")
Back to Journals » Research and Reports in Urology » Volume 12
Evaluation of Functional Bladder Capacity in Children with Nocturnal Enuresis According to Type and Treatment Outcome
Authors Kang BJ, Chung JM , Lee SD
Received 21 July 2020
Accepted for publication 29 August 2020
Published 15 September 2020 Volume 2020:12 Pages 383—389
DOI https://doi.org/10.2147/RRU.S267417
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jan Colli
Byeong Jin Kang,1,2 Jae Min Chung,1,3,4 Sang Don Lee1,3,4
1Department of Urology, Pusan National University School of Medicine, Yangsan, Korea; 2Department of Urology, Pusan National University Hospital, Busan, Korea; 3Department of Urology, Pusan National University Yangsan Hospital, Yangsan, Korea; 4Research Institute for Convergence of Biomedical Science and Technology, Pusan National University Yangsan Hospital, Yangsan, Korea
Correspondence: Jae Min Chung
Department of Urology, Pusan National University Yangsan Hospital, 20 GeumoRo, Mulgeum-Eup, Yangsan 626-700, Korea
Tel +82-55-360-2678
Fax +82-55-360-2164
Email [email protected]
Purpose: This study aimed to identify whether functional bladder capacity (FBC) differs among subgroups of nocturnal enuresis (NE) patients and can be used to predict treatment response.
Methods: A total of 69 children with NE were included in this study between July 2017 and February 2019 according to medical chart review, retrospectively. All patients completed a questionnaire about voiding symptoms and 48-hour frequency/volume (48-h F/V) charts. FBC was obtained from the 48-h F/V charts and uroflowmetry (UFM) with post-void residual volume (PVR). All patients were primarily treated with standard urotherapy and pharmacological therapy. The response rate was analyzed at 3 months after treatment.
Results: The mean age of the 69 patients (42 male, 27 female) was 83.3 ± 22.4 months (range, 5– 13 years) at the first visit. The percentages of children with monosymptomatic NE (MNE) and non-monosymptomatic NE (NMNE) on the questionnaire were 40.6% (28/69) and 59.4% (41/69), respectively. FBC of all patients was lower than the normal range of expected bladder capacity, and there were no significant differences between measurement methods, NE types (MNE vs NMNE), or response rates (p > 0.05).
Conclusion: Children with NE had diminished FBC in both 48-h F/V charts and UFM with PVR. We found no difference in FBC by NE type or treatment outcome. Therefore, FBC cannot be used to distinguish between NE types or predict treatment responses.
Keywords: nocturnal enuresis, functional bladder capacity, outcome
Introduction
Nocturnal enuresis (NE) refers to intermittent incontinence displayed during sleep. The prevalence of NE is 16.1% and 10.1% at 5 and 7 years of age, respectively, and decreases with age.1,2 The etiology of NE includes nocturnal polyuria (NP), small functional bladder capacity (FBC), an arousal problem, or a mixture of these.1
In NE patients, the evaluation of small FBC is important in the diagnosis and monitoring treatment response. The International Children’s Continence Society (ICCS) recommends the use of 48-hour frequency/volume (48-h F/V) charts for evaluating FBC. Maximal voided volume (MVV), which can be obtained using these charts, is known to represent FBC.3–5 Uroflowmetry (UFM) with ultrasound post-void residual volume (PVR) measurements and radionuclide cystography are alternative methods of assessing FBC.6–8
NE is divided into monosymptomatic NE (MNE) and non-monosymptomatic NE (NMNE). MNE means NE in children without any other lower urinary tract symptoms (LUTS), while NMNE means NE in children with any other LUTS and a history of bladder dysfunction according to the ICCS terminology.8
Of the 3 etiologic factors, the small FBC – not only nighttime but also daytime – is presumed more common in NMNE than MNE. This study aimed to confirm that small daytime FBC in NE is a clue for NMNE and check for differences between NE subgroups (MNE vs NMNE). We also aimed to evaluate whether the response rate can be predicted by small daytime FBC.
Materials and Methods
This study was conducted in accordance with the Declaration of Helsinki and approved by the institutional review board of the Pusan National University Yangsan Hospital (IRB number 05–2019-163). The parent or legal guardian provided informed consent about diagnosis and treatment plan, together with the children’s informed assent. A total of 69 children with NE (more than 3 times per week) were included in the study between July 2017 and February 2019 according to medical chart review, retrospectively. Patients with congenital urinary tract anomaly, congenital or acquired neurologic disorders, urinary tract infection, and spine anomaly were excluded. Spine anomaly include spinal bifida occulta.
All patients completed the questionnaire and 48-h F/V charts. Our questionnaire included items on medical history and urinary symptoms (frequency, urgency, urge incontinence, and dysuria, etc.).
The presence of LUTS was confirmed according to the questionnaire and 48-h F/V chart findings, and the NE patients were classified into MNE and NMNE subgroups.
We also evaluated the UFM with PVR findings. We assessed the UFM pattern (bell, plateau, interrupted, tower, and staccato), average flow rate (Qave), maximum flow rate (Qmax), and voided volume (VV).
The expected bladder capacity (EBC) and daytime FBC were evaluated and compared in each patient. The EBC is estimated using the formula [(age in years + 2) × 30] mL introduced by Koff.9 The FBC was obtained from the 48-h F/V chart and UFM with PVR, comparably. The MVV on the 48-h F/V chart represented FBC in the chart, and the VV in UFM with PVR represented FBC in UFM. Both of the FBC values mentioned above were considered small or large if less than 65% or greater than 150% of the EBC, respectively.10 We verified the difference in the daytime FBC and FBC/EBC ratio between the MNE and NMNE subgroups.
After conducting pre-treatment evaluations (characteristics, 48-h F/V chart, UFM with PVR, etc.) of NE patients, treatments with standard urotherapy and pharmacological therapy were provided according to ICCS recommendations.11 Standard urotherapy included an introduction on how to resolve LUTS, lifestyle advice (balanced fluid intake, regular bladder and bowel emptying, optimal posture during voiding, restriction of night fluid intake). Primary pharmacological therapy included desmopressin, propiverine, and imipramine. These drugs were used according to symptoms and used the same way, with or without any other LUTS and a history of bladder dysfunction. Especially imipramine was used for a short period of time in patients with insignificant symptom improvement despite initial therapy for more than 3 months. The treatment was performed until complete remission was achieved.
The response rates were analyzed after 3 months of treatment. The NE patients were divided into complete response (CR), partial response (PR), and no response (NR) groups based on the response rates.12 CR was defined as a reduction greater than 99% in wet nights, PR was defined as a reduction of 50–99% in the number of wet nights, while NR was defined as a reduction less than 50% in wet nights. We verified the difference in the daytime FBC and FBC/EBC ratio before treatment in each group.
SPSS version 20 (SPSS, Chicago, IL, USA) was used for statistical analyses. P values <0.05 were considered statistically significant. The Mann–Whitney U-test and Kruskal–Wallis test were used to compare FBC between the NE subgroups (MNE vs NMNE) and among the CR, PR, and NR groups.
Results
The mean age of the 69 patients (42 male, 27 female) at the first visit was 83.3 ± 22.4 months (range, 5–13 years). The mean EBC was 268.2 ± 56.1 mL, while the mean FBC was 152.6 ± 74.6 mL an1d 141.3 ± 64.2 mL in the 48-h F/V chart and UFM with PVR, respectively. The values were not significantly different between the two measurement methods (p > 0.05). The mean FBC/EBC ratios did not differ significantly between the two measurement methods (55.6% vs 52.6%; p > 0.05). The mean FBC/EBC ratios were lower than the lower limit of the normal range (65–150%). Of the total 69 patients, a lower FBC/EBC ratio was found in 47 patients on the 48-h F/V chart and 48 patients on UFM with PVR, respectively. On UFM with PVR, the UFM pattern was most commonly a bell shape (46.4%), the mean VV was 127.3 ± 60.9 mL, and the mean PVR was 14.0 ± 12.5 mL (Tables 1 and 2).
 |
Table 1 Patients’ Characteristics According to NE Types |
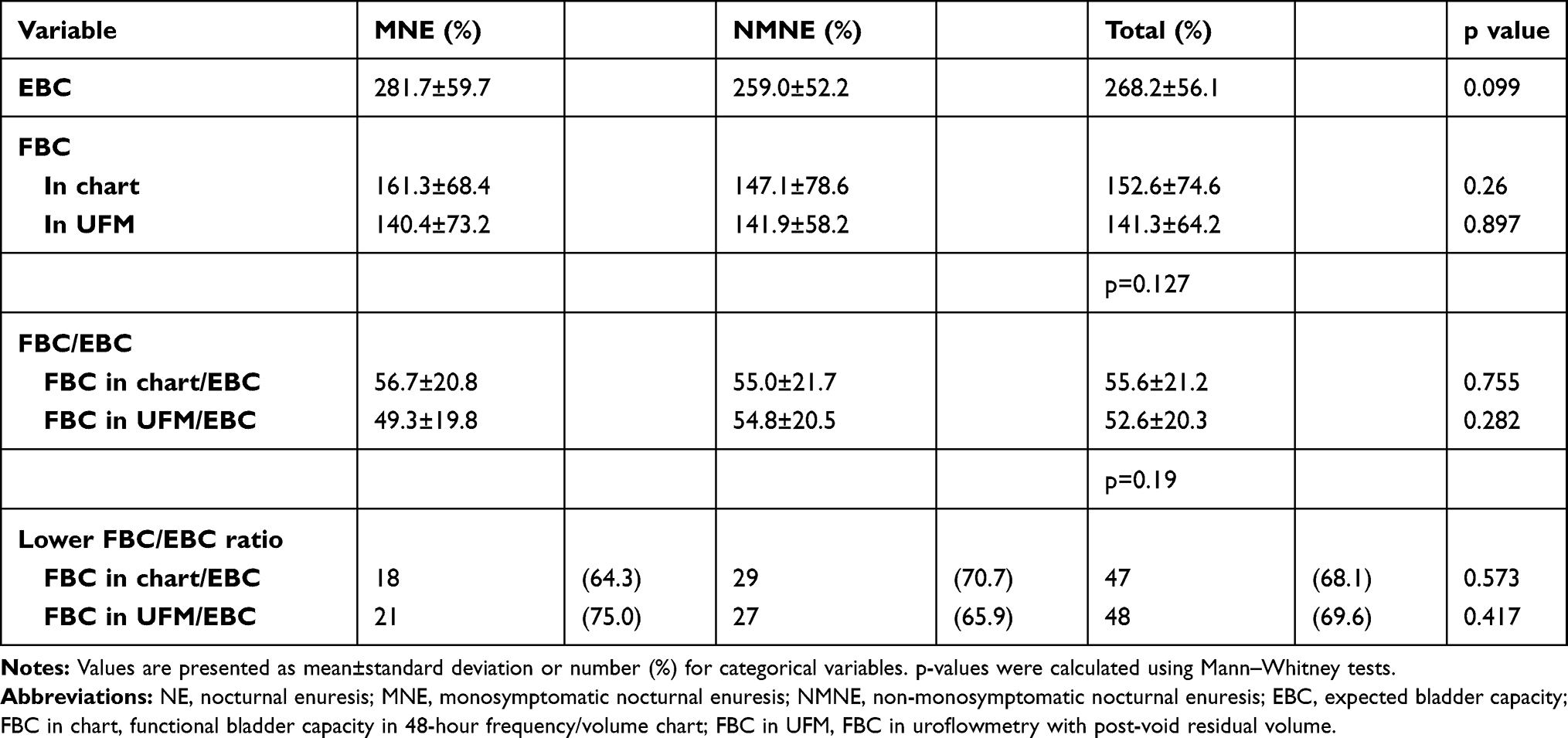 |
Table 2 Functional Bladder Capacity of Patients According to NE Types |
NE Subtypes
The percentages of children with MNE and NMNE according to the questionnaire were 40.6% (28/69) and 59.4% (41/69), respectively. There was no difference between MNE and NMNE in the pattern of UFM, Qmax, Qave, or PVR (p > 0.05). The mean age, height and weight were similar between NE subgroups. After 3 months of treatment, CR and PR were more common in patients with MNE than in those with NMNE. However, there was no statistically significant difference (67.9% vs 63.4%, p > 0.05) (Table 1).
The mean daytime FBC of MNE and NMNE obtained from the 48-h F/V charts were similar (161.3 ± 68.4 mL and 147.1 ± 78.6 mL, respectively; p = 0.26). The mean FBC values obtained from UFM with PVR of MNE and NMNE were also similar (140.4 ± 73.2 mL and 141.9 ± 58.2 mL, respectively; p = 0.90). In both MNE and NMNE, the FBC/EBC ratios were equally lower than the normal range and no significant difference was seen between measurement methods or the NE subgroups (MNE vs NMNE). The numbers of patients with lower FBC/EBC ratios were also similar between the NE subgroups (Table 2).
Treatment Responses
The percentages of children with CR, PR, and NR at 3 months were 21.7% (15/69), 43.5% (30/69), and 34.8% (24/69), respectively. A larger FBC and FBC/EBC ratio tended to indicate a better treatment response. However, there was no significant difference among the 3 subgroups (p > 0.05) (Table 3). The same was observed in a one-on-one group comparison (CR vs NR, CR vs PR, and PR vs NR; p > 0.05) (Figure 1). The percentages of patients with lower FBC/EBC ratios were similar among the CR, PR, and NR subgroups (p > 0.05). There was no significant adverse effect like a headache, dry mouth, aggravation of constipation, mood change, and cardiac function due to pharmacological therapy.
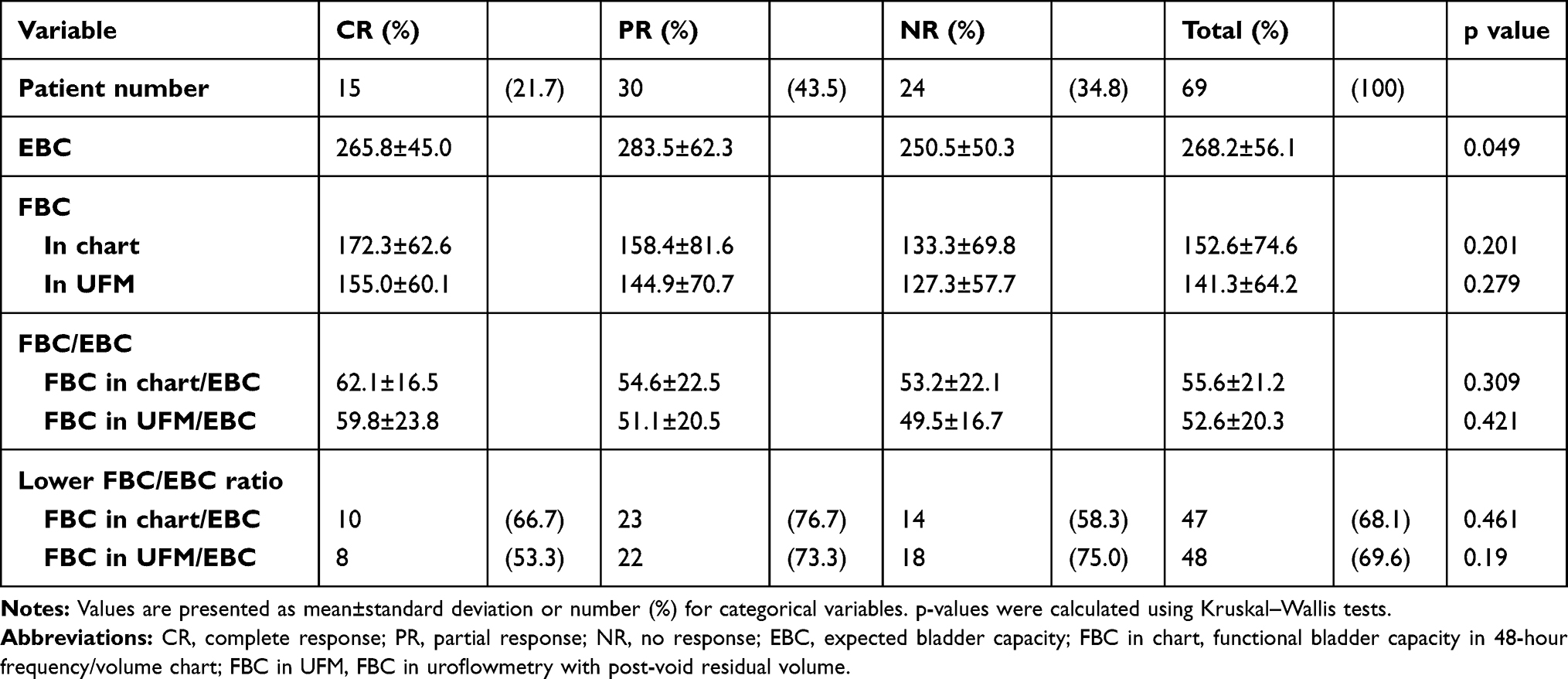 |
Table 3 Bladder capacity According to Treatment Response |
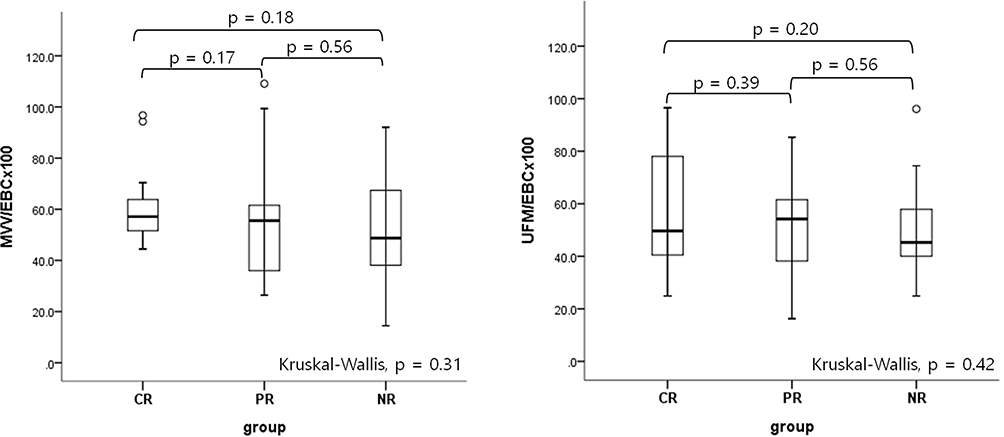 |
Figure 1 Functional bladder capacity according to treatment outcome. |
Discussion
In children with NE, the evaluation of FBC can provide an important information about NP and bladder capacity.13 ICCS recommends the use of 48-h F/V charts for this assessment. During this test, the volume and timing of all voids and fluid intake must be recorded. The MVV excluding the first morning void is considered the FBC on the 48-h F/V chart. This method is non-invasive and represents the FBC of the everyday environment, but it must be performed for at least 48 hours to obtain objective MVV results. This is rather time-consuming for both parents and children, and it is difficult to obtain reliable results, especially in less motivated families. In addition, the chart evaluation does not recognize PVR; thus, this method may underestimate FBC.6
Alternatively, FBC can be estimated using the UFM with PVR measurement. FBC is recorded from UFM as the sum of VV and its corresponding PVR.6,12 The disadvantage of this FBC measurement method in all children presenting with LUTS is its higher cost and unnatural situation. FBC can also be measured using cystography as the volume of contrast media infused to the point at which the child is able to void.7,8 This method is accurate and reliable, however, it is most invasive and costly. In addition, the last method features urinary tract infection as a complication.14
Here, we measured FBC using the 48-h F/V chart and UFM with PVR. There was no significant difference in the FBC values obtained from the two measurement methods. Maternik et al also reported no significant difference between the MVV obtained from the 48-h F/V chart and the FBC obtained from UFM with PVR in patients with several LUTS (MNE, overactive bladder, and dysfunctional voiding).6 Therefore, both methods are reliable for measuring FBC; thus, when one method cannot be used, the other method can be used instead.
According to ICCS, the MVV, which represents FBC, is considered small or large if less than 65% or greater than 150% of the EBC value, respectively.10 Several studies have shown that FBC is reduced by up to 50% in children with NE.15 According to Kim, 46.5% of all patients had reduced FBC for age, and this was similar to other studies (30–50%).16 However, Acosta et al reported that 85% of patients with NE showed an MVV value less than 70% of the EBC value.15 This is probably because the lower limit of the normal range is set at 70%. In the present study, 68–70% (according to the measurement methods, MVV vs UFM) of total patients had a small FBC for age, regardless of the NE subgroup. Our hospital is a tertiary institution to which severely affected patients who had failed treatment have been referred from other institutions. Indications for referral were described by Shinha et al.17 These include refractory MNE, NMNE, and developmental, psychosocial, or suspected neurologic problems. This tendency can explain why the small FBC rate is higher than those reported by other studies. It is also presumed to be related to the large proportion of NMNE patients versus those of other reports (59.4% vs 15–30%, respectively).18
Recent studies have proposed several candidate biomarkers for distinguishing between MNE and NMNE.19 Because many patients with LUTS show a small FBC, patients with NMNE also could show a small FBC. Therefore, we thought that a small FBC can be biomarkers for distinguishing between MNE and NMNE. However, based on this and other studies, we confirmed that a significantly high proportion of NE patients have a small FBC for age with or without other LUTS. Therefore, it is difficult to distinguish between MNE and NMNE using only a small FBC.
Previous studies investigating the predictive factors of treatment response mainly focused on lower FBC, NP, and arousal problems.1 Several studies revealed the relationship between reduced FBC, NE severity, and treatment resistance. Kim reported a significant correlation between NE severity and FBC reduction degree.16 Yeung et al reported that the significantly small FBC patient group relapsed with a decrease in desmopressin response.20 Thus, practical consensus guidelines for the management of NE suggest that a reduced FBC for age is associated with a lower response rate to desmopressin.1
However, some studies reported that a small FBC was not associated with treatment response. Chang et al found no significant association between a reduced FBC and response to medical treatment. Instead, they confirmed that elevated PVR and NP were significant predictors for medical treatment.1 Beksac et al also revealed that PVR could predict treatment prognosis.12
In this study, the response rate increased with FBC and FBC/EBC ratio, but there was no significant difference among CR, PR, and NR. The NE patients included in this study were often referred from primary care clinics and usually had various mixtures of etiological factors. Thus, despite the absence of a significant difference in FBC and FBC/EBC ratio, the response rates may have differed among other etiologies.
It is generally known that a delayed maturation of normal bladder development can cause NE with a small FBC. This delayed bladder maturation can be accompanied by other developmental delays. There are reports that some children with NE may have low height and young bone age. There is a higher incidence of NE in children with delayed motor and language development as well.17 Thus, it can be inferred that bladder and other maturations may be delayed together during the development process. Therefore, we confirmed in this study that it is difficult to predict the treatment response rate by measuring the FBC and FBC/EBC ratio.
There are several limitations to this study. First, it was retrospective and could have involved a selection bias. Second, the number of patients was small and it may be not enough to determine the bladder capacity through a 48-hour frequency volume chart and one uroflowmetry. Third, there was a lack of normal data representative of a normal FBC. So, we could not compare the NE patients with a normal control group. Fourth, patients with severe symptoms visited our tertiary institution; thus, patients with mild symptoms were not included. Fifth, a UFM with PVR evaluation was performed only once. It has been recognized that UFM requires repetition to improve its accuracy, reliability, and correct interpretation.6,13 Finally, we did not confirm whether FBC increased after treatment.
In a recent study, the written checklist method increased the success rate of the extended urtherapy up to 60%, while the success rates of urotherapy ranges between 18% and 22% in previous studies.21–23 The compliance and response rates of NE treatment are closely related.
NE is a complex disease that stems from many etiological factors. FBC is calculated to confirm the NE characteristics and determine the treatment method. The 48-h F/V chart and UFM with PVR are reliable methods for measuring FBC. Children with NE in this study, particularly those with severe NE, had small FBC on the 48-h F/V charts and UFM with PVR, regardless of the measurement method or NE subgroup. Thus, a small FBC is not a good parameter for distinguishing between MNE and NMNE and common sign of NE. Other biomarkers should be further evaluated to subdivide the NE groups. A small FBC is associated with delayed bladder maturation but could not predict NE treatment outcomes. Further larger studies are needed to verify the mechanism and effect of FBC.
Conclusions
The most children with NE in this study had small daytime FBC on the 48-h F/V charts and UFM with PVR, regardless of the measurement method. The mean daytime FBC values and the FBC/EBC ratios of MNE and NMNE were also similar. Thus, a small daytime FBC could not distinguish between MNE and NMNE. Moreover, a small daytime FBC could not predict treatment outcomes of NE. However, further larger studies are needed to verify the mechanism and effect of FBC.
Disclosure
The authors report no potential conflicts of interest to this work.
References
1. Chang SJ, Yang SSD. Are uroflowmetry and post-void residual urine tests necessary in children with primary nocturnal enuresis? Int Braz J Urol. 2018;44(4):805–811. doi:10.1590/s1677-5538.ibju.2017.0464
2. Kim SO, Kim KD, Kim YS, et al. Evaluation of maximum voided volume in Korean children by use of a 48‐h frequency volume chart. BJU Int. 2012;110(4):597–600. doi:10.1111/j.1464-410X.2011.10799.x
3. Austin PF, Bauer SB, Bower W, et al. The standardization of terminology of lower urinary tract function in children and adolescents: update report from the standardization committee of the International Children’s Continence Society. J Urol. 2014;191(6):1863–1865. doi:10.1016/j.juro.2014.01.110
4. Van Batavia JP, Combs AJ, Fast AM, Glassberg KI. Use of noninvasive uroflowmetry with simultaneous electromyography to monitor patient response to treatment for lower urinary tract conditions. J Pediatr Urol. 2014;10(3):532–537. doi:10.1016/j.jpurol.2013.11.015
5. Chung JM, Lee SD, Kang DI, et al. An epidemiologic study of voiding and bowel habits in Korean children: a nationwide multicenter study. Urology. 2010;76(1):215–219. doi:10.1016/j.urology.2009.12.022
6. Maternik M, Chudzik I, Krzeminska K, Żurowska A. Evaluation of bladder capacity in children with lower urinary tract symptoms: comparison of 48-hour frequency/volume charts and uroflowmetry measurements. J Pediatr Urol. 2016;12(4):
7. Kaefer M, Zurakowski D, Bauer SB, et al. Estimating normal bladder capacity in children. J Urol. 1997;158(6):2261–2264. doi:10.1016/S0022-5347(01)68230-2
8. Kogan BA, Giramonti K, Feustel PJ, Lin WY. Bladder volume on voiding cystourethrogram correlates with indications and results in male infants. Urology. 2011;77(2):458–462. doi:10.1016/j.urology.2010.07.463
9. Koff SA. Estimating bladder capacity in children. Urology. 1983;21(3):248. doi:10.1016/0090-4295(83)90079-1
10. Nevéus T, von Gontard A, Hoebeke P, et al. The standardization of terminology of lower urinary tract function in children and adolescents: report from the standardisation committee of the International Children’s Continence Society. J Urol. 2006;176(1):314–324. doi:10.1016/S0022-5347(06)00305-3
11. Neveus T, Eggert P, Evans J, et al. Evaluation of and treatment for monosymptomatic enuresis: a standardization document from the International Children’s Continence Society. J Urol. 2010;183(2):441–447. doi:10.1016/j.juro.2009.10.043
12. Beksac AT, Koni A, Bozacı AC, Dogan HS, Tekgul S. Postvoidal residual urine is the most significant non-invasive diagnostic test to predict the treatment outcome in children with non-neurogenic lower urinary tract dysfunction. J Pediatr Urol. 2016;12(4):
13. Hofmeester I, Brinker AE, Steffens MG, van Capelle JW, Feitz WF, Blanker MH. Reference values for frequency volume chart and uroflowmetry parameters in adolescent and adult enuresis patients. Neurourol Urodyn. 2017;36(2):463–468. doi:10.1002/nau.22955
14. Sinha R, Saha S, Maji B, Tse Y. Antibiotics for performing voiding cystourethrogram: a randomised control trial. Arch Dis Child. 2018;103(3):230–234. doi:10.1136/archdischild-2017-313266
15. Acosta J, Lopez E, Olvera GI, Ortega R. Functional bladder capacity by ultrasound in patients with monosymptomatic primary enuresis. Rev Chil Pediatr. 2017;88(5):608–613. doi:10.4067/S0370-41062017000500006
16. Kim JM. Diagnostic value of functional bladder capacity, urine osmolality, and daytime storage symptoms for severity of nocturnal enuresis. Korean J Urol. 2012;53(2):114–119. doi:10.4111/kju.2012.53.2.114
17. Sinha R, Raut S. Management of nocturnal enuresis-myths and facts. World J Nephrol. 2016;5(4):328. doi:10.5527/wjn.v5.i4.328
18. Franc I, Von Gontard A, De Gennaro M, members of the International Childrens’s Continence Society. Evaluation and treatment of nonmonosymptomatic nocturnal enuresis: a standardization document from the International Children’s Continence Society. J Pediatr Urol. 2013;9(2):234–243. doi:10.1016/j.jpurol.2012.10.026
19. Morizawa Y, Aoki K, Iemura Y, et al. Urinary nerve growth factor can predict therapeutic efficacy in children with monosymptomatic nocturnal enuresis. Neurourol Urodyn. 2019;38(8):2311–2317. doi:10.1002/nau.24142
20. Yeung CK, Sit FKY, To LKC, et al. Reduction in nocturnal functional bladder capacity is a common factor in the pathogenesis of refractory nocturnal enuresis. BJU Int. 2002;90(3):302–307. doi:10.1046/j.1464-410X.2002.02884.x
21. Fai-Ngo Ng C, Wong SN, The Hong Kong Childhood Enuresis study Group. Comparing alarms, desmopressin and combined treatment in Chinese enuretic children. Pediatr Nephrol. 2005;20(2):163–169. doi:10.1007/s00467-004-1708-5
22. Kruse S, Hellstrom AL, Hanson E, Hjälmås K, Sillén U, Swedish Enuresis Trial (SWEET) Group. Treatment of primary mono symptomatic nocturnal enuresis with desmopressin: predictive factors. Br J Urol. 2001;88(6):572–576. doi:10.1046/j.1464-410X.2001.02321.x
23. Hascicek AM, Kilinc MF, Yildiz Y, Yuceturk CN, Doluoglu OG. A new checklist method enhances treatment compliance and response of behavioural therapy for primary monosymptomatic nocturnal enuresis: a prospective randomised controlled trial. World J Urol. 2019;37(6):1181–1187. doi:10.1007/s00345-018-2478-1
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.