")
Back to Journals » Drug Design, Development and Therapy » Volume 16
Evolving Role of Silodosin for the Treatment of Urological Disorders – A Narrative Review
Authors Jindan L, Xiao W, Liping X
Received 6 May 2022
Accepted for publication 26 July 2022
Published 26 August 2022 Volume 2022:16 Pages 2861—2884
DOI https://doi.org/10.2147/DDDT.S373659
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Tuo Deng
Luo Jindan,* Wang Xiao,* Xie Liping
Department of Urology, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xie Liping, Department of Urology, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China, Email [email protected]
Abstract: Use of α-androgenic receptor blockers remains a mainstay therapeutic approach for the treatment of urological diseases. Silodosin is recommended over other α-blockers for the treatment of lower urinary tract symptoms (LUTS) and benign prostate hyperplasia (BPH), due to its high α1A uroselectivity. Current research data suggest that silodosin is efficacious in the management of various urological diseases. Thus, we herein review the current evidence of silodosin related to its efficacy and tolerability and appraise the available literature that might ultimately aid in management of various urological conditions at routine clinical practice. Literature reveals that silodosin is beneficial in improving nocturia events related to LUTS/BPH. Silodosin exerts effect on relaxing muscles involved in detrusor obstruction, therefore prolonging the need for patients undergoing invasive surgery. Silodosin treatment, either as a monotherapy or combination, significantly improves International Prostate Symptom Score (IPSS) including both storage and voiding symptoms in patients with BPH/LUTS. Patients on other treatment therapies such as phosphodiesterase 5 inhibitors or other α-blockers are well managed with this drug. Steadily, silodosin has proved beneficial in the treatment of other urological disorders such as chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS), overactive bladder/acute urinary retention (AUR), premature ejaculation (PE), and prostate cancer post brachytherapy-induced progression. In patients with distal ureteral stones, silodosin treatment is beneficial in decreasing stone expulsion time without affecting stone expulsion rate or analgesic need. Moreover, there were significant improvements in intravaginal ejaculation latency time, quality of life scores, and decrease in PE profile among patients with PE. Silodosin has also demonstrated promising results in increasing the likelihood of successful trial without catheter in patients with AUR and those taking antihypertensive drugs. Reports from Phase II studies have shown promising role of silodosin in the treatment of CP/CPPS as well as facilitating ureteral stone passage. From the robust data in this review, further silodosin treatment strategies in the management of different urological conditions need to be focused on.
Keywords: efficacy, benign prostate hyperplasia, ureteral calculi, prostatitis, silodosin, urological
Introduction
The field of urology encompasses disorders of the urinary tract and the genital system, both benign and malignant.1 Most men and women with urological disorders hugely suffer from a decreased quality of life (QoL) ultimately leading to economic burden.2,3 Urological disorders include urinary tract infections (UTIs), kidney stones, problems with bladder control and prostate, among others.4 While a few urological conditions prevail for a shorter period, others are long-lasting.4 With age, men in particular, experience urinary changes, which may be caused by inflammation or enlargement of the prostate gland.5
A typical bacterial infection acquired in the community and hospital settings is a UTI.6 Lower urinary tract symptoms (LUTS) are accompanied along with many other disorders such as acute urinary retention (AUR), bladder outlet obstruction (BOO), benign prostatic hyperplasia (BPH), ureteral calculi, chronic pelvic pain syndrome (CPPS), overactive bladder (OAB). The pathologies of each urological disorder are different, and there is still much progress to be made in available therapeutic options in order to minimize adverse events (AEs) and provide effective care.1 The conservative approach to treatment remains watchful waiting (WW), behavioral and dietary modifications till date. When conservative treatment fails to cure the disease, medical therapy with either α1-adrenoceptor antagonists (α1-blockers), 5α-reductase inhibitors, muscarinic receptor antagonists, phosphodiesterase 5 (PDE5) inhibitors, phytotherapy or β-3 agonist in monotherapy or in combination is preferred. In an era of an increasing array of treatment options, it has become of utmost clinical importance to refine therapeutic strategies in order to optimize efficacy while limiting systemic toxicity.1 Urological treatment often carries a high rate of undesirable AEs leading to greater rates of patient noncompliance.1
The American Urological Association (AUA) and European Association of Urology (EAU) guidelines state that, α1-blockers are the preferred treatment modality for patients with moderate/severe LUTS, BPH/LUTS, ureteral calculi, CPPS, OAB, and so on. α1-androgenic receptors (ARs) are highly concentrated along the urinary tract, bladder, and prostate.7 Typically, the α1B-receptors are found in vascular tissue, where they mediate arterial contraction, whereas α1A and α1D are more specific in the lower urinary tract. In general, α1-blockers focus on reducing the smooth muscle tone in the prostate and bladder neck by inhibiting the action of endogenously released noradrenaline on smooth muscle cells in the prostate.8 The smooth muscle tension within the prostate and bladder neck was found to be relieved, after 2 weeks of administration of α1-blockers.8 Previously published studies have established that α1-blockers reduce the International Prostate Symptom Score (IPSS) by 30–40% and increase maximum urinary flow rate (Qmax) by 20–25%.9 The most common AEs include dizziness, orthostatic hypotension, ejaculatory dysfunction (EjD), and asthenia. Treatment with doxazosin and terazosin increases vasodilating effects which are less pronounced with tamsulosin and alfuzosin. Similarly, it seemed that EjD was more frequent with tamsulosin or silodosin whereas it was less with doxazosin and terazosin. Based on such promising results, EAU has suggested the use of α1-blockers as the first-line treatment for LUTS since these agents do not prevent urinary retention or need for surgery.9
The first selective α-blocker, prazosin, was useful in lowering blood pressure.10 The efficacy and tolerability of prazosin have been proved by several trials.11,12 But, prazosin required multiple daily dosing and was associated with orthostatic hypotension. Terazosin was the first long-acting α1-AR blocker, which had an elimination half-life two to three times that of prazosin.13 Early clinical studies confirmed significant improvements in IPSS symptoms and flow rate in patients with LUTS.14–16 Doxazosin was first approved by the US Food and Drug Administration (FDA) for the treatment of symptomatic BPH based on 2 clinical trials17,18 and later, was approved for the treatment of BPH, due to its selectivity for subtype of α1-antagonist.19,20 Tamsulosin is known to achieve a therapeutic effect without dose titration and with minimal effects on blood pressure; however, EjD was a common side effect observed. Thus, alfuzosin was developed as a fourth-generation α1-blocker and approved by FDA based on 2 randomized clinical trials (RCTs).21,22 Alfuzosin 10 mg has proven to be clinically significant in LUTS without dose titration and showed comparable efficacy to tamsulosin without causing EjD.23 It has been a goal to create a therapeutic drug that suppresses the urethral contractions while reducing hypotension, including postural hypotension, in patients with BPH-related LUTS. The use of drugs that selectively antagonize the α1A-adrenergic receptor can reduce this effect. During the 1990s, Shibata et al24 discovered that the investigational drug silodosin had approximately 10-fold higher affinity at the cloned human alpha α1-AR than at the cloned rat alpha α1-AR. Subsequently, silodosin was developed in the treatment of BPH/LUTS. In this review, we aim to summarize the current evidence of silodosin, to appraise the available literature with respect to the efficacy and tolerability due to its uroselectivity, which may ultimately aid in the management of different urological conditions at routine clinical practices.
Methods
We performed a literature search on PubMed and Embase for articles published preferably in English as well as from other languages and were extrapolated if relevant from inception till June 2021, focusing on articles related to efficacy, safety, and tolerability of silodosin either in monotherapy or in combination with other therapies for urological disorders. We included the Medical Subject Headings (MeSH) terms “silodosin”, “alpha-blockers”, “alpha-adrenoreceptor antagonists”, “lower urinary tract symptoms”, “LUTS”, “Benign prostate hyperplasia”, “chronic pelvic pain syndrome”, “chronic prostatitis”, “ureteral calculi”, “ureteral stone/s”, “prostate cancer”, “urinary incontinence”, “premature ejaculation”, “pathophysiology”, “symptoms”, “overactive bladder”. We excluded publications if no clinical comparative information about efficacy/safety/tolerability of silodosin were reported.
Evolution of Silodosin for Treatment of Urological Disorders
Silodosin, is the most selective antagonist of the α1A-adrenoreceptors (ARs) family. Silodosin was approved first in Japan in 2006, and later received approval in the USA25 and Europe.26,27 Receptor-binding studies were conducted to study the effect of silodosin and other α1-AR antagonists on the increase in intraurethral pressure (IUP) induced by phenylephrine, as well as blood pressure (BP), in anesthetized rats.28 In this study, all drugs inhibited the increase in IUP and decreased BP, but silodosin, in particular, demonstrated higher uroselectivity followed by tamsulosin, naftopidil in both intravenous and intraduodenal administration. These findings suggested that silodosin, an α1A-AR selective antagonist might be useful in the LUTS without causing hypotension.28 An early randomized, placebo-controlled trial in Japan showed a greater reduction in IPSS with silodosin after 12 weeks of treatment compared to both tamsulosin and placebo. This clinical benefit in IPSS was observed from the first week of therapy. Compared with tamsulosin, silodosin selectivity was 38 times higher toward α1A-receptor blockade.29 Multiple in vivo studies and those using cloned human subtypes have underscored varying degrees of uroselectivity of silodosin for α1A-ARs compared with both α1B or α1D ARs. In humans, α1A-ARs are located in the prostate, bladder base, bladder neck, prostatic capsule and prostatic urethra and mediate smooth muscle contraction in these tissues.30 Thus, blocking α1A-ARs is the first line of action in the treatment of LUTS and other associated urological disorders.
Pharmacokinetic-Pharmacodynamic Features
Silodosin exerts its effect by blocking α1A-ARs, which prevents the binding of the neurotransmitter epinephrine, thus relaxing bladder and prostate smooth muscle, alleviating urinary flow.31 Silodosin has low affinity for α1B-ARs. An in vitro receptor binding study showed that the affinity of silodosin for human prostate tissue was ≈200-fold higher than for the mesenteric human aorta tissue and 100-fold higher for human mesenteric artery tissue.32 Preclinical studies have investigated the effect of silodosin on bladder and prostate function. Goi et al observed that after 8 weeks of treatment, silodosin was able to suppress the chronic bladder ischemia decrease in empty bladder, reduced signs of bladder overactivity in spontaneously hypertensive male rats.33 Similarly in a male rat model for BOO, silodosin-treated rats had small numbers of non-voiding contractions and a lower single unit afferent activities compared with control group rats.34 A competition-binding assay on human embryonic kidney showed that silodosin and tamsulosin had higher affinity for α1A-AR, but had Ki ratios of 25.3 and 50.2 for the α1D and α1B-AR, respectively, compared with 2.92 and 5.1 for tamsulosin.35
The absolute bioavailability of silodosin is ≈32% and follows linear pharmacokinetics over a dose range 0.1 to 24 mg/day. The drug has a volume distribution of 49.5 L and is ≈97% protein bound. It is extensively metabolized by UDP-glucoronosyltransferase-2B7 (UGT2B7), alcohol and aldehyde dehydrogenase, and cytochrome P450 3A4. It is excreted primarily in urine (≈34%) and feces (≈55%), with a half-life (t1/2) of approximately 13 hours.26,36 Administration of silodosin with food decreased maximum concentration (Cmax) by 18–43% and area under curve (AUC) by 4–49%.36 The pharmacokinetic profile of silodosin and its metabolites were similar in geriatric populations. In addition, unbound exposure to total silodosin resulted in a 1.6-fold increase of Cmax and 1.7-fold AUC relative to normal renal controls.26 These changes were greater on exposure of total (unbound + bound) silodosin with AUC, Cmax, and elimination t1/2, which were 3.2-, 3.1-, and 2-fold higher compared with patients with normal renal function.36 In case of severe renal impaired function, unbound silodosin Cmax, and AUC values were 2.2 and 3.7-fold higher than normal renal function patients.26 No dose adjustment is required for patients with mild renal impairment whereas an initial dose of 4 mg/day is advised for patients with moderate renal impairment.26,36
Silodosin has been associated with low rate of serum aminotransferase elevations (<2%); however, these effects are transient and do not require dose modification.37 The instances of acute symptomatic liver injury due to silodosin has been rarely reported in literature.38 In addition, the cause of hepatotoxicity remains to be elucidated. It is speculated that partial metabolism of silodosin by the cytochrome P450 enzymes of the liver (predominantly CYP 3A4) results in generation of a mildly toxic intermediate.37
Mechanism of Action
The α1A-ARs belongs to the family of G protein-coupled receptors. Phospholipase C is activated by the binding of norepinephrine and epinephrine, which results in the production of second messengers such as inositol triphosphate and diacylglycerol. Finally, they cause smooth muscle contraction and intracellular calcium level rises.39 Blocking α1A-ARs causes prostatic and urethral smooth muscle to relax, which may alleviate voiding symptoms. Silodosin, however, also acts on symptoms of bladder overactivity and storage by targeting afferent nerves in the bladder.40
Potential Drug Interactions
Numerous studies have been conducted to understand putative interactions of silodosin with other drugs. Co-administration of silodosin with a diltiazem, a CYP3A4 inhibitor, increases AUC of silodosin by ∼30%, without any dose adjustment and without affecting Cmax and t1/2.26 The use of silodosin is discouraged in patients taking cyclosporine, as it increases the concentration of drug. Co-administration of digoxin with silodosin is safe and no dose adjustment is required.26,36 Similarly, the administration of antihypertensive drugs with silodosin causes no clinically significant orthostatic effects and is considered safe. Higher but insignificant orthostatic hypotension was observed on concomitant administration of tadalafil with silodosin in healthy men. The co-administration of sildenafil or both tadalafil and silodosin may be an appropriate treatment for patients who experience EjD. Therefore, its concomitant treatment with PDE5 inhibitors needs to be closely monitored, particular in patients with symptomatic hypotension.41
Benign Prostate Hyperplasia/Lower Urinary Tract Symptoms
Lower urinary tract symptoms (LUTS) are very common disorders affecting both the sexes, especially in aged population and adversely affecting the QoL of affected individuals. LUTS have been historically linked to BPH and its symptoms include storage, voiding, and post-micturition.42 Several large epidemiological studies have been conducted to evaluate the prevalence and inconvenience of LUTS in population-based analysis,43,44 with over 60% of men and women affected by LUTS. The probability of developing moderate-to-severe LUTS were higher post 50 years of age with 3.5 times more frequent in men with a prostate volume ≥50 mL and 2.4 times more in those with prostate volume <50 mL.45 LUTS are associated with OAB syndrome as well as AUR. The prevalence of BPH is strongly related to age, present in about 50% of men between 51 and 60 years old, and it reaches 90% over 80 years.4 Furthermore, LUTS are linked to greater problems such as AUR, with 6.8 episodes per 1000 patients per year in the general population, and 34.7 episodes in patients aged more than 70 years.45
Silodosin Monotherapy
A pooled analysis of 2 RCTs (n = 923) revealed significant and rapid recovery in patients treated with silodosin in terms of IPSS score (−4.2 ± 5.3 vs −2.3 ± 4.4; P<0.0001) and Qmax (2.8 ± 3.4 vs 1.5 ± 3.8) compared with placebo. Within 3 to 4 days of commencing treatment, patients receiving silodosin achieved significant improvement in total IPSS score (difference −1.9, P<0.0001), as well as irritative (−0.5, P = 0.0002) and obstructive (−1.4, P<0.0001) sub scores. Significant improvement in urinary flow rate occurred at 2–6 hours. The proportion of orthostatic hypotension was similar in both groups (2.6% vs 1.5%).46 An extended follow-up study (n = 661) in the same patient population for 40 weeks reconfirmed the efficacy of the drug and also suggested that the risk of orthostatic hypotension is unlikely to increase with increasing duration of therapy.47 Yamanishi et al reported mean improvement in total IPSS, voiding IPSS sub score, storage IPSS sub score, and QoL sub score of 7.9, 3.8, 2.0, and 1.1 points, respectively, over a year on treatment with silodosin in at least 44% of patients with LUTS. Also, the BOO index and detrusor opening (DO) pressure significantly reduced within 3 months after receiving treatment. This highlights that silodosin has a significant effect on DO and obstruction grades, making them less likely to undergo invasive surgery and manage the condition safely for at least 1 year.48 These results were in agreement with another study conducted in Japan.49 Similarly, in this study the silodosin mean detrusor pressure at maximum flow was decreased from 72.5 mm to 51.4 mm and BOO index reduced significantly from 60.6 to 33.8 in patients with benign prostatic obstruction (BPO). Thus the mean improvements in total IPSS, voiding IPSS sub score, storage IPSS sub score, and QoL sub score were 6.2, 3.6, 2.6, and 1.6 points, respectively.49 However, Fusco et al reported 10.7, 4.0, 6.7, and 3.0 points of mean improvements in total IPSS, voiding IPSS sub score, storage IPSS sub score, and QoL sub scores, respectively with silodosin at 8 weeks of treatment. The authors speculated that these lower rates might be due to differences in the baseline characteristics of patients. It is hypothesized that the subjects with a moderate-to-high compromised baseline level might have a greater margin of improvement compared with subjects that are less compromised at baseline, however, further studies are needed.50 Chapple et al provided evidence that silodosin can be used for the treatment of both storage and voiding LUTS associated with BPH. Here the change from baseline in the IPSS total score with silodosin (difference, −2.3, 95% confidence interval [CI], −3.2, −1.4) and tamsulosin (difference, −2.0; 95% CI: −2.9, −1.1) was significantly superior to that with placebo (P < 0.001); number of responders with total IPSS were significantly higher (P < 0.001) with silodosin (66.8%) and tamsulosin (65.4%) than with placebo (50.8%) after 12 weeks of treatment. In addition, only silodosin significantly reduced nocturia versus placebo along with improved Qmax and QoL. The authors particularly emphasized that silodosin might be more helpful in elderly patients where there is a high risk for drug-drug interactions and greater risk of cardiovascular (CV) side effects.51 The SiRe study, a Phase IV trial in elderly population, investigated the benefit-risk balance of silodosin in the real-world setting. About 77.1% had ≥25% decrease in IPSS score, and nocturia decreased from 85.7% to 52.4% after 24 weeks of treatment. Overall, 74.2% patients were satisfied with silodosin.52 In a post hoc analysis of 2 Phase III trials, patients were treated with 8-mg silodosin once daily or placebo. Those treated with silodosin were stratified into two groups, namely, by absence or presence of retrograde ejaculation (RE). Irrespective of ejaculatory status, patients receiving silodosin experienced significant improvement in IPSS (P<0.0001), Qmax (P<0.02), and QoL (P<0.0001). RE (+) patients experienced numerically greater improvement in voiding symptoms compared with RE (−) patients, though not statistically significant (P>0.05). Further interesting observation was noticed in this study. Patients with RE (+) receiving silodosin achieved more improvement of at least 30% in IPSS points and Qmax than in placebo and RE (−) with silodosin-treated groups (27.5% vs 9.2% vs 20.9%). Similarly, total IPSS improved by ≥3 points and Qmax by ≥3 mL/sec in RE (+) and with silodosin-treated groups (34.4% vs 12.9% vs 23.0%). The odds of achieving improvement of ≥3 points in IPSS and ≥3 mL/sec in Qmax over 12 weeks were 1.75 times than those for RE (−) patients (P = 0.0127). These observations suggest that the absence of seminal emission in silodosin-treated patients may predict greater treatment efficacy. Having said that, the biological basis for differences in treatment response among individual patients remains to be elucidated.53 Table 1 describes the summary of the included studies.
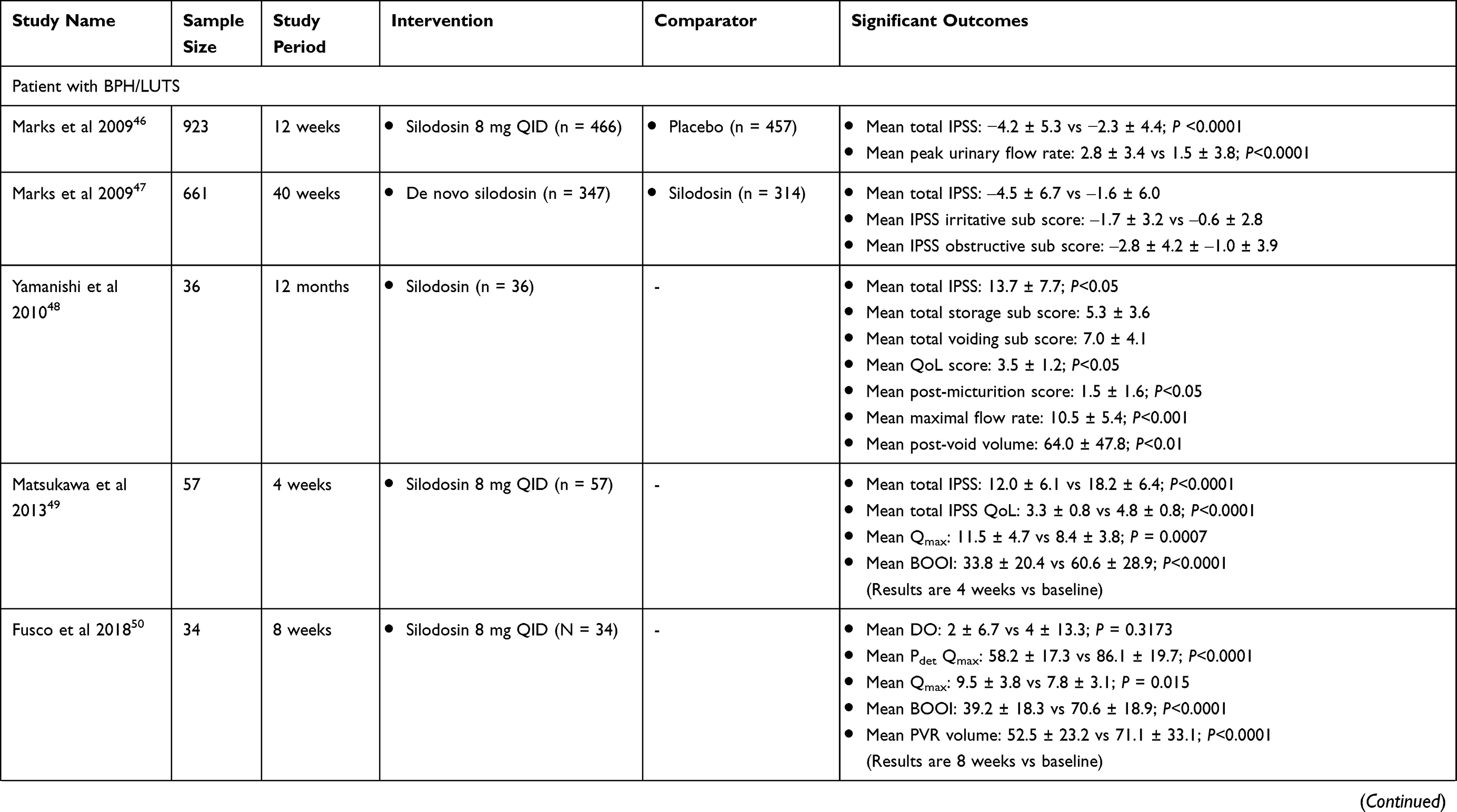 | 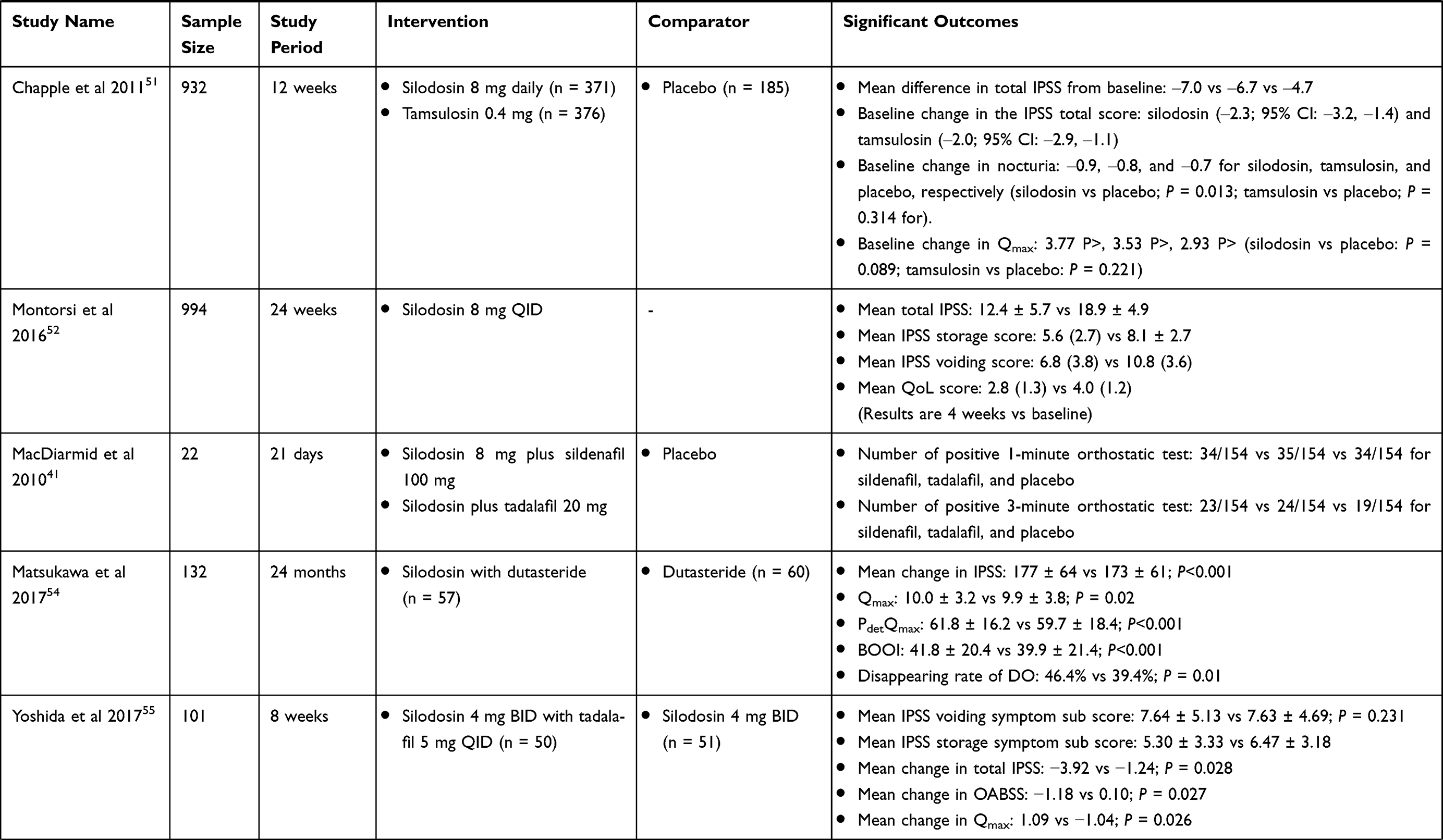 | 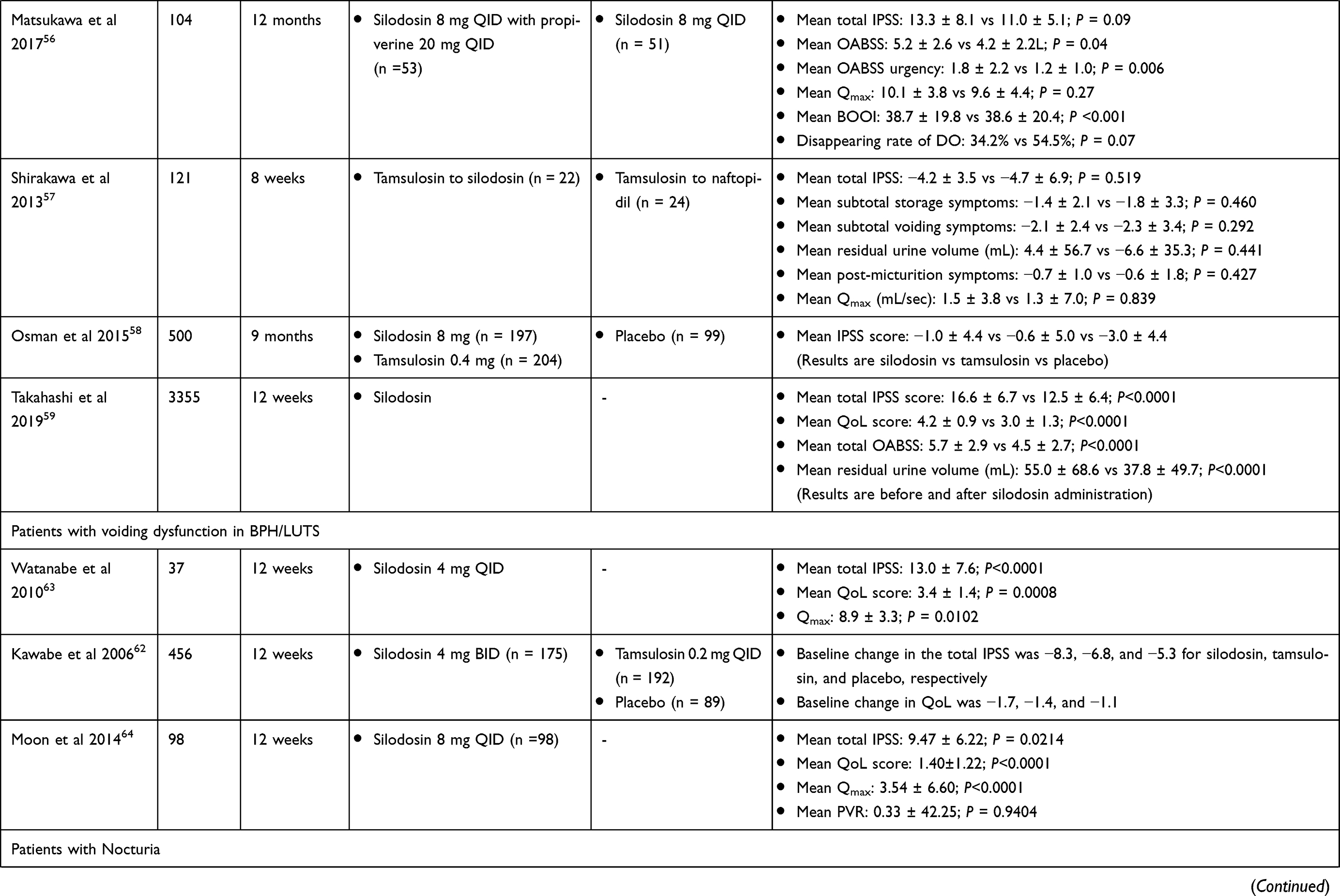 | 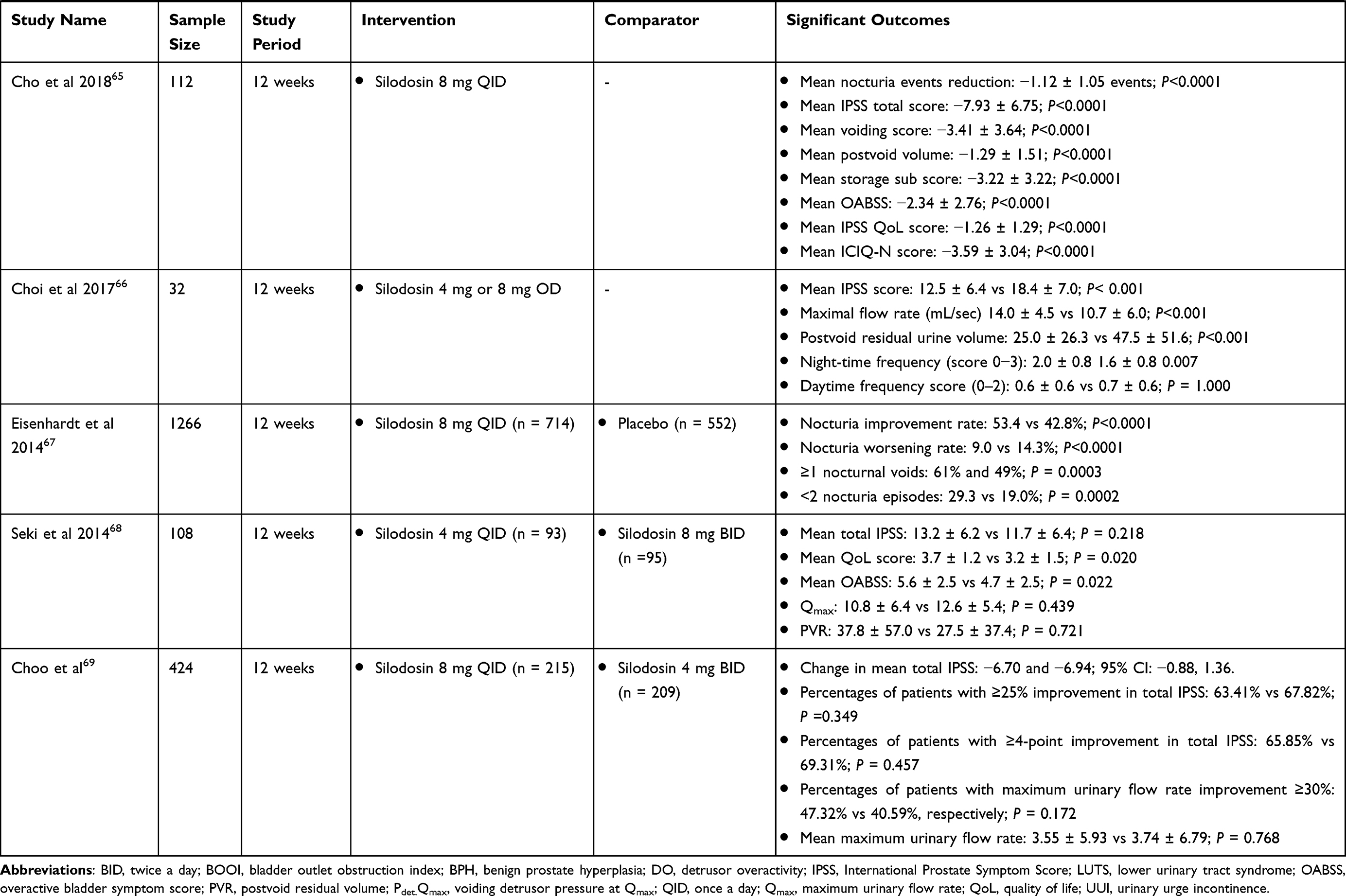 |
Table 1 Summary of Included Studies for Patients with LUTS/BPH/Voiding Symptom/Nocturia |
Silodosin Combination Therapy
The co-administration of silodosin with sildenafil or tadalafil was clinically significant in the treatment of BPH in healthy men with no history of symptomatic hypertension. The number of post-dose positive orthostatic tests was similar for all treatments (sildenafil with silodosin: 57/154; tadalafil with silodosin: 59/154; placebo: 53/154). In comparison with placebo, sildenafil or tadalafil was able to reduce the blood pressure significantly in smaller levels, however, there were no significant orthostatic changes in systolic blood pressure (SBP), diastolic blood pressure (DBP), or heart rate (HR; P > 0.05).41 A recent study showed that patients treated with silodosin and dutasteride combination demonstrated similar efficacy to those who switched from silodosin to dutasteride monotherapy after 12 months of therapy. Both the groups showed significant improvements in the subjective and objective symptoms of urodynamics. However, 38.3% patients who continued with dutasteride after silodosin withdrawal reported worsening of IPSS, as well as BOO index and storage function especially in those with higher body mass index (BMI). The mechanism behind this phenomenon remains unknown. However, it has been postulated earlier that patients with higher BMI achieved greater clinical efficacy with α1-blocker, and the withdrawal of the same resulted in more adverse effects. These indicate that caution needs to be exerted while deciding switch in medical treatment course for patients with LUTS/BPH.54 A total of 103 patients with LUTS/BPH and IPSS >8 after ≥4 weeks of silodosin treatment were further treated with silodosin 4 mg twice daily (BID) or silodosin 4 mg BID plus tadalafil 5 mg once daily (QD). After 8 weeks of treatment, the analysis revealed that the IPSS, OAB symptom score (OABSS), and Qmax scores showed a greater improvement in the silodosin plus tadalafil combination therapy than monotherapy group (−3.92 vs −1.24, −1.18 vs 0.10, and 1.09 vs −1.04, respectively; all P<0.05). Further subgroup analysis in patients with overactive bladder (n = 55) also showed significantly greater improvements in the IPSS storage symptom sub score, IPSS urgency sub score, and OABSS urgency sub score in the combination therapy than monotherapy group (−2.23 vs 0.17, −0.88 vs 0.28, and −1.5 vs −0.48, respectively; all P<0.05).55
A randomized prospective study of silodosin monotherapy (n = 53) and silodosin 8 mg/day in combination with propiverine 20 mg/day (n = 51) was conducted by Matsukawa et al. The mean IPSS and OABSS significantly improved in both groups, however, the combination group showed statistically significant improvement in OABSS (−3.4 vs −2.4, P = 0.04), IPSS-QOL (−1.9 vs −1.2, P = 0.01), and OAB-urgency score (−1.8 vs −1.2, P<0.01). Further there was a greater improvement in the disappearance rate of DO (54.5% vs 34.2%, P = 0.07) and bladder capacity (+61 mL vs +33 mL, P = 0.02) compared with the monotherapy group. A decrease in the residual urine volume from baseline by 20 mL (range −9 to +64 mL) with silodosin monotherapy was observed, whereas, an increased urine volume (range −51 to +140 mL) was observed on treatment with combination therapy after 1 year. At 1 year, the disappearance rate of DO in the combination group tended to be superior with that in the monotherapy group (54.5% vs 34.2%; P = 0.07). This observation signifies that silodosin in combination therapy is also a suitable treatment option in patients with LUTS/BPH.56
Switching Therapy
A study exhibited improved total IPSS and QoL scores in patients with LUTS/BPH when treated with silodosin compared with those treated with naftopidil at 4 or 8 weeks (P<0.05). It was observed that patients treated with silodosin took shorter time (at 4 weeks) to obtain subtotal IPSS storage and voiding symptoms scores while improvement with naftopidil was obtained at 8 weeks. Switching of patients from tamsulosin therapy to either silodosin or naftopidil showed significant improvements in total IPSS and QoL scores with both the drugs, with no significant differences. As for Qmax, residual urine volume and safety events, there was no significant change in all the treatment groups. The present study reported the clinical usefulness of silodosin in treating storage and voiding symptoms in BPH-associated LUTS. However, the study was limited due to the sample size necessitating a larger study population.57 A long-term study among European patients with LUTS demonstrated a marked reduction in IPSS in patients having de novo silodosin compared with previously treated silodosin and tamsulosin therapy; QoL also improved among these patients. In patients with arterial hypertension, the drug was well tolerated and no event of orthostatic hypotension was observed.58 A large prospective observational study in 3355 patients with BPH was conducted who switched from another α-blocker to silodosin due to therapy failure. This post-marketing surveillance study showed that mean total IPSS improved from 16.6 ± 6.7 to 12.5 ± 6.4 after silodosin treatment (P < 0.0001). OABSS, residual urine volume, and QoL score showed significant improvement after switching from other α-blockers. There was no increase in the incidence of AEs with the use of any type of concomitant drug for LUTS treatment.59 In a crossover study, 40 patients with LUTS/BPH were assigned to 2 treatment groups: (a) silodosin 4 mg 4 weeks, followed by tamsulosin 0.2 mg 4 weeks and (b) tamsulosin at 0.2 mg, 4 weeks, followed by silodosin at 4 mg 4 weeks. Though there was significant improvement in IPSS and QoL, an interesting observation was that Qmax decreased after switching to tamsulosin in group a, while in group b, Qmax continued to rise after switching to silodosin. This signifies that continued use of silodosin could significantly improve the Qmax.60
Voiding Dysfunction in BPH/LUTS
In patients with LUTS aged ≥45 years and suggestive of BPH, early and timely diagnosis of BPH with silodosin showed signs of improvement in voiding symptoms and QoL scores from day 1 of administration. Moreover, silodosin also improved the storage and post-micturition symptoms.61 These observations were similar to those reported by Kawabe et al who observed improvement after 1 month of therapy.62 Watanabe et al63 also reported similar findings. The study reported that daytime frequency in those who voided over 8 times/day declined significantly (P = 0.0391) after 1 month, and nocturnal frequency in those who voided over 2 times tended to decrease (P = 0.0833) after 3 months, using a frequency/volume chart (FVC). After 1 and 3 months, mean voided volume in those who at the beginning voided <250 mL increased significantly (P = 0.0446 and P = 0.0138, respectively), while maximum voided volume in those who initially voided <300 mL tended to rise (P = 0.0833) after 1 month. AEs were mostly mild in nature (5%), where the dose reduction to 2 mg in a patient due to dizziness also showed symptom improvement as evidenced by his low IPSS and Qmax at 1 and 3 months of treatment. These rates of AEs were quite low when compared with a Phase III study by Kawabe et al.62 The reason for this difference in AEs may be that in this study the patient was satisfied with the therapy despite AE.63 Continuous administration of silodosin monotherapy in patients with severe LUTS/BPH (IPSS ≥20) in Korea showed statistically significant improvements in total IPSS and QoL scores after 12 weeks of therapy. There was no difference in postvoid residual volume (PVR) and the presence of CV AEs was low (3%). None of them discontinued treatment due to improved health. Thus, silodosin proved to be effective and safe.64
Nocturia in BPH/LUTS
Among patients with BPH, approximately 85% experience two or more episodes per night. Several studies have shown the efficacy of silodosin in reducing nocturia. Silodosin reduced the incidence of nocturia in patients with BPH after 12 weeks of treatment (−1.12 ± 1.05, P<0.0001). There were also improvements in the IPSS total score, voiding, postvoid and storage sub scores as well as the OABSS (P<0.0001). Both the IPSS QoL score (−1.26 ± 1.29, P<0.0001) and the International Consultation on Incontinence Questionnaire-Nocturia (ICIQ-N) score measures (−3.59 ± 3.04, P<0.0001) improved significantly. The subjects with ≥25% decrease in rate of nocturia and the IPSS were 65.18% (n = 73) and 63.39% (n = 71), respectively.65 Intake of silodosin among elderly patients with LUTS/BPH and hypertension also resulted in beneficial effects. Patients on antihypertensive medications showed decrease in total IPSS, voiding score sum, storage score sum, and QoL score after receiving silodosin. Though the frequency of nocturia and urgency scores on the OABSS questionnaire improved, the daytime frequency or urge incontinence scores did not improve. There was also an objective rise in the Qmax and a decrease in PVR. After treatment, only 2.5% of patients had orthostatic hypotension. A notable finding in this study was that adding silodosin to treatment in individuals who already had orthostatic hypotension did not worsen the condition, but rather showed improvement in 2 patients.66
A pooled analysis of 3 Phase III studies (n = 1479), reported that 8-mg silodosin improved the frequency of nocturia (53.4% vs 42.8%; P<0.0001) and prevented worsening events (9.0% vs 14.3%; P<0.0001) compared with placebo. Silodosin 8 mg QD reduced nocturia from ≥1 episode to <2 episodes/night at the end of the study.67 In a study involving 268 Japanese men with BPH, comparing QD vs BID of 4 mg of silodosin, Seki et al68 reported a significant reduction in IPSS voiding and storage subtotal scores, total IPSS, QoL index, PVR, and increase in Qmax in both groups. However, only QoL gained more significance from 8 mg/day dosage of silodosin. Although the rates of AEs were lower in the 4 mg QD group, it did not reach statistical significance. The SILVER study compared whether silodosin 8 mg QD is as effective as 4 mg BID in patients with BPH. The results showed that 8 mg QD administration of silodosin was not inferior to 4 mg BID in terms of efficacy and safety.69 Another study by Gul et al70 outlined that both 4-mg silodosin was as effective as 8-mg silodosin QD in patients with moderate LUTS but not with severe LUTS. A meta-analysis evaluating the efficacy and safety of silodosin in patients with non-neurogenic male LUTS/benign prostate enlargement (BPE), found that 8-mg silodosin was significantly more effective than placebo and tamsulosin 0.2 mg in improving void symptoms and was noninferior to tamsulosin 0.4 mg.71 Novara et al conducted a systematic literature review to evaluate the effect of silodosin in various patient subgroups with LUTS/BPH. They found that silodosin was more effective than placebo in improving total IPSS, all IPSS-related parameters, and Qmax (all P<0.0414) in both patients aged <65 years and ≥65 years old. Silodosin proved to be more effective than placebo in reducing all IPSS-related parameters regardless of baseline IPSS and Qmax (P≤0.0011 and P≤0.0197).72
Newer Indications for Silodosin Treatment
Overactive Bladder and Acute Urinary Retention in LUTS/BPH Patients
Sometimes, LUTS/BPH syndrome is accompanied by OAB. Despite management of such patients with α1-blockers, storage problems still persist. In such cases, guidelines recommend the addition of an anticholinergic agent or a β3-AR agonist.9,73,74 Add-on treatment with fesoterodine in patients with persistent OAB symptoms and taking silodosin monotherapy for 12 weeks showed greater significant improvements in storage functions, detrusor overactivity alleviation rate and PVR urine flow compared with mirabegron group.75 Silodosin exhibited greater improvement in total OABSS (P = 0.03), OABSS urgency score (P < 0.001), and IPSS-QOL score (P = 0.005) at 12 weeks compared with the naftopidil group. In voiding function, the Qmax in the silodosin group (+3.6 mL/sec) at 12 weeks was significantly greater as compared with that in the naftopidil group (+2.1 mL/sec). Therefore, silodosin is the first choice of treatment for patients with BPE/OAB.76 In patients with AUR in BPH, success rate of trial without catheter (TWOC) was 76.7% in the silodosin group compared with 36.7% in placebo group. Multivariate analysis revealed lesser odds of having failure with silodosin than placebo group (P = 0.008). No AEs were observed with this treatment, facilitating the double effect of silodosin in management of AUR.77 Similarly, in patients with a first episode of AUR (n = 80), the success rate of TWOC was 88.8% with 8 mg silodosin and 0.5 mg dutasteride therapy. Void volume and Qmax were significantly higher, while IPSS and IPSS-QOL were significantly lower at 2, 4, 8, and 12 weeks. However, a control group was lacking in this study to determine the superiority of this treatment.78 The SNIPER study evaluated the efficacy of silodosin and naftopidil in LUTS patients complicated with OAB (n = 350). There was a greater and significant improvement in the silodosin group than in the naftopidil group in total OABSS (P = 0.03), IPSS-QoL score (P = 0.005), and OABSS urgency score (P < 0.001) at 12 weeks. The Qmax significantly improved in both groups, but the change was greater in the silodosin group (+3.6 mL/sec) at 12 weeks compared with the naftopidil group (+2.1 mL/sec). These findings suggest silodosin is clinically meaningful in improving storage symptoms. The difference in the selectivity for α1-AR subtypes play a significant role in achieving storage and OAB symptoms. The suppression of α1A AR subtype is more important in voiding and storage function compared with α1D-AR subtype.76 A summary of included studies is summarized in Table 2.
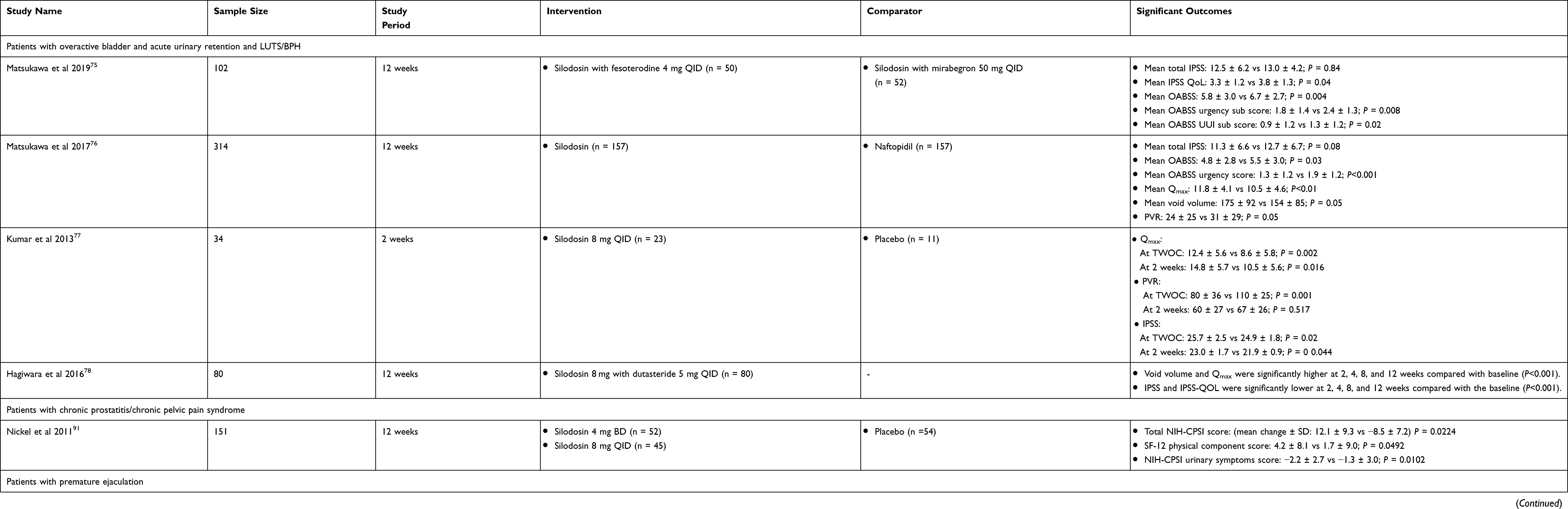 |
Table 2 Summary of Included Studies for Overactive Bladder and Acute Urinary Retention in Patients with LUTS/BPH, Chronic Prostatitis/Chronic Pelvic Pain Syndrome (CP-CPPS), and Premature Ejaculation |
Chronic Prostatitis/Chronic Pelvic Pain Syndrome
About 35–50% of men have symptoms suggesting prostatitis during their life time,79 reflecting an approximate prevalence of 8.2% (range: 2.2% to 9.7%).80 The different types of symptomatic and chronic forms of prostatitis are chronic bacterial prostatitis (category II), chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS; category III) and asymptomatic inflammatory prostatitis (AIP; category IV).81 CP/CPPS is known to worsen the QoL and has presented diagnostic and therapeutic challenges for physicians. Despite these limitations, this syndrome has been less investigated as compared with other urological conditions.82 This can be attributed to the unknown etiology of CP/CPPS. Though limited, treatment with α1-blockers have shown significant efficacy in reducing CP/CPPS-specific symptoms in several randomized, double-blind, placebo-controlled trials.83–88 α1-blockers have the ability to block mediated signaling in the peripheral or central nervous system (CNS) thus ameliorating CP/CPPS-associated LUTS and pain by reducing voiding pressures and void flow patterns.85,89 The EAU guidelines recommend the use of α-blockers for patients with a duration of prostate pain syndrome (PPS) <1 year.90 A Phase II study was conducted to evaluate the response rate on treatment with silodosin 4 mg (n = 52) or 8 mg (n = 45) in patients with CP/CPPS based on total change in National Institutes of Health Chronic Prostatitis Symptom Index (NIH-CPSI) score from baseline to 12 weeks. There was significant decrease in NIH-CPSI score compared with placebo (mean ± SD change, −12.1 ± 9.3 vs − 8.5 ± 7.2, P = 0.0224), with improved urinary scores (−2.2 ± 2.7 vs −1.3 ± 3.0, P = 0.0102) and QoL (−4.1 ± 3.1 vs −2.7 ± 2.5, P = 0.0099), and SF-12 physical component scores (4.2 ± 8.1 vs 1.7 ± 9.0, P = 0.0492). Nearly twice as many patients achieved marked improvement in global response assessment (GRA) (56% vs 29%) with the 4-mg silodosin (P = 0.0069). The increase in dose from 4 mg to 8 mg showed no additional treatment effects.91 RE was common in patients with 4-mg silodosin compared with those treated with placebo (26.9% vs 1.9%). The proportion of drug-related AEs was greater in the 8-mg silodosin group than in the 4-mg silodosin group. The remaining AEs were similar to that in the placebo group.91 These results indicate that treatment with silodosin is more beneficial in comparison to other α1-blockers as observed in other clinical studies.92,93 A summary of included studies is summarized in Table 2.
Premature Ejaculation
Premature ejaculation (PE) is the most common sexual disorder in men and affects 30% of men, though it is not fatal. It is assumed that contractile dysfunction of seminal vesicle and spermatic duct is the major cause of onset of ejaculation by α1-blockers.94,95 A comparison of 5 α1-blockers in patients with PE demonstrated that the success rate of treatment was 85.7% with silodosin, 69.6% with tamsulosin, 45.5% with alfuzosin, 52.4% with terazosin, and 66.7% with doxazosin. Additionally, there were statistical improvements in intravaginal ejaculation latency time (IELT), QoL scores and decrease in premature ejaculation profile (PEP) in patients treated with silodosin compared with other groups.96 A preliminary study among 8 patients with PE in Japan showed that off-label silodosin significantly prolonged IELT from 3.4 to 10.1 minutes (P = 0.003). Based on these findings, the authors carried out further investigations in 26 patients with PE. Here also, 4-mg silodosin produced greater improvements in these patients by prolonging IELT and PEP scores compared with naftopidil (P < 0.001). Though 2 (25%), 3 (37.5%), and 7 (87.5%) patients experienced an ejaculation, reduced semen volume and discomfort during orgasm, these problems were reported to be insignificant to the study participants.97 Due to clinical global impression change (CGIC), 24 patients (92.3%) and 12 patients (46.1%) reported that their own PE problems improved with silodosin and naftopidil administration, respectively. However, the authors noticed that 50% of patients had reduced semen volume with silodosin. This issue was resolved on limiting the dose to half its actual volume. Furthermore, 42% of patients with EjD were managed by PDE5 inhibitors before enrollment to the study. This shows that demographics of patients treated for PE are varied and frequently suffered from PE combined with EjD.98 Dapoxetine 30 mg is widely used for the treatment of PE; however, the patient adherence is low due to its adverse effects or inefficacy.99 In such conditions, about 123 patients dissatisfied with dapoxetine treatment were administered with 4-mg silodosin and were evaluated for its effects on PE. On treatment with silodosin, patients showed improvement in the IELT, PEP score, and CGIC for PE whereas only 4 patients reported uncomfortably delayed ejaculation.99 A summary of included studies is summarized in Table 2.
Ureteral Calculi
Ureteroscopy and shockwave lithotripsy (SWL) remain the most effective treatment modalities for DUS,100–102 however, these treatments are expensive and accompanied by adverse events. Medical expulsion therapy (MET) with α1-blockers is recommended for the treatment of ureteral stones >5 mm as per the latest EAU guidelines.102 With time it has been observed that the site of stone formation has migrated from the lower to the upper urinary tract.103 A previous study reported that SER of ureteric stones after WW was 25% to 54% with a mean expulsion time >10 days, associated with high analgesic requirement for stones >5 mm. Thus to improve the expulsion rate and requirement for analgesics, MET is the preferred treatment for ureteral stones.104,105 Itoh was the first researcher to perform a prospective randomized study with silodosin in patients with proximal, mid, or DUS. They found that silodosin did not affect SER (66.3% vs 50%), expulsion duration (10.27 ± 8.35 days vs 15.19 ± 7.14 days; P = 0.0058), or analgesic need when compared with those not receiving any treatment. However, silodosin decreased stone expulsion time (SET) without affecting SER or analgesic need in patients with DUS. A subgroup analysis of patients with ureteral stones 6 mm to 9 mm in diameter reported that silodosin increased SER and decreased stone expulsion duration but did not affect analgesic need. However, the findings should be interpreted with caution because the study included only men.106 Another study demonstrated that a higher proportion of patients achieved stone expulsion with silodosin (82% vs 58%; P = 0.008) and a shorter duration of expulsion (12.5 ± 3.5 vs 19.5 ± 7.5 days, P = 0.01) than tamsulosin.103 These findings are consistent with the silodosin’s greater selectivity for the α1A-receptor compared with tamsulosin. Kumar et al107 demonstrated that patients treated with silodosin had significantly higher SER compared with tamsulosin (83.3% vs 64.4%; P = 0.006) and tadalafil (83.3% vs 66.67%; P = 0.016) treated groups. The mean SET was significantly less in silodosin-treated groups (14.8 ± 3.3 days vs 16.5 ± 4.6 days, P = 0.005; 14.8 ± 3.3 days vs 16.2 ± 4.2 days, P = 0.013). Compared with tamsulosin (1.70 ±1.2) and tadalafil (1.60 ± 0.8), there was a decrease in the average episodes of colicky pain with silodosin (0.8 ± 0.9; P<0.001). The analgesic requirements were also significantly less with silodosin than other drugs. Thus, the authors concluded that the use of silodosin increases ureteric stone significantly along with better control of pain and lesser analgesic requirement. Probably, α1-blockers decrease analgesic requirement by two ways ie, expulsion of stones and blockade of C fibers; however, it is difficult to know the primary responsible factor.107 However, Imperatore et al108 observed that there was no significant difference in the stone clearance rates and expulsion time between silodosin and tamsulosin groups. Here the incidence of side effects related to peripheral vasodilation (dizziness, postural hypotension, headache, nasal congestion) were significantly higher in the tamsulosin arm.108 A multicenter study on silodosin was found to be beneficial and well tolerated in facilitating passage of DUS 4 mm to 10 mm compared with placebo. Commonly observed AEs were RE, nausea, dizziness, headache, and nasal congestion.109 A prospective randomized study in 115 patients with DUS ≤10 mm was randomized to either 8-mg silodosin or 0.4-mg tamsulosin QD. After 1 month of treatment, the SER was significantly different between the groups, at 83% with silodosin and 57% with tamsulosin (P = 0.007). The SET was also significantly shorter in silodosin-treated patients than with tamsulosin (mean ± SD: 13.3 ± 4.1 vs 16.7 ± 5.4 days; P < 0.001). Silodosin-treated patients exhibited fewer ureteric colic episodes and lower incidences of orthostatic hypotension (3.8% vs 7.8%). Abnormal ejaculation was recorded more in silodosin-treated patients than tamsulosin; however, this result was non-significant (P = 0.18).110 Similar findings were obtained where silodosin reported higher efficacy and safety against tamsulosin in reducing SET (82.4% vs 61.5%; P = 0.007) in patients having a single unilateral stone ≤10 mm.111 A summary of included studies is summarized in Table 3.
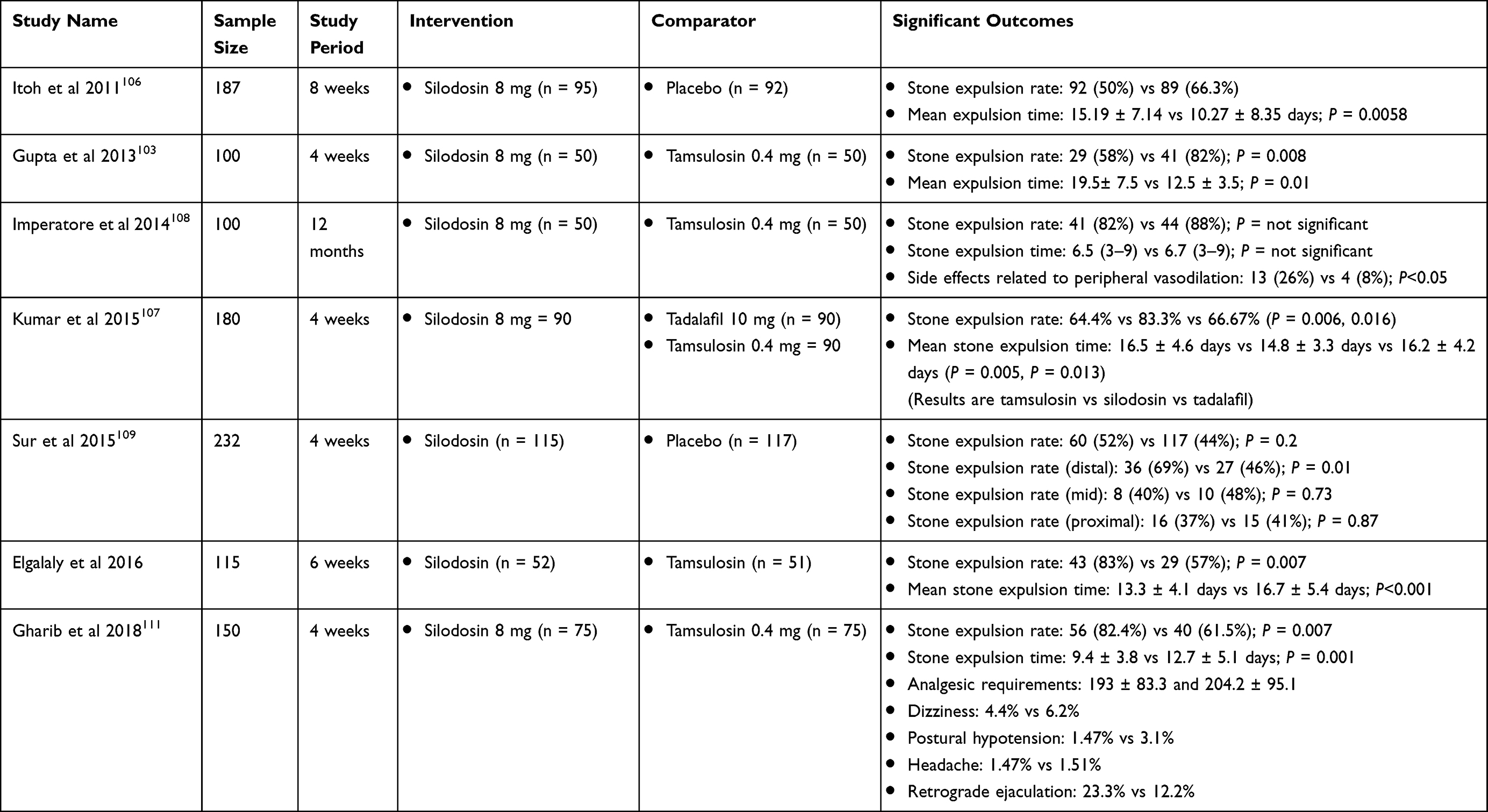 |
Table 3 Summary of Included Studies for Ureteral Stones |
Prostate Cancer Post Brachytherapy-Induced Progression
Prostate cancer is one the main causes of death in men with a 5.6% death rate annually. Urinary frequency and urgency are the frequently observed adverse events.112,113 A comparison of 2 α1-ARs in patients who underwent low-dose-rate (LDR) brachytherapy for prostate cancer showed no significant difference between the naftopidil and silodosin groups (P = 0.728). For the first 12 months after seed implantation, the FVC indicated a similar increase in urine frequency and a decrease in total urinated volume and mean voided volume. Patients with a urethral dose (UD30) <200 Gy had a better IPSS recovery rate at 12 months after seed implantation.114 In contrast, Tsumura et al found greater efficacy for silodosin compared with tamsulosin and naftopidil in improving total IPSS at 1 month after prostate implantation (+7.5, +10.3, and +8.9, respectively). A significant decrease was observed with silodosin than naftopidil in the straining on urination score at 6 months (0.4 vs 1.1, P = 0.02). Thus silodosin better resolves the urinary symptoms of voiding, emptying, and nocturia after prostate implantation than naftopidil and tamsulosin.115 Oyama et al also made a similar observation in patients with LUTS who received α1-blockers after 1 year of brachytherapy. The patients administered with tamsulosin and naftopidil reported a worsening of health condition than those receiving silodosin. These findings suggest that silodosin may have an added advantage in management of LUTS after125 I prostate brachytherapy compared with other α1-blockers.116 A pressure flow study to check the urodynamics of silodosin treatment revealed a significantly enlarged bladder capacity when first non-voiding contraction was seen at 3 and 12 months (3M: 127.1 ± 74.8 vs 118.2 ± 83.9 mL, P = 0.001; 12M: 123.7 ± 79.3 vs 100.3 ± 73.4 mL, P = 0.01).117 A summary of included studies is summarized in Table 4.
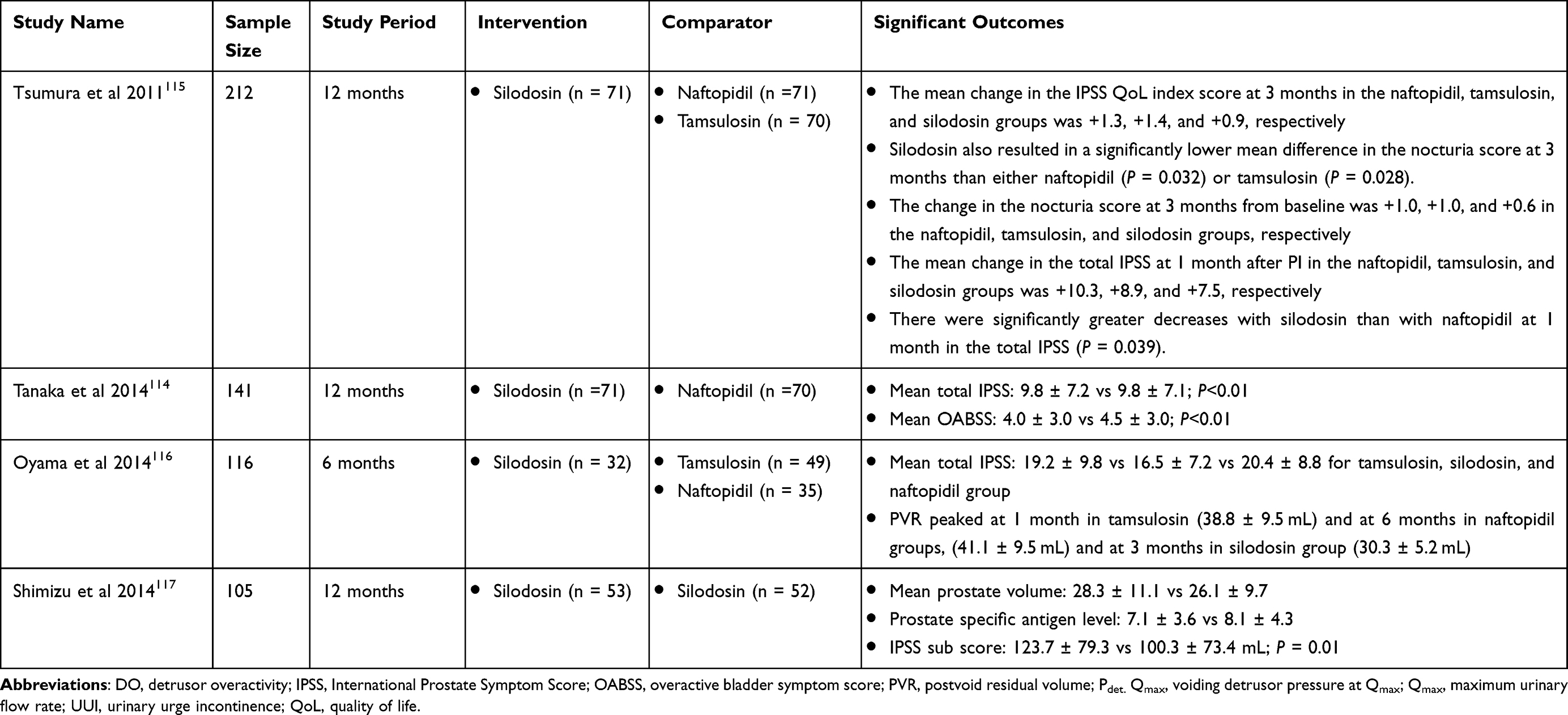 |
Table 4 Summary of Included Studies for Prostate Cancer Post Brachytherapy-Induced Progression |
Limitations, Future Implications for Research and Clinical Practice
We reviewed the various α-blockers in the available literature and found that silodosin, due to its high uroselectivity, has advantages over other α-blockers in improving the voiding symptoms, urinary flow, and improved QoL in patients dissatisfied with other therapeutic options as well as those newly diagnosed with any urologic disease. Though certain adverse events such as orthostatic hypotension, dizziness, diarrhea are observed occasionally, patients prefer to continue their treatment due to its superior and well-improved efficacy.
Fusco et al in a meta-analysis of 23 RCTs for various medical therapy reported that BOO index, PdetQmax, and Qmax were significantly improved in patients receiving α-blockers and 5-alpha reductase inhibitors while PDE5 inhibitors and phytotherapy compounds had no significant effects on urodynamic parameters in LUTS related to BPH.118 Another meta-analysis of 22 RCTs comprising >9000 patients with LUTS/BPH established that silodosin and tadalafil were more effective than placebo in improving LUTS but these drugs had more AEs. The authors stated that the evidence gathered was insufficient to assess long-term efficacy, need for surgical intervention, prevention of symptom progression, or long-term AEs. To assess the effect of these therapies on response rates using established minimal detectable difference thresholds, disease progression, and harms, long-term studies were suggested to gather enough evidence.119 Creta et al performed a post hoc analysis of Phase III and IV trials containing 8-mg silodosin as the main therapeutic regimen in patients with severe LUTS/BPO. Here, when compared with placebo, patients receiving silodosin experienced significantly higher mean improvements in total IPSS (8.1 vs 4.7), storage (3.1 vs 2.0), voiding (5.0 vs 2.7), and QoL (1.3 vs 0.7) (all P<0.0001), including for patients with severe LUTS.120 A systematic review and subsequent meta-analysis has proven that α1-AR blockers are superior to placebo in achieving successful voiding in patients with AUR. They reported that a suprapubic catheter (SPC) might provide superior advantages over urethral catheterization. Catheterization for <3 days is a safe option in avoiding catheterization-related complications.121
In terms of ureteral calculi, a study showed that silodosin achieved significantly higher expulsion rates (pooled risk difference [RD]: 0.13, 95% CI: 0.09, 0.18) and SET (pooled mean difference [MD]: −2.55 days, 95% CI: −4.06, −1.04) than tamsulosin. A subgroup analyses demonstrated a significantly higher expulsion rate on stone sizes of 5–10 mm with silodosin compared with tamsulosin (pooled RD: 0.14, 95% CI: 0.06, 0.22). With stone sizes <5 mm, the superior effect was not observed. After adjusting for age and gender, multivariate regression analysis revealed that the RD was negatively linked with the control expulsion rate (coefficient −0.658, P = 0.01). Also, these patients had fewer incidences of pain episodes (pooled MD: −0.3, 95% CI: −0.51, −0.09) compared with those receiving tamsulosin.122 Ozsoy et al123 compared the efficacy of silodosin with tamsulosin in a pooled data of 409 patients. The meta-analysis results favored silodosin in terms of SER with an RR of 1.33 (95% CI: 1.17, 1.50). Similarly, faster SET were observed with silodosin when compared with tamsulosin (−2.49; 95% CI: −3.40, 1.58). Recently, Sharma et al reviewed the three most commonly used α-blockers (tamsulosin, alfuzosin, and silodosin) as MET for ureteral calculi. They observed that all the treatment groups were more effective for both SER and SET compared with placebo. However, silodosin had the highest surface under the cumulative ranking area curves (94.8 and 90.4) values followed by alfuzosin (58.8 and 64.9) and tamsulosin (46.2 and 44.5) in terms of SER and SET. The incidence of postural hypotension was similar with all the drugs, whereas silodosin emerged as the most efficacious drug as MET for lower ureter stones.124 The same researchers reported that a tadalafil plus silodosin combination and silodosin as an individual drug are the best for treating lower ureter stones considering the SET and SER.125 A meta-analysis carried out by Liu et al reported similar findings stating that tadalafil plus silodosin has the highest probability of reducing SET, and treating ureteral stones ≤10 mm.126
Considering that α-blockers show improved efficacy in various urological disorders, these findings could serve as an evidence-based practice and can be considered by physicians and researchers to develop clinical-based guidelines. The overall efficacy and tolerability of treatment has been confirmed by the various Phase II and III trials as discussed above. In addition, the evidence from the recent meta-analysis also confirms these findings. Though the short-term effects of silodosin reported in the above literature is promising, the long-term benefit of silodosin in a larger sample size and scientifically sound study needs to be observed. The small amount of published meta-analysis available at present has limitations of small sample sizes, poor quality of included trials, and no proper conduct of study. Given these limitations, further research needs to assess the findings of this review to obtain a more efficient performance of high-quality, long-term RCTs to verify and explore the efficacy and safety of silodosin.
Nonselective drugs, such as doxazosin and terazosin, are associated with a higher incidence of cardiovascular AEs. In contrast, silodosin has shown to be effective and safe for management of LUTS in elderly patients taking antihypertensive medications.66 It is speculated that due to the high uroselectivity for α1β adrenergic receptors is mainly responsible for controlling BP enabling silodosin to have minimum effects on CV system. Silodosin has demonstrated promising results in increasing the probability of successful TWOC in patients with AUR and those taking antihypertensive drugs. The use of silodosin should be explored in the treatment of brachytherapy-induced progression of urinary function in patients with prostate cancer. Another advantage of silodosin is that the dose does not need to be adjusted according to age, concurrent medication with antihypertensives, and PDE5 inhibitors.127 Future consideration of research areas might also include further studies that analyze silodosin as a MET for distal ureteral stones >5 mm, and the combination of silodosin and oral chemolysis for distal ureteral stones >8 mm. More often, the influence of factors such as age, gender, ethnicity, previous history is overlooked or not reported in the RCTs, thus these factors need to be considered in the research to understand the subgroup population who will benefit the most from silodosin. Considering the robust data available from this review, further treatment strategies where silodosin may play a role in the management of different urological conditions needs to be focused. Finally, it was reported that LUTS/BPH patients had decreased storage function and deteriorated LUTS after withdrawal of silodosin from 12-month combination therapy with 5α-reductase inhibitors, dutasteride.54 The combination of silodosin and β-3 agonists/PDE5 inhibitors for BPE patients with OAB showed safety and significantly greater improvement on IPSS and OABSS over silodosin monotherapy.55,56 This approach warrants further investigation in combination of silodosin with β-3 agonists, or with 5α-reductase inhibitors and beta-3-agonists on improving symptoms of patients with LUTS/BPH so as to reduce the risk of progression of the disease as well as to avoid the need for invasive therapy in long-term.
Conclusion
In light of the advancement of treatment approaches for urological disease, therapies that offer high satisfaction rates for patients and compliance need to be focused on. From our review, it is evident that silodosin, a selective α1A-blocker, is versatile in the treatment of various urological diseases. Silodosin demonstrated high efficacy and well generalized tolerability in treatment of LUTS/BPH. Despite mild AEs, silodosin demonstrates significant clinical improvement with a good CV profile. Silodosin is also beneficial in improving nocturia events. Silodosin has proven to be beneficial in decreasing SET without affecting SER or analgesic need in patients with DUS. Patients on other treatment therapies such as PDE5 inhibitors or another α-blocker are well managed with this drug. Phase II results have reported significant evidence of silodosin in the treatment of CP/CPPS and facilitating ureteral stone passage, as well.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Zhejiang Provincial Natural Science Foundation of China (Grant/Award Number LY21H160038), the Scientific Research Fund of the Health Commission of Zhejiang Province (Grant No 2022499171).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Crane A, Isharwal S, Zhu H. Current therapeutic strategies in clinical urology. Mol Pharmaceut. 2018;15(8):3010–3019. doi:10.1021/acs.molpharmaceut.8b00383
2. Pintarelli VL, Perchon LFG, Lorenzetti F, Toniolo Neto J, Dambros M. Elderly men’s quality of life and lower urinary tract symptoms: an intricate relationship. Int Braz J Urol. 2011;37:758–765. doi:10.1590/S1677-55382011000600012
3. Fosså SD, Woehre H, Kurth KH, et al. Influence of urological morbidity on quality of life in patients with prostate cancer. Eur Urol. 1997;31(Suppl 3):3–8. doi:10.1159/000474553
4. NIDDK. National Institute of Diabetes and Digestive and Kidney Diseases. Urologic diseases. Available from: https://www.niddk.nih.gov/health-information/urologic-diseases.
5. Prostate gland and urinary problems - better health channel. Available from: https://www.betterhealth.vic.gov.au/health/conditionsandtreatments/prostate-gland-and-urinary-problems.
6. Foxman B. The epidemiology of urinary tract infection. Nat Rev Urol. 2010;7(12):653–660. doi:10.1038/nrurol.2010.190
7. Michel MC, Vrydag W. Alpha1-, alpha2- and beta-adrenoceptors in the urinary bladder, urethra and prostate. Br J Pharmacol. 2006;147(Suppl 2):S88–119. doi:10.1038/sj.bjp.0706619
8. Romics I. The role of alpha-adrenoreceptors in the treatment of urological diseases. Neurochem Int. 2007;51(5):328–331. doi:10.1016/j.neuint.2007.05.023
9. Gratzke C, Bachmann A, Descazeaud A, et al. EAU guidelines on the assessment of non-neurogenic male lower urinary tract symptoms including benign prostatic obstruction. Eur Urol. 2015;67(6):1099–1109. doi:10.1016/j.eururo.2014.12.038
10. Cambridge D, Davey MJ, Massingham R. Prazosin, a selective antagonist of post-synaptic alpha-adrenoceptors [proceedings]. Br J Pharmacol. 1977;59(3):514P–515P.
11. Martorana G. The effect of prazosin in benign prostatic hypertrophy, a placebo controlled double-blind study. IRCS Med Sci. 1984;12:11–12.
12. Kirby RS, Coppinger SW, Corcoran MO. Prazosin in the treatment of prostatic obstruction. A placebo-controlled study. Br J Urol. 1987;60(2). doi:10.1111/j.1464-410x.1987.tb04950.x
13. Titmarsh S, Monk JP. Terazosin. A review of its pharmacodynamic and pharmacokinetic properties, and therapeutic efficacy in essential hypertension. Drugs. 1987;33(5):461–477. doi:10.2165/00003495-198733050-00003
14. Lepor H, Auerbach S, Puras-Baez A, et al. A randomized, placebo-controlled multicenter study of the efficacy and safety of terazosin in the treatment of benign prostatic hyperplasia. J Urol. 1992;148(5):1467–1474. doi:10.1016/S0022-5347(17)36941-0
15. Lloyd SN, Buckley JF, Chilton CP, Ibrahim I, Kaisary AV, Kirk D. Terazosin in the treatment of benign prostatic hyperplasia: a multicentre, placebo-controlled trial. Br J Urol. 1992;70(Suppl 1):17–21. doi:10.1111/j.1464-410x.1992.tb15862.x
16. Brawer MK, Adams G, Epstein H. Terazosin in the treatment of benign prostatic hyperplasia. Terazosin Benign Prostatic Hyperplasia Study Group. Arch Fam Med. 1993;2(9):929–935. doi:10.1001/archfami.2.9.929
17. Gillenwater JY, Conn RL, Chrysant SG, et al. Doxazosin for the treatment of benign prostatic hyperplasia in patients with mild to moderate essential hypertension: a double-blind, placebo-controlled, dose-response multicenter study. J Urol. 1995;154(1):110–115. doi:10.1016/S0022-5347(01)67243-4
18. Fawzy A, Braun K, Lewis GP, Gaffney M, Ice K. Doxazosin in the treatment of benign prostatic hyperplasia in normotensive patients: a multicenter study. J Urol. 1995;154(1):105–109. doi:10.1016/S0022-5347(01)67240-9
19. Narayan P, Tewari A. A second phase III multicenter placebo controlled study of 2 dosages of modified release tamsulosin in patients with symptoms of benign prostatic hyperplasia. United States 93-01 Study Group. J Urol. 1998;160(5):1701–1706. doi:10.1016/S0022-5347(01)62386-3
20. Lepor H. Phase III multicenter placebo-controlled study of tamsulosin in benign prostatic hyperplasia. Tamsulosin Investigator Group. Urology. 1998;51(6):892–900. doi:10.1016/s0090-4295(98)00126-5
21. van Kerrebroeck P, Jardin A, Laval KU, van Cangh P. Efficacy and safety of a new prolonged release formulation of alfuzosin 10 mg once daily versus alfuzosin 2.5 mg thrice daily and placebo in patients with symptomatic benign prostatic hyperplasia. ALFORTI Study Group. Eur Urol. 2000;37(3):306–313. doi:10.1159/000052361
22. Roehrborn CG. Efficacy and safety of once-daily alfuzosin in the treatment of lower urinary tract symptoms and clinical benign prostatic hyperplasia: a randomized, placebo-controlled trial. Urology. 2001;58(6):953–959. doi:10.1016/S0090-4295(01)01448-0
23. Nordling J. Efficacy and safety of two doses (10 and 15 mg) of alfuzosin or tamsulosin (0.4 mg) once daily for treating symptomatic benign prostatic hyperplasia. BJU Int. 2005;95(7):1006–1012. doi:10.1111/j.1464-410X.2005.05456.x
24. Shibata K, Foglar R, Horie K, et al. KMD-3213, a novel, potent, alpha 1a-adrenoceptor-selective antagonist: characterization using recombinant human alpha 1-adrenoceptors and native tissues. Mol Pharmacol. 1995;48(2):250–258.
25. Drug approval package: RAPAFLO (Silodosin) NDA #022206. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2008/022206s000TOC.cfm.
26. Urorec. European medicines agency; 2018. Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/urorec.
27. Yamazaki Y. Development of Silodosin. Yakugaku Zasshi. 2006;126(Special):207–208. doi:10.1248/yakushi.KJ00004483554
28. Tatemichi S, Kobayashi K, Maruyama I, Kobayashi M, Yamazaki Y, Shibata N. Effects of silodosin (KMD-3213) on phenylephrine-induced increase in intraurethral pressure and blood pressure in rats—study of the selectivity for lower urinary tract. Yakugaku Zasshi. 2006;126(Special_Issue):217–223. doi:10.1248/yakushi.126.217
29. Rossi M, Roumeguère T. Silodosin in the treatment of benign prostatic hyperplasia. Drug Des Devel Ther. 2010;4:291–297. doi:10.2147/DDDT.S10428
30. Yoshida M, Kudoh J, Homma Y, Kawabe K. New clinical evidence of silodosin, an α(1A) selective adrenoceptor antagonist, in the treatment for lower urinary tract symptoms. Int J Urol. 2012;19(4):306–316. doi:10.1111/j.1442-2042.2011.02957.x
31. Curran MP. Silodosin: treatment of the signs and symptoms of benign prostatic hyperplasia. Drugs. 2011;71(7):897–907. doi:10.2165/11204780-000000000-00000
32. Murata S, Taniguchi T, Takahashi M, Okada K, Akiyama K, Muramatsu I. Tissue selectivity of KMD-3213, an alpha(1)-adrenoreceptor antagonist, in human prostate and vasculature. J Urol. 2000;164(2):578–583. doi:10.1016/S0022-5347(05)67426-5
33. Goi Y, Tomiyama Y, Maruyama I, et al. Silodosin, an α(1A)-adrenoceptor antagonist, may ameliorate ischemia-induced bladder denervation and detrusor dysfunction by improving bladder blood flow. Pharmacology. 2016;97(3–4):161–170. doi:10.1159/000443965
34. Aizawa N, Watanabe D, Fukuhara H, et al. Inhibitory effects of silodosin on the bladder mechanosensitive afferent activities and their relation with bladder myogenic contractions in male rats with bladder outlet obstruction. Neurourol Urodyn. 2018;37(6):1897–1903. doi:10.1002/nau.23547
35. Quaresma BMCS, Pimenta AR, Santos da Silva AC, et al. Revisiting the pharmacodynamic uroselectivity of α1-adrenergic receptor antagonists. J Pharmacol Exp Ther. 2019;371(1):106–112. doi:10.1124/jpet.119.260216
36. Watson Laboratories Inc. Us prescribing information: rapaflo (silodosin). Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2013/022206s012lbl.pdf.
37. Silodosin. In: LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. National Institute of Diabetes and Digestive and Kidney Diseases; 2012. Available from: http://www.ncbi.nlm.nih.gov/books/NBK548170/.
38. Nomura N, Ito T, Kanada Y, et al. A case of severe liver injury induced by silodosin. Kanzo. 2014;55(11):670–676. doi:10.2957/kanzo.55.670
39. Hawrylyshyn KA, Michelotti GA, Cogé F. Update on human alpha1-adrenoceptor subtype signaling and genomic organization. Trends Pharmacol Sci. 2004;25(9). doi:10.1016/j.tips.2004.06.011
40. Yokoyama O, Ito H, Aoki Y, Oyama N, Miwa Y, Akino H. Selective α1A-blocker improves bladder storage function in rats via suppression of C-fiber afferent activity. World J Urol. 2010;28(5):609–614. doi:10.1007/s00345-009-0481-2
41. MacDiarmid SA, Hill LA, Volinn W, Hoel G. Lack of pharmacodynamic interaction of silodosin, a highly selective alpha1a-adrenoceptor antagonist, with the phosphodiesterase-5 inhibitors sildenafil and tadalafil in healthy men. Urology. 2010;75(3):520–525. doi:10.1016/j.urology.2009.10.042
42. Albisinni S, Biaou I, Marcelis Q, Aoun F, De Nunzio C, Roumeguère T. New medical treatments for lower urinary tract symptoms due to benign prostatic hyperplasia and future perspectives. BMC Urol. 2016;16(1):58. doi:10.1186/s12894-016-0176-0
43. Coyne KS, Sexton CC, Thompson CL, et al. The prevalence of lower urinary tract symptoms (LUTS) in the USA, the UK and Sweden: results from the Epidemiology of LUTS (EpiLUTS) study. BJU Int. 2009;104(3):352–360. doi:10.1111/j.1464-410X.2009.08427.x
44. Irwin DE, Kopp ZS, Agatep B, Milsom I, Abrams P. Worldwide prevalence estimates of lower urinary tract symptoms, overactive bladder, urinary incontinence and bladder outlet obstruction. BJU Int. 2011;108(7):1132–1138. doi:10.1111/j.1464-410X.2010.09993.x
45. Russo GI, Urzì D, Cimino S. Chapter 1 - Epidemiology of LUTS and BPH. In: Morgia G, Russo GI, editors. Lower Urinary Tract Symptoms and Benign Prostatic Hyperplasia. Academic Press; 2018:1–14. doi:10.1016/B978-0-12-811397-4.00001-9
46. Marks LS, Gittelman MC, Hill LA, Volinn W, Hoel G. Rapid efficacy of the highly selective alpha1A-adrenoceptor antagonist silodosin in men with signs and symptoms of benign prostatic hyperplasia: pooled results of 2 Phase 3 studies. J Urol. 2009;181(6):2634–2640. doi:10.1016/j.juro.2009.02.034
47. Marks LS, Gittelman MC, Hill LA, Volinn W, Hoel G. Silodosin in the treatment of the signs and symptoms of benign prostatic hyperplasia: a 9-month, open-label extension study. Urology. 2009;74(6):1318–1322. doi:10.1016/j.urology.2009.06.072
48. Yamanishi T, Mizuno T, Tatsumiya K, Watanabe M, Kamai T, Yoshida KI. Urodynamic effects of silodosin, a new alpha 1A-adrenoceptor selective antagonist, for the treatment of benign prostatic hyperplasia. Neurourol Urodyn. 2010;29(4):558–562. doi:10.1002/nau.20802
49. Matsukawa Y, Gotoh M, Komatsu T, Funahashi Y, Sassa N, Hattori R. Efficacy of silodosin for relieving benign prostatic obstruction: prospective pressure flow study. J Urol. 2013;189(1 Suppl):S117–121. doi:10.1016/j.juro.2012.11.031
50. Fusco F, Creta M, Longo N, Persico F, Franco M, Mirone V. Silodosin 8 mg improves benign prostatic obstruction in Caucasian patients with lower urinary tract symptoms suggestive of benign prostatic enlargement: results from an explorative clinical study. BMC Urol. 2018;18(1):12. doi:10.1186/s12894-018-0326-7
51. Chapple CR, Montorsi F, Tammela TLJ, et al. Silodosin therapy for lower urinary tract symptoms in men with suspected benign prostatic hyperplasia: results of an international, randomized, double-blind, placebo- and active-controlled clinical trial performed in Europe. Eur Urol. 2011;59(3):342–352. doi:10.1016/j.eururo.2010.10.046
52. Montorsi F, Gandaglia G, Chapple C, Cruz F, Desgrandchamps F, Llorente C. Effectiveness and safety of silodosin in the treatment of lower urinary tract symptoms in patients with benign prostatic hyperplasia: a European phase IV clinical study (SiRE study). Int J Urol. 2016;23(7):572–579. doi:10.1111/iju.13088
53. Roehrborn CG, Kaplan SA, Lepor H, Volinn W. Symptomatic and urodynamic responses in patients with reduced or no seminal emission during silodosin treatment for LUTS and BPH. Prostate Cancer Prostatic Dis. 2011;14(2):143–148. doi:10.1038/pcan.2010.46
54. Matsukawa Y, Takai S, Funahashi Y, et al. Effects of withdrawing α1-blocker from combination therapy with α1-blocker and 5α-reductase inhibitor in patients with lower urinary tract symptoms suggestive of benign prostatic hyperplasia: a prospective and comparative trial using urodynamics. J Urol. 2017;198(4):905–912. doi:10.1016/j.juro.2017.05.031
55. Yoshida T, Kinoshita H, Shimada S, Taguchi M, Matsuda T. Comparison of silodosin monotherapy vs silodosin with tadalafil add-on therapy in patients with benign prostatic hyperplasia. Urology. 2017;106:153–159. doi:10.1016/j.urology.2017.04.012
56. Matsukawa Y, Takai S, Funahashi Y, Kato M, Yamamoto T, Gotoh M. Long-term efficacy of a combination therapy with an anticholinergic agent and an α1-blocker for patients with benign prostatic enlargement complaining both voiding and overactive bladder symptoms: a randomized, prospective, comparative trial using a urodynamic study. Neurourol Urodyn. 2017;36(3):748–754. doi:10.1002/nau.23013
57. Shirakawa T, Haraguchi T, Shigemura K, et al. Silodosin versus naftopidil in Japanese patients with lower urinary tract symptoms associated with benign prostatic hyperplasia: a randomized multicenter study. Int J Urol. 2013;20(9):903–910. doi:10.1111/iju.12055
58. Osman NI, Chapple CR, Tammela TL, Eisenhardt A, Oelke M. Open-label, 9-month extension study investigating the uro-selective alpha-blocker silodosin in men with LUTS associated with BPH. World J Urol. 2015;33(5):697–706. doi:10.1007/s00345-015-1519-2
59. Takahashi H, Kubono S, Taneyama T, et al. Post-marketing surveillance of silodosin in patients with benign prostatic hyperplasia and poor response to existing Alpha-1 blockers: the SPLASH Study. Drugs R D. 2019;19(1):47–55. doi:10.1007/s40268-018-0258-4
60. Gang WANG. Efficacy and safety of silodosin and tamsulosin in the treatment of lower urinary tract symptoms associated with benign prostatic hyperplasia. Available from: http://www.cqvip.com/qk/97417a/201824/6100115650.html.
61. Takao T, Tsujimura A, Kiuchi H, et al. Early efficacy of silodosin in patients with lower urinary tract symptoms suggestive of benign prostatic hyperplasia. Int J Urol. 2008;15(11):992–996. doi:10.1111/j.1442-2042.2008.02154.x
62. Kawabe K, Yoshida M, Homma Y; Silodosin Clinical Study Group. Silodosin, a new alpha1A-adrenoceptor-selective antagonist for treating benign prostatic hyperplasia: results of a phase III randomized, placebo-controlled, double-blind study in Japanese men. BJU Int. 2006;98(5):1019–1024. doi:10.1111/j.1464-410X.2006.06448.x
63. Watanabe M, Yamanishi T, Mizuno T, et al. Effects of silodosin on lower urinary tract symptoms in patients with benign prostatic hyperplasia: evaluation by frequency/volume chart. Low Urin Tract Symptoms. 2010;2(1):31–36. doi:10.1111/j.1757-5672.2010.00059.x
64. Moon KH, Song PH, Yang DY, et al. Efficacy and safety of the selective α1A-adrenoceptor blocker silodosin for severe lower urinary tract symptoms associated with benign prostatic hyperplasia: a prospective, single-open-label, multicenter study in Korea. Korean J Urol. 2014;55(5):335–340. doi:10.4111/kju.2014.55.5.335
65. Cho KJ, Lee JZ, Song YS, et al. Evaluating the efficacy and safety of silodosin on nocturia in patients with benign prostatic hyperplasia: a multicenter, prospective, open-label, single-arm, Phase IV trial. Urology. 2018;121:153–157. doi:10.1016/j.urology.2018.07.008
66. Choi WS, Cho MC, Lee JW, et al. Efficacy and safety of silodosin in the treatment of lower urinary tract symptoms in elderly men taking antihypertensive medications. Prostate Int. 2017;5(3):113–118. doi:10.1016/j.prnil.2017.02.001
67. Eisenhardt A, Schneider T, Cruz F, Oelke M. Consistent and significant improvement of nighttime voiding frequency (nocturia) with silodosin in men with LUTS suggestive of BPH: pooled analysis of three randomized, placebo-controlled, double-blind phase III studies. World J Urol. 2014;32(5):1119–1125. doi:10.1007/s00345-013-1228-7
68. Seki N, Takahashi R, Yamaguchi A, et al. Non-inferiority of silodosin 4 mg once daily to twice daily for storage symptoms score evaluated by the International Prostate Symptom Score in Japanese patients with benign prostatic hyperplasia: a multicenter, randomized, parallel-group study. Int J Urol. 2015;22(3):311–316. doi:10.1111/iju.12680
69. Choo MS, Song M, Kim JH, et al. Safety and efficacy of 8-mg once-daily vs 4-mg twice-daily silodosin in patients with lower urinary tract symptoms suggestive of benign prostatic hyperplasia (SILVER Study): a 12-week, double-blind, randomized, parallel, multicenter study. Urology. 2014;83(4):875–881. doi:10.1016/j.urology.2013.11.013
70. Gul A, Coban S, Turkoglu AR, Guzelsoy M, Ozturk M, Kankilic NA. Comparative efficacy and safety profile of 4 vs 8 mg of silodosin once daily usage in patients with benign prostatic hyperplasia–related lower urinary tract symptoms divided into subgroups according to International Prostate Symptom Score severity. Prostate International. 2020;8(4):152–157. doi:10.1016/j.prnil.2020.04.002
71. Novara G, Tubaro A, Sanseverino R, et al. Systematic review and meta-analysis of randomized controlled trials evaluating silodosin in the treatment of non-neurogenic male lower urinary tract symptoms suggestive of benign prostatic enlargement. World J Urol. 2013;31(4):997–1008. doi:10.1007/s00345-012-0944-8
72. Novara G, Chapple CR, Montorsi F. Individual patient data from registrational trials of silodosin in the treatment of non-neurogenic male lower urinary tract symptoms (LUTS) associated with benign prostatic hyperplasia (BPH): subgroup analyses of efficacy and safety data. BJU Int. 2015;115(5):802–814. doi:10.1111/bju.12906
73. Homma Y, Gotoh M, Kawauchi A, et al. Clinical guidelines for male lower urinary tract symptoms and benign prostatic hyperplasia. Int J Urol. 2017;24(10):716–729. doi:10.1111/iju.13401
74. McVary KT, Roehrborn CG, Avins AL, et al. Update on AUA guideline on the management of benign prostatic hyperplasia. J Urol. 2011;185(5):1793–1803. doi:10.1016/j.juro.2011.01.074
75. Matsukawa Y, Takai S, Majima T, et al. Comparison in the efficacy of fesoterodine or mirabegron add-on therapy to silodosin for patients with benign prostatic hyperplasia complicated by overactive bladder: a randomized, prospective trial using urodynamic studies. Neurourol Urodyn. 2019;38(3):941–949. doi:10.1002/nau.23935
76. Matsukawa Y, Funahashi Y, Takai S, et al. Comparison of silodosin and naftopidil for efficacy in the treatment of benign prostatic enlargement complicated by overactive bladder: a randomized, prospective study (SNIPER Study). J Urol. 2017;197(2):452–458. doi:10.1016/j.juro.2016.08.111
77. Kumar S, Tiwari DP, Ganesamoni R, Singh SK. Prospective randomized placebo-controlled study to assess the safety and efficacy of silodosin in the management of acute urinary retention. Urology. 2013;82(1):171–175. doi:10.1016/j.urology.2013.02.020
78. Hagiwara K, Koie T, Iwamura H, et al. Efficacy and safety of silodosin and dutasteride combination therapy in acute urinary retention due to benign prostatic hyperplasia: a single-arm prospective study. Biomed Res Int. 2016;2016:4975851. doi:10.1155/2016/4975851
79. Rees J, Abrahams M, Doble A, Cooper A. Prostatitis Expert Reference Group (PERG). Diagnosis and treatment of chronic bacterial prostatitis and chronic prostatitis/chronic pelvic pain syndrome: a consensus guideline. BJU Int. 2015;116(4):509–525. doi:10.1111/bju.13101
80. Krieger JN, Lee SWH, Jeon J, Cheah PY, Liong ML, Riley DE. Epidemiology of prostatitis. Int J Antimicrob Agents. 2008;31(Suppl 1):S85–90. doi:10.1016/j.ijantimicag.2007.08.028
81. Krieger JN, Nyberg L, Nickel JC. NIH consensus definition and classification of prostatitis. JAMA. 1999;282(3):236–237. doi:10.1001/jama.282.3.236
82. Pavone-Macaluso M. Chronic prostatitis syndrome: a common, but poorly understood condition. Part I. EAU-EBU Update Series. 2007;5(1):1–15. doi:10.1016/j.eeus.2006.10.002
83. Tuğcu V, Taşçi AI, Fazlioğlu A, et al. A placebo-controlled comparison of the efficiency of triple- and monotherapy in category III B chronic pelvic pain syndrome (CPPS). Eur Urol. 2007;51(4):
84. Evliyaoğlu Y, Burgut R. Lower urinary tract symptoms, pain and quality of life assessment in chronic non-bacterial prostatitis patients treated with alpha-blocking agent doxazosin; versus placebo. Int Urol Nephrol. 2002;34(3):351–356. doi:10.1023/a:
85. Mehik A, Alas P, Nickel JC, Sarpola A, Helström PJ. Alfuzosin treatment for chronic prostatitis/chronic pelvic pain syndrome: a prospective, randomized, double-blind, placebo-controlled, pilot study. Urology. 2003;62(3):425–429. doi:10.1016/S0090-4295(03)00466-7
86. Cheah PY, Liong ML, Yuen KH, et al. Terazosin therapy for chronic prostatitis/chronic pelvic pain syndrome: a randomized, placebo controlled trial. J Urol. 2003;169(2):592–596. doi:10.1097/01.ju.0000042927.45683.6c
87. Nickel JC, Narayan P, McKay J, Doyle C. Treatment of chronic prostatitis/chronic pelvic pain syndrome with tamsulosin: a randomized double blind trial. J Urol. 2004;171(4):1594–1597. doi:10.1097/01.ju.0000117811.40279.19
88. Jeong CW, Lim DJ, Son H, Lee SE, Jeong H. Treatment for chronic prostatitis/ chronic pelvic pain syndrome: levofloxacin, doxazosin and their combination. UIN. 2008;80(2):157–161. doi:10.1159/000112606
89. Barbalias GA, Nikiforidis G, Liatsikos EN. Alpha-blockers for the treatment of chronic prostatitis in combination with antibiotics. J Urol. 1998;159(3):883–887. doi:10.1016/S0022-5347(01)63761-3
90. Professionals SO. EAU guidelines: chronic pelvic pain. Uroweb. Available from: https://uroweb.org/guideline/chronic-pelvic-pain/.
91. Nickel JC, O’Leary MP, Lepor H, et al. Silodosin for men with chronic prostatitis/chronic pelvic pain syndrome: results of a phase II multicenter, double-blind, placebo controlled study. J Urol. 2011;186(1):125–131. doi:10.1016/j.juro.2011.03.028
92. Alexander RB, Propert KJ, Schaeffer AJ, et al. Ciprofloxacin or tamsulosin in men with chronic prostatitis/chronic pelvic pain syndrome: a randomized, double-blind trial. Ann Intern Med. 2004;141(8):581–589. doi:10.7326/0003-4819-141-8-200410190-00005
93. Nickel JC, Krieger JN, McNaughton-Collins M, et al. Alfuzosin and symptoms of chronic prostatitis-chronic pelvic pain syndrome. N Engl J Med. 2008;359(25):2663–2673. doi:10.1056/NEJMoa0803240
94. Hisasue S-I, Furuya R, Itoh N, Kobayashi K, Furuya S, Tsukamoto T. Ejaculatory disorder caused by alpha-1 adrenoceptor antagonists is not retrograde ejaculation but a loss of seminal emission. Int J Urol. 2006;13(10):1311–1316. doi:10.1111/j.1442-2042.2006.01535.x
95. Moriyama N, Nasu K, Takeuchi T, et al. Quantification and distribution of alpha 1-adrenoceptor subtype mRNAs in human vas deferens: comparison with those of epididymal and pelvic portions. Br J Pharmacol. 1997;122(6):1009–1014. doi:10.1038/sj.bjp.0701485
96. Akin Y, Gulmez H, Ates M, Bozkurt A, Nuhoglu B. Comparison of alpha blockers in treatment of premature ejaculation: a pilot clinical trial. Iran Red Crescent Med J. 2013;15(10):e13805. doi:10.5812/ircmj.13805
97. Sato Y, Tanda H, Nakajima H, et al. Silodosin and its potential for treating premature ejaculation: a preliminary report. Int J Urol. 2012;19(3):268–272. doi:10.1111/j.1442-2042.2011.02941.x
98. Sato Y, Otani T, Amano T, et al. Silodosin versus naftopidil in the treatment of premature ejaculation: a prospective multicenter trial. Int J Urol. 2017;24(8):626–631. doi:10.1111/iju.13392
99. Bhat GS, Shastry A. Effectiveness of “on demand” silodosin in the treatment of premature ejaculation in patients dissatisfied with dapoxetine: a randomized control study. Cent European J Urol. 2016;69(3):280–284. doi:10.5173/ceju.2016.843
100. Preminger GM, Tiselius HG, Assimos DG, et al. 2007 Guideline for the management of ureteral calculi. J Urol. 2007;178(6):2418–2434. doi:10.1016/j.juro.2007.09.107
101. Taguchi K, Cho SY, Ng AC, et al. The Urological Association of Asia clinical guideline for urinary stone disease. Int J Urol. 2019;26(7):688–709. doi:10.1111/iju.13957
102. Professionals SO. EAU guidelines: urolithiasis. Uroweb. Available from: https://uroweb.org/guideline/urolithiasis/#3.
103. Gupta S, Lodh B, Singh AK, Somarendra K, Meitei KS, Singh SR. Comparing the efficacy of tamsulosin and silodosin in the medical expulsion therapy for ureteral calculi. J Clin Diagn Res. 2013;7(8):1672–1674. doi:10.7860/JCDR/2013/6141.3241
104. Bos D, Kapoor A. Update on medical expulsive therapy for distal ureteral stones: beyond alpha-blockers. Can Urol Assoc J. 2014;8(11–12):442–445. doi:10.5489/cuaj.2472
105. Tzortzis V, Mamoulakis C, Rioja J, Gravas S, Michel MC, de la Rosette JJ. Medical expulsive therapy for distal ureteral stones. Drugs. 2009;69(6):677–692. doi:10.2165/00003495-200969060-00003
106. Itoh Y, Okada A, Yasui T, et al. Efficacy of selective α1A adrenoceptor antagonist silodosin in the medical expulsive therapy for ureteral stones. Int J Urol. 2011;18(9):672–674. doi:10.1111/j.1442-2042.2011.02810.x
107. Kumar S, Jayant K, Agrawal MM, Singh SK, Agrawal S, Parmar KM. Role of tamsulosin, tadalafil, and silodosin as the medical expulsive therapy in lower ureteric stone: a randomized trial (a pilot study). Urology. 2015;85(1):59–63. doi:10.1016/j.urology.2014.09.022
108. Imperatore V, Fusco F, Creta M, et al. Medical expulsive therapy for distal ureteric stones: tamsulosin versus silodosin. Arch Ital Urol Androl. 2014;86(2):103–107. doi:10.4081/aiua.2014.2.103
109. Sur RL, Shore N, L’Esperance J, et al. Silodosin to facilitate passage of ureteral stones: a multi-institutional, randomized, double-blinded, placebo-controlled trial. Eur Urol. 2015;67(5):959–964. doi:10.1016/j.eururo.2014.10.049
110. Elgalaly H, Sakr A, Fawzi A, et al. Silodosin vs tamsulosin in the management of distal ureteric stones: a prospective randomised study. Arab J Urol. 2016;14(1):12–17. doi:10.1016/j.aju.2015.11.004
111. Gharib T, Mohey A, Fathi A, Alhefnawy M, Alazaby H, Eldakhakhny A. Comparative study between silodosin and tamsulosin in expectant therapy of distal ureteral stones. Urol Int. 2018;101(2):161–166. doi:10.1159/000490623
112. Mohammed N, Kestin L, Ghilezan M, et al. Comparison of acute and late toxicities for three modern high-dose radiation treatment techniques for localized prostate cancer. Int J Radiat Oncol Biol Phys. 2012;82(1):204–212. doi:10.1016/j.ijrobp.2010.10.009
113. Tanaka N, Asakawa I, Anai S, et al. Periodical assessment of genitourinary and gastrointestinal toxicity in patients who underwent prostate low-dose-rate brachytherapy. Radiat Oncol. 2013;8:25. doi:10.1186/1748-717X-8-25
114. Tanaka N, Torimoto K, Asakawa I, et al. Use of alpha-1 adrenoceptor antagonists in patients who underwent low-dose-rate brachytherapy for prostate cancer - a randomized controlled trial of silodosin versus naftopidil. Radiat Oncol. 2014;9:302. doi:10.1186/s13014-014-0302-7
115. Tsumura H, Satoh T, Ishiyama H, et al. Comparison of prophylactic naftopidil, tamsulosin, and silodosin for 125I brachytherapy-induced lower urinary tract symptoms in patients with prostate cancer: randomized controlled trial. Int J Radiat Oncol Biol Phys. 2011;81(4):e385–392. doi:10.1016/j.ijrobp.2011.04.026
116. Oyama N, Aoki Y, Ito H, et al. Alpha 1-adrenoceptor blocker may improve not only voiding but also storage lower urinary tract symptoms caused by (125) I brachytherapy for prostate cancer. ISRN Urol. 2014;2014:140654. doi:10.1155/2014/140654
117. Shimizu N, Minami T, Sugimoto K, et al. Efficacy of silodosin in patients undergoing brachytherapy: a randomized trial involving a pressure flow study. World J Urol. 2014;32(6):1423–1432. doi:10.1007/s00345-014-1239-z
118. Fusco F, Creta M, De Nunzio C, Gacci M, Li Marzi V, Finazzi Agrò E. Alpha-1 adrenergic antagonists, 5-alpha reductase inhibitors, phosphodiesterase type 5 inhibitors, and phytotherapic compounds in men with lower urinary tract symptoms suggestive of benign prostatic obstruction: a systematic review and meta-analysis of urodynamic studies. Neurourol Urodyn. 2018;37(6):1865–1874. doi:10.1002/nau.23554
119. MacDonald R, Brasure M, Dahm P, et al. Efficacy of newer medications for lower urinary tract symptoms attributed to benign prostatic hyperplasia: a systematic review. Aging Male. 2019;22(1):1–11. doi:10.1080/13685538.2018.1434503
120. Creta M, Cornu JN, Roehrborn CG, et al. Clinical efficacy of silodosin in patients with severe lower urinary tract symptoms related to benign prostatic obstruction: a pooled analysis of Phase 3 and 4 trials. Eur Urol Focus. 2021;7(2):440–443. doi:10.1016/j.euf.2020.01.014
121. Yoon PD, Chalasani V, Woo HH. Systematic review and meta-analysis on management of acute urinary retention. Prostate Cancer Prostatic Dis. 2015;18(4):297–302. doi:10.1038/pcan.2015.15
122. Hsu YP, Hsu CW, Bai CH, Cheng SW, Chen KC, Chen C. Silodosin versus tamsulosin for medical expulsive treatment of ureteral stones: a systematic review and meta-analysis. PLoS One. 2018;13(8):e0203035. doi:10.1371/journal.pone.0203035
123. Özsoy M, Liatsikos E, Scheffbuch N, Kallidonis P. Comparison of silodosin to tamsulosin for medical expulsive treatment of ureteral stones: a systematic review and meta-analysis. Urolithiasis. 2016;44(6):491–497. doi:10.1007/s00240-016-0872-y
124. Sharma G, Pareek T, Kaundal P, et al. Comparison of efficacy of three commonly used alpha-blockers as medical expulsive therapy for distal ureter stones: a systematic review and network meta-analysis. Int Braz J Urol. 2021;47. doi:10.1590/S1677-5538.IBJU.2020.0548
125. Sharma G, Kaundal P, Pareek T, et al. Comparison of efficacy of various drugs used for medical expulsive therapy for distal ureter stones: a systematic review and network meta-analysis. Int J Clin Pract. 2021;75:e14214. doi:10.1111/ijcp.14214
126. Liu H, Wang S, Zhu W, Lu J, Wang X, Yang W. Comparative efficacy of 22 drug interventions as medical expulsive therapy for ureteral stones: a systematic review and network meta-analysis. Urolithiasis. 2020;48(5):447–457. doi:10.1007/s00240-019-01159-5
127. Montorsi F. Profile of silodosin. Urologiia. 2013;4:
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.