")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 12
Evaluation of anxiety condition among type 1 and type 2 diabetic patients
Received 2 February 2016
Accepted for publication 26 April 2016
Published 11 October 2016 Volume 2016:12 Pages 2573—2579
DOI https://doi.org/10.2147/NDT.S105588
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Aliye Bulut,1 Aziz Bulut2
1Department of Nursing, Higher School of Health, Bingol University, 2Department of General Surgery, Bingol State Hospital, Bingol, Turkey
Purpose: This study was conducted for the purpose of determining the relationship between type 1 and type 2 diabetic patients and anxiety.
Method: This study was conducted between August and September 2015 at Bingol State Hospital. The study included 131 patients with diabetes mellitus (DM) followed up at the Internal Diseases Polyclinic of Bingol State Hospital. The questionnaire used in the study consisted of two parts. The first part of the questionnaire comprised a set of questions querying the sociodemographic characteristics and the second part comprised the Beck Anxiety Inventory.
Results: The incidence of Type 1 DM was found to be higher among female compared to male patients, whereas type 2 DM was found to be higher among male compared to female patients, and this difference was statistically significant. According to the results of Beck Anxiety Scale (BAS) applied to the patients to examine their psychological states, 94.2% of male and 96.8% of female patients were found to be in the severe anxiety group. Among both male and female patients, BAS scores of the type 2 DM patients were higher than those of type 1 DM patients. When the distribution of BAS scores among the patients was examined, it was found that males received 44.7±13.2 points and females received 47.0±13.0 as mean value, but no statistically significant difference was found between BAS scores by sex. Unlike female patients, the difference between duration of disease and BAS score was found to be statistically significant in male patients.
Conclusion: In planning the treatment of patients with diabetes, evaluating them mentally will help to provide optimal treatment and care services.
Keywords: type 1 diabetes, type 2 diabetes, anxiety
Introduction
Diabetes is a chronic disease resulting from the lack of production of insulin hormone by the pancreas or inability to use the produced insulin effectively, leading to disorders in carbohydrate, fat, and protein metabolism.1 Insulin hormone enables the cells to take in blood glucose and further convert it to energy. Inability to produce insulin or to use it effectively results in elevated blood glucose levels, which, in the long term, lead to damage of various tissues and organs in the body, and consequently, loss of their functions.2
Type 1 diabetes mellitus (DM) corresponds to 10%–20% of the overall diabetes population. Pancreas beta cell destruction occurs depending on autoimmune events. Islet cell antibodies (ICA) and antibodies against glutamic acid decarboxylase (GAD) are positive at the rate of 85%. Type 2 DM is a complex metabolic disease characterized by a deterioration in pancreatic insulin secretion and/or insulin resistance in target tissues. Its prevalence in the overall diabetic patient population is between 80% and 90%. Type 2 DM develops in genetically vulnerable individuals and is also influenced by various environmental factors. Sex, age, and ethnic origin are among the important risk factors determining type 2 DM.3,4
Diabetes develops in ~6–7 million people every year worldwide, and furthermore, almost half of the diabetics are not aware of their condition. The region with the highest diabetes prevalence of 9.2% is North America.5,6 According to the Turkish Diabetes Epidemiology Study conducted in Turkey in the years 1997 and 1998, diabetes prevalence was found to be 7.2%, and deteriorated glucose tolerance was found to be 6.7% in the age group of 20–80 years.7
Diabetes is a disease that affects the whole life of the patient like other chronic physical diseases and might lead to social or psychological adaptation problems. Diabetes Mellitus is a condition with psychiatric and psychosocial aspects besides being a physical disease, and a diabetic patient faces a range of physical, social and sexual problems.8,9 It is often difficult for a diabetic patient to accept that he/she has a chronic disease and that he/she has to change his/her lifestyle.10
Emotional stress indirectly disrupts the treatment and monitoring of diabetes and deteriorates adaptation. Nutrition, insulin intake, and adaptation to the rules concerning physical effects become difficult in a patient experiencing stress, denial, and anger. Free fatty acids, cortisone, and blood glucose levels increase even when the person experiences simplest psychosocial strain and mental conflict. When an organism is under stress, increased levels of glucagon, catecholamines, cortisone, and growth hormone lead to hyperglycemia and ketonemia. Stress is an important factor in the cases in which blood glucose cannot be regulated despite medical treatment. Therefore, many studies have been conducted in recent years on the levels of mental problems suffered by diabetic patients and the factors associated with mental problems.11
Cortisol, which increases during stress, increases appetite in vulnerable individuals, resulting in the rise of blood glucose and blood pressure. Rise of blood pressure further increases the physiological stress of the individual.13
Disorder of adaptation to diabetes, its complications, or its treatment method may develop in the form of anxiety, which is usually expressed as tediousness, worry, and boredom; anxiety is the disturbing feeling of concern and fear, which is a threat against life or is perceived as a threat. It is a mood experienced in the face of a possibility hazard from inner or outer world or any situation that is perceived and interpreted as dangerous by the individual.14,15 Anxiety is a universal, subjective, and observable experience. Therefore, the existence of anxiety can be predicted with the symptoms and observable behaviors. A person can experience different levels of anxiety: mild, moderate, or severe; moderate anxiety is useful in ensuring motivation.16 An individual with anxiety experiences a fear of uncertain future or feeling of concern accompanying the feeling of uncertainty and helplessness.
Blood glucose level directly affects the brain and mental functions, while emotional and mental changes affect the blood glucose levels.17 Stress and worry are important risk factors where blood glucose levels cannot be regulated despite undergoing medical treatment. Moreover, incidence of anxiety has been increasing in the patients in whom diabetes-dependent complication develops. As the complication develops, the quality of life of the patient decreases and barriers in the life increase, resulting in disability and increase of severity of the anxiety.18 Psychological and psychosocial evaluation should be made in such cases. Psychological interventions not only reduce emotional stress but may also decrease the symptoms associated with diabetes and improve prognosis. Therefore, patients are recommended to learn coping with stress through individual or group psychotherapies.19
The main purpose in the control of diabetes is to prevent long-term complications associated with the disease and to enhance the quality of life. To achieve this, evaluation of the psychological elements during the course of treatment in diabetic patients will help in overcoming many of the problems more easily. We aimed to determine the relationship between the type 1 and type 2 diabetic patients and the anxiety.
Materials and methods
The study included 103 type 2 DM patients and 28 type 1 DM patients followed up at the Internal Diseases Polyclinic of Bingol State Hospital. The sample was constituted by patients who were followed up with the diagnosis of diabetes, who could communicate, and who volunteered to participate in the study. Exclusion criteria in the constitution of the study group were existence of physical disease or cognitive insufficiency at a level that hinders the completion of the questionnaires and currently undergoing treatment due to a psychiatric disease. No patients were excluded from the study for the aforementioned reasons. The study included a total of 131 diabetic patients. The study protocol was approved by the local Ethics Committee at the University of Bingol. The study was carried out in accordance with the principles of declaration of Helsinki, and written inform consent was obtained from all participants.
The questionnaire used in the study consisted of two parts. The first part of the questionnaire comprised a set of questions querying the sociodemographic characteristics and the second part comprised the Beck Anxiety Inventory (BAI).
Beck Anxiety Scale (BAS) is a self-evaluation scale developed by Beck et al and is used for the purpose of determining frequency of the anxiety symptoms experienced by the individuals. Turkish validity and reliability studies were conducted by Ulusoy et al. This scale contains a total of 21 questions.20
High total score shows that anxiety level or severity is high. Anxiety levels of the patients can be interpreted according to the scores received from BAS: 0–17 points indicate low, 18–24 points indicate moderate, and 25 and higher points indicate the presence of severe anxiety.
The data were evaluated on the statistical package program. Mean values were given together with standard deviation and P<0.05 was set as significance level. Frequency was utilized for illustration of the indicative data, and chi-square test and analysis of variance were conducted for the evaluation of statistical significance of other data.
Results
The study included a total of 131 patients followed up at the Internal Diseases Polyclinic of Bingol State Hospital, 103 of whom were type 2 DM patients and 28 were type 1 DM patients. A total of 52.7% of the patients were male and 47.3% were female. It was found that the majority of the patients lived in the province center (63.4%), most of them were married (77.1%), almost half of them were illiterate (43.5%), 67.1% were earning an income less than Turkish Lira (TL) 2,000, and 35% had green card, whereas 3.8% had no social security (Table 1). Moreover, 64.1% of the patients lived with their spouses and 58.8% did not smoke.
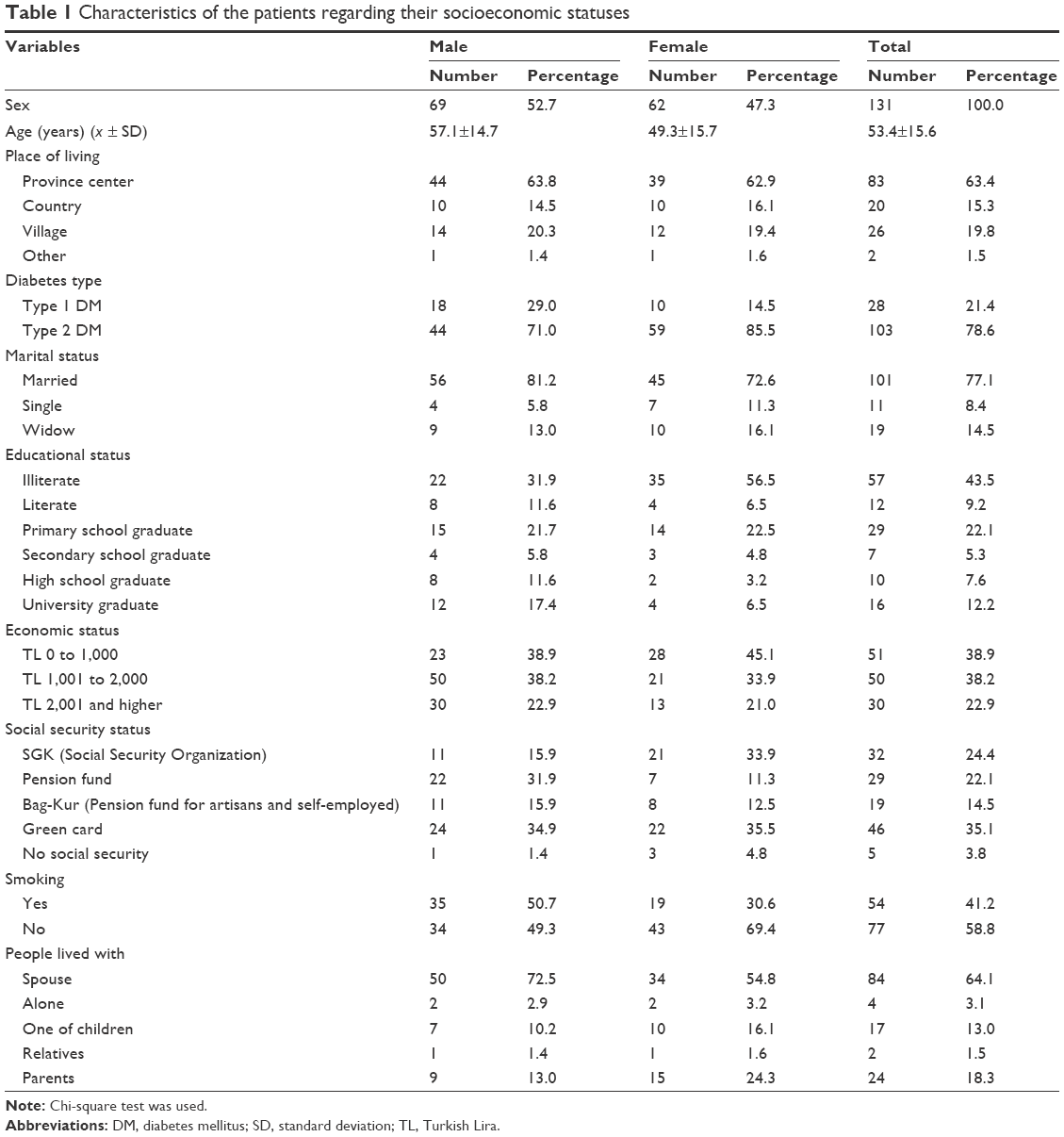 | Table 1 Characteristics of the patients regarding their socioeconomic statuses |
Information regarding diseases of the patients by sex is given in Table 2. A total of 85% of male and 71% of female patients were type 2 DM patients. When examined for how long the patients have been diabetic, it was seen that 39.1% of the male and 40.3% of the female patients were within the first 3 years of the disease. A total of 45.0% of the male patients go for a medical checkup when they feel unwell and 42.0% go once a month, whereas 62.9% of the female patients go for a checkup when they feel unwell. More than half of the diabetic patients (male: 55.1% and female: 59.7%) suffer from other diseases, and mostly (male: 60.5% and female: 70.3%) cardiovascular diseases accompany diabetes. No statistically significant difference was found except for diabetes type distribution among the sexes (P>0.05).
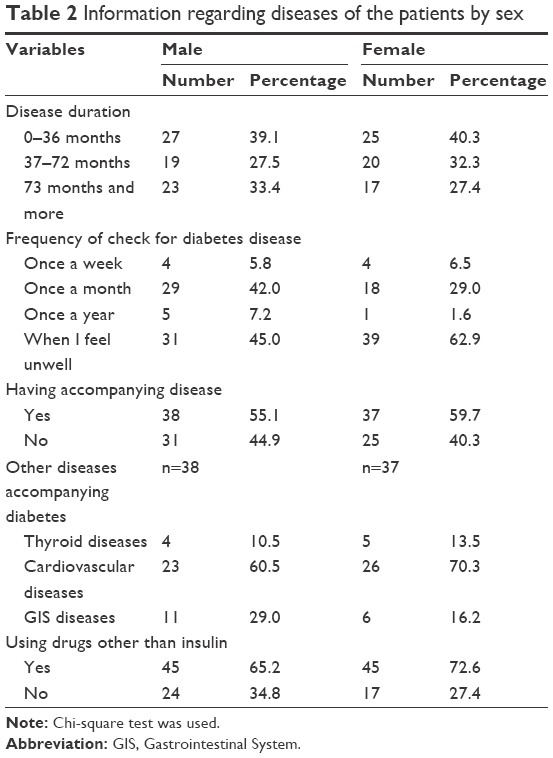 | Table 2 Information regarding diseases of the patients by sex |
When the mean and standard deviation values of BAS scores of the patients in terms of different variables were evaluated, a significant difference was found in the mean and standard deviation values between the diabetes types in both male and female patients (P<0.05). The fact that type 2 DM is more prevalent than type 1 DM among male and female patients may have also influenced the higher BAS scores in type 2 DM patients compared to type 1 DM patients among both male and female patients. Moreover, BAS score was found to be higher in patients who use drugs other than insulin among both male and female patients compared to the patients who do not use other drugs, and this difference was statistically significant (P<0.05). Unlike female patients, the difference between duration of disease and BAS score was found to be statistically significant in male patients (P<0.05). Accordingly, BAS score was significantly higher in male subjects who have been diabetic for 3–6 years when compared to the individuals who have been diabetic for less than 3 years. In female patients, unlike male patients, a significant difference was found between mean and standard deviation values of BAS scores with respect to the place of living, marital status, and educational status (P<0.05). Accordingly, among those living in villages, BAS score was significantly higher in the widows than in others, and BAS score was significantly higher in the illiterate than in others (Table 3).
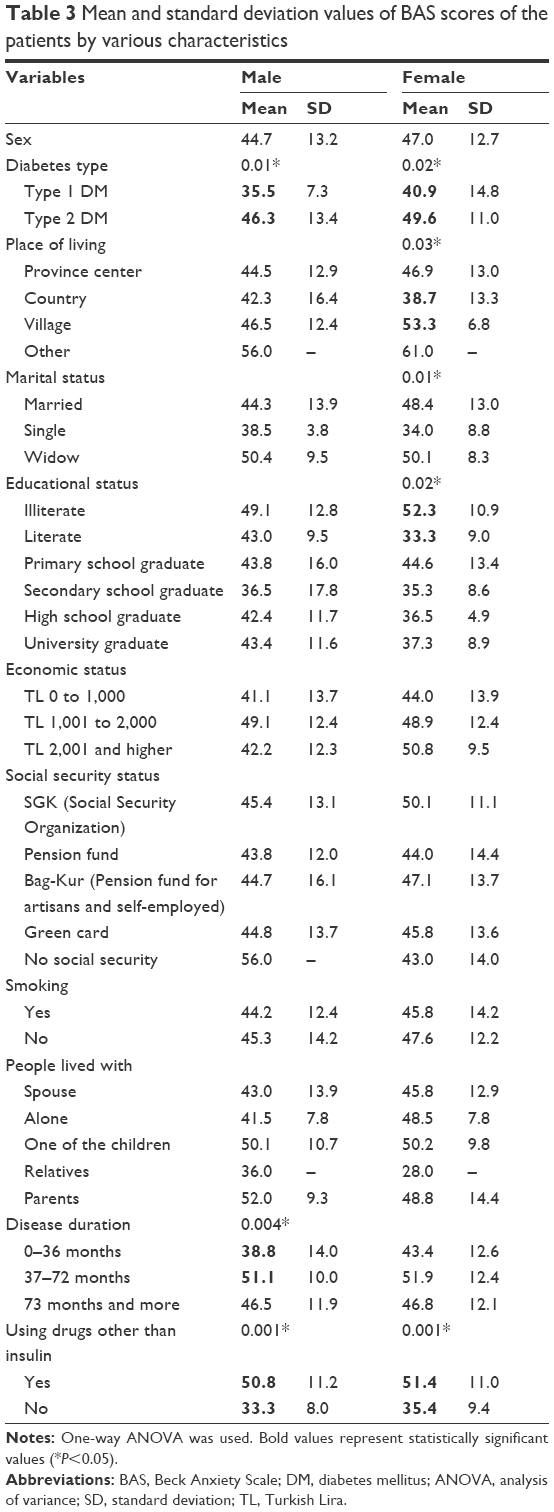 | Table 3 Mean and standard deviation values of BAS scores of the patients by various characteristics |
Discussion
A total of 52.7% of the patients were male and 47.3% were female. In the study conducted by Gulseren et al in patients with DM, of 180 patients, 128 (71.1) were female and 52 (28.9) were male.21 In the study conducted by Eren et al, of 104 patients, 57 (54.8) were female.22 It was found that the majority of diabetes patients (63.4%) lived in province center. In many regions, diabetes was more prevalent in the urban than in rural populations. Social collapse, unemployment, and poverty may coexist with diabetogenic lifestyle factors such as reduced physical activity, Western diet, and obesity.23 It is observed that the majority of the participants (77.1%) were married; in a study conducted by Kara et al, 82.5% were married and 15% were widow(er)s.24
In our study, it was found that almost half of the patients (43.5%) were illiterate. In a study conducted by Gokdogan et al, regarding educational status of the patients, they reported that 51.4% of the 70 patients were literate or primary school graduates.25 While it was seen that 67.1% of the participants had an income below TL 2,000, they reported in a study that 47% of the diabetic patients had middle income. Thirty-five percent of the patients participating in the study had green card, whereas 3.8% were found not to have social security.26 Gokdogan et al, in a study, reported that 68.6% had social security depending on the pension fund.25 They also reported that 58.8% of the patients do not smoke. In a study conducted by Eren et al, 72.8% of the patients do not smoke.22
Type 1 DM was found to be higher among female than male patients and type 2 DM was found to be higher among male than female patients, and this difference was statistically significant (P<0.05). More than half of the patients (male: 55.1% and female: 59.7%) had cardiovascular diseases along with diabetes (male: 60.5% and female: 70.3%). Essential hypertension, which is frequent in the overall population, may also coexist with diabetes.27 The results obtained in our study was found to be consistent with those reported in the literature. It was found that 65.2% of males and 72.6% of females use drugs other than insulin. No statistically significant difference was found except for diabetes type distribution by sex (P>0.05).
According to the results of BAS, applied to the patients to examine their psychological states, 94.2% of male and 96.8% of female patients were in the severe anxiety group. Allison et al found common anxiety disorder in 14% of the diabetes patients.28
When the distribution of BAS scores among the patients was examined, it was found that males took 44.7±13.2 points and females took 47.0±13.0 points as mean value, but no statistically significant difference was found between BAS scores by sex (P>0.05). There are also studies reporting that anxiety is more prevalent in women compared to men.29,30
When mean and standard deviation values of BAS scores of the patients in terms of various characteristics were compared, a significant difference was found in mean and standard deviation values between the diabetes types in both male and female patients (P<0.05). Among both male and female patients, BAS scores of the type 2 DM patients were higher than those of the type 1 DM patients. In this study, it was found that there was no significant difference between anxiety levels in patients with type 1 and type 2 DM.31 There are also studies where anxiety score was found to be high in type 2 DM patients.32
Unlike female patients, the difference between the duration of disease and BAS score was seen to be statistically significant (P<0.05). Accordingly, BAS scores of the male individuals who have been diabetic for 3–6 years was significantly higher than the scores of those who have been diabetic for less than 3 years. The findings of Alpar and Tosun showed that the effects of diabetes increases as the length of time affected by the disease increases, and that the level of anxiety also decreases with time.33 According to the results attained from the meta-analysis of 42 studies conducted by Anderson et al, it was found that in a 10-year course of diabetes, although the prevalence of psychiatric disorders such as anxiety disorder increased, the psychological condition of most of the children and adult diabetics was good.34
In female patients, unlike male patients, a significant difference was found between mean and standard deviation values of BAS scores with respect to the place of living, marital status, and educational status (P<0.05). Some studies reported that anxiety tendencies in the singles were higher than in the married.35
Conclusion and recommendations
In conclusion, diabetes is a chronic disease that persists lifelong, affects many aspects of an individual’s life, and might lead to complications in the patient unless treated well. After being diagnosed, it becomes difficult for the patient to accept that he/she has a chronic disease that will affect his/her life and that he/she has to organize and change his/her life accordingly. Although the patient is required to make changes in his/her life for adaptation to the disease, difficulty of adaptation and organic effect of the disease increase the incidence of anxiety in the patients; at the same time, anxiety disorder is important in terms of increasing disease-dependent devastation and mortality as well as making the adaptation of the patient more difficult. From this aspect, early intervention and support to the patient will be beneficial in terms of adaptation of the patient and prevention of the complications, and effect on life will be minimized.
Disclosure
The authors report no conflicts of interest in this work.
References
Unlusoy F. Effect of Blood Glucose Monitoring on Life Quality and Diabetes Control in Diabetics [postgraduate thesis]. Istanbul, Turkey: University Institute of Health Sciences; 2009. | ||
About diabetes; 2015. Available from: http://www.idf.org/about-diabetes. Accessed August 24, 2015. | ||
Ferrannini E, Gastaldelli A, Matsuda M, et al. Influence of ethnicity and familial diabetes on glucose tolerance and insulin action: a physiological analysis. J Clin Endocrinol Metab. 2003;88:3251–3257. | ||
Goran MI, Coronges K, Bergman RN, et al. Influence of family history of type 2 diabetes on insulin sensitivity in prepubertal children. J Clin Endocrinol Metab. 2003;88:192–195. | ||
American Diabetes Association (ADA). Diagnosis and classification of diabetes mellitus. Diabetes Care. 2008;31:55–60. | ||
King H, Aubert RE, Herman WH. Global burden of diabetes, 1995–2005: prevalance, numerical estimates, and projections. Diabetes Care. 1998;21:1414–1431. | ||
Turkish Diabetes Foundation. Diabetes Treatment. Available from: http://www.turkdiab.org/page.aspx?u=1&s=17. Accessed July 20, 2015. | ||
Buzlu S. Psychosocial aspect of diabetes. In: Erdogan S, editor. Diabetes Nursing Fundamental Information. Istanbul, Turkey: Yuce Yayim Dagitim; 2002. | ||
Ongider N. Examination of Hopelessness and Survival Reasons In People with Chronic Physical Disease [postgraduate thesis]. Izmir, Turkey: Ege University; 1997. | ||
Akbay Pirildar S, editors. Internal medicine and psychiatry V. In: Depression and Anxiety Disorders in Diabetes. 1st ed. Istanbul, Turkey: Okuyan Us Yayin; 2003. | ||
Ozkan S. Psychiatric Medicine, Consultation and Liaison Psychiatry. Roche; 1995:95–99. | ||
Guven T. Investigation of Life Quality and Depression Effect in Patients with Diabetes Mellitus [postgraduate thesis]. Istanbul, Turkey: Ministry of Health Sisli Etfal Training and Research Hospital Psychiatry Clinic; 2007. | ||
Kumcagiz H, Ozenoglu A, Avci AA, Ugurlu S. Anxiety levels and coping with stress in patients with type 2 diabetes mellitus. Cumhuriyet Med J. 2009;31:122–129. | ||
Isik E, Taner Y. Anxiety disorders in children, adolescents and adults. Asimetrik Parelel Kitabevi. 2006;1(1):3–29. | ||
Ozmen M. Psycho-Social Problems in Diabetes, Turkish Diabetes Almanac 2000–2001. Istanbul, Turkey: Turkish Diabetes Society Annual Publication Organ; 2001. | ||
Spencer P. Anxiety. In: Kim KK, Peg E, editors. Palliative Practices from A–Z for the Bedside Clinician. Pittsburgh, PA: Oncology Nursing Society; 2002:23–26. | ||
Kovacs M, Goldston D, Obrosky DS, et al. Psychiatric disorders in youths with IDDM: rates and risk factors. Diabetes Care. 1997;20:36–44. | ||
Bahar A, Sertbas G, Sonmez A. Determination of depression and anxiety levels of patients with diabetes mellitus. Anadolu Psychiatry J. 2006;7:16–18. | ||
Yuksel S. Evaluation of Sleep Quality, Anxiety, Depression and Life Quality condition of Type 1 and Type 2 Diabetic Patients [postgraduate thesis]. Afyon, Turkey: Afyonkarahisar Kocatepe University Institute of Health Sciences; 2007. | ||
Güleç H, Sayar K, Özkorumak E. Somatic symptoms of depression. Turkish Psychiatry Journal. 2005;16:90–96. | ||
Gulseren L, Hekimsoy Z, Gulseren S, Bodur Z, Kultur S. Depression, anxiety, life quality and disability in patients with diabetes mellitus. Turkish Psychiatry J. 2001;12(2):89–98. | ||
Eren I, Erdi O, Ozcankaya R. Relationship of blood glucose control and psychiatric disorders in type II diabetic patients. Turkish Psychiatry J. 2003;14(3):184–191. | ||
King H, et al. Diabetes in the world. Number of cases among adults aged between 20–79 in selected countries. Diabetes Care. 1993;16:157–177. | ||
Kara B, Akbayrak N. Examination of continuous anxiety levels of type II diabetes mellitus patients. J Trends Endocrinol. 2002;11(5): 202–211. | ||
Gokdogan F, Akinci F. Perception of the diabetics living in Bolu about their health and diseases and their practices, C.U. J Higher School Nurs. 2001;5(1):10–16. | ||
Dietrich UC. Factors influencing the attitudes held by women with type II diabetes: a qualitative study. Patient Educ Couns. 1996;29(1):13–23. | ||
Glasgow, RE, Toobert, DJ. Social environment and regimen adherence among type II diabetic patients. Diabetes Care. 1988;11:377–386. | ||
Allison B, Grigsby RJ, Anderson KE, et al. Prevalence of anxiety in adults with diabetes: a systematic review. J Psychosom Res. 2002;53:1053–1060. | ||
Ozer SK, Demir B, Tugal O, et al. Montgomery-Asberg depression rating scale: inter-rater reliability and validity study. Turkish Psychiatry J. 2001;12:185–194. | ||
Ozturk MO. Mental Health and Disorders. 9th ed. Ankara, Turkey: Feryal Matbaasi; 2002. | ||
Rohlfing CL, Wiedmeyer HM, Little RR, et al. Defining the relationship between plasma glucose and HbA(1c): analysis of glucose profiles and HbA(1c) in the Diabetes Control and Complications Trial. Diabetes Care. 2002;25(2):275–278. | ||
Winocour PH, Main CJ, Medlicott G, et al. A psychometric evaluation of adult patients with type I (insulindependent) diabetes mellitus. Prevalence of psychological dysfunction and relationship to demographic variables, metabolic control and complications. Diabetes Research. 1990;14:171–176. | ||
Schram MT, Baan CA, Pouwer F. Depression and quality of life in patients with diabetes: a systematic review from the European depressionin diabetes (EDID) research consortium. Curr Diabetes Rev. 2009;5: 112–119. | ||
Anderson RJ, Freedland KE, Clouse RE, Lustman PJ. The prevalance of comorbid depression in adults with diabetes: a metaanalysis. Diabetes Care. 2001;24:1069–1078. | ||
Leedom L, Meehan WP, Procci W, Zeidler A. Symptoms of depression in patients with type II diabetes mellitus. Psychosomatics. 1991;32:280–286. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.