")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Evaluation of the Efficacy of an Ecobiological Dermo-Cosmetic Product to Help Manage and Prevent Relapses of Eyelid Atopic Dermatitis
Authors Bergera-Virassamynaïk S, Ardiet N, Sayag M
Received 2 January 2023
Accepted for publication 5 March 2023
Published 18 March 2023 Volume 2023:16 Pages 677—686
DOI https://doi.org/10.2147/CCID.S401576
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Sandrine Bergera-Virassamynaïk, Nathalie Ardiet, Michèle Sayag
NAOS Group, Research and Development Department, Aix-en-Provence, 13290, France
Correspondence: Sandrine Bergera-Virassamynaïk, NAOS Group, Research and Development Department, Aix-en-Provence, 13290, France, Tel +33 (0)4 26 20 65 04, Email [email protected]
Purpose: Atopic dermatitis (AD) is a chronic relapsing, inflammatory disease which causes eczematous lesions. Itching and symptoms visibility can have a significant impact on quality of life. This is the case when eyelids are affected. Therefore, we evaluated a dermo-cosmetic product designed to care AD on eyelids.
Subjects and Methods: An initial analysis of the product included 20 healthy women with no AD signs. A clinical evaluation of the effect of the product on AD sign severity was performed on 33 subjects presenting AD symptoms on eyelids. We also analyzed the product’s capacity to prevent relapses in a parallel group clinical evaluation performed on 66 subjects.
Results: First, on the forearm skin of healthy subjects, the product reduces erythema and decreases transepidermal water loss when used for 28 days. Second, when clinically evaluated on subjects with eyelid symptoms undergoing a corticoid treatment, the product leads to reduced AD signs scored by a dermatologist, better self-evaluation of symptoms by subjects, and improved quality of life. Besides, upon assessment in a randomized controlled clinical evaluation with subjects prone to AD relapses but without symptoms, the product also drastically reduces relapse frequency. If erythema reduction is the only sign identified by a dermatologist, the product greatly and rapidly improves the quality of life of subjects.
Conclusion: These effects can be explained by the known actions of the product’s ingredients. Rich in hydrating compounds, fatty acids and anti-inflammatory compounds, it aims at maintaining and restoring the epidermis structure and function to preserve it from irritants. It effectively shows that a daily care and hygiene routine with a dermo-cosmetic product designed according to an ecobiological approach leads to objective improvement of AD and subjective perception of quality of life.
Keywords: atopic dermatitis, eyelid, dermo-cosmetic, relapse, ecobiology
Introduction
Atopic dermatitis (AD) is a chronic, relapsing, inflammatory skin disease affecting up to 20% of children and 5% of adults.1,2 Characterized by sensitive, dry skin and eczematous lesions, the intense induced pruritus is a major diagnostic criterion as it affects 91% of patients.3 Repeated scratchings trigger a self-perpetuating itch-scratch cycle that profoundly impacts patients’ lives.4 Abnormal itch frequency affects 85% of patients, and 55% present sleep disturbance exceeding five days a week. These lead to behavioral problems and social withdrawal, which have significant psychological impacts.4,5
In adults, lesions can be located anywhere on the body but often affect the face and neck, with or without limb flexure symptoms.6,7 Eyelids, which present lesions in 22% of adults, are a particular concern as eyes are essential for facial attractiveness and important cosmetic organs.8 Eyelid skin is particularly susceptible due to its peculiar characteristics.9,10 If all skin layers (epidermis, dermis, and hypodermis) are present, the hypodermis is almost absent, and the dermis is very thin but highly vascularized. The epidermis is also extremely thin, with a reduced stratum corneum presenting half the cell layers generally present. Corneocytes are large. Their turnover is slow, yet, leading to insufficient maturation and a poor barrier function with a weakly protective hydrolipidic film. Beyond these anatomical characteristics, eyelids are subjected to intense mechanical constraints with around 10,000 eyelid beats per day and to environmental assaults. It also possesses folds – the palpebral folds – that can accumulate molecules, some of which may affect the skin. This is important, knowing that 24% of adults presenting AD also present positive patch-test reactions to chemical allergens.6 Therefore, in the case of women, symptoms could be amplified by using allergen-containing eye makeup and remover. Besides, the friction involved in their application could participate in the itch-scratch cycle.
If flares-up treatment has been the subject of intensive research, relapse prevention remains largely under-investigated. Topical medications exist. Yet, any irritant-free emollient, including over-the-counter or dermo-cosmetic emollients, is efficient. By retaining and replenishing epidermal moisture, they decrease flare-up severity and increase remission periods.11 Their successful use shows that maintaining or restoring the ecobiology of the skin is essential to manage AD and prevent relapses. Still, to the best of our knowledge, no study addresses the peculiarities of eyelids.
Ecobiology is an original approach developed by NAOS. It considers the skin as a living world composed of cutaneous cells and a complex microbiome that constitute a real ecosystem in which the various components interact with each other and adapt to their environment. Preserving the skin’s ecological balance is essential. It is the ultimate goal of ecobiology, an original approach that also considers its ever-evolving microbiome and environment, the resources and mechanisms of which must be preserved.12,13 Skin cares and cosmetics development can take these principles into account, possibly leading to better-adapted products.14 This was done when elaborating a dermo-cosmetic product specifically dedicated to eyelids AD. With care and makeup-removing properties, it only consists of a few high-quality ingredients. To investigate its efficacy, we first analyzed its effects on the forearm of subjects without AD records. We then performed a first clinical evaluation of its efficacy with subjects presenting mild to moderate AD symptoms at the eyelid level and following a topical corticoid treatment. Finally, we assessed the product’s capacity to prevent relapses in subjects with recurrent AD but symptom-free.
Materials and Methods
Ethic
Both clinical studies on AD subjects were conducted in Poland. According to local and EU regulations, no approval by ethics committees was required for the study on subjects under topical corticoid treatment. The clinical evaluation of relapsing prevention, carried out in Poland (Gdansk), was approved by the Bioethics Committee from the Regional Chamber of Physicians from Gdansk (Poland) under the reference 0000308843.
For all studies, the principles of the Declaration of Helsinki were strictly followed. All subjects received detailed information about the purpose of the study, its procedure, and goals. All gave their written informed consent before enrolment.
Investigated Product
The product investigated is a commercially available dermo-cosmetic cream (Atoderm Intensive eye, NAOS, LABORATOIRE BIODERMA). It consists of an oil-in-water emulsion containing, among other ingredients, enoxolone, a lipid complex (Lipigenium), high molecular weight hyaluronic acid, and sucrose stearate (Skin Barrier Therapy patent). A complete list of its ingredients and their role is presented in Table 1.
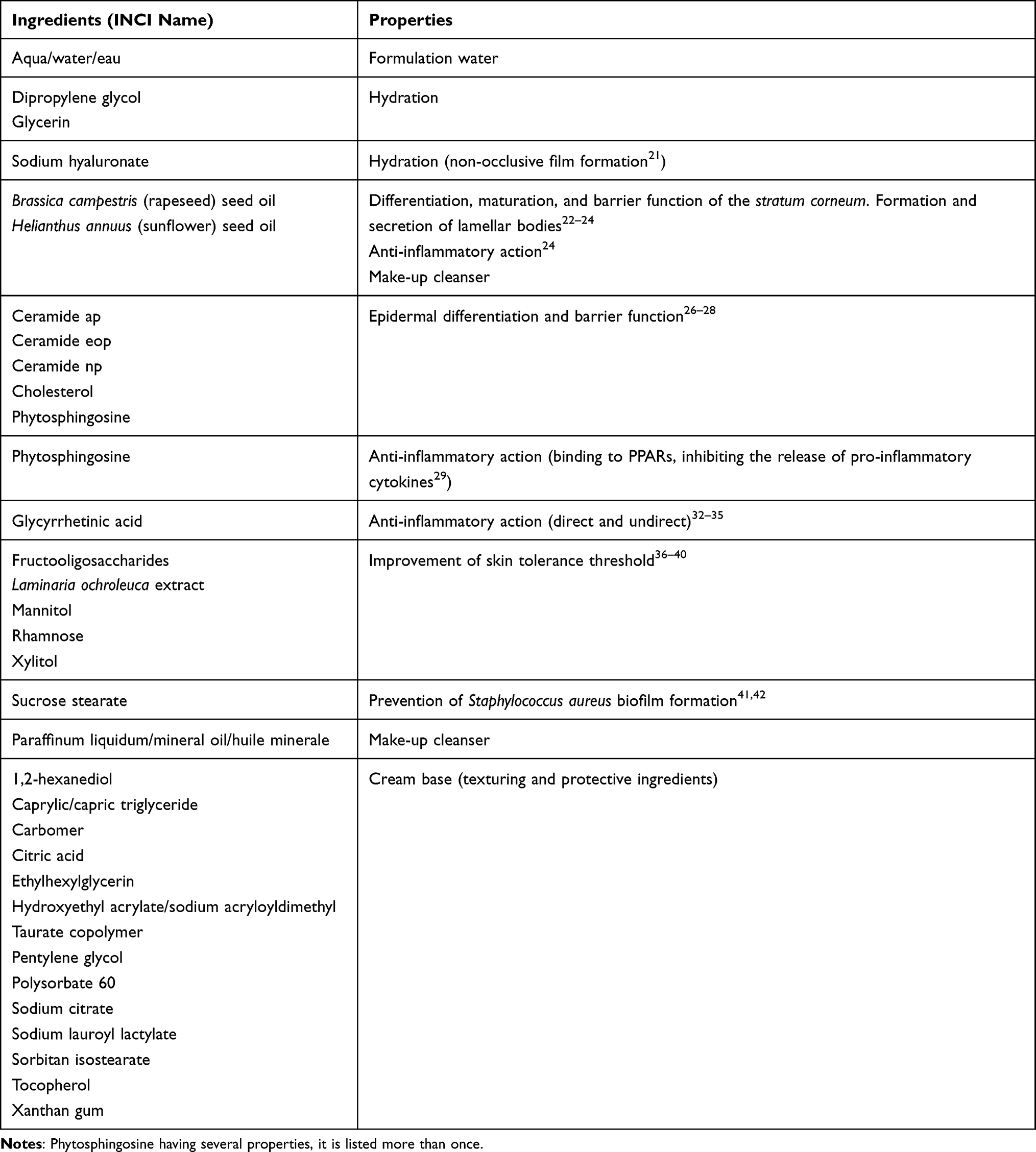 |
Table 1 List of Ingredients Entering the Product Evaluated and Their Properties |
Biometrological Analyses of the Effects of the Product
Subjects included in this evaluation had no history of AD. Inclusion criteria were the absence of cutaneous problems and excessive hairiness on the inner side of the forearms.
The soothing effect was analyzed on 20 Caucasian women (18- to 60-year-old, mean: 36-year-old, phototype I–III). Cutaneous microcirculation was measured using TiVi600 (Wheels Bridge, Sweden) before, immediately, and 30 minutes after inducing erythema by stripping, comparing results from a randomly selected inner forearm that received, immediately after the stripping, a standardized application of the product (2 µL/cm2) to those of a similar zone on the second forearm that received no cream.
The protective/anti-redness effect was assessed by patch tests performed on one man and 21 women (20- to 66-year-old, mean: 42-year-old, phototype I–III). Hill Top patch test Chambers (Cliantha Research, FL, USA) containing 1% sodium lauryl sulfate with 350 µL of the product or an identical amount of a neutral cream (without positive or negative effects) were applied to the inner side of subjects’ forearms. After 18 hours, patches were removed. Skin L* (dark to light) and a* (green to red) CIEL color parameters were determined 6 hours after patch removal using a CM700-d spectrophotometer (Konica Minolta, Japan).
Finally, the effect of the product on transepidermal water loss (TEWL) was examined on 9 Caucasian women (23- to 69-year-old, mean: 48-year-old) presenting dry to very dry skin (tewametric values over 6 and 8 g/m2/h respectively). TEWL measurements (Tewameter TM300, Courage+Khazaka electronic, Germany) were performed on day 0, and after 28 days on both forearms, one of which (randomly selected) received two applications per day on the entire forearm, the other one remaining untreated.
Clinical Evaluation of Subjects Presenting AD Symptoms on Eyelids
A first clinical evaluation was performed between December 2018 and April 2019. It included 33 subjects (4 men and 29 women, 22- to 83-year-old, mean age: 44-year-old, phototype II–III). All subjects had mild to moderate symptoms of AD on eyelids. All were undergoing a corticoid treatment (systemic: n=16, local: n=16, unknown: n=1) for at least 9 days (maximum: 36 days) and continued to do so during part of the study (mean±SD: 22±8 days, minimum: 9 days). Exclusion criteria were the presence of cutaneous pathology other than AD on eyelids, ophthalmological pathology in the six previous months, and the use of possibly interfering systemic treatment. Pregnant, nursing women, or women planning to get pregnant were excluded.
Each subject received the product and applied it twice daily to the eyelids without rinsing it. Applications were carried out in the morning as skincare (allowing make-up) and in the evening as skincare or make-up removal.
Clinical Evaluation of the Anti-Relapsing Effect of the Product
A second clinical investigation was conducted between January and December 2021. Subjects (14 men and 53 women, 19- to 74-year-old, mean age: 46-year-old, phototype II–III) had mild to moderate AD with at least three episodes within the previous six months but no symptoms at the beginning of the study. Corticoid treatments (58 out of 66, 89% were using a systemic medicine while the others a local treatment) were over and discontinued on day 0 of the study. Exclusion criteria were identical to those of the first clinical evaluation.
Subjects were divided into two groups. Half of them, randomly chosen, kept their usual hygiene and eyelid skin care. The others applied the product twice daily (morning and evening) on the eyelids without rinsing it.
Clinical Assessments
For both clinical evaluations, adverse effects were recorded throughout the study. The type of reaction, circumstances, date, duration, evolution, and intolerance causality were analyzed. For the relapse-preventing effect, subjects also recorded any relapse occurring throughout the evaluation.
In both studies, a dermatologist scored AD symptoms on the eyelids. He evaluated AD severity by scoring dryness, erythema, edema, desquamation, and roughness according to a 0 (no sign) to 10 (obvious sign) scale. These dermatological evaluations were performed on days 0 and 28 for the clinical assessment of product performances on subjects having AD symptoms on eyelids. They were conducted on days 0, 56, 112, and 168 to assess the relapse-preventing capacity of the product. In addition, subjects rated the impact of AD on their quality of life using a 10-question Dermatological Life Quality Index (DLQI) they filled out at the end of each visit. Each question was scored on a 0 (good) to 3 (bad) scale, leading to a final rating between 0 and 30.
For the clinical evaluation of product performances on subjects having AD symptoms on eyelids, subjects also self-evaluated tightness, stinging, burning, and itching sensations. These features, scored using a 0 (no sensation) to 10 (very perceptible sensation) scale, were evaluated on days 0 and 28.
Statistical Analysis
Results are presented as mean ± standard error of the mean (SEM). Data distributions were first analyzed by a Shapiro–Wilk test (α=0.01). Data with a Normal distribution were analyzed with a paired Student’s t-test. A Wilcoxon signed-rank test was otherwise used. A statistical difference of p<0.05 was considered significant.
Results
Analysis of the Product’s Effects on the Skin of Subjects Without AD
We started by analyzing whether the dermo-cosmetic product (Atoderm Intensive eye, NAOS, LABORATOIRE BIODERMA) protects the skin. We first followed the fate of induced erythema on forearm regions receiving, or not, a single product application. Results show that, 30 minutes after induction, erythema is weaker when the product is applied (−29.8±5.5 AU without the product versus −24.9±4.6 with the product, −16.4%, p=0.05). We also analyzed skin color changes after a mild irritation induced by sodium lauryl sulfate. After 24 hours, the product leads to lower L* and a* values than the cream base (DL*: −1.0±0.2 for the product versus −3.8±0.4 for the neutral cream, p<0.001; Da*: +1.3±0.3 for the product versus +4.1±0.4 for the neutral cream, p<0.001). These results indicate that, at the end of the experiment, the erythema is less pronounced with the product.
In a last experimental series, we monitored TEWL changes in subjects presenting dry to very dry skin. Analysis was performed after 28 days of product application. In the untreated control area, TEWL remains stable (8.12±0.43 AU on day 0 versus 8.43±0.63 AU on day 28, +3.8%, p=0.550), but upon product application, a TEWL decrease is observed (8.14±0.52 AU on day 0 versus 6.14±0.66 AU on day 28; −24.6%, p=0.002).
Clinical Evaluation of Product Performances on Subjects Having AD Symptoms on Eyelids
Knowing that the product reduces erythema and decreases TEWL, we tested it on subjects presenting AD symptoms at the level of eyelids. These subjects were using a corticoid treatment, at least at the beginning of the study.
During the 28 days, four subjects reported minor physical signs lasting from a few minutes to a day, but none were judged relevant. Nine subjects had mild burning, itching, or stinging episodes lasting from a few minutes to a few hours. These signs, possibly imputable to the product, mainly occurred in the first days of use, and no clinical signs were observed on day 28.
Evaluations of eyelids by a dermatologist on days 0 and 28 (Figure 1A) indicate that the product improves all symptoms scored. The efficacy of the products ranges from a minimum of −61.9% for edema (p<0.001, 76% of subjects showing an effect) to −100% for desquamation (p<0.001, 73% of subjects). The product also improves all symptoms self-evaluated by subjects (Figure 1B). Self-assessed tightness, stinging, burning, and itching sensations decrease from a minimum of 89.4% for stinging (p=0.011, 33% of subjects) to a maximum value of 100% for burning (p<0.001, 48% of subjects). These improvements are reflected by the quality of life of subjects, which global score drops by 91.2% (10.97±0.91 on day 0 versus 0.97±0.33 on day 28, p<0.001).
 |
Figure 1 Scoring of AD signs in subjects having AD symptoms at the beginning of the clinical evaluation and following a local topical corticoid treatment. Scorings were performed on day 0 and after 28 days of product use. (A) Evaluation by a dermatologist. (B) Self-evaluation by subjects. For the statistical significance: * p<0.05, ** p<0.01, and *** p<0.001. |
Clinical Evaluation of Product Performances on Subjects Having Relapsing AD but No Symptoms on Eyelids
As the product showed excellent results when used on eyelids with AD symptoms, we further tested its capacity to prevent AD relapses. We, therefore, performed a randomized controlled clinical evaluation with subjects presenting no AD symptoms but prone to relapses.
Among the 33 subjects using the product, 11 (33%) reported mild physical or functional signs at some point in the study. These signs were mild itching or erythema lasting up to a few days, and all were judged irrelevant.
Subjects using the product show no difference to those who were not when considering the time at which the first relapse occurs (29.4±16.1 days versus 32.3±6.24 days respectively, p=0.392) or in relapse duration (3.7±0.6 days versus 3.85±0.28 respectively, p=0.681). Yet, 25 subjects (76%) using the product had no relapse, while all 33 subjects of the control group had at least one relapse (Figure 2). This corresponds to an 86.9% relapse frequency decrease (p<0.001). Additionally, the total number of relapses is only 22 for subjects using the product but 168 in the control groups, with up to 54.5% of subjects having five relapses or more.
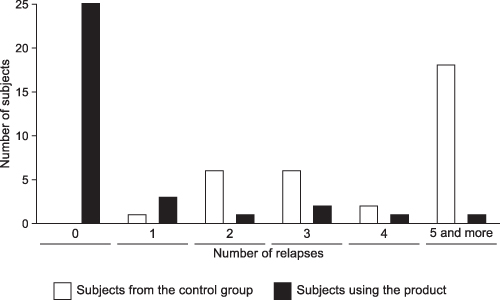 |
Figure 2 Number of relapses during the 168 days of the clinical evaluation carried on subjects presenting no AD symptoms on eyelids for the control group (in white) and the group using twice daily the product (in black). |
As expected by the inclusion criteria, dermatologist scorings of eyelids show few symptoms on day 0 in the group using the product and the control group. Therefore, little evolution over the 168 days of the study is observed (Figure 3). The only clinical sign evolving is erythema severity. If similar at day 0 (p=0.309), it only decreases in the group using the product at days 56 and 168 (−60.0%, p=0.023 and −95%, p=0.004 respectively). The decrease observed on day 112 is at the significance limit (p=0.077) as the fewer subjects affected presented more severe symptoms.
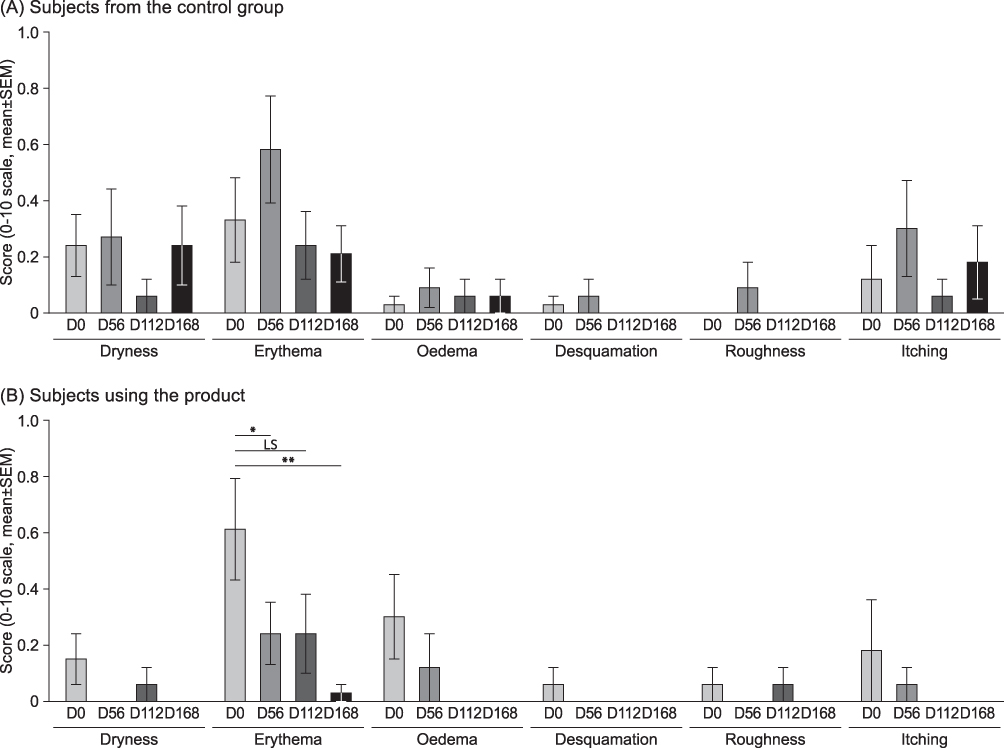 |
Figure 3 Scoring of AD signs in subjects having no AD symptoms at the beginning of the clinical evaluation. Scorings were performed on days 0, 56, 112, and 168. (A) Scoring of AD signs in the control group. (B) Scoring of AD signs in the group of subjects using the product. For the statistical significance: LS: 0.01<p ≤0.05, * p<0.05, and ** p<0.01. |
Finally, the quality of life assessment by subjects improves in both groups (Figure 4). Still, the decrease in the DLQI score is much more rapid and important in the group using the product (−97.2% at day 56, p<0.001) than in the control group (maximum decrease: −88.1% at day 168, p<0.001). Besides, the score reached after 168 days is 140 folds lower upon product use (p=0.005).
 |
Figure 4 Quality of life assessment from subjects having no AD symptoms at the beginning of the clinical evaluation. Scorings were performed on days 0, 56, 112, and 168 by subjects of the control group (in white) and the group using twice daily the product (in black). For the statistical significance: *** p<0.001. |
Discussion
AD is a complex disease encompassing epidermal barrier dysfunction, immune dysregulation, and microbiome dysbiosis.15,16 Flare-up treatments have been extensively studied.17 Yet, research on relapse prevention is sparse. Some medical treatments are available.18 However, besides probiotics, whose benefits are debated,19 one of the best prevention remains emollient applications. They prolong time to flares-up, reduce flare-up frequency, and the amount of corticosteroid to treat them.11 As long as they do not contain irritants, all moisturizers have beneficial effects,11 indicating that restoring the skin barrier to prevent inflammation is essential. Studies on emollients did not focus on eyelids, which are frequently affected and where symptoms strongly impact the quality of life. It also involves skin with specific characteristics. The product evaluated in this study aims at filling this gap as it was specifically developed to maintain, restore, and reinforce the eyelid skin barrier function and prevent inflammation.
In subjects without AD, a single application has a soothing effect upon the induction of mechanical or chemical stresses. It also reduces TEWL when applied for 28 days. On subjects with eyelid AD symptoms, it significantly improves all signs evaluated. Not only does it do so upon objective evaluation, but also when subjects assess symptoms severity. Another important aspect is that for subjects prone to AD but showing no symptoms, the product drastically reduces the number of relapses. If no improvement of AD signs was evidenced by subjects having no AD symptoms, the Dermatological Life Quality Index evaluated by subjects improved more and faster upon product use. Even if we only monitored AD at the level of eyelids, precluding us from analyzing the impact of relapses on other body sites, the DLQI difference observed can only be attributed to the product-induced decrease in eyelid AD.
Focusing on the ingredients other than those entering the composition of the cream base (ingredients that are supposed to have no or limited effect), the product’s composition (Table 1) can explain these results. Based on the importance of skin hydration, it contains high molecular weight hyaluronic acid that can retain 1000 times its weight in water.20 Applied to the epidermis, high molecular weight hyaluronic acid does not penetrate the skin but forms a non-occlusive film regulating water fluxes.21 The aqueous phase also contains humectants – dipropylene glycol and glycerin – that complete the hydrating action thanks to their hygroscopic properties. Multifunctional, these polyols also have a preservative effect by decreasing the amount of water available for micro-organisms development.
The product also includes a lipid complex to maintain/restore the stratum corneum lipids. This complex consists of a blend of refined sunflower and rapeseed oils, known to penetrate and influence skin structure and functioning.22,23 Moreover, this mixture contains omega-3 and −6 essential fatty acids. Among other roles, they are key to the differentiation, maturation, and barrier function of the stratum corneum, the formation and secretion of lamellar bodies, and the inhibition of inflammation.24 The lipid complex also contains biomimetic lipids: ceramides, cholesterol, and phytosphingosine, which are major stratum corneum lipids.25,26 Present in the product as a multi-lamellar emulsion similar to the in vivo organization of skin lipids, these three compounds are essential for epidermal differentiation and barrier function.26–28 Phytosphingosine is also a base for ceramide synthesis and induces key proteins deficient in AD (filaggrin, involucrin).29,30 Besides, it has an anti-inflammatory action by binding to PPARs (peroxisomal proliferator-activated receptors) and inhibiting the release of pro-inflammatory cytokines.31 Yet, phytosphingosine is not the only component known for its anti-inflammatory action as the product also contains 18ß-glycyrrhetinic acid. Glycyrrhetinic acid has a direct anti-inflammatory action by lowering the secretion of inflammatory mediators and reducing histamine synthesis and release.32–34 It also has an indirect action by maintaining cortisol in its active form due to its capacity to inhibit 11β-hydroxysteroid dehydrogenase (11β-HSD).35
The product also contains ingredients meant to improve skin tolerance by acting on various mechanisms. Xylitol increases skin hydration by stimulating filaggrin expression, the natural moisturizing factor (NMF) precursor.36 Mannitol, a mannose derivative, was shown to have excellent free radical scavenging properties in isolated human keratinocytes, limiting oxidative damage.37 Rhamnose, by its capacity to bind to the lectins of keratinocytes, decrease IL-8 secretion, thus reducing the spread of inflammation.38 Laminaria ochroleuca extract is a natural skin-soothing ingredient that reduces irritation-induced inflammation by boosting the skin’s immune response.39 The last ingredient, fructooligosaccharides, is a recognized prebiotic, which has been shown to restrict the growth of potentially harmful bacteria in favour of beneficial ones in vitro, therefore having a positive role in preserving or restoring a healthy skin microbiome.40
In summary, the product was developed with an ecobiological approach. Natural skin mechanisms inspire its composition to reinforce them, help protect the cutaneous ecosystem by reducing inflammation and pruritus, as well as stimulating the synthesis of lipids and proteins essential for the barrier function. It also provides biomimetic lipids and hygroscopic molecules that immediately protect the skin from external aggression and prevent water loss. Altogether, ingredients aim at rebalancing the cutaneous ecosystem to strengthen it against AD-inducing factors and avoid over-reaction, thus contributing to better symptom healing and decreased relapse frequency.
Finally, the product has two additional properties not evaluated in this study. It includes sucrose stearate, a compound preventing Staphylococcus aureus biofilm formation,41,42 thus helping the skin to balance its microbiome. This activity could be significant considering the prevalence of S. aureus in AD lesions,43–45, and could have participated in relapse prevention. Further, the richness of the product in fatty acids provides makeup-removing properties. Therefore, it is not only a daily care and hygiene product but also a cleanser that avoids multiple scratches on eyelids and prevents triggering itch-scratch cycles.
Conclusion
Results show that a daily care and hygiene routine with a dermo-cosmetic product designed according to an ecobiological approach and aimed at maintaining and restoring the epidermis structure leads to objective improvement of AD and subjective perception of quality of life. Determining the actual role of the various ingredients would be of interest, as would be comparing the product with emollients. Having anti-inflammatory properties, testing the product on subjects affected by other dermatitis, such as irritant contact dermatitis, would also be relevant.
Acknowledgments
Authors wish to thank Dermscan Poland, especially Aleksandra Taraszkiewicz and Ewa Karamon, for data collection and preliminary analysis. They are also thankful to Christelle Graizeau, Santana Thach and Marlène Chavagnac for critical reading of the manuscript. They wish to thank Dr Philippe Crouzet, Estium-Concept, for scientific writing services.
Funding
The present study was funded by NAOS, France.
Disclosure
All authors are full-time employees of NAOS Group.
References
1. Barbarot S, Auziere S, Gadkari A, et al. Epidemiology of atopic dermatitis in adults: results from an international survey. Allergy. 2018;73(6):1284–1293. doi:10.1111/all.13401
2. Silverberg JI, Barbarot S, Gadkari A, et al. Atopic dermatitis in the pediatric population: a cross-sectional, international epidemiologic study. Ann Allergy Asthma Immunol. 2021;126:417–428.e2.
3. Dawn A, Papoiu ADP, Chan YH, et al. Itch characteristics in atopic dermatitis: results of a web-based questionnaire. Br J Dermatol. 2009;160:642–644.
4. Simpson EL, Bieber T, Eckert L, et al. Patient burden of moderate to severe atopic dermatitis (AD): insights from a phase 2b clinical trial of dupilumab in adults. J Am Acad Dermatol. 2016;74:491–498.
5. Paller A, Jaworski JC, Simpson EL, et al. Major comorbidities of atopic dermatitis: beyond allergic disorders. Am J Clin Dermatol. 2018;19:821–838.
6. Zeppa L, Bellini V, Lisi P. Atopic dermatitis in adults. Dermatitis. 2011;22:40–46.
7. Silvestre Salvador JF, Romero-Pérez D, Encabo-Durán B. Atopic dermatitis in adults: a diagnostic challenge. J Investig Allergol Clin Immunol. 2017;27:78–88.
8. Buchanan AG, Holds JB. The beautiful eye: perception of beauty in the periocular area. In: Massry G, Murphy M, Azizzadeh B, editors. Master Techniques in Blepharoplasty and Periorbital Rejuvenation. New York: Springer; 2011:25–29.
9. Dailey RA, Wobig JL. Eyelid anatomy. J Dermatol Surg Oncol. 1992;18:1023–1027.
10. Pratchyapruit W, Kikuchi K, Gritiyarangasan P, Aiba S, Tagami H. Functional analyses of the eyelid skin constituting the most soft and smooth area on the face: contribution of its remarkably large superficial corneocytes to effective water-holding capacity of the stratum corneum. Skin Res Technol. 2007;13(2):169–175. doi:10.1111/j.1600-0846.2007.00183.x
11. van Zuuren EJ, Fedorowicz Z, Christensen R, et al. Emollients and moisturisers for eczema. Cochrane Database Syst Rev. 2017;2:CD012119.
12. Dréno B. The microbiome, a new target for ecobiology in dermatology. Eur J Dermatol. 2019;29:15–18.
13. Radman M. Ecobiological approach to research regarding ageing and diseases. Eur J Dermatol. 2019;29:11–14.
14. Polena H, Chavagnac-Bonneville M, et al. Improvement of quality of life in dialysis and diabetic patients by skin dryness and pruritus management with an ecobiological dermo-cosmetic product. Clin Cosmet Investig Dermatol. 2022;15:2143–2152.
15. Wollenberg A, Kraft S, Oppel T, et al. Atopic dermatitis: pathogenetic mechanisms. Clin Exp Dermatol. 2000;25:530–534.
16. Weidinger S, Beck LA, Bieber T, et al. Atopic dermatitis. Nat Rev Dis Primers. 2018;4:1.
17. Bieber T. Atopic dermatitis: an expanding therapeutic pipeline for a complex disease. Nat Rev Drug Discov. 2022;21:21–40.
18. Berke R, Singh A, Guralnick M. Atopic dermatitis: an overview. Am Fam Physician. 2012;86:35–42.
19. Jiang W, Ni B, Liu Z, et al. The role of probiotics in the prevention and treatment of atopic dermatitis in children: an updated systematic review and meta-analysis of randomized controlled trials. Paediatr Drugs. 2020;22:535–549.
20. Pavicic T, Gauglitz GG, Lersch P, et al. Efficacy of cream-based novel formulations of hyaluronic acid of different molecular weights in anti-wrinkle treatment. J Drugs Dermatol. 2011;10:990–1000.
21. Essendoubi M, Gobinet C, Reynaud R, et al. Human skin penetration of hyaluronic acid of different molecular weights as probed by Raman spectroscopy. Skin Res Technol. 2016;22:55–62.
22. Lodén M. Biophysical properties of dry atopic and normal skin with special reference to effects of skin care products. Acta Derm Venereol Suppl. 1995;192:1–48.
23. Lodén M, Andersson AC. Effect of topically applied lipids on surfactant-irritated skin. Br J Dermatol. 1996;134:215–220.
24. Balić A, Vlašić D, Žužul K, Marinović B, Bukvić Mokos Z. Omega-3 versus omega-6 polyunsaturated fatty acids in the prevention and treatment of inflammatory skin diseases. Int J Mol Sci. 2020;21:741.
25. Feingold KR. Thematic review series: skin lipids. The role of epidermal lipids in cutaneous permeability barrier homeostasis. J Lipid Res. 2007;48:2531–2546.
26. Coderch L, López O, de la Maza A, et al. Ceramides and skin function. Am J Clin Dermatol. 2003;4:107–129.
27. Brod J. Characterization and physiological role of epidermal lipids. Int J Dermatol. 1991;30:84–90.
28. Choi HK, Cho YH, Lee EO, et al. Phytosphingosine enhances moisture level in human skin barrier through stimulation of the filaggrin biosynthesis and degradation leading to NMF formation. Arch Dermatol Res. 2017;309:795–803.
29. Sigruener A, Tarabin V, Paragh G, et al. Effects of sphingoid bases on the sphingolipidome in early keratinocyte differentiation. Exp Dermatol. 2013;22:677–679.
30. Choi HK, Cho YH, Lee EO, et al. Phytosphingosine enhances moisture level in human skin barrier through stimulation of the filaggrin biosynthesis and degradation leading to NMF formation. Arch Dermatol Res. 2017;309:795.
31. Pavicic T, Wollenweber U, Farwick M, et al. Anti-microbial and -inflammatory activity and efficacy of phytosphingosine: an in vitro and in vivo study addressing acne vulgaris. Int J Cosmet Sci. 2007;29:181–190.
32. Wang CY, Kao TC, Lo WH, et al. Glycyrrhizic acid and 18ß-glycyrrhetinic acid modulate lipopolysaccharide-induced inflammatory response by suppression of NF-κB through PI3K p110δ and p110γ inhibitions. J Agric Food Chem. 2011;59:7726–7733.
33. Lee YM, Kim YC, Kim HM. Effect of glycyrrhetinic acid on histamine synthesis and release. Arch Pharm Res. 1996;19:36–40.
34. Kowalska A, Kalinowska-Lis U. 18β-Glycyrrhetinic acid: its core biological properties and dermatological applications. Int J Cosmet Sci. 2019;41:325–331.
35. Teelucksingh S, Mackie AD, Burt D, et al. Potentiation of hydrocortisone activity in skin by glycyrrhetinic acid. Lancet. 1990;335:1060–1063.
36. Korponyai C, Kovács RK, Erös G, et al. Antiirritant properties of polyols and amino acids. Dermatitis. 2011;22:141–146.
37. Pelle E, Huang X, Mammone T, et al. Ultraviolet-B-induced oxidative DNA base damage in primary normal human epidermal keratinocytes and inhibition by a hydroxyl radical scavenger. J Invest Dermatol. 2003;121:177–183.
38. Baba T, Yoshida T, Yoshida T, et al. Suppression of cell-mediated immune reactions by monosaccharides. J Immunol. 1979;122:838–841.
39. Ferreira MS, Resende DISP, Lobo JMS, et al. Marine ingredients for sensitive skin: market overview. Mar Drugs. 2021;19:464.
40. Le Bourgot C, Meunier C, Gaio E, et al. Effects of short chain fructo-oligosaccharides on selected skin bacteria. Sci Rep. 2022;12:9702.
41. Gayraud F, Sayag M, Jourdan E. Efficacy and tolerance assessment of a new type of dermocosmetic in infants and children with moderate atopic dermatitis. J Cosmet Dermatol. 2015;14:107–112.
42. Callejon S, Gayraud F, Chavagnac-Bonneville M, et al. S. aureus biofilm formation to reduce the occurrence and the severity of flares-up in children with atopic dermatitis. EADV Meeting. 2021;1:548.
43. Di Domenico EG, Cavallo I, Bordignon V, et al. Inflammatory cytokines and biofilm production sustain Staphylococcus aureus outgrowth and persistence: a pivotal interplay in the pathogenesis of Atopic Dermatitis. Sci Rep. 2018;8:9573.
44. Di Domenico EG, Cavallo I, Capitanio B, et al. Staphylococcus aureus and the cutaneous microbiota biofilms in the pathogenesis of atopic dermatitis. Microorganisms. 2019;7:301.
45. Geoghegan JA, Irvine AD, Foster TJ. Staphylococcus aureus and atopic dermatitis: a complex and evolving relationship. Trends Microbiol. 2018;26:484–497.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.