")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 14
Evaluation of Antihyperglycemic Effect of Extract of Moringa stenopetala (Baker f.) Aqueous Leaves on Alloxan-Induced Diabetic Rats
Authors Woldekidan S, Mulu A , Ergetie W, Teka F, Meressa A, Tadele A, Abebe A, Gemechu W, Gemeda N , Ashebir R , Sileshi M , Tolcha Y
Received 17 September 2020
Accepted for publication 4 December 2020
Published 15 January 2021 Volume 2021:14 Pages 185—192
DOI https://doi.org/10.2147/DMSO.S266794
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Prof. Dr. Antonio Brunetti
Samuel Woldekidan,1 Abay Mulu,2 Wondwossen Ergetie,3 Frehiwot Teka,1 Asfaw Meressa,1 Ashenif Tadele,1 Abiy Abebe,1 Worku Gemechu,1 Negero Gemeda,1 Rekik Ashebir,1 Meron Sileshi,4 Yoseph Tolcha4
1Directorate of Traditional and Modern Medicine Research, Ethiopian Public Health Institute, Addis Ababa, Ethiopia; 2Department of Anatomy, School of Medicine, College of Health Science, Addis Ababa University, Addis Ababa, Ethiopia; 3Department of Pathology, School of Medicine, College of Health Science, Addis Ababa University, Addis Ababa, Ethiopia; 4National Clinical Chemistry Reference Laboratory, Addis Ababa, Ethiopia
Correspondence: Samuel Woldekidan
Directorate of Traditional and Modern Medicine Research, Ethiopian Public Health Institute, P.O. Box 1242, Addis Ababa, Ethiopia
Email [email protected]
Background: Diabetes is a serious metabolic disorder with complications that result in significant morbidity and mortality. Current drugs used for diabetes therapy are not free from side effects and do not restore normal glucose homeostasis. Therefore, the purpose of this study is to evaluate the antidiabetic effect of Moringa stenopetala (Baker f.) aqueous leaves extract.
Methods: Thirty rats of weight 90– 150 gram were distributed to five groups (n= 6). Then labelled as diabetic control (DC), normal control (NC), extract treated (MS 250 and 500mg/kg), and glibenclamide treated (GL 5mg/kg). The experimental rats were induced by intra-peritoneal injection of Alloxan monohydrate at a dose of 180 mg/kg after dissolving in normal saline. Clinical biochemistry such as AST, ALT, ALP, urea, creatinine, and cholesterol, blood glucose level, histopathological and preliminary phytochemical screening were evaluated.
Results: Phytochemical tests revealed the presence of different secondary metabolites. Alkaloid, flavonoid, tannin, saponin, phytosteroids, phenols and terpenoids. Moringa stenopetala (Baker f.) leaves aqueous extract (250 and 500mg/kg) improved the body weight of rats, showed remarkable reduction in blood glucose concentration (P< 0.05), and significantly decreased serum urea, creatinine, ALT, AST and ALP (P < 0.05). Levels of serum cholesterol remained unaltered in the experimental groups when compared with diabetic control. Histopathology of non-treated rats showed deterioration of insulin producing pancreas cells; nevertheless, β-cells restoration was observed due to administration of Moringa stenopetala (Baker f.) aqueous leaves extract.
Conclusion: It is possible to conclude that oral administration of Moringa stenopetala (Baker f.) aqueous leaf extracts (250mg/kg and 500mg/kg) for 28 days showed beneficial effects on antihyperglycemia, improved body weight and Alloxan damaged pancreatic β-cells, and restored biochemical changes.
Keywords: diabetes, Moringa stenopetala, pancreatic β-cells, alloxan monohydrate
Introduction
A serious disorder of carbohydrate metabolism, which causes blood glucose to rise in blood streams abnormally emanating from the difficulty in insulin secretion1,2,3 is referred as diabetes mellitus. It is characterized by hyperglycemia (fasting blood glucose ≥ 126 mg/dL; random plasma glucose ≥ 200mg/dL) manifesting often with symptoms and signs of osmotic diuresis such as polydipsia, polyuria, generalized weakness, calorie loss, polyphagia and weight loss resulting from either an absolute deficiency (Type 1) or a relative deficiency (Type 2) of the hormone, insulin.2,4 Diabetes mellitus, among the most common chronic diseases occurring worldwide, continues to escalate in magnitude and significance due to changing lifestyles such as reduced physical activity and increased obesity mainly resulted from economic development and urbanization.5
It is the most rampant and rapidly growing global problem which poses huge health and socioeconomic burdens.6 According to 2017 reports, there were 425 million diabetic adults worldwide and this number is supposed to increase to 629 million by 2045.3 The anti-diabetic agents which are currently in use result in serious side effects such as renal failure, anemias, weight gain, cholestatic jaundice, hypoglycemia, and drug resistance, among others. This calls for a search for safe, effective and alternative anti-diabetic agents from medicinal plants.7,8
Moringa stenopetala (Baker f.) is a green, drought-resistant plant.9 It is endemic to East Africa, the coverage includes Southern Ethiopia, North Kenya and East Somalia. Some medicinal values were noted in a report such as expelling retained placenta and stomach pain,10 antileshimania,11 antitrypanosomial12 and antimicrobial.13 Its crude aqueous extract of leaves showed hypoglycemic effect on rabbit and mice.14,15 In many of its ecological areas, roots and leaves mixed with water are used to treat hypertension, stomach disorders, asthma, diabetes, malaria16 and high blood cholesterol.17 The aim of the present study was, therefore, to evaluate antidiabetic, and pancreatic damage effect of Moringa stenopetala (Baker f.) aqueous extract on diabetic rats.
Materials and Methods
Plant Collection
Based on its ethnobotanical information, the fresh Moringa stenopetala (Baker f.) leaves was collected from Arbaminch, (6° 2′ 0″ N, 37° 33′ 0″ E), Southern part of Ethiopia, about 500km from Addis Ababa. The plant material was authenticated by a taxonomist from the Ethiopian Public Health Institute (EPHI) and a voucher number AL-001was deposited in the herbarium for future reference.18
Extraction of Plant Material
Fresh leaves of the Moringa stenopetala (Baker f.) were cleaned of tiny particles, chopped, dried under shade (at room temperature), grinded to powder using mortar and pestle, and stored in cool and dry place. Then 1.208 and 2.130Kg of powdered leaves were kept in Erlenmeyer flasks and macerated with water (distilled) for 4hrs with intermittent agitation by orbital shaker DS-500. The extract solution was filtered using cotton of 0.1 mm2 mesh gauze and freeze-dried at lower temperature (˗46°C to ˗51°C) and lower pressure (133x10-3mbr) to form crude extract. Then kept in a desiccator at room temperature.18
Animals
Thirty rats of weight 90–150 gram indiscriminately distributed to five groups (n= 6). Then labelled in the following manner: diabetic control (DC), normal control (NC), extract treated (MS 250 and 500mg/kg), and diabetic glibenclamide treated (GL 5mg/kg). All groups were allowed to have standard rat pellets and water throughout the experiment in a separated cage, 21±1°C and light periods. Animals used for this study were acclimatized to laboratory conditions for two weeks prior to the experiment to avoid any non-specific stress.19
Induction of Diabetes Mellitus
The experimental rats were induced by intra-peritoneal injection of Alloxan monohydrate at a dose of 180 mg/kg after dissolving in normal saline. Prior to diabetes induction, the animals were fasted for 12 hours. Confirmation of diabetes was done seven days after Alloxan monohydrate treatment (Fasting Blood Sugar), using one touch glucometer and blood sample for the FBS obtained from tail puncture of the rats, and those with FBS ≥126mg/dL were included in the study.
Experimental Procedure
The normal and diabetic control groups were kept without treatment only receiving normal saline. The two test groups 250 and 500mg/kg/day of Moringa stenopetala (Baker f.) aqueous leaf extract while the other group was given 5mg/kg/day glibenclamide for 28 days orally using oral gavages.
Blood Glucose Level Determination/Pharmacological Evaluation
By tail puncture method, blood sample was collected from each group for determination of blood sugar level starting from day 0 and every seventh day, 12 hours of fasted animals using one touch glucometer (i-QARE ds-w, Taiwan).
Blood Collection and Biochemical Determinations
At the end of the treatment period, the animals were anesthetized and sacrificed, then blood samples were collected into non anti-coagulated tubes after overnight fasting. Clinical biochemistry such as aspartate aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase (ALP), urea, creatinine and cholesterol level were evaluated to determine the liver and kidney functions of experimental animals.
Histological Examination
The fixation process started quickly after removal of the sample. On labeling tape, label the plastic sample jar with the names of the experimental group members, date, and type of sample. The vial filled about 2/3 full with the fixative, the experimental rats were sacrificed and pancreas were removed then placed into separate vials. After overnight fixation, pancreases were washed with tap water to remove excess fixatives for several times. The water was removed from tissue block by the process of dehydration with increased concentration of ethanol 70% (2hrs), 80% (1hr), 90% (1hr), absolute alcohol (I, II and III for one and half hours each, and IV overnight). Prior to sectioning, tissue was cleared in two changes of xylene I (one and half hours) and xylene II (for two and half hours). Then tissue was infiltrated with three steps of paraffin wax I, II, and III for one and half hours, two and half hours, and overnight, respectively. After infiltration, the tissue was allowed to solidify in a mold, embedded within a small cube of paraffin forming tissue blocks, whereby each tissue block was labelled and stored at room temperature. The microtome drove a knife across the surface of the paraffin cube and produced a series of thin sections of very precise thickness.
Tissue blocks were sectioned in ribbons at a thickness of 5 µm with Leica rotary microtome (LEICA RM 2125RT, Germany). The ribbons of sections were taken at every 5th section and put onto the surface of a warm water bath at temperature of 40°C. The floating ribbons over the surface of warm water were mounted onto pre cleaned slides. The slides containing paraffin wax sections were arranged within the slide holder and placed in an oven with temperature of 40°C overnight, to fix the tissue to the slides. The tissue sections were washed with tap water for five minutes and stained progressively with Harris haematoxylin for 10 minutes, then washed under running tap water for five minutes. The slides were immersed in acidic alcohol for differentiation and controlling over stained haematoxylin, for 1–3 seconds, and then put in Sodium bicarbonate until they became blue. Then, the slides were counter stained with eosin for one minute and then washed in tap water for five minutes. The sections were dehydrated with increasing alcohol concentration of 80%, 95%, absolute II and I for three minutes, each. The dehydrated sections were cleared with xylene II and I for three minutes each and permanently mounted on microscopic slides using DPX and cover slips and then observed by light microscope for investigations of any histological change, thereby the histology of the treated groups were compared with histology of the control group.20
Phytochemical Screening
Preliminary phytochemical screening was performed using standard methods as described.21
Data Analysis
Data was analyzed using SPSS version 24. Mean ± SEM given for variables of quantitative. Differences of group mean and which group differs were observed by applying ANOVA (one way analysis of variation) and post Hoc Tukey’s test respectively. Statistical significance was considered at p-value of < 0.05.
Ethical Consideration
The study was conducted in accordance with ethical clearance approved and obtained from Department of Anatomy Graduate Committee; School of Medicine, College of Health Sciences, AAU and Ethiopian Public Health Institute; Ref EHNRI/SERO/SERC/49/2003.
Results
Blood Sugar Level Result
After IP administration of Alloxan monohydrate, the fasted blood glucose level except the NC group raised above 126 mg/dL in all experimentally induced diabetic groups. Only rats having fasted blood sugar level more than 126 mg/dL were considered diabetic. Blood sugar level at Day 0 significantly increased when compared with NC. Administration of Moringa stenopetala (Baker f.) leaf aqueous extract to diabetic rats showed remarkable reduction in blood glucose concentration, there were significant (P<0.05) differences on Day 21 and 28 when compared with DC . Moreover, treatment with both doses of MS extract to diabetic rats produced significant reduction in the blood glucose levels of rats when compared with diabetic control group as indicated in the following Table 1.
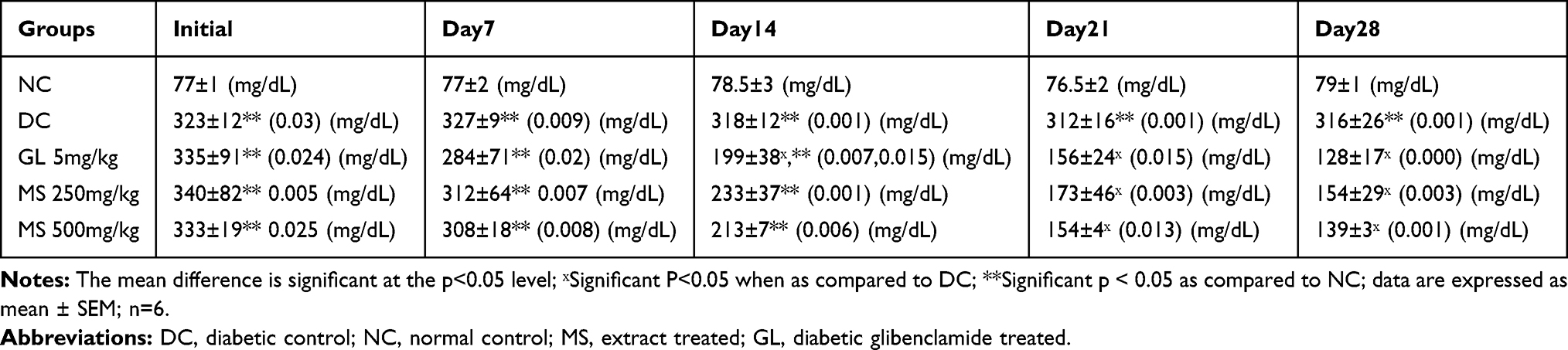 |
Table 1 Normal, Diabetic, and Treated Rats’ Blood Sugar Level |
Body Weight Result
Body weight were measured every seventh day of the experiment. The two doses of the extract improved the body weight of rats significantly from Day 14, 21 and Day 28 when compared with the DC group as shown in Table 2.
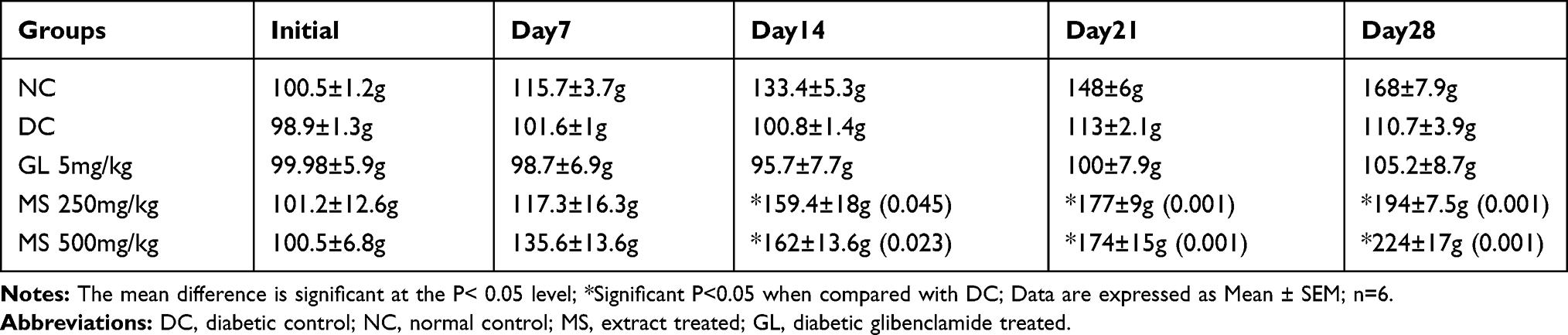 |
Table 2 Body Weight Change in Normal, Diabetic, and Treated Rats |
Biochemical Result
Continuous oral administration for 28 days of M. Stenopetala leaves aqueous extract for diabetic rats led to a significant decrease in serum urea, creatinine, ALT, AST and ALP (P < 0.05) as compared with DC showed significantly concentrated. This significant reduction was equivalent that occurred on application of glibenclamide. Levels of serum cholesterol remained unaltered in the extract treated, and glibenclamide treated groups when compared with control rats as shown in Table 3.
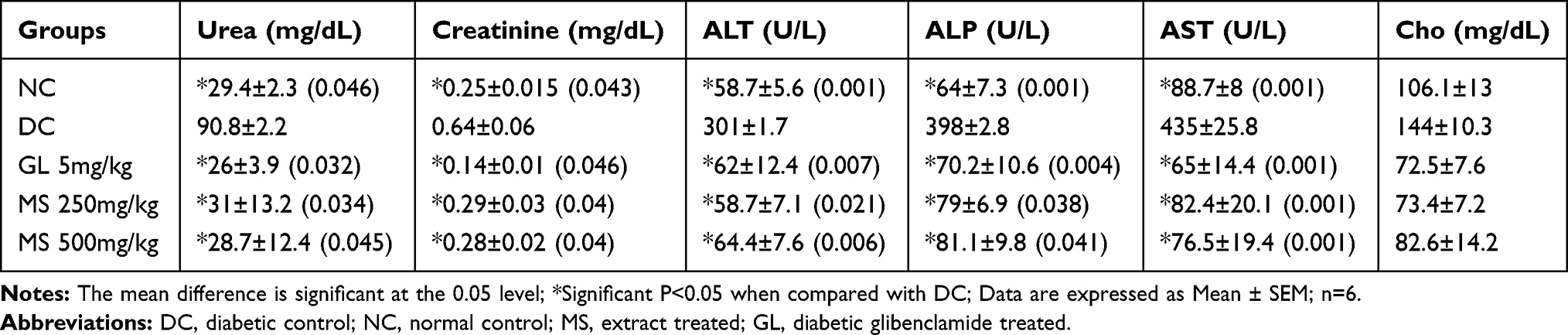 |
Table 3 Biochemical Results in Normal, Diabetic and Treated Rats |
Phytochemical Screening Result
Preliminary phytochemical analysis showed that the presence of alkaloid, flavonoid, tannin, saponin, phytosteroids, phenols and terpenoids in the aqueous leaf extract of Moringa stenopetala (Baker f.)
Histopathology Result
Histopathological results are shown in figure 1 and 2.
 |
Figure 1 Photomicrograph of Alloxan treated diabetic control (A) compared with normal control (B), and glibenclamide treated (C). (A) Arrow indicates the Alloxan induced damage of islets of Langerhans. (B) Arrow indicates healthy islets of Langerhans. (C) Arrow indicates glibenclamide restoration of cellular population size of islets of Langerhans. Stained with haematoxylin and eosin, Magnification 100x. |
 |
Figure 2 Photomicrograph of Alloxan treated diabetic control (A) compared with M. stenopetala 500mg/kg treated (B) and M. stenopetala 250mg/kg treated (C). (A) Arrow indicates the Alloxan induced damage of islets of Langerhans. (B and C) Arrow indicates M. stenopetala restoration and sprouting of islets of Langerhans from pre-existing. Stained with haematoxylin and eosin, Magnification 100x. |
Discussions
Different mechanisms of action of plant extracts to reduce blood glucose levels are already known. Some plants exhibit properties similar to the well-known sulfonylurea drugs like glibenclamide,22 while others do not affect blood glucose in normal state and act instead much like biguanides such as metformin which is a known antihyperglycemic compound.23,24 The use of Moringa stenopetala (Baker f.) in diabetics has been reported in the literature along with several other traditional claims. Hence, it was thought that investigations of these medicinal properties should be scientifically authenticated to validate the traditional claims. In the present study, in order to establish the scientific basis for the utility of the said plant in the treatment of diabetes, evaluation of antihyperglycemic and pancreatic damage effects of aqueous leaves extracts were performed in Alloxan-induced diabetic rats.
Alloxan is a specific toxin that destroys the pancreatic β-cells, provoking a state of primary deficiency in insulin without affecting other types of islets and is used in the laboratory to induce both T1DM and T2DM in animals. The diabetic effect of Alloxan is due to an excess in the production of free radicals. This excess leads to toxicity in pancreatic cells, which, in turn, reduces the synthesis and release of insulin while concurrently affecting other organs, such as the liver. Increased lipid peroxidation products and decreased plasma or tissue concentrations of superoxide dismutase, catalase, and glutathione have been well documented in the literature on Alloxan induced diabetes.25 The increase in fasting blood glucose concentration is an important characteristic feature of diabetes mellitus (DM). In this study, there were elevations in fasting blood glucose (FBG) level in diabetic group. The results of the present study on diabetic rats following daily oral administration for 28 days with aqueous leaves extract of Moringa stenopetala (Baker f.) (dose: 250mg/kg and 500mg/kg) demonstrated significant reduction in fasted blood glucose level after 21 days of treatment. This result is in agreement with other studies.26,27 Therefore, the present study revealed that aqueous leaves extract of Moringa stenopetala (Baker f.) (dose: 250mg/kg and 500mg/kg) have a significant antihyperglycemic effect on Alloxan-induced diabetic rats in a dose- and time-dependent manner.
There was weight reduction in diabetic control rats. Weight loss has been known to be one of the symptoms of DM. Alloxan induced diabetes was characterized by severe loss in body weight which is result of β-cells destruction and reduced production of insulin in animals.
This deficiency of insulin led to decreased amino acids uptake by tissues with a consequent reduction in the level of protein synthesis and also results in lipolysis in adipose tissues and protein breakdown (Mohan et al., 2013).28 Similar observations were detected in many experimental studies.29,30 In this study, daily oral treatment with extract showed significant increase (p<0.05) in body weight at the end of the experiment when compared with diabetic control. This result matched with the results reported by Toma et al, Geleta et al, Ghebreselassie et al, Musa et al, 2015.15,17,27,31
Diabetic nephropathy is a microvascular complication of diabetes. A key morphological change associated with sustained hyperglycemia is the accumulation of glycogen granules in distal tubules, which leads to renal hypertrophy.32 In this recent study, significantly increasing serum urea and creatinine indicate impairment of renal functions in diabetic animals. Moringa stenopetala aqueous leaves extract decreased significantly the serum creatinine and urea levels by enhancing renal functions and, the serum total cholesterol content did not show significant change, which agreed with an earlier study33 which reported that Moringa stenopetala (Baker f.) improved renal functions in diabetic rats by reducing serum urea and creatinine levels.
The AST, ALT and ALP are physiologically and clinically important enzymes. Since ALT occurs in much higher concentration in the liver than elsewhere, therefore increased ALT activity specifically reflects hepatic damage, which is a normal occurrence in diabetes may be due to leakage of the enzymes to blood stream. Within limits AST and ALT levels act as indicators of normal liver function.34 Diabetes and hyperlipidemia also cause cellular damage by altering the cell membrane architecture resulting in enhanced activities of ALP in diabetic rats. Presently in treated diabetic rats, restoration of these enzymes to normal levels indicates restoration of liver normal functioning upon treatment with M. stenopetala aqueous leaves extract. The present results appear consistent with a previous report, the restoration of transaminases to their normal levels after treatment indicates revival of insulin secretion and regenerative activities of islets of Langerhans cells of pancreas after administration of the plant material, by Toma et al27 who studied the effects of M. stenopetala extracts in Streptozotocin- induced diabetic rats and26 alloxan induced diabetic mice.
It has been suggested that enhanced production of free radicals and oxidative stress are central events to the development of diabetic complications. Use of antioxidants reduces oxidative stress and alleviates diabetic complications.35 Alloxan produce hyperglycemia by selective cytotoxic effect on pancreatic beta cells, via disruption of the cell membrane integrity. The pancreatic beta - cells are known to be involved in the storage, synthesis, and release of insulin, peptide hormone regulating protein, carbohydrate, and lipid metabolism. One of the intracellular phenomena for its cytotoxicity is through generation of free radicals as reviewed by Ijaola et al.30 It is equally possible for Moringa stenopetala (Baker f.) to have regenerated remnants of the already Alloxan- destroyed cells. It probably prevented the destruction of beta cells of islets in the pancreas.
In the present study, non-treated rats (Figures 1A and B and 2A) disclosed deterioration of insulin producing cells of pancreas, due to the chemical used to induce experimental diabetes which was Alloxan monohydrate. On the other hand, restoration of β-cells (Figures 1C and 2B and C) was revealed due to treatment/administration of glibenclamide and Moringa stenopetala (Baker f.) leaf extracts as reported by Toma et al.27 A review on the mode of action of flavonoids36 discussed about the various effects of the drug candidates in regulating diabetic syndromes. It has been demonstrated that flavonoids act against diabetes mellitus either through their capacity to avoid glucose absorption (inhibition of α-glucosidase activity in the intestine), or to improve glucose tolerance. Moreover, it has also been demonstrated that flavonoids can act as insulin secretagogues or insulin mimetics, probably by influencing the pleiotropic mechanisms, to attenuate the diabetic complications, besides, the drug candidates have been found to stimulate glucose uptake in peripheral tissues, and regulate activities of enzymes involved in metabolism of carbohydrate pathway.
Researchers have found that the antihyperglycemic effect of plant extract may be due to the presence of tannin. Tannins are excellent free radical scavengers, this property arising mainly from the presence of well-known antioxidants.37 Reduction of blood glucose level action of saponins is through restoration of insulin response, improvement in insulin signaling, increase plasma insulin levels and induction of insulin release from the pancreas, inhibition of disaccharides activity, activation of glycogen synthesis, inhibition of gluconeogenesis, inhibition of α- glucosidase activity and inhibition of mRNA expression of glycogen phosphorylase and glucose 6 phosphatase.38
The preliminary phytochemical screening of the extract in this recent study revealed the presence of alkaloids, steroids, terpenoids, tannins, saponins and flavonoids. Hence, the biological effect of aqueous leaf extract of Moringa stenopetala (Baker f.) are connected with their active principles including flavonoids, tannins and alkaloids which have been reported to have antihyperglycemic properties amongst others, however, required in order to ascertain the actual mechanism of this plant. This finding is in line with those of the previous studies carried out on antidiabetic and antihyperglycemic activity of different solvent extracts of Moringa stenopetala (Baker f.) leaves (Bakerf.) Cufod. Using various models: 70% EtOH and fractions in Alloxan monohydrate-induced mice26 n-butanol fraction of 70% EtOH in alloxan induced diabetic mice (Toma et al, 2015) and AQ,70% EtOH and n-butanol fractions in STZ induced diabetic rats.27,31
Conclusion
The medicinal plant is endowed with bioactive secondary metabolites possessing antihyperglycemic properties such as alkaloids, phenols, flavonoids, tannins, terpenoids, steroids and saponins. Repeated oral administration of Moringa stenopetala (Baker f.) aqueous leaf extracts (250mg/kg and 500mg/kg) for 28 days has shown beneficial effects on antihyperglycemia, improved body weight, restore biochemical changes of blood, improve alloxan pancreatic damage. After further investigation it is possible to say that Moringa stenopetala (Baker f.) leaves can be exploited as an alternative herbal supplement for the management of diabetes.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Khawandanah J. Double or hybrid diabetes: a systematic review on disease prevalence, characteristics and risk factors. Nutr Diabetes. 2019;9(1):1–9. doi:10.1038/s41387-019-0101-1
2. Ozougwu JC, Obimba KC, Belonwu CD, Unakalamba CB. The pathogenesis and pathophysiology of type 1 and type 2 diabetes mellitus. J Physiol Pathophysiol. 2013;4(4):46–57. doi:10.5897/JPAP2013.0001
3. Riaz Z, Ali MN, Qureshi Z, Mohsin M. In vitro investigation and evaluation of novel drug based on polyherbal extract against type 2 diabetes. J Diabetes Res. 2020. doi:10.1155/2020/7357482
4. Huang TH, Peng G, Kota BP, et al. Anti-diabetic action of Punica granatum flower extract: activation of PPAR-γ and identification of an active component. Toxicol Appl Pharmacol. 2005;207(2):160–169. doi:10.1016/j.taap.2004.12.009
5. Whiting DR, Guariguata L, Weil C, Shaw J. IDF diabetes atlas: global estimates of the prevalence of diabetes for 2011 and 2030. Diabetes Res Clin Pract. 2011;94(3):311–321. doi:10.1016/j.diabres.2011.10.029
6. Basit A, Fawwad A, Qureshi H, Shera AS. Prevalence of diabetes, pre-diabetes and associated risk factors: second national diabetes survey of Pakistan (NDSP), 2016–2017. BMJ Open. 2018;8(8):e020961. doi:10.1136/bmjopen-2017-020961
7. Hussain SN, Uzair M, Qaisar MN, Abbas K, Ashfaq K, Chaudhari BA. Assessment of anti-diabetic activity of Cassia sophera (Caesalpiniaceae). Trop J Pharm Res. 2018;17(3):443–449. doi:10.4314/tjpr.v17i3.9
8. Kooti W, Farokhipour M, Asadzadeh Z, Ashtary-Larky D, Asadi-Samani M. The role of medicinal plants in the treatment of diabetes: a systematic review. Electron Physician. 2016;8(1):1832. doi:10.19082/1832
9. Berhe G, Belihu K, Asfaw Y. Sero epidemiological investigation of bovine brucellosis in the extensive cattle production system of Tigray region of Ethiopia. Int. J. Appl. Res. Vet. Med. 2007;5(2):65.
10. Mekonnen Y. Effects of ethanol extracts of Moringa stenopetala leave on guinea pig and mouse smooth muscle. Phytother Res. 1999;13:442–444. doi:10.1002/(SICI)1099-1573(199908/09)13:5<442::AID-PTR476>3.0.CO;2-7
11. Mekonnen Y, Gessesse A. Documentation on the use of Moringa stenopetala and its possible antileishmanial and antifertility effects. SINET: Ethiop J Health Sci. 1998;21:287–295.
12. Mekonnen Y, Yardely V, Rock P, Croft S. In vitro antitrypanosomal activity of Moringa stenopetala leaves and roots. Phytother Res. 1999;13:538–539. doi:10.1002/(SICI)1099-1573(199909)13:6<538::AID-PTR486>3.0.CO;2-K
13. Biffa D. In vitro antimicrobial activities of bark and leaf extracts of Moringa stenopetala against mastitis causing bacterial pathogens. Ethiop Pharm J. 2005;23:15–22.
14. Mekonnene E, Hunde A, Damecha G. Hypoglycemic effect of Moringa stenopetala aqueous extracts in Rabbits. Phytother Res. 1997;11:147–148. doi:10.1002/(SICI)1099-1573(199703)11:2<147::AID-PTR41>3.0.CO;2-V
15. Mussa A, Makonnen E, Urga K. Effects of the crude aqueous extract and isolated fraction of moringa stenopetala leaves in normal and diabetic mice. Pharmacologyonline. 2008;3:1049–1055.
16. Padayachee B, Baijnath H. An overview of the medicinal importance of Moringaceae. J Med Plants Res. 2012;6(48):5831–5839.
17. Ghebreselassie D, Mekonnen Y, Gebru G, Ergete W, Huruy K. The effects of Moringa stenopetala on blood parameters and histopathology of liver and kidney in mice. Ethiop J Health Dev. 2011;25(1):51–57. doi:10.4314/ejhd.v25i1.69850
18. Debella A. Manual for Phytochemical Screening of Medicinal Plants. Addis Ababa, Ethiopia: EHNRI; 2002:26–71.
19. Guideline OO. Acute oral toxicity—up-and-down procedure. OECD Guidelines for the testing of chemicals; 2008.
20. Conn HJ. Biological Stains: A Handbook on the Nature and Uses of the Dyes Employed in the Biological Laboratory.
21. Harborne AJ. Phytochemical Methods a Guide to Modern Techniques of Plant Analysis. Springer science & business media; 1998.
22. Davis SN, Granner DK. Insulin, oral hypoglycemic agents, and the pharmacology of the endocrine pancreas. In: Hardman JG, Limbird LE, Molinoff PB, Ruddon RW, Gilman AG, editors.
23. De Fronzo RA, Goodman AM. Efficacy of metformin in patients with non-insulin dependent diabetes mellitus. N Eng J Med. 1995;333:550–554.
24. Stumvoll M, Nurjan W, Periello G, Dailey G, Gerich JE. Metabolic effects of metformin in non-insulin-dependent diabetes mellitus. N Engl J Med. 1995;333:541–549.
25. Aloulou A, Hamden K, Elloumi D. Hypoglycemic and antilipidemic properties of kombucha tea in alloxan-induced diabetic rats. Complement Altern Med. 2012;12(63):1–9. doi:10.1186/1472-6882-12-63
26. Sileshi T, Makonnen E, Debella A, Tesfaye B. Antihyperglycemic and subchronic toxicity study of Moringa stenopetala leaves in mice. J Coastal Life Med. 2014;2:214–221. doi:10.12980/JCLM.2.2014C300
27. Toma A, Makonnen E, Mekonnen Y, Debella A, Adisakwattana S. Antidiabetic activities of aqueous ethanol and n-butanol fraction of Moringa stenopetala leaves in streptozotocin-induced diabetic rats. BMC Comp Alt Med. 2015;15:242–249. doi:10.1186/s12906-015-0779-0
28. Mohan Y, Jesuthankaraj GN, Thangavelu NR. Antidiabetic and Antioxidant Properties of Triticum aestivum in Streptozotocin-Induced Diabetic Rats. Advances in Pharmacological and Pharmaceutical Sciences. 2013;2013. doi:10.1155/2013/716073
29. Akter S, Rahman MM, Abe SK, Sultana P. Prevalence of diabetes and prediabetes and their risk factors among Bangladeshi adults: a nationwide survey. Bull World Health Organ. 2014;92:204–13A. doi:10.2471/BLT.13.128371
30. Ijaola TO, Osunkiyesi A, Taiwo A, et al. Antidiabetic effect of ipomoea batatas in normal and alloxan-induced diabetic rats. J Appl Chem. 2014;7:16–25.
31. Geleta B, Makonnen E, Debella A, Tadele A. In vivo antihypertensive and antihyperlipidemic effects of the crude extracts and fractions of Moringa stenopetala (Baker f.) Cufod. leaves in rats. Front Pharmacol. 2016;7:97. doi:10.3389/fphar.2016.00097
32. Kang J, Dai X-S, Yu T-B, Wen B, Yang Z-W. Glycogen accumulation in renal tubules, a key morphological change in the diabetic rat kidney. Acta Diabetol. 2005;42:110–116. doi:10.1007/s00592-005-0188-9
33. Toma A, Deyno S. Phytochemistry and pharmacological activities of Moringa oleifera. IJP. 2014;1:222–231.
34. Stanely P, Prince M, Menon VP. Hypoglycaemic and other related actions of Tinospora cordifolia roots in alloxan-induced diabetic rats. J Ethnopharmacol. 2000;70(1):9–15. doi:10.1016/S0378-8741(99)00136-1
35. Hasani-Ranjbar S, Larijani B, Abdollahi M. A systematic review of Iranian medicinal plants useful in diabetes mellitus. Arch Med Sci. 2008;4(3):285.
36. Brahmachari G. Bio-flavonoids with promising antidiabetic potentials: a critical survey. Res Signpost. 2011;661:187–212.
37. Borgohain R, Lahon K, Das S, Gohain K. Evaluation of mechanism of antidiabetic activity of terminalia chebula on alloxan and adrenaline induced diabetic albino rats. Int J Pharm Bio Sci. 2012;3(3):256–266.
38. Lavle N, Shukla P, Panchal A. Role of flavonoids and saponins in the treatment of diabetes mellitus. J Pharm Sci Bioscientific Res. 2016;6(4):535–541.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.