")
Back to Journals » Journal of Pain Research » Volume 15
Evaluation of Sensory Loss and Postoperative Analgesia Obtained by Diaphragmatic Apposition Zone Block Under Direct Laparoscopic Visualization in Patients Undergoing Nephrectomy: A Descriptive Study
Authors Shi R, Wang M, Yang X, Shao P, Liang J , Wang Y
Received 30 April 2022
Accepted for publication 18 July 2022
Published 23 July 2022 Volume 2022:15 Pages 2015—2023
DOI https://doi.org/10.2147/JPR.S371140
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jinlei Li
Rong Shi,1,* Mingshuai Wang,2,* Xiaoyong Yang,2 Peiqi Shao,1 Jinghan Liang,1 Yun Wang1
1Department of Anesthesiology, Beijing Chaoyang Hospital, Capital Medical University, Beijing, 100020, People’s Republic of China; 2Department of Urology, Beijing Chaoyang Hospital, Capital Medical University, Beijing, 100020, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yun Wang, Department of Anesthesiology, Beijing Chaoyang Hospital, Capital Medical University, No. 8, South Gongti Road, Beijing, 100020, People’s Republic of China, Tel +86-10-85231463, Fax +86-10-65077808, Email [email protected]
Purpose: Local anesthetics can spread into the subendothoracic fascia compartment via the arcuate ligament and apposition zone of the diaphragm after the anterior quadratus lumborum blocks. Therefore, a new block may be achieved if local anesthetic is administered into the diaphragmatic apposition zone (DAZ) under direct laparoscopic visualization by surgeons. Therefore, we evaluated the sensory loss and postoperative analgesic efficacy of this new block in patients receiving laparoscopic nephrectomy.
Methods: A total of 28 patients scheduled to receive elective laparoscopic nephrectomy under general anesthesia were enrolled in this study. The DAZ blocks were performed in patients under direct laparoscopic visualization with 20 mL of 0.5% ropivacaine before the dissected kidneys or renal tumors were taken out from the incision. All patients received the intravenous patient-controlled analgesia after surgery. The dermatomes of sensory loss and the muscle weakness of quadriceps femoris were assessed at 2 h post-surgery in the wards. The postoperative pain was scored. The opioid consumption in the first 24 h after surgery was recorded.
Results: The average number of dermatomes of sensory block was 8.6 ± 1.2. The highest level of sensory loss was T6 (T5-T6) [median (interquartile range, IQR)], and the lowest level of sensory block was L1 (L1–L2). The postoperative pain scores at rest or on movement at 2 h, 6 h, 12 h, 24 h and 48 h were kept at the low levels (less than 4). The muscle strength of the quadriceps femoris evaluated was 5 (5– 5) points [median (IQR)]. Total dose of intravenous morphine equivalent consumption in the first 24 h after surgery was 21.2 ± 4.1 mg.
Conclusion: The DAZ block manifests a wide dermatomal coverage of sensory loss and is associated with the low levels of postoperative pain intensity and opioid use. It provides a new postoperative analgesia option for patients undergoing laparoscopic nephrectomy.
Keywords: diaphragmatic apposition zone, laparoscopy, nephrectomy, sensory block, postoperative analgesia
Introduction
It has been reported that the anterior quadratus lumborum (QL) block provides effective postoperative analgesia in laparoscopic nephrectomy.1–3 The anterior QL block includes two subtypes, the transmuscular and subcostal QL blocks.4,5 The former involves the local anesthetic (LA) injection between QL and psoas muscle, and the latter targets the LA into the potential compartment between the QL and transversalis fascia at L1-2 level.4,6 The transversalis fascia divides into upper and lower leaflets when it approaches medial and lateral arcuate ligament, and the upper leaflet, also known as endothoracic fascia, covers the inferior surface of the diaphragm in the diaphragmatic apposition zone (DAZ).6–8 Therefore, anterior QL block allows the LA to diffuse cranially via the arcuate ligaments and DAZ, and into the subendothoracic fascia compartment.6,7,9–11
Interestingly, the medial arcuate ligament (MAL) serves as a critical anatomic landmark for urologists in renal artery dissection during laparoscopic nephrectomy.12,13 Therefore, the transversalis fascia is possibly disrupted during the renal artery dissection, since the posterior renal fascia fuses with transversalis fascia.14–16 The disruption of the integrity of transversalis fascia can affect the blocking efficacy of anterior QL blocks due to LA leak. Alternatively, a reliable block may be obtained if the LA is directly administered into the DAZ via the MAL under direct laparoscopic visualization.17–19
Even as nephrectomies are moving away from open procedures, laparoscopic cases continue to be associated with moderate-to-severe pain.20 In the context of laparoscopic nephrectomy, gas distension of the abdominal wall, abdominal port placement, and dissection in the retroperitoneal cavity can result in visceral and somatic pain arising from the T6–T12 somatic nerves and the extensive sympathetic innervation of the abdominal viscera. Thus, the current study was designed to assess the dermatomal coverage of sensory loss and postoperative analgesic efficacy of the DAZ block in patients undergoing laparoscopic nephrectomy.
Methods
The Ethics Committee of Beijing Chaoyang Hospital Affiliate to Capital Medical University, China, approved the study protocol on August 3, 2020, with the reference number of 2020-ke-420. This study has been registered with the number ChiCTR2000035812 at the Chinese Clinical Trial Registry on August 17, 2020. The Consolidated Standards of Reporting Trials (CONSORT) statement, and the Helsinki Declaration were followed in the study.
The inclusion criteria were as follows: American Society of Anesthesiologists (ASA) physical status I–III, body mass index (BMI) 20–30, 18 years or older. The exclusion criteria included allergy to medications used in the standardized anesthesia regimen, local or systemic infection, pregnancy, inability to complete pain scorings for any reasons such as psychiatric problems, and inability to operate the patient-controlled analgesia (PCA) system. Patient demographic details such as age, sex, height and weight were collected. After written informed consent, 27 subjects scheduled for elective laparoscopic nephrectomy under general anesthesia were recruited between August 28, 2020 and September 12, 2021, in Beijing Chaoyang Hospital Affiliate to Capital Medical University (Figure 1).
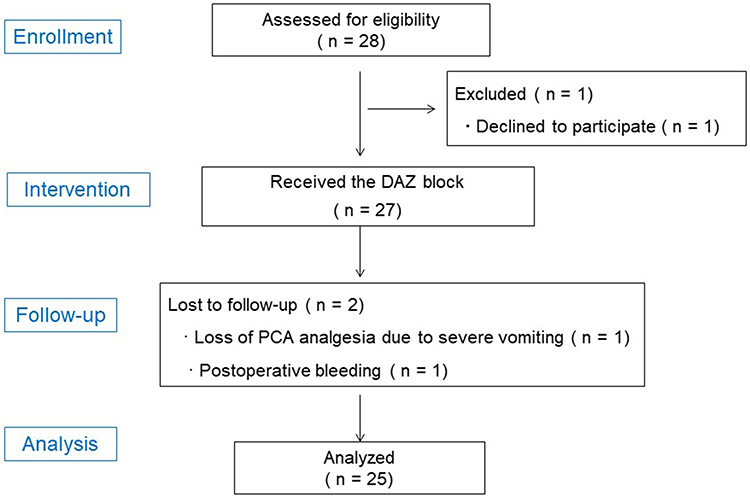 |
Figure 1 CONSORT study flow chart. Abbreviations: CONSORT, Consolidated Standards of Reporting Trials; PCA, patient-controlled analgesia; DAZ, diaphragmatic apposition zone. |
All patients recruited in the study received a standardized anesthetic regimen. When the patients entered the operation room, the monitors including noninvasive blood pressure, electrocardiography, end-tidal carbon dioxide, pulse oxygen saturation were established. Next, a peripheral venous line was placed, and intravenous infusion of Ringer’s lactate solution was administered. Finally, an invasive radial arterial line was established. Then, general anesthesia was induced by intravenous administration of propofol 1.5–2.5 mg kg−1 (Fresenius Kabi AB, Uppsala, Sweden), sufentanil 0.15 μg kg−1 (Yichang Renfu Pharma, Yichang, China), and rocuronium 0.9 mg kg−1 (Xianju Pharma, Xianju, China). The tracheal intubation and mechanical ventilation were performed. The general anesthesia was maintained by the continuous intravenous infusion with propofol at 0.12–0.15 mg kg−1 min−1 and remifentanil (Yichang Renfu Pharma, Yichang, China) at 0.15–0.3 μg kg−1 min−1. Additional dose of rocuronium was intermittently given as needed during surgery. At 10 min prior to the incision suture, sufentanil 0.15 μg kg−1 was intravenously given for postoperative pain control. At the end of the surgery, the intravenous neostigmine (Shanghai Xinyijinzhu Pharma, Shanghai, China) was administered at a dose of 40μg kg−1 for neuromuscular blockade reversal.
During the operation, the urologists first dissected the MAL which curves over the psoas major muscle, followed by renal artery, renal vein, and ureter dissection. Just before a 6 −8 cm-long longitudinal incision 5 cm medial to the anterior superior iliac spine was made to remove the dissected kidney or tumor from the retroperitoneal cavity, the DAZ block via the MAL under direct laparoscopic visualization was performed in patients by the skilled urologists (MW, XY). They had successfully performed the same procedures in more than 30 patients before the current study was initiated. Specifically, a sterile 21G needle (2 cm long) attached to a 30 cm tube and a 20 mL syringe was prepared. The needle was placed into the retroperitoneal cavity via the trocar with the syringe outside. The urologists clipped the needle via an operating lever and directed the needle at a 15-degree angle toward the ventral surface of psoas major muscle with the puncture site at the MAL. Then, the needle was advanced cranially and reached the DAZ. A total of 20 mL of 0.5% ropivacaine (AstraZeneca AB, Sodertalje, Sweden) was administered into the DAZ (Figures 2 and 3). Hemodynamic indices such as mean artery pressure (MAP) and heart rate (HR) were recorded at 0, 5, 10, and 15-minute intervals after the injections.
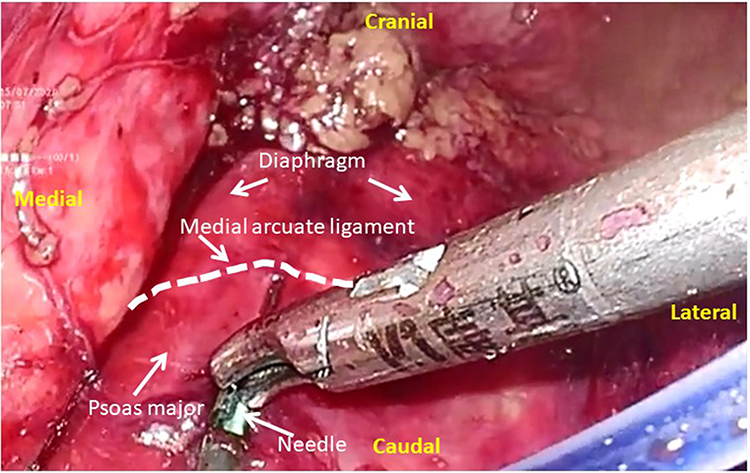 |
Figure 2 The DAZ block with 20 mL of 0.5% ropivacaine via the medial arcuate ligament under direct laparoscopic visualization was performed. Abbreviation: DAZ, diaphragmatic apposition zone. |
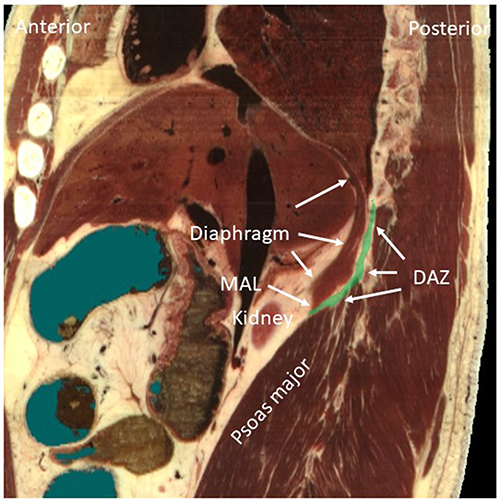 |
Figure 3 The sagittal schematic diagram shows the positions of the MAL and DAZ. The MAL is the inferior edge of diaphragm, which is curved over the psoas major muscle. The green-colored area indicates the DAZ. Abbreviations: MAL, medial arcuate ligament; DAZ, diaphragm apposition zone. |
After extubation, all subjects were admitted into the recovery room. In the recovery room, the intravenous PCA system containing 1 μg mL−1 of sufentanil was attached to the subjects. The system was set to administer 1.5 mL of intravenous bolus on demand, with a 15-min lockout interval. Pain intensity at rest or on movement was scored by using the numerical rating scale (NRS) by a staff nurse who was blinded to the anesthesia regimen at 2, 6, 12, 24, and 48 hours.21,22 All the subjects received the instruction on the use of intravenous PCA system and on pain severity rating with 0 defined as “no pain” to 10 indicating “worst pain” prior to the surgery. The pain intensity of movement was assessed with a single cough. The first-line rescue analgesia was performed by intravenously administration of Flurbiprofen (Beijing Taide Pharma, Beijing, China) (50 mg), when the pain intensity at rest was greater than 4. The postoperative intravenous equivalent morphine dose consumed in the first 24 h was recorded (the morphine milligram equivalent of sufentanil is 1000). The possible adverse events associated with the opioid use, such as nausea, vomiting, pruritus, hypotension, and respiratory depression (respiratory rate <10/min), were recorded.
An anesthesia nurse who was blinded to the study evaluated the dermatomal coverage of sensory block by using a cool roller at 2 h post-surgery. A markedly reduced sensation or sensory loss to cold was identified as a sensory block. The normal sensation on the shoulder was used for comparison. The dermatomes in the thoracoabdominal area were detected at the anterior axillary line. L1 dermatome was detected 2 cm caudal to the midpoint of the inguinal ligament, L2 dermatome around the midpoint of the anterior aspect of the thigh, L3 dermatome at the patella, L4 dermatome at the anteromedial midpoint of the leg, L5 dermatome at the midpoint of the dorsal foot.
The strength of the quadriceps femoris muscle was evaluated at 2 h following the laparoscopic nephrectomy. The muscle strength scoring was identified by flexing the hip and knee.23 In detail, 0 point indicated there was no muscle contraction; 1 point was given if muscle contraction without joint movement was observed; Joint movement but no gravity resistance meant 2 points; gravity resistance stood for 3 points; gravity and partial counterforce resistance showed 4 points; and normal joint function represented 5 points.
Statistical Analysis
The sample size was empirically identified, since this was a pilot study. The previous literature indicated that a sample size of 10–40 is appropriate.24 The sample size of 25 patients was set in the study. The final sample size was adjusted to 28 patients, considering a drop-out rate of 10%. Continuous variables with normal distribution are presented as mean ± standard deviation (SD), whereas median values [interquartile range (IQR)] are used for those not subject to normal distribution. Categorical variables are expressed as number and frequency. Statistical analysis was performed by using SPSS software (version 18.0, IBM Corporation, Armonk, NY, USA). Data normal distribution was identified by the Kolmogorov–Smirnov test. The hemodynamic changes were analyzed by using the repetitive measure analysis of variance (ANOVA). For all comparisons, a P value <0.05 was considered to be significant.
Results
A total of 28 subjects were recruited for the study. One patient declined to participate in the study. One patient withdrew the PCA analgesia due to severe vomiting. One patient received a repeat surgery due to bleeding in the first 24 hours following surgery. Finally, the data from 25 subjects were included and analyzed (Figure 1). The demographics and surgical details of subjects are presented in Table 1. The subjects had an average age of 58 (12.4) yr, and BMI 26.6 (3.2). The mean duration from intubation to extubation was 145.2 ±17.2 min.
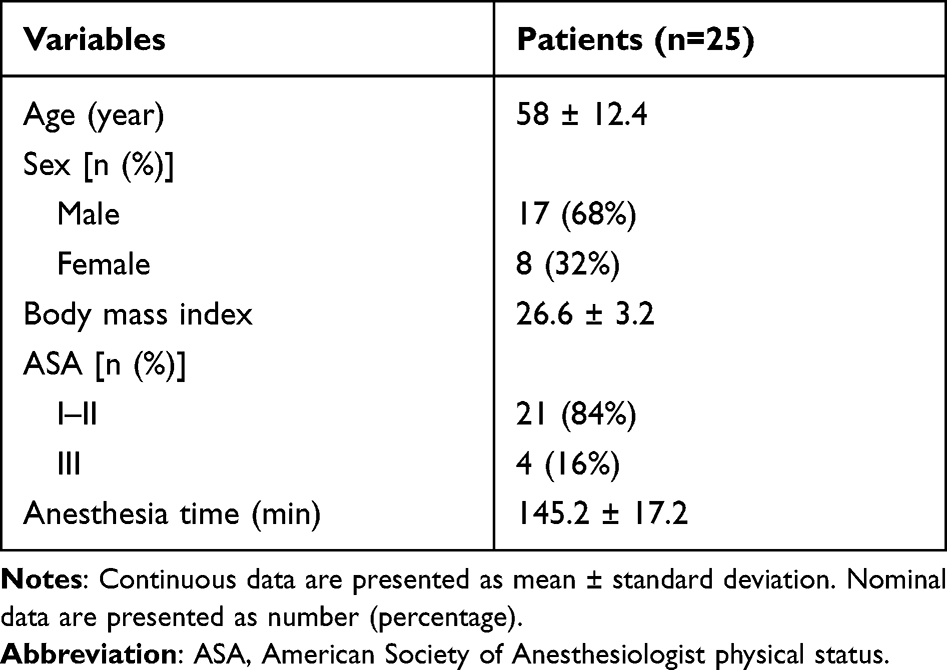 |
Table 1 Demographics and Operation Details |
The DAZ block via the posterior pathway of MAL was successfully performed in all patients (Figure 2). During the period of injection, the bulge of the diaphragm was clearly observed, which indirectly indicated the injectate preferentially spread in the cephalad, medial, and lateral directions. Almost no injectate spread in the caudal direction.
After the injections of 0.5% ropivacaine for DAZ block, no significant difference was observed in HR and MAP at different time-points (P > 0.05) (Table 2).
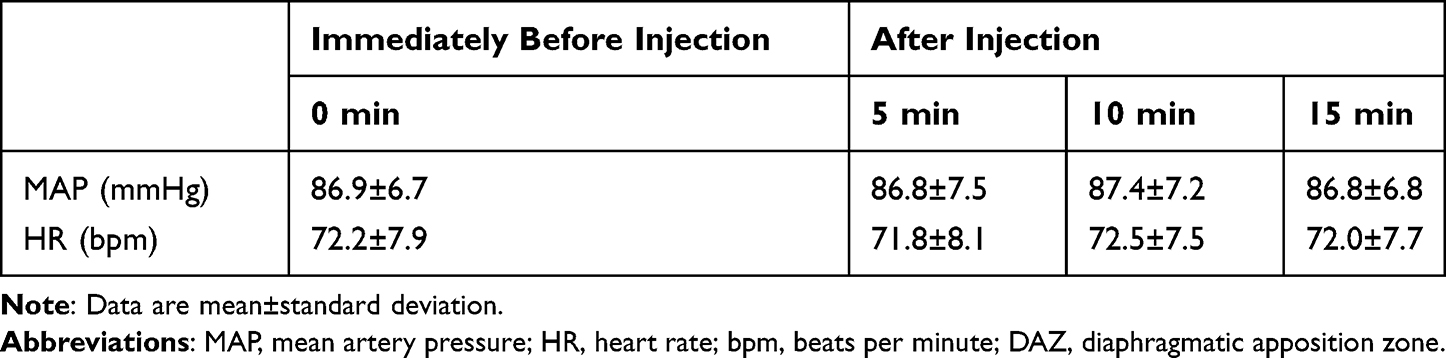 |
Table 2 Hemodynamic Changes After Intraoperative Injections of 0.5% Ropivacaine for DAZ Block |
The blocking dermatomes were detected at 2 h following laparoscopic nephrectomy. The highest and lowest dermatomes of sensory block were T6 (T5–T6) and L1 (L1–L2) [median (IQR)], respectively. The average number of dermatomes of sensory block was 8.6 ± 1.2. The dermatomal coverage from T7 – T12 was achieved in every patient. One patient showed the dermatomal coverage as cephalad as T4 and 8 patients showed the dermatomal coverage as caudal as L2. The blocked frequency of dermatomes is shown in Table 3.
 |
Table 3 Dermatomal Coverage of Sensory Block Achieved at 2 h After Surgery |
The strength of the quadriceps femoris muscle at 2 h following surgery was scored as 5 (5–5) [median (IQR)]. 92% subjects showed the 5 points in muscle strength assessment. The 4 points was observed in 8% subjects. No subjects acquired the points less than 4 (Table 4).
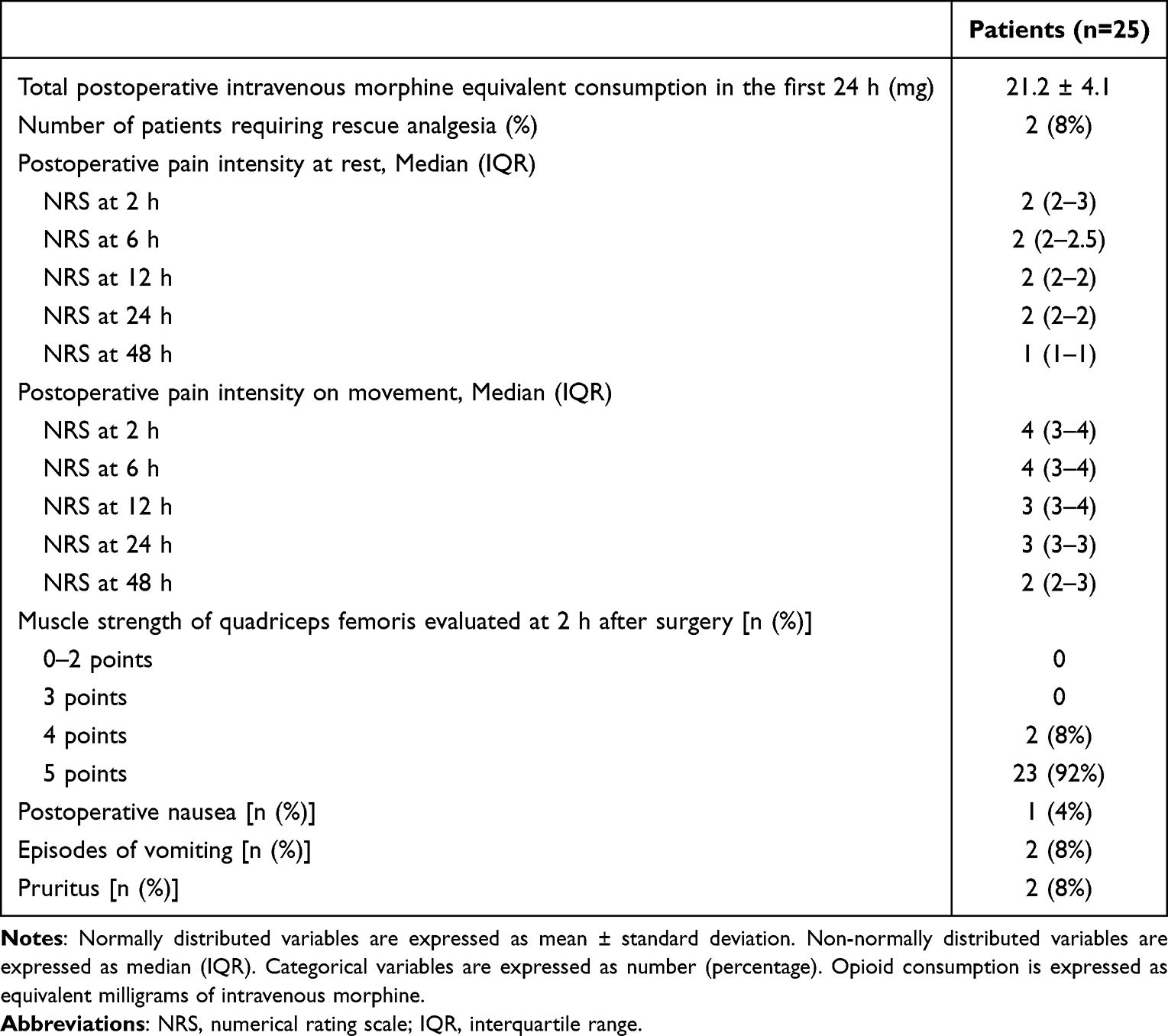 |
Table 4 The Postoperative Data |
The postoperative pain intensity assessment was shown in (Table 4). The pain NRS scores at rest or on movement were kept at the low levels (less than 4). Total postoperative intravenous opioid consumption in the first 24 h following surgery was 21.2 ± 4.1 mg equivalent morphine (Table 4). An additional rescue analgesia in the first 24 h after surgery was given in 2 patients. One subject manifested the nausea, 2 subjects suffered from vomiting and 2 subjects had pruritus in the first 24 h following surgery. No respiratory depression or LA systemic toxicity was observed.
Discussion
This prospective, descriptive study demonstrates that the DAZ block via the MAL under direct laparoscopic visualization resulted in the dermatomal sensory block from T6 (T5–T6) and L1 (L1–L2), which was tested at 2 h following surgery. Furthermore, the postoperative pain scores at rest or on movement, and opioid consumption were maintained at the relatively low levels in the first 24 h following surgery, while the strength of quadriceps femoris muscle was almost kept intact.
Although laparoscopic nephrectomy has many benefits, such as minimal trauma and enhanced recovery, the postoperative pain derived from incision and visceral stimuli cannot be underestimated. The QL blocks have been reported for the postoperative analgesia for laparoscopic nephrectomy and other abdominal or hip surgery.2,25–31 There are several approaches to QL blocks with different characteristics.4,17,32–35 The subcostal approach allows the LA to inject into the compartment between the QL muscle and transversalis fascia, while the transmuscular approach targets the LA into the compartment between the QL and psoas major muscle. Both approaches allow the LA to diffuse cranially under the arcuate ligaments and reach the diaphragmatic zone of apposition and then the subendothoracic compartment (Figure 3).6,7,35,36 Therefore, the intact transversalis fascia is required for the complete block action of both approaches. However, the urologists often consider the medial arcuate ligament as a landmark for dissecting the renal artery during the nephrectomy and the procedure often does damage to the transversalis fascia.12,13 It may lead to the failure of LA spread into the subendothoracic compartment after the transmuscular or subcostal QL block. Our group has recently proposed this problem.37,38
In the current study, our group developed a novel DAZ block via the MAL under the direct visualization. With this new approach, the spread of LA during the injection was clearly visualized under direct visualization during the surgery. Especially, the injectate preferentially spread in the cephalad, medial, and lateral directions. Almost no injectate spreads in the caudal direction, indicating that the new approach is not influenced by the damage to the integrity of transversalis fascia. Alansary et al reported a transincisional QL block in open renal surgeries.39 In their study, an 18-gauge Tuohy needle was inserted from the anteromedial side to the posterolateral side at the level of L1-2, penetrating the transversalis fascia and the LA was finally deposited in the space between the psoas and QL muscle. Although the new ultrasound-guided trans-incisional QL block was reported as effective, the authors did not show whether the transversalis fascia was intact during the open surgery in patients and the dermatomal coverage for sensory block. The efficacy of trans-incisional QL block is possibly influenced by the integrity extent of the transversalis fascia.37,38
Additionally, the relevant anatomic landmarks such as psoas major, MAL, and diaphragm were very clear under laparoscopy after completing the renal surgery. This makes this new technique easy to be performed by urologists. In the current study, the skilled urologists performed all the blocks, who had successfully completed more than 30 DAZ blocks before the current study was initiated. The lateral abdominal wall is the most common surgical incision site in laparoscopic nephrectomy, which is innervated by the anterior branches of T8–L1 spinal nerves. In the current study, we detected the dermatomes coverage of sensory block in patients at 2 h following surgery. 96% of patients receiving DAZ blocks achieved sensory block from T6 to L1 dermatomes, which is similar to the dermatomal coverage acquired by the subcostal QL block.4,26 The mean numbers of block dermatomes were 8.6 ± 1.2. Our data indicate that the new approach has consistent dermatomal coverage of sensory block, which can cover the complete abdominal area and is very suitable for the postoperative analgesia for the abdominal surgery.
All the patients underwent the surgery under general anesthesia. For general anesthesia, the large doses of opioids are required to inhibit the surgical nociceptive stimuli. However, opioids are usually associated with increased postoperative shivering, nausea, vomiting, and pruritus.27,40–42 Also, opioids could result in postoperative hyperalgesia. In the current study, the intravenous morphine equivalent use in the first 24 h after laparoscopic nephrectomy was only 21.2 ± 4.12 mg in patients receiving the DAZ block, which is much less than the intravenous morphine equivalent dose (34.3 ± 6.3 mg) used in patients with transmuscular QL block reported by our previous study.20 This suggests that the new approach is very effective and can help reduce the postoperative opioid demand in patients with laparoscopic nephrectomy. Correspondingly, the pain scores at rest or on movement after surgery were kept at a low level (less than 4), indicating the effectiveness of the new block.
Wikner et al43 reported an unexpected motor weakness following lateral quadratus lumborum block. In the current study, 92% patients acquired the 5 points in muscle strength scoring and the 4 points was given in 8% patients. We did not observe the apparent lower limb weakness, which may be associated with the LA cranial spread with this new approach.
Our study has some limitations. First, this new block can only be used for procedures when relevant anatomical structures are visible to surgeons, such as nephrectomy, resection of renal cyst, and so on, under the laparoscopy. Second, this study was designed to focus on the effectiveness of this new block. In the future, the work should be performed to compare this new block with the other blocks, such as QL block, transversus abdominis plane block, and so on.
Conclusions
The DAZ block via the MAL under direct visualization is feasible, and provides effective analgesia with low levels of postoperative opioid consumption and pain scores in patients undergoing laparoscopic nephrectomy.
Data Sharing Statement
We all agree to share all the data for this article. The data are available from the corresponding author upon reasonable request.
Acknowledgments
This work was supported by the Beijing Hospitals Authority Clinical Medicine Development of Special Funding Support (XMLX202106).
Disclosure
The authors declare no conflicts of interest.
References
1. Corso RM, Piraccini E, Sorbello M, Bellantonio D, Tedesco M. Ultrasound-guided transmuscular quadratus lumborum block for perioperative analgesia in open nephrectomy. Minerva Anestesiol. 2017;83(12):1334–1335. doi:10.23736/S0375-9393.17.12167-X
2. Dam M, Hansen C, Poulsen TD, et al. Transmuscular quadratus lumborum block reduces opioid consumption and prolongs time to first opioid demand after laparoscopic nephrectomy. Reg Anesth Pain Med. 2020;46:18–24.
3. Warusawitharana C, Basar S, Jackson BL, Niraj G. Ultrasound guided continuous transmuscular quadratus lumborum analgesia for open renal surgery: a case series. J Clin Anesth. 2017;42:100–101. doi:10.1016/j.jclinane.2017.08.025
4. Elsharkawy H. Quadratus lumborum block with paramedian sagittal oblique (subcostal) approach. Anaesthesia. 2016;71(2):241–242. doi:10.1111/anae.13371
5. Elsharkawy H, El-Boghdadly K, Barrington M. Quadratus lumborum block: anatomical concepts, mechanisms, and techniques. Anesthesiology. 2019;130(2):322–335. doi:10.1097/ALN.0000000000002524
6. Dam M, Moriggl B, Hansen CK, Hoermann R, Bendtsen TF, Børglum J. The pathway of injectate spread with the transmuscular quadratus lumborum block: a cadaver study. Anesth Analg. 2017;125:303–312.
7. Elsharkawy H, El-Boghdadly K, Kolli S, et al. Injectate spread following anterior sub-costal and posterior approaches to the quadratus lumborum block: a comparative cadaveric study. Eur J Anaesthesiol. 2017;34(9):587–595. doi:10.1097/EJA.0000000000000680
8. Shao P, Li H, Shi R, Li J, Wang Y. Understanding fascial anatomy and interfascial communication: implications in regional anesthesia. J Anesth. 2022. doi:10.1007/s00540-022-03082-3
9. Balocco AL, López AM, Kesteloot C, et al. Quadratus lumborum block: an imaging study of three approaches. Reg Anesth Pain Med. 2020;46(1):35–40. doi:10.1136/rapm-2020-101554
10. Carrillo-Esper R, Perez-Calatayud AA, Arch-Tirado E, et al. Standardization of sonographic diaphragm thickness evaluations in healthy volunteers. Respir Care. 2016;61(7):920–924. doi:10.4187/respcare.03999
11. Petroll WM, Knight H, Rochester DF. Effect of lower rib cage expansion and diaphragm shortening on the zone of apposition. J Appl Physiol. 1990;68(2):484–488. doi:10.1152/jappl.1990.68.2.484
12. Cai W, Li HZ, Zhang X, et al. Medial arcuate ligament: a new anatomic landmark facilitates the location of the renal artery in retroperitoneal laparoscopic renal surgery. J Endourol. 2013;27(1):64–67. doi:10.1089/end.2012.0152
13. Luo L, Liu YN, Zhang Y, et al. An easy and effective method to locate renal vein during retroperitoneal laparoscopic radical nephrectomy: single-center experience. Med Sci Monit. 2018;24:5147–5151. doi:10.12659/MSM.911199
14. Coffin A, Boulay-Coletta I, Sebbag-Sfez D, Zins M. Radioanatomy of the retroperitoneal space. Diagn Interv Imaging. 2015;96:171–186. doi:10.1016/j.diii.2014.06.015
15. Kanemura T, Satake K, Nakashima H, et al. Understanding retroperitoneal anatomy for lateral approach spine surgery. Spine Surg Relat Res. 2017;1:107–120. doi:10.22603/ssrr.1.2017-0008
16. Li H, Shi R, Wang Y. A modified approach below the lateral arcuate ligament to facilitate the subcostal anterior quadratus lumborum block. J Pain Res. 2021;14:961–967. doi:10.2147/JPR.S306696
17. Li H, Ma D, Liu Y, Wang Y. A transverse approach for ultrasound-guided anterior quadratus lumborum block at the lateral supra-arcuate ligament. Anaesthesia. 2020;75(10):1400–1401. doi:10.1111/anae.15058
18. Shi R, Li H, Wang Y. Dermatomal coverage of single-injection ultrasound-guided parasagittal approach to anterior quadratus lumborum block at the lateral supra-arcuate ligament. J Anesth. 2021;35:307–310. doi:10.1007/s00540-021-02903-1
19. Li H, Liang J, Shao P, Zheng J, Shi R, Wang Y. Supra-arcuate ligament blocks: anatomy, mechanisms, and techniques. J Pain Res. 2021;14:3837–3848. doi:10.2147/JPR.S347071
20. Li H, Shi R, Shi D, Wang R, Liu Y, Wang Y. Anterior quadratus lumborum block at the lateral supra-arcuate ligament versus transmuscular quadratus lumborum block for postoperative analgesia in patients undergoing laparoscopic nephrectomy: a randomized controlled trial. J Clin Anesth. 2021;75:110561. doi:10.1016/j.jclinane.2021.110561
21. Kolacz M, Mieszkowski M, Janiak M, et al. Transversus abdominis plane block versus quadratus lumborum block type 2 for analgesia in renal transplantation: a randomised trial. Eur J Anaesthesiol. 2020;37:773–789. doi:10.1097/EJA.0000000000001193
22. Zhu M, Qi Y, He H, Lou J, Pei Q, Mei Y. Analgesic effect of the ultrasound-guided subcostal approach to transmuscular quadratus lumborum block in patients undergoing laparoscopic nephrectomy: a randomized controlled trial. BMC Anesthesiol. 2019;19:154. doi:10.1186/s12871-019-0825-4
23. Li H, Shi R, Shao P, Wang Y. Evaluation of sensory loss obtained by circum-psoas blocks in patients undergoing total Hip replacement: a descriptive pilot study. J Pain Res. 2022;15:827–835. doi:10.2147/JPR.S354829
24. Hertzog MA. Considerations in determining sample size for pilot studies. Res Nurs Health. 2008;31:180–191. doi:10.1002/nur.20247
25. Dam M, Hansen CK, Poulsen TD, et al. Transmuscular quadratus lumborum block for percutaneous nephrolithotomy reduces opioid consumption and speeds ambulation and discharge from hospital: a single centre randomised controlled trial. Br J Anaesth. 2019;123:e350–e358. doi:10.1016/j.bja.2019.04.054
26. Elsharkawy H, Ahuja S, DeGrande S, Maheshwari K, Chan V. Subcostal approach to anterior quadratus lumborum block for pain control following open urological procedures. J Anesth. 2019;33(1):148–154. doi:10.1007/s00540-018-02605-1
27. Hansen C, Dam M, Nielsen MV, et al. Transmuscular quadratus lumborum block for total laparoscopic hysterectomy: a double-blind, randomized, placebo-controlled trial. Reg Anesth Pain Med. 2020;43:25–30.
28. Hansen CK, Dam M, Steingrimsdottir GE, et al. Ultrasound-guided transmuscular quadratus lumborum block for elective cesarean section significantly reduces postoperative opioid consumption and prolongs time to first opioid request: a double-blind randomized trial. Reg Anesth Pain Med. 2019;44(9):896–900. doi:10.1136/rapm-2019-100540
29. Ince I, Hamadnalla H, Hassan M, Qiu Y. Ultrasound-guided quadratus lumborum plane block for congenital Hip dislocation surgery: dermatomes and osteotomes. J Clin Anesth. 2019;54:140. doi:10.1016/j.jclinane.2018.10.044
30. Irwin R, Stanescu S, Buzaianu C, et al. Quadratus lumborum block for analgesia after caesarean section: a randomised controlled trial. Anaesthesia. 2020;75(1):89–95. doi:10.1111/anae.14852
31. Kukreja P, MacBeth L, Sturdivant A, et al. Anterior quadratus lumborum block analgesia for total Hip arthroplasty: a randomized, controlled study. Reg Anesth Pain Med;2019. doi:10.1136/rapm-2019-100804
32. Dam M, Hansen CK, Børglum J, Chan V, Bendtsen TF. A transverse oblique approach to the transmuscular quadratus lumborum block. Anaesthesia. 2016;71(5):603–604. doi:10.1111/anae.13453
33. Elsharkawy H, El-Boghdadly K, Barnes TJ, et al. The supra-iliac anterior quadratus lumborum block: a cadaveric study and case series. Can J Anaesth. 2019;66:894–906. doi:10.1007/s12630-019-01312-z
34. Iwamitsu R, Ueshima H, Otake H. Intermittent bilateral posterior quadratus lumborum block was effective for pain management in lumbar spinal fusion. J Clin Anesth. 2017;42:16. doi:10.1016/j.jclinane.2017.08.012
35. Tamura T, Kitamura K, Yokota S, Ito S, Shibata Y, Nishiwaki K. Spread of quadratus lumborum block to the paravertebral space via intramuscular injection: a volunteer study. Reg Anesth Pain Med. 2018;43(4):372–377. doi:10.1097/AAP.0000000000000735
36. Gorman RB, McKenzie DK, Butler JE, Tolman JF, Gandevia SC. Diaphragm length and neural drive after lung volume reduction surgery. Am J Respir Crit Care Med. 2005;172(10):1259–1266. doi:10.1164/rccm.200412-1695OC
37. Li H, Shi R, Wang Y. Use of transmuscular quadratus lumborum block for postoperative analgesia after laparoscopic nephrectomy. Reg Anesth Pain Med. 2021;46(12):1118–1119. doi:10.1136/rapm-2021-102478
38. Li H, Shi R, Wang Y. Transincisional ultrasound-guided quadratus lumborum block in open renal surgeries. Pain Physician. 2021;24:E127–E128.
39. Alansary AM, Badawy A, Elbeialy MAK. Dexmedetomidine added to bupivacaine versus bupivacaine in transincisional ultrasound-guided quadratus lumborum block in open renal surgeries: a randomized trial. Pain Physician. 2020;23:271–282.
40. Korgvee A, Junttila E, Koskinen H, Huhtala H, Kalliomaki ML. Ultrasound-guided quadratus lumborum block for postoperative analgesia: a systematic review and meta-analysis. Eur J Anaesthesiol. 2020;38:115–129.
41. Roda R, Uppal V, Allen VM, Woolcott CG, McKeen DM. The addition of lateral quadratus lumborum block to a multimodal analgesic regimen that includes intrathecal morphine is associated with a longer time to first analgesic request for elective cesarean section. J Clin Anesth. 2020;61:109667. doi:10.1016/j.jclinane.2019.109667
42. Uppal V, Retter S, Kehoe E, McKeen DM. Quadratus lumborum block for postoperative analgesia: a systematic review and meta-analysis. Can J Anaesth. 2020;67:1557–1575. doi:10.1007/s12630-020-01793-3
43. Wikner M. Unexpected motor weakness following quadratus lumborum block for gynaecological laparoscopy. Anaesthesia. 2017;72(2):230–232. doi:10.1111/anae.13754
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.