")
Back to Journals » Vascular Health and Risk Management » Volume 13
Evaluation of pain during endovenous laser ablation of the great saphenous vein with ultrasound-guided femoral nerve block
Authors Al Wahbi AM
Received 21 February 2017
Accepted for publication 6 July 2017
Published 10 August 2017 Volume 2017:13 Pages 305—309
DOI https://doi.org/10.2147/VHRM.S135308
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Daniel Duprez
Abdullah M Al Wahbi
Division of Vascular Surgery, Department of Surgery, King Abdulaziz Medical City, Riyadh, Saudi Arabia
Background: Endoluminal laser ablation is now considered the method of choice for treating greater saphenous vein insufficiency. General anesthesia and peripheral nerve blocks with sedation have the risk of post-procedural delay in discharge and prolonged immobilization with the risk of deep vein thrombosis. The main pain experienced by patients during the procedure is during the laser ablation and the multiple needle punctures given along and around the great saphenous vein. The aim of our study was to evaluate the safety and efficacy of blocking the femoral nerve only under ultrasound-guidance without sedation, to reduce or prevent pain during injectable tumescent anesthesia in endovenous laser ablation of the greater saphenous vein.
Methods: Sixty patients in two groups underwent endovenous laser ablation for the greater saphenous vein insufficiency at an outpatient clinic. All patients received tumescent anesthesia. However, one group received a femoral nerve block (FNB) under ultrasound guidance before the procedure. All patients were asked to record the pain or discomfort, using the visual analog score, from the start of the procedure until the end of the great saphenous vein laser ablation. The length of the great saphenous vein and duration of the procedure were also recorded. The results were analyzed using statistical methods.
Results: No complications from FNB were observed. The pain associated with application of tumescent anesthesia and laser ablation was more intense in the group without an FNB (P < 0.001). There was no significant difference between the two groups in the length of the great saphenous vein or procedure duration.
Conclusion: Ultrasound-guided FNB (without other peripheral nerve blocks) is a safe, adequate, and effective option to decrease and/or eliminate the intraoperative discomfort associated with tumescent anesthesia injections and laser ablation during endoluminal laser ablation of the greater saphenous vein.
Keywords: femoral nerve block, endovascular laser ablation, tumescent anesthesia, varicose veins
Introduction
Lower extremity venous disease secondary to saphenous vein insufficiency is a common medical condition that decreases the patient’s quality of life.1 Traditionally, it was treated with high ligation and stripping, which required hospital admissions, prolonged immobilization, and complications such as wound infections, hematoma, and deep vein thrombosis. Advances in duplex ultrasound (DU) and the use of its detailed imaging, together with advances in the understanding the anatomy of truncal veins insufficiency, began the evolution of minimally invasive procedures using endoluminal venous thermal ablation techniques, such as endovenous laser ablation (EVLA). EVLA eliminates reflux with less morbidity, faster recovery, and improved cosmetic results with high patient satisfaction. As such, it has become the preferred treatment method for varicose veins since it was first introduced a decade ago, and it has evolved to being conducted as an outpatient procedure.2–5 However, one of the most uncomfortable steps in the procedure for patients is the multiple tumescent anesthesia (TA) injections given along the great saphenous vein (GSV) to avoid pain and complications in the surrounding tissue by heat. In fact, many new endovenous ablation techniques are being invented to mainly overcome this annoying step. Regional nerve blocks have been used in varicose vein surgeries and EVLAs.6 Anatomically, the sensory area of the medial side of the thigh over the GSV that is usually punctured to initiate TA is supplied by the femoral nerve.6,7 The femoral nerve block (FNB) under DU guidance is a short, technically easy, and fast-acting procedure.6,7 Furthermore, it has been reported to have great effect in reducing the discomfort of TA injections, making the whole procedure very tolerable. Multiple studies have shown the effectiveness of FNB; however, it has been used in combination with other nerve blocks or sedation that affect procedure time, postoperative mobility, and hospital stay.8–11 Few studies have reported using FNB only, followed by TA or with sedation.12–14 I report the effect of FNB and TA only for a completely painless EVLA procedure in an outpatient setting.
Methods
Sixty patients with symptomatic varicose veins and a unilateral symptomatic GSV reflux diagnosed by DU were included in the study. The detailed DU of the deep and superficial lower limbs venous systems was undertaken by certified vascular ultrasound technologists. All patients were informed about the details of the EVLA procedure on visiting the clinic, and the preoperative, postoperative, and discharge instructions. It was interesting how they were all excited at the short outpatient procedure; however, the majority were concerned about pain during TA injections as well as the pain and damage to the surrounding structures near the GSV during laser ablation. Then all patients were explained about the FNB under ultrasound guidance in detail and how it would minimize the pain from the multiple TA punctures. In addition, the purpose of the study, which was to observe and record pain or discomfort during TA injection that they may experience by filling the visual analog scale (VAS), was explained to them thoroughly. After all the discussions and answers, patients were divided into two groups: Group I (22 patients) declined the FNB before TA and Group II (38 patients) agreed to the FNB. After the approval of the Dr Suleiman Al Habib Medical Group Institutional Review Board and Ethics Committee for this study, I included two types of consents. Group I consent (NO FNB with TA) and Group II consent (FNB with TA).
All patients signed the written informed consents. All procedures, including intraoperative DU and FNB, TA injections, and EVLA, were undertaken by the author in the outpatient procedure room.
Procedures in both groups were conducted in the outpatient minor operating room with usual antiseptic techniques from the groin till the foot and sterile drabs. Vital signs and pulse monitoring with an oxygen monitor were affixed. Patients were positioned supine, with the leg slightly abducted and externally rotated. All patients were given the VAS at the beginning of the procedure.
EVLA for Group I (TA with no FNB)
The patient was placed supine, with the table in the reverse Trendelenburg position. After intradermal injection (30G; of a small amount of 1% lidocaine (Mercury Pharma International Ltd, Dublin, Ireland), the incompetent GSV was punctured with an 18G needle under ultrasound guidance. An angled tip 0.035 inch guidewire was then advanced and passed through the saphenofemoral junction (SFJ). The catheter was advanced over the guidewire and placed near to the junction. The guidewire was then removed and TA [lidocaine 400 mg/L (0.04%), epinephrine 1 mg/L (1: 1,000,000), and sodium bicarbonate 10 mEq/L] in a physiologic saline solution were then injected by a power pump, both along and around the vein, under ultrasound guidance. After TA, the laser fiber was inserted into the catheter and its tip was positioned several centimeters below the SFJ. Ablation was performed using 980-nm (A.R.C. Laser GmbH Nuremberg, Germany) or 810-nm (Angiodynamics, Queensbury, NY, USA) laser fibers giving 50–120 J/cm energy, depending on the diameter of reflux veins.
Group II (FNB + TA)
With the patients in the same position as in Group I, I started with the FNB procedure. The ultrasound transducer (Sono Site Micro Maxx, L25 probe; Sono Site, Bothell, WA, USA) was positioned transversely on the inguinal ligament to visualize the common femoral artery (CFA) and vein. The femoral nerve is identified as an oval hyperechoic structure lying lateral to the CFA. A 30G hypodermic needle was used to numb the skin, and a 25G needle was introduced at a 45-degree angle toward the nerve and lateral to the CFA. Aspiration was done to avoid intravascular injection. Then, 10 mL of 1% lidocaine was injected slowly and the clear spread of local anesthetic around the femoral nerve was confirmed. Patients were asked to notify the surgeon if they felt any tingling sensation along the medial side of the thigh.
After a few minutes of the block, the EVLA procedure was undertaken as in Group I. After an intradermal injection (30G) of a small amount of 1% lidocaine, the incompetent GSV was punctured with an 18G needle under ultrasound guidance. An angled tip 0.035 inch guidewire was then advanced and passed through the SFJ. The catheter was advanced over the guidewire and placed near to the junction. The guidewire was then removed and TA (lidocaine 400 mg/L [0.04%], epinephrine 1 mg/L [1:1,000,000], and sodium bicarbonate 10 mEq/L) in a physiologic saline solution was then injected by a power pump along and around the vein under ultrasound guidance. After TA, the laser fiber was inserted into the catheter and its tip was positioned several centimeters below the SFJ. Ablation was performed using 980-nm (A.R.C. Laser GmbH Nuremberg) or 810-nm (Angiodynamics) laser fibers emitting 50–120 J/cm of energy, depending on the diameter of reflux veins.
Legs were wrapped with compression bandages after the procedure. Patients were discharged after walking 15–20 minutes under the supervision of a nurse. No patient who underwent FNB reported muscle weakness or some noticeable tingling sensations. Intraoperative pain associated with applying the TA and laser ablation was analyzed using the VAS (0–10) in both groups.
Results
All 60 patients completed the study. There were no significant differences between the two groups with regard to age, gender, comorbidities, or the side of the procedure (Table 1), difference in procedure time, or the length of the GSV treated (Table 2). For both groups, pain on application of TA and laser ablation was measured using VAS. It revealed statistically significant differences between the two groups, where Group I (no FNB) had more intense pain during TA punctures than Group II (with FNB; p < 0.001; Table 2). All patients were discharged after a routine 20–25 minutes of walking under observation and instructed to be active (walking or performing foot exercises) for at least 4 hours while at home. No complications associated with the FNB were observed.
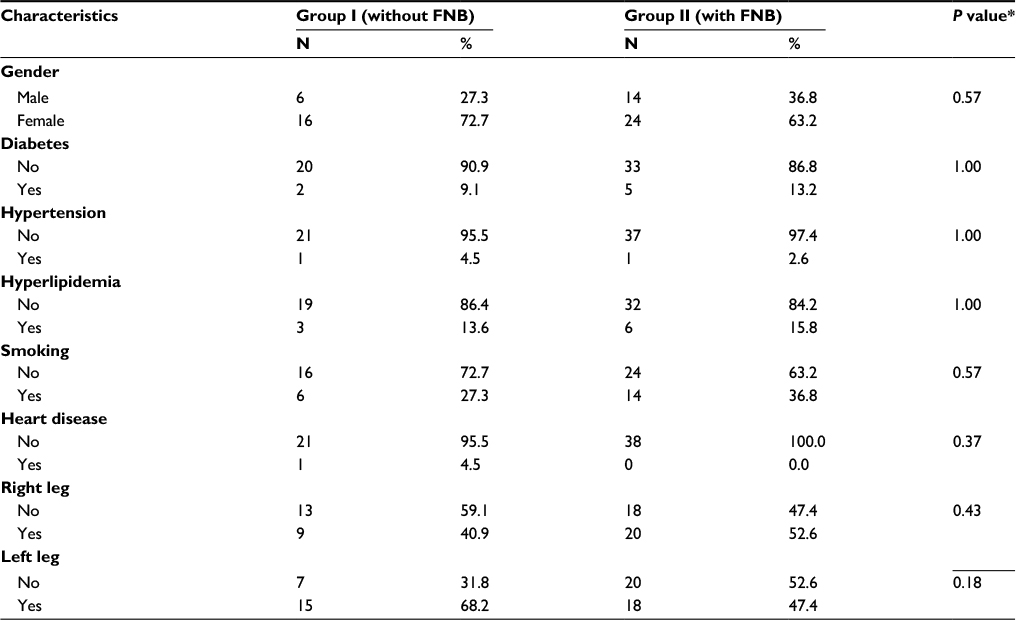 | Table 1 Demographic and side of EVLA data for both groups (with or without femoral nerve nlock [FNB]) Note: *Fisher’s exact test. |
 | Table 2 Comparison of both groups (with and without FNB) in GSV length, procedure time, and pain score (VAS) Abbreviations: FNB, femoral nerve block; GSV, great saphenous vein; VAS, visual analog scale. |
Discussion
Minimally invasive procedures using EVLA are a safe and effective way for eliminating reflux with less morbidity, faster recovery, and improved cosmetic results.5 This procedure is typically performed in an outpatient setting, and patients are discharged home several hours after the procedure.
Complications of surgical varicose veins management such as infection and nerve damage are common.4 General anesthesia and postoperative pain lead to longer hospital stay and post-procedural recovery.4,10
EVLA causes direct thermal injury to the endothelium and results in vessel occlusion. Multiple needle punctures are required to deliver TA around the GSV to prevent pain and protect the surrounding tissues from the heat of laser energy on the venous wall.3,5
Anesthesia of various kinds are used during EVLA mainly to prevent pain from the direct thermal injury of the vein and injury to the surrounding tissue. However, the multiple needle punctures given along the vein to deliver TA to most patients are the most annoying, painful experiences during the procedure. The use of epidural and general anesthesia or conscious sedation has a risk of deep vein thrombosis due to delayed mobilization as well as the high cost of dedicated staff and hospital stay.14–16 Furthermore, using regional nerve blocks such as spinal and sciatic blocks, in addition to the FNB, has the same risk of delayed mobilization and recovery.8–11
The femoral nerve is located lateral to the CFA in the triangular area formed by the iliac fascia, where the iliopsoas muscle forms the medial part of the triangle. The sensory innervation of the femoral nerve covers the skin and muscles along the medial aspect of the thigh and knee, which is the area used to administer TA during EVLA of the GSV. DU gives a very clear visualization of the anatomy of the triangle, and the femoral nerve is very clearly outlined lateral to the CFA, which makes its blocking technique easy, with minimal complications. Peripheral nerve blocks, as with any procedure, have known complications, and many factors contribute to that. The location of the nerve, the learning curve, patient conditions such as obesity, or whether it is a single injection block or a longer term catheter all play a role. The FNB has its share of complications such as infection, hematoma, and inadvertent femoral artery puncture. However, these complications are very rare now with the use of ultrasound guidance.7 I was fortunate that none of my patients who had FNB developed any complications. Further, I believe that the addition of an FNB under ultrasound guidance will significantly reduce the pain and discomfort caused by TA injections and allow early mobiliziation.12,13
Conclusion
For EVLA, I recommend using an FNB under DU guidance routinely as it is a short procedure, safe, efficient, technically easy, fast acting, and significantly reduces pain and discomfort.
Disclosure
The author reports no conflicts of interest in this work
References
Evans CJ, Fowkes FG, Ruckley CV, Lee AJ. Prevalence of varicose veins and chronic venous insufficiency in men and women in the general population: Edinburgh Vein Study. J Epidemiol Community Health. 1999;53(3):149–153. | ||
Min RJ, Khilnani NM. Endovenous laser ablation of varicose veins. J Cardiovasc Surg (Torino). 2005;46(4):395–405. | ||
Yılmaz S, Ceken K, Alparslan A, Sindel T, Lüleci E. Endovenous laser ablation for saphenous vein insufficiency: immediate and short-term results of our first 60 procedures. Diagn Interv Radiol. 2007;13:156–163. | ||
Hoggan BL, Cameron AL, Maddern GJ. Systematic review of the endovenous laser therapy versus surgery for the treatment of saphenous varicose veins. Ann Vasc Surg. 2009;23(2):277–287. | ||
Oğuzkurt L. Endovenous laser ablation for the treatment of varicose veins. Diagn Interv Radiol.2012;18(4):417–422. | ||
Meier G, Buettner J. Peripheral Regional Anesthesia. An Atlas of Anatomy and Techniques. New York: Georg Thieme Verlag; 2007:92–94 | ||
Jeng CL, Torrillo TM, Rosenblatt MA. Complications of peripheral nerve blocks. Br J Anaesth. 2010;105 (Suppl 1):i97–i107. | ||
Vloka JD, Hadzić A, Mulcare R, Lesser JB, Kitain E, Thys DM. Femoral and genitofemoral nerve blocks versus spinal anesthesia for outpatients undergoing long saphenous vein stripping surgery. Anesth Analg. 1997;84(4):749–752. | ||
Yilmaz S, Ceken K, Alimoglu E, Sindel T. US-guided femoral and sciatic nerve blocks for analgesia during endogenous laser ablation. Cardiovasc Intervent Radiol. 2013;36(1):150–157. | ||
Youssef K, Hakim K. Comparison of tumescent versus ultrasound guided femoral and obturator nerve blocks for treatment of varicose veins by endogenous laser ablation. Eg J Anaesth. 2014;30(3):279–283. | ||
Öztürk T, Çevikkalp E, Nizamoglu F, Özbakkaloğlu A, Topcu İ. The efficacy of femoral block and unilateral spinal anaesthesia on analgesia, haemodynamics and mobilization in patients undergoing endovenous ablation in the lower extremity. Turk J Anaesthesiol Reanim. 2016;44(2):91–95. | ||
Dzieciuchowicz L, Espinosa G, Grochowicz L. Evaluation of ultrasound-guided femoral nerve block in endoluminal laser ablation of the greater saphenous vein. Ann Vasc Surg. 2010;24(7):930–934. | ||
Hillermann T, Dullenkopf A, Joechle W, Traber J. Tumescent anaesthesia in combination with femoral nerve block for surgery of varicose veins: prilocaine 0.1% versus 0.2%. Phlebology. 2011;26(7):292–297. | ||
Van Den Bos RR, Neumann M, De Roos KP, Nijsten T. Endovenous laser ablation-induced complications: review of the literature and new cases. Dermatol Surg. 2009;35(8):1206–1214. | ||
Marsh P, Price BA, Holdstock J, Harrison C, Whiteley MS. Deep vein thrombosis (DVT) after venous thermoablation techniques: rates of endovenous heat-induced thrombosis (EHIT) and classical DVT after radiofrequency and endovenous laser ablation in a single center. Eur J Vasc Endovasc Surg. 2010;40(4):521–527. | ||
Doğru S, Kaya Z, Yılmaz Doğru H. Complications of spinal anaesthesia. J Contemp Med. 2012;2:127–134. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.