")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 13
Evaluation of the Sociodemographic, Behavioral and Clinical Influences on Complete Antiretroviral Therapy Adherence Among HIV-Infected Adults Receiving Medical Care in Houston, Texas
Authors Sok P, Mgbere O, Pompeii L, Essien EJ
Received 30 January 2021
Accepted for publication 10 April 2021
Published 18 May 2021 Volume 2021:13 Pages 539—555
DOI https://doi.org/10.2147/HIV.S303791
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Professor Bassel Sawaya
Pagna Sok,1,2 Osaro Mgbere,3,4 Lisa Pompeii,1,2 Ekere James Essien1,4,5
1The University of Texas School of Public Health, Texas Medical Center, Houston, TX, USA; 2Department of Pediatrics, Baylor College of Medicine, Texas Medical Center, Houston, TX, USA; 3Disease Prevention and Control Division, Houston Health Department, Houston, TX, USA; 4Institute of Community Health, University of Houston, Texas Medical Center, Houston, TX, USA; 5Department of Pharmaceutical Health Outcomes and Policy, University of Houston College of Pharmacy, Houston, TX, USA
Correspondence: Osaro Mgbere
Disease Prevention & Control Division, Houston Health Department, 8000 North Stadium Drive, Houston, TX, 77054-1823, USA
Tel +1-832-393-4593
Email [email protected]
Introduction: Few studies have estimated complete antiretroviral therapy (ART) adherence following HIV infection since the advent of the new ART guidelines in 2012. This study determined the prevalence and influence of sociodemographic, behavioral, and clinical factors on complete ART adherence among people living with HIV (PLWH) receiving medical care in Houston/Harris County, Texas.
Methods: Data from the Houston Medical Monitoring Project survey collected from 2009 to 2014 among 1073 participants were used in this study. The primary outcome evaluated was combined adherence, defined as complete, partial, and incomplete combined adherence based on three ART adherence types—dose, schedule, and instruction adherence. The duration living since initial HIV diagnosis was classified as < 5, 5– 10 and > 10 years. Rao–Scott Chi-square test and multivariable proportional-odds cumulative logit regression models were employed to identify the sociodemographic, behavioral, and clinical characteristics of complete combined adherence among the three groups of PLWH living with HIV infection.
Results: More than one-half (54.4%) of PLWH had complete, 37.4% had partial, and 8.3% had incomplete combined adherence. Among these PLWH, 52.2% had been infected with HIV for > 10 years, and 26.5% and 21.4% were infected for < 5 years and 5– 10 years, respectively. PLWH who were diagnosed < 5 and 5– 10 years were two times (aOR=1.71, 95% CI=1.13– 2.57; aOR=1.69, 95% CI=1.10– 2.59; respectively) more likely to experience complete combined adherence than those with > 10 years of infection. Multiple sociodemographic, behavioral, and clinical characteristics were significantly associated with complete adherence and varied by the duration of HIV infection.
Conclusion: Measures of adherence should include all adherence types (dose, schedule, instruction), as utilizing a single adherence type will overestimate adherence level in PLWH receiving medical care. Intervention efforts to maintain adherence should target recently infected PLWH, while those aimed at improving adherence should focus on longer infected PLWH.
Keywords: HIV, people living with HIV, antiretroviral therapy, medication adherence, Medical Monitoring Project
Introduction
With the introduction of antiretroviral therapy (ART), human immunodeficiency virus (HIV) infection has transitioned from an ailment that once required urgent treatment to a chronic disease manageable with long-term medical care.1–5 ART optimizes immunity and prolong life expectancy by increasing CD4 T-cells count and suppressing viral load.6–9 Thus, receiving ART is critical in preventing Acquired Immune Deficiency Syndrome (AIDS) development for people living with HIV (PLWH). However, achieving virologic suppression and preventing AIDS infection depend on high ART adherence levels and uninterrupted treatments. In effect, ART adherence is an important indicator of HIV treatment effectiveness.
Despite the benefits of ART on HIV treatment, high or complete ART adherence levels among PLWH are generally low.10–13 Moreover, ART adherence has been observed to fluctuate across time hindering HIV treatment success.11,14 Patients’ aptness to adhere to ART can be influenced by numerous factors, which can be classified broadly as patient-related, treatment-related, and healthcare system-related factors.15–17 For instance, studies on aging PLWH indicated higher adherence level among older PLWH compared to their younger cohorts.18–21 Better adherence among older PLWH can be attributed to patients’ experience with long-term medication usage and their knowledge on optimal adherence effectiveness.20,22,23 Conversely, aging PLWH can encounter unique barriers to adherence and age-related comorbidities such as diabetes and cardiovascular disease that negatively affect treatment, which are not generally common in younger PLWH.20,21
Clinical outcomes among PLWH are more likely to be predicted by measuring multiple dimensions of medication-taking behaviors than by measuring missed doses.24 Failure to inquire about adherence to medication schedule and instruction may lead to inaccurate estimates of patients’ adherence level.13 Additionally, ART adherence risks have been described to be dynamic and fluctuate after ART initiation.23,25–29 Despite these findings, few studies have attempted to estimate complete ART adherence and any associated predictors across time following HIV infection since the advent of the new ART guidelines in 2012.30 Therefore, this study aimed to determine the prevalence and influence of sociodemographic, behavioral, and clinical factors on complete ART adherence among PLWH receiving medical care in Houston/Harris County, Texas.
Methods
Study Population and Data Collection
The Houston Medical Monitoring Project or HMMP is part of a nationwide (the Medical Monitoring Project or MMP) ongoing cross-sectional HIV surveillance, designed to produce representative estimates of behavioral and clinical characteristics of PLWH receiving outpatient medical care in the United States (US) and Puerto Rico.22,31 Details about MMP study population, sampling process, and questionnaire can be found elsewhere.22,32,33 In brief, MMP involves a three-stage probability sampling method that samples PLWH 18 years or older who had received at least one medical care treatment from providers between January and April of every calendar year since 2005. All information concerning the sociodemographic and behavioral characteristics of participants were self-reported via face-to-face or telephone interviews. Clinical information was abstracted from participants’ medical records by trained MMP staff at participating medical facilities.
The current study was based on data collected from Houston/Harris County, Texas, between 2009 and 2014 and comprised of reported 1073 PLWH (weighted N=10,274). Participants who 1) were at least 18 years old at the time of interview; 2) received antiretroviral medications at the time of the interview; and 3) received at least one medical treatment at HMMP participating facilities were included in subsequent analyses.
Analytical Measures
Dependent Measures: ART Dose, Instruction, Schedule Adherence, and Combined Adherence
The MMP questionnaire included questions inquiring about ART dose, instruction, and schedule completion within the past 3 days prior to the interview.25,33 For dose adherence, participants were asked to recall the number of times they missed taking a dose or set of pills/spoonful’s/injections of their prescribed ART medication. For instruction adherence, participants were asked if their ART medications had special instructions, such as take with food, take on an empty stomach, or take with plenty of fluids, with a follow-up question ascertaining whether they followed those instructions. For schedule adherence, participants were asked if their ART medications needed to be taken on a schedule such as 2 times a day or every 8 hours, and whether they were adherent to the specific schedule.
A complete medication adherence was defined as missing none of the prescribed dose, instruction, or scheduled ART requirements, respectively. A combined adherence index, accounting for dose, instruction and schedule adherence, was defined as complete, partial, or incomplete. Complete combined adherence indicated PLWH who had complete dose, instruction, and schedule adherence, while PLWH had partial combined adherence if they had one or two adherences to ART dose, instruction, or schedule. Lastly, incomplete combined adherence characterized PLWH without adherence to all three ART requirements.
Independent Measures: Duration of HIV Infection, Sociodemographic, Behavioral, and Clinical Characteristics
To numerate the duration of HIV infection, participants reported the month and year they had received their first positive HIV test. Positive HIV diagnosis date was also confirmed by HMMP staffs through medical record abstraction. The duration of HIV infection was then enumerated between the first positive HIV test and interview date and subsequently categorized as <5, 5–10, and >10 years. This categorization is consistent with reports generated by the Center for Disease Control and Prevention (CDC) and other published literatures allowing for comparability across studies utilizing MMP data.13,31 Additionally, factors of adherence were identified and characterized as sociodemographic, behavioral, or clinical characteristics.18,20,21,34 All identified factors were reported in the past 12 months prior to the interview unless otherwise noted and are described below.
Sixteen sociodemographic factors were identified and evaluated, which included 1) age at HIV diagnosis; 2) gender (male, female, transgender); 3) level of education (less than, high school or more); 4) race/ethnicity (White, Black, Hispanic, Other), 5) born in foreign country (yes, no); 6) English-speaking fluency (yes, no); 7) homelessness (yes, no); 8) incarceration (yes, no); 9) insurance coverage (continuous, lapsed, no coverage); 10) annual income ($0–20,000, $20,000–39,999, $40,000 or more); 11) smoking status (never, former, current); 12) any drug use (yes, no); 13) poverty level (above/at, below poverty level); 14) heavy drinking (yes, no); 15) depression (major, other, no depression); and 16) disability (yes, no).
Poverty level was determined using the midpoint of the income range and the number of dependents according to the US Department of Health and Human Services poverty guidelines between 2009 and 2014.35 Heavy drinking (2 drinks per day or 14 drinks per week for male; 1 drink per day or 7 drinks per week for female) was based on the CDC standard definition of heavy drinking.35 Depression classification was based on the Kroenke and Spitzer algorithm that classified major, other, or no depression on two evaluations: 1) feeling little interest or pleasure in doing things and 2) feeling down, depressed, or hopeless.27,35 Respondents described how often they experienced these emotions, ie, not at all, several times per month, more than half the month, or nearly every day. Major depression applied to participants that responded more than half of the days or nearly every day to either category, and other depression to those who responded more than half of the days or nearly every day to either category. Otherwise, participants were considered as having no depression. Additionally, HMMP evaluated PLWH with a disability (yes) if they experienced either: 1) deafness or serious difficulty hearing; 2) blindness or serious difficulty seeing, even when wearing glasses; 3) serious difficulty concentrating, remembering, or making decisions because of physical, mental, or emotional condition; 4) serious difficulty walking or climbing stairs; 5) difficulty dressing or bathing; or 6) difficulty doing errands such as visiting a doctor’s office or shopping because of physical, mental, or emotional condition.
Nine behavioral predictors evaluated included: 1) number of visits to HIV doctor/other care provider; 2) care received in the past 6 months (care, no care); 3) have unmet needs (yes, no); 4) ability to take all or most medications as directed (sure, not sure); 5) have friends or family members help taking medications (a lot, somewhat, not at all); 6) belief HIV will become resistant to medications if not taken as directed (very sure, somewhat sure, not at all sure); 7) any previous free condoms received (yes, no); 8) any HIV education supports received (yes, no); and 9) experienced any stigma (yes, no).
Unmet needs were evaluated based on 19 services (yes, no). Participants had unmet needs (yes) if they did not receive at least one of the required services. Participants were designated as having received HIV education supports (yes) if they: 1) had talked to counselors about HIV prevention; 2) had one-to-one conversations with health care workers about ways to protect themselves or their partners from getting HIV or other STDs; or 3) participated in an organized session involving a small group of people to discuss ways to protect themselves or their partners from getting HIV or other STDs. Participants experienced stigma (yes) if they: 1) had difficulty telling people about HIV infection; 2) felt dirty, guilty, shameful, or worthless because they were HIV positive; or 3) hid their HIV status from others.
Ten clinical predictors were evaluated including: 1) lowest non-missing CD4 count (<200, ≥200 cell/mm3); 2) viral loads (<200, ≥200 viral copies/mL); 3) previous hepatitis vaccine (yes, no); 4) previous skin (purified protein derivative or PPD) test or blood test for tuberculosis (TB) (yes, no); 5) previous vaccine for Human papillomavirus (HPV) (yes, no); 6) previous clinical AIDS (yes, no); 7) previous Gonorrhea, Chlamydia, and Syphilis screening (yes, no); 8) number of CD4/viral load tests (<3, ≥3 tests); 9) number of visits to emergency room (ER) or urgent care clinic for HIV care; and 10) number of times admitted to a hospital because of HIV-related illness.
Statistical Analysis
Proportions and percentages of ART medication dose, schedule, instruction, and combined adherence were evaluated for all PLWH and stratified by the duration of HIV infection. Tests for bivariate associations between the independent and dependent variables were conducted using the Rao–Scott χ2 test. Subsequently, we applied proportional-odds cumulative logit regression model analysis with backward stepwise elimination technique to compare the odds of complete combined adherence events to the partial and incomplete combined adherence non-events. Only independent variables that met the statistical threshold of p≤0.20 in the bivariate analyses were included in the multivariable logistic regression models. The final models were selected and compared using Akaike’s Information Criterion (AIC), applying Burnham and Anderson rule of thumb for interpreting AIC Scores.36,37 All results reported were based on weighted data, and two-tail tests with p<0.05 was used as the significant level threshold. Data were weighted based on the probability of selection at each sampling stage to provide for local estimates and were adjusted for predictors of nonresponse bias especially in sensitive categories such as facility size, race/ethnicity, and group composition.22,31,32 All data management and statistical analyses were performed using SAS 9.4 (SAS Institute, Cary, NC, USA).
Human Subjects Protection
MMP was determined by the National Center for HIV, Viral Hepatitis, STD and TB Prevention’s Office of the Associate Director for Science at the CDC to be a non-research, public health surveillance activity used for disease control program or policy purposes. All data collection was Health Insurance Portability and Accountability Act compliant. However, for the purpose of the current study, study documents were submitted to The University of Texas Health Science Center Committee for Protection of Human Subjects and the Houston Health Department Investigative Review Committee for review. The study received exempt status approvals as the data used had no identifiable information traceable to the surveyed participants.
Results
Study Sample Characteristics
As indicated in Table 1, the study population was mostly male (71.0%) of 40 years of age or older (69.6%). Fewer than half identified as Black (47.7%) while 27.4% and 22.9% were Hispanic and White, respectively. More than three-quarters (77.8%) of PLWH had at least a high school education. The majority of PLWH had either continuous or lapsed insurance coverage (62.4%), were living at or below the poverty line (51.4%), and had an average annual income less than $40,000 (90.3%). Most PLWH were not homeless (92.2%), not incarcerated (94.4%), not heavy drinkers (95.1%), not drug users (85.5%), or were never/former smokers (68.7%). While 80.9% of PLWH had no depression, up to 45.0% had experienced some disabilities.
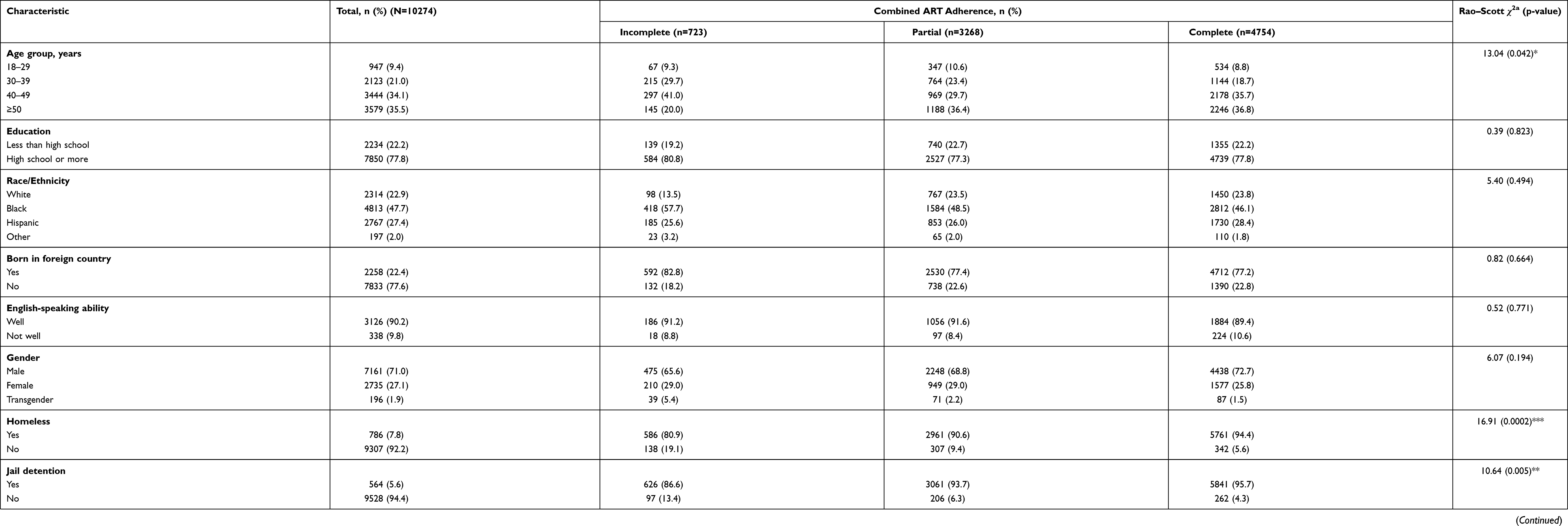 |
Table 1 Sociodemographic Characteristics by Combined ART Adherence Among PLWH Receiving Medical Care in Houston/Harris County, Texas |
The behavioral characteristics of the study population are outlined in Table 2. The majority of PLWH had not received medical care (94.6%) in the past 6 months and had an average of five visits to an HIV or healthcare provider within the past 12 months. Half of the study sample had at least one unmet need (49.2%) but only a few (18.7%) experienced HIV-related stigmas in the past 12 months. Although most PLWH (95.2%) were sure of taking their medications as directed, almost half (44.8%) indicated that they needed assistance remembering to take those medications. Clinically (Table 3), most PLWH had never experienced clinical AIDS (73.9%) and had lowest non-missing CD4 counts of ≥200 cell/mm3 (82.8%). While the majority of PLWH had hepatitis vaccination (70.2%) and skin or blood testing for TB (92.5%), only a few had HPV vaccination (11.3%) or Gonorrhea, Chlamydia and Syphilis screening (17.0%).
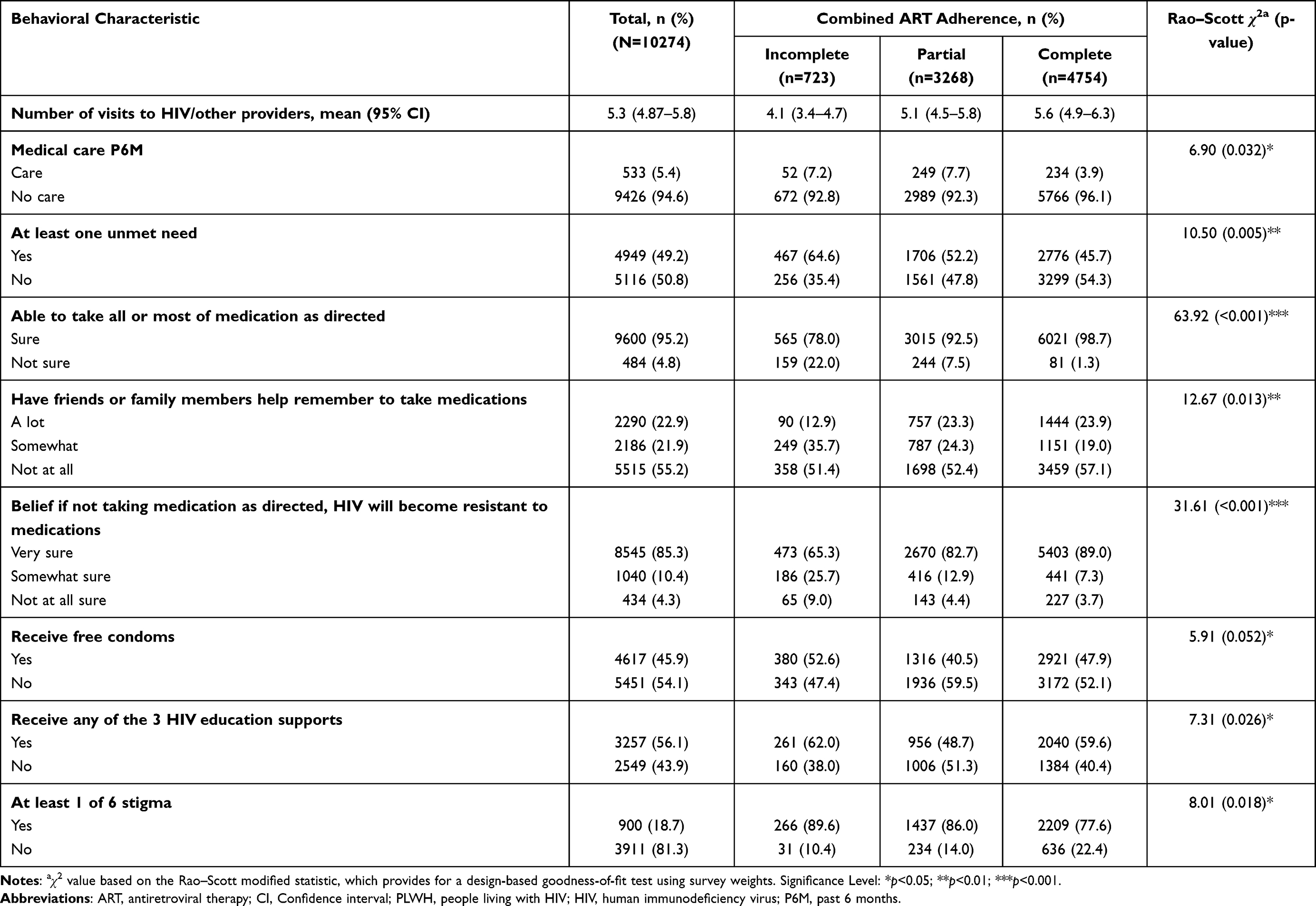 |
Table 2 Behavioral Characteristics by Combined ART Adherence Among PLWH Receiving Medical Care in Houston/Harris County, Texas |
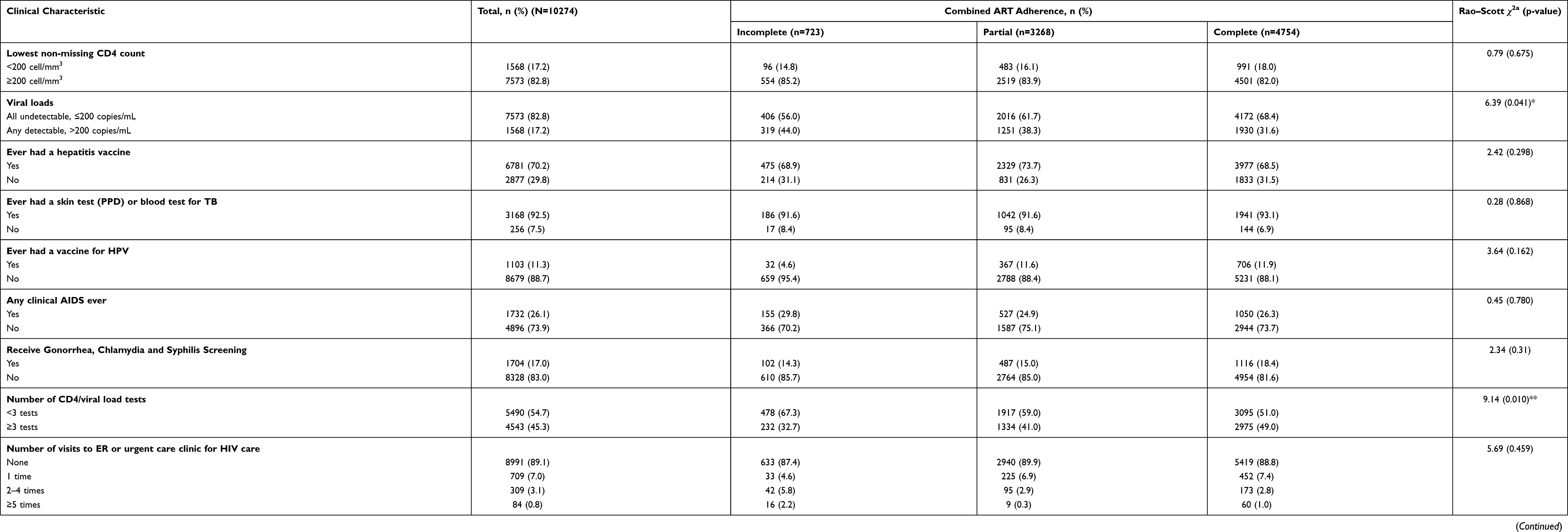 |
Table 3 Clinical Characteristics by Combined ART Adherence Among PLWH Receiving Medical Care in Houston/Harris County, Texas |
ART Adherence by Duration of HIV Infection
About half of PLWH (52.2%) had been infected with HIV for >10 years, and 26.5% and 21.4% of PLWH were infected for <5 years and 5–10 years, respectively. ART adherence to medication dose, schedule, and instruction were high at 85%, 71.2%, and 73.3%, respectively (Table 4). However, only medication schedule adherence varied significantly by duration of HIV infection (χ2=10.49, p=0.005). When evaluating the overall combined ART adherence, 54.4% of PLWH had complete combined adherence, 37.4% had partial combined adherence, and 8.3% had incomplete combined adherence. Combined ART adherence varied significantly by duration of infection (χ2=11.15, p=0.022), with 56.8%, 59.0%, and 51.1% reported for PLWH infected for <5, 5–10, and >10 years, respectively.
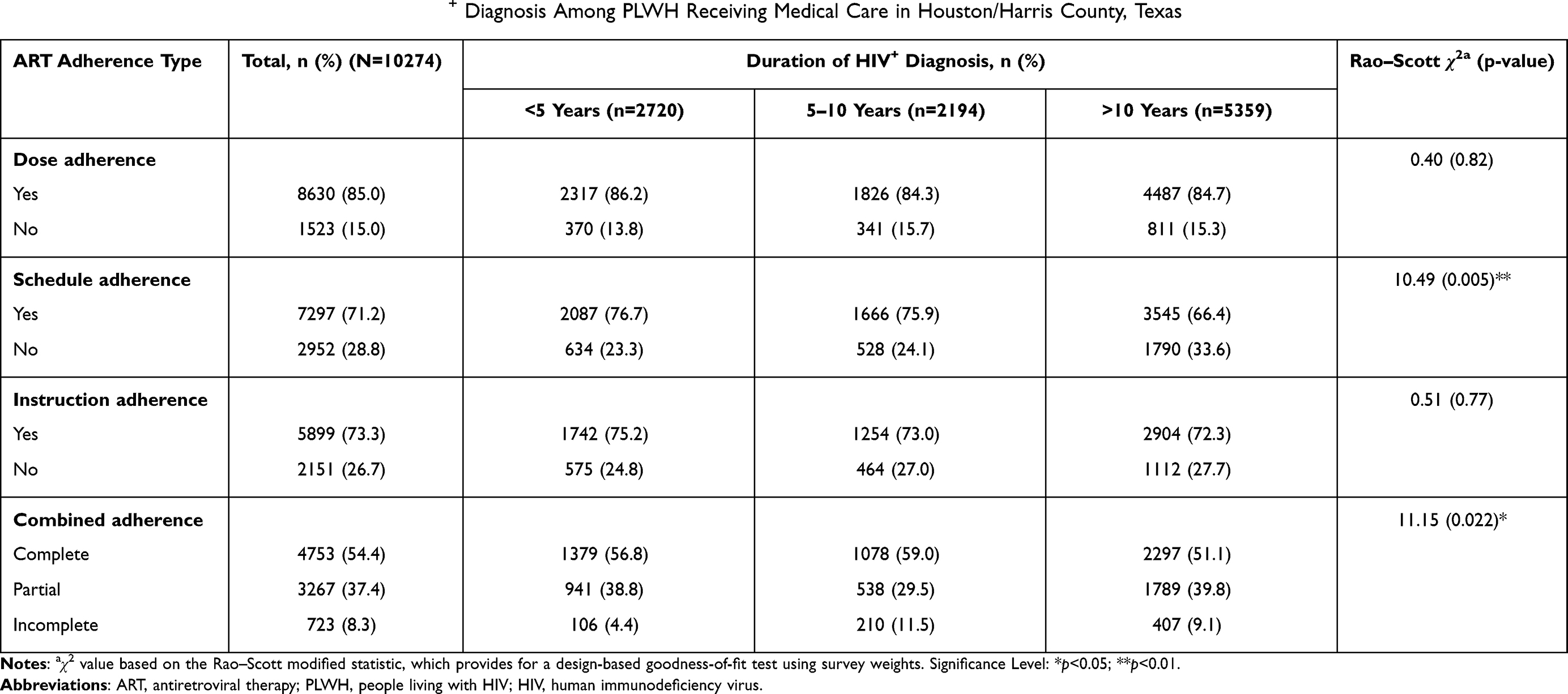 |
Table 4 ART Adherence Types by Duration of HIV+ Diagnosis Among PLWH Receiving Medical Care in Houston/Harris County, Texas |
Characteristics of Complete Combined Adherence
Among all PLWH (Table 5), those with HIV infection for 5–10 years were two times (aOR=1.71, 95% CI=1.13–2.57, p<0.05) more likely than those infected with HIV for >10 years to be completely adherent to all three medication assessment forms (dose, schedule, and instruction). PLWH infected for <5 years with HIV also had similar odds (aOR=1.69, 95% CI=1.10–2.59, p<0.05) of complete combined adherence than PLWH infected for >10 years. Characteristics that were favorable to complete combined adherence included age ≥50 years old (aOR=1.95, 95% CI=1.07–3.58, p<0.05), no injection or non-injection drug use (aOR=1.67, 95% CI=1.11–2.52, p<0.05), high self-efficacy in taking all or most medication as directed (aOR=5.74, 95% CI=2.90–11.35, p<0.001), and receiving ≥3 CD4/viral load tests (aOR=1.44, 95% CI=1.08–1.91, p<0.05).
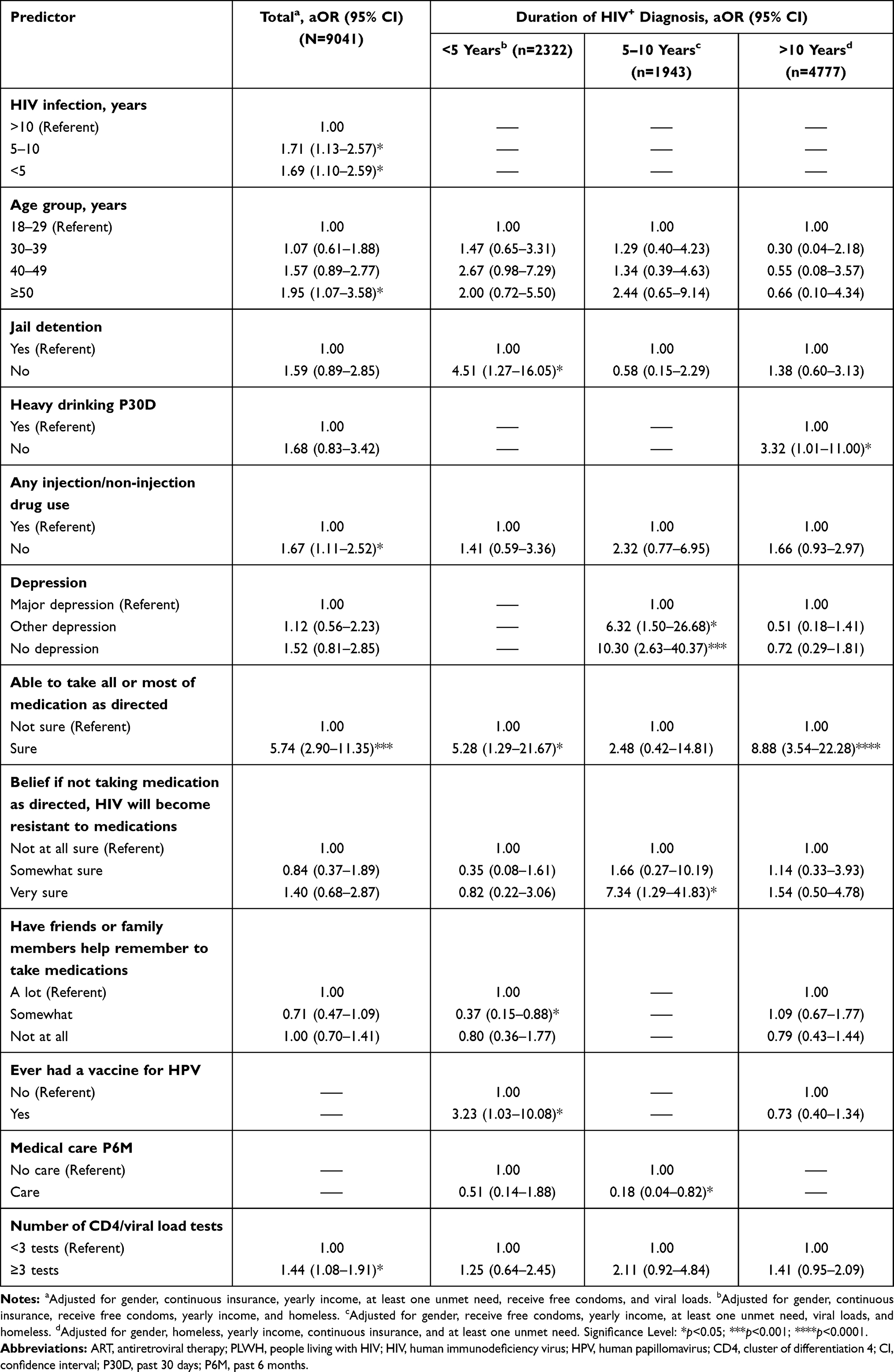 |
Table 5 Adjusted Odds Ratios (aOR) of Complete Combined ART Adherence Among PLWH Receiving Medical Care in Houston/Harris County, Texas |
Characteristics of complete combined ART adherence were found to differ by the duration of HIV infection. For PLWH with <5 years of HIV infection, predictors significantly associated with complete combined ART adherence were no incarceration (aOR=4.51, 95% CI=1.27–16.05, p<0.05), strong self-efficacy in taking all or most medication as directed (aOR=5.28, 95% CI=1.29–21.67, p<0.05), and history of HPV vaccinations (aOR=3.23, 95% CI=1.03–10.08, p<0.05). For PLWH with 5–10 years of HIV infection, those with no depression (aOR=10.30, 95% CI=2.63–40.37, p<0.001) and those with strong personal conviction (beliefs and morals) in HIV resistance to the medication (aOR=7.34, 95% CI=1.29–41.83, p<0.05) were more likely to experience complete combined ART adherence. However, in this sub-population, having received medical care within the past 6 months was negatively associated (aOR=0.18, 95% CI=0.04–0.82, p<0.05) with complete combined ART adherence. By comparison, no heavy drinking (aOR=3.32, 95% CI=1.01–10.00, p<0.05) in the past 30 days and high confidence in taking required medication as directed (aOR=8.88, 95% CI=3.54–22.28, p<0.0001) were the only two characteristics associated with complete combined ART adherence among PLWH with >10 years of HIV infection.
Discussion
For PLWH, maintaining viral load suppression, and preventing AIDS prognosis, and achieving positive health outcomes are contingent on high and continual ART adherence.38 This study reported high adherence to complete medication dose (85.0%) among PLWH in Houston/Harris county compared to adherence to complete medication schedule (71.2%) and instruction (73.3%) adherence. However, when adherence to medication dose, schedule, and instruction were evaluated as a single combined adherence index, only one in two (54.4%) PLWH was completely adherent. Complete combined ART adherence was significantly varied by duration of HIV infection where recently infected PLWH, ie, <5 and 5–10 years were more likely to experience complete adherence. Characteristics of complete combined adherence also differed across duration of HIV infection, though these characteristics spanned across multiple sociodemographic, behavioral, and clinical factors.
Antiretroviral regimen complexity and pill burden, i.e., once daily vs twice daily dosing, single vs multiple pill treatments, are extensively evaluated barriers to optimal adherence and viral suppression among PLWH.39–43 Guidelines to the standard of antiretroviral therapy typically adhered to the three-drug regimens due to its proven efficacy in suppressing development of AIDS and increasing survival.44 However, this antiretroviral regimen also introduced PLWH to high pill burdens, long-term toxicities, and potential drug–drug interactions resulting in treatment discontinuation and drug resistance. Further, as the number of PLWH with polypharmacy increased due to longer survival, comorbidity and co-medication are additional resultant barriers of poor adherence.45–48 Though antiretroviral regimen complexity and pill burden were not directly evaluated in this study, we observed lower overall combined adherence when compared to adherence evaluated as medication dose, schedule, and instruction adherence separately. This finding suggested poorer antiretroviral adherence in PLWH, and supports previous reports that estimating adherence based on medication dose alone may overestimate the true adherence level.49–51 Consequentially, a more appropriate measurement of adherence may need to consider all antiretroviral requirements including medication dose, schedule, and instruction.
Older PLWH were observed to have better antiretroviral adherence compared to younger adults. However, longer HIV-infected adults experienced poorer adherence compared to more recently infected individuals, a finding that was similarly reported in a study utilizing MMP at the national level.31 Younger PLWH had been numerously reported to be at higher risks of non-adherence and were often subjected to unique barriers in maintaining high antiretroviral adherence.52–54 For instance, adolescents and young PLWH were less likely to be retained in care, more likely to delay initiation of ART, and had lower rates of virologic suppression, all of which had been associated with poorer antiretroviral adherence.55–57 Conversely, poor adherence in longer HIV-infected adults may be related to modifiable patient-related factors such as access to insurance, employment, and mental illness, which may affect PLWH ability to maintain care.58,59 Other factors such as personal beliefs and low health literacy could negatively impact levels of adherence and ability to remain in care.60,61 Thus, improving overall adherence in PLWH may require tailoring adherence strategies to target longer HIV-infected adults on improving adherence and those recently infected on maintaining adherence.
We noted multiple characteristics of complete adherence across the sociodemographic, behavioral, and clinical domains of PLWH. Similar to prior studies reporting age-specific barriers to antiretroviral adherence and virologic suppression, we observed variability in barriers to complete adherence on duration of HIV infection.52,53 Differences in barriers by duration of HIV infection were attributed to exposures of PLWH to specific barriers throughout the antiretroviral treatment continuum. In particular, among persons recently infected with HIV for <5 years, no incarceration and self-efficacy in taking medication as directed were positively associated with high adherence. Incarceration had been described as a major barrier to adherence among HIV-infected adults, and while correctional facilities may have appropriate ART supports some were under-prescribing and -administering antiretroviral medications with accepted guidelines.28,29 For recent HIV-infected adults who received care in the community, incarceration had been identified as a major impediment to continual HIV care due to disruption of social networks and patient–provider relationships.62,63 Furthermore, accessibility to ART may not necessarily be sustained after integration back to the community causing therapy interruptions.62,63 These factors should be taken into account during counseling and in the design of effective adherence interventions for PLWH.
Among adults infected with HIV for 5–10 years, having no major depression and strong beliefs in medications efficacy were positive indicators of complete antiretroviral adherence, findings that have been similarly reported elsewhere.14,64,65 In contrast, adults infected with HIV for >10 years with complete antiretroviral were more likely to be non-heavy drinkers and to have high self-efficacy in taking medications as prescribed. Of note, exposure to HIV stigma is a novel experience that negatively delays initiation of antiretroviral treatment for individuals with early-stage HIV, and as a consequence disclosure of HIV status and seeking social supports were less likely among this HIV-infected population.66–68 Presentation of symptoms and ailments, which described individuals with later-stage HIV infection, may also catalyze HIV disclosure and access to treatment. Additionally, Belayihun et al reported negative associations between ART durations and adherence.63 These stemmed from individuals’ loss of interests in taking medications over long periods of time and a shift in beliefs that displaying no symptoms of HIV is an indication of being and staying healthy.63 This finding may explain differences in adherence characteristics by duration of HIV infection. The burden of life-long ART medication requirements may influence HIV-infected adults’ knowledge and experience with HIV disease, affecting adherence over time. Among PLWH recently diagnosed with HIV, knowledge of HIV disease is critical to high adherence; however, as they aged their experience with long-term medication usage reduced their ability to adhere to ART medication.18,20,21
Our findings support previous studies’ assertion that the success of ART depends on the extent of patient adherence to the prescribed doses, dosing intervals, and other medication instructions.69,70 Overall, differential barriers to antiretroviral adherence highlight the need to provide PLWH with continual adherence supports and education to enhance their HIV treatment outcomes. Therefore, it is important for HIV care providers to use patients’ office visits as teachable moments to engage them in regular and ongoing discussions about the benefits of strict adherence to prescribed medication doses, schedules, and instructions. Such duologue may help uncover new barriers, identify strategies, and set behavioral goals that could help improve adherence among PLWH.
Study Strengths and Limitations
There were several strengths associated with this study. The sampling procedure used in MMP allowed for a representative sample of all PLWH living in Houston/Harris County, Texas and generalization of our findings across the area. As part of a national survey with multiple representative sites in the US of which Houston is one of the study locations, findings from this analysis can be used to compare ART adherence levels with other locations nationally. Moreover, MMP collected the most current and a broad range of information regarding the sociodemographic, behavioral, and clinical characteristics of PLWH living in Houston/Harris County, Texas, and thus, cover comprehensively the potential characteristics affecting abilities of PLWH to adhere to ART medication.
Nonetheless, interpretation of the results should be evaluated with some limitations. This study utilized three measurements to capture ART adherence level though additional measures can be considered to assess adherence. Although adherence to medication is a dynamic process influenced by participants’ behavioral change over time,71 our current study applied a cross-sectional design, and therefore, only estimated ART adherence at one point in time. The cross-sectional nature of the analysis also limited inferring definite causality between the evaluated characteristics and ART adherence. Several characteristics were collected through self-reports by participants and thus subject to potential recall and social desirability response biases. Lastly, findings in this analysis may be limited by the sample size as indicated by some large confidence intervals. This limitation may explain to some extent the negative associations for factors that have been previously found to be positively associated with adherence.72 Despite these limitations, however, little or no research had evaluated adherence in PLWH residing in Houston/Harris County, Texas, in relation to changes in adherence level and associated adherence characteristics by the duration of HIV infection.
Conclusion
We reported one in two PLWH was adherent to complete medication dose, schedule, and instruction in a large sample of PLWH receiving medical care in Houston/Harris County, Texas, between 2009 and 2014. PLWH infected with HIV for <10 years were more likely to be completely adherent than those infected for >10 years. Multiple sociodemographic, behavioral, and clinical factors were associated with complete adherence, and these factors differed by the duration of HIV infection. Our findings supported previous studies that measure of ART adherence should capture medication dose, schedule, and instruction adherence, as a single medication adherence will overestimate adherence level.13,31 Furthermore, adherence intervention programs should be tailored to individual or group characteristics in order to provide effective support systems to recent and longer infected PLWH who may experience different and unique adherence barriers. Specifically, efforts should be made to target recently infected PLWH on maintaining adherence and longer infected PLWH on improving adherence such that PLWH can achieve virologic suppression throughout their treatment.
Disclaimers
The findings and conclusions of this article are solely the responsibility of the authors and do not necessarily represent the official position of the US Centers for Disease Control and Prevention or the Houston Health Department. This article is an abridged form of the thesis work submitted by the lead author to the University of Texas Health Science Center at Houston School of Public of Health in partial fulfillment for the award of a master’s degree in Public Health (MPH) in Epidemiology in May 2018. Part of this work has been previously presented as a poster titled “Complete Adherence to Antiretroviral Therapy Among HIV Infected Adults Receiving Medical care: Influence of Duration Since HIV Diagnosis” at the 24th Annual International Society for Pharmacoeconomic and Outcomes Research (ISPOR) Conference in New Orleans, LA, USA. May 18–22, 2019, Abstract ID#: 92738 and appeared as conference proceedings’ abstract in April 2019 Value in Health 22: S205.
Acknowledgments
The authors would like to thank the HIV care facilities and sampled persons who participated in the MMP in Houston/Harris County, Texas, during the 2009–2014 data collection cycles. We would also like to acknowledge the MMP staffs for the data collection and members of the Community and Provider Advisory Boards, and the management of the Houston Health Department and members of the Clinical Outcomes Team in CDC’s Behavioral and Clinical Surveillance Branch of the Division of HIV/AIDS Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention for their respective support and contributions.
Funding
The MMP data collection activities in Houston for the 2009–2014 cycles was funded by the Centers for Disease Control and Prevention (CDC) under the Cooperative Agreement Number PS09-937.
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Moreno S, Lopez Aldeguer J, Arribas JR, et al. The future of antiretroviral therapy: challenges and needs. J Antimicrob Chemother. 2010;65(5):827–835. doi:10.1093/jac/dkq061
2. Este JA, Cihlar T. Current status and challenges of antiretroviral research and therapy. Antiviral Res. 2010;85(1):25–33. doi:10.1016/j.antiviral.2009.10.007
3. Palmisano L, Vella S. A brief history of antiretroviral therapy of HIV infection: success and challenges. Ann Ist Super Sanita. 2011;47(1):44–48. doi:10.4415/ANN_11_01_10
4. Deeks SG, Lewin SR, Havlir DV. The end of AIDS: HIV infection as a chronic disease. Lancet. 2013;382(9903):1525–1533. doi:10.1016/S0140-6736(13)61809-7
5. De Cock KM, Jaffe HW, Curran JW. The evolving epidemiology of HIV/AIDS. Aids. 2012;26(10):1205–1213. doi:10.1097/QAD.0b013e328354622a
6. Stricker SM, Fox KA, Baggaley R, et al. Retention in care and adherence to ART are critical elements of HIV care interventions. AIDS Behav. 2014;18(Suppl 5):S465–75. doi:10.1007/s10461-013-0598-6
7. Castel AD, Magnus M, Greenberg AE. Update on the epidemiology and prevention of HIV/AIDS in the United States. Curr Epidemiol Rep. 2015;2(2):110–119. doi:10.1007/s40471-015-0042-8
8. Mannheimer S, Hirsch-Moverman Y. What we know and what we do not know about factors associated with and interventions to promote antiretroviral adherence. Curr Infect Dis Rep. 2015;17(4):466. doi:10.1007/s11908-015-0466-9
9. Mannheimer SB, Matts J, Telzak E, et al. Quality of life in HIV-infected individuals receiving antiretroviral therapy is related to adherence. AIDS Care. 2005;17(1):10–22. doi:10.1080/09540120412331305098
10. Ortego C, Huedo-Medina TB, Llorca J, et al. Adherence to highly active antiretroviral therapy (HAART): a meta-analysis. AIDS Behav. 2011;15(7):1381–1396. doi:10.1007/s10461-011-9942-x
11. Al-Dakkak I, Patel S, McCann E, Gadkari A, Prajapati G, Maiese EM. The impact of specific HIV treatment-related adverse events on adherence to antiretroviral therapy: a systematic review and meta-analysis. AIDS Care. 2013;25(4):400–414. doi:10.1080/09540121.2012.712667
12. Mocroft A, Youle M, Moore A, et al. Reasons for modification and discontinuation of antiretrovirals: results from a single treatment centre. Aids. 2001;15(2):185–194. doi:10.1097/00002030-200101260-00007
13. Beer L, Heffelfinger J, Frazier E, et al. Use of and adherence to antiretroviral therapy in a large U.S. sample of HIV-infected adults in care, 2007–2008. Open AIDS J. 2012;6:213–223. doi:10.2174/1874613601206010213
14. Schaecher KL. The importance of treatment adherence in HIV. Am J Manag Care. 2013;19(12 Suppl):S231–7.
15. Glass T, Cavassini M. Asking about adherence - from flipping the coin to strong evidence. Swiss Med Wkly. 2014;144:w14016. doi:10.4414/smw.2014.14016
16. Cooke CE, Lee HY, Xing S. Adherence to antiretroviral therapy in managed care members in the United States: a retrospective claims analysis. J Manag Care Pharm. 2014;20(1):86–92. doi:10.18553/jmcp.2014.20.1.86
17. Genberg BL, Lee Y, Rogers WH, Wilson IB. Four types of barriers to adherence of antiretroviral therapy are associated with decreased adherence over time. AIDS Behav. 2015;19(1):85–92. doi:10.1007/s10461-014-0775-2
18. Burgess MJ, Zeuli JD, Kasten MJ. Management of HIV/AIDS in older patients-drug/drug interactions and adherence to antiretroviral therapy. HIV AIDS. 2015;7:251–264. doi:10.2147/HIV.S39655
19. Ghidei L, Simone MJ, Salow MJ, et al. Aging, antiretrovirals, and adherence: a meta-analysis of adherence among older HIV-infected individuals. Drugs Aging. 2013;30(10):809–819. doi:10.1007/s40266-013-0107-7
20. Wutoh AK, Brown CM, Kumoji EK, et al. Antiretroviral adherence and use of alternative therapies among older HIV-infected adults. J Natl Med Assoc. 2001;93(7–8):243–250.
21. Sankar A, Nevedal A, Neufeld S, Berry R, Luborsky M. What do we know about older adults and HIV? A review of social and behavioral literature. AIDS Care. 2011;23(10):1187–1207. doi:10.1080/09540121.2011.564115
22. Iachan R, Johnson CH, Harding RL, et al. Design and weighting methods for a nationally representative sample of HIV-infected adults receiving medical care in the United States-Medical Monitoring Project. Open AIDS J. 2016;10:164–181. doi:10.2174/1874613601610010164
23. Weiser J, Beer L, Frazier EL, et al. Service delivery and patient outcomes in Ryan White HIV/AIDS program-funded and -nonfunded health care facilities in the United States. JAMA Intern Med. 2015;175(10):1650–1659. doi:10.1001/jamainternmed.2015.4095
24. Reynolds NR, Sun J, Nagaraja HN, Gifford AL, Wu AW, Chesney MA. Optimizing measurement of self-reported adherence with the ACTG adherence questionnaire: a cross-protocol analysis. J Acquir Immune Defic Syndr. 2007;46(4):402–409. doi:10.1097/QAI.0b013e318158a44f
25. Langebeek N, Gisolf EH, Reiss P, et al. Predictors and correlates of adherence to combination antiretroviral therapy (ART) for chronic HIV infection: a meta-analysis. BMC Med. 2014;12:142. doi:10.1186/s12916-014-0142-1
26. Thompson-Paul AM, Wei SC, Mattson CL, et al. Obesity among HIV-infected adults receiving medical care in the United States: data from the cross-sectional Medical Monitoring Project and National Health and Nutrition Examination Survey. Medicine. 2015;94(27):e1081. doi:10.1097/MD.0000000000001081
27. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
28. Uthman OA, Oladimeji O, Nduka C. Adherence to antiretroviral therapy among HIV-infected prisoners: a systematic review and meta-analysis. AIDS Care. 2017;29(4):489–497. doi:10.1080/09540121.2016.1223799
29. Westergaard RP, Spaulding AC, Flanigan TP. HIV among persons incarcerated in the US: a review of evolving concepts in testing, treatment and linkage to community care. Curr Opin Infect Dis. 2013;26(1):10–16. doi:10.1097/QCO.0b013e32835c1dd0
30. Aberg JA, Gallant JE, Ghanem KG, Emmanuel P, Zingman BS, Horberg MA. Primary care guidelines for the management of persons infected with HIV: 2013 update by the HIV Medicine Association of the Infectious Diseases Society of America. Clin Infect Dis. 2014;58(1):1–10. doi:10.1093/cid/cit757
31. Beer L, Skarbinski J. Adherence to antiretroviral therapy among HIV-infected adults in the United States. AIDS Educ Prev. 2014;26(6):521–537. doi:10.1521/aeap.2014.26.6.521
32. Frankel MR, McNaghten A, Shapiro MF, et al. A probability sample for monitoring the HIV-infected population in care in the U.S. and in selected states. Open AIDS J. 2012;6:67–76. doi:10.2174/1874613601206010067
33. Mgbere O, Khuwaja S, Bell TK, et al. System and patient barriers to care among people living with HIV/AIDS in Houston/Harris County, Texas: HIV medical care providers’ perspectives. J Int Assoc Provid AIDS Care. 2015;14(6):505–515. doi:10.1177/2325957414539045
34. Nokes K, Johnson MO, Webel A, et al. Focus on increasing treatment self-efficacy to improve human immunodeficiency virus treatment adherence. J Nurs Scholarsh. 2012;44(4):403–410. doi:10.1111/j.1547-5069.2012.01476.x
35. Centers for Disease Control and Prevention. Behavioral and clinical characteristics of persons receiving medical care for HIV infection—Medical Monitoring Project, United States, 2014 cycle (June 2014–May 2015); 2020. Available from: https://www.cdc.gov/hiv/pdf/library/reports/surveillance/cdc-hiv-hssr-mmp-2014.pdf.
36. Burnham KP, Anderson DR. P values are only an index to evidence: 20th- vs. 21st-century statistical science. Ecology. 2014;95(3):627–630. doi:10.1890/13-1066.1
37. Vrieze SI. Model selection and psychological theory: a discussion of the differences between the Akaike information criterion (AIC) and the Bayesian information criterion (BIC). Psychol Methods. 2012;17(2):228–243. doi:10.1037/a0027127
38. Maartens G, Celum C, Lewin SR. HIV infection: epidemiology, pathogenesis, treatment, and prevention. Lancet. 2014;384(9939):258–271. doi:10.1016/S0140-6736(14)60164-1
39. Scott Sutton S, Magagnoli J, Hardin JW. Impact of pill burden on adherence, risk of hospitalization, and viral suppression in patients with HIV infection and AIDS receiving antiretroviral therapy. Pharmacotherapy. 2016;36(4):385–401. doi:10.1002/phar.1728
40. Saberi P, Neilands TB, Vittinghoff E, Johnson MO, Chesney M, Cohn SE. Barriers to antiretroviral therapy adherence and plasma HIV RNA suppression among AIDS clinical trials group study participants. AIDS Patient Care STDS. 2015;29(3):111–116. doi:10.1089/apc.2014.0255
41. Nachega JB, Parienti JJ, Uthman OA, et al. Lower pill burden and once-daily antiretroviral treatment regimens for HIV infection: a meta-analysis of randomized controlled trials. Clin Infect Dis. 2014;58(9):1297–1307. doi:10.1093/cid/ciu046
42. Manzano-García M, Pérez-Guerrero C, Álvarez de Sotomayor Paz M, Robustillo-Cortés MLA, Almeida-González CV, Morillo-Verdugo R. Identification of the medication regimen complexity index as an associated factor of nonadherence to antiretroviral treatment in HIV positive patients. Ann Pharmacother. 2018;52(9):862–867. doi:10.1177/1060028018766908
43. Altice F, Evuarherhe O, Shina S, Carter G, Beaubrun AC. Adherence to HIV treatment regimens: systematic literature review and meta-analysis. Patient Prefer Adherence. 2019;13:475–490. doi:10.2147/PPA.S192735
44. Moreno S, Perno CF, Mallon PW, et al. Two-drug vs. three-drug combinations for HIV-1: do we have enough data to make the switch? HIV Med. 2019;20(Suppl 4):2–12. doi:10.1111/hiv.12716
45. Cantudo-Cuenca MR, Jiménez-Galán R, Almeida-Gonzalez CV, Morillo-Verdugo R. Concurrent use of comedications reduces adherence to antiretroviral therapy among HIV-infected patients. J Manag Care Spec Pharm. 2014;20(8):844–850. doi:10.18553/jmcp.2014.20.8.844
46. Borrego Y, Gómez-Fernández E, Jiménez R, Cantudo R, Almeida-González CV, Morillo R. Predictors of primary non-adherence to concomitant chronic treatment in HIV-infected patients with antiretroviral therapy. Eur J Hosp Pharm. 2018;25(3):127–131. doi:10.1136/ejhpharm-2016-001000
47. Cordova E, Cecchini D, Rodriguez C. Potential drug-drug interactions in HIV-perinatally infected adolescents on antiretroviral therapy in Buenos Aires, Argentina. J Int AIDS Soc. 2014;17(Suppl 4):19764. doi:10.7448/IAS.17.4.19764
48. Gimeno-Gracia M, Crusells-Canales MJ, Javier Armesto-Gómez F, Rabanaque-Hernández MJ. Prevalence of concomitant medications in older HIV+ patients and comparison with general population. HIV Clin Trials. 2015;16(3):117–124. doi:10.1179/1528433614Z.0000000012
49. Costa JM, Torres TS, Coelho LE, Luz PM. Adherence to antiretroviral therapy for HIV/AIDS in Latin America and the Caribbean: systematic review and meta-analysis. J Int AIDS Soc. 2018;21(1):e25066. doi:10.1002/jia2.25066
50. Mills EJ, Nachega JB, Buchan I, et al. Adherence to antiretroviral therapy in sub-Saharan Africa and North America: a meta-analysis. JAMA. 2006;296(6):679–690. doi:10.1001/jama.296.6.679
51. Morowatisharifabad MA, Movahed E, Nikooie R, et al. Adherence to medication and physical activity among people living with HIV/AIDS. Iran J Nurs Midwifery Res. 2019;24(5):397–399. doi:10.4103/ijnmr.IJNMR_205_18
52. Shubber Z, Mills EJ, Nachega JB, et al. Patient-reported barriers to adherence to antiretroviral therapy: a systematic review and meta-analysis. PLoS Med. 2016;13(11):e1002183. doi:10.1371/journal.pmed.1002183
53. Ferrand RA, Briggs D, Ferguson J, et al. Viral suppression in adolescents on antiretroviral treatment: review of the literature and critical appraisal of methodological challenges. Trop Med Int Health. 2016;21(3):325–333. doi:10.1111/tmi.12656
54. Soares RCA, Brito AM, Lima K, Lapa TM. Adherence to antiretroviral therapy among people living with HIV/AIDS in northeastern Brazil: a cross-sectional study. Sao Paulo Med J. 2019;137(6):479–485. doi:10.1590/1516-3180.2019.0212170919
55. Shaw S, Amico KR. Antiretroviral therapy adherence enhancing interventions for adolescents and young adults 13–24 years of age: a review of the evidence base. J Acquir Immune Defic Syndr. 2016;72(4):387–399. doi:10.1097/QAI.0000000000000977
56. Zanoni BC, Mayer KH. The adolescent and young adult HIV cascade of care in the United States: exaggerated health disparities. AIDS Patient Care STDS. 2014;28(3):128–135. doi:10.1089/apc.2013.0345
57. Thompson MA, Mugavero MJ, Amico KR, et al. Guidelines for improving entry into and retention in care and antiretroviral adherence for persons with HIV: evidence-based recommendations from an International Association of Physicians in AIDS care panel. Ann Intern Med. 2012;156(11):817–833. doi:10.7326/0003-4819-156-11-201206050-00419
58. Krentz HB, Gill MJ. Increased costs of HIV care associated with aging in an HIV-infected population. HIV Med. 2015;16(1):38–47. doi:10.1111/hiv.12176
59. Chambers LA, Wilson MG, Rueda S, Gogolishvili D, Shi MQ, Rourke SB. Evidence informing the intersection of HIV, aging and health: a scoping review. AIDS Behav. 2014;18(4):661–675. doi:10.1007/s10461-013-0627-5
60. Knobel H, Urbina O, González A, et al. Impact of different patterns of nonadherence on the outcome of highly active antiretroviral therapy in patients with long-term follow-up. HIV Med. 2009;10(6):364–369. doi:10.1111/j.1468-1293.2009.00696.x
61. Kalichman S, Kalichman MO, Cherry C. Medication beliefs and structural barriers to treatment adherence among people living with HIV infection. Psychol Health. 2016;31(4):383–395. doi:10.1080/08870446.2015.1111371
62. Culbert GJ. Violence and the perceived risks of taking antiretroviral therapy in US jails and prisons. Int J Prison Health. 2014;10(2):94–110. doi:10.1108/IJPH-05-2013-0020
63. Belayihun B, Negus R. Antiretroviral treatment adherence rate and associated factors among people living with HIV in Dubti Hospital, Afar Regional State, East Ethiopia. Int Scholarly Res Notices. 2015;2015:5. doi:10.1155/2015/187360
64. Sin NL, DiMatteo MR. Depression treatment enhances adherence to antiretroviral therapy: a meta-analysis. Ann Behav Med. 2014;47(3):259–269. doi:10.1007/s12160-013-9559-6
65. Nilsson Schonnesson L, Williams ML, Ross MW, Bratt G, Keel B. Factors associated with suboptimal antiretroviral therapy adherence to dose, schedule, and dietary instructions. AIDS Behav. 2007;11(2):175–183. doi:10.1007/s10461-006-9160-0
66. Haberer JE, Bwana BM, Orrell C, et al. ART adherence and viral suppression are high among most non-pregnant individuals with early-stage, asymptomatic HIV infection: an observational study from Uganda and South Africa. J Int AIDS Soc. 2019;22(2):e25232. doi:10.1002/jia2.25232
67. Ayieko J, Brown L, Anthierens S, et al. “Hurdles on the path to 90-90-90 and beyond”: qualitative analysis of barriers to engagement in HIV care among individuals in rural East Africa in the context of test-and-treat. PLoS One. 2018;13(8):e0202990. doi:10.1371/journal.pone.0202990
68. Katz IT, Ryu AE, Onuegbu AG, et al. Impact of HIV-related stigma on treatment adherence: systematic review and meta-synthesis. J Int AIDS Soc. 2013;16(Suppl 3):18640. doi:10.7448/IAS.16.3.18640
69. Chesney MA. Factors affecting adherence to antiretroviral therapy. Clin Infect Dis. 2000;30(Suppl 2):S171–S176. doi:10.1086/313849
70. Atkinson MJ, Petrozzino JJ. An evidence-based review of treatment-related determinants of patients’ nonadherence to HIV medications. AIDS Patient Care STDS. 2009;23(11):903–914. doi:10.1089/apc.2009.0024
71. Hansana V, Sanchaisuriya P, Durham J, et al. Adherence to antiretroviral therapy (ART) among people living with HIV (PLHIV): a cross-sectional survey to measure in Lao PDR. BMC Public Health. 2013;13:617. doi:10.1186/1471-2458-13-617
72. Damulira C, Mukasa MN, Byansi W, et al. Examining the relationship of social support and family cohesion on ART adherence among HIV-positive adolescents in southern Uganda: baseline findings. Vulnerable Child Youth Stud. 2019;14(2):181–190. doi:10.1080/17450128.2019.1576960
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.