")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 14
Evaluation of rescue medication use and medication adherence receiving umeclidinium/vilanterol versus tiotropium bromide/olodaterol
Authors Moretz C, Bengtson LGS, Sharpsten L, Koep E , Le L, Tong J, Stanford RH , Hahn B , Ray R
Received 26 April 2019
Accepted for publication 15 August 2019
Published 4 September 2019 Volume 2019:14 Pages 2047—2060
DOI https://doi.org/10.2147/COPD.S213520
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Chad Moretz1, Lindsay GS Bengtson2, Lucie Sharpsten2, Eleena Koep2, Lisa Le2, Junliang Tong2, Richard H Stanford1, Beth Hahn1, Riju Ray1
1Glaxo Smith Kline, Research Triangle Park, Durham, NC, USA; 2Optum, Eden Prairie, MN, USA
Correspondence: Chad Moretz
GlaxoSmithKline, Research Triangle Park, 5 Moore Drive, Durham, NC, USA
Tel +1 828 442 6294
Email [email protected]
Background: This was the first real-world head-to-head study comparing inhaled long-acting muscarinic antagonist/long-acting β2-agonist fixed-dose combination treatments as maintenance therapy.
Methods: Retrospective observational study including commercial, Medicare Advantage with Part D or Part D-only enrollees aged ≥40 years from the Optum Research Database. Patients initiated umeclidinium/vilanterol (UMEC/VI) or tiotropium bromide/olodaterol (TIO/OLO) between June 1, 2015 and November 30, 2016 (index date) with 12 months of pre- and post-index continuous enrollment. Outcomes were modeled following the inverse probability of treatment weighting. The primary endpoint, rescue medication use, was modeled using weighted ordinary least squares regression with bootstrapped variance estimation. Intent-to-treat analysis evaluated non-inferiority and superiority of UMEC/VI to TIO/OLO with thresholds of 0.30 and 0 units, respectively. On-treatment sensitivity analysis evaluated the superiority of UMEC/VI to TIO/OLO for rescue medication use. The secondary endpoint, medication adherence (proportion of days covered [PDC]≥80%), was evaluated using weighted logistic regression. Post hoc weighted Cox proportional hazards regression analysis evaluated escalation to multiple inhaler triple therapy (MITT).
Results: The study population included 14,324 patients; 9549 initiated UMEC/VI and 4775 initiated TIO/OLO. During the 12-month post-index period, UMEC/VI initiators used 0.16 fewer adjusted mean units of rescue medication than TIO/OLO initiators (95% CI: −0.28, −0.04), meeting pre-specified non-inferiority (P<0.001) and superiority (P=0.005) criteria; the on-treatment sensitivity analysis for superiority was not statistically significant. Significantly more UMEC/VI than TIO/OLO initiators (28.6% vs 22.7%; P<0.001) achieved a clinically meaningful level (PDC≥80%) of medication adherence. The adjusted risk of escalation to MITT was similar between treatment groups (HR=0.93; 95% CI: 0.81, 1.06; P=0.268).
Conclusion: UMEC/VI was superior to TIO/OLO for rescue medication use and UMEC/VI initiators had better medication adherence than TIO/OLO initiators. This study supports findings from a head-to-head trial that demonstrated significant, clinically meaningful improvements in lung function with UMEC/VI versus TIO/OLO.
Keywords: COPD, long-acting β2-agonists, long-acting muscarinic antagonists, adherence, rescue medication, real world
Plain language summary
Why was the study done? Patients with COPD are often treated with several single inhalers containing medicines called long-acting muscarinic antagonists (LAMA) and long-acting β2-agonists (LABA). LAMA/LABA medications combine these two treatments into one single inhaler to improve convenience for the patient. There are many types of LAMA/LABA medications and there might be differences between commonly used LAMA/LABA medications.
What did the researchers do and find? In this study, the researchers used information from a large US health insurer database to compare two of the most commonly used LAMA/LABA medications in the US. Patients treated with a LAMA/LABA medication called umeclidinium/vilanterol (UMEC/VI) used less rescue medication (reliever inhaler) over a 12-month period than patients treated with another LAMA/LABA medication called tiotropium/olodaterol (TIO/OLO). Patients treated with UMEC/VI also had better adherence to their medication than patients treated with TIO/OLO. However, patients receiving both UMEC/VI and TIO/OLO were prescribed an additional inhaler containing a different medicine called inhaled corticosteroids at a similar rate.
What do these results mean? This study supports the findings of a previous clinical trial. The previous trial also found that patients with moderate COPD who still have symptoms and were treated with UMEC/VI used less rescue medication than patients treated with TIO/OLO. Treatment of COPD with UMEC/VI compared with TIO/OLO might reduce the need for rescue medication. If patients use less rescue medication, it generally means that their COPD symptoms have improved. Patients treated with UMEC/VI had better medication adherence than patients treated with TIO/OLO, even though both medications are taken once daily.
Introduction
Long-acting bronchodilators are the cornerstone of maintenance therapy for patients with COPD, a progressive disease characterized by persistent airflow limitation and respiratory symptoms.1 The GOLD and COPD Foundation recommend long-acting muscarinic antagonists/long-acting β2-agonists (LAMA/LABA) as an initial treatment option for many patients with severe COPD symptoms, and as a step-up option for patients with persistent breathlessness or exacerbations on LAMA or LABA monotherapy.1,2
Umeclidinium/vilanterol (UMEC/VI), administered once daily via the ELLIPTA inhaler, and tiotropium bromide/olodaterol (TIO/OLO), administered once daily via the Respimat inhaler, are LAMA/LABA fixed-dose combinations (FDCs) approved for maintenance treatment in patients diagnosed with COPD.3,4 Meta-analyses of randomized controlled trials (RCT) comparing LAMA/LABA FDCs suggest a gradient of efficacy within the LAMA/LABA class, at least with regard to lung function,5,6 and one meta-analysis found higher probabilities of improved lung function outcomes with UMEC/VI versus TIO/OLO.6 The efficacy of these once-daily LAMA/LABA FDCs has also been directly compared in a cross-over RCT involving 236 symptomatic patients with moderate COPD.7 UMEC/VI was superior to TIO/OLO with regard to lung function, doubling the odds of achieving a clinically meaningful increase in trough FEV1 at 8 weeks compared with TIO/OLO.7 Patients receiving UMEC/VI also reported significantly less rescue medication use compared with those receiving TIO/OLO.7 In addition, a post hoc analysis of the maintenance-naïve subgroup from the same study also showed greater improvements in lung function and reduced rescue medication use with UMEC/VI compared with TIO/OLO.8
Previous RCT findings, therefore, suggest that treatment with UMEC/VI can lead to improved outcomes compared with TIO/OLO in patients with COPD. However, real-world observational studies are required to assess whether differences within the LAMA/LABA class correspond to improvements in symptom control in a larger sample over a longer period of time, which is not feasible in an RCT design. The present study compared UMEC/VI with TIO/OLO using real-world data in order to complement existing RCT findings. The primary objectives were to evaluate the non-inferiority and superiority of UMEC/VI compared with TIO/OLO on rescue medication use in patients initiating these medications. The secondary objective was to evaluate medication adherence, defined as the proportion of days covered (PDC) ≥80%, and a post hoc analysis evaluated time to escalation to multiple inhaler triple therapy (MITT).
Patients and methods
Patients and study design
This was a retrospective cohort study of commercial, Medicare Advantage with Part D (MAPD) and Part D prescription drug plan (PDP) – only enrollees who initiated UMEC/VI or TIO/OLO between June 1, 2015 and November 30, 2016 (patient identification period; Figure 1). Medicare Advantage (Medicare Part C) is a managed care health insurance option offered to Medicare-eligible individuals and provided by private companies under contract to the Centers for Medicare and Medicaid Services (CMS). Part D is the Medicare PDP. Members often have combined MAPD plans with both Medicare Advantage and Part D coverage.
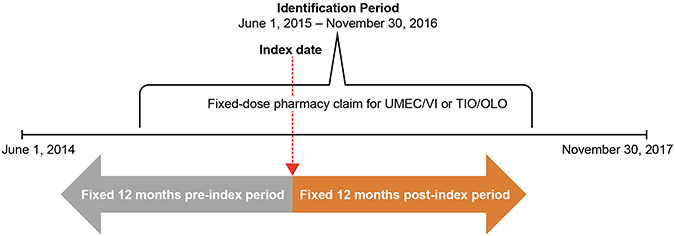 |
Figure 1 Study design. Abbreviations: TIO/OLO, tiotropium bromide/olodaterol; UMEC/VI, umeclidinium/vilanterol. |
Patients were identified and analyses conducted using health care claims data contained in the Optum Research Database. The Optum Research Database is a large US health care claims database containing fully adjudicated medical and pharmacy claims and linked enrollment information for MAPD and PDP enrollees. In 2016, claims data were included for approximately 19% of the US population enrolled in a commercial health plan and 17% of those enrolled in a Medicare Advantage plan.
Patients were included in the study population if they had ≥1 pharmacy claim for UMEC/VI or TIO/OLO during the patient identification period, were aged ≥40 years as of the year of the index date (the date of first pharmacy fill for UMEC/VI or TIO/OLO), and had 12 months of continuous enrollment both before (pre-index) and after (post-index) the index date. Patients were excluded if they had a pharmacy or medical claim for an inhaled corticosteroid (ICS)- or LABA-containing controller medication during the pre-index period; pharmacy fills for both UMEC/VI and TIO/OLO, MITT (ie, triple therapy with ICS+LABA+LAMA), or non-index controller medication on the index date; or missing demographic information.
Endpoints
The primary endpoint was rescue medication use, defined as units of inhaled or nebulized medication containing a short-acting muscarinic antagonist or short-acting β2-agonist. One unit of rescue medication corresponded to one canister (ie, 200 puffs) of a metered-dose inhaler or approximately 100 doses of nebulized medication.
Medication adherence, defined as PDC≥80%, was a secondary endpoint. PDC was calculated by dividing the number of days with available index medication (based on the number of days supplied for filled prescriptions) by the number of days between the index prescription claim and a fill for a non-index controller medication or end of the study period, whichever came first. The calculation was corrected for inpatient events under the assumption that medication was supplied by the facility during hospitalization and overlapping pharmacy fills were pushed out.
Time to escalation to MITT was evaluated in a post hoc analysis. A binary variable was created to designate escalation to MITT during the post-index period (ie, the first day of overlapping days’ supply with ICS, LAMA, and LABA), and the time from the index date +1 to triple therapy was calculated.
Inverse probability of treatment weighting
Inverse probability of treatment weighting (IPTW) was used to remove systematic differences and to balance pre-index characteristics between study cohorts. Models were created separately for the commercial/MAPD population and for the PDP population. The model created for the PDP population included fewer variables, as medical claims data were not available for these patients. Pre-index variables included in the commercial and MAPD population and PDP IPTW models are shown in Table S1.
Logistic regression was used to estimate weights; potential predictors of treatment initiation were included as independent variables with cohort (UMEC/VI vs TIO/OLO) as the outcome. The weights for each cohort are the inverse fitted probability of being in that cohort, for a given covariate pattern. Weights were created separately for the commercial/MAPD population, including enrollment information and variables from both medical and pharmacy claims, and the PDP population, including enrollment information and variables from pharmacy claims. The populations were then combined to create a single weighting variable for the analyses. Following the weighting procedure, the distribution of the weights was reviewed for outliers, and the performance of the weighting was examined by comparing pre-index variables between the UMEC/VI and TIO/OLO cohorts using standardized differences and P-values. The weighting procedure accounts for differences in the number of patients included in each cohort, allowing data from all eligible patients to be retained in the analysis.
Statistical analysis
Patient demographics and clinical characteristics were assessed during a 12-month pre-index period and analyzed descriptively.
Treatment effects were estimated in two separate models; directly in the weighted sample (with no additional covariates), and using multivariable models with additional adjustment for pre-index variables with a post-IPTW standardized difference >0.10 (10%) or P<0.05 (Table S2).
For the primary endpoint, non-inferiority and superiority of UMEC/VI compared with TIO/OLO on rescue medication use were evaluated. The non-inferiority margin was set at 0.30 units of rescue medication (based on clinical relevance and previous RCT data7), and the superiority margin was set at 0 units in order to determine if UMEC/VI initiators had statistically fewer units of rescue medication compared with TIO/OLO initiators.
In the primary intent-to-treat (ITT) analysis, patients were not censored during the 12-month post-index period, and the number of rescue medication units was captured during the entire post-index period. In the on-treatment sensitivity analysis, patients were censored at the time of discontinuation of the index medication (defined as a gap in therapy of 45 days from the dispense date for a retail pharmacy fill or 115 days from the dispense date for a mail-order pharmacy fill), at the time of a pharmacy fill for a non-index controller medication, or at the end of the 12-month post-index period, whichever occurred first. In both analyses, weighted ordinary least squares regression with bootstrapped variance estimation was used. A total of 10,000 bootstrap iterations were conducted to produce variance parameters and P-values. The 95% CI and one-sided (α=0.025) bootstrapped P-values were used to determine if the non-inferiority and superiority criteria were met, with P<0.025 considered statistically significant.
Medication adherence (PDC≥80%) was modeled using weighted logistic regression with a robust variance estimator, and evaluated using an on-treatment analysis, in which patients were censored at the earliest of the time of a pharmacy fill for a non-index controller medication or the end of the 12-month post-index period.
Time to escalation to MITT was modeled using weighted Cox proportional hazards regression with a robust variance estimator and evaluated using an ITT analysis in which patients were not censored during the 12-month post-index period.
Sample size
Sample size calculations were based on a conservative approach assuming independent samples using a two-sample t-test (one-sided α=0.025) and 80% power. It was calculated that if the true mean difference in the number of rescue medication units between the UMEC/VI and TIO/OLO cohorts (SD) was −0.5 (8.67),9 a total of 2906 patients (1453 patients per group) and 7438 patients (3719 patients per group) would be required to demonstrate non-inferiority and superiority of the UMEC/VI to TIO/OLO, respectively.
Results
Study population
The study population comprised 14,324 patients, of whom 9549 initiated UMEC/VI (commercial/MAPD [N=3149]; PDP [N=6400]) and 4775 initiated TIO/OLO (commercial/MAPD [N=1114]; PDP [N=3661]; Figure 2).
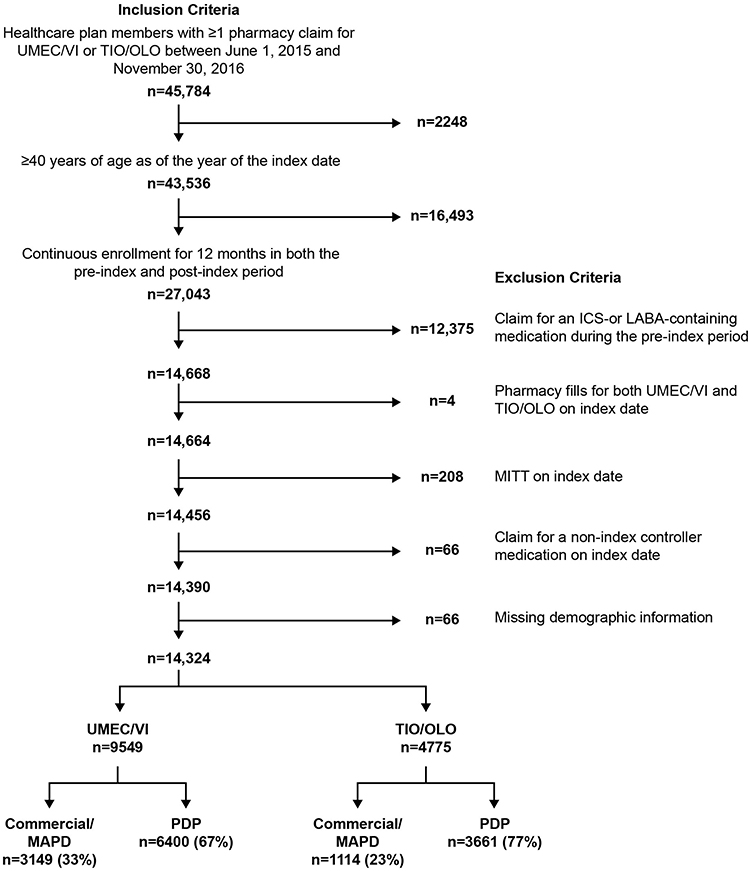 |
Figure 2 Patient enrollment. Abbreviations: ICS, inhaled corticosteroid; LABA, long-acting β2-agonist; MAPD, Medicare Advantage with Part D; MITT, multiple inhaler triple therapy; PDP, Part D-only, TIO/OLO, tiotropium bromide/olodaterol; UMEC/VI, umeclidinium/vilanterol. |
Baseline characteristics before and after IPTW are described in Tables 1 and 2, respectively. Most patients (UMEC/VI: 67.0%; TIO/OLO: 76.7%) were enrolled in a PDP health plan, and consequently, medical claims data were unavailable for these patients.
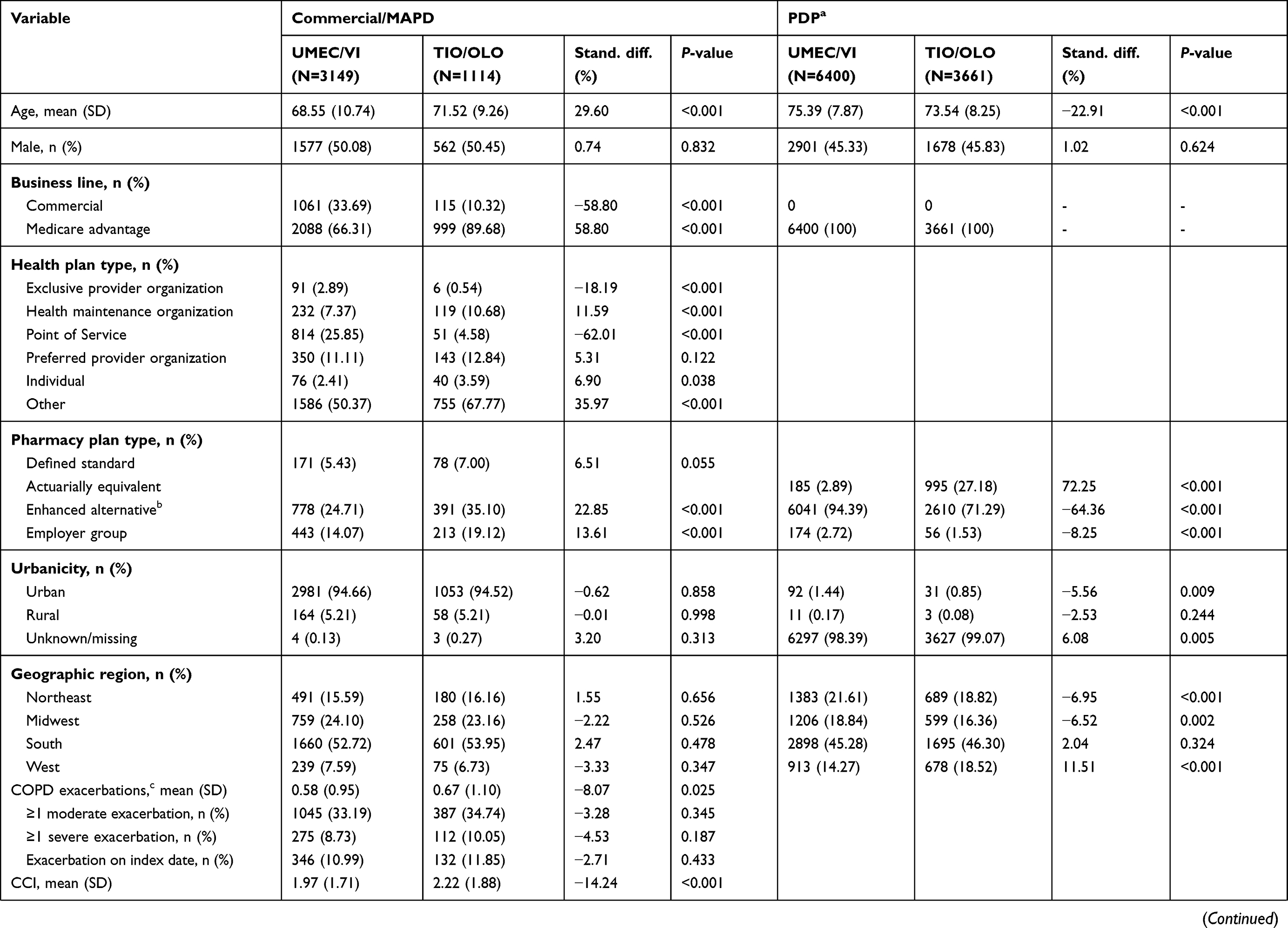 | 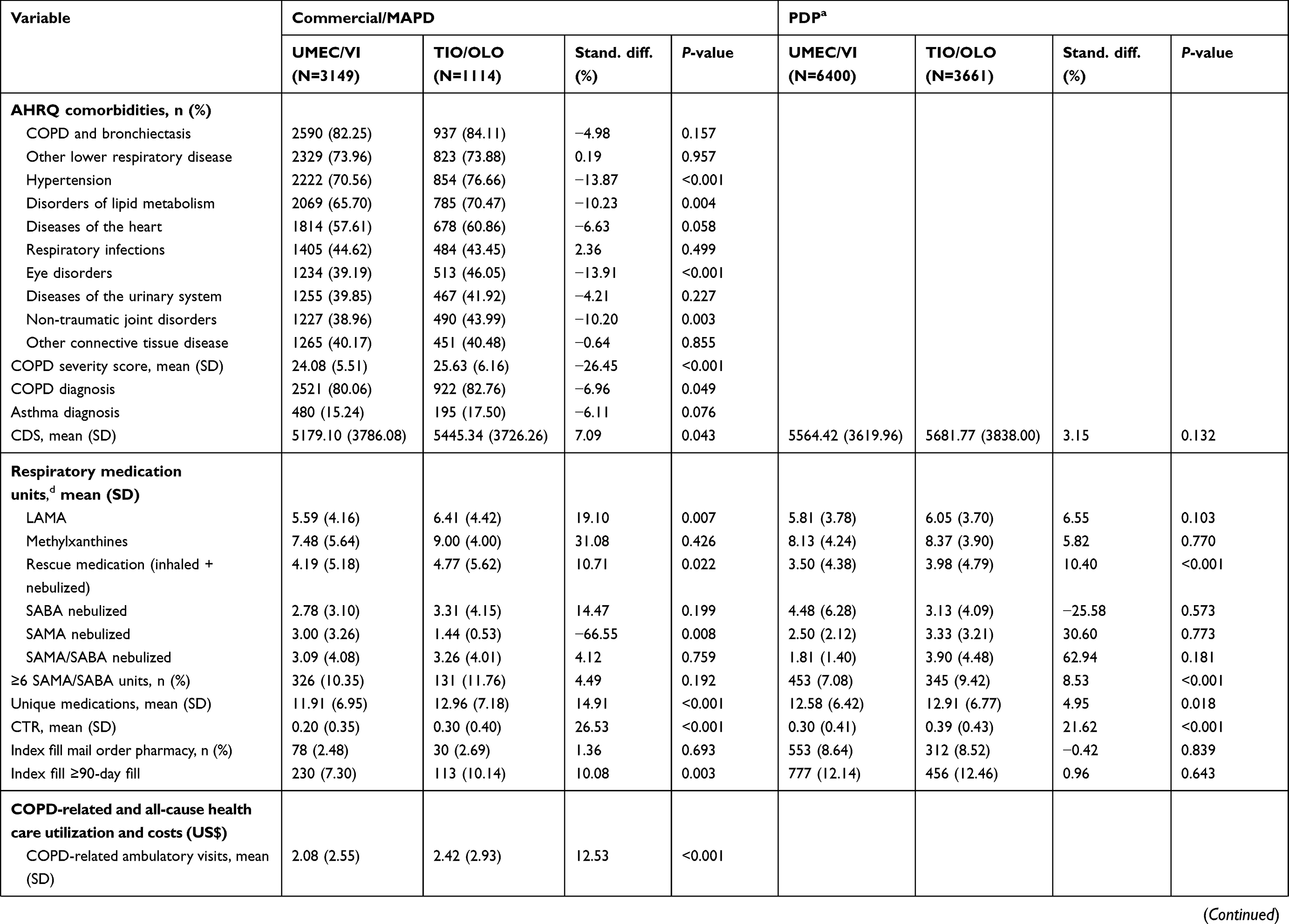 | 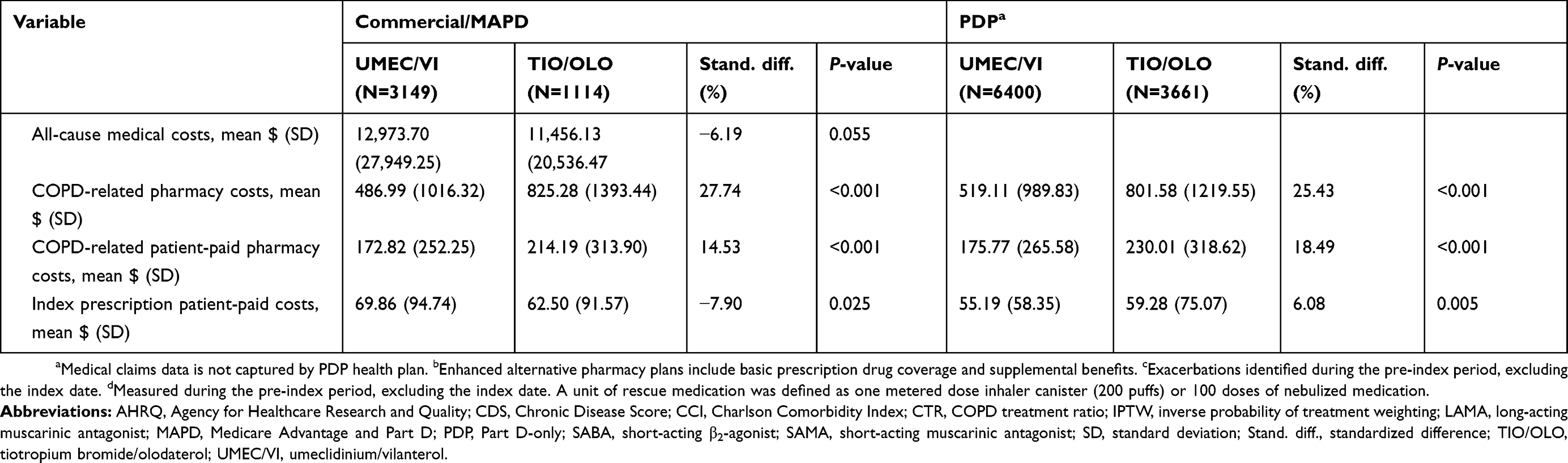 |
Table 1 Pre-index patient demographics and clinical characteristics before IPTW |
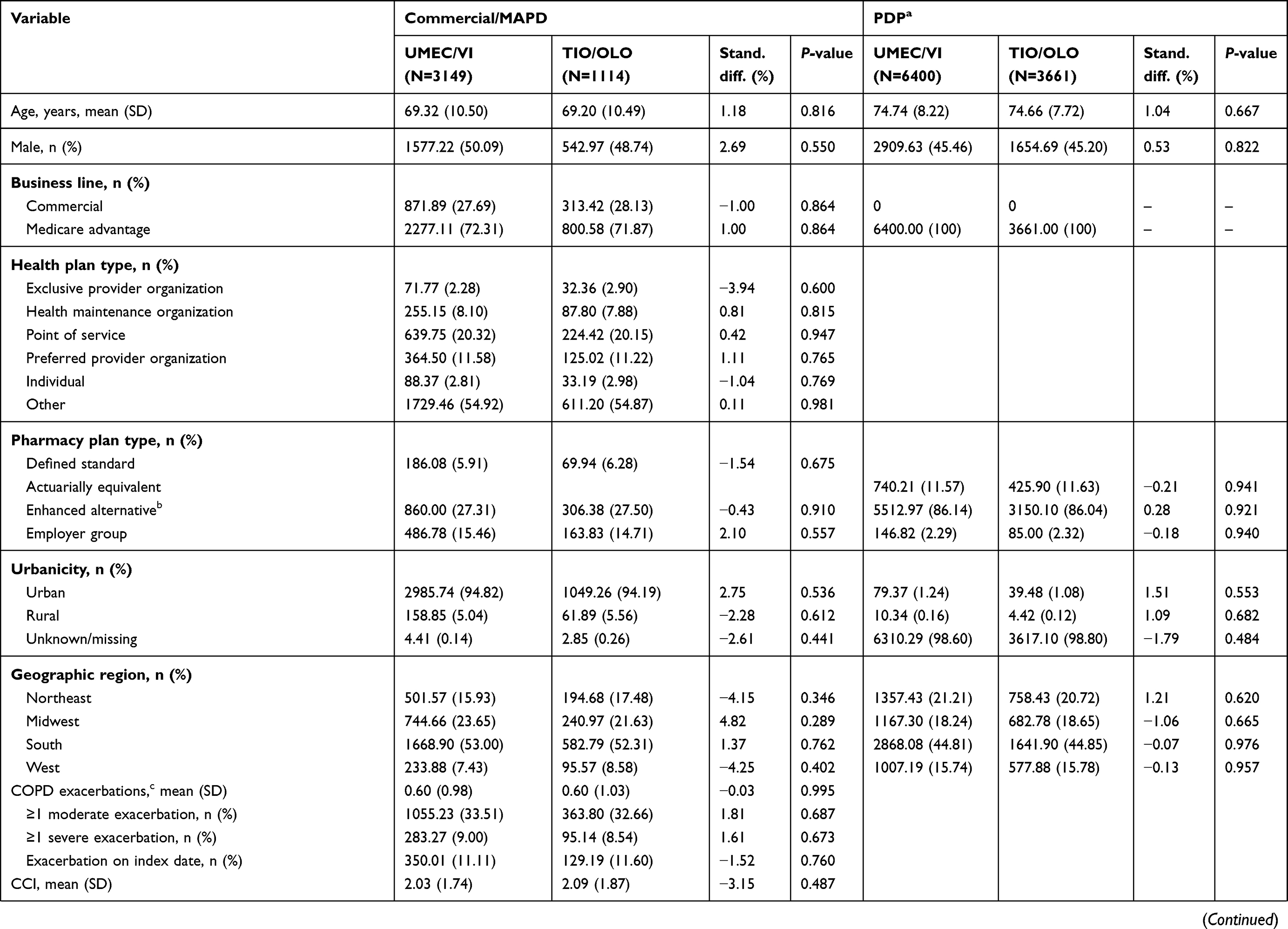 | 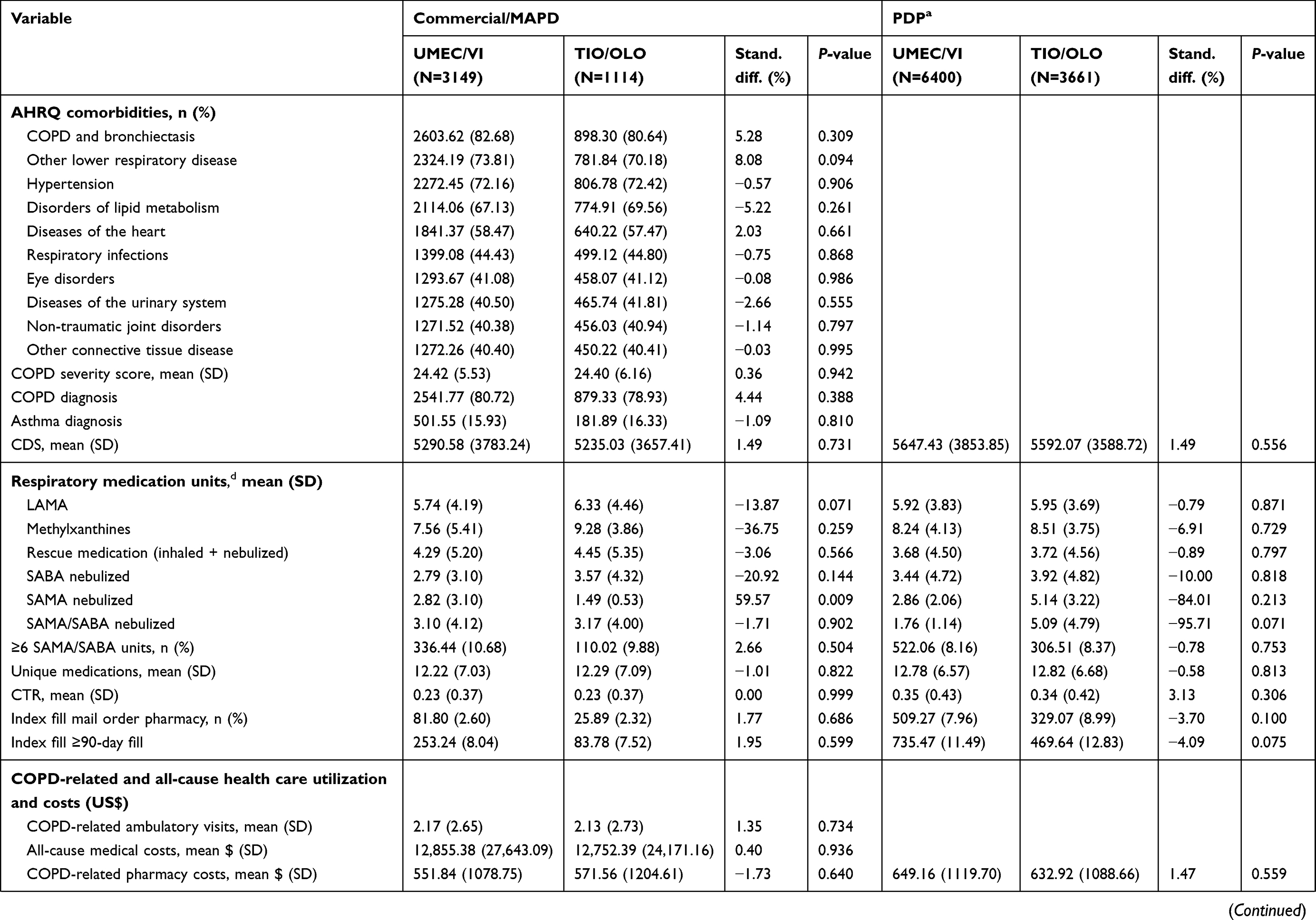 |  |
Table 2 Pre-index patient demographics and clinical characteristics after IPTW |
There were significant differences in the business line distribution between UMEC/VI and TIO/OLO initiators prior to IPTW in the commercial/MAPD population. In the overall population, 11.1% of UMEC/VI and 2.4% of TIO/OLO initiators were enrolled in a commercial plan; correspondingly, 88.9% of UMEC/VI initiators were enrolled in a Medicare Advantage plan (MAPD: 21.9%, PDP: 67.0%) and 97.6% of TIO/OLO initiators were enrolled in a Medicare Advantage plan (MAPD: 20.9%, PDP: 76.7%).
Most pre-index patient demographics and clinical characteristics were balanced following IPTW; however, balance (a standardized difference >0.10 [10%] or P<0.05) was not achieved for a subset of variables (Table S2).
All patients were ICS- and LABA-free during the pre-index period, as per the eligibility criteria. Most patients were also LAMA-naïve; pre-IPTW, 1858 (19.5%) patients in the UMEC/VI cohort and 1486 (31.1%) patients in the TIO/OLO cohort (P<0.001) had LAMA therapy in the pre-index period. After IPTW, the prevalence of LAMA treatment in the pre-index period was similar between cohorts (2293 [24.0%] patients and 1124 [23.5%] patients in the UMEC/VI and TIO/OLO cohorts, respectively [P=0.568]).
ITT analysis of rescue medication use
During the 12-month post-index period, the mean (SD) number of rescue medication units before adjustment was 1.87 (3.88) for the UMEC/VI cohort and 1.91 (3.75) units for the TIO/OLO cohort (P=0.607). After adjustment for residual imbalance in pre-index covariates, UMEC/VI initiators had 0.16 fewer rescue medication units PPPY than the TIO/OLO cohort (95% CI: −0.28, −0.04; Figure 3, Table S3). UMEC/VI met the pre-specified non-inferiority and superiority criteria, indicating that UMEC/VI was both non-inferior (P<0.001) and superior (P=0.005) to TIO/OLO on rescue medication use.
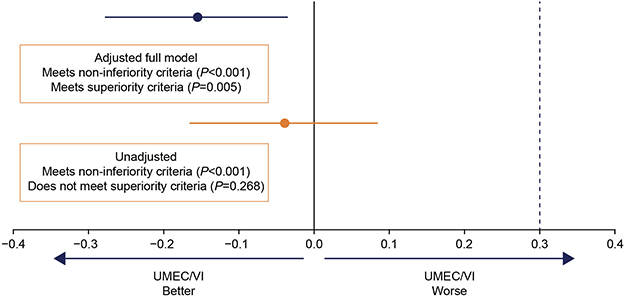 |
Figure 3 ITT analysis of difference in rescue medication use between the UMEC/VI and TIO/OLO cohorts. Covariates included in the adjusted model are shown in Table S2. Abbreviations: ITT, intent-to-treat; SABA, short-acting β2-agonist; SAMA, short-acting muscarinic antagonist; TIO/OLO, tiotropium bromide/olodaterol; UMEC/VI, umeclidinium/vilanterol. |
On-treatment sensitivity analysis of rescue medication use
The mean (SD) observed post-index on-treatment duration of index therapy (prior to censoring) was 104.6 (100.3) days in UMEC/VI initiators and 98.1 (93.5) days in TIO/OLO initiators.
After adjustment, UMEC/VI initiators had 0.18 fewer units of rescue medication PPPY than TIO/OLO initiators; the results of the on-treatment sensitivity analysis did not meet the pre-specified superiority criteria (95% CI: −0.38, 0.02; P=0.040; Figure 4, Table S4).
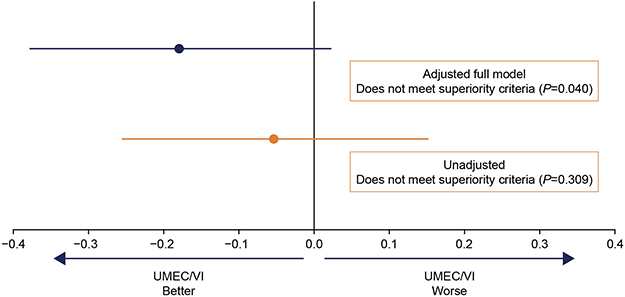 |
Figure 4 On-treatment sensitivity analysis of difference in rescue medication use between the UMEC/VI and TIO/OLO cohorts. Covariates included in the adjusted model are shown in Table S2. Abbreviations: SABA, short-acting β2-agonist; SAMA, short-acting muscarinic antagonist; TIO/OLO, tiotropium bromide/olodaterol; UMEC/VI, umeclidinium/vilanterol. |
On-treatment analysis of medication adherence
The mean (SD) observed post-index treatment duration of index therapy (prior to censoring) was 320.9 (99.5) days for UMEC/VI initiators and 315.8 (102.0) for TIO/OLO initiators.
The mean (SD) PDC was significantly higher in UMEC/VI initiators (0.50 [0.33]) compared with TIO/OLO initiators (0.47 [0.32]; P<0.001). Further, a significantly higher proportion of patients achieved PDC≥80% among UMEC/VI initiators (28.6%) compared with TIO/OLO initiators (22.7%; P<0.001). The adjusted odds of adherence (PDC≥80%) were 1.36 times higher among UMEC/VI initiators compared with TIO/OLO initiators (95% CI: 1.24, 1.49; P<0.001).
Post hoc ITT analysis of time to escalation to MITT
The incidence rate of MITT was similar between the UMEC/VI cohort (0.026 per 100 days) and the TIO/OLO cohort (0.027 per 100 days; P=0.361) during the 12-month post-index period. After adjustment, UMEC/VI initiators had a similar risk of escalation to MITT compared with TIO/OLO initiators (HR=0.93; 95% CI: 0.81, 1.06; P=0.268).
Discussion
This retrospective study using claims data from US patients evaluated rescue medication use and medication adherence with a post hoc analysis of the risk of escalation to MITT among a population of UMEC/VI and TIO/OLO initiators.
On the primary outcome of rescue medication use in the ITT population, UMEC/VI initiators met the pre-specified superiority criteria when compared with TIO/OLO initiators. Patients who initiated UMEC/VI used statistically significantly fewer units of rescue medication over the 12-month post-index period than those who initiated TIO/OLO. The observed difference of 0.16 units suggests that patients in the UMEC/VI cohort required 32 fewer puffs of rescue medication delivered via a metered-dose inhaler, or approximately 16 fewer doses of nebulized medication, per patient per year compared with the TIO/OLO cohort. However, the superiority criteria were not met in the on-treatment sensitivity analysis, despite a similar treatment difference in both analyses (0.16 vs 0.18 rescue medication units PPPY in the ITT vs sensitivity analyses). The results of this real-world study corroborate the findings of a recent head-to-head RCT, which demonstrated a significant reduction in rescue medication use as well as improvements in lung function with UMEC/VI compared with TIO/OLO over an 8-week period in both the ITT population7 and in a maintenance-naïve subgroup.8
For the secondary endpoint of medication adherence, mean PDC and the proportion of patients achieving a clinically significant level of adherence (PDC≥80%) were statistically significantly higher in the UMEC/VI cohort compared with the TIO/OLO cohort. Low levels of medication adherence are known to be an issue in patients with COPD. A previous retrospective study of US health care claims data showed that adherence to maintenance therapies for COPD (including LAMA and LAMA/LABA therapies) was low, with mean adherence of 0.47 for COPD maintenance therapy, which is consistent with low adherence seen for other classes of medication in patients with COPD (mean PDC of 0.33─0.71).10 Furthermore, low adherence to COPD maintenance medication is associated with increased morbidity and mortality,11 more frequent hospitalizations and greater health care spending per patient.12 In the present study, adherence (as assessed by mean PDC) was similar to previously reported values for other maintenance bronchodilator regimens; however, UMEC/VI initiators had 36% higher adjusted odds of clinically relevant adherence to their index treatment (PDC≥80%) than TIO/OLO initiators.
A number of factors can affect rates of adherence, including patients’ understanding and views of the disease and treatment, complexity of the treatment regimen with respect to the number of agents and dosing frequency, and ease of use of the inhaler device.13–15 UMEC/VI and TIO/OLO are both once-daily medications administered via a single inhaler, but are administered using different devices, which may influence adherence. Findings from a head-to-head trial suggest that patients who were inhaler-naïve preferred the ELLIPTA inhaler (used to administer UMEC/VI) over the Respimat inhaler (used to administer TIO/OLO) in terms of ease of use.7 Furthermore, fewer patients with COPD made critical errors when using the ELLIPTA inhaler compared with other inhalers in a randomized cross-over study,16 highlighting the ease of use associated with this device. Differences between the inhaler devices used to deliver UMEC/VI and TIO/OLO could contribute to the differences in rescue medication use and medication adherence among patients initiating these two LAMA/LABA FDCs.
In a post hoc analysis, there was no difference in the incidence of escalation to MITT between UMEC/VI and TIO/OLO treatment groups. A previous study showed an 87% higher risk of escalation to triple therapy in patients receiving TIO compared with UMEC/VI,17 which suggests that the risk of MITT may be reduced with LAMA/LABA compared LAMA monotherapy.
The present study had several important strengths. The study was conducted in a population of commercial and Medicare Advantage enrollees that represented a geographically diverse sample of the US population. IPTW was used to control for confounding of the association between the outcomes and the index treatments.
Several limitations should also be considered when interpreting the findings of the present study. Since clinical observations such as lung function outcomes are not recorded in claims data, an analysis of improvement in lung function outcomes during treatment with UMEC/VI compared with TIO/OLO was not possible. However, as noted above, a previous RCT has demonstrated that patients receiving UMEC/VI were twice as likely to achieve a clinically meaningful improvement in lung function over 8 weeks compared with patients receiving TIO/OLO.7 A general limitation of any observational study conducted using claims data is the dependence of the definition of study variables on administrative codes contained in the claims data. The presence of an administrative code does not guarantee, for example, that a patient has been diagnosed, has received medication, or whether medication received has actually been taken. To minimize the impact of these limitations on the results of the study, code lists were developed with clinical coding experts.
The design of this study also contained additional limitations. The definition of medication discontinuation may also have resulted in censoring of patients who later continued to take their index medication. Survivor bias may also have been introduced by the requirement for patients to have been continuously enrolled for 12 months following the index date, which could exclude patients with more severe or advanced COPD who did not survive.
Conclusion
This study is the first real-world head-to-head comparison of FDCs within the LAMA/LABA class. In the primary ITT analysis, patients initiating UMEC/VI used significantly less rescue medication and were more adherent to the treatment than patients initiating TIO/OLO. The results of this study provide further support of differences between LAMA/LABA FDCs, and may support the use of UMEC/VI as a preferred therapy within the LAMA/LABA class for patients.
Ethics approval and informed consent
This study utilized de-identified retrospective claims data, and as such, this study does not require institutional review board review and approval or informed consent procedures.
Data sharing statement
Information on GlaxoSmithKline’s (GSK) data sharing commitments and requesting access to anonymized individual participant data and associated documents from GSK-sponsored studies can be found at www.clinicalstudydatarequest.com. The data reported in this publication are contained in a database owned by Optum and contains proprietary elements. Therefore, it cannot be broadly disclosed or made publicly available at this time. The disclosure of this data to third-party clients assumes certain data security and privacy protocols are in place and that the third-party client has executed Optum’s standard license agreement which includes restrictive covenants governing the use of the data.
Acknowledgment
This study (207968/HO-17-18427) was funded by GSK. The funders of the study had a role in the study design, data analysis, data interpretation, and writing of the report. Employees of Optum were not paid for manuscript development. The authors would like to acknowledge Michael J Asmus (an employee of GSK at the time of the study) for his role in the design and interpretation of the study. The authors would like to acknowledge the following individuals for their contributions to this study: Lee Brekke of Optum for statistical consultation; Randall Gerdes, Priyanka Koka, and Feng Cao of Optum for programming support; Ashley Sluis of Optum for analytic support; and Megan Sipper and Caroline Jennermann of Optum for project management. Medical writing support was provided by Katie White, PhD, and Mark Condon, DPhil, of Fishawack Indicia Ltd, UK, funded by GSK.
Author contributions
CM, BH, RHS, and RR were involved in the conception/design of the study and analysis/interpretation of data. LGSB and LS were involved in the conception/design of the study, acquisition of data and analysis/interpretation of data. EK, LL, and JT were involved in the acquisition of data and analysis/interpretation of data. The authors take complete responsibility for the integrity of the data and accuracy of the data analysis, contributed to the writing and reviewing of the manuscript, gave final approval for the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
CM, BH, RR, and RHS are employees of GSK and hold stocks/shares in GSK. LGSB, EK, LL, and JT are employees of Optum. EK reports grant from GlaxoSmithKline, during the conduct of the study. LS was an employee of Optum at the time of the study, which was contracted by GSK to conduct the study. The authors report no other conflicts of interest in this work.
References
1. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease; 2019.
2. Chronic Obstructive Pulmonary Disorder Foundation. The COPD pocket consultant: COPD foundation guide for management of COPD; 2018. Available from: https://www.copdfoundation.org/Learn-More/Educational-Materials-Resources/Downloads-Library.aspx.
3. Boehringer Ingelheim Pharmacuticals Inc. Stiolto respimat US prescribing information; 2018. Available from: https://docs.boehringer-ingelheim.com/Prescribing%20Information/PIs/Stiolto%20Respimat/stiolto.pdf?DMW_FORMAT=pdf.
4. GlaxoSmithKline. Anoro Ellipta US prescribing information; 2017. Available from: https://www.gsksource.com/pharma/content/dam/GlaxoSmithKline/US/en/Prescribing_Information/Anoro_Ellipta/pdf/ANORO-ELLIPTA-PI-MG-IFU.PDF.
5. Calzetta L, Rogliani P, Matera MG, Cazzola M. A systematic review with meta-analysis of dual bronchodilation with LAMA/LABA for the treatment of stable COPD. Chest. 2016;149(5):1181–1196. doi:10.1016/j.chest.2016.02.646
6. Sion KYJ, Huisman EL, Punekar YS, Naya I, Ismaila AS. A network meta-analysis of long-acting muscarinic antagonist (LAMA) and long-acting β2-agonist (LABA) combinations in COPD. Pulm Ther. 2017;3(2):297–316. doi:10.1007/s41030-017-0048-0
7. Feldman GJ, Sousa AR, Lipson DA, et al. Comparative efficacy of once-daily umeclidinium/vilanterol and tiotropium/olodaterol therapy in symptomatic chronic obstructive pulmonary disease: a randomized study. Adv Ther. 2017;34(11):2518–2533. doi:10.1007/s12325-017-0626-4
8. Alcázar Navarrete B, Boucot I, Naya I, et al. Umeclidinium/vilanterol versus tiotropium/olodaterol in maintenance-naïve patients with moderate symptomatic chronic obstructive pulmonary disease: a post hoc analysis. Pulm Ther. 2018;4:171–183. doi:10.1007/s41030-018-0057-7
9. Buikema AR, Brekke L, Anderson A, et al. The effect of delaying initiation with umeclidinium/vilanterol in patients with COPD: an observational administrative claims database analysis using marginal structural models. Multidiscip Respir Med. 2018;13:38. doi:10.1186/s40248-018-0151-6
10. Dhamane AD, Schwab P, Hopson S, et al. Association between adherence to medications for COPD and medications for other chronic conditions in COPD patients. Int J Chron Obstruct Pulm Dis. 2017;12:115–122. doi:10.2147/COPD.S114802
11. Vestbo J, Anderson JA, Calverley PM, et al. Adherence to inhaled therapy, mortality and hospital admission in COPD. Thorax. 2009;64(11):939–943. doi:10.1136/thx.2009.113662
12. Simoni-Wastila L, Wei YJ, Qian J, et al. Association of chronic obstructive pulmonary disease maintenance medication adherence with all-cause hospitalization and spending in a Medicare population. Am J Geriatr Pharmacother. 2012;10(3):201–210. doi:10.1016/j.amjopharm.2012.04.002
13. Sanduzzi A, Balbo P, Candoli P, et al. COPD: adherence to therapy. Multidiscip Respir Med. 2014;9(1):60. doi:10.1186/2049-6958-9-60
14. Makela MJ, Backer V, Hedegaard M, Larsson K. Adherence to inhaled therapies, health outcomes and costs in patients with asthma and COPD. Respir Med. 2013;107(10):1481–1490. doi:10.1016/j.rmed.2013.04.005
15. Duarte-de-Araujo A, Teixeira P, Hespanhol V, Correia-de-Sousa J. COPD: understanding patients’ adherence to inhaled medications. Int J Chron Obstruct Pulm Dis. 2018;13:2767–2773. doi:10.2147/COPD.S160982
16. van der Palen J, Thomas M, Chrystyn H, et al. A randomised open-label cross-over study of inhaler errors, preference and time to achieve correct inhaler use in patients with COPD or asthma: comparison of ELLIPTA with other inhaler devices. NPJ Prim Care Respir Med. 2016;26:16079. doi:10.1038/npjpcrm.2016.79
17. Hahn B, Hull M, Blauer-Peterson C, Buikema AR, Ray R, Stanford RH. Rates of escalation to triple COPD therapy among incident users of LAMA and LAMA/LABA. Respir Med. 2018;139:65–71. doi:10.1016/j.rmed.2018.04.014
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.