")
Back to Journals » International Journal of General Medicine » Volume 15
Evolution of Endoscopic Thyroidectomy: Will a Novel Single Channel Flexible Endoscopic Approach Change the Treatment Paradigm?
Received 27 January 2022
Accepted for publication 28 February 2022
Published 10 March 2022 Volume 2022:15 Pages 2795—2798
DOI https://doi.org/10.2147/IJGM.S360138
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Bowen Hu,1 Huanfei Ding2
1Department of Hepatobiliary and Pancreatic Surgery, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, 450052, Henan, People’s Republic of China; 2Department of Ultrasound, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, 450052, Henan, People’s Republic of China
Correspondence: Bowen Hu, Department of Hepatobiliary and Pancreatic Surgery, The First Affiliated Hospital of Zhengzhou University, No. 1 Eastern Jianshe Road, Zhengzhou, 450052, Henan, People’s Republic of China, Tel +86-15286819833, Email [email protected]
Abstract: Endoscopic thyroidectomy has evolved from a hybrid approach utilizing a laparoscopic assistant and robotic-assistance to pure flexible endoscopic thyroidectomy without laparoscopic assistance. However, all the hybrid approaches are complicated and results in scar somewhere on the body surface. Current experimental and clinical studies focus on the implementation of new minimally invasive approaches such as flexible endoscopic thyroidectomy which leaves no scar on the body surface and easier to perform. Flexible endoscopic thyroidectomy is seeming to be a relatively safe and feasible technique with good outcomes. However, more research, particularly using newly developed tools to further improve this technique, and large scaled practice is needed to make it more available to patients worldwide. This article summarizes established endoscopic thyroidectomy techniques and highlight the pros and cons of different available endoscopic approaches to thyroid resection, and discussed how flexible endoscopic thyroidectomy compares to the well establish techniques and future perspective.
Keywords: NOTES, endoscopic thyroidectomy, flexible endoscopy, laparoscopy, robotic endoscopic surgery
Introduction
Thyroid Surgery including thyroidectomy is an area potentially amenable to minimally invasive surgery using a vestibular incision to facilitate endoscopic and robotic transoral approaches.1–3 The initial approaches have utilized rigid endoscopes or linear robotic platforms which require a large working space. Hybrid NOTES or laparoscopic-assisted procedures have also been used for thyroidectomy using a vestibular approach.4,5 Although these approaches are less invasive they have been associated with complications with a proportion requiring conversion to open surgery. The newest approach of pure flexible endoscopic thyroidectomy has been studied in porcine models and has the potential advantages of compared to hybrid NOTES or laparoscopic instrument-assisted rigid endoscopic operations.6 Here we summarize established endoscopic thyroidectomy techniques, highlight the pros and cons of different popular available endoscopic approaches to thyroid resection, and discuss how flexible endoscopic thyroidectomy compares to the well establish laparoscopic and robotic thyroidectomy techniques.
Laparoscopic-Assisted Thyroidectomy
Endoscopic surgery theoretically allows surgeons to perform thyroidectomy from remote sites without leaving a visible scar on the neck and a number of remote-access approaches have been developed for thyroid surgery over the past 2 decades. Most still result in a visible scar somewhere on the body. For example, Angkoon et al and others reported hybrid NOTES thyroidectomy using a vestibular approach.4,5,7,8 The technique’s evolution began with a sublingual transoral approach which involved piercing through the floor of the mouth. Because of severe tissue damages and a high risk of complications the technique was modified to utilize the oral vestibular approach (laparoscopic-assisted/hybrid NOTES) which employs vestibular incisions anterior to the mandible between the mentalis muscles. The laparoscopic-assisted vestibular approach is currently being utilized at various centers and requires three ports and a large operative field (Figure 1A).7,8 However, even with the large working space it may be difficult to reach all parts of the thyroid gland and 5 to 10% of procedures must be converted to open surgery. With this approach precise dissection is a challenge and only thyroid specimens less than 2 to 3 cm can be removed via the intraoral midline incision. Larger or specimens with as hard consistency must be fragmented in order to be removed through the midline incision. Such tumor manipulation may also cause capsule disruption which increases the risk of tumor spillage into the operative field.
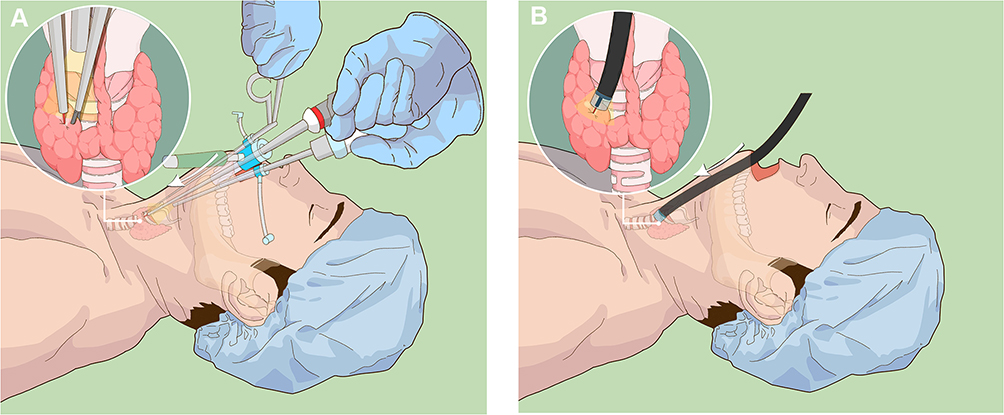 |
Figure 1 (A) Schematic of laparoscopic-assisted surgery with three ports and a large operative field. (B) Schematic of pure flexible endoscopic thyroidectomy. |
Robotic Thyroidectomy
Transoral robotic thyroidectomy was the introduction of robot technology to thyroidectomy and combination with the transoral vestibular approach provided new solutions.9 Elizabeth et al reported transoral thyroidectomy using a flexible robotic system and noted no major limitations to its use.10 However, they found that lateral ports would still be necessary for the introduction of instruments. The technique embodies minimally invasive principles, including limited tissue dissection and retraction, close access to the thyroid gland, natural orifice surgery, and produces no visible cutaneous scar. These improvements addressed many of the limitations of current robotic technology. However, there are still obstacles to overcome for transoral robotic thyroidectomy. As well all robotic surgery, the surgeon cannot directly receive real-time tactile feedback as is available using laparoscopic instruments. Moreover, robotic thyroidectomies require additional time for robot docking and currently require a relatively longer operation time compared to the transoral endoscopic vestibular approach. Furthermore, while conventional laparoscopic instruments are readily available in most hospital facilities nowadays, access to robotic systems remains limited. Robotic surgery is also still relatively more expensive than laparoscopic-assisted thyroidectomy. Nonetheless, with the increasing number of companies investing and competing in robotic surgical system production and development, such financial barriers may diminish over time in the future.
Flexible Endoscopic Thyroidectomy
Liu et al proposed a novel technique of flexible endoscopic thyroidectomy based on their success with flexible endoscopy for pure NOTES. They reported a pilot study in the porcine model to assess the feasibility of flexible endoscopic transoral thyroidectomy.6 Using a transoral incision a subcutaneous tunnel was produced from the mouth to the thyroid gland to perform a partial thyroidectomy. Flexible endoscopic thyroidectomy includes the following steps: (1) locate the thyroid site using Ultrasound, (2) make a vestibular incision of 15 mm in the midline, (2) make a tunnel using forceps through the mandible (3) insertion of single channel flexible endoscope into the tunnel to access the thyroid gland, (4) dissection of thyroid gland using hook and insulated tip knives, and (5) complete the resection of gland using snare and removed the specimen with endoscopic assistance. The procedure was successfully performed in six swine, with a mean procedure time of 35 min; none of the swine experienced adverse events. The experiment showed that endoscopic thyroidectomy could be performed using a single operating channel which obviated the need for hybrid NOTES or laparoscopic instrument-assisted rigid endoscopes (Figure 1B). With flexible endoscopy it proved possible to reach all parts of the thyroid gland. The gland was partially resected, among the skills needed for successful total thyroidectomy in humans include reliable Identification and preservation of the recurrent laryngeal nerve and parathyroid glands as well as Identification and ligation of the superior and inferior thyroid vessels. However, there is a limitation in the current pilot study because the pig thyroid gland anatomy is bit different from that of humans. Translation of these techniques to humans will require modification and practice but this first step showing safe and rapid thyroid resection in humans should be feasible. However, by flexible endoscopic techniques we can perform all kinds of procedures and if this is performed in humans, the parathyroid gland and recurrent laryngeal nerve can be detected and protected in the same way as done by rigid endoscope (laparoscopic-assisted). There are several existed methods surgeon uses for retraction of specimen and same can be used with flexible endoscope as well. In this current study only snare was used to retract as this was the normal gland tissue. For cancerous lesion basket/bag can be used which can cover the cancerous tissue completely and not letting the cancerous cell spread. Further development of a flexible endoscopic thyroidectomy approach should aim not only for larger scale preclinical studies but also for conducting randomized controlled trials comparing this novel modality to well establish laparoscopic and robotic thyroidectomy techniques.
Conclusion and Future Perspective
Flexible endoscopes provide the much needed freedom for tissue access, manipulation, traction, resection, and suturing.9,10 Flexible endoscopic thyroidectomies is likely to be a relatively safe and feasible technique and have potential advantages over laparoscopic or other hybrid techniques including requiring a limited working space, little tissue damage, less procedure time, and quick recovery. However, more research, particularly using newly developed tools to further improve this technique, and large scaled practice is needed to make it more available to patients worldwide. Clinical application of the technique will require cooperation between gastroenterologists and ENT/Aesthetic surgeons to take advantage of the gastroenterologist’s skills with flexible endoscopy and the surgeon’s practical knowledge and experience with thyroidectomy. Acquisition of skills learned from the endoscopist may eventually allow ENT surgeons to perform these types of surgery either independently or as combined GI-ENT procedures.
Funding
This study was financially supported by grants from Hepatobiliary foundation of Henan Charity General Federation (No: GDXZ2019006) and Hepatobiliary foundation of Henan Charity General Fedration (No: GDXZ2022003).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cottrill EE, Funk EK, Goldenberg D, et al. Transoral thyroidectomy using a flexible robotic system: a Preclinical Cadaver Feasibility Study. Laryngoscope. 2019;129(6):1482–1487. doi:10.1002/lary.27543
2. Jongekkasit I, Jitpratoom P, Sasanakietkul T, et al. Transoral endoscopic thyroidectomy for thyroid cancer. Endocrinol Metab Clin North Am. 2019;48(1):165–180. doi:10.1016/j.ecl.2018.11.009
3. Fernandez-Ranvier G, Meknat A, Guevara DE, et al. Transoral endoscopic thyroidectomy vestibular approach. JSLS. 2019;23(4):
4. Anuwong A, Ketwong K, Jitpratoom P, et al. Safety and outcomes of the transoral endoscopic thyroidectomy vestibular approach. JAMA Surg. 2018;153(1):21–27. doi:10.1001/jamasurg.2017.3366
5. Anuwong A, Sasanakietkul T, Jitpratoom P, et al. Transoral endoscopic thyroidectomy vestibular approach (TOETVA): indications, techniques and results. Surg. Endosc. 2018;32(1):456–465. doi:10.1007/s00464-017-5705-8
6. Liu BR, Qiu XG, Li DL, et al. Flexible endoscopic transoral thyroidectomy: a pilot study in a porcine model (with video). Gastrointest Endosc. 2021;93(1):224–228. doi:10.1016/j.gie.2020.07.033
7. Anuwong A. Transoral endoscopic thyroidectomy vestibular approach: a series of the first 60 human cases. World J Surg. 2016;40(3):491–497. doi:10.1007/s00268-015-3320-1
8. Zorron R, Bures C, Brandl A, et al. [Tips and technical issues for performing transoral endoscopic thyroidectomy with vestibular approach (TOETVA): a novel scarless technique for neck surgery]. Chirurg. 2018;89(7):529–536. German. doi:10.1007/s00104-018-0658-6
9. Richmon JD, Kim HY. Transoral robotic thyroidectomy (TORT): procedures and outcomes. Gland Surg. 2017;Jun(3):285–289. doi:10.21037/gs.2017.05.05
10. Bernhardt J, Sasse S, Ludwig K, et al. Update in Natural Orifice Translumenal Endoscopic Surgery (NOTES). Curr Opin Gastroenterol. 2017;33(5):346–351. doi:10.1097/MOG.0000000000000385
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.