")
Back to Journals » Infection and Drug Resistance » Volume 15
Evaluation of Neisseria gonorrhoeae Isolates Susceptibility to Tetracycline Antibiotics from 9 Provinces in China Since 2020
Authors Zhou Q , Xu W , Zhu X, Zhang J, Zhang Y , Han Y, Chen K, Yin Y
Received 7 December 2021
Accepted for publication 16 March 2022
Published 30 March 2022 Volume 2022:15 Pages 1383—1389
DOI https://doi.org/10.2147/IDR.S352932
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Qian Zhou,1,2,* Wenqi Xu,1,2,* Xiaoyu Zhu,1,2 Jin Zhang,1,2 Yan Zhang,1,2 Yan Han,1,2 Kai Chen,1,2 Yueping Yin1,2
1Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College, Nanjing, People’s Republic of China; 2STD Reference Laboratory, National Center for Sexually Transmitted Diseases Control, Chinese Center for Disease Control and Prevention, Nanjing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yueping Yin, Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College, Nanjing, People’s Republic of China, Email [email protected]
Purpose: The increasing drug resistance of Neisseria gonorrhoeae has become a serious public health concern. This study investigated N. gonorrhoeae isolates susceptibility to tetracycline antibiotics and the correlation between minimum inhibitory concentrations (MICs) of different antibiotics. The presence of resistance determinants in N. gonorrhoeae strains displaying different levels of tigecycline resistance was also compared.
Methods: The minimum inhibitory concentrations (MICs) of tetracycline, minocycline, tigecycline, eravacycline, omadacycline on 412 N. gonorrhoeae isolates were measured by the agar dilution method. The MICs of ceftriaxone and azithromycin were also measured to determine the correlations between antibiotics by the value of the correlation coefficient R. The presence of resistance determinants was identified through polymerase chain reaction (PCR) and sequencing.
Results: The MIC90 was 64mg/L for tetracycline, 64mg/L for minocycline, 0.5mg/L for tigecycline, 0.5mg/L for eravacycline, 4mg/L for omadacycline, 0.25 mg/L for ceftriaxone, and 1mg/L for azithromycin. The MIC90 and mode of tigecycline and eravacycline were much lower than those of tetracycline and minocycline. A poor correlation between omadacycline, eravacycline and tetracycline susceptibility was observed. Minocycline has a strong correlation with tetracycline. PorB1 typing, TetM-encoding plasmid, and mtrR promoter adenine deletion were significantly correlated with tigecycline MIC > 0.25mg/L.
Conclusion: This study suggested that tigecycline and eravacycline had better in vitro activity and might be alternative antibiotics against resistant N. gonorrhoeae infections. Nevertheless, further in vitro experiments and clinical studies are needed for verification.
Keywords: Neisseria gonorrhoeae, antibiotics susceptibility, tigecycline, eravacycline, omadacycline
Introduction
Neisseria gonorrhoeae (N. gonorrhoeae) is the etiologic agent of gonorrhea which causes a sexually transmitted infection that presents a major global public health concern.1 According to the WHO estimation, there were 86.9 million incident global cases of gonorrhea among 15 to 49-year-old individuals in 2016.2 Currently, the treatment of N. gonorrhoeae infection mainly relies on a variety of antibiotics.3 Notably, as the sensitivity of N. gonorrhoeae to various therapeutic drugs decreases with time, multidrug-resistant (MDR) N. gonorrhoeae cases have been reported intermittently in many countries, including China.4–6 Hence, the detection of putative alternative antibiotics and search for new therapeutic options are the key to the accurate treatment of patients with gonorrhea and to hindering the progress of drug resistance.7
Tetracyclines are a type of antibiotic discovered in the 1940s. They were used in the early years to treat gonorrhea, especially in patients with penicillin allergies. With increasing drug resistance and the emergence of tetM-encoding plasmids, the clinical status of these antibiotics has gradually declined.8 In the last two decades, tetracyclines have reappeared on the market as the third-generation tetracycline antibiotics (tigecycline, eravacycline, sarecycline and omadacycline) were discovered.9,10
The existing studies on the susceptibility of these tetracycline antibiotics of N. gonorrhoeae remain limited. While research on tetracyclines has progressed, subsequent evaluation of these antibiotics against N. gonorrhoeae is imperative. In this study, we analyzed the susceptibility of 412 N. gonorrhoeae isolates to seven antibiotics including five tetracycline antibiotics, ceftriaxone, and azithromycin.
Materials and Methods
Gonococcal Isolates
Clinical strains of 412 N. gonorrhoeae isolates were collected from 9 Chinese provinces (Guangdong (n=68), Sichuan (n=43), Hainan (n=36), Yunnan (n=47), Shanxi (n=18), Chongqing (n=49), Jiangsu (n=46), Guangxi (n=64), Shaanxi (n=41)) between 1 January and 31 December 2020. All the isolated strains were from urogenital secretions of confirmed gonorrhea patients and identified as N. gonorrhoeae after isolation, identification and pure culture. This project was approved by the Medical Ethics Committee at the Institute of Dermatology, the Chinese Academy of Medical Sciences & Peking Union Medical College and the National Center for Sexually Transmitted Disease Control (2014-LS-026). This study complies with Declaration of Helsinki. Participants no less than 18 years of age who signed an informed consent form to provide urine, vaginal and rectal swabs were enrolled in the study. All the strains were stored in skim milk in a deep freezer at −80°C before antimicrobial agent susceptibility testing. The WHO reference N. gonorrhoeae strains G, J, K, O, P, V, X, Y, and Z were used for quality control.
Antimicrobial Susceptibility Testing
Based on the WHO standard operation of the agar dilution method,11 the antimicrobial susceptibility of all isolates was tested to seven antibiotics (ceftriaxone, azithromycin, tetracycline, minocycline, tigecycline, eravacycline and omadacycline). Eravacycline and omadacycline were obtained from Shanghai ZZBIO Co., Ltd (Shanghai, China). Tigecycline was obtained from Beijing BIOBW Co., Ltd (Beijing, China). Tetracycline, minocycline, ceftriaxone and azithromycin were obtained from the United States Pharmacopeia.
First, the N. gonorrhoeae isolates were revived on culture media overnight and then suspended in Mueller-Hinton (MH) broth. Subsequently, 2 μL of bacterial suspension at 107 CFU/mL was transferred onto antimicrobial medium which was a mixture of antibiotic and GC agar bases. Thereafter, the plates were incubated for 18–24 hours at 36°C in a 5% CO2-enriched atmosphere. Ultimately, the growth of N. gonorrhoeae in each concentration of antimicrobial-containing media was observed and recorded. The susceptibility test was conducted following the WHO guidelines11 and the results were interpreted according to CLSI guidelines.12
Sequence Analysis of Resistance Determinants
There are no standardized criteria in the breakpoint of tigecycline against N. gonorrhoeae. According to the susceptibility test results, US Food and Drug Administration (FDA) interpretive criteria,13 and relevant reference,14 we chose 0.25mg/L as the breakpoint to distinguish the different levels of tigecycline resistance. Forty N. gonorrhoeae isolates with tigecycline MIC >0.25mg/L and 40 N. gonorrhoeae isolates with tigecycline MIC ≤0.25mg/L were randomly selected to investigate the possible resistance determinants of tigecycline and the source of the correlation between the MICs of tigecycline and other antibiotics. PCR was utilized to amplify five loci (rpsJ, mtrR, porB, tetM and 23S rRNA) using previously reported primers14,15 (Table 1). DNAs were sequenced using Sanger sequencing. DNA sequences were analyzed using Snapgene 5.3. Moreover, the AMR markers of mtrR, porB, and 23S rRNA were analyzed via the NG-STAR website (https://ngstar.canada.ca).16
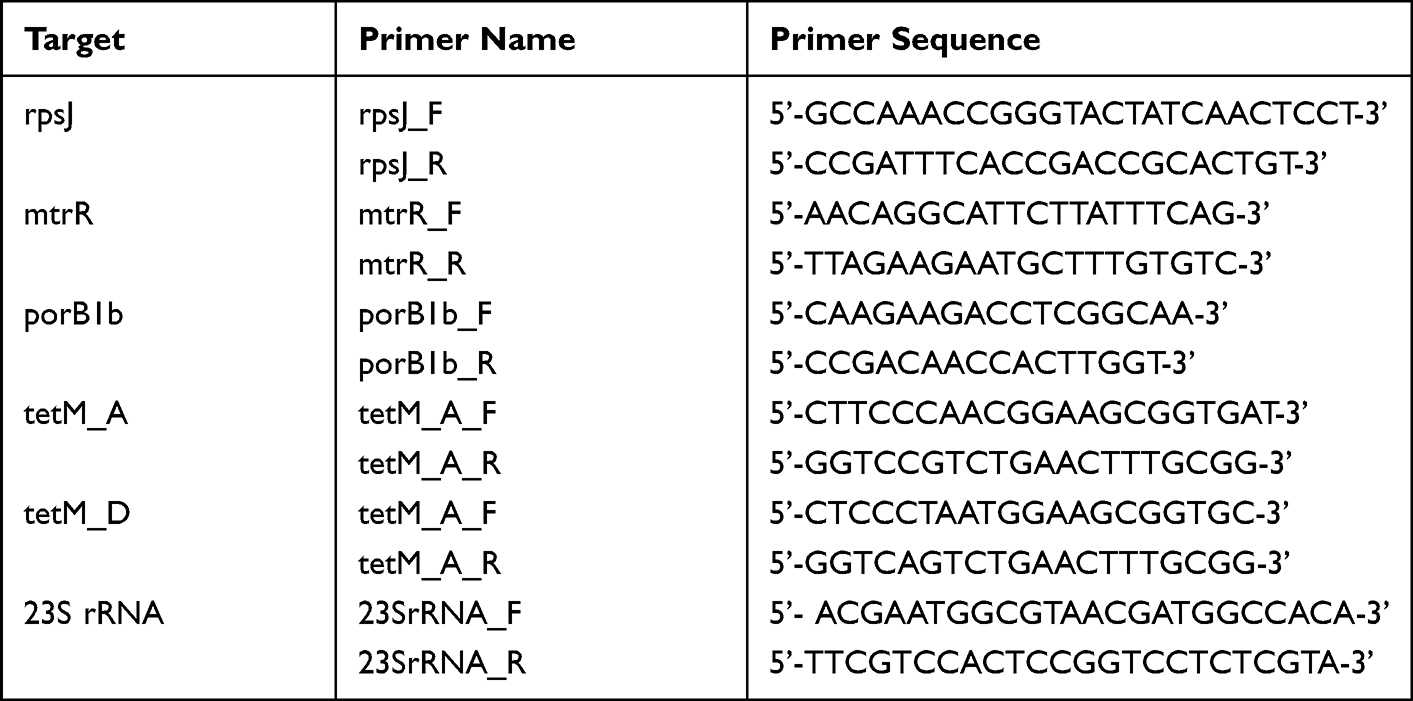 |
Table 1 Primers Implemented for PCR Assay and Target Mutations |
Statistical Analysis
Descriptive statistics (range, mode, MIC50, MIC90) were calculated to characterize the distribution of antibiotic MIC results. Furthermore, the correlations between antibiotics were determined by the value of the correlation coefficient R after logarithmic conversion of the MIC value. More specifically, poor, medium and strong correlations correspond to R values between 0.3–0.5, 0.5–0.8 and 0.8–1 respectively. The relation between gene mutation and drug resistance was interpreted through the chi-square test or Fisher’s exact test, in which P values lower than 0.05 indicated statistical significance. SPSS software 22.0 (SPSS Inc., Chicago, USA) and Excel 2019 (Microsoft, Washington, USA) were applied for data analysis. Figures were made in RStudio.
Results
Antimicrobial Susceptibility Results of 412 N. gonorrhoeae Isolates
The susceptibility of the 412 clinical isolates was summarized in Tables 2 and S1. In total, tetracycline MIC values of 84.7% of these isolates were greater than or equal to 2mg/L, which was considered a clinical breakpoint for tetracycline resistance.17 In comparison, the MIC range of minocycline was 0.25–64mg/L, while its MIC90 was the same as that of tetracycline. Meanwhile, the MIC90 and mode of tigecycline and eravacycline were 0.5mg/L and 0.25mg/L respectively, which were much lower than those of tetracycline and minocycline. 70.1% of the isolates showed a tigecycline MIC≤0.25mg/L and 88.3% showed an eravacycline MIC≤0.25 mg/L. However, only 3 of 412 clinical isolates had a tigecycline MIC of 1mg/L. All the strains displayed a MIC≤0.5mg/L for eravacycline. Furthermore, the MIC90 and mode of omadacycline were 4mg/L, which was higher than those of other third-generation tetracyclines.
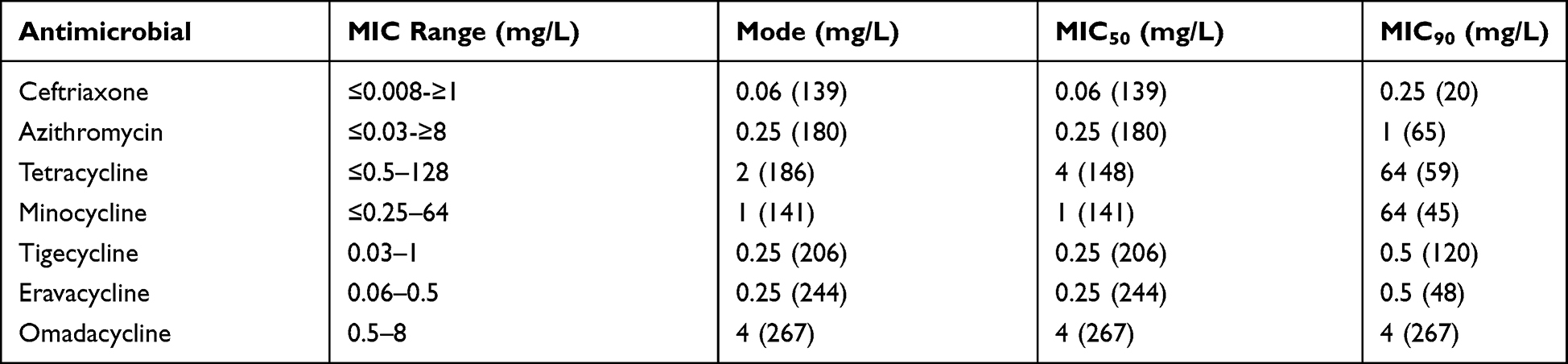 |
Table 2 Antimicrobial Susceptibility Results of 412 N. gonorrhoeae Isolates (Number of Strains Were Indicated in Parentheses) |
Cross-Resistance Analysis for Different Drugs
To detect potential cross-resistance of N. gonorrhoeae between different antibiotics, the correlation between the MICs of four tetracycline antibiotics (minocycline, tigecycline, eravacycline and omadacycline) with tetracycline, ceftriaxone and azithromycin was compared (Figure 1). Among them, only minocycline and tetracycline showed a strong correlation (R=0.96). Apart from that, only weak correlations were observed: tigecycline with azithromycin (R=0.44), omadacycline with tetracycline (R=0.36) and eravacycline with tetracycline (R=0.38).
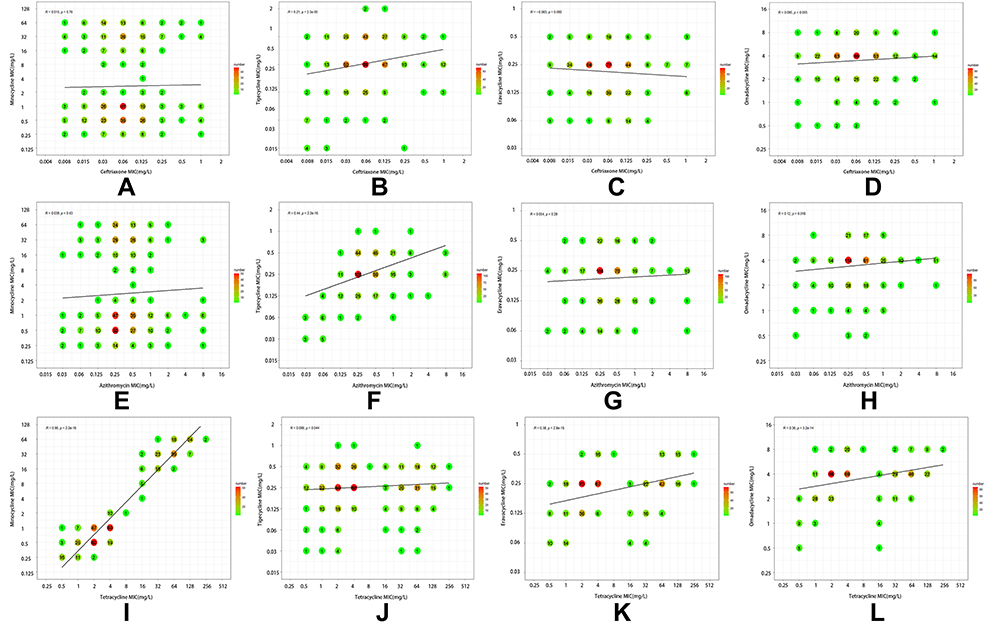 |
Figure 1 Correlation between MICs of four tetracycline antibiotics and tetracycline, ceftriaxone or azithromycin. Each symbol with specific numbers and colors represents one or multiple isolates. MIC values were log-transformed (log2) before calculating the regression line. (A–D) Correlation between MICs of minocycline, tigecycline, eravacycline, omadacycline and ceftriaxone. (E–H) Correlation between MICs of minocycline, tigecycline, eravacycline, omadacycline and azithromycin. (I–L) Correlation between MICs of minocycline, tigecycline, eravacycline, omadacycline and tetracycline. |
Possible Resistance Determinants of Tigecycline
Considering the susceptibility test results, US Food and Drug Administration (FDA) MIC interpretative breakpoints,13 and relevant reference,14 0.25mg/L was chosen as the breakpoint of different levels of tigecycline resistance to delve into possible resistance determinants (Table 3). All porb1a strains were detected to be tigecycline sensitive through drug resistance gene scanning. In particular, susceptibility to porb1b mutations significantly correlated with tigecycline resistance (MIC>0.25mg/L). Moreover, the tetM plasmid correlated significantly with tigecycline (MIC>0.25mg/L), while tetM typing demonstrated no correlation with tigecycline susceptibility. Further typing of mtrR and 23S rRNA genes showed that mtrR promoter-35ΔA was significantly correlated with tigecycline MIC > 0.25mg/L.
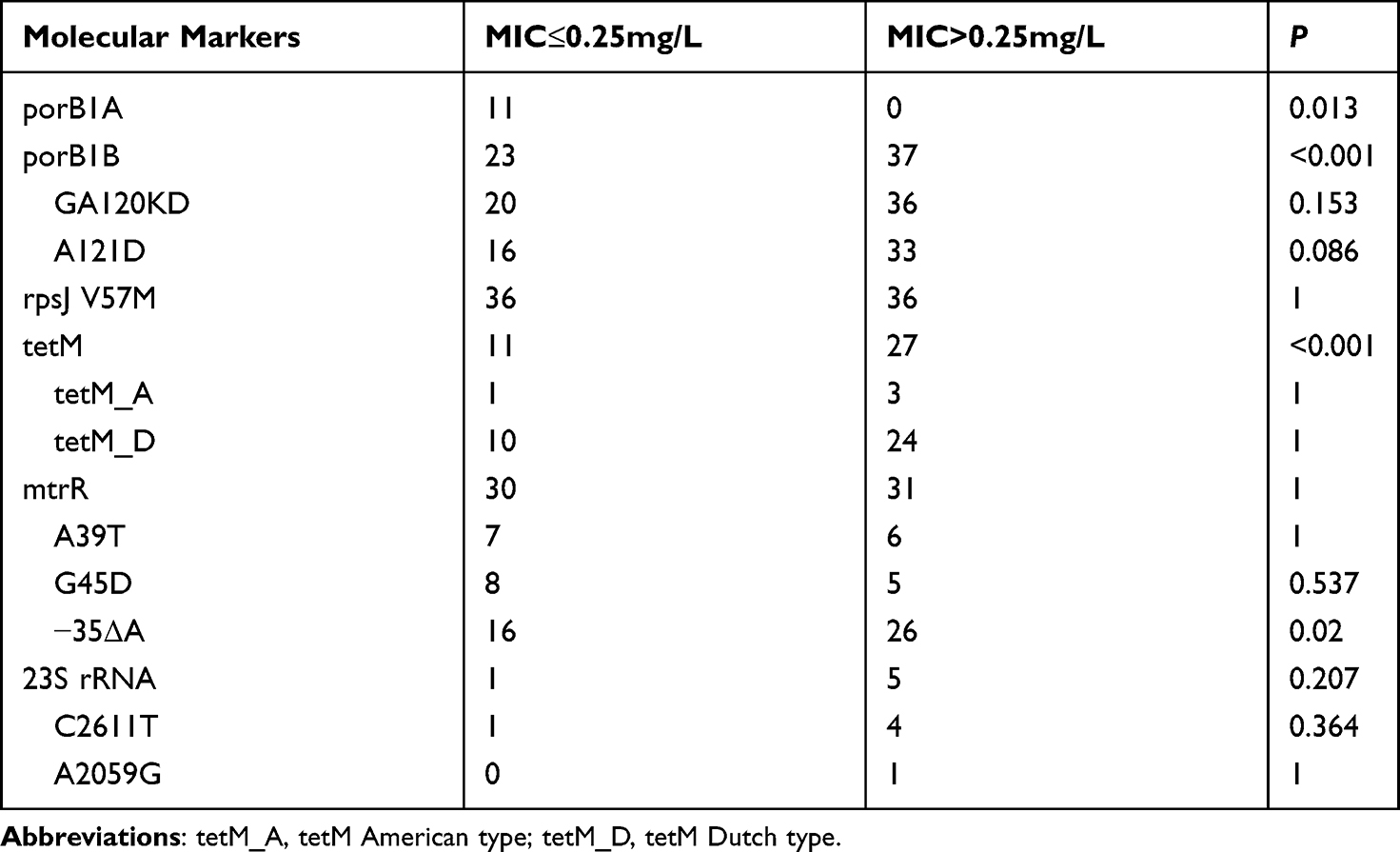 |
Table 3 Presence of Resistance Determinants in N. gonorrhoeae Strains Displaying High Tigecycline MICs or Low Tigecycline MICs |
Discussion
According to some national and WHO current treatment guidelines,18–20 combination therapy with ceftriaxone and azithromycin is the recommended way to treat gonorrhea.21 However, the constant emergence of multidrug-resistant (MDR) N. gonorrhoeae isolates continues to hamper the curative effect of the aforementioned dual antibiotic therapy.22 Against the tendency of increased antibiotic resistance, suggestions from the WHO include “development of new antibiotics”, “recycling of old drugs”, etc.23 With the listing of new tetracycline antibiotics, the effect of the second generation and third generation of tetracyclines against N. gonorrhoeae need to be further reevaluated. For this purpose, this study investigated for the first time all three generations of tetracyclines simultaneously, which can serve as an alternative therapy for N. gonorrhoeae infection.
Minocycline is a second-generation tetracycline antibiotic that was discovered in the 1970s. Its effectiveness against drug-resistant bacteria has made it favored in the clinic. In this study, the MIC range of minocycline was 0.25–64mg/L and the MIC90 was the same as that of tetracycline. It could also be seen from the correlation analysis of the MIC values that minocycline has a strong correlation with tetracycline. Until then, no in vitro experiments on the resistance of N. gonorrhoeae to minocycline have been carried out. Only studies proved the synergistic effect of minocycline, azithromycin and ceftriaxone in vitro.24 Therefore, further trials should be conducted to confirm the effect of minocycline.
Tigecycline is a third-generation tetracycline antibiotic that has been widely studied in recent years. The results showed that the MIC90 of tigecycline was 0.5mg/l, and only 3 of 412 clinical isolates had a tigecycline MIC of 1mg/L. Through correlation analysis, tigecycline was only found to be weakly correlated with azithromycin and had no correlation with tetracycline and ceftriaxone. In the possible resistance determinants analysis, tigecycline (MIC>0.25mg/L) demonstrated no correlation with 23S rRNA mutation, which can lead to the medium and high resistance to azithromycin.25,26 This result indicates that tigecycline can be used in patients infected with ceftriaxone and tetracycline resistant N. gonorrhoeae. Our results were consistent with previous studies in Zhejiang/China and Canada,14,27 suggesting that tigecycline can be a candidate for gonococcal treatment in the future.
Eravacycline and omadacycline are both third-generation tetracycline antibiotics approved by the FDA in 2018.28 Some countries have approved the former in the treatment of complicated intra-abdominal infections.29 In our experiments, the MIC range of eravacycline against N. gonorrhoeae isolates was 0.06–0.5 mg/L. Approximately 88.3% of N. gonorrhoeae isolates had an eravacycline MIC below the susceptible breakpoint provided by the CLSI guidelines for Staphylococcus aureus (≤0.25 mg/L) and 100% had an eravacycline MIC below the susceptible breakpoint for Escherichia coli (≤0.5mg/L). Correlation analysis revealed a weak correlation with tetracycline and no correlation with ceftriaxone and azithromycin. These conclusions on antimicrobial susceptibility were similar to those proposed by other researchers.27 Both in vitro results suggest the possibility of applying eravacycline in the treatment of gonococcal infection.
Omadacycline is a semisynthetic drug that is effective against Gram-positives and some Gram-negatives.30 It is currently approved by the FDA for the treatment of acute bacterial skin, skin structure infection and community-acquired bacterial pneumonia.31 As observed in our experiment, the MIC90 of omadacycline was 4mg/L, which was higher than that of the other two third-generation tetracyclines. In consideration of the correlation with other antibiotics, only a weak correlation was found between it and tetracycline. In the pharmacokinetic study of Rodvold et al, omadacycline exhibited unsatisfactory in vivo availability, a single oral dose of 300 mg or intravenous injection dose of 100 mg of omadacycline resulted in a maximum plasma concentration of approximately 0.5–0.6 mg/L.32 Considering the difficult availability and high price of omadacycline, it is not suggested as a candidate drug to treat the gonococcal infection.
Conclusion
In this study, the activities of tetracycline antibiotics against N. gonorrhoeae were assayed in vitro. Compare to minocycline and omadacycline, tigecycline and eravacycline had better in vitro activity and might be alternative antibiotics against resistant N. gonorrhoeae infections, while the effect of minocycline and omadacycline needs further investigation. Hence, more in vitro experiments and clinical studies are needed to validate the findings in this paper and provide possible doses used for human clinical practice.
Data Sharing Statement
The data that supports the findings of this study are available in the Supplementary Material of this article.
Acknowledgments
This work was supported by the National Science and Technology Major Project (2018ZX101010 01-004-003), the Nanjing Incubation Program for National Clinical Research Center (20190600010) and the Natural Science Foundation of Jiangsu Province (BK20180156). The sponsors of this study had no role in study design, data collection, data analysis, data interpretation and writing of the article.
Disclosure
The authors declare that there is no conflict of interest regarding the publication of this article.
References
1. Quillin SJ, Seifert HS. Neisseria gonorrhoeae host adaptation and pathogenesis. Nat Rev Microbiol. 2018;16(4):226–240. doi:10.1038/nrmicro.2017.169
2. Rowley J, Vander Hoorn S, Korenromp E, et al. Chlamydia, gonorrhoea, trichomoniasis and syphilis: global prevalence and incidence estimates, 2016. Bull World Health Organ. 2019;97(8):548–562p. doi:10.2471/BLT.18.228486
3. Unemo M, Seifert HS, Hook EW
4. Dong HV, Klausner JD. Neisseria gonorrhoeae resistance driven by antibiotic use. Nat Rev Urol. 2019;16(9):509–510. doi:10.1038/s41585-019-0206-2
5. Chen SC, Han Y, Yuan LF, Zhu XY, Yin YP. Identification of internationally disseminated ceftriaxone-resistant Neisseria gonorrhoeae strain FC428, China. Emerg Infect Dis. 2019;25(7):1427–1429. doi:10.3201/eid2507.190172
6. Williamson DA, Fairley CK, Howden BP, et al. Trends and risk factors for antimicrobial-resistant Neisseria gonorrhoeae, Melbourne, Australia, 2007 to 2018. Antimicrob Agents Chemother. 2019;63(10). doi:10.1128/AAC.01221-19
7. Seña AC, Bachmann L, Johnston C, et al. Optimising treatments for sexually transmitted infections: surveillance, pharmacokinetics and pharmacodynamics, therapeutic strategies, and molecular resistance prediction. Lancet Infect Dis. 2020;20(8):e181–e191. doi:10.1016/S1473-3099(20)30171-7
8. Nelson ML, Levy SB. The history of the tetracyclines. Ann N Y Acad Sci. 2011;1241:17–32. doi:10.1111/j.1749-6632.2011.06354.x
9. Lee YR, Burton CE. Eravacycline, a newly approved fluorocycline. Eur J Clin Microbiol Infect Dis. 2019;38(10):1787–1794. doi:10.1007/s10096-019-03590-3
10. Dougherty JA, Sucher AJ, Chahine EB, Shihadeh KC. Omadacycline: a new tetracycline antibiotic. Ann Pharmacother. 2019;53(5):486–500. doi:10.1177/1060028018818094
11. Unemo M, Ballard R, Ison C, et al. Laboratory diagnosis of sexually transmitted infections, including human immunodeficiency virus; 2013.
12. Wayne P Clinical and laboratory standards institute. Performance standards for antimicrobial susceptibility testing; 2011.
13. Pfizer Inc. (Wyeth Pharmaceuticals). Tygacil® product insert. Philadelphia, PA. Available from: http://labeling.pfizer.com/showlabeling.aspx?id=491&pagename=tygacil_fly.
14. Yang F, Yan J, Zhang J, van der Veen S. Evaluation of alternative antibiotics for susceptibility of gonococcal isolates from China. Int J Antimicrob Agents. 2020;55(2):105846. doi:10.1016/j.ijantimicag.2019.11.003
15. Dong Y, Yang Y, Wang Y, Martin I, Demczuk W, Gu W. Shanghai Neisseria gonorrhoeae isolates exhibit resistance to extended-spectrum cephalosporins and clonal distribution. Front Microbiol. 2020;11:580399. doi:10.3389/fmicb.2020.580399
16. Demczuk W, Sidhu S, Unemo M, et al. Neisseria gonorrhoeae sequence typing for antimicrobial resistance, a novel antimicrobial resistance multilocus typing scheme for tracking global dissemination of N. gonorrhoeae strains. J Clin Microbiol. 2017;55(5):1454–1468. doi:10.1128/JCM.00100-17
17. Patel J, Weinstein M, Eliopoulos G, et al. M100 Performance Standards for Antimicrobial Susceptibility Testing. Wayne, PA, USA: Clinical and Laboratory Standards Institute; 2017.
18. Bignell C, Unemo M. 2012 European guideline on the diagnosis and treatment of gonorrhoea in adults. Int J STD AIDS. 2013;24(2):85–92. doi:10.1177/0956462412472837
19. Workowski KA. Centers for disease control and prevention sexually transmitted diseases treatment guidelines. Clin Infect Dis. 2015;61(Suppl 8):S759–762. doi:10.1093/cid/civ771
20. Unemo M, Shafer WM. Antimicrobial resistance in Neisseria gonorrhoeae in the 21st century: past, evolution, and future. Clin Microbiol Rev. 2014;27(3):587–613. doi:10.1128/CMR.00010-14
21. Buder S, Dudareva S, Jansen K, et al. Antimicrobial resistance of Neisseria gonorrhoeae in Germany: low levels of cephalosporin resistance, but high azithromycin resistance. BMC Infect Dis. 2018;18(1):44. doi:10.1186/s12879-018-2944-9
22. Yin YP, Han Y, Dai XQ, et al. Susceptibility of Neisseria gonorrhoeae to azithromycin and ceftriaxone in China: a retrospective study of national surveillance data from 2013 to 2016. PLoS Med. 2018;15(2):e1002499. doi:10.1371/journal.pmed.1002499
23. Xu WQ, Zheng XL, Liu JW, et al. Antimicrobial susceptibility of ertapenem in Neisseria gonorrhoeae isolates collected within the China Gonococcal Resistance Surveillance Programme (China-GRSP) 2018. Infect Drug Resist. 2021;14:4183–4189. doi:10.2147/IDR.S335252
24. Wind CM, de Vries HJ, van Dam AP. Determination of in vitro synergy for dual antimicrobial therapy against resistant Neisseria gonorrhoeae using Etest and agar dilution. Int J Antimicrob Agents. 2015;45(3):305–308. doi:10.1016/j.ijantimicag.2014.10.020
25. Zhou Q, Liu J, Chen S, Xu W, Han Y, Yin Y. The accuracy of molecular detection targeting the mutation C2611T for detecting moderate-level azithromycin resistance in Neisseria gonorrhoeae: a systematic review and meta-analysis. Antibiotics (Basel, Switzerland). 2021;10(9):1027.
26. Wang F, Liu J, Liu H, et al. Evaluation of the accuracy of molecular assays targeting the mutation A2059G for detecting high-level azithromycin resistance in Neisseria gonorrhoeae: a systematic review and meta-analysis. Infect Drug Resist. 2019;12:95–104. doi:10.2147/IDR.S183754
27. Lagacé-Wiens PRS, Adam HJ, Laing NM, et al. Antimicrobial susceptibility of clinical isolates of Neisseria gonorrhoeae to alternative antimicrobials with therapeutic potential. J Antimicrob Chemother. 2017;72(8):2273–2277. doi:10.1093/jac/dkx147
28. Terreni M, Taccani M, Pregnolato M. New antibiotics for multidrug-resistant bacterial strains: latest research developments and future perspectives. Molecules (Basel, Switzerland). 2021;26(9):2671. doi:10.3390/molecules26092671
29. Eljaaly K, Ortwine JK, Shaikhomer M, Almangour TA, Bassetti M. Efficacy and safety of eravacycline: a meta-analysis. J Glob Antimicrob Resist. 2021;24:424–428. doi:10.1016/j.jgar.2021.02.009
30. Xiao M, Huang JJ, Zhang G, et al. Antimicrobial activity of omadacycline in vitro against bacteria isolated from 2014 to 2017 in China, a multi-center study. BMC Microbiol. 2020;20(1):350. doi:10.1186/s12866-020-02019-8
31. Zhanel GG, Esquivel J, Zelenitsky S, et al. Omadacycline: a novel oral and intravenous aminomethylcycline antibiotic agent. Drugs. 2020;80(3):285–313. doi:10.1007/s40265-020-01257-4
32. Rodvold KA, Burgos RM, Tan X, Pai MP. Omadacycline: a review of the clinical pharmacokinetics and pharmacodynamics. Clin Pharmacokinet. 2020;59(4):409–425. doi:10.1007/s40262-019-00843-4
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.