")
Back to Journals » International Journal of General Medicine » Volume 15
Evaluation of Lipid Profile and Inflammatory Marker in Patients with Gastric Helicobacter pylori Infection, Ethiopia
Authors Temesgen GB , Menon M, Gizaw ST , Yimenu BW , Agidew MM
Received 22 October 2021
Accepted for publication 23 December 2021
Published 6 January 2022 Volume 2022:15 Pages 271—278
DOI https://doi.org/10.2147/IJGM.S345649
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Gelagey Baye Temesgen,1 Menakath Menon,2 Solomon Tebeje Gizaw,2 Bayu Wondimneh Yimenu,1 Melaku Mekonen Agidew3
1Department of Biomedical Sciences, Debre Markos University, Debre Markos, Ethiopia; 2Department of Medical Biochemistry School of Medicine, College of Health Sciences Addis Ababa University, Addis Ababa, Ethiopia; 3Department of Medical Biochemistry, School of Medicine, Debre Tabor University, Debre Tabor, Ethiopia
Correspondence: Gelagey Baye Temesgen Tel +251 918479703
Fax +251 587780673
Email [email protected]
Introduction: H. pylori are gram-negative, microaerophilic helical-shaped bacteria with multiple flagella and commonly exist in the stomach. This infection may cause significant mucosal inflammation and damage, leading to ulcers in the stomach. It can also affect organ systems external to the gastrointestinal tract. To assess cardiovascular risk factors and to predict cardiovascular disorders, we are evaluating and comparing lipid profile and inflammatory marker between H. pylori-positive and negative patients.
Objective: To evaluate and compare lipid profile (TC; TG; LDL; HDL) and inflammatory marker (hs-CRP) in dyspeptic patients with and without H. pylori infection.
Methods: Comparative cross-sectional study was conducted from September 2020 to January 2021 at Debre Markos Referral Hospital, Debre Markos Health Center, and Hidassie Health Center, Ethiopia. Each of 50 H. pylori-positive and negative dyspeptic patients were studied. The data were checked for completeness and analyzed by SPSS version 25.0 Software. A p-value < 0.05 was considered statistically significant.
Results: Serum mean high-density lipoprotein (HDL) values were 37.54 ± 7.98 mg/dL and 43.12 ± 7.86 mg/dL (p < 0.05) for H. pylori-positive and negative dyspeptic patients, respectively, and median serum high sensitive C reactive protein (hs-CRP) levels were 6.29 mg/L (1.66– 41.34) and 3.35 mg/L (0.39– 10.01) (p < 0.05) for H. pylori-positive and negative dyspeptic patients, respectively.
Conclusion: H. pylori infection significantly alters serum high-density lipoprotein (HDL) and high sensitive C reactive protein (hs-CRP) levels in dyspeptic patients, as a result, increase the potential risk of cardiovascular diseases.
Keywords: H. pylori, dyspepsia, lipid profile, hs-CRP, inflammation, cardiovascular diseases
Introduction
The Genus Helicobacter has different species but only H. pylori can survive in human beings. Other species of helicobacter can survive in different animals.1
H. pylori are a spiral-shaped, gram-negative, microaerophilic rod with 4–7 flagella. The flagella help in the settlement of the bacterium to the gastric mucosa layer.2
H. pylori produce outer membrane vesicles that contain different virulence factors encompassing cell-bound components, secreted molecules, and antigens that could be injected into a host cell by the type IV secretion system (T4SS) or direct secretion of soluble compounds to the gastric area. Outer membrane vesicles are described as 20–300 nm blebs, which are secreted during the logarithmic phase of Gram-negative bacteria growth. Outer membrane vesicles can be crossing the cellular barrier which is the effective way of H. pylori antigens and virulence factors translocation via the gastric mucosa towards the immune cells. H. pylori outer membrane vesicles contains lipopolysaccharide, Vacuolating cytotoxin gene A (VacA), Cytotoxin associated gene A (CagA), blood group antigen-binding adhesin, sialic acid-binding adhesin, outer inflammatory protein A, H. pylori neutrophil-activating protein, adherence associated lipoprotein, and urease. Those proteins and lipids are involved in the pathogenesis of H. pylori infection.3
The virulence factors of H. pylori can cause gastric inflammation, disruption of the gastric mucosal barrier, and extra gastric effect.4 Chronic inflammations are the critical component of the disease process of H. pylori, which is the initial step starting from superficial gastritis to chronic gastritis, intestinal metaplasia to dysplasia, and until invasive adenocarcinoma.5
The virulence factors of H. Pylori have a greater contribution to the disease process by inducing gastric inflammation and disruption of the gastric mucosal barrier. H. pylori promote gastric inflammation by stimulating interleukin (IL-8) secretion from the gastric cell, inducing neutrophil-endothelial cell interactions, activating platelet-activating factor, injecting the lipopolysaccharide of H. pylori to the gastric mucus coat, and secreting urease enzyme.6
H. pylori also disrupt the gastric mucosal barrier because by expressing phospholipases (A2 and C), mucinase like gene, vacuolating cytotoxin, reactive oxygen species, and induce programmed cell death.4,7
H. pylori infection not only causes a gastric problem but also induces extra gastric diseases. Common extra gastric diseases related to H. Pylori include iron deficiency anemia, Henoch Schönlein Purpura, immune thrombocytopenic purpura, chronic urticaria, hepatocellular carcinoma, laryngeal cancer, insulin resistance, metabolic syndrome, cardiovascular diseases, and asthma.8,9
The potential mechanism of H. pylori infection to induce cardiovascular disorders is related to inflammation and immunity.10 The common mechanisms that H. Pylori infection promoting cardiovascular diseases (CVDs) are:
Endothelial Dysfunction
Infected with H. pylori leads to an increase in inflammatory adhesion molecules such as intracellular adhesion molecule-1 and inflammatory mediator cytokines such as hs-CRP, IL-1, IL-6, and tumor necrosis factor-α (TNF-a). These molecules affect the microvascular vasomotor functions and resulting in vasoconstriction and endothelial dysfunction.11
H. pylori infection causes malabsorption of nutrition such as vitamin B12 and folic acid which leads to an increase in serum homocysteine levels and results in endothelial dysfunction.12
H. pylori infection cause alteration of asymmetric dimethylarginine (ADMA) which plays a crucial role at the beginning of H. pylori-induced endothelial dysfunction. ADMA is a competitive inhibitor of endothelial nitric oxide synthase (NOS) which reduces nitric oxide production from L-arginine by nitric oxide synthase in the endothelium to carry out its fundamental role in the regulation of vascular tone.5
Oxidative Stress
H. pylori infection resulting not only in inflammation but also causes the accumulation of reactive oxygen species (ROS) and oxidative DNA damage in the gastric mucosal layer. Therefore, the accumulation of ROS has been resulting in the initiation of multiple disease processes which have a contribution to the pathogenesis of cardiovascular disorders through the expression of adhesion molecules, stimulation of vascular smooth muscle proliferation and migration, apoptosis in the endothelium, and oxidation of lipids.5
Autoimmunity
The autoimmune responses triggered by cross-reactions between H. pylori antigens, such as cytotoxin-associated gene A (CagA), heat shock proteins (HSPs), and self-antigens, also help the role of H. pylori in the pathogenesis of atherosclerosis.13
Alter Lipid Metabolism
H. pylori infection is also linked with an atherogenic modified lipid profile. These alterations are may be mediated by cytokines, particularly TNF-α, which inhibits lipoprotein lipase and thus results in the mobilization of lipids from tissues as well as increased serum TG and reductions in HDL. An altered lipid profile, including an increased LDL level and decreased HDL level, is one of the most important risk factors for atherosclerotic disease.14
However, there are different kinds of controversial pieces of evidence that show the interrelationship of H. pylori infection and predictive risk factors of cardiovascular disorders such as lipid profile and hs-CRP levels. This research was conducted to assess cardiovascular risk factors and to predict cardiovascular disorders, we are evaluating and comparing lipid profile and inflammatory marker between H. pylori-positive and negative patients that will help for better management of H. pylori-infected patients to reduce further complications and to perform a different kind of preventive and therapeutic measurement by the health professionals and insight to pay attention to laboratory investigation of lipid profile and hs-CRP in H. pylori-infected dyspeptic patients. The term dyspepsia comprises a wide and common clinical entity that presents in one of the three ways: Epigastric pain/burning (epigastric pain syndrome), Postprandial fullness, or Early satiety.12
Materials and Methods
A comparative hospital-based cross-sectional study was conducted at Debre Markos Referral Hospital, Debre Markos Health Center, and Hidassie Health Center from September 2020 to January 2021, Debre Markos, Ethiopia. Each of 50 H. pylori-positive and negative dyspeptic patients were selected during a health check-up in the outpatient department (OPD) health by purposive sampling technique those fulfill inclusion criteria. Sample sizes of 100 participants were used by using a sample size calculation formula for comparing the mean between two independent populations. All dyspeptic patients attending at Debre Markos Referral Hospital, Debre Markos Health Center, and Hidassie Health Center during the data collection period were included in the study but subjects with liver disease, renal dysfunction, obesity, diabetes, cardiovascular disorders, malignancy, rheumatoid arthritis, gouty arthritis, who receive the antihyperlipidemic drug, and patients with a history of H. pylori eradication therapy were excluded from the study. After we obtain informed consent from the study participants, 5 mL of blood was drawn and the blood was allowed to stand for 30 minutes for complete clotting, centrifuged at 3000 rpm for 15 minutes to extract serum, and stored at −70 °C before the day of analysis.
Laboratory Tests
H. Pylori was detected by linear H. Pylori Ag cassette, which is a chromatographic immunoassay for the qualitative detection of H. Pylori antigen in the human fecal specimen (Joaquim Costa 18 2ª planta. 08390 Montgat (Barcelona) SPAIN). Serum HDL, Triglyceride, total cholesterol, and hs-CRP levels were analyzed by Cobas C 501 chemistry analyzer (Roche Diagnostic, USA) but serum levels of LDL-cholesterol were calculated by Friedewald formula. All biochemical analysis was done in the Ethiopian public health institute, Addis Ababa, Ethiopia. The reference range of HDL (40–60 mg/dL), TG (<130 mg/dL), TC (<200 mg/dL), LDL (<130 mg/dL) and hs-CRP (<5 mg/L) in adults.
Data Processing and Analysis
Data analysis was done by SPSS software version 25.0 package. Simple descriptive statistics are used to present the socio-demographic data. While Pearson Chi-square (χ2) tests and Pearson correlation are used to describing the association between variables. Continuous variables with normal distribution are presented as mean ± standard deviation and skewed variables are presented as median (range). Student’s t-tests, ANOVA test, and Mann–Whitney-test were used to compare variables. A p-value of <0.05 at a 95% confidence level is considered to be statistically significant.
Result
Socio-Demographic Data of Dyspeptic Patients
This study was conducted on 100 dyspeptic patients with 50 H. pylori-positive and 50 H. pylori-negative dyspeptic patients. The mean age of H. pylori-positive and negative dyspeptic patients was 43.63 ±13.31 and 35.54 ±12.59 years, respectively. In H. pylori-positive dyspeptic patients, 26 participants were males and 24 participants were females. The age category of this study indicated that in H. pylori-infected patients 4 participants were ages ≤ 20 years,16 participants were ages from 21 to 40 years, and 30 participants were ages from 40 to 60 years. H. pylori status is significantly associated with the age category of dyspeptic patients at p-value < 0.05.
Serum Lipid Profile and hs-CRP Levels in Dyspeptic Patients
Serum HDL and hs-CRP levels were significantly different between H. pylori-positive and negative dyspeptic patients (Table 1).
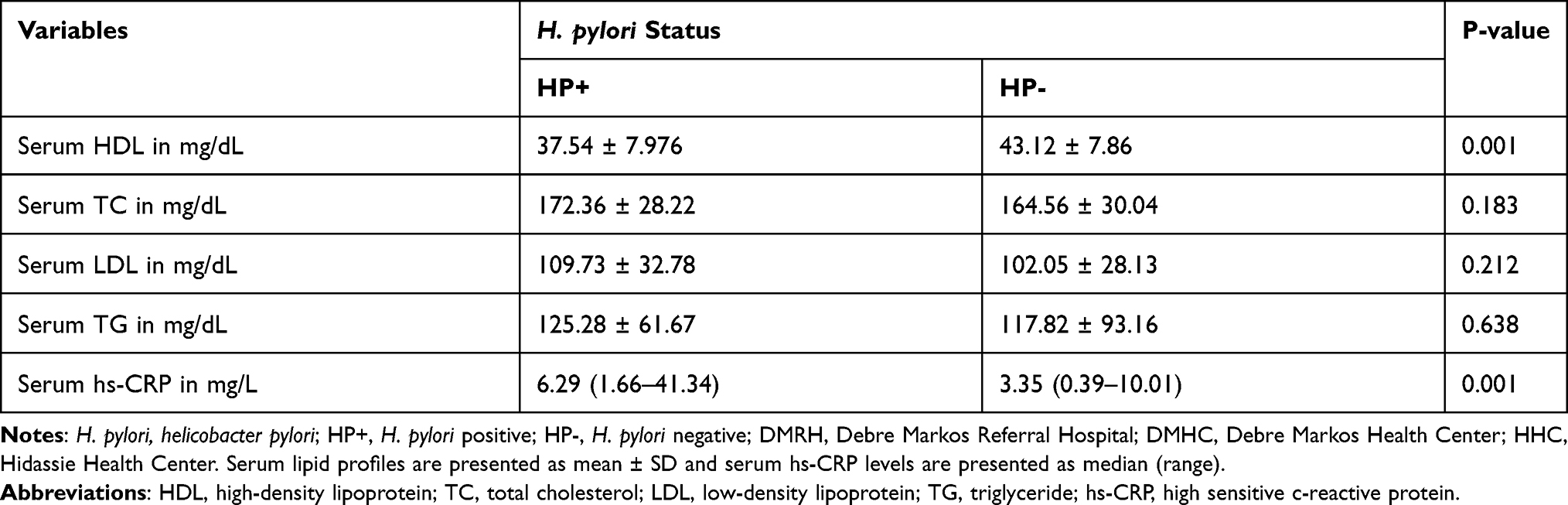 |
Table 1 The Comparison of Serum Lipid Profile and hs-CRP Levels Between H. pylori-Positive and Negative Dyspeptic Patient at DMRH, DMHC, and HHC, Debre Markos, Ethiopia (Each of 50 HP+ and HP- Participants) (N=100) |
Serum Lipid Profile and hs-CRP Levels in Dyspeptic Patients Based on Gender
There is no significant difference between males and females in serum levels of lipid profile and hs-CRP (Table 2). In females, both serum HDL and hs-CRP levels were significantly different between H. pylori-positive and negative dyspeptic patients but, in males, only hs-CRP levels were significantly different between H. pylori-positive and negative dyspeptic patients (Table 3).
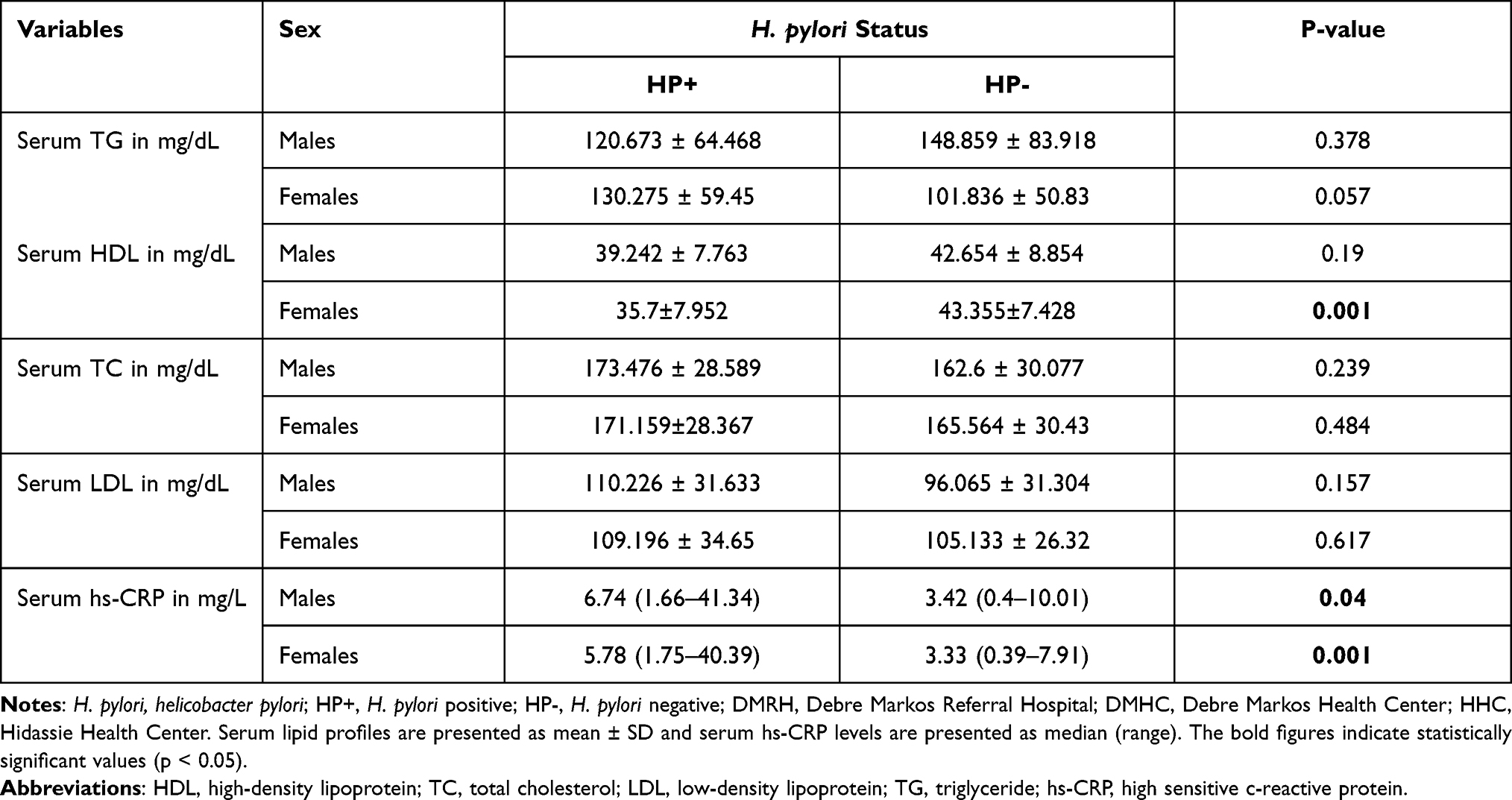 |
Table 2 The Comparison of Serum Lipid Profile and hs-CRP Between H. pylori-Positive and H. pylori-Negative Dyspeptic Patients for the Same Gender at DMRH, DMHC, and HHC, Debre Markos, Ethiopia (N=100) |
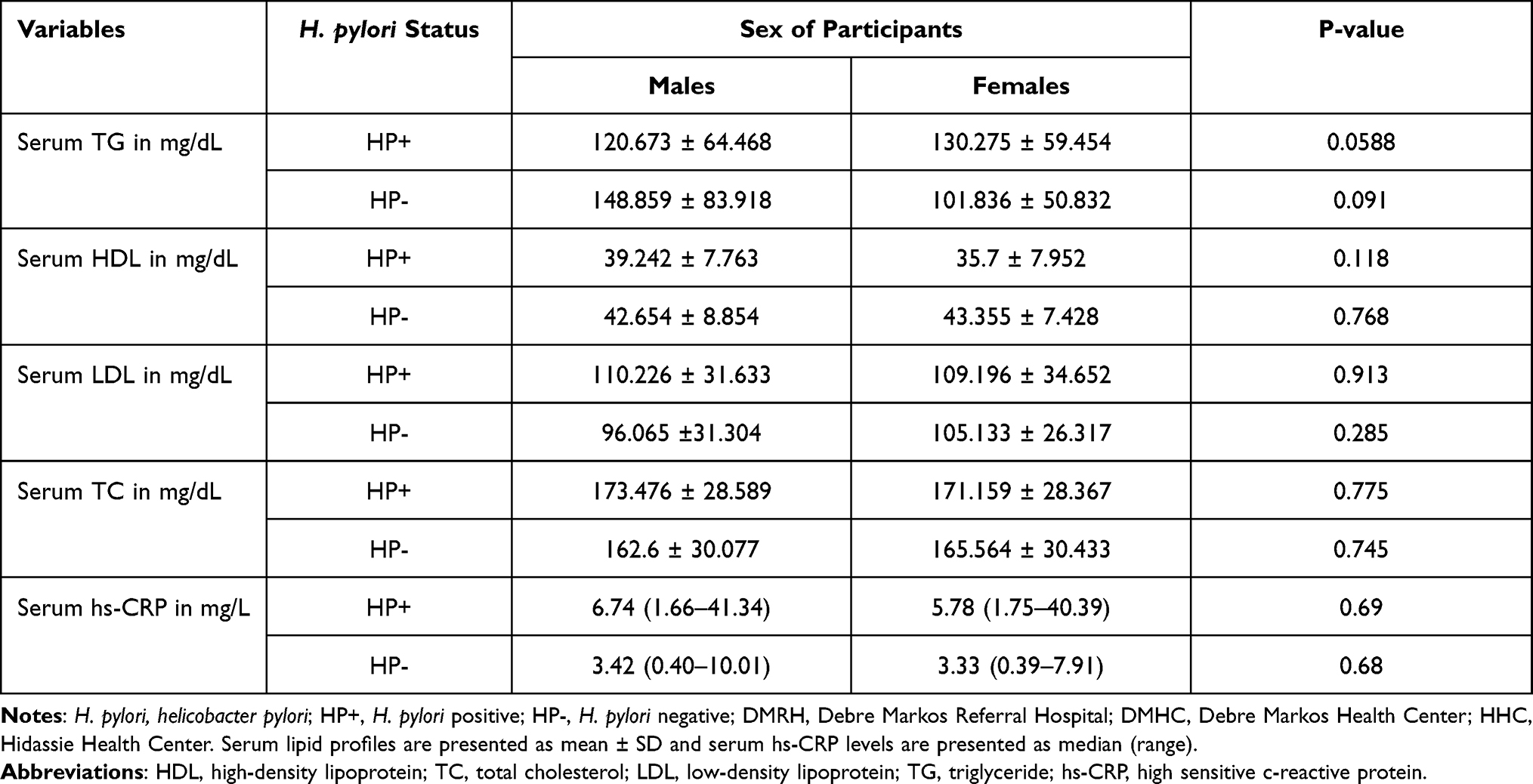 |
Table 3 The Comparison of Serum Lipid Profile and hs-CRP Levels Between Male and Female Dyspeptic Patients at DMRH, DMHC, and HHC, Debre Markos, Ethiopia (N=100) |
Serum Lipid Profile and hs-CRP in Dyspeptic Patients Based on Age Groups
Serum LDL and TC levels were significantly different among different age categories in H. pylori-positive patients (Table 4).
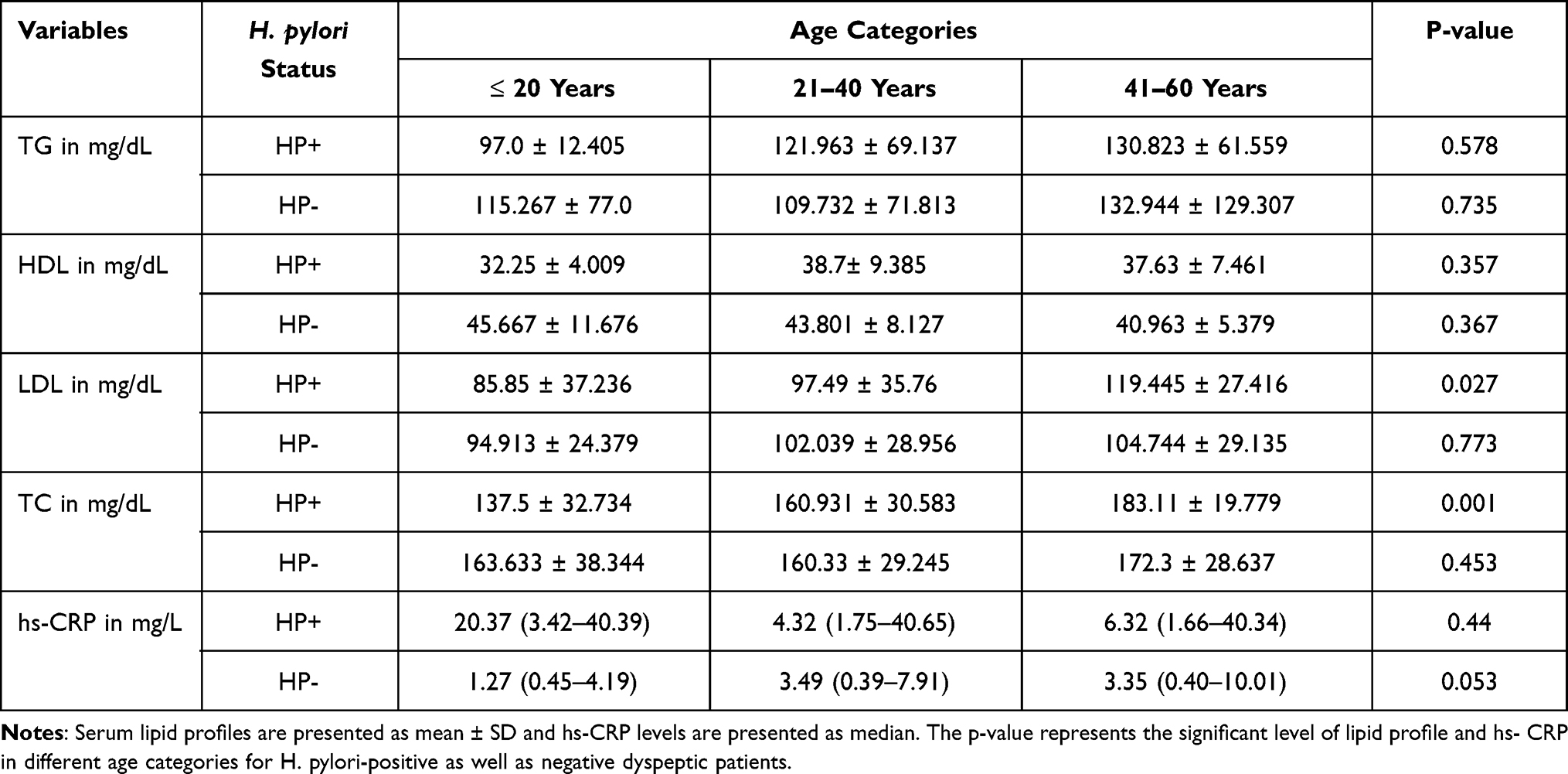 |
Table 4 The Comparison of Serum Lipid Profile and hs-CRP Levels Among Different Age Group in Dyspeptic Patients at DMRH, DMHC, and HHC, Debre Markos, Ethiopia (N=100) |
Discussion
The Role of H. pylori-Infection in Lipid Metabolism
Earlier studies had indicated that H. pylori might be implicated in the alteration of serum lipid profile concentration and increase the potential risk of cardiovascular disorders.15–22 But, some studies have reported that H. pylori infection did not significantly alter lipid profile.23 We have found that the mean serum TG (125.28 ± 61.67 mg/dL), TC (172.36 ± 28.22 mg/dL), and LDL (109.73 ± 32.78 mg/dL) levels were higher among H. pylori-positive dyspeptic patients than the mean serum TG (117.82 ± 93.16 mg/dL), TC (164.56 ± 30.04 mg/dL), and LDL (102.05 ± 28.13 mg/dL) levels of H. pylori-negative patients. But, the difference was not statistically significant. This was in agreement with studies done in Iran and Peru.23,24 But, in contrast with studies done in Jimma and Iraq.14,18 We have found that serum HDL levels of H. pylori-positive dyspeptic patients (37.54 ± 7.98 mg/dL) were significantly lower than negative dyspeptic patients (43.117 ± 7.858 mg/dL). A similar result was reported in studies conducted in Iraq and a meta-analysis was done in Japan.18,25 This significant difference of HDL between H. pylori-infected and non-infected might be due to metabolic and inflammatory effects of H. pylori infection. Inflammation caused by H. pylori infection is bringing significant changes in the protein (apoA-I), and lipid content of HDL, as well as reducing the concentration of HDL.26 Inflammation causes an increase in reactive oxygen species such as Myeloperoxidase and superoxide anion radical, that resulting in the generation of oxidized and modified lipoproteins and reduce the concentration of HDL.27 The metabolic effects of H. pylori infection are mediated by cytokines, predominantly TNF-α, which inhibit lipoprotein lipase and that results in the mobilization of lipids from tissues along with an increase in serum TG and decrease in HDL levels.5
Serum HDL has an atheroprotective function through different mechanisms. The first one is, HDL has an antiatherogenic component called paraoxonase-1, which is an enzyme produced in the liver and has various biochemical functions in the body including protection of oxidation/lipid peroxidation, inducing natural immunity, and detoxification.28 It has also the ability to limit the expression of proinflammatory cytokines and to decrease the expression of leukocyte adhesion molecules when stimulated by inflammatory cytokines. Besides, HDL can induce the production of IL-10 which is an anti-inflammatory and atheroprotective cytokine.26 However, in our study, H. pylori-positive dyspeptic patients’ serum HDL levels were significantly reduced due to the metabolic and inflammatory effect of H. pylori infection as a result, they are potentially at higher risk for atherosclerosis and other cardiovascular diseases.
Except for the levels of HDL, the serum TG, TC, and LDL were found higher in males when compared with females. This was mainly due to the positive effect of estrogen on lipid profile in females and the negative effect of androgen on lipid profile in males.29 In females’, estrogen increases hepatic cell surface LDL receptors and consequently rapid clearance of LDL particles.30 Estrogen suppresses lipase activity in the liver as a result HDL levels increase. It also increases lipoprotein lipase activity, and lipoprotein lipase is responsible for hydrolyzing TG.31 In males’, testosterone increases the degradation of HDL molecule by stimulating the expression of genes encoding for hepatic lipase and scavenger receptor B. On the other hand, testosterone reduced the expression of LDL receptors and the activity of lipoprotein lipase. Therefore, HDL decrease, and LDL, TG and TC levels increased in males.29 But, in our finding, there was no significant difference in lipid levels between males’ and females’ dyspeptic patients, and this might be due to the effect of H. pylori infection, inflammation, and other confounding factors such as alcohol consumption, smoking, and khat chewing on lipid profile.
We have found that serum LDL and TC levels in H. pylori-infected patients were significantly correlated with the age of dyspeptic patients and significantly higher among the age group > 40 years old. This was inconsistent with studies conducted in Iran.17 This significant association might be due to hormonal changes following increasing in age. In females, estrogen levels are decreasing after menopause which is resulting in the reduction of hepatic cell surface LDL receptors and consequently slowing the catabolism of LDL.30 Besides, the reduction of estrogen causes dysregulation of lipoprotein lipase activity and results in to increase in LDL and TC levels.31
The Role of H. pylori-Infection in Inflammation
H. pylori-infection increases gastric and systemic inflammation through different mechanisms such as inducing inflammatory cytokines, inducing neutrophil-endothelial cell interactions, activate platelet-activating factor, by secreting lipopolysaccharide and urease enzyme which is a powerful stimulus of mononuclear phagocyte activation and inflammatory cytokine production.4,6
H. pylori infection also induces an immune-inflammatory reaction through activation of cyclooxygenase enzyme-2 (COX-2), which leads to an increment of production of prostaglandin (PGE2).32
A study conducted in Japan showed that serum hs-CRP levels were significantly higher in H. pylori-positive than those negative dyspeptic patients.13 This was in agreement with the present study with hs-CRP levels for H. pylori-positive (14.148 ± 20.59 mg/dL) and H. pylori-negative (3.51 ± 8.39 mg/dL; p<0.01). This significant increment of hs-CRP levels among H. pylori-positive dyspeptic patients might be due to the inflammatory effect of H. pylori bacterium since the bacterium contain various virulent factors such as CagA and VacA. CagA, a highly virulent factor that is produced by H. pylori bacterium that has a greater role in H. pylori-induced inflammation. H. pylori cause gastric and extra gastric low-grade systemic inflammation. H. pylori infection promotes inflammation by activating nuclear factor Kappa-B (NF-κB) which mediates inflammation through activation of pro-inflammatory cytokines such as IL-6, TNF-alpha, and IL-18. The activated IL-6 stimulates acute phase reactant protein production such as hs-CRP from the liver and is used as an inflammatory marker.9
In a study conducted in Japan, serum hs-CRP levels were significantly higher in females than males H. pylori-positive dyspeptic patients.15 This variation of serum hs-CRP levels between males and females might be probably due to the effects of androgen hormone on inflammatory mediators. Androgen hormone has an immunosuppressive effect and reduces the concentration of inflammatory markers including hs-CRP levels in males. The immunosuppressive effect of androgens could be either a direct effect on the expression of inflammatory genes or an indirect effect via inhibition of nuclear factor-kB activation.33 But, in our study, serum hs-CRP levels were insignificantly different between males and females H. pylori-positive dyspeptic patients. The variation might be due differences in statistical analysis.
In the present study, serum hs-CRP levels were significantly different between H. pylori-positive and negative dyspeptic patients in both sex and this significant difference might be due to the inflammatory effect of H. pylori bacteria both in males and females.9
Conclusion and Recommendation
H. pylori significantly alters serum HDL and hs-CRP levels. However, serum TC, TG, and LDL levels were higher in H. pylori-positive dyspeptic patients than negative dyspeptic patients, but statistically insignificant. The decreased HDL and the increased hs-CRP levels in H. pylori-infected dyspeptic patients are potentially increasing the risk for atherosclerosis, endothelial dysfunction, and other cardiovascular disorders. Lipid profile and inflammatory markers need to be tested in H. pylori-positive chronic dyspeptic patients to prevent and predict future complications.
Ethics Approval and Informed Consent
This study was conducted in accordance with the Declaration of Helsinki. The ethical clearance with reference number (SOM/BCHM/092/2012) was obtained from the Departmental Research and Ethics Review Committee, Department of Biochemistry, College of Health Sciences, Addis Ababa University. We collect data after we obtain written informed consent from each study subject.
Acknowledgments
We would like to thank Addis Ababa University College of Health Sciences, School of Medicine, and Department of Medical Biochemistry for their limitless assistance in the research and delivery of any necessary things. We would also thank Debre Markos University for sponsoring us to participate in this education program. Our heartfelt thanks are also to the staff members of EPHI, for their technical help during the laboratory analysis of serum. It is indeed our privilege to thank Debre Markos Hospital and Health Center staff members who helped us during sample collection at the study site. This paper was uploaded to the Addis Ababa University repository as a thesis in June 2021 (http://213.55.95.56/handle/123456789/27047.34
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Lee A. The microbiology and epidemiology of helicobacter infection. Scand J Gastroenterol. 1994;29(SUPPI201):2–6. doi:10.3109/00365529409105352
2. Lacy BE, Rosemore J. Symposium: emerging role of pathogens in chronic diseases requiring nutritional intervention Helicobacter pylori: ulcers and more: the beginning of an Era 1. J Nutr. 2001;131(5):2789–2793. doi:10.1093/jn/131.10.2789S
3. Chmiela M, Gajewski A, Rudnicka K. Helicobacter pylori vs coronary heart disease. World J Cardiol. 2015;7(4):187–203. doi:10.4330/wjc.v7.i4.187
4. Dunn BE, Cohen H. Helicobacter pylori. Clin Microbiol Rev. 2000;10(4):720–741.
5. He C, Yang Z, Lu N. Helicobacter pylori — an infectious risk factor for atherosclerosis? J Atheroscler Thromb. 2014;21:1–15. doi:10.5551/jat.25775
6. Costa AC, Figueiredo C, Touati E. Pathogenesis of Helicobacter pylori infection. Helicobacter. 2009;14(Suppl. 1):15–20. doi:10.1111/j.1523-5378.2009.00702.x
7. Bohr URM, Annibale B, Franceschi F, Roccarina D, Gasbarrini A. Extragastric manifestations of Helicobacter pylori infection. Helicobacter. 2007;12(Suppl. 1):45–53. doi:10.1111/j.1523-5378.2007.00533.x
8. Testerman TL, Morris J. Beyond the stomach: an updated view of Helicobacter pylori pathogenesis, diagnosis, and treatment. World J Gastroenterol. 2014;20(36):12781–12808. doi:10.3748/wjg.v20.i36.12781
9. Aksoy H, Sebin SO. General medicine: open access. Rev Artic Gen Med. 2015;s1(1):1–6. doi:10.4172/2327-5146.1000S1-007
10. Jamkhande PG, Gattani SG, Farhat SA. Helicobacter pylori and cardiovascular complications: a mechanism based review on role of Helicobacter pylori in cardiovascular diseases. Integr Med Res. 2016;5(4):244–249. doi:10.1016/j.imr.2016.05.005
11. Rasmi Y, Rouhrazi H, Khayati-shal E, Shirpoor A, Saboory E. Cytotoxin-associated A. ScienceDirect Association of endothelial dysfunction and cytotoxin-associated gene A-positive Helicobacter pylori in patients with cardiac syndrome X. Biomed J. 2016;39(5):339–345. doi:10.1016/j.bj.2016.01.010
12. Rasool S, Abid S, Iqbal MP, Mehboobali N, Haider G. Relationship between vitamin B 12, folate and homocysteine levels and H. pylori infection in patients with functional dyspepsia: a cross-section study. BMC Res Notes. 2012;5(206):1–6. doi:10.1186/1756-0500-5-206
13. Ishida Y, Suzuki K, Taki K, et al. Significant association between Helicobacter pylori infection and serum C-reactive protein. Int J Med Sci. 2008;5(4):224–229. doi:10.7150/ijms.5.224
14. Abdu A, Cheneke W, Adem M, Belete R, Getachew A. Dyslipidemia and associated factors among patients suspected to have Helicobacter pylori infection at Jimma University Medical Center. Int J Gen Med. 2020;13:311–321. doi:10.2147/IJGM.S243848
15. Satoh H, Saijo Y, Yoshioka E, Tsutsui H. Helicobacter pylori infection is a significant risk for modified lipid profile in Japanese male subjects. J Atheroscler Thromb. 2010;17(10):1041–1048. doi:10.5551/jat.5157
16. Isiktas Sayilar E, Celik B, Dumlu S. Relationship between Helicobacter pylori infection and metabolic syndrome. Turk J Gastroenterol. 2020;26(6):468–473. doi:10.5152/tjg.2015.0197
17. Haeri M, Parham M, Habibi N, Vafaeimanesh J. Effect of Helicobacter pylori infection on serum lipid profile. J Lipids. 2018;2018:1–6. doi:10.1155/2018/6734809
18. Moutar FT, Alsamarai AM, Ibrahim F. Lipid profile in patients with gastritis. World J Pharm Pharm Sci. 2016;5(7):74–90. doi:10.20959/wjpps20167-6122
19. Hassan M, Ansari K, Omrani M, Sayyah B, Khadem S. Effect of Helicobacter pylori infection on the lipid, lipoproteins, apolipoprotein-A1, lipoprotein (a) and apolipoprotein-B in patients with gastritis. Afr J Microbiol Res. 2010;4(2):084–087.
20. Niemela S, Karttunen T, Korhonen T, Ldara E, Karttunen R. Could Helicobacter pylori infection increase the risk of coronary heart disease by modifying serum lipid concentrations? Heart. 2016;75:573–575. doi:10.1136/hrt.75.6.573
21. Ibrahim HA, Mohammed MO, Dhahir HAR, Mahmood KA, Nuradeen BE. Impact of Helicobacter pylori infection on serum lipid profile and atherosclerosis of carotid artery. Int J Clin Med. 2014;05(15):933–939. doi:10.4236/ijcm.2014.515125
22. Kim HL, Jeon HH, Park IY, Choi JM, Kang JS, Min KW. Helicobacter pylori infection is associated with elevated low density lipoprotein cholesterol levels in elderly Koreans. J Korean Med Sci. 2011;26(5):654–658. doi:10.3346/jkms.2011.26.5.654
23. Guzmán E, Montes P, Monge E. Relation between patients with gastric Helicobacter pylori infection and dyslipidemia. J Gastrointestin Dis Liver Func. 2015;1(1):11–14. doi:10.15436/2471-0601.15.004
24. Aarabi MH. LIPID profile in subjects with helicobacter pylori infection. Iran J Pathol. 2010;5(4):199–203.
25. Shimamoto T, Yamamichi N, Gondo K, et al. The association of Helicobacter pylori infection with serum lipid profiles: an evaluation based on a combination of meta-analysis and a propensity score-based observational approach. PLoS One. 2020;15(6):1–14. doi:10.1371/journal.pone.0234433
26. Fantidis. Inflammation as a Modulator of the HDL Cholesterol- Induced Inteleukin-10 Production by Human Circulating Mononuclear Cells. Vol. 202; 2009. doi:10.1016/j.atherosclerosis.2008.03.015
27. Bonnin A, Nazir S, Van Der Vorst EPC. High-density lipoprotein modifications: a pathological consequence or cause of disease progression? Biomedicines. 2020;8(549):1–20.
28. Ceron JJ, Tecles F, Tvarijonaviciute A. Serum paraoxonase 1 (PON1) measurement: an update. BMC Vet Res. 2014;10(1):1–11. doi:10.1186/1746-6148-10-74
29. Kolovou G, Bilianou H, Marvaki A, Mikhailidis DP. Aging men and lipids. Am J Mens Health. 2011;5(2):152–165. doi:10.1177/1557988310370360
30. Abdrabo AA, Lutfi MF, Sciences M. Effects of age and gender on serum lipid profile in over 55 years-old apparently healthy Sudanese individuals. Asian J Biomed Pharm Sci. 2013;3(19):10–14.
31. Ariadi A, Jamsari J, Yanwirasti Y, Fidel M, Siregar G, Yusrawati Y. Correlation between estrogen levels with lipid profile in menopause women in West Sumatera. Maced J Med Sci. 2019;7(13):2084–2087. doi:10.3889/oamjms.2019.627
32. Zhao J, Wen S, Wang X, Zhang Z. Helicobacter pylori modulates cyclooxygenase-2 and 15-hydroxy prostaglandin dehydrogenase in gastric cancer. Oncol Lett. 2017;14(5):5519–5525. doi:10.3892/ol.2017.6843
33. Tsilidis KK, Rohrmann S, Mcglynn KA, et al. inflammatory biomarkers in US men. Andrology. 2014;1(6):1–21. doi:10.1111/j.2047-2927.2013.00129
34. Baye G. Evaluation of Lipid Profile and Inflammatory Marker in Patients with Gastric Helicobacter Pylori Infection [Dissertation]. Addis Ababa: University of Addis Ababa; 2021. Available from: http://213.55.95.56/handle/123456789/27047.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.