")
Back to Journals » International Journal of General Medicine » Volume 15
Evidence-Based Guideline on Management of Postoperative Delirium in Older People for Low Resource Setting: Systematic Review Article
Authors Mossie A , Regasa T , Neme D, Awoke Z , Zemedkun A, Hailu S
Received 12 January 2022
Accepted for publication 5 April 2022
Published 14 April 2022 Volume 2022:15 Pages 4053—4065
DOI https://doi.org/10.2147/IJGM.S349232
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Addisu Mossie,1 Teshome Regasa,2 Derartu Neme,2 Zemedu Awoke,2 Abebayehu Zemedkun,2 Seyoum Hailu2
1Anesthesia Department, Hawassa University, Hawassa, Ethiopia; 2Anesthesia Department, Dilla University, Dilla, Ethiopia
Correspondence: Teshome Regasa, Email [email protected]
Background: Postoperative delirium is the highest prevalence and life-threatening complication following geriatric surgery. The overall incidence rate varies from 5% to 52% of hospitalized surgical patients based on the type of surgery that often began in the postanesthesia care unit and continues up to 5 days post-surgery. Postoperative delirium manifests as a hypoactive, hyperactive and mixed subtype. The mechanism of delirium development is not clear, but it is accepted that delirium is a result of the patient’s underlying vulnerabilities or risk factors combined with an outside stressor such as infection or surgery.
Objective: To develop evidence-based recommendations for the prevention, diagnosis, and treatment of postoperative delirium.
Methods: Literature was searched from PubMed, CINAH, Google Scholar, and Cochrane databases that are published from 2010 to 2021 by formulating inclusion and exclusion criteria. Filtering was made depending on methodological quality, outcome, and data on population. Finally, 11 meta-analysis, 11 systematic reviews, 7 interventional studies, 11 observational studies, and recommendations of the previous clinical practice guideline developed by the American and European are included in this review.
Results: A total of 43 studies were considered in this evaluation. The development of this guideline was based on nine studies on risk stratification for postoperative delirium, eighteen studies on risk minimization and prevention for postoperative delirium, five studies on diagnosis for postoperative delirium, and eleven studies on treatments for postoperative delirium.
Conclusion: Postoperative delirium management can be categorized into risk assessment, risk minimization, early diagnosis, and treatment. Early diagnosis is critical to trigger focused and effective treatment. Non-pharmacological interventions are the first-line management for both hypoactive and hyperactive postoperative with considering contributory factors and underlying causes. Antipsychotics should only be used for hyperactive delirium individuals who try to harm themselves. Current evidence suggested that dexmedetomidine can be used as a treatment option for postoperative delirium.
Keywords: postoperative delirium, delirium prevention, delirium screening, elderly people, delirium treatment
Introduction
Background
Delirium is defined as disturbances of mental abilities that affect thinking perception, memory, emotion, and sleep-wake disturbance. Based on the American Psychiatric Association (DSM V), a delirium diagnosis can be made when a patient presents with disorganized thinking, disturbance in attention, and level of consciousness which develops over a short period and fluctuates over time.1,2
Postoperative delirium (POD) refers to delirium in patients after completion of a surgical procedure and is defined as an acute mental disorder, characterized by disturbances in awareness, attention, and cognition. As a common postoperative complication, all age groups of patients can affect by this complication, but this postoperative complication is highly affected geriatric patients, with an incidence rate ranging from 5% to 52% depending on the risk to patients and surgical procedure of an elderly population which often began in the post-anesthesia care unit and continuous up to 5 days post-surgical procedure.3,4
Surgeries strongly associated with delirium include vascular, orthopedic, and cardiac surgery, with the condition occurring in up to 50% of the patient’s postoperative. Postoperative delirium is highly associated with emergency surgery, which is an account for 1.5 to three times non-emergency surgical procedure.5
A review by Abate et al found that the global prevalence of POD among geriatric surgical patients was 20% with the highest in patients who undergo general surgery followed by orthopedics and malignant surgeries, 23%, 22%, and, 19%, respectively.6
POD can manifest as hypoactive (drowsy, reduced motor activity), hyperactive (agitation, aggressive behavior, restlessness and harm to themselves or another individual) and mixed delirium which is characterized by showing both delirium symptoms. Hypoactive delirium is the commonest type present in around 40% of delirium cases and is unrecognized. Hypoactive delirium prognosis may be worse, secondary to under-detection by health professionals and delayed response to treatment.7 Based on the onset time, delirium in the postoperative period can be divided into emergence delirium (ED) and POD. Emergence delirium happens lasting approximately 30 minutes after emergent from surgical anesthesia procedure. Whereas POD is often notable from postoperative day 1 to a week after surgery.8
Adverse outcomes of POD include 2–3 days increase hospital stay, minimized mental activity, risk of dementia increment, and increase dependency. Furthermore, delayed recognition and treatment are related to 30-day mortality of 7% to 10% and overall mortality was up to 25%.6,9–11
The most common complication of geriatric surgery is POD with an overall incidence rate of 5% to 52% of the geriatric surgical patient.3,4,10 According to a recent review study, the prevalence of mortality from patients with POD was 25%.12 This indicates that POD has a huge burden on the health-care system and the patients.
Management of postoperative delirium can be categorized into risk assessment and stratification, risk reduction, early diagnosis, and treatment. Up to forty percent of POD can be preventable and the most effective management of POD is prevention.10,11
Identifying patients at the highest risk of developing delirium is a necessary first step, risk reduction technique by the non-pharmacological and pharmacological second step, early diagnosis is critical to trigger focused and effective treatment is an important technique in the management of postoperative delirium.13
Previous published clinical practice guidelines recommend the Confusion assessment method (CAM) and Nursing Delirium Screening Scale (Nu-DESC) as gold standards for the detection of POD, but recent evidence suggests that both screening tools have low sensitivity and specificity when compared to the 4ʹA’s Test, which has high sensitivity and specificity, requires no time or special training, and is useful in resource-limited areas.14
Furthermore, when nonpharmacological approaches have failed to control severe agitation, low-dose antipsychotics are indicated, and now, non-antipsychotic drugs such as dexmedetomidine are suggested as an alternative therapeutic agent for POD, which is included in the current guideline.15 Physicians, anesthetists, and nurses are the most common clinicians involved in the care of POD patients. Since there are different health personnel they are doing it in different ways. As a result, the purpose of these guidelines is to give guidance for clinical practice in the prevention, diagnosis, and treatment of POD. The main research questions for this systematic review are whether there are risk stratifications for POD, the use of pharmacologic and non-pharmacologic strategies for prevention of POD, identification of a quick and easy assessment tool, and determining evidence-based recommendations for the treatments of POD in old people.
Methodology
The review was conveyed based on preferred reporting items for systematic review and meta-analysis (PRISMA) protocol. Literature was searched from PubMed, Google Scholar, CINAHL, and Cochrane database in the last ten years from 2010 to 2021 to specify studies that are relevant to do this clinical practice guideline using the keywords postoperative delirium, delirium prevention, delirium screening, elderly people, and delirium treatment. From a lot of evidence obtained from a search engine, the repetition was removed using the EndNote reference manager. Studies assessing the postoperative delirium in older people management that investigating the delirium risk stratification, risk reduction, diagnosis, treatment which were published in the English language were included in the review. Articles with a pediatric patient population, not a clinical study post operative delirium based, poor methodological quality, and studies written other than the English language were excluded. Based on Critical Appraisal articles were appraised and graded depending on their level of evidence. Systematic reviews were appraised and graded according to the AMSTAR-2 appraisal checklist.16 Randomized controlled trials and prospective or retrospective cohort studies were also appraised according to the appraisal checklist of the critical appraisal skill program tool (CASP).17 Finally, 11 Meta-analyses, 11 systematic reviews, 7 RCT, 11 observational studies, and 3 recommendations of previous clinical practice guidelines by the American and European were used for this review (see Figure 1) by using the keywords (Risk assessment AND postoperative delirium, Risk-reducing AND postoperative delirium, early diagnosis AND postoperative delirium and, postoperative delirium AND Management). Two evaluators independently reviewed and determined the eligibility of articles based on the methodological quality of inclusion and exclusion criteria, as well as outcome variables. The third assessor evened out any discrepancies. The conclusion was reached using the degree of evidence provided by the Oxford Center for Evidence-Based Medicine (Table 1).18
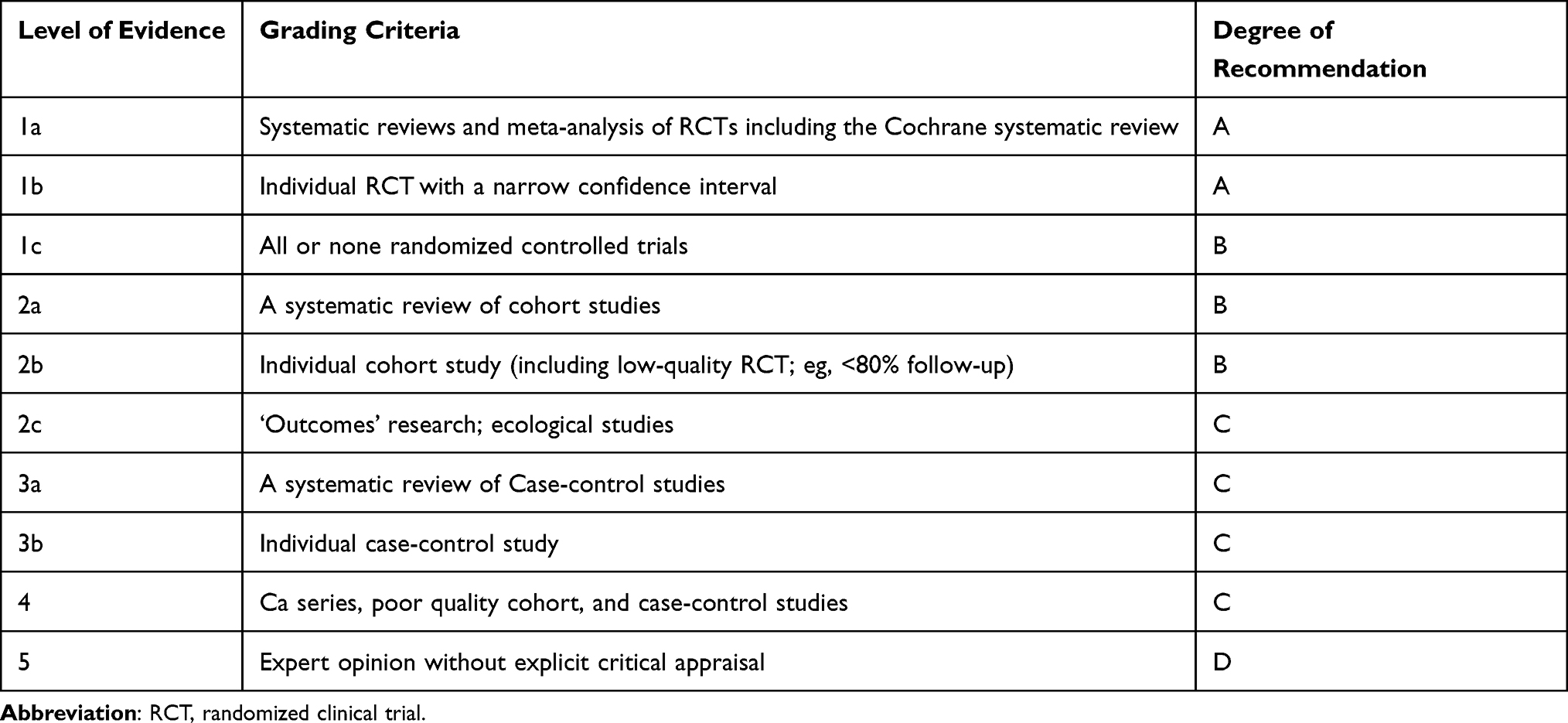 |
Table 1 Levels of Evidence and Grades of Recommendations |
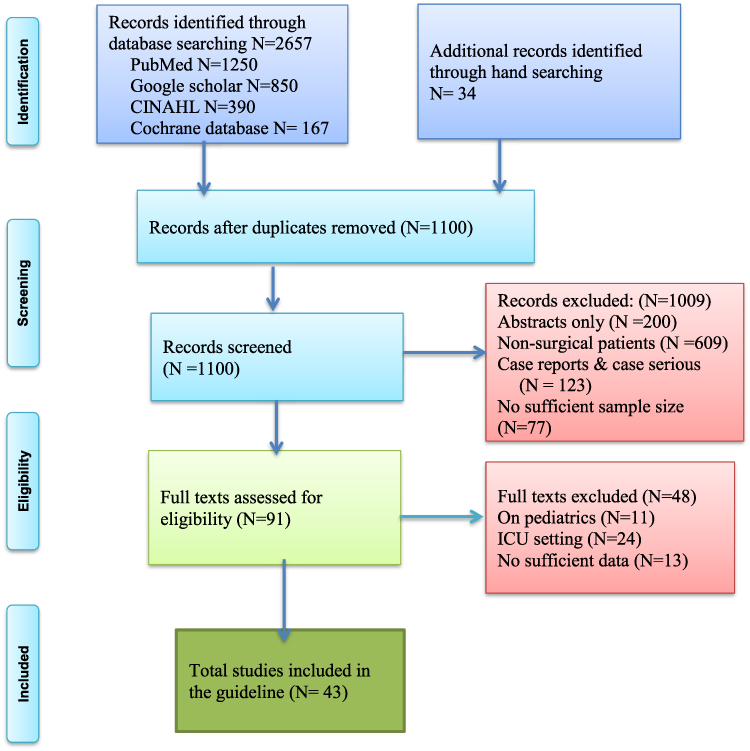 |
Figure 1 PRISMA flowchart adapted from Liberati A, Altman D, Tetzlaff J et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Journal of Clinical Epidemiology. 2009. |
Discussion
Postoperative delirium management can be divided into risk assessment, risk minimization, early diagnosis, and treatment. Up to forty percent of POD can be preventable and the most effective management of POD is prevention.10,11 Level 1a
Risk Assessment of Postoperative Delirium
Risk factors: risk identification is an important step in the prevention and management of POD. Many risk factors are associated with postoperative delirium like age, type of surgical procedure, substance abuse, premedication with diazepam, and so on. But also there is another risk factor for POD not only the mentioned condition.6,19 Level 1a
The risk factors are categorized into aggravating and predisposing conditions. The most common predisposing factors include advanced age, baseline cognitive impairment, ASA physical status ≥III, frailty, presence of multiple medical comorbidities, alcohol abuse or smoking, and sensory impairment. Aggravating factors are many drugs use, low nutritional status, poor pain management, catheter in place, blood loss, preoperative anemia, intraoperative hypotension, fluid/electrolyte disorders, duration of surgery, type of surgery.7,12,20 Level 1a
Gracie et al conducted a review that suggests the relationship b/n preoperative weakness and POD in patients undergoing surgery with the age of 65 and above with an odds ratio for POD in weakness vs non-weakness patients with an odds of 2.14.13 Level 1a
The Mini-Cog© Screening tool is used to categorize older clients at risk of POD. It is simple, free, and is effective in populations of varying ethnicity and educational level with adequate predictive power. Mini-Cog score of 4 has (PPV = 21% and NPV = 94%), score of 2 or worse has PPV 36% NPV & 90% and score of 0 or 1 has PPV 60% and NPV 88%((0–2 = high risk, 3–5 = low risk).21 Level 2b
At-risk patients: AGS stated that one or more of the following conditions are at risk for the patients for POD: 65 years and older age, any past or present cognitive dysfunction, present fracture of the hip, critically ill, and coexisting disease).10 Level 1a
High-risk patient: Any patient with a pre-existing diagnosis of delirium/dementia and/or Alzheimer’s disease. Any patient age 65 years or older that scores <2 on the Mini-Cog© preoperative screening tool.22 Level 2a
Risk-Reducing Interventions
Multicomponent Nonpharmacological Management for the Prevention of Postoperative Delirium
Multidisciplinary activity in all health-care institutions regarding the nonpharmacological multicomponent approach for at-risk geriatric clients undergoing a surgical procedure to prevent postoperative delirium (strong recommendation: moderate quality of evidence).10 Level 1a
Preventing Increasing (>6 h) Fluid Fasting Time
According to NPO guidelines clear fluid takes 2 hours for gastric emptying, but clients are usually prolonged fasting in clinical practice. A study shows that greater than 6-hour fasting fluid is an independent risk factor for POD, with an OR of 10.57 confidence interval 1.4–78.6.23 Level 2b
Avoidance of Inappropriate Medications
American Geriatric Society recommends health-care professionals have to prevent drugs that induce POD in geriatrics to avoid delirium. Medications or medication classes associated with postoperative delirium include benzodiazepines, anticholinergics, histamine2-receptor antagonists, promethazine, tricyclic antidepressants, and meperidine (strongly recommended; low quality of evidence).10 Level 1a
Dexmedetomidine During General Anesthesia
Recent review by Qi-Hong Shen et al shows that postoperative delirium incidence was low in the dexmedetomidine group than in the control group with P-values of <0.01.24 Level 1a
Another review by Zeng et al revealed that dexmedetomidine highly decreases the prevalence of postoperative delirium when compared with a control group with a P-value of = 0.001). Even though, dexmedetomidine risk of decreasing heart rate with a P-value of = 0.003. Begin bolus of 1mcg/kg over 10 minutes before induction and then initiate infusion. Maintain infusion between 0.2–0.7 mcg/kg/hr throughout the entirety of the case unless contraindicated25,26 Level 1a, 2b. Many ways were expressed to state how dexmedetomidine decreases the incidence and prevalence of POD post-surgical procedure and anesthesia. These include reducing the number of sedatives and algesia used while surgical procedures, attenuating the immune cascade and inflammatory mediators, and dexmedetomidine making a natural sleep-like sedative stress, which might support to decrease the risk of postoperative delirium.27 Level 1a
Anesthetic Techniques
General or regional anesthesia: A systematic study by Patel et al in 2018 showed that there was no difference between the type of anesthesia and POD28 Level 2a. However, another recent meta-analysis in 2021 by Abate et al POD was around 3 times in client surgery done with general anesthesia when compared to neuraxial anesthesia.6 Level 1a
Choice of general anesthetic: In cardiac surgery procedure Ketamine was minimized post-operative delirium prevalence if delivered preoperative period, an induction with 0.5mg/kg ketamine, also minimize the incidence of POD.29 Another multicenter RCT study by Avidan et al indicates there is no difference in POD prevalence b/n both ketamine and the placebo group. But postoperative hallucinations and nightmares were increased depending on ketamine doses increment with the placebo group.30 Level 1b. The study by Zhang et al suggested that inhalational anesthesia techniques can exacerbate the POD31 Level 2b. Nevertheless, other cohort studies do not show the incidence of postoperative delirium between inhalational and IV anesthesia techniques.32 Level 2b
Volatile agents or TIVA: Evidence from reviews of 28 randomized control trials show that type of anesthesia maintenance had no difference regarding the incidence of postoperative delirium evidence of a difference in incidences of POD, mortality of 30 days, and length of hospital stay. But some studies suggest that TIVA-based maintenance may decrease POD.33 Level 1a
Depth of anesthesia: Punjasawadwong et al found that Anesthesia administration guided by bispectral index may decrease the incidence of POD during the post-surgical procedure with RR of 0.7 1 in geriatric patients for the procedure of non‐neurosurgical and non‐cardiac surgical procedure34 Level 1a. Another systematic review also shows that BIS is related to a highly decreased risk of postoperative delirium and cognitive decrement with an OR of 0.51.35 Level 1a
Multimodal analgesia technique use: acute: Pain is the major issue during post-surgical procedures and a higher pain score assessment was increased postoperative delirium36 Level 2b. Publication by the USA Geriatrics Society and USA College of Surgeons recommends the use of regional anesthesia and multi-modal pain techniques as a way of minimizing opioid administration, as narcotics are associated with increases in delirium incidence (strong recommendation: moderate quality of evidence).12 Level 1a
Use of paracetamol and magnesium sulfate: It has been suggested that postoperative IV paracetamol had a decrease in postoperative delirium (10% vs 28%) placebo by directly alleviating neuroinflammation in geriatrics clients for cardiac surgery procedure37 Level 1b. In a recent clinical intraoperative administration of magnesium sulfate (30mg/kg and followed by 9mg/kg up to the completion of the surgery) reduce the incidence of postoperative agitation to 59% and 74% in the placebo group (P < 0.0001) in patients undergoing endoscopic sinus surgery.38 Level 1b
Regarding Diagnosis of Delirium
For postoperative delirium management, early diagnosis is very important. Since POD cannot be diagnosed by laboratory tests clinical and frequent observation is very important for the diagnosis of delirium.4,10 Level 1a
4AT test versus Nu-DESC: The study by Saller et shows that POD assessment of recovery with 4AT has highly sensitive and specific. 4AT sensitivity and specificity were 95.5% and 99.2%, respectively. However, Nu-DESC sensitivity and specificity were 27.3% and 99.4%, respectively. So 4AT was high sensitive than the Nu-DESC with a p-value <0.001.14 Level 2b
4AT versus CAM: Prospective diagnostic test accuracy study by Shenkin et al presented that the sensitivity and the specificity 4AT were 76% and 94% respectively. While the CAM sensitivity and specificity were 40% and 100%, respectively, and requires up to 10 min for the administrator, this study concluded that 4AT is a time-saving technique and is easily used in routine clinical activity.39 Level 2b
Another recent review by Tieges et al in 2020 also qualified the diagnostic accuracy of the 4AT with the sensitivity and specificity of 0.88 and 0.88, respectively. The 4 ‘A’s Test tool is important for postoperative delirium diagnosis with good sensitivity and brief do not need a unique technique, easy to use, and allows for the assessment of patients with drowsy and agitation condition.40 Level 1a
Postoperative Delirium Management
The first step in the management of POD is identifying and treating associated risk factors like acute pain, infection, fluid loss acid-base imbalance, and failure to urinate. The PINCH ME technique gives a clue to guide the treatment of delirium clients in the acute setting.41 Level 2a
P = pain
I = infection/intoxication
N = nutrition
C = constipation/urinary retention
H = hydration/hypoxia
M = medication
E = environmental risk factors
Non-Pharmacological Management of POD
In postoperative delirium prevention, management of POD technique requires a multidisciplinary approach regarding the non-pharmacological approach for prevention of preoperative risk factors for POD. Evidence from the Cochrane database of systematic reviews by Burton et al conclude that nonpharmacological interventions are effective for treatments of POD in the non-intensive unit care area. These strategies include reorientation, sleep enhancement, hearing and vision optimization by using hearing and vision aids, early mobilization, adequate hydration, infection prevention, pain management, and assessment.42 Level 1a
A clinical trial by Colombo R has shown that orientation can decrease the incidence of postoperative delirium by 40%. This activity may be performed by reducing changes in staff and clients transfer, periodic staff members introduction, nature of light assessment and maintaining of keeping time, the previous situation reminding regarding the previous issue, and planning for future events.43 Level 1b
Pharmacological Treatment
Currently, pharmacologically based managements of postoperative delirium options were limited, and their usage is considered depending on expected adverse effects. Drug-based treatment for POD does not consider for all clients and is used only for patients who do not respond to non-pharmacological treatments.27 Level 1a
Antipsychotics: Evidence of systematic reviews recently show that antipsychotic medication did not decrease the post-operative delirium severity, treat signs and symptoms of delirium, or did not change mortality. But adequate evidence was not concluded regarding antipsychotic drug treatment for postoperative delirium.44 Level 1a
AGS recommends patients with hyperactive delirium who show aggressive behavior and harm themself and other staff members as a second-line minimum dose of antipsychotic drugs was used to management of postoperative delirium (weak recommendation; low quality of evidence).10 Level 1a
Olanzapine VS Haloperidol for Managements of POD
The multicenter, Phase III RCT by van der Vorst et al, management of delirium by olanzapine and haloperidol show that there is no significant difference regarding the efficacy of the two drugs with P-value= 0.1845 Level 1b. Another systematic review by Schrijver EJ & de Graaf K found haloperidol and olanzapine were equally efficacious and well tolerated and can be safely used in the treatment of delirious patients, but the difference was not significant statistically (P = 0.765). Haloperidol is a highly selected drug since it is available in different formulations (oral, IM, and IV), it is affordable, and had a low risk of sedation and decreasing blood pressure complications but the risk of heart conduction problems was high. It mostly begins with low doses,4 hourly with a maximum dose of 3–5 mg daily for the elderly.46 Level 2a
Dexmedetomidine for Treatment of POD
Current evidence has suggested that dexmedetomidine is a promising agent, not only for prevention but also for the management of POD. A non RCT by Carrasco et al shows that an adequate stage of sedation was achieved by dexmedetomidine than haloperidol with the percentage of 92.7% and 59.3%, respectively, with a p-value = 0.0001. Infusion of 0.2 μg/kg/h titrated up to 0.7h μg/kg/h15 in non-intubated clients who did not respond to haloperidol treatments and it has good effectiveness and low cost. Level 1c
Benzodiazepines
Recent evidence from the Cochrane Database of Systematic Reviews by Li Y, Ma J, in 2020 does not recommend treatments of postoperative delirium with benzodiazepine because it increases the hypoactive delirium condition.47 Level 1a
A clinical practice guideline developed by AGS also recommends not using even these drugs for hyperactive delirium or agitated clients unless otherwise, the cause was secondary to alcohol withdrawal syndrome.10 Level 2b. An observation study by Levine et al conclude that there was no difference between Lorazepam and Diazepam for the management of alcohol withdrawal hyperactive delirium with a P- value = 0.534). Lorazepam was the same effect as diazepam for the treatment of alcohol withdrawal syndrome.48 Level 2b
A meta-analysis that was done by Wu et al found that a combination of haloperidol and lorazepam give the highest response rate with an odds ratio of 28.13 (CI 2.38–333.08) among Lorazepam OR 5.34 (CI0.28–101.95), Olanzapine OR 2.46 (CI 0.71–8.57), Haloperidol OR 2.37 (CI 1.04–5.43) and Dexmedetomidine OR 2.06 (CI 0.51–8.34) (Table 2).49 Level 1a
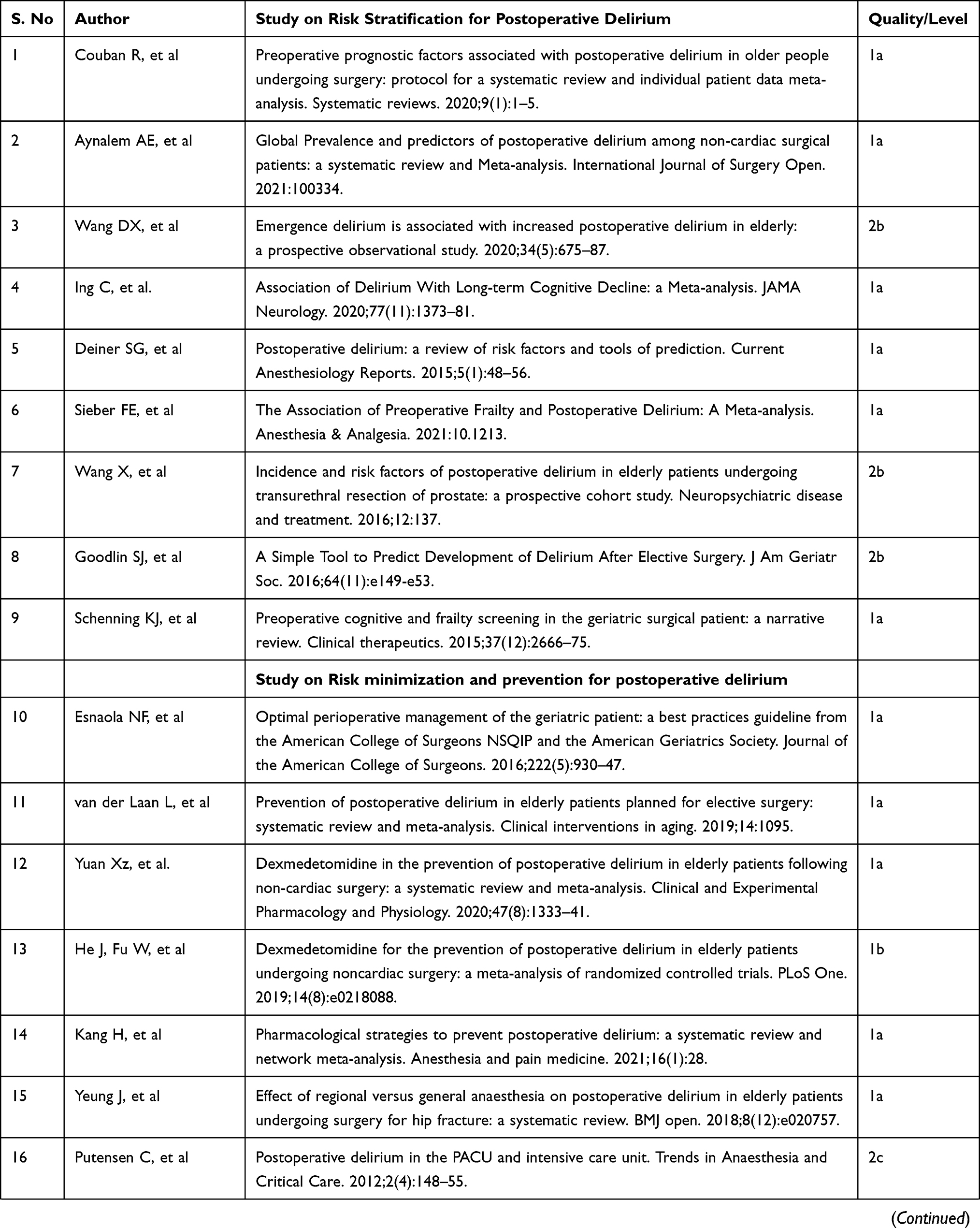 | 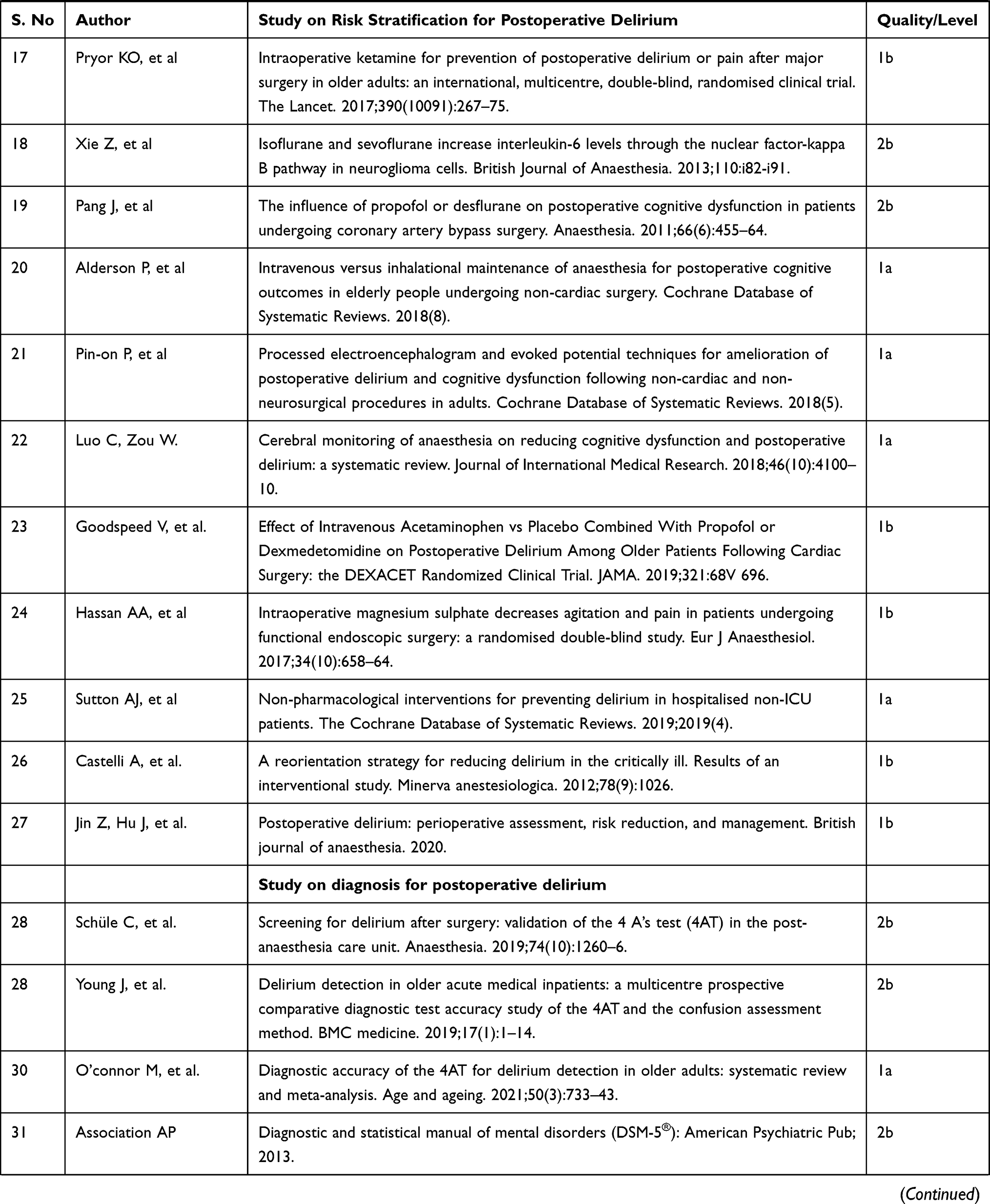 | 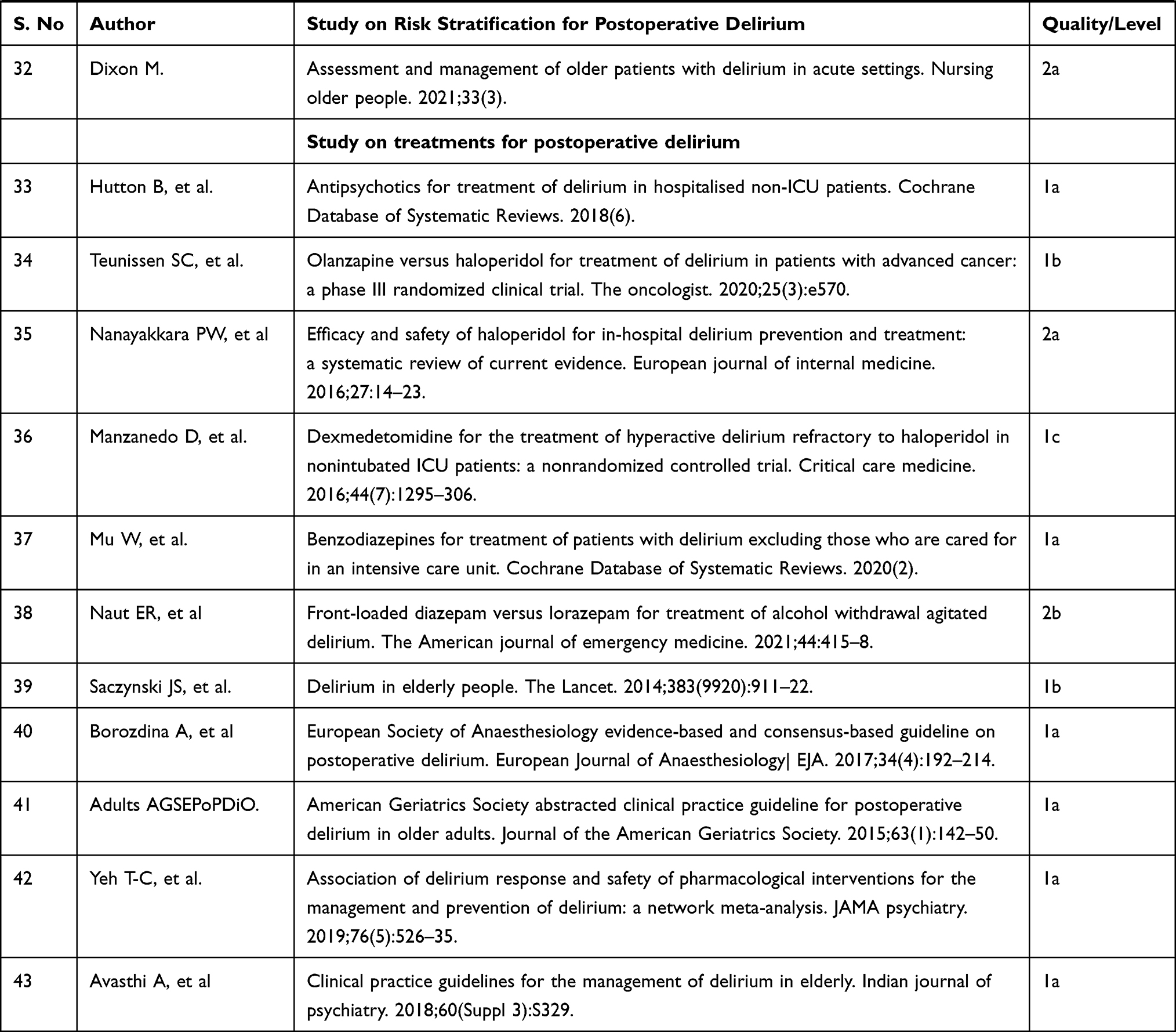 |
Table 2 The Result of the Studies Included in This Evidence-Based Guideline |
Conclusion
Management of postoperative delirium includes specifying risks that were helpful for prevention, early diagnosis, and treatment. Early diagnosis is critical to trigger focused and effective treatment. The 4 ‘A’s Test tool is important for postoperative delirium diagnosis with good sensitivity and brief does not need a unique technique to perform. In the recovery room screening for POD Patients who are at risk of postoperative delirium was recommended. The first-line management for both hyperactive and hypoactive types of delirium is the nonpharmacological approach. Even if currently limited pharmacological options, it is recommended when non-pharmacological management fails. Based on currently available evidence, Dexmedetomidine is effective for the prevention of POD and is suggested as a treatment option for POD. It has also been suggested intraoperative administration of magnesium sulfate and postoperative IV acetaminophen reduces the incidence of postoperative agitation (see Figure 2).
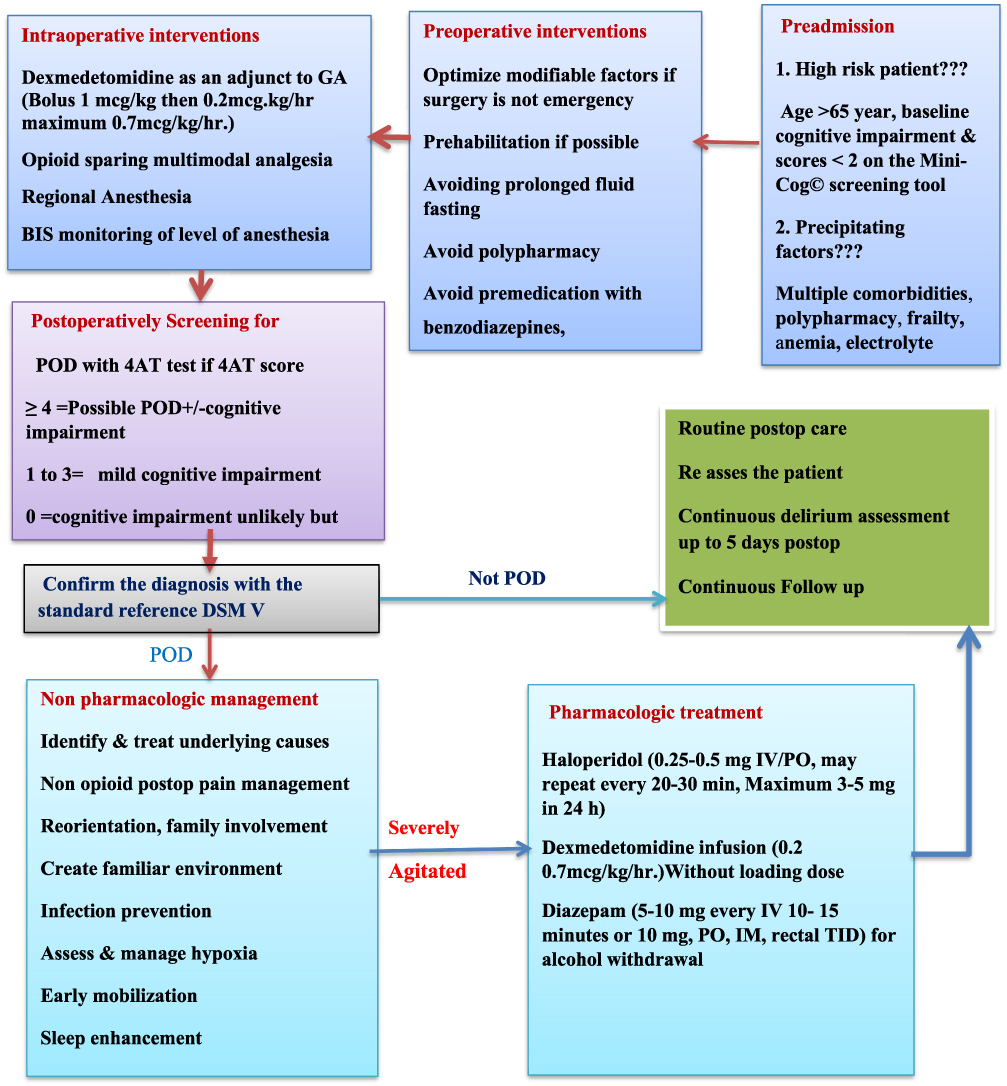 |
Figure 2 Flow chart on perioperative management of post-operative delirium. |
Abbreviations
AGS, American geriatric society; AMT4, abbreviated mental test 4; CAM, confusion assessment method; CPG, clinical practice guideline; DSM V, diagnostic and statistical manual of the mental disorders; GRADE, Grading of Recommendations Assessment, Development, and Evaluation; ICU, intensive care unite; Nu-DESC, Nursing Delirium Screening Scale; PACU, Post Anesthesia Care Unit; POD, Postoperative delirium; PRISMA, preferred reporting item for systematic review and meta-analysis; RCT, Randomized Controlled Trial.
Registration UIN
It was sent for registration.
Disclosure
The authors declare that there are no conflicts of interest.
References
1. American Psychiatric Pub. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®). American Psychiatric Pub; 2013.
2. World Health Organization. International Statistical Classification of Diseases and Related Health Problems: Tabular List. Vol. 1. World Health Organization; 2004.
3. Buchan TA, Sadeghirad B, Schmutz N, et al. Preoperative prognostic factors associated with postoperative delirium in older people undergoing surgery: protocol for a systematic review and individual patient data meta-analysis. Syst Rev. 2020;9(1):1–5. doi:10.1186/s13643-020-01518-z
4. Aldecoa C, Bettelli G, Bilotta F, et al. European Society of Anaesthesiology evidence-based and consensus-based guideline on postoperative delirium. Eur J Anaesthesiol. 2017;34(4):192–214. doi:10.1097/EJA.0000000000000594
5. Inouye SK, Westendorp RG, Saczynski JS. Delirium in elderly people. Lancet. 2014;383(9920):911–922. doi:10.1016/S0140-6736(13)60688-1
6. Abate SM, Checkole YA, Mantedafro B, et al. Global prevalence and predictors of postoperative delirium among non-cardiac surgical patients: a systematic review and meta-analysis. Int J Surg Open. 2021;32:100334. doi:10.1016/j.ijso.2021.100334
7. Janssen T, Alberts AR, Hooft L, et al. Prevention of postoperative delirium in elderly patients planned for elective surgery: systematic review and meta-analysis. Clin Interv Aging. 2019;14:1095. doi:10.2147/CIA.S201323
8. Zhang Y, He S-T, Nie B, et al. Emergence delirium is associated with increased postoperative delirium in elderly: a prospective observational study. J Anesth. 2020;34(5):675–687. doi:10.1007/s00540-020-02805-8
9. Goldberg TE, Chen C, Wang Y, et al. Association of delirium with long-term cognitive decline: a meta-analysis. JAMA Neurol. 2020;77(11):1373–1381. doi:10.1001/jamaneurol.2020.2273
10. American Geriatrics Society Expert Panel on Postoperative Delirium in Older Adults. American Geriatrics Society abstracted clinical practice guidelines for postoperative delirium in older adults. J Am Geriatr Soc. 2015;63(1):142–150. doi:10.1111/jgs.13281
11. Jin Z, Hu J, Ma D. Postoperative delirium: perioperative assessment, risk reduction, and management. Br J Anaesth. 2020;125(4):492–504. doi:10.1016/j.bja.2020.06.063
12. Mohanty S, Rosenthal RA, Russell MM, et al. Optimal perioperative management of the geriatric patient: a best practices guideline from the American College of Surgeons NSQIP and the American Geriatrics Society. J Am Coll Surg. 2016;222(5):930–947. doi:10.1016/j.jamcollsurg.2015.12.026
13. Gracie TJ, Caufield-Noll C, Wang NY, Sieber FE. The association of preoperative frailty and postoperative delirium: a meta-analysis. Anesth Analg. 2021;133(2):314–323.
14. Saller T, MacLullich AMJ, Schäfer ST, et al. Screening for delirium after surgery: validation of the 4 A’s test (4AT) in the post-anesthesia care unit. Anaesthesia. 2019;74(10):1260–1266. doi:10.1111/anae.14682
15. Carrasco G, Baeza N, Cabré L, et al. Dexmedetomidine for the treatment of hyperactive delirium refractory to haloperidol in non-intubated ICU patients: a nonrandomized controlled trial. Crit Care Med. 2016;44(7):1295–1306. doi:10.1097/CCM.0000000000001622
16. Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomized or non-randomized studies of healthcare interventions, or both. BMJ. 2017;358:j4008.
17. Long HA, French DP, Brooks JM. Optimising the value of the critical appraisal skills program (CASP) tool for quality appraisal in qualitative evidence synthesis. Res Methods Med Health Sci. 2020;1(1):31–42. doi:10.1177/2632084320947559
18. Phillips B. Oxford center for evidence-based medicine-levels of evidence (March 2009); 2009.
19. Grover S, Avasthi A. Clinical practice guidelines for the management of delirium in elderly. Indian J Psychiatry. 2018;60(Suppl 3):S329. doi:10.4103/0019-5545.224473
20. Schenning KJ, Deiner SG. Postoperative delirium: a review of risk factors and tools of prediction. Curr Anesthesiol Rep. 2015;5(1):48–56. doi:10.1007/s40140-014-0086-1
21. Dworkin A, Lee DSH, An AR, et al. A simple tool to predict development of delirium after elective surgery. J Am Geriatr Soc. 2016;64(11):e149–e153. doi:10.1111/jgs.14428
22. Axley MS, Schenning KJ. Preoperative cognitive and frailty screening in the geriatric surgical patient: a narrative review. Clin Ther. 2015;37(12):2666–2675. doi:10.1016/j.clinthera.2015.10.022
23. Radtke FM, Franck M, MacGuill M, et al. Duration of fluid fasting and choice of analgesic are modifiable factors for early postoperative delirium. Eur J Anaesthesiol. 2010;27(5):411–416. doi:10.1097/EJA.0b013e3283335cee
24. Shen QH, Li H-F, Zhou X-Y, et al. Dexmedetomidine in the prevention of postoperative delirium in elderly patients following non‐cardiac surgery: a systematic review and meta‐analysis. Clin Exp Pharmacol Physiol. 2020;47(8):1333–1341. doi:10.1111/1440-1681.13312
25. Zeng H, Li Z, He J, et al. Dexmedetomidine for the prevention of postoperative delirium in elderly patients undergoing noncardiac surgery: a meta-analysis of randomized controlled trials. PLoS One. 2019;14(8):e0218088. doi:10.1371/journal.pone.0218088
26. Lee C, Lee CH, Lee G, et al. The effect of the timing and dose of dexmedetomidine on postoperative delirium in elderly patients after laparoscopic major non-cardiac surgery: a double-blind randomized controlled study. J Clin Anesth. 2018;47:27–32. doi:10.1016/j.jclinane.2018.03.007
27. Lee JM, Cho YJ, Ahn EJ, et al. Pharmacological strategies to prevent postoperative delirium: a systematic review and network meta-analysis. Anesth Pain Med. 2021;16(1):28. doi:10.17085/apm.20079
28. Patel V, Champaneria R, Dretzke J, et al. Effect of regional versus general anesthesia on postoperative delirium in elderly patients undergoing surgery for hip fracture: a systematic review. BMJ Open. 2018;8(12):e020757. doi:10.1136/bmjopen-2017-020757
29. Theuerkauf N, Guenther U, Putensen C. Postoperative delirium in the PACU and intensive care unit. Trends Anaesth Crit Care. 2012;2(4):148–155. doi:10.1016/j.tacc.2012.03.002
30. Avidan MS, Maybrier HR, Abdallah AB, et al. Intraoperative ketamine for prevention of postoperative delirium or pain after major surgery in older adults: an international, multicentre, double-blind, randomized clinical trial. Lancet. 2017;390(10091):267–275. doi:10.1016/S0140-6736(17)31467-8
31. Zhang L, Zhang J, Yang L, et al. Isoflurane, and sevoflurane increase interleukin-6 levels through the nuclear factor-kappa B pathway in neuroglioma cells. Br J Anaesth. 2013;110:i82–i91. doi:10.1093/bja/aet115
32. Royse CF, Andrews DT, Newman SN, et al. The influence of propofol or desflurane on postoperative cognitive dysfunction in patients undergoing coronary artery bypass surgery. Anaesthesia. 2011;66(6):455–464. doi:10.1111/j.1365-2044.2011.06704.x
33. Miller D, Lewis SR, Pritchard MW, et al. Intravenous versus inhalational maintenance of anesthesia for postoperative cognitive outcomes in elderly people undergoing non‐cardiac surgery. Cochrane Database Syst Rev. 2018;8:CD012317.
34. Punjasawadwong Y, Chau‐in W, Laopaiboon M, et al. Processed electroencephalogram and evoked potential techniques for the amelioration of postoperative delirium and cognitive dysfunction following non‐cardiac and non‐neurosurgical procedures in adults. Cochrane Database Syst Rev. 2018;5:CD011283.
35. Luo C, Zou W. Cerebral monitoring of anesthesia on reducing cognitive dysfunction and postoperative delirium: a systematic review. J Int Med Res. 2018;46(10):4100–4110. doi:10.1177/0300060518786406
36. Xue P, Wu Z, Wang K, et al. Incidence and risk factors of postoperative delirium in elderly patients undergoing transurethral resection of the prostate: a prospective cohort study. Neuropsychiatr Dis Treat. 2016;12:137. doi:10.2147/NDT.S97249
37. Subramaniam B, Shankar P, Shaefi S, et al. Effect of intravenous acetaminophen vs placebo combined with propofol or dexmedetomidine on postoperative delirium among older patients following cardiac surgery: the DEXACET randomized clinical trial. JAMA. 2019;321:68V 696. doi:10.1001/jama.2019.0234
38. Elsersy HE, Metyas MC, Elfeky HA, et al. Intraoperative magnesium sulfate decreases agitation and pain in patients undergoing functional endoscopic surgery: a randomized double-blind study. Eur J Anaesthesiol. 2017;34(10):658–664. doi:10.1097/EJA.0000000000000642
39. Shenkin SD, Fox C, Godfrey M, et al. Delirium detection in older acute medical inpatients: a multicentre prospective comparative diagnostic test accuracy study of the 4AT and the confusion assessment method. BMC Med. 2019;17(1):1–14. doi:10.1186/s12916-019-1367-9
40. Tieges Z, Maclullich AMJ, Anand A, et al. Diagnostic accuracy of the 4AT for delirium detection in older adults: systematic review and meta-analysis. Age Ageing. 2021;50(3):733–743. doi:10.1093/ageing/afaa224
41. Dixon M. Assessment, and management of older patients with delirium in acute settings. Nurs Older People. 2021;33(3):35–42.
42. Burton JK, Harrison JK, Clegg A, et al. Non‐pharmacological interventions for preventing delirium in hospitalized non‐ICU patients. Cochrane Database Syst Rev. 2019;2019(4). doi:10.1002/14651858.CD013307
43. Colombo R, Corona A, Praga F, et al. A reorientation strategy for reducing delirium in the critically ill. Results of an interventional study. Minerva Anestesiol. 2012;78(9):1026.
44. Burry L, Mehta S, Perreault MM, et al. Antipsychotics for treatment of delirium in hospitalized non‐ICU patients. Cochrane Database Syst Rev. 2018;2018(6). doi:10.1002/14651858.CD005594.pub3
45. van der Vorst MJ, Neefjes ECW, Boddaert MSA, et al. Olanzapine versus haloperidol for treatment of delirium in patients with advanced cancer: a phase III randomized clinical trial. oncologist. 2020;25(3):e570. doi:10.1634/theoncologist.2019-0470
46. Schrijver EJ, de Graaf K, de Vries OJ, et al. Efficacy and safety of haloperidol for in-hospital delirium prevention and treatment: a systematic review of current evidence. Eur J Intern Med. 2016;27:14–23. doi:10.1016/j.ejim.2015.10.012
47. Li Y, Ma J, Jin Y, et al. Benzodiazepines for treatment of patients with delirium excluding those who are cared for in an intensive care unit. Cochrane Database Syst Rev. 2020;2020(2). doi:10.1002/14651858.CD012670.pub2
48. Levine AR, Thanikonda V, Mueller J, et al. Front-loaded diazepam versus lorazepam for treatment of alcohol withdrawal agitated delirium. Am J Emerg Med. 2021;44:415–418. doi:10.1016/j.ajem.2020.04.095
49. Wu Y-C, Tseng P-T, Tu Y-K, et al. Association of delirium response and safety of pharmacological interventions for the management and prevention of delirium: a network meta-analysis. JAMA Psychiatry. 2019;76(5):526–535. doi:10.1001/jamapsychiatry.2018.4365
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.