")
Back to Journals » Psychology Research and Behavior Management » Volume 15
Evaluation of the Behavioral and Psychological Symptoms in Patients with Vitiligo in China
Authors Ning X, Zhang Y, Wang W, Yan H, Xia Y
Received 13 April 2022
Accepted for publication 3 August 2022
Published 11 August 2022 Volume 2022:15 Pages 2107—2116
DOI https://doi.org/10.2147/PRBM.S370445
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Xiaoying Ning, Yanfei Zhang, Wei Wang, Huling Yan, Yumin Xia
Department of Dermatology, the Second Affiliated Hospital of Xi’an Jiaotong University, Xi’an, People’s Republic of China
Correspondence: Yanfei Zhang, Department of Dermatology, the Second Affiliated Hospital of Xi’an Jiaotong University, Xi’an, People’s Republic of China, Email [email protected]
Background: Vitiligo is a common, acquired depigmenting disorder. The pathogenesis is not clear, neuropsychological factors may be involved. Vitiligo will affect the individual’s physical and psychological health, leading to different levels of psychological behavior problems. However, there are few research on psychological symptoms in patients with vitiligo in China.
Methods: Adult patients with vitiligo were selected in convenient sampling method from March 2019 to November 2019 from the dermatology clinic. They were evaluated by the DLQI (Dermatology Life Quality Index), SCL-90 (Symptom Checklist-90), SADS (Social Avoidance and Distress Scale) and MCMQ (Medical Coping Modes Questionnaire).
Results: The DLQI score was 7.56 ± 6.11, which was in the third level. The SCL-90 score of patients with vitiligo was 136.44 ± 39.19, significantly higher than the Chinese norms (P < 0.05), and it mainly manifested as interpersonal sensitivity, depression, anxiety and phobia, which may be affected by the patient’s gender, marital status, severity of disease, stage and location of skin lesions. The total score of SADS in patients was 10.30 ± 6.38. The total score and scores in all dimensions of SADS were significantly higher than the Chinese norms (all P < 0.05), which were related with the patient’s gender, educational attainment, severity, type and stage of skin lesions. For MCMQ, the facing score was significantly lower than the Chinese norms (P < 0.05), and the avoiding and yielding scores were significantly higher than the Chinese norms (all P < 0.05).
Conclusion: In China, vitiligo affects the patient’s quality of life to varying degrees, resulting in a series of psychological and behavioral problems. We should actively concern and improve the psychological health status and behavior of patients, and multidisciplinary treatment strategies and education about vitiligo should be given to the patients.
Keywords: vitiligo, quality of life, psychological health status, behavioral and psychological symptoms
Introduction
Vitiligo is a common depigmentation skin disease due to the loss of melanocytes.1 The clinical manifestations are depigmentation spots of different sizes in skin and mucosa, which can be involved in any part of the body and hair. The incidence of vitiligo in the whole world is about 0.5–1% and the incidence varies from race to region and population.2,3 Skin lesions range from very limited to generalized. It also is a disfigurement disease. In addition to affecting individual mental and physical health, it also increases the economic burden of patients and their families, and affects the quality of life of patients.4
The etiology and pathogenesis of vitiligo are very complex. It is generally believed that individuals with genetic tendency show abnormalities in autoimmunity, oxidative stress, endocrine metabolism, neuropsychiatric and other aspects under the stimulation of a variety of inflammatory factors, resulting in melanin synthesis disorder or melanocyte destruction, and finally lead to depigmentation.1 Vitiligo is often misunderstood as a cosmetic disease.5 A large number of clinical practice have shown that patients with vitiligo often have stress events such as overwork, tension, anxiety and mental trauma before the onset of vitiligo.6,7 Psychosocial conditions affect the immune system and play a role in the disease process. More and more attention has been paid to the role of psychosocial factors in the occurrence and development of psychosomatic diseases. Researches on the psychosocial factors in vitiligo have been reported.7–9 Therefore, vitiligo is a skin psychological disease that will not directly lead to physical damage, but will lead to serious psychological problems in daily life.10
In general, clarifying the psychological and behavioral characteristics of patients with vitiligo, understanding their potential psychological and behavioral symptoms (such as anxiety, depression and social disorder), can help optimize the management of vitiligo, improve the treatment effect, improve the quality of life and promote their physical and mental health development.11
However, there are few researches on psychological symptoms in patients with vitiligo in China. This study aim to investigate the psychological and behavioral status in patients with vitiligo in China through psychological and behavioral related questionnaires, analyze the influencing factors of psychological and behavioral problems, and provide theoretical basis for comprehensive treatment and clinical intervention of vitiligo.
Methods
Ethics
The study and protocols were approved by the Institutional Review Board of the Xi’an Jiaotong University, and performed according to guidelines governing ethics care in China. This study was performed in accordance with the rules laid down in the Declaration of Helsinki. Informed consent has been obtained from all patients for study participation, data collection and publication.
Participants
The convenient sampling method was used to select adult patients with vitiligo who came to the dermatology clinic of the Second Affiliated Hospital of Xi’an Jiaotong University from March 2019 to November 2019 as the research object. The inclusion criteria were: 1. All patients were over 18 years old. 2. The diagnosis of vitiligo was made by two dermatologists and wood lamp. 3. All patients had no previous history of mental illness. 4. All patients had no cognitive orientation disorder, had primary school education or above, and could understand the meaning of the questionnaires. 5. All patients voluntarily participated, and expressed their willingness to cooperate to complete the questionnaires carefully. Exclusion criteria were: 1. Patients were under 18 years old. 2. Patients with other skin diseases or major physical or neurological diseases (tumors, heart problems, liver and kidney dysfunction, epilepsy, etc.) that may impair their quality of life or psycho-behavioral status.
Measures
The initial sample consisted of 120 participants, after eliminating the questionnaires invalidated by their incorrect completion, the final sample was 117 (97.5%) in this study. The researcher gave explanation and guidance when necessary. All questionnaires were filled in on site and completed by the patients themselves. All patients who met the inclusion criteria were evaluated by general information questionnaire, dermatology quality of life index (DLQI), symptom checklist 90 (SCL-90), social avoidance and distress scale (SADS) and medical coping style scale (MCMQ). All questionnaires were in Chinese and the validated forms were used.
DLQI is currently the most widely used dermatological life quality questionnaire. It includes 10 questions related to symptoms and feelings, daily activities, leisure, work and school, interpersonal relationship and treatment, to evaluate the impact of skin diseases on patients’ quality of life during the previous 1 week.12 According to the total score of DLQI, the score is divided into 5 grades. 0~1 indicates almost no influence, 2~5 indicates small influence, 6~10 indicates moderate influence, 11~20 indicates very large influence, and 21~30 indicates extremely large influence.
The SCL-90 scale is used for self-assessment by people over the age of 16 and is one of the most well-known mental health testing scales in the world. It consists of 90 items, assessed from 10 factors of somatization, obsessive-compulsive, interpersonal sensitivity, depression, anxiety, hostility, phobia, paranoid ideation, psychoticism, sleeping and eating state. According to their self-perception of the psychological state, the subjects rate their symptoms using a scale ranging from 1 to 5 on a scale corresponding to “none”, “very light”, “moderate”, “heavy”, and “severe”. The higher the score, the worse the mental health of the subject.13
SADS was compiled by Waston et al in 1969, and the Chinese version was revised by Hong Ma et al, which has been proved to have good reliability and validity.14 The scale consists of 28 items, including two dimensions of social avoidance and social distress, with 14 questions for each dimension and the score range from 0 to 28 points. The higher the score, the more severe the degree of social avoidance and distress.
MCMQ was formed into a formal Chinese version of the questionnaire by Qianjin Jiang et al, combined with the original Chinese translation version and revised several times.15 Twenty items are assigned to three coping styles: facing (8 items), avoiding (7 items) and yielding (5 items). Using a four-point scoring method (1–4 points), the total score is 20 to 80 points, and the higher the subscale score, the more obvious the coping style.
Statistical Analyses
The collected data were entered into excel and checked by two investigators, and the data were statistically analyzed by SPSS 18.0 statistical software. The mean ± standard deviation was used to describe the measurement data. Single sample t-test, one way analysis of variance (ANOVA) and two independent sample t-test were used to compare the differences. Spearman two-variable correlation analysis was used to analyze the correlation. P < 0.05 was statistically significant.
Results
Basic Demographic Data
As shown in Table 1, a total of 117 patients completed the questionnaires, including 49 males (41.9%) and 68 females (58.1%). The ratio of men to women was 1:1.39. Most patients (67.5%) were younger than 40 years old and had no positive family history (76.9%). For severity of disease, 65.8% patients were mild. More than half of the patients (58.1%) were in progressive stage and 12.0% in rapid progress stage.
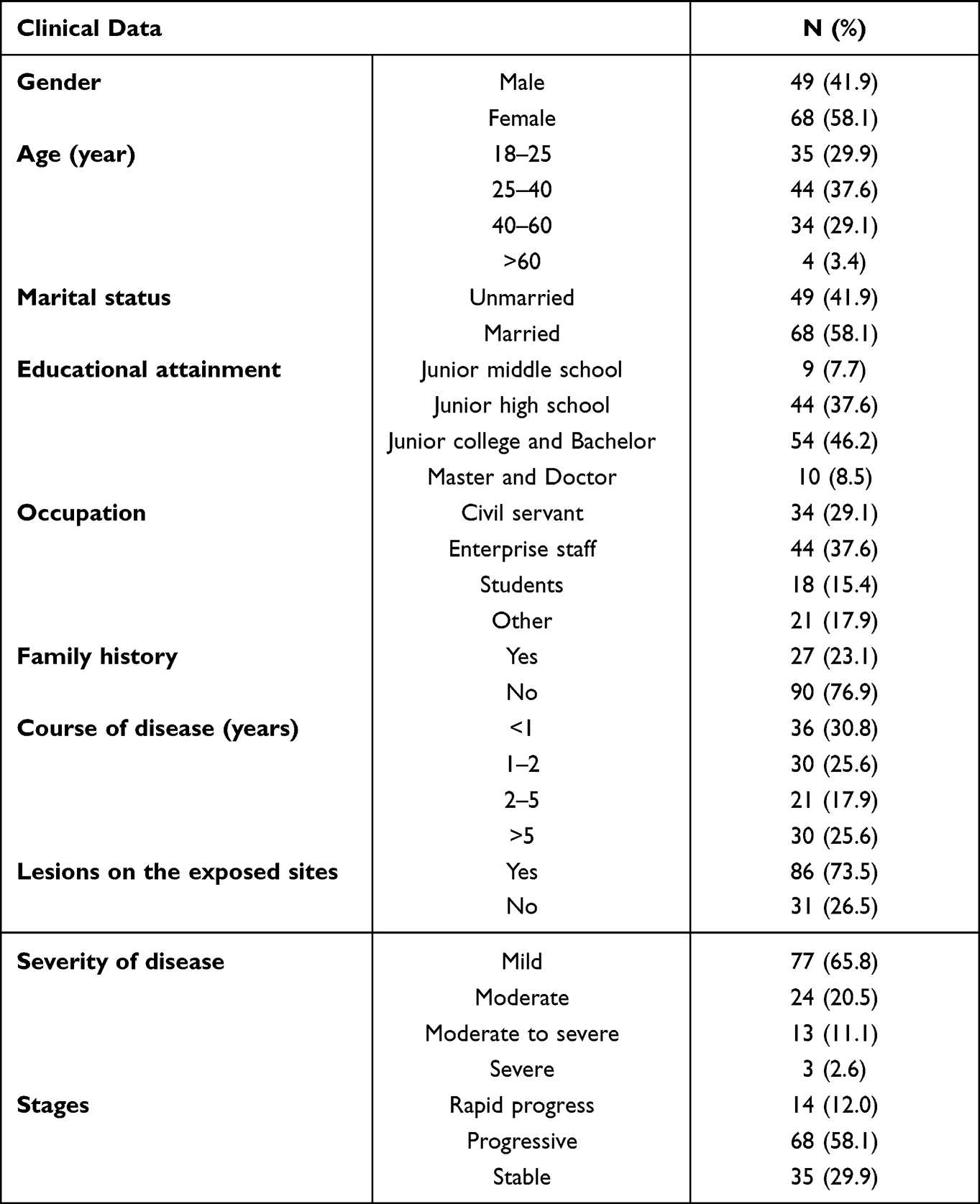 |
Table 1 Demographic Data of Patients with Vitiligo |
DLQI Scores of Patients with Vitiligo
The DLQI scores of 117 patients with vitiligo in this survey ranged from 0 to 26 points, and the mean score was 7.56 ± 6.11. 15 of 117 patients (12.8%) had a score of 0–1, indicating that vitiligo had almost no impact on their quality of life, and 39 patients scored 2–5, up to 33.3%, 31 patients (26.5%) had a score of 6–10, meaning that vitiligo had a moderate impact on them. There were 25 (21.4%) patients with 11–20 points. 7 (6.0%) scored more than 20, which impacted of the quality of life greatly, see Figure 1.
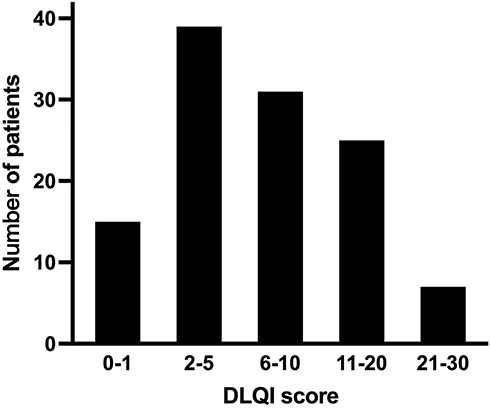 |
Figure 1 The distribution of DLQI (dermatology quality of life index) scores of patients with vitiligo. |
Mental Health Status and Univariate Analysis of Patients with Vitiligo
The mental health status of 117 patients with vitiligo was evaluated by SCL-90 questionnaire. As shown in Table 2, the mean score was 136.44 ± 39.19, which was significantly higher than the Chinese norm of SCL-90 (129.19 ± 40.25)13 (P < 0.05). Among the 10 factors, the scores of depression, anxiety, interpersonal sensitivity and phobia were significantly higher than the Chinese norms13 (all P < 0.05).
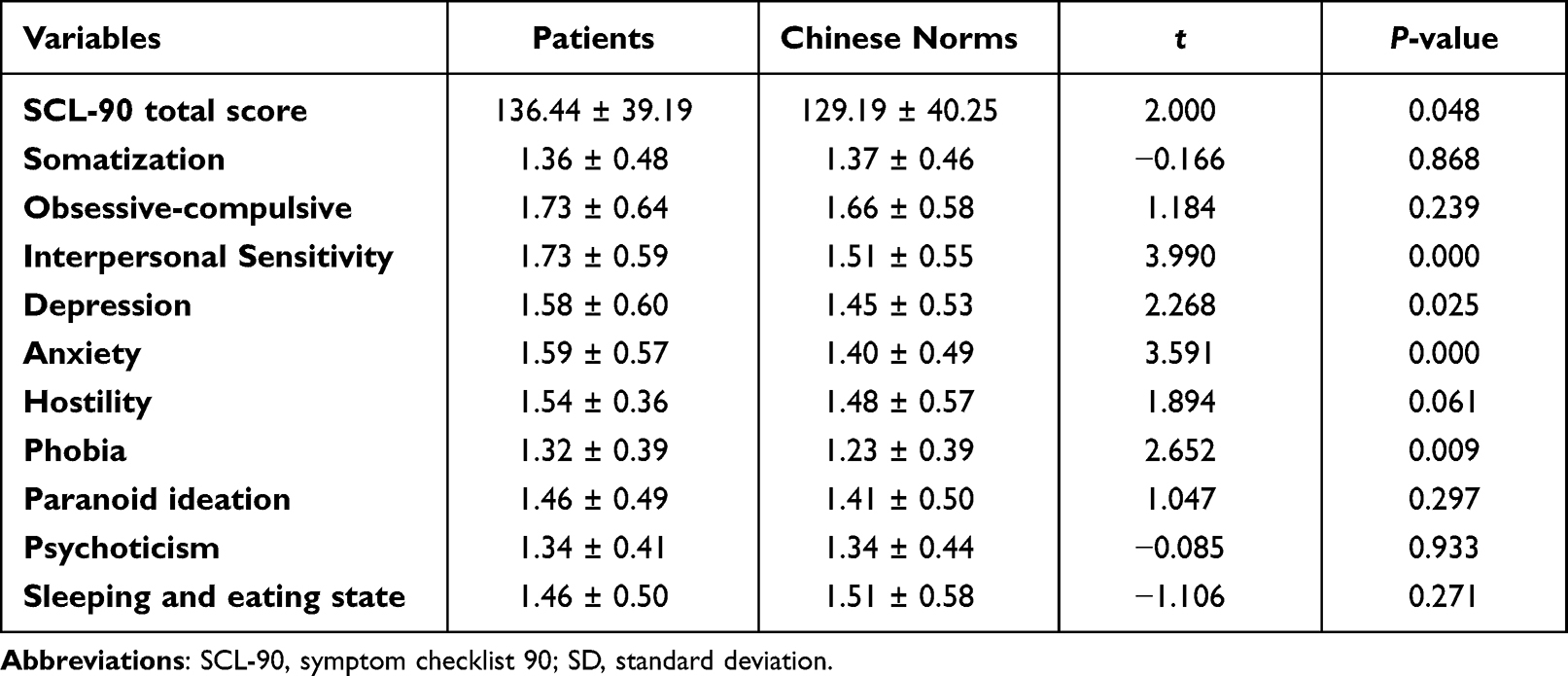 |
Table 2 Comparison Between SCL-90 Score in Patients with Vitiligo and Chinese Norms (mean±SD) |
For Single factor analysis, as shown in Table 3, in terms of the total score of SCL-90 and the scores of interpersonal sensitivity, depression, anxiety and phobia, it was found that female patients were significantly higher than those of men (P < 0.05), the married group were lower than those in the unmarried group (P < 0.05), the patients in rapid progression stage were significantly higher than those in progressive and stable stage (P < 0.05), and patients with skin lesions on the exposed site also scored significantly higher compared with those without exposed lesions (P < 0.05). In addition, it was found that there were significant differences in interpersonal sensitivity and depression scores among patients with different diseases severity (both P < 0.05).
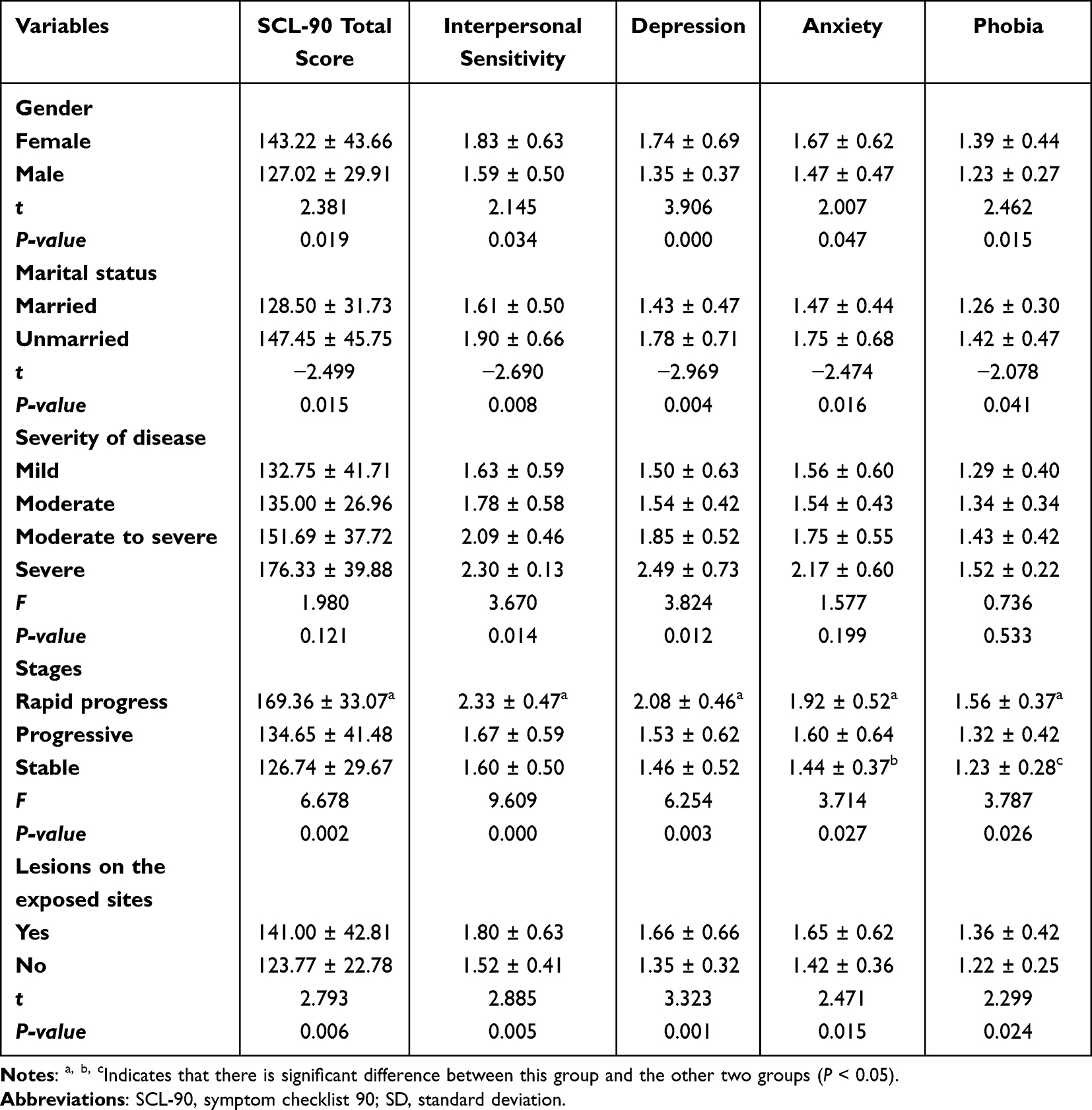 |
Table 3 Univariate Analysis of Patients with Vitiligo in the Score of Total SCL-90 and Interpersonal Sensitivity, Depression, Anxiety and Phobia (Mean ± SD) |
Social Status and Univariate Analysis of Patients with Vitiligo
The scores of SADS in 117 patients with vitiligo in this survey ranged from 0 to 26, the mean score was 10.30 ± 6.38, and the mean score of social avoidance was 5.13 ± 3.38 and social distress was 5.17 ± 3.67. Compared with the Chinese norm,14 it was found that the differences were statistically significant (P < 0.05), see Table 4.
 |
Table 4 Comparison Between SADS Score in Patients with Vitiligo and Chinese Norms (mean±SD) |
For single factor analysis of social status of patients with vitiligo, the score of social avoidance in women was higher than that in men (5.69 ± 3.39 vs 4.35 ± 3.24, t = 2.156, P = 0.033). The total scores of SADS and social distress in the junior middle school group were significantly higher than those in the other three groups (all P < 0.05). For severity of disease, the total SADS and social avoidance scores in mild group were significantly lower than that of severe group (all P < 0.05). The total score of SADS, social avoidance and social distress score of patients in rapid progressive stage were significantly higher than those in the other two groups (P < 0.05), see Table 5.
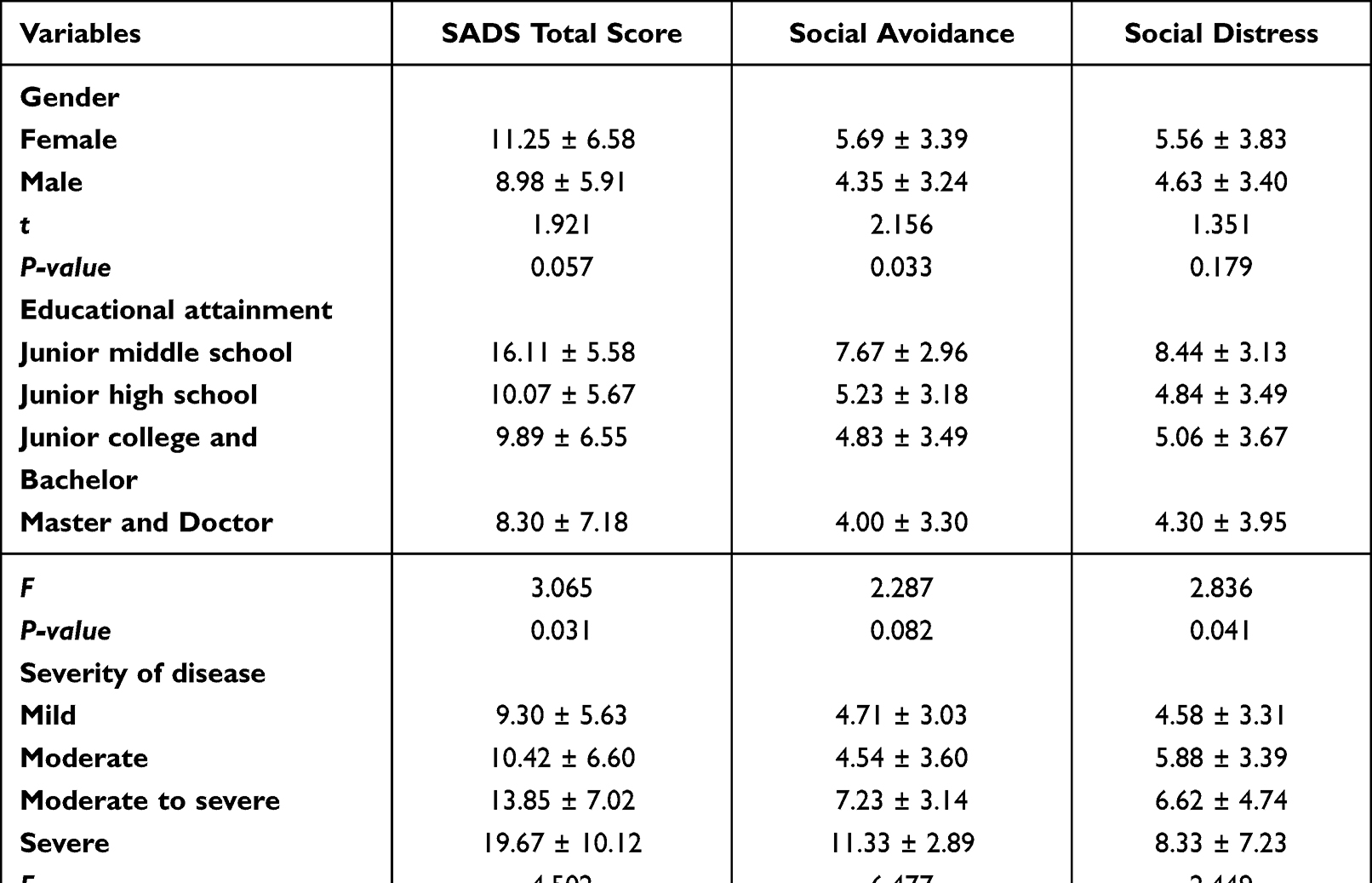 |
Table 5 Univariate Analysis of Patients with Vitiligo in the Score of Total SADS, Social Avoidance and Social Distress (mean±SD) |
Medical Coping Mode in Patients with Vitiligo
The score of face coping was lower than the Chinese norm,15 and the scores of yield coping and avoidance coping were higher than the Chinese norm (P < 0.05), see Table 6.
 |
Table 6 Comparison Between MCMQ Score in Patients with Vitiligo and Chinese Norms (mean±SD) |
Impact of Medical Coping Style on Patients’ Mental Health
As shown in Table 7, yield coping and avoidance coping were positively correlated with the scores of interpersonal sensitivity, depression, anxiety and phobia (all P < 0.05). Face coping was negatively correlated with social avoidance and distress (P < 0.05), and yield coping and avoidance coping were positively correlated with social avoidance and distress (all P < 0.05), see Table 8.
 |
Table 7 Impact of Medical Coping on Patients’ Mental Health |
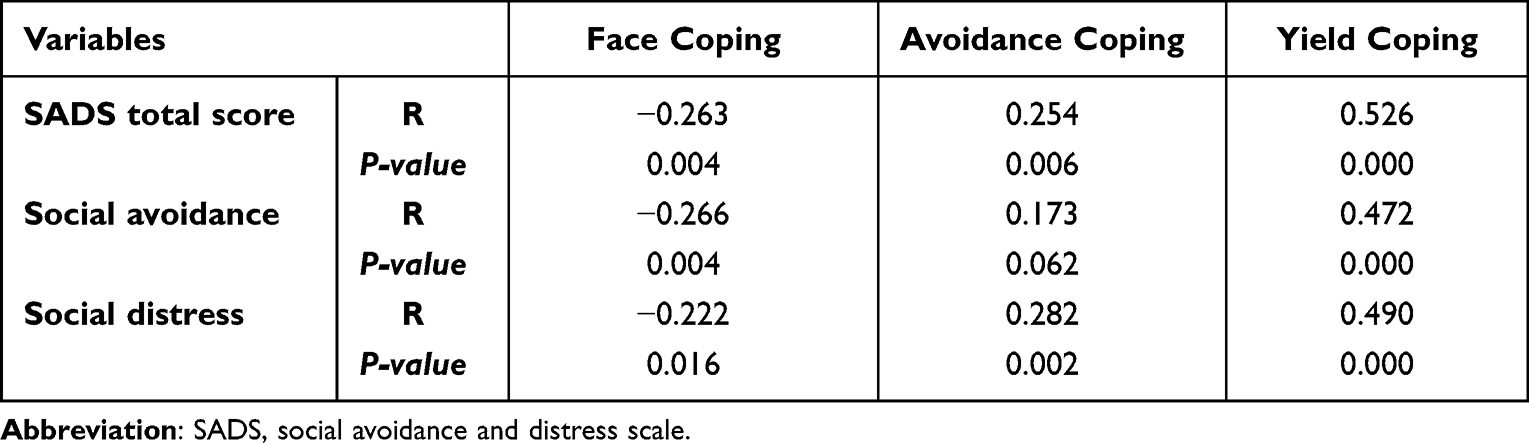 |
Table 8 Impact of Medical Coping on Patients’ Social Status |
Discussion
Vitiligo is a common acquired depigmentation skin and mucous membrane disease, which can involve hair follicles. This disease is easy to diagnose, but difficult to treat. Repeated recurrence, and the change of appearance will damage the physical and mental health of patients to varying degrees.
Vitiligo will not bring serious health problems to patients, but lead to serious cosmetic problems. Many studies have shown that vitiligo lesions have a certain impact on the quality of life of patients.16,17 Consistent with the DLQI score in the world,17 the overall average score was 8.2, which was in the third level. The DLQI score of the 117 patients investigated in our study was (7.56 ± 6.11), in the third-level effect, indicating that vitiligo had a moderate impact on the quality of life of patients. DLQI scores are concentrated in 2–20 points, which is in the second to fourth level of influence. It is worth noting that 32 (27.4%) patients had DLQI scores higher than 10 in our research, indicating that the disease had a great impact on their quality of life. The change of appearance will affect the personality characteristics and social relations of patients to a certain extent. Studies have shown that the quality of life of patients with vitiligo is significantly related to their psychological distress and mental health.18 Importantly, the quality of life of vitiligo may be largely affected by psychosocial comorbidity.19
Skin plays an important role in our interaction with the world, and skin color is an important factor in perceiving someone’s health.20 The results of our study showed that the total score of SCL-90 was 136.44, which is significantly higher than the Chinese norm. The mental health problems of patients with vitiligo in China are mainly manifested as interpersonal sensitivity, depression, anxiety and phobic anxiety. In this study, the total scores and all dimensions of SADS in vitiligo patients were significantly higher than the Chinese norms, indicating that compared with the general population, vitiligo patients had obvious social distress and social avoidance.
Many studies have shown that vitiligo has a greater impact on women’s mental health, and women are more prone to have mental symptoms and social disorders. Vitiligo sufferers experience limited participation in social interactions, job opportunities, religious activities, making friends, etc., showing significant social anxiety and avoidance.21 Compared with men, women experienced severe social distress, anxiety, and avoidance. In the study of Sawant,22 it was found that the degree of helplessness, depression and anxiety, social anxiety/avoidance and participation restriction of women were significantly higher than that of men. In our study, the scores of interpersonal sensitivity, depression, anxiety, phobia and social avoidance in women were significantly higher than men. Men and women have different psychosocial reactions to vitiligo. Women may pay more attention to their self-image, have more sensitive thoughts, and are more likely to feel embarrassed and ashamed of the reactions of people around them. Adverse emotional reactions make them become more helpless and negative when face to diseases. They take the initiative to avoid some social activities and avoid going out to contact with people. Moreover, men and women have different understanding and value to the relationship between marriage and love. Female patients are more worried about the impact of vitiligo on their mate selection and marital status, and the social acceptance of women suffering from vitiligo is low, which makes them more vulnerable.
Studies have shown that vitiligo has a negative impact on patients’ life and marital status. Patients with vitiligo feel troubled and ashamed when they start sexual relations and emotional experience.10 Our study showed that unmarried patients have more negative symptoms of interpersonal sensitivity, depression, anxiety and phobia than married patients. The score of social avoidance and distress were slightly higher than that of married people, but the difference is not significant, indicating that both unmarried people and married people all suffer from social distress and avoidance. Education level is an important demographic characteristic of an individual, which affects person’s cognitive behavior to a great extent. A study showed that the higher the level of education, the more the patients can rationally understand the disease and reduce the burden caused by the disease.23 Consistent with the results of our study, the scores of interpersonal sensitivity, depression, anxiety, phobia, social avoidance and distress of patients with junior high school education are higher than those with senior high school, junior college, undergraduate, graduate and above education. With the increase of disease severity, the scores of vitiligo patients in interpersonal sensitivity, depression, anxiety, phobia, social avoidance and distress showed an upward trend. Patients with severe pigmented diseases have an increased frequency of mental illness.24 The scores of interpersonal sensitivity, depression, anxiety, phobia, social avoidance and distress in skin lesions with rapid progression were significantly higher than those in progressive and stable stage. The scores of interpersonal sensitivity, depression, anxiety, phobia, social distress and avoidance of patients with skin lesions at the exposed site were higher than those without skin lesions at the exposed site, but only significant difference in the level of mental health, indicating that the mental health status of patients with the exposed lesions was worse than that of patients without lesions at the exposed site.23
In this study, the face coping score of patients with vitiligo was significantly lower than the Chinese norm, and the yield and avoidance coping scores were significantly higher than the Chinese norms. And face coping was negatively correlated with patients’ social avoidance and distress, and yield and avoidance coping were positively correlated with patients’ interpersonal sensitivity, depression, anxiety, phobia, social avoidance and distress. Scholars believe that the psychological intervention treatment of vitiligo should start with the treatment education of patients. Through the education of disease and standardized treatment, we can improve patients’ cognitive level of disease, significantly reduce the anxiety and fear, and increase their belief in actively facing disease.11
Participants with a good understanding of vitiligo were more likely to show a positive attitude toward vitiligo patients than those with insufficient knowledge of the disease.25 In addition to psychotherapy and/or counseling for patients, general education on vitiligo for unaffected people may help to reduce the stigma associated with vitiligo and improve the psychosocial health of patients and their caregivers.
This study also has some limitations: 1. This study only conducted a sampling survey in one hospital. 2. The sample size is limited, resulting in a small number of cases collected in some age, diseases severity and stage. Multicenter and large sample research should be done in the future. 3. We not used VitiQoL tool to analyze the quality of life of patients with vitiligo.26 4. There is no research on the effect of psychotherapy in patients with vitiligo.
Conclusion
In China, vitiligo affects the quality of life of patients to varying degrees, resulting in a series of psychological and behavioral problems, including interpersonal sensitivity, depression, anxiety, phobia, social avoidance and distress, which are mainly affected by the patients’ social demographic situation (gender, marital status, educational level), disease-related situation (stage, severity, whether there are skin lesions at the exposed site) and coping style. At the same time of routine treatment, clinicians should also actively pay attention to and improve the mental health and behavior of patients with vitiligo.
Disclosure
The authors declare no conflict of interest.
References
1. Ezzedine K, Eleftheriadou V, Whitton M, van Geel N. Vitiligo. Lancet. 2015;386(9988):74–84. doi:10.1016/S0140-6736(14)60763-7
2. Talsania N, Lamb B, Bewley A. Vitiligo is more than skin deep: a survey of members of the Vitiligo Society. Clin Exp Dermatol. 2010;35(7):736–739. doi:10.1111/j.1365-2230.2009.03765.x
3. Kruger C, Schallreuter KU. A review of the worldwide prevalence of vitiligo in children/adolescents and adults. Int J Dermatol. 2012;51(10):1206–1212. doi:10.1111/j.1365-4632.2011.05377.x
4. Morrison B, Burden-Teh E, Batchelor JM, Mead E, Grindlay D, Ratib S. Quality of life in people with vitiligo: a systematic review and meta-analysis. Br J Dermatol. 2017;177(6):e338–e339. doi:10.1111/bjd.15933
5. Ezzedine K, Sheth V, Rodrigues M, et al. Vitiligo is not a cosmetic disease. J Am Acad Dermatol. 2015;73(5):883–885. doi:10.1016/j.jaad.2015.07.039
6. Picardi A, Pasquini P, Cattaruzza MS, et al. Stressful life events, social support, attachment security and alexithymia in vitiligo. A case-control study. Psychother Psychosom. 2003;72(3):150–158. doi:10.1159/000069731
7. Lai YC, Yew YW, Kennedy C, Schwartz RA. Vitiligo and depression: a systematic review and meta-analysis of observational studies. Br J Dermatol. 2017;177(3):708–718. doi:10.1111/bjd.15199
8. Osinubi O, Grainge MJ, Hong L, et al. The prevalence of psychological comorbidity in people with vitiligo: a systematic review and meta-analysis. Br J Dermatol. 2018;178(4):863–878. doi:10.1111/bjd.16049
9. Wang G, Qiu D, Yang H, Liu W. The prevalence and odds of depression in patients with vitiligo: a meta-analysis. J Eur Acad Dermatol Venereol. 2018;32(8):1343–1351. doi:10.1111/jdv.14739
10. Bidaki R, Majidi N, Moghadam Ahmadi A, et al. Vitiligo and social acceptance. Clin Cosmet Investig Dermatol. 2018;11:383–386. doi:10.2147/CCID.S151114
11. Taïeb A, Meurant JM. Should we prioritize psychological interventions in the management of vitiligo? J Eur Acad Dermatol Venereol. 2018;32(12):2053–2054. doi:10.1111/jdv.15297
12. Patel KR, Singam V, Vakharia PP, et al. Measurement properties of three assessments of burden used in atopic dermatitis in adults. Br J Dermatol. 2019;180(5):1083–1089. doi:10.1111/bjd.17243
13. Liu YY, Wu SJ, Li YQ, Shao F, Su JK, Liu XF. A survey of mental symptoms of Chinese population based on SCL-90. Chin Ment Health J. 2018;32(5):437–441.
14. Wang XD, Wang XL, Ma H. Manual of mental health assessment scale. Beijing. 1999;13:213–214.
15. Shen XH, Jiang QJ. Report on application of Chinese version of MCMQ in 701 patients. Chin J Behav Med Sci. 2000;9(1):18–20.
16. Gupta V, Sreenivas V, Mehta M, et al. What do vitiligo impact scale-22 scores mean? Studying the clinical interpretation of scores using an anchor-based approach. Br J Dermatol. 2019;180(3):580–585. doi:10.1111/bjd.17040
17. Amer AAA, Gao XH. Quality of life in patients with vitiligo: an analysis of the dermatology life quality index outcome over the past two decades. Int J Dermatol. 2016;55(6):608–614. doi:10.1111/ijd.13198
18. Bonotis K, Pantelis K, Karaoulanis S, et al. Investigation of factors associated with health-related quality of life and psychological distress in vitiligo. J Dtsch Dermatol Ges. 2016;14(1):45–49. doi:10.1111/ddg.12729
19. Ezzedine K, Eleftheriadou V, Jones H, et al. Psychosocial effects of vitiligo: a systematic literature review. Am J Clin Dermatol. 2021;22(6):757–774. doi:10.1007/s40257-021-00631-6
20. Silverberg JI, Silverberg NB. Association between vitiligo extent and distribution and quality-of-life impairment. JAMA Dermatol. 2013;149(2):159–164. doi:10.1001/jamadermatol.2013.927
21. Salman A, Kurt E, Topçuoglu V, et al. Social anxiety and quality of life in vitiligo and acne patients with facial involvement: a cross-sectional controlled study. Am J Clin Dermatol. 2016;17(3):305–311. doi:10.1007/s40257-016-0172-x
22. Sawant NS, Vanjari NA, Khopkar U. Gender differences in depression, coping, stigma, and quality of life in patients of vitiligo. Dermatol Res Pract. 2019;2019:6879412. doi:10.1155/2019/6879412
23. Mishra N, Rastogi MK, Gahalaut P, et al. Dermatology specific quality of life in vitiligo patients and its relation with various variables: a hospital based cross-sectional study. J Clin Diagn Res. 2014;8(6):YC01–YC03. doi:10.7860/JCDR/2014/8248.4508
24. Dabas G, Vinay K, Parsad D, et al. Psychological disturbances in patients with pigmentary disorders: a cross-sectional study. J Eur Acad Dermatol Venereol. 2019;34(2):392–399. doi:10.1111/jdv.15987
25. Tsadik AG, Teklemedhin MZ, Mehari Atey T, Gidey MT, Desta DM. Public knowledge and attitudes towards vitiligo: a survey in Mekelle City, Northern Ethiopia. Dermatol Res Pract. 2020;2020:3495165. doi:10.1155/2020/3495165
26. Lilly E, Lu PD, Borovicka JH, et al. Development and validation of a vitiligo-specific quality-of-life instrument (VitiQoL). J Am Acad Dermatol. 2013;69(1):e11–e18. doi:10.1016/j.jaad.2012.01.038
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.