation.
Ethics Approval and Consent to Participate
The study was in accordance with the principles of the Declaration of Helsinki. The study was approved by the Ethical Committee of the Xiamen Aviation and the Quanzhou First Hospital (20162016). Each subject provided written informed consent before participating.
Funding
This work was supported by the Scientific Research Funds of Huaqiao University (Z16Y0017, T.S.), and the National Natural Science Foundation of China (31771141).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Richette P, Bardin T. Gout. Lancet. 2010;375(9711):318–328. doi:10.1016/S0140-6736(09)60883-7
2. Reginato AM, Mount DB, Yang I, Choi HK. The genetics of hyperuricaemia and gout. Nat Rev Rheumatol. 2012;8(10):610–621. doi:10.1038/nrrheum.2012.144
3. Shipley M. Hyperuricaemia and gout. J R Coll Physicians Edinb. 2011;41(3):229–233. doi:10.4997/JRCPE.2011.311
4. Wang X, Wang J, Zhao C, Song J, Tian G, Li Y. Polymorphism of ABCG2 gene in hyperuricemia patients of Han and Uygur ethnicity with phlegm/non-phlegm block in Xinjiang, China. Med Sci Monit. 2018;24:6305–6312. doi:10.12659/MSM.908552
5. Borghi C, Rosei EA, Bardin T, et al. Serum uric acid and the risk of cardiovascular and renal disease. J Hypertens. 2015;33(9):
6. Li X, Meng X, Timofeeva M, et al. Serum uric acid levels and multiple health outcomes: umbrella review of evidence from observational studies, randomised controlled trials, and Mendelian randomisation studies. BMJ. 2017;357:j2376.
7. Johnson RJ, Nakagawa T, Sanchez-Lozada LG, et al. Sugar, uric acid, and the etiology of diabetes and obesity. Diabetes. 2013;62(10):3307–3315.
8. Wu J, Qiu L, Cheng XQ, et al. Hyperuricemia and clustering of cardiovascular risk factors in the Chinese adult population. Sci Rep. 2017;7(1):5456.
9. Dalbeth N, Merriman TR, Stamp LK. Gout. Lancet. 2016;388(10055):2039–2052.
10. Sakurai H. Urate transporters in the genomic era. Curr Opin Nephrol Hypertens. 2013;22(5):545–550. doi:10.1097/MNH.0b013e328363ffc8
11. Liu R, Han C, Wu D, et al. Prevalence of hyperuricemia and gout in Mainland China from 2000 to 2014: a systematic review and meta-analysis. Biomed Res Int. 2015;2015:762820. doi:10.1155/2015/762820
12. Cascorbi I. Significance of pharmacogenomics in precision medicine. Clin Pharmacol Ther. 2018;103(5):732–735. doi:10.1002/cpt.1052
13. Dalbeth N, Stamp LK, Merriman TR. The genetics of gout: towards personalised medicine? BMC Med. 2017;15(1):108. doi:10.1186/s12916-017-0878-5
14. Köttgen A, Albrecht E, Teumer A, et al. Genome-wide association analyses identify 18 new loci associated with serum urate concentrations. Nat Genet. 2013;45(2):145–154. doi:10.1038/ng.2500
15. Tin A, Marten J, Halperin Kuhns VL, et al. Target genes, variants, tissues and transcriptional pathways influencing human serum urate levels. Nat Genet. 2019;51(10):1459–1474. doi:10.1038/s41588-019-0504-x
16. Stiburkova B, Pavelcova K, Pavlikova M, Ješina P, Pavelka K. The impact of dysfunctional variants of ABCG2 on hyperuricemia and gout in pediatric-onset patients. Arthritis Res Ther. 2019;21(1):77. doi:10.1186/s13075-019-1860-8
17. Dehghan A, Köttgen A, Yang Q, et al. Association of three genetic loci with uric acid concentration and risk of gout: a genome-wide association study. Lancet. 2008;372(9654):1953–1961. doi:10.1016/S0140-6736(08)61343-4
18. Major TJ, Dalbeth N, Stahl EA, Merriman TR. An update on the genetics of hyperuricaemia and gout. Nat Rev Rheumatol. 2018;14(6):341–353. doi:10.1038/s41584-018-0004-x
19. Yang B, Mo Z, Wu C, et al. A genome-wide association study identifies common variants influencing serum uric acid concentrations in a Chinese population. BMC Med Genomics. 2014;7(1):10. doi:10.1186/1755-8794-7-10
20. Kamatani Y, Matsuda K, Okada Y, et al. Genome-wide association study of hematological and biochemical traits in a Japanese population. Nat Genet. 2010;42(3):210–215. doi:10.1038/ng.531
21. Zhou ZW, Cui LL, Han L, et al. Polymorphisms in GCKR, SLC17A1 and SLC22A12 were associated with phenotype gout in Han Chinese males: a case-control study. BMC Med Genet. 2015;16(1):66. doi:10.1186/s12881-015-0208-8
22. Wrigley R, Phipps-Green AJ, Topless RK, et al. Pleiotropic effect of the ABCG2 gene in gout: involvement in serum urate levels and progression from hyperuricemia to gout. Arthritis Res Ther. 2020;22(1):45. doi:10.1186/s13075-020-2136-z
23. Narang RK, Topless R, Cadzow M, et al. Interactions between serum urate-associated genetic variants and sex on gout risk: analysis of the UK biobank. Arthritis Res Ther. 2019;21(1):13. doi:10.1186/s13075-018-1787-5
24. Chen CJ, Tseng CC, Yen JH, et al. ABCG2 contributes to the development of gout and hyperuricemia in a genome-wide association study. Sci Rep. 2018;8(1):3137. doi:10.1038/s41598-018-21425-7
25. Cheng ST, Wu S, Su CW, Teng MS, Hsu LA, Ko YL. Association of ABCG2 rs2231142-A allele and serum uric acid levels in male and obese individuals in a Han Taiwanese population. J Formos Med Assoc. 2017;116(1):18–23. doi:10.1016/j.jfma.2015.12.002
26. Lukkunaprasit T, Rattanasiri S, Turongkaravee S, et al. The association between genetic polymorphisms in ABCG2 and SLC2A9 and urate: an updated systematic review and meta-analysis. BMC Med Genet. 2020;21(1):210. doi:10.1186/s12881-020-01147-2
27. Duong NT, Ngoc NT, Thang NTM, et al. Polymorphisms of ABCG2 and slc22a12 genes associated with gout risk in Vietnamese population. Medicina. 2019;55(1). doi:10.3390/medicina55010008.
28. Tu HP, Ko AM, Chiang SL, et al. Joint effects of alcohol consumption and ABCG2 Q141K on chronic tophaceous gout risk. J Rheumatol. 2014;41(4):749–758. doi:10.3899/jrheum.130870
29. Stiburkova B, Pavelcova K, Zavada J, et al. Functional non-synonymous variants of ABCG2 and gout risk. Rheumatology. 2017;56(11):1982–1992. doi:10.1093/rheumatology/kex295
30. Kolz M, Johnson T, Sanna S, et al. Meta-analysis of 28,141 individuals identifies common variants within five new loci that influence uric acid concentrations. PLoS Genet. 2009;5(6):e1000504. doi:10.1371/journal.pgen.1000504
31. Tu HP, Min-Shan Ko A, Lee SS, et al. Variants of ALPK1 with ABCG2, SLC2A9, and SLC22A12 increased the positive predictive value for gout. J Hum Genet. 2018;63(1):63–70. doi:10.1038/s10038-017-0368-9
32. Lee YH, Seo YH, Kim JH, Choi SJ, Ji JD, Song GG. Associations between SLC2A9 polymorphisms and gout susceptibility: a meta-analysis. Z Rheumatol. 2017;76(1):64–70. doi:10.1007/s00393-016-0070-x
33. Miao J, Liu J, Xiao L, et al. The single nucleotide polymorphism rs1014290 of the SLC2A9 gene is associated with uric acid metabolism in parkinson’s disease. Parkinson's Dis. 2017;2017:7184927. doi:10.1155/2017/7184927
34. Stiburkova B, Ichida K, Sebesta I. Novel homozygous insertion in SLC2A9 gene caused renal hypouricemia. Mol Genet Metab. 2011;102(4):430–435. doi:10.1016/j.ymgme.2010.12.016
35. Shan R, Ning Y, Ma Y, et al. Incidence and risk factors of hyperuricemia among 2.5 million Chinese adults during the years 2017–2018. Int J Environ Res Public Health. 2021;18(5):2360. doi:10.3390/ijerph18052360
36. Cao J, Wang C, Zhang G, et al. Incidence and simple prediction model of hyperuricemia for urban Han Chinese adults: a prospective cohort study. Int J Environ Res Public Health. 2017;14(1):67. doi:10.3390/ijerph14010067
37. Nesthus T, Schroeder D, Connors M, Rentmeister-Bryant H, DeRoshina C. Flight attendant fatigue. Final report DOT/FAA/AM-07/21. Office of aerospace medicine, federal aviation administration: Washington, DC; 2007. Available from: http://www.dtic.mil/cgibin/GetTRDoc?AD=ADA471470.
38. Castro M, Carvalhais J, Teles J. Irregular working hours and fatigue of cabin crew. Work. 2015;51(3):505–511. doi:10.3233/WOR-141877
39. Griffiths RF, Powell DM. The occupational health and safety of flight attendants. Aviat Space Environ Med. 2012;83(5):514–521. doi:10.3357/ASEM.3186.2012
40. Hu CJ, Hong RM, Yeh GL, Hsieh IC. Insomnia, work-related burnout, and eating habits affecting the work ability of flight attendants. Aerosp Med Hum Perform. 2019;90(7):601–605. doi:10.3357/AMHP.5349.2019
41. McNeely E, Gale S, Tager I, et al. The self-reported health of U.S. flight attendants compared to the general population. Environ Health. 2014;13(1):13. doi:10.1186/1476-069X-13-13
42. Feijo D, Luiz RR, Camara VM. Common mental disorders among civil aviation flight attendants. Aviat Space Environ Med. 2014;85(4):433–439. doi:10.3357/ASEM.3768.2014
43. Shi YY, He L. SHEsis, a powerful software platform for analyses of linkage disequilibrium, haplotype construction, and genetic association at polymorphism loci. Cell Res. 2005;15(2):97–98. doi:10.1038/sj.cr.7290272
44. Nakashima A, Ichida K, Ohkido I, et al. Dysfunctional ABCG2 gene polymorphisms are associated with serum uric acid levels and all-cause mortality in hemodialysis patients. Hum Cell. 2020;33(3):559–568.
45. Wang L, Ma Q, Yao H, et al. Association of GCKR rs780094 polymorphism with circulating lipid levels in type 2 diabetes and hyperuricemia in Uygur Chinese. Int J Clin Exp Pathol. 2018;11(9):4684–4694.
46. Matsuo H, Takada T, Nakayama A, et al. ABCG2 dysfunction increases the risk of renal overload hyperuricemia. Nucleosides Nucleotides Nucleic Acids. 2014;33(4–6):266–274.
47. Hoque KM, Dixon EE, Lewis RM, et al. The ABCG2 Q141K hyperuricemia and gout associated variant illuminates the physiology of human urate excretion. Nat Commun. 2020;11(1):2767.
48. Zhang L, Spencer KL, Voruganti VS, et al. Association of functional polymorphism rs2231142 (Q141K) in the ABCG2 gene with serum uric acid and gout in 4 US populations: the PAGE study. Am J Epidemiol. 2013;177(9):923–932.
49. Yamagishi K, Tanigawa T, Kitamura A, Köttgen A, Folsom AR, Iso H. The rs2231142 variant of the ABCG2 gene is associated with uric acid levels and gout among Japanese people. Rheumatology. 2010;49(8):1461–1465.
50. Takeuchi F, Yamamoto K, Isono M, et al. Genetic impact on uric acid concentration and hyperuricemia in the Japanese population. J Atheroscler Thromb. 2013;20(4):351–367.
51. Nakayama A, Matsuo H, Nakaoka H, et al. Common dysfunctional variants of ABCG2 have stronger impact on hyperuricemia progression than typical environmental risk factors. Sci Rep. 2014;4:5227.
52. Higashino T, Takada T, Nakaoka H, et al. Multiple common and rare variants of ABCG2 cause gout. RMD Open. 2017;3(2):e000464.
53. Sumino H, Ichikawa S, Kanda T, Nakamura T, Sakamaki T. Reduction of serum uric acid by hormone replacement therapy in postmenopausal women with hyperuricaemia. Lancet. 1999;354(9179):650.
54. Merino G, van Herwaarden AE, Wagenaar E, Jonker JW, Schinkel AH. Sex-dependent expression and activity of the ATP-binding cassette transporter breast cancer resistance protein (BCRP/ABCG2) in liver. Mol Pharmacol. 2005;67(5):1765–1771.
55. Espinosa-Salinas I, de la Iglesia R, Colmenarejo G, et al. GCKR rs780094 polymorphism as a genetic variant involved in physical exercise. Genes. 2019;10(8):570.
56. Wang J, Liu S, Wang B, et al. Association between gout and polymorphisms in GCKR in male Han Chinese. Hum Genet. 2012;131(7):1261–1265.
57. Phipps-Green AJ, Merriman ME, Topless R, et al. Twenty-eight loci that influence serum urate levels: analysis of association with gout. Ann Rheum Dis. 2016;75(1):124–130.
58. Sandoval-Plata G, Morgan K, Abhishek A. Variants in urate transporters, ADH1B, GCKR and MEPE genes associate with transition from asymptomatic hyperuricaemia to gout: results of the first gout versus asymptomatic hyperuricaemia GWAS in Caucasians using data from the UK biobank. Ann Rheum Dis. 2021;80(9):1220–1226.
59. Hollis-Moffatt JE, Phipps-Green AJ, Chapman B, et al. The renal urate transporter SLC17A1 locus: confirmation of association with gout. Arthritis Res Ther. 2012;14(2):R92.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.