")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Evaluation of the Individual Activity Descriptors of the mMRC Breathlessness Scale: A Mixed Method Study
Authors Yorke J, Khan N, Garrow A, Tyson S, Singh D, Vestbo J , Jones PW
Received 16 May 2022
Accepted for publication 17 August 2022
Published 15 September 2022 Volume 2022:17 Pages 2289—2299
DOI https://doi.org/10.2147/COPD.S372318
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Janelle Yorke,1,2 Naimat Khan,1,3 Adam Garrow,1 Sarah Tyson,1 Dave Singh,1,3 Jorgen Vestbo,1,4 Paul W Jones5
1Faculty of Biology, Medicine and Health, University of Manchester, Manchester, UK; 2Christie Patient Centred Research, The Christie NHS Foundation Trust, Whittington, Manchester, UK; 3Medicines Evaluation Unit, Wythenshawe, Manchester, UK; 4Department of Respiratory Medicine, Wythenshawe Hospital, Manchester, UK; 5St George’s Hospital, University of London, London, UK
Correspondence: Janelle Yorke, Tel +44920 264411, Email [email protected]
Purpose: The modified-Medical Research Council (mMRC) breathlessness scale consists of five grades that contain of a description of different activities. It has wide utility in the assessment of disability due to breathlessness but was originally developed before the advent of modern psychometric methodology and, for example contains more than one activity per grade. We conducted an evaluation of the mMRC structure.
Patients and Methods: Cognitive debriefing was conducted with COPD patients to elicit their understanding of each mMRC activity. In a cross-sectional study, patients completed the mMRC scale (grades 0– 4) and an MRC-Expanded (MRC-Ex) version consisting of 10-items, each containing one mMRC activity. Each activity was then given a 4-point response scale (0 “not at all” to 4 “all of the time”) and all 10 items were given to 203 patients to complete Rasch analysis and assess the pattern of MRC item severity and its hierarchical structure.
Results: Cognitive debriefing with 36 patients suggested ambiguity with the term “strenuous exercise” and perceived severity differences between mMRC activities. 203 patients completed the mMRC-Ex. Strenuous exercise was located third on the ascending severity scale. Rasch identified the mildest term was “walking up a slight hill” (logit − 2.76) and “too breathless to leave the house” was the most severe (logit 3.42).
Conclusion: This analysis showed that items that were combined into a single mMRC grade may be widely separated in terms of perceived severity when assessed individually. This suggests that mMRC grades as a measure of individual disability related to breathlessness contain significant ambiguity due to the combination of activities of different degrees of perceived severity into a single grade.
Keywords: psychometrics, Rasch analysis, patient reported outcomes, qualitative, scale development
Introduction
Breathlessness is a complex subjective sensation that is common and debilitating in patients with Chronic Obstructive Pulmonary Disease (COPD). Breathlessness is an important predictor of exercise tolerance1 and both factors have been shown to influence patients’ health status at all levels of COPD severity.2 Breathlessness can be quantified directly using scales such as the Borg and Visual Analogue Scales (VAS) or indirectly through its impact on physical activity.3,4 The modified-Medical Research Council (mMRC) breathlessness scale classifies the disability associated with breathlessness by identifying different levels of activities that induce or are restricted by breathlessness.5
The MRC breathlessness scale was first published in 1959 by Fletcher et al based on their study of respiratory symptoms experienced by Welsh coal miners in the 1940s.5 It was originally developed as an epidemiological tool for studies of the general population, but over many decades has morphed into a tool that is applied at an individual patient level. The questionnaire is frequently used in COPD as breathlessness is a crucial symptom in this condition.3 The original version of the MRC consists of scale ranges from grade 1 to 5. The mMRC version is now used which is similar in wording for each grade but consists of scale ranges from grade 0 to 4. It is important to note that it does not measure breathlessness directly, unlike other scales such as the Borg scale. Rather it measures the degree of activity at which a person gets breathlessness (such as “with strenuous exercise”) or limits what a person can do (such as “too breathless to leave the house”). It consists of five grades (1 to 5) that contain statements describing a range of physical limitations associated with breathlessness.
There is an assumption that the mMRC Grades are Guttman scaled6 in which a person who fulfils the criteria for Grade 4, should also fulfil the criteria for Grade 3, 2 etc. Except for MRC Grade 0 (“not troubled by breathlessness except on strenuous exercise”), each grade consists of two different activity descriptions. For example, the components of Grade 4 include “too breathless to leave the house” or “breathless when dressing”; reflecting potentially large differences in activity level. To our knowledge the comparability of different mMRC grade components has not been previously subjected to rigorous testing.
The mMRC breathlessness scale has good discriminative ability and is a simple method of categorising patients with COPD in terms of their disability7,8 and survival.9 Thus, it is recommended for use as a marker of disability in international COPD guidelines10,11 and used to assess suitability for pulmonary rehabilitation in the UK.10 However, due to the wide spread of severity between MRC grades it is too insensitive to detect relevant changes in activity limitation due to breathlessness following an intervention.3 Despite the widespread use of the scale, there has been little work to evaluate its psychometric properties, particularly the effect of combining different activity descriptions within the mMRC grades and the ordering of the grade severity. It is important to confirm whether the different components within each grade represent the same level of exertion. This study aimed to examine the content and construct validity of the MRC scale using cognitive debriefing with COPD patients and modern psychometric techniques. Specific objectives included: i) to determine how patients with COPD understand and interpret each mMRC grade descriptor; ii) to determine if patient responses to individual mMRC activities meet the requirements for Guttman scaling; and iii) to measure the similarity of scores between different activity descriptors within a single mMRC grade.
Methods
We used both qualitative and quantitative approaches to explore patients understanding more fully of the mMRC descriptors and to quantify the hierarchical structure of the scale. To achieve this, the study was conducted in two phases: Phase 1: cognitive debriefing to ascertain patients’ comprehension and views of each mMRC activity and Phase 2: application of descriptive statistics and Rasch analysis to assesses the performance of each mMRC grade component. This study complies with the Declaration of Helsinki and ethical approval for was provided by the National Research Ethics Committee for Greater Manchester East (ref: 12/NW/0608). This study was conducted between January 2013 – July 2015.
In each phase of the study, the participants were identified from a research database of COPD patients (n>800) recruited from primary care and hospital clinics; these patients had volunteered to participate in research studies at the Medicines Evaluation Unit, adjacent to Wythenshawe Hospital (South Manchester). Potential participants for each study phase were contacted by telephone to ascertain their interest in taking part. If interested, a study information pack was mailed to the patient and a suitable time to attend the research facility for consenting and data collection was agreed which were completed on the same day. Participants were paid a nominal fee for taking part in the study.
Inclusion and Exclusion Criteria
Inclusion criteria were: male and female patients aged 40 years or older diagnosed with COPD by General Practitioner or respiratory specialists using established criteria.12 Airflow limitation was graded according to post-bronchodilator Forced Expired Volume in 1 second (FEV1) spirometry. Patients with FEV1 ≥ 80% predicted were classified as Global Initiative for Chronic Obstructive Lung Disease (GOLD) Grade 1 (Mild), 50% ≤ FEV1 <80% predicted Grade 2 (Moderate); 30% ≤ FEV1 <50% predicted Grade 3 (Severe) and FEV1 <30% predicted Grade 4 (Very Severe).12 Patients were excluded if they had a medically confirmed and documented chest infection in the previous three months or any other respiratory illness such as asthma, cystic fibrosis, and lung cancer.
Data Collection
Phase 1
The initial phase involved cognitive debriefing13 in a focus group with patients diagnosed with COPD. The groups were facilitated by two of the authors both with qualitative research experience (JY & AG), audio-recorded and transcribed verbatim. Participants were presented with a list of 10 items, each consisting of an individual activity from the original MRC questionnaire (Table 1). Firstly, participants were asked to describe their understanding of the meaning of each item and their experience of it. Next, they were asked to comment on whether or not the combination of items within the mMRC grades was logical and appropriate and if such combinations reflected their experience (eg “Do the items ‘I am too breathless to leave the house’ and ‘I am breathlessness when dressing/undressing’ represent a similar experience?” and “What are your thoughts regarding the combination of different descriptors within each grade?”).
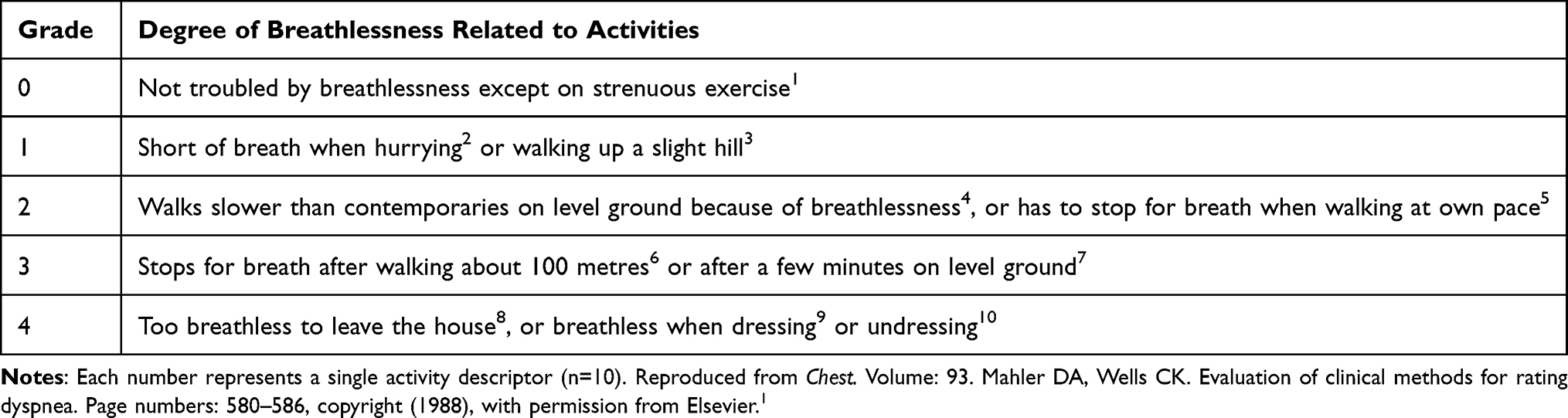 |
Table 1 mMRC Breathlessness Scale |
Phase 2
In Phase 2, a sample of COPD patients was asked to complete the mMRC breathlessness scale (grades 0 to 4) by placing a tick in the box next to the grade that best described their current experience. They also completed the MRC-expanded (MRC-Ex) version made up of the 10 MRC activities created for the purposes of this study (Figure 1). Each item used a 4-point response scale (0 “not at all” to 4 “all of the time”). Participants were instructed to complete both questionnaires during a study specific visit to the research facility in random order.
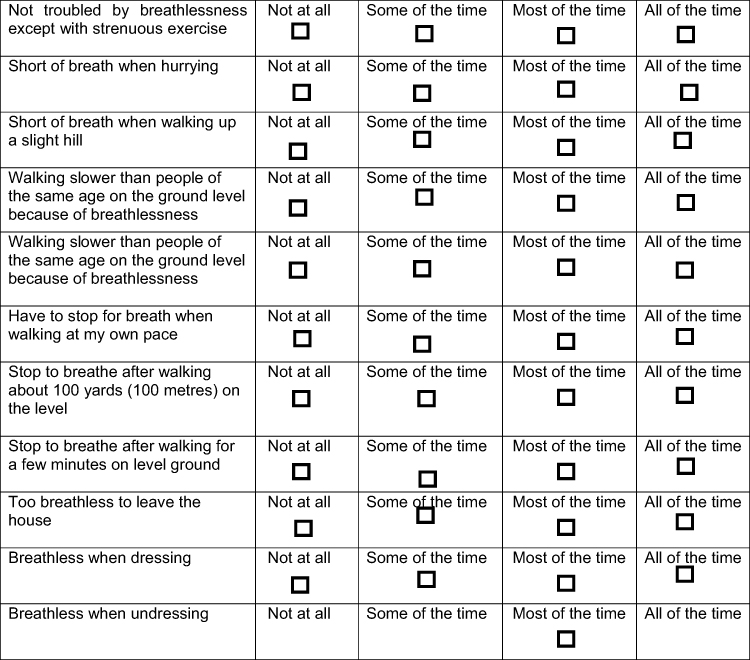 |
Figure 1 MRC-Expanded version. |
Data Analysis
Statistical analyses were conducted using SPSS Statistics for Windows, Version 20.0. Armonk, NY. The Polytomous Rasch model was applied using RUMM2030 programme (www.eumlab.com). In a Rasch model, severity associated with any given item (ie “strenuous exercise”) is measured in “logits” – which is the log odds of a patient of a given level of activity limitation, as assessed by their response to all the items combined, having a 50% chance of responding positively to that item.
Phase 1
Focus group meetings were recorded, transcribed, and analysed using a modified thematic analysis approach.14 Thematic analysis is a method for describing data across, for example, interviews or focus groups, to describe data through the generation of themes. Our modified approach analysed data across the different focus-group sets to describe participants perceptions and understanding of the mMRC descriptions; we did not move to the next step of theme generation.
Phase 2
Descriptive statistics summarised demographic details and compared participant’s self-allocation to an mMRC grade with their responses to the 10-item MRC-Ex. In particular, we assessed whether patients scored positively for items in the MRC-Ex that indicated more severe disability than their response on the mMRC grading.
Rasch analysis allowed several scale assumptions to be tested. It is an advanced psychometric methodology that is closely related to item-response theories.15,16 The Rasch model is based on a probabilistic relationship between people who complete a questionnaire and the items on that questionnaire. In the context of a breathlessness scale, we would expect that a person with very severe breathlessness would be more likely to affirm any given item than another person who had no difficulties with their breathing. Using this methodology it is possible to separately model the level of breathlessness (i.e its severity) exhibited by the respondents and the level of breathlessness assessed by the individual items. By doing so, items can be ordered on a continuum of breathlessness severity using a linear logit scale. A higher logit value indicates a greater severity of breathlessness.6,16 Individual item fit was assessed using a chi-squared statistic to compare the difference between the observed responses and those expected by the model. The presence of any item-trait interaction was tested using a chi-square test to assess whether all items perform consistently, regardless of overall mMRC-Ex grade severity (determined by p>0.05) (16).
Rasch analysis was used to assess the ordering of item severity of MRC-Ex items. Individual item fit was assessed to determine if all 10 item descriptors met the requirements of a unidimensional scale. In the context of this study, Rasch fit statistics were used to examine the measurement properties of the MRC-Ex and extrapolate these to the original mMRC grade to highlight measurement anomalies with its individual items rather than to present the MRC-Ex as a new scale for the assessment of breathlessness in COPD.
Results
Phase 1
36 patients took part in six focus groups, each including 2–9 participants. Their characteristics are shown in Table 2. With the exception of mMRC Grade 0 (strenuous exercise), participants were able to describe the meaning of each individual activity (Table 3). There was a consensus that combining items within a mMRC grade was not logical, particularly the combination of descriptors located in Grade 4. In general, participants viewed the mMRC scale as quick and easy to use but questioned the appropriateness of combining different grade components.
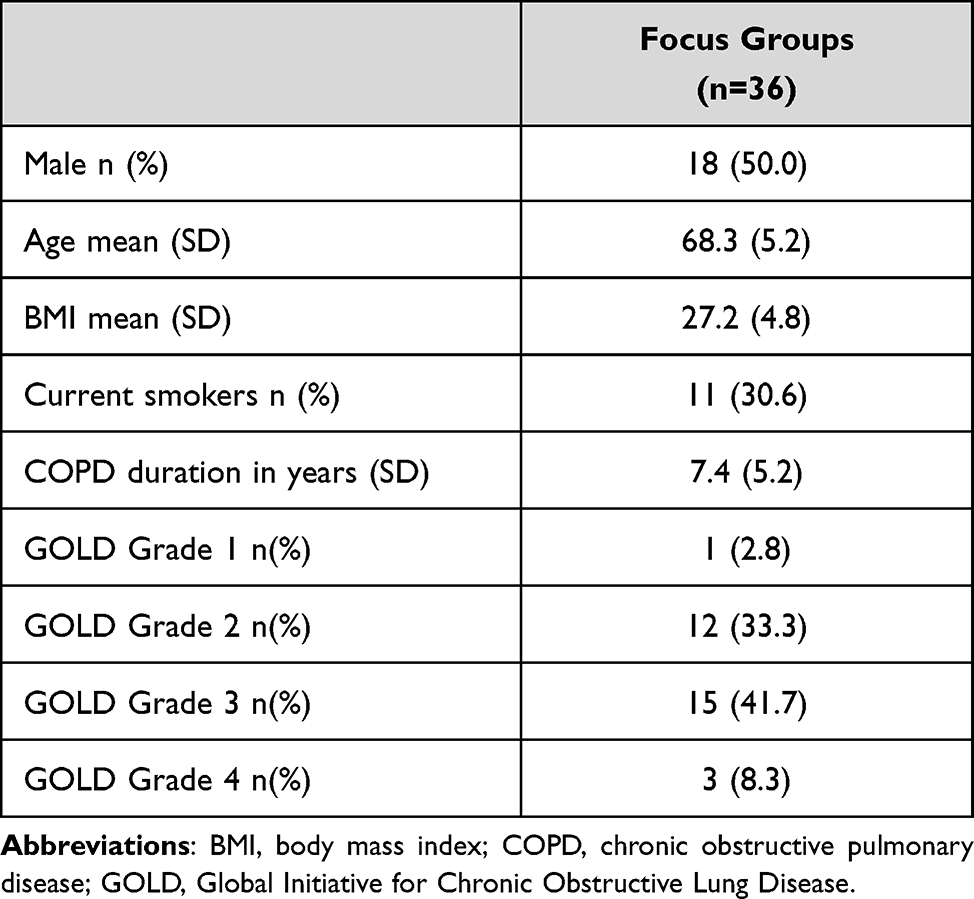 |
Table 2 Participant Characteristics for Phase 1 |
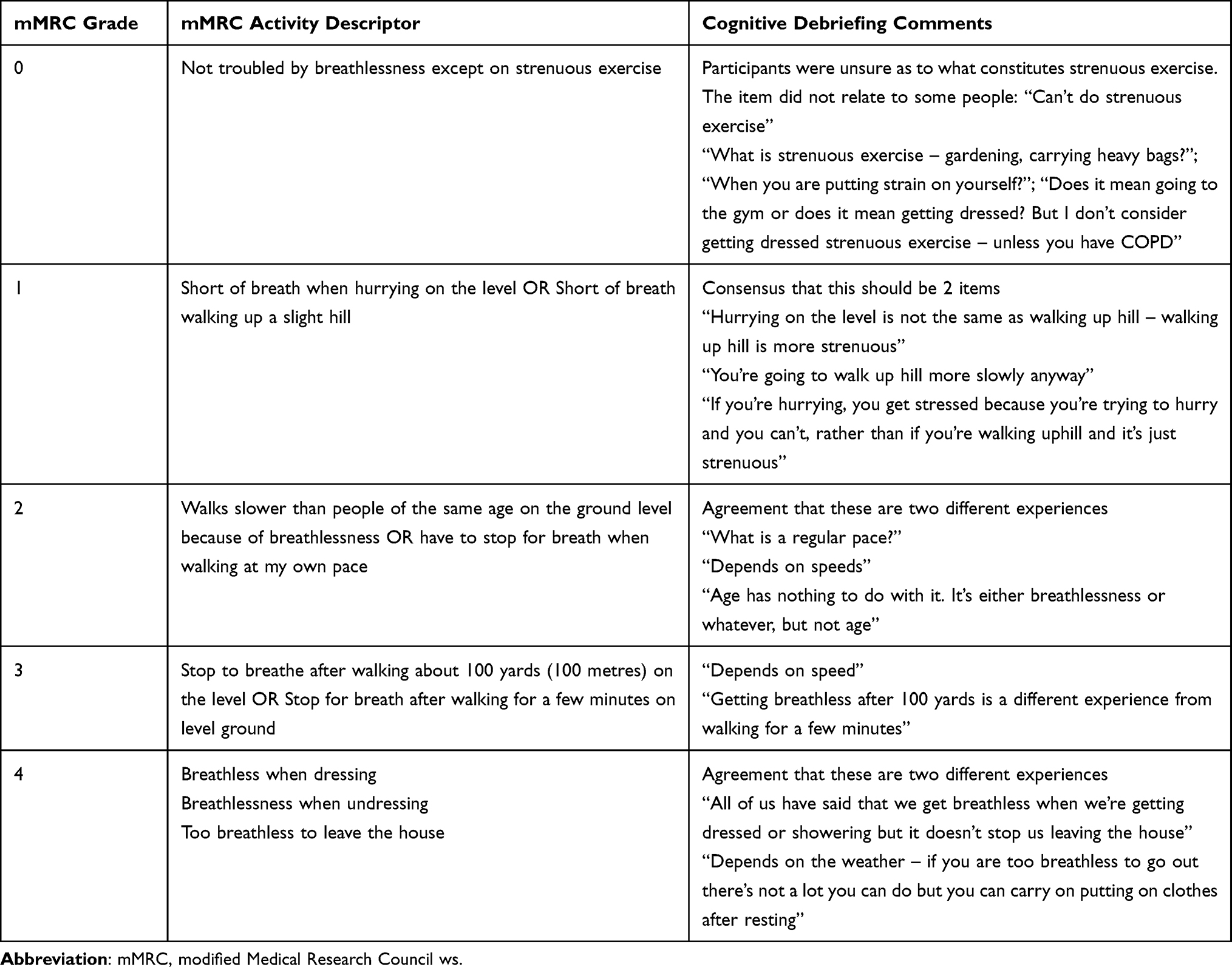 |
Table 3 Focus Group Comments for Each MRC Grade |
Phase 2
203 patients with a confirmed diagnosis of COPD completed the questionnaires. Their characteristics are shown in Table 4. There was a good spread of patients across the five mMRC grades (0: 9.9%; 1: 31.5%; 2: 19.7; 3: 21.6%; 4: 11.3%) enabling comparisons to be made across the full range of possible disabilities.
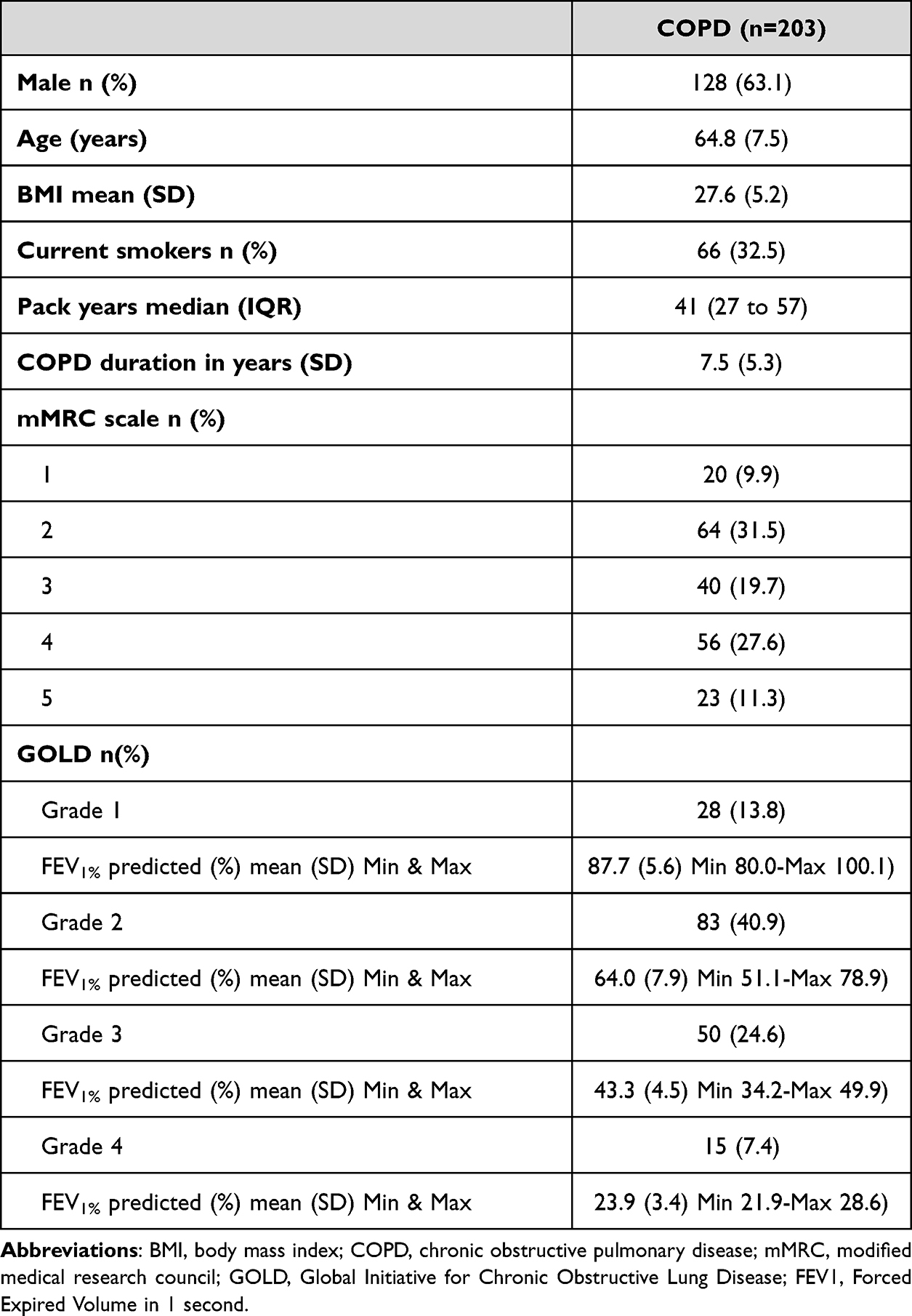 |
Table 4 Participant Characteristics – Phase 2 |
The first stage of analysis included an assessment of patients’ responses to the original mMRC grading compared with their responses to the MRC-Ex (Table 5). For each mMRC grade a proportion of patients also responded positively to experiencing a more severe level of disability on the MRC-Ex at least “some of the time”. For example, 20 patients were in mMRC Grade 0 yet most also experienced breathlessness during activities that were assigned to other mMRC grades such as such as Grade 1 (“going up a slight hill”; 15/20 and “hurrying on the level”; 14/20), even MRC grade 4 (dressing/undressing; both 4/20); none of the 20 “Grade 0” participants responded that they were too breathless “to leave the house”. For MRC-Ex items 1, 3, 5, 6, 7, 8, 9 and 10, a proportion of patients indicated they did not experience an item at least “some of the time”, despite responding positively to the relative MRC grade. For example, of the 23 patients in mMRC Grade 4, 30% (7/20) responded “not at all” to the MRC-Ex item “too breathless to leave the house”. For mMRC Grade 3 13% (7/56) patients responded “not at all” to its corresponding items MRC-Ex 6 and 7.
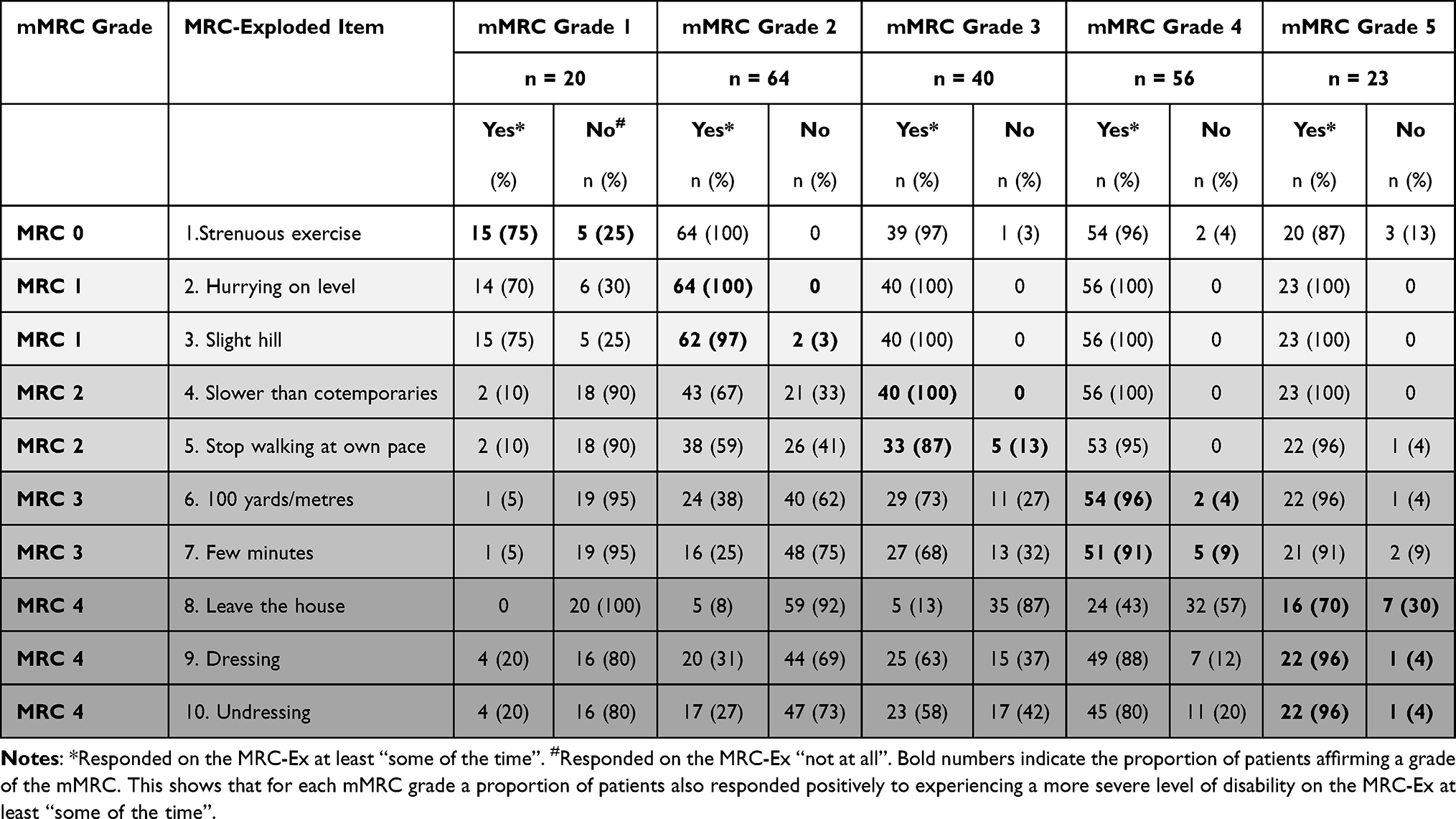 |
Table 5 mMRC Grade and Corresponding MRC-Ex Responses |
Rasch analysis was used to determine the severity location (measured in logits) for each MRC-Ex item and to test whether its severity matched the ordering according to mMRC grades (Table 6). The mildest item was “breathless when going up a slight hill” (logit −2.76) and “too breathless to leave the house” was the most severe item (logit 3.422). MRC-Ex item 1 (“strenuous exercise”) was located third on the ascending severity scale with a logit of −1.389. mMRC Grade 4 components “breathless when dressing” (MRC-Ex 9) and “breathless when undressing” (MRC-Ex 10) were much milder (at least 2 logits) than “too breathlessness to leave the house” (MRC-Ex 8). The level of information provided by each item at different levels of breathlessness is plotted in Figure 2.
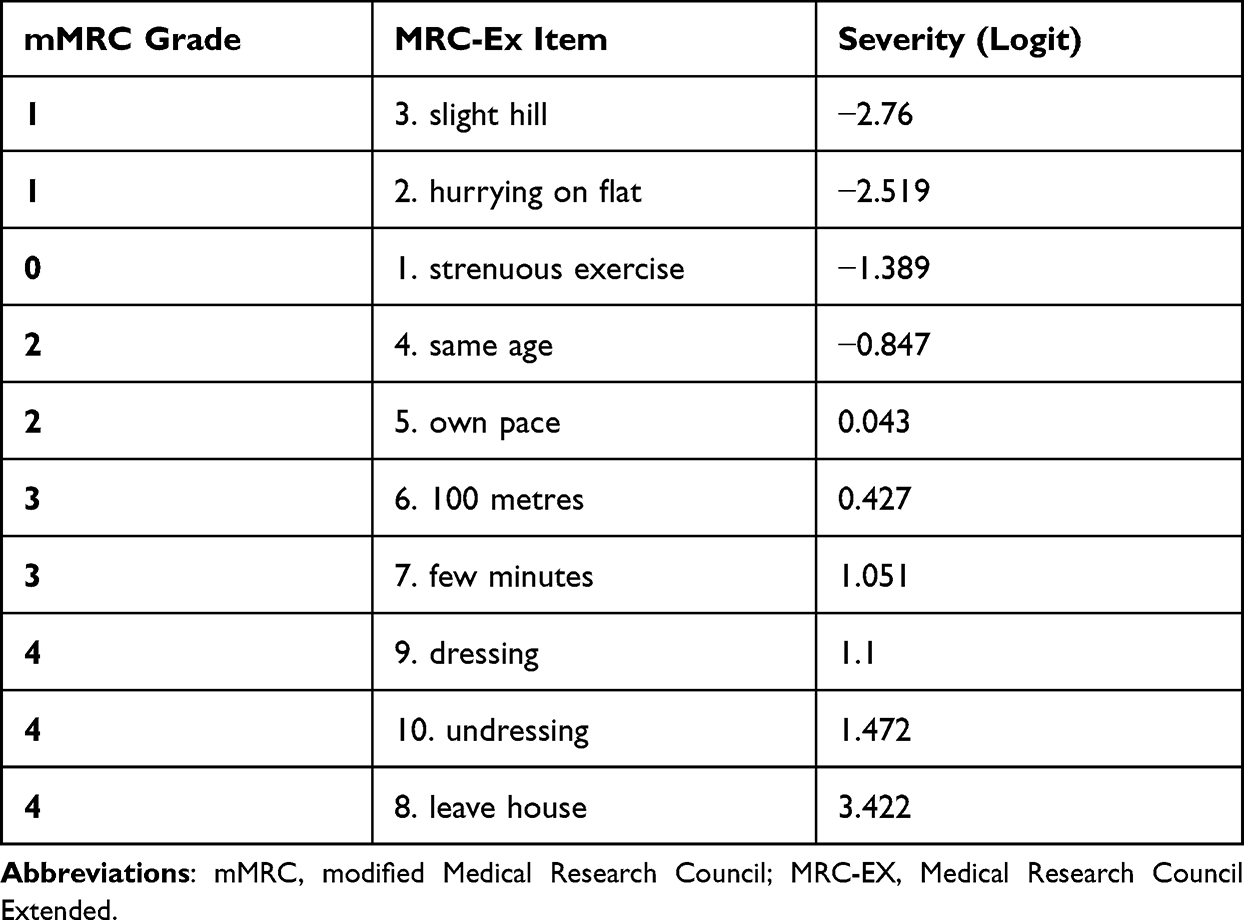 |
Table 6 Logit (Severity) Location for Each mMRC Component |
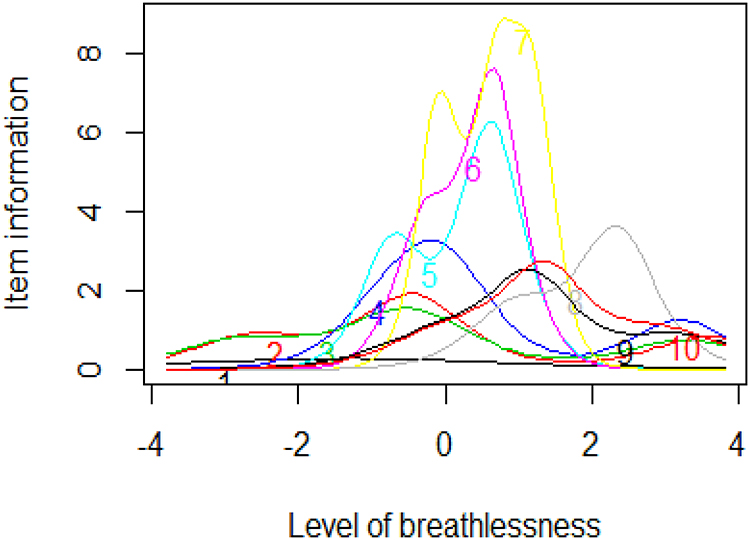 |
Figure 2 Individual item information plot for MRC-Ex. |
The MRC-Ex 10-items did not fit the Rasch model (chi-square = 11.2, p <0.00001). This was due to one item – “not troubled by breathlessness except on strenuous exercise” (MRC-EX item 1) which demonstrated significant mis-fit to the model due to a high positive fit residual, indicating that the item does not reliably discriminate between respondents at any level of breathlessness (item residual +7.2, p = 0.00004) (Figure 3) leading it to provide very little information at all levels of breathlessness. The removal of this item resulted in overall fit of the remaining 9 items to the Rasch model (chi-square = 21.5, p = 0.25).
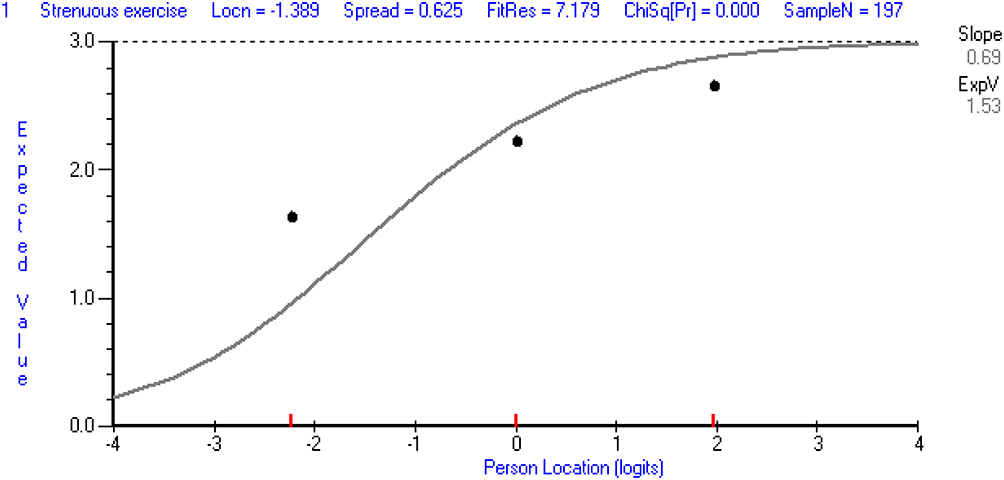 |
Figure 3 Item characteristic curve – MRC-Ex 1 “Not troubled by breathlessness except on strenuous exercise”. |
Discussion
The aim of this study was to examine the performance of different components of the mMRC breathlessness scale and to determine the appropriateness of combining different activity descriptors within each grade. To our knowledge, this is the first mixed method analysis to examine the validity of presenting more than one activity descriptor within the mMRC grades and its Guttman scaling properties in patients with COPD.
The results from both Phases 1 and 2 bring into question the hierarchical structure of the mMRC scale. Notably, mMRC grade 0 presents a number of measurement challenges. Firstly, some patients stated that the term was difficult to place in context of their current experience because they did not undertake strenuous exercise. For others, the description was confusing as it could cover a very broad spectrum of activities. This ambiguity is likely to have resulted in some patients being allocated to Grade 0 whilst also responding positively to an MRC-Ex item that denoted greater disability. Rasch analysis confirmed that patients were not responding to this item in the intended manner, resulting in item “mis-fit”; when this item was removed the remaining item-set demonstrated good fit to the Rasch unidimensional model. Rasch analysis also demonstrated that this item did not denote the mildest breathlessness – it was positioned third on the MRC-Ex severity scale. These results highlight mMRC grade 0 as an anomaly. It is difficult for patients to comprehend, has poor measurement properties and its logit value does not represent the lowest level of activity limitation.
The mMRC grades 1 to 4 contain more than one activity that it is assumed evoke the same level of disability due to breathlessness, however there was a consensus during focus group meetings that the inclusion of more than one activity in a single mMRC grade was unhelpful and confusing. Compared to other grades, grade 1 components (“hurrying on the flat” and “walking up a slight hill”) demonstrated the closest logit severity level – they were less than 0.2 logits apart. Interestingly, one focus group participant associated the term “hurrying” with being stressed as opposed to representing breathlessness due to physical exertion/walking quickly. This brings into question the comparability of these two grade components. However, of the 64 participants located in mMRC grade 1, all responded positively to MRC-Ex item 2 (“hurrying up a hill”) and only two responded “not at all” to MRC-Ex item 3 (“slight hill”).
During cognitive interviewing, the activities contained in both Grade 2 and 3 were also perceived as representing different levels of disability associated with breathlessness. There was also some confusion about what each descriptor meant, as each experience was dependent on different factors such as speed/pace of walking. This made it challenging for participants to come to firm agreement on the meaning of each description. There was approximately 0.5 logit difference between each component in grade 2 and grade 3, which is large for items that are meant to reflect the same degree of severity.6,15,16
The largest mismatch between grade components was seen within mMRC grade 4. Patients agreed that there was little difference in activity limitation due to breathlessness when “dressing or undressing”, although during cognitive debriefing some expressed more concern with morning-time activities which is related to getting dressed; however, the difference in logits was minimal. The perceived impact of COPD on morning activities has previously been shown to be substantial.17,18 The main concern with Grade 4 was the descriptor “too breathless to leave the house”. There was a clear consensus that breathlessness associated with dressing/undressing represented a lower level of disability than being unable to leave the house. Such views were supported by the results of MRC-Ex Rasch analysis in which “too breathless to leave the house” was located at the severe end of the scale and much higher (two logits) than the dressing items. Combining of these descriptors into one MRC grade is inappropriate.
Based on our analyses, the main concerns relate to the extreme ends of the MRC questionnaire: “strenuous exercise” and “too breathless to leave the house”. As most COPD patients are symptomatic, strenuous exercise does not fit well with the application of the mMRC questionnaire to this population. In addition, combining items in Grade 4 is illogical as is the use of “too breathless to leave the house” when respondents are completing the questionnaire at a venue outside their house. As patients can attend a focus group interview for research purposes, they can clearly leave the house.
This study leaves a question hanging - what are the implications of this study? The mMRC scale is extremely widely used and is incorporated into guidelines for the management of individual patients; however this study has shown that it has significant weakness at both a qualitative and a quantitative level. Part of the problem lies with mMRC grade zero and the unavoidable conclusion from this study is that this grade is unreliable. The other nine activities, when used individually, have good measurement properties and also moderately good properties when activities are grouped as into mMRC grades 1–4, but it is clear that when grouped in this way there is a loss of precision. We cannot recommend that the 9-point scale is used, because there has been no qualitative study to identify all the candidate items for a scale of dyspnoea-induced disability, and the analysis was not designed to identify the minimum number of items that are required to form a such a scale. The mMRC-ex was developed to enable Rasch analysis to be performed and provide indication of the mMRC structure. However, we recommend that such as scale is developed to help clinicians make a reliable assessment of individual patients in routine practice; robust testing of a further modified mMRC that replaces “strenuous exercise” and includes a one activity description for any single item may be a sensible approach to rectifying the issues identified in this study. For clinicians, we conclude that whilst there is some value in recording the mMRC grade, the patient should always be asked about limitation of activities that are important to them and this analysis shows that the 9 individual mMRC items, excluding strenuous exercise, would form a helpful guide to answering the patient’s question “What type of activity do you mean?”.
This study had a number of limitations. Participants were recruited using a database of COPD patients living in one area of England, Greater Manchester. However, many of the sample characteristics are representative of similar COPD cohorts of primary care patients.7 The MMRC-Ex was not developed with patient input – the researchers simply separated each activity description and retained the same wording and nominated a scaling range for each (0–4). Participants for both study phases attended the research clinic to complete focus groups/questionnaires and hence were able to leave the house which is likely to have biased responses to mMRC Grade 4. We recommend further research that explores mMRC responses with people unable to leave the house. It has been shown that gender differences in the experience and reporting of breathlessness exists between males and females. We did not specifically examine this in our study but would recommend that this is explored in future work examining patients’ views of the mMRC scale. We did not include clinicians views which would be an important aspect of any follow-on study to further modify the mMRC.
In conclusion, the mMRC generally meets the criteria for hierarchical ordering however, Grade 0 (strenuous exercise) presents as an anomaly. There was a general consensus among focus group participants that the combining of descriptors into single mMRC grades was inappropriate and this was confirmed by quantitative analyses with large severity difference between some categories. We recommend further development of the mMRC to address the measurement issues identified through this study.
Acknowledgments
Thank you to all our patients who took the time to participate in this study.
The abstract of this paper was presented at the European Respiratory Society Conference ‘Evaluation of individual activity descriptors of the MRC Dyspnoea Scale: do they add up? As a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in European Respiratory Journal 2015 46: PA681; DOI: 10.1183/13993003.congress-2015.PA681.
Funding
The study was supported by a Innovate UK through a Knowledge Transfer Partnership. JY and JV are supported by the NIHR Manchester Biomedical Research Centre.
Disclosure
Professor Dave Singh reports personal fees from Aerogen, AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, CSL Behring, Epiendo, personal fees from Genentech, GlaxoSmithKline, Glenmark, Gossamerbio, Kinaset, Menarini, Novartis, Pulmatrix, Sanofi, Synairgen, Teva, Theravance, Verona, outside the submitted work. Dr Jorgen Vestbo reports personal fees from AstraZeneca, grants from Boehringer-Ingelheim, personal fees from Chiesi, GSK, Novartis, ALK-Abello, Teva, Boehringer-Ingelheim, outside the submitted work. Professor Paul W Jones reports he is an employee of GlaxoSmithKline, outside the submitted work. The authors have no other conflicts of interest in relation to this work.
References
1. Mahler DA, Wells CK. Evaluation of clinical methods for rating dyspnea. Chest. 1988;93:580–586. doi:10.1378/chest.93.3.580
2. Oga T, Nishimura K, Tsukino M, Hajiro T, Ileda A, Mishima M. Relationship between different indices of exercise capacity and clinical measures in patients with chronic obstructive pulmonary disease. Heart Lung. 2002;31:374–381. doi:10.1067/mhl.2002.127941
3. Bausewein C, Farquhar M, Booth S, Gysels M, Higginson IJ. Measurement of breathlessness in advance disease: a systematic review. Respir Med. 2007;101(3):399–410. doi:10.1016/j.rmed.2006.07.003
4. Dorman S, Byrne A, Edwards A. Which measurement scales should we use to measure breathlessness in palliative care? A systematic review. Palliat Med. 2007;21(3):177–191. doi:10.1177/0269216307076398
5. Fletcher CM, Elmes PC, Fairbairn AS, Wood CH. The significance of respiratory symptoms and the diagnosis of chronic bronchitis in a working population. Br Med J. 1959;2:256–266. doi:10.1136/bmj.2.5147.257
6. Pallant JF, Tennant A. An introduction to the Rasch measurement model: an example using the hospital anxiety and depression scale (Hads). Br J Clin Psychol. 2007;46(Pt 1):1–18. doi:10.1348/014466506X96931
7. Bestall JC, Paul EA, Garrod R, et al. Usefulness of the Medical Research Council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax. 1999;54:581–586. doi:10.1136/thx.54.7.581
8. Stavem K, Boe J, Erikssen J. Health status, dyspnea, lung function, and exercise capacity in patients with chronic obstructive pulmonary disease. Int J Tuberc Lung Dis. 1999;3:920–926.
9. Celli BR, Cote CG, Lareau SC, Meek PM. Predictors of survival in COPD: more than just the FEV1. Resp Med. 2008;102(Suppl 1):S27–35. doi:10.1016/S0954-6111(08)70005-2
10. National Clinical Guideline Centre. Chronic obstructive pulmonary disease: management of chronic obstructive pulmonary disease in adults in primary and secondary care. London: National Clinical Guideline Centre; 2010. Available from: Hyyp://giudeance.nice.org.uk/.
11. O’Donnell DE, Aaron S, Bourbeau J, et al. Canadian Thoracic Society recommendations for management of chronic obstructive pulmonary disease – 2007 update. Can Respir J. 2007;14(Suppl B):5B–32B. doi:10.1155/2007/830570
12. Vestbo J, Hurd SS, Agusti AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease GOLD executive summary. Am J Respir Crit Care Med. 2013;187:347–365. doi:10.1164/rccm.201204-0596PP
13. Drennan J. Cognitive interviewing: verbal data in the design and pretesting of questionnaires. JAN. 2003;42:57–63. doi:10.1046/j.1365-2648.2003.02579.x
14. Green J, Thorogood N. Qualitative Methods for Health Research. London: Sage Publications; 2004.
15. Rasch G. Probabilistic Models for Some Intelligence and Attainment Tests. Amsterdam: Danish Institute of Educational Research; 1960.
16. Holland P, Wainer H. Differential Item Functioning. New Jersey: Lawrence Erlbaum Associates; 2012.
17. Partridge MR, Karlsson N, Small IR. Patient insight into the impact of chronic obstructive pulmonary disease in the morning: an internet survey. Curr Med Res Opin. 2009;25(8):2043–2048. doi:10.1185/03007990903103006
18. Roche N, Chavannes NH, Miravitlles M. COPD symptoms in the morning: impact evaluation and management. Respir Res. 2013;14:112.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.