")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 15
Evaluation of Medication Adherence and Rescue Medication Use in Non-Exacerbating Patients with COPD Receiving Umeclidinium/Vilanterol or Budesonide/Formoterol as Initial Maintenance Therapy
Authors Moretz C, Cole AL, Mu G , Wu B, Guisinger A, Liu Y, Hahn B , Baylis L
Received 25 April 2020
Accepted for publication 18 August 2020
Published 16 September 2020 Volume 2020:15 Pages 2207—2215
DOI https://doi.org/10.2147/COPD.S259850
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Russell
Chad Moretz,1 Ashley L Cole,2 George Mu,2 Benjamin Wu,1 Amy Guisinger,1 Yunhao Liu,2 Beth Hahn,1 Lee Baylis3
1US Value Evidence & Outcomes, GlaxoSmithKline, Research Triangle Park, Durham, NC, USA; 2VEO Data, Methods, and Analytics, GlaxoSmithKline, Collegeville, PA, USA; 3US Medical Affairs, GlaxoSmithKline, Research Triangle Park, Durham, NC, USA
Correspondence: Beth Hahn
GlaxoSmithKline, 5 Moore Drive, Research Triangle Park, Durham, NC, USA
Tel +1 919 274 0660
Email [email protected]
Background: Adherence to inhaled maintenance therapy is critical to managing chronic obstructive pulmonary disease (COPD), while increasing rescue medication usage may indicate worsening symptoms. This study evaluated adherence and rescue medication use in patients with COPD without a history of exacerbation who initiated combination therapy with budesonide/formoterol (B/F) or umeclidinium/vilanterol (UMEC/VI).
Methods: Retrospective observational study of commercially insured and Medicare Advantage with Part D enrollees who initiated UMEC/VI or B/F between January 1, 2014 and December 31, 2017 (earliest fill defined as index date). Eligibility criteria included age ≥ 40 years, 12 months continuous enrollment pre- and post-index, ≥ 1 pre-index COPD diagnosis, no pre-index asthma diagnosis, COPD-related exacerbations, or medication fills containing inhaled corticosteroids, long-acting β2-agonists, or long-acting muscarinic antagonists. Inverse probability of treatment weighting (IPTW) was used to balance treatment groups on potential confounders. Medication adherence (primary endpoint) was evaluated by the proportion of days covered (PDC). Rescue medication use (secondary endpoint) was standardized to canister equivalents (1 metered dose inhaler [200 puffs] or ∼ 100 nebulized doses of short-acting β2-agonist- and/or short-acting muscarinic agonist-containing medication).
Results: After IPTW, covariates were balanced between cohorts (UMEC/VI: N=4082; B/F: N=9529). UMEC/VI initiators had a significantly greater mean PDC (UMEC/VI: 0.47 [0.33]; B/F: 0.38 [0.30]; P< 0.001) and significantly higher rates of adherence (PDC≥ 0.80) than B/F initiators (UMEC/VI: n=1004 [25%], B/F: n=1391 [15%]; relative risk: 1.68, 95% CI: 1.57, 1.81; P< 0.001). In the year following initiation, UMEC/VI initiators filled significantly fewer rescue medication canister equivalents than B/F initiators (predicted mean [95% CI]: 1.78 [1.69, 1.88] vs 2.15 [2.08, 2.23]; mean difference [95% CI]: − 0.37 [− 0.50, − 0.24]; P< 0.001), corresponding to 17% less (estimated) rescue medication use (incidence rate ratio [95% CI]: 0.83 [0.78, 0.88]).
Conclusion: Among non-exacerbating patients with COPD initiating dual therapy, UMEC/VI demonstrated improved adherence and reduced rescue medication use compared with B/F.
Keywords: COPD, LAMA/LABA, ICS/LABA, medication adherence, rescue medication use
Plain Language Summary
Why was the study done?
Patients with chronic obstructive pulmonary disease (COPD) are often prescribed an inhaler containing both steroids and bronchodilator medicines called long-acting β2-agonists (LABAs). LABAs open the airways to make breathing easier. Another type of inhaler contains LABAs and medicines called long-acting muscarinic antagonists (LAMAs), which relax the airways in a different way. Inhalers containing LAMA/LABA combinations might be better than inhalers containing steroid/LABA combinations at treating patients with COPD who have not had recent flare-ups.
What did the researchers do and find?
We used information from a commercial and Medicare Advantage database in the USA to compare patients starting treatment for COPD with two different combination inhalers. Patients had been diagnosed with COPD but not asthma and had not had any recent COPD flare-ups. One inhaler contained a steroid called budesonide and a LABA called formoterol, while the other inhaler contained a LAMA called umeclidinium and a LABA called vilanterol. Patients treated with umeclidinium/vilanterol were more likely to take their medication regularly than patients treated with budesonide/formoterol, and also used their rescue inhaler less often.
What do these results mean?
Patients with COPD who take their medication regularly are less likely to experience flare-ups, including costly hospital admissions. If patients use their rescue inhaler less often, it is likely that they have less severe breathlessness and related symptoms. Based on this, our results suggest that patients treated with umeclidinium/vilanterol might have better control of their COPD symptoms than patients treated with budesonide/formoterol.
Introduction
The aims of initial maintenance therapy for chronic obstructive pulmonary disease (COPD) include the preservation of lung function, prevention of exacerbations, and reduction of symptom burden.1 To meet these aims, the 2020 Global Initiative for Chronic Obstructive Lung Disease (GOLD) strategy report recommends initial maintenance treatment with inhaled bronchodilator (long-acting muscarinic antagonists [LAMA] or long-acting β2-agonists [LABA]) monotherapy for most patients with COPD, or LAMA/LABA combination therapy for patients with severe symptoms.1 GOLD strategy recommends inhaled corticosteroids (ICS)/LABA combination therapy should be used only in patients with a recent history of exacerbations, history of asthma, and/or elevated blood eosinophil counts.1 However, a recent study of patients with COPD in the USA found that over half were prescribed an ICS-containing therapy as their first maintenance therapy after diagnosis, and that ICS/LABA was the most common initial maintenance therapy regardless of symptom severity or exacerbation risk.2 This suggests that the GOLD strategy recommendations are not being effectively implemented in clinical practice, which may lead to suboptimal treatment and inadequate control of COPD symptoms.3,4
Real-world studies comparing LAMA/LABA with ICS/LABA combinations could help to provide further evidence on the relative benefits of inhaled bronchodilator therapies as initial maintenance therapy in non-exacerbating patients with COPD. Adherence to inhaled maintenance therapy is critical to the management of COPD symptoms.5–7 Greater rescue medication use is associated with worse lung function, more severe COPD symptoms, impaired health status, and increased risk of exacerbations;8–11 therefore, it may be considered a marker of inadequate treatment or treatment adherence. Medications associated with increased adherence and reduced rescue medication use may, therefore, provide better control of COPD symptoms. However, few studies have directly compared adherence and rescue medication use between patients receiving different inhaled maintenance therapies. This study evaluated adherence and rescue medication use in patients diagnosed with COPD without a recent history of exacerbations or a diagnosis of asthma who initiated maintenance therapy with the once-daily LAMA/LABA combination umeclidinium/vilanterol (UMEC/VI) or the twice-daily ICS/LABA combination budesonide/formoterol (B/F).
Materials and Methods
Study Design
This was a retrospective observational cohort study using fully adjudicated medical and pharmacy claims data from Optum’s de-identified Clinformatics Data Mart Database. Claims data were used to identify commercial and Medicare Advantage with Part D enrollees who initiated treatment with UMEC/VI dry powder inhaler or B/F metered dose inhaler between January 1, 2014 and December 31, 2017 (identification period; Figure 1). For each eligible patient, the index date was defined as the date of their earliest claim for fixed-dose combination therapy with UMEC/VI or B/F. The baseline period was defined as the 365-day period prior to the index date, and the follow-up period was defined as the 365-day period after the index date. Patient characteristics were assessed during the baseline period, and study outcomes were assessed during the follow-up period.
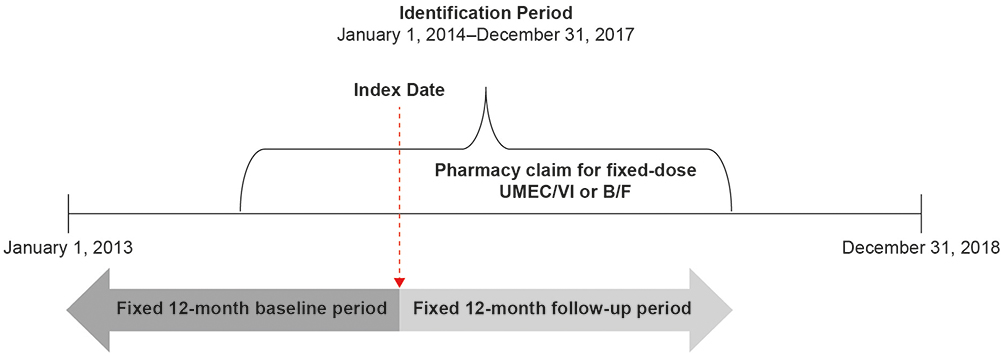 |
Figure 1 Patient identification period and study design. |
This study utilized statistically de-identified retrospective claims data, and as such, did not require institutional review board review and approval or informed consent procedures.
Patients
Eligible patients had ≥1 medical claim with an International Classification of Diseases 9th Edition (ICD-9; prior to October 1, 2015) or 10th Edition (ICD-10; on or after October 1, 2015) diagnosis code for COPD in any position on the index date or during the baseline period. Patients were also required to be ≥40 years of age at the time of index and to have had continuous enrollment in the baseline and follow-up periods.
This observational study was conducted in a non-exacerbating population; patients with any moderate or severe exacerbation on the index date or during the baseline period were excluded. Moderate exacerbations were defined as an emergency room and/or ambulatory visit with a primary diagnosis code indicating a COPD-related exacerbation and a dispensing of antibiotics or systemic corticosteroids within 5 days; severe exacerbations were defined as a hospitalization with a primary diagnosis of COPD. In addition, patients who had any of the following were excluded from the study: any outpatient pharmacy claim for ICS-, LABA-, or LAMA-containing maintenance medications during the baseline period; any outpatient pharmacy claims for a non-index maintenance medication on the index date (including patients with claims for both UMEC/VI and B/F on the index date); or inpatient or outpatient medical claims with an ICD-9 or ICD-10 diagnosis code for asthma in any position on the index date or during the baseline period.
Outcomes
The primary outcome was the proportion of adherent patients, defined as those with a proportion of days covered (PDC) ≥0.80. PDC reflects the proportion of time during the patient’s treatment during which they had medication available, and is calculated as the number of days for which medications were available to the patient (based on days supplied on filled prescriptions) divided by the total number of days between the index date and a pharmacy fill for a different medication or the end of follow-up (whichever is earliest). The PDC calculation was corrected for inpatient hospitalizations under the assumption that medication was supplied by the facility during hospitalizations. Overlapping pharmacy fills for the index medication were corrected for by pushing out the days supplied for the new fill to the end of the previous fill, under the assumption that patients who refilled early waited until their existing supply was exhausted before using the new fill.
The secondary outcome was the number of canister-equivalent rescue medication units filled over the entire follow-up period regardless of treatment switching, where 1 unit was equivalent to 1 metered dose inhaler canister (200 puffs) or 100 doses of nebulized medication. Rescue medications included inhaled and nebulized short-acting β2-agonists (SABA), short-acting muscarinic antagonists (SAMA), and SAMA/SABA combinations.
Statistical Analysis
Inverse probability of treatment weighting (IPTW) was used to control for confounding by balancing pre-index characteristics between study cohorts. In this approach, treatment groups are weighted on the propensity for treatment to produce a pseudo-randomized population, in which treatment groups are balanced on all hypothesized confounders (assuming that there are no confounding differences on unmeasured variables). Propensity for treatment was calculated using a logistic regression model with index treatment as the dependent variable and all hypothesized confounders as independent variables. The weighting for each patient was calculated as the marginal probability of treatment divided by the predicted probability of receiving that treatment given the individual’s specific covariates. The threshold for adequate balance between treatment groups after IPTW was an absolute standard difference <10%. Post-IPTW results are reported for each endpoint.
For the primary endpoint of adherence to the index therapy, the relative risk of achieving adherence (PDC≥0.8) was modeled using weighted log-binomial regression. The secondary endpoint of rescue medication use was modeled using weighted negative binomial regression. The average monthly rate of baseline rescue medication use was calculated for each treatment group and used to estimate the corresponding mean difference in months’ supply of rescue medication between treatment groups in the follow-up period.
Results
Study Population
The final study population included 4082 patients who initiated UMEC/VI and 9530 patients who initiated B/F between January 1, 2014, and December 31, 2017.
Selected demographics and clinical characteristics for each cohort before and after IPTW are shown in Table 1; full demographics and clinical characteristics are shown in Supplementary Table S1. Before IPTW, more patients initiating UMEC/VI had at least one COPD-related outpatient visit during the baseline period than those initiating B/F (56% vs 45%), but the mean number of COPD-related outpatient visits per patient was similar between the cohorts (1.7 vs 1.6). A greater proportion of UMEC/VI initiators had at least one visit with a pulmonologist during the baseline period compared with B/F initiators before IPTW (38% vs 23%).
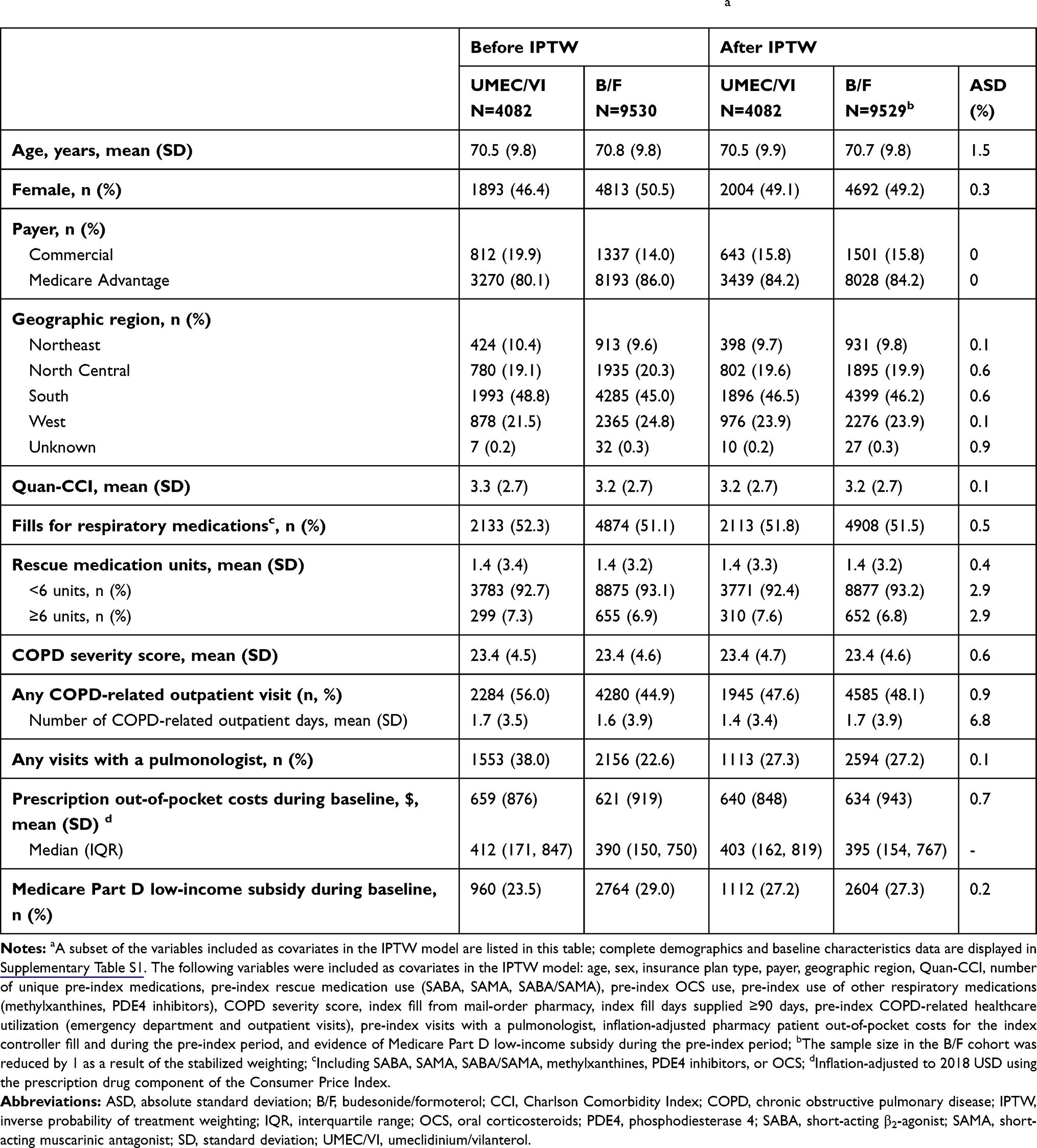 |
Table 1 Selected Patient Demographics and Clinical Characteristics Before and After IPTWa |
Following IPTW, cohorts were balanced on all covariates as indicated by absolute standardized differences <10%, indicating that the treatment groups were similar on measured confounders.
Medication Adherence
The mean (standard deviation [SD]) adherence observation period (from the index date until a fill for a different maintenance medication or the end of the 1-year follow-up period) was similar between groups (UMEC/VI: 334 [83] days; B/F: 328 [93] days). In the 12-month follow-up period, 630 (15.4%) patients receiving UMEC/VI and 1640 (17.2%) patients receiving B/F had a fill for a non-index maintenance medication. The proportion of patients with ≥1 hospitalization in the observation period was similar between treatment cohorts (UMEC/VI: 842 [20.6%]; B/F: 1953 [20.5%]). Mean (SD) PDC was significantly higher in patients initiating UMEC/VI than in patients initiating B/F (UMEC/VI: 0.47 [0.33]; B/F: 0.38 [0.30]; P<0.001; Figure 2A). A greater proportion of UMEC/VI initiators were adherent to their index medication (PDC≥0.80) than B/F initiators (UMEC/VI: n=1004 [25%], B/F: n=1391 [15%]; Figure 2B), and the relative risk (95% confidence interval [CI]) of adherence was significantly greater with UMEC/VI compared with B/F (1.68 [1.57, 1.81]; P<0.001).
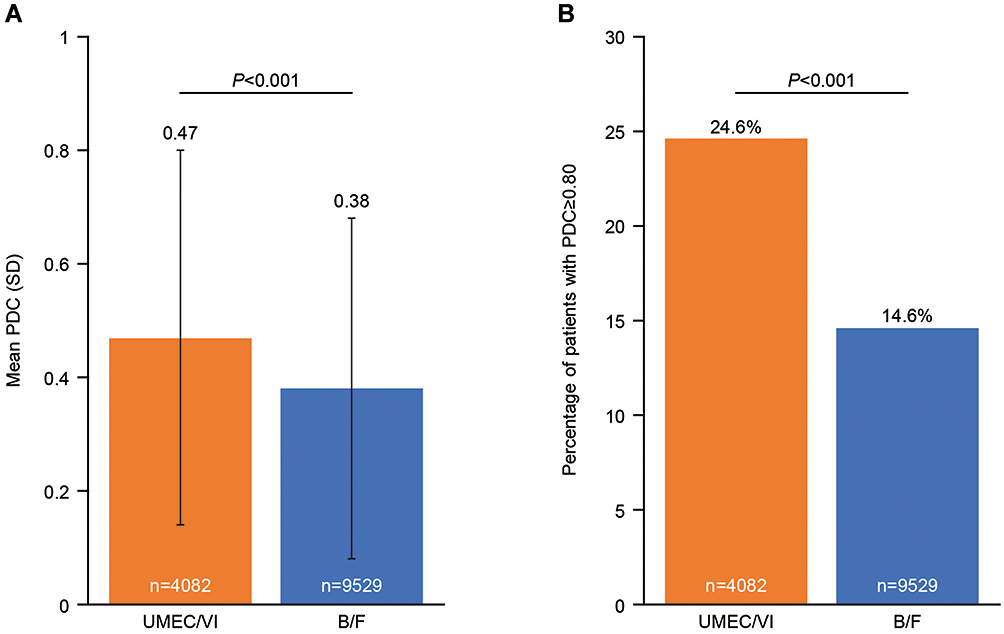 |
Figure 2 (A) Mean PDC in the follow-up period with UMEC/VI versus B/F and (B) Percentage of patients achieving adherence (PDC≥0.80). |
Rescue Medication Use
During the 12-month follow-up period, 2084 (51%) UMEC/VI initiators and 5545 (58%) B/F initiators filled ≥1 prescription for rescue medication (SABA, SAMA, or SAMA/SABA). After IPTW, the mean (SD) number of rescue medication canister equivalents filled by UMEC/VI initiators was 1.78 (1.69, 1.88), which was significantly fewer than the 2.15 (2.08, 2.23) canister equivalents filled by B/F initiators, with a mean (95% CI) difference of −0.37 (−0.50, −0.24) canister equivalents (P<0.001; Figure 3). Patients initiating UMEC/VI filled an estimated 17% fewer rescue medication canister equivalents than patients initiating B/F (incidence rate ratio [95% CI]: 0.83 [0.78, 0.88]).
 |
Figure 3 Mean difference in canister-equivalent units of rescue medication in the follow-up period. aOver the 12-month follow-up period. |
The mean difference of −0.37 units of rescue medication in the follow-up period corresponds to 74 fewer metered dose rescue inhaler puffs per year or approximately 37 fewer doses of nebulized medication per year among patients initiating UMEC/VI compared with those initiating B/F. As rescue medication is not typically taken daily, a more meaningful metric is the corresponding difference in months’ supply. Since each group used an average of 0.12 canister-equivalent units per month during the baseline period, rescue medication use was reduced by approximately 3 months’ supply among patients initiating UMEC/VI compared with B/F (0.37 units/0.12 units per month=3.08 months’ supply).
Discussion
This study compared medication adherence and rescue medication use in patients without a recent history of exacerbations or a diagnosis of asthma, initiating UMEC/VI or B/F. Patients initiating UMEC/VI had significantly higher mean PDC, indicating better adherence, and were significantly more likely to maintain optimal adherence (PDC≥0.80) than patients initiating B/F. In addition, a significantly smaller proportion of patients initiating UMEC/VI filled any rescue medications in the year following treatment initiation, compared with patients initiating B/F. We calculated that the −0.37-unit difference in rescue medication use in this study corresponds to a reduction of approximately 3 months’ supply over the entire follow-up period.
Previous studies have demonstrated poor disease outcomes and increased healthcare costs among patients with low adherence to inhaled maintenance therapies,5–7 while better adherence is associated with a reduced risk of exacerbations, hospitalizations, and death.12,13 Rescue medication use is an important indicator of disease severity and exacerbation risk.8–11,14 In a systematic review including 46 studies reporting rescue medication use and other outcomes in patients with COPD, rescue medication use was negatively correlated with lung function and dyspnea and positively correlated with health status over 6 months.8 A retrospective claims-based study of patients with COPD diagnoses showed a relationship between filled prescriptions for rescue medications and exacerbations over 1 year of follow-up.10 In addition, a prospective 3-month study demonstrated greater dyspnea among patients with COPD who overused their rescue medication,9 and in a post hoc analysis of another study comparing B/F with formoterol, greater rescue medication use at 2 months was associated with a significant increase in exacerbation risk at 10 months in patients with moderate to very severe COPD.11 Our finding that patients initiating UMEC/VI had better adherence and used less rescue medication, therefore, supports the suggestion that UMEC/VI treatment provided better symptom control and may improve outcomes for non-exacerbating patients with COPD compared with B/F. Furthermore, the different dosing frequencies of these two medications may have contributed to the observed difference in adherence, since lower adherence has been previously demonstrated with twice-daily treatments compared with once-daily treatments for COPD.7 To our knowledge, this is the first study to compare UMEC/VI with B/F in a non-exacerbating and non-asthmatic population.
These findings complement those of previous studies comparing UMEC/VI with other inhaled maintenance medications for COPD. A claims-based study demonstrated that patients initiating UMEC/VI had better adherence to their medication than those initiating the ICS/LABA fluticasone propionate/salmeterol.15 In another real-world study, patients treated with LAMA/LABA medications had better self-reported adherence than those receiving ICS/LABA.16 Two meta-analyses also found a statistically significant reduction in rescue medication use with LAMA/LABA, including UMEC/VI, compared with ICS/LABA.17,18 Of these two analyses, one compared a total of 3275 patients receiving LAMA/LABA with a total of 3289 patients receiving ICS/LABA, and reported a mean difference of −0.18 rescue medication inhalations/day favoring LAMA/LABA.17 The other meta-analysis, which did not report an overall difference, found differences in rescue medication use favoring LAMA/LABA compared with ICS/LABA in four studies, although another two studies did not find significant treatment differences.18 In the US, ICS/LABA is frequently prescribed as initial maintenance therapy for patients with COPD regardless of symptom severity or history of exacerbations.2 The frequent use of an ICS/LABA as initial maintenance therapy for patients with COPD contrasts with current GOLD recommendations1 and the accumulating evidence to suggest that LAMA/LABA medications, including UMEC/VI, are associated with better adherence and lower rescue medication use.15,19,20 Furthermore, UMEC/VI has also been shown to be associated with better adherence and reduced rescue medication use compared with tiotropium/olodaterol, another LAMA/LABA medication. A previous real-world study showed lower rescue medication use and improved adherence among patients initiating UMEC/VI compared with those initiating the LAMA/LABA tiotropium/olodaterol.21 In addition, an 8-week randomized open-label trial also reported lower rescue medication use with UMEC/VI versus tiotropium/olodaterol.22 This study, therefore, corroborates the existing evidence supporting a move towards the use of UMEC/VI, rather than ICS/LABA, for the initial treatment of symptomatic patients with COPD without a recent history of exacerbations.
Several limitations should be considered in the interpretation of the findings of this study. Currently, UMEC/VI and B/F are only available in the US via dry powder inhaler and metered dose inhaler, respectively. As a result, it was not possible to determine how far the observed difference in adherence was attributable to the difference in inhaler type. This study was based on claims data collected for the purposes of payment, and as such, it is not possible to verify that all treatments and diagnoses have been coded correctly. Furthermore, the presence of a claim for a filled prescription does not conclusively demonstrate that the medication was taken as prescribed, and diagnosis codes may not always indicate the presence or absence of disease. Of particular relevance to this study, PDC is an imperfect measure of adherence as it measures the average availability of medication over time, and cannot distinguish between more complex patterns of use (such as skipping doses) and discontinuation of therapy. Furthermore, any medication use not captured in the claims data could not be included in the PDC calculation. Finally, while IPTW was used to balance observed differences in pre-index characteristics between study cohorts, this method cannot control for unmeasured confounders.
Conclusions
In a real-world population of patients with COPD without a history of exacerbations, initial maintenance therapy with UMEC/VI led to better adherence and reduced rescue medication use compared with B/F.
Abbreviations
ASD, absolute standardized difference; B/F, budesonide/formoterol; CCI, Charlson Comorbidity Index; CI, confidence interval; COPD, chronic obstructive pulmonary disease; ED, emergency department; EPO, exclusive provider organization; GOLD, Global Initiative for Obstructive Lung Disease; HMO, health maintenance organization; ICD-9, International Classification of Diseases 9th Edition; ICD-10, International Classification of Diseases 10th Edition; ICS, inhaled corticosteroid; IPTW, inverse probability of treatment weighting; IQR, interquartile range; LABA, long-acting β2-agonist; LAMA, long-acting muscarinic antagonist; OCS, oral corticosteroid; PDC, proportion of days covered; PDE-4, phosphodiesterase-4; POS, point of service; PPO, preferred provider organization; SABA, short-acting β2-agonist; SAMA, short-acting muscarinic antagonist; SD, standard deviation; UMEC/VI, umeclidinium/vilanterol; USD, United States Dollars.
Data Sharing Statement
Information on GlaxoSmithKline’s (GSK) data sharing commitments and requesting access to anonymized individual participant data and associated documents from GSK-sponsored studies can be found at www.clinicalstudydatarequest.com. The data reported in this publication are contained in a database owned by Optum and contain proprietary elements. Therefore, it cannot be broadly disclosed or made publicly available at this time. The disclosure of this data to third-party clients assumes certain data security and privacy protocols are in place and that the third-party client has executed Optum’s standard license agreement which includes restrictive covenants governing the use of the data.
Ethical Approval and Informed Consent
This study utilized statistically de-identified retrospective claims data, and as such, did not require institutional review board review and approval or informed consent procedures.
Acknowledgments
Editorial support (in the form of writing assistance during the development of the initial draft, assembling tables and figures, collating authors’ comments, grammatical editing, and referencing) was provided by Mark Condon, DPhil, of Fishawack Indicia Ltd, UK, and funded by GSK.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
CM was an employee of GSK at the time of the study. ALC, GM, AG, and BH are employees of GSK and hold stocks/shares in GSK. YL is an employee of GSK. BW was a GSK Research Fellow at the time of the study. LB was an employee of GSK at the time of the study and holds stocks/shares in GSK. The authors report no other conflicts of interest in this work.
References
1. Global initiative for chronic obstructive lung disease (GOLD). Global Strategy Diagnosis, Management, Prevention Chronic Obstructive Pulmonary Disease. 2020. Available from: https://goldcopd.org/gold-reports/. Accessed August, 2020.
2. Wallace AE, Kaila S, Bayer V, et al. Health care resource utilization and exacerbation rates in patients with COPD stratified by disease severity in a commercially insured population. J Manag Care Spec Pharm. 2019;25(2):205–217. doi:10.18553/jmcp.2019.25.2.205
3. Restrepo RD, Alvarez MT, Wittnebel LD, et al. Medication adherence issues in patients treated for COPD. Int J COPD. 2008;3(3):371–384. doi:10.2147/COPD.S3036
4. Mannino DM, Yu T-C, Zhou H, Higuchi K. Effects of GOLD-adherent prescribing on COPD symptom burden, exacerbations, and health care utilization in a real-world setting. COPD. 2015;2(3):223–235. doi:10.15326/jcopdf.2.3.2014.0151
5. Davis JR, Wu B, Kern DM, et al. Impact of nonadherence to inhaled corticosteroid/LABA therapy on COPD exacerbation rates and healthcare costs in a commercially insured US population. Am Drug Health Benefits. 2017;10(2):91–102.
6. Makela MJ, Backer V, Hedegaard M, Larsson K. Adherence to inhaled therapies, health outcomes and costs in patients with asthma and COPD. Respir Med. 2013;107(10):1481–1490. doi:10.1016/j.rmed.2013.04.005
7. Toy EL, Beaulieu NU, McHale JM, et al. Treatment of COPD: relationships between daily dosing frequency, adherence, resource use, and costs. Respir Med. 2011;105(3):435–441. doi:10.1016/j.rmed.2010.09.006
8. Punekar YS, Sharma S, Pahwa A, Takyar J, Naya I, Jones PW. Rescue medication use as a patient-reported outcome in COPD: a systematic review and regression analysis. Respir Res. 2017;18(1):86. doi:10.1186/s12931-017-0566-1
9. Fan VS, Gylys-Colwell I, Locke E, et al. Overuse of short-acting beta-agonist bronchodilators in COPD during periods of clinical stability. Respir Med. 2016;116:100–106. doi:10.1016/j.rmed.2016.05.011
10. Stanford RH, Nag A, Mapel DW, et al. Validation of a new risk measure for chronic obstructive pulmonary disease exacerbation using health insurance claims data. Ann Am Thorac Soc. 2016;13(7):1067–1075. doi:10.1513/AnnalsATS.201508-493OC
11. Jenkins CR, Postma DS, Anzueto AR, et al. Reliever salbutamol use as a measure of exacerbation risk in chronic obstructive pulmonary disease. BMC Pulm Med. 2015;15:97. doi:10.1186/s12890-015-0077-0
12. Simoni-Wastila L, Wei YJ, Qian J, et al. Association of chronic obstructive pulmonary disease maintenance medication adherence with all-cause hospitalization and spending in a Medicare population. Am J Geriatr Pharmacother. 2012;10(3):201–210. doi:10.1016/j.amjopharm.2012.04.002
13. Vestbo J, Anderson JA, Calverley PM, et al. Adherence to inhaled therapy, mortality and hospital admission in COPD. Thorax. 2009;64(11):939–943. doi:10.1136/thx.2009.113662
14. Leidy NK, Sexton CC, Jones PW, et al. Measuring respiratory symptoms in clinical trials of COPD: reliability and validity of a daily diary. Thorax. 2014;69(5):443–449. doi:10.1136/thoraxjnl-2013-204428
15. Moretz C, Sharpsten L, Bengtson LG, et al. Real-world effectiveness of umeclidinium/vilanterol versus fluticasone propionate/salmeterol as initial maintenance therapy for chronic obstructive pulmonary disease (COPD): a retrospective cohort study. Int J Chron Obstruct Pulmon Dis. 2019;14:1721–1737. doi:10.2147/COPD.S204649
16. Casas A, Montes de Oca M, Menezes AM, et al. Respiratory medication used in COPD patients from seven Latin American countries: the LASSYC study. Int J Chron Obstruct Pulmon Dis. 2018;13:1545–1556. doi:10.2147/COPD.S154097
17. Rodrigo GJ, Price D, Anzueto A, et al. LABA/LAMA combinations versus LAMA monotherapy or LABA/ICS in COPD: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2017;12:907–922. doi:10.2147/COPD.S130482
18. Rogliani P, Calzetta L, Braido F, et al. LABA/LAMA fixed-dose combinations in patients with COPD: a systematic review. Int J Chron Obstruct Pulmon Dis. 2018;13:3115–3130. doi:10.2147/COPD.S170606
19. Vogelmeier CF, Gaga M, Aalamian-Mattheis M, et al. Efficacy and safety of direct switch to indacaterol/glycopyrronium in patients with moderate COPD: the CRYSTAL open-label randomised trial. Respir Res. 2017;18(1):140. doi:10.1186/s12931-017-0622-x
20. Wedzicha JA, Banerji D, Chapman KR, et al. Indacaterol-Glycopyrronium versus Salmeterol-Fluticasone for COPD. N Engl J Med. 2016;374(23):2222–2234. doi:10.1056/NEJMoa1516385
21. Moretz C, Bengtson LG, Sharpsten L, et al. Evaluation of rescue medication use and medication adherence receiving umeclidinium/vilanterol versus tiotropium bromide/olodaterol. Int J Chron Obstruct Pulmon Dis. 2019;14:2047–2060. doi:10.2147/COPD.S213520
22. Feldman GJ, Sousa AR, Lipson DA, et al. Comparative efficacy of once-daily umeclidinium/vilanterol and tiotropium/olodaterol therapy in symptomatic chronic obstructive pulmonary disease: a randomized study. Adv Ther. 2017;34:2518–2533. doi:10.1007/s12325-017-0626-4
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.