")
Back to Journals » Infection and Drug Resistance » Volume 12
Evaluation of agar culture plates to efficiently identify small colony variants of methicillin-resistant Staphylococcus aureus
Authors Watanabe Y , Oikawa N, Hariu M, Seki M
Received 27 February 2019
Accepted for publication 22 May 2019
Published 21 June 2019 Volume 2019:12 Pages 1743—1748
DOI https://doi.org/10.2147/IDR.S207057
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Joachim Wink
Yuji Watanabe,1,2 Nozomi Oikawa,1,2 Maya Hariu,1,2 Masafumi Seki1
1Division of Infectious Diseases and Infection Control; 2Laboratory for Clinical Microbiology, Tohoku Medical and Pharmaceutical University Hospital, Sendai City, Miyagi, Japan
Background: Small-colony variants of methicillin-resistant Staphylococcus aureus (SCV-MRSA) recently were described as slow-growing, thymidine-dependent strains; typically, SCV-MRSA were isolated from patients receiving sulfamethoxazole-trimethoprim, but detection of these strains frequently was delayed because of their small colony size and slow growth. Bacteremia cases due to SCV-MRSA sometimes become lethal when the initiation of treatment with intravenous anti-methicillin-resistant Staphylococcus aureus (MRSA) drugs starts too late.
Methods: Here, we evaluated the use of general MRSA-specific agar plates in Japan, including MS-CFX, X-MRSA, and CHROMagar, for the efficient detection of SCV-MRSA, including the comparative detection efficiencies of these media for stock strains and clinical isolates.
Results: Among the three MRSA-specific agar plates that were tested, X-MRSA and CHROMagar showed similar detection efficiencies for both 24 and 48 hrs culturing; in contrast, MS-CFS did not permit the detection of SCV-MRSA in stock strains. For clinical isolates of SCV-MRSA, X-MRSA plates permitted detection of the smallest and slowest-growing colonies of SCV-MRSA at 48 hrs of culturing; in contrast, CHROMagar and MS-CFX sometimes did not identify SCV-MRSA at 24 and 48 hrs.
Conclusion: Optimization of media and incubation times will be necessary for efficient identification for SCV-MRSA, which would prevent delays in diagnosis and treatment with anti-MRSA drugs.
Keywords: SCV-MRSA, thymidine-dependent MRSA, X-MRSA, CHROMagar, MS-CFS, sheep blood agar
Introduction
Methicillin-resistant Staphylococcus aureus (MRSA) is responsible for a large proportion of infections in communities and hospitals, and a recent prospective, multinational surveillance study showed the high prevalence of MRSA in many Asian countries.1 It has been suggested that various MRSA clones have spread between the community and hospitals as well as between countries. In Japan, bacteremia caused by MRSA is a serious problem, occurring at increasing frequency while exhibiting resistance to treatment and associated high mortality.2
Among MRSA isolates, “small-colony variants” (SCV-MRSA) were recently reported.3–6 SCV-MRSA usually grow on sheep blood agar as tiny, nonpigmented, nonhemolytic colonies that show decreased metabolic activity.3 SCV-MRSA can be cultured only in the presence of distinct growth factors, such as hemin, menadione, or thymidine. Among them, thymidine-dependent SCVs (TD-SCVs) are well known in the context of cystic fibrosis (CF) lung disease, especially after prior use of trimethoprim-sulfamethoxazole (SXT).3,6
It has been shown recently that random mutations in the thymidylate synthase-encoding thyA gene that lead to an intracellular lack of dTMP are responsible for the formation of the colonies with the TD-SCV phenotype.4,5 TD-SCVs are apparently able to use thymidine and/or the metabolize dTMP from the environment; as a result, TD-SCVs can bypass the antibiotic effect of folic acid antagonists and consequently are resistant to SXT. The detection of SCV-MRSA, including TD-SCVs, is indispensable to the efficient and quick implementation of treatment by anti-MRSA drugs; agar plates capable of detecting both regular MRSA and SCV-MRSA are necessary for clinical applications.7–9
In the present study, we investigated several MRSA-specific agar plates for their ability to efficiently detect SCV-MRSA. Specifically, we compared these media for their efficiency of detection of SCV-MRSA in stock strains and clinical samples from patients at 24 and 48 hrs of culturing.
Methods
SCV-MRSA strains
SCV-MRSA strains from adult patients were cultured from several matrices, including blood, sputum, pus, ear secretions, pharyngeal swabs, and urine; the resulting isolates were stocked systematically at −80ºC. Five original stocked strains, SCVs-1–5, were derived from sputum, ear secretions, pharyngeal swab, sputum, and sputum, respectively. All strains were recovered from the frozen stocks by streaking to sheep blood agar plates. Following incubation for 24 hrs at 35ºC, the colonies were resuspended in xx medium to a density of approximately 0.5 adjusted McFarland units (corresponding to 1 x 106–1×108 cells/mL) as determined by a turbidity meter before streaking to the solid growth medium being tested. Characteristics of stocked SCV-MRSA were determined biochemically, genetically, and microbiologically by analysis of catalase, mannitol, and coagulase production; thymidine-dependency; presence of the pbp-2ʹ and mecA genes, and susceptibility to cefoxitin (CFX) and STX.
In addition, 36 clinical swabs including SCV-MRSA from patients also were cultured and tested for detection on various solid media at 24 and 48 hrs. Clinical samples were routinely identified by the growth of the bacteria on regular sheep agar plates; when we identified MRSA, especially in patients who had received SXT treatment, we streaked on all three of the tested solid media. This screening yielded a total of 36 clinical samples from which SCV-MRSA were isolated.
This study was approved by the Committee for Clinical Scientific Research of Tohoku Medical and Pharmaceutical University Hospital on July 30, 2017 (ID: 2017-2-030); all patients provided written informed consent for use of their specimens.
TOF-MS and its scoring
The identification of bacteria by MALDI-TOF MS also was performed serially in parallel with the phenotypic characterization described above. The MALDI-TOF MS was performed at the clinical laboratory of Tohoku Medical and Pharmaceutical University Hospital according to a standard protocol and using Bruker Daltonics equipment (Bremen, Germany).10,11 The positive colonies were simultaneously assessed for bacterial identification using conventional procedures, including MicroScan Walkaway panels (Beckman Coulter, Jersey City, NJ, USA), and complementary individual biochemical or enzymatic tests. Spectral scores of >1.700–1.999 and >2.000 indicated identification at the genus and species levels, respectively.
Agar plates
In addition to sheep agar plates, which are used regularly for bacterial isolation, we used three MRSA detection plates, including MS-CFX and X-MRSA (Nissui, Tokyo, Japan), and CHROMagar (Kanto-kagaku, Tokyo, Japan; originally from Becton Dickinson, Franklin Lakes, NJ, USA). The MRSA colonies were detected on the respective agar plates as yellow, blue, and red colonies. Additionally, we noted that while Corynebacterium species grew as white colonies and regular-MRSA grew as bigger colonies on these media, the resulting colonies could be distinguished from SCV-MRSA based on appearance (Corynebacterium were white) and on size (regular-MRSA were larger).
Results
Detection of SCV-MRSA from stocks using MS-CFX, chomagar, and X-MRSA plates
For this comparison of the MRSA detection plates, we prepared and re-cultured five SCV-MRSA strains from stocks (Table 1). All five of the stocked SCV-MRSA showed similar characteristics, including thymidine dependence, SXT resistance, biochemical reactions, and susceptibility to other antibiotics.
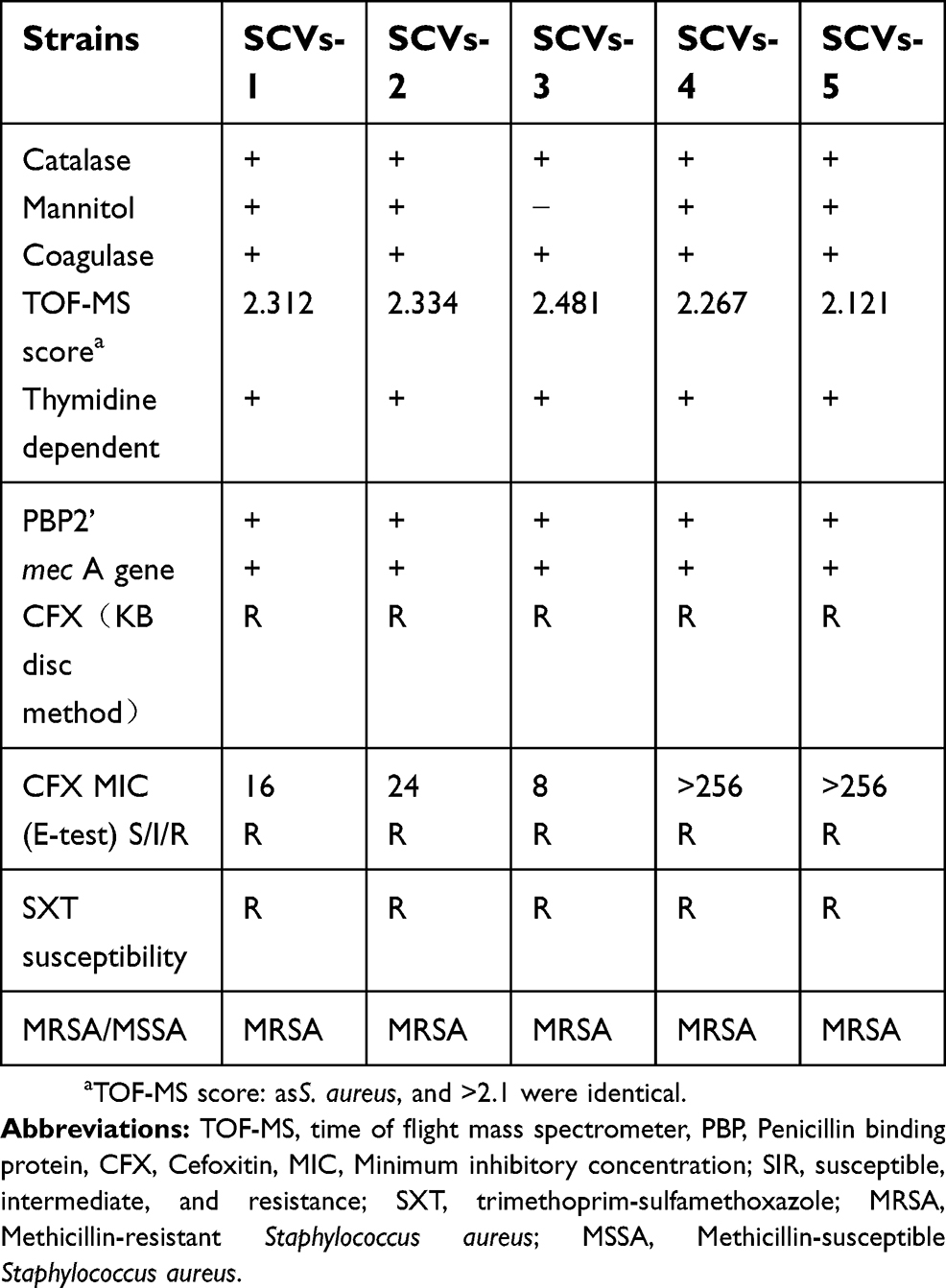 | Table 1 Characteristics of stocked SCV-MRSA strains |
These pure SCV-MRSA strains grew well and were detected easily after either 24 and 48 hrs on both X-MRSA and CHROMagar plates; in contrast, colonies of these pure SCV-MRSA strains were not readily detected on MS-CFX plates at either time point (Table 2). In the case of SCV-3, we observed smaller-than-expected MRSA colonies on the MS-CFX plates, and colony numbers were lower than those observed on regular sheep agar plates. Furthermore, larger numbers of colonies were detected more clearly on X-MRSA and CHROMagar than on MS-CFX plates (Figure 1).
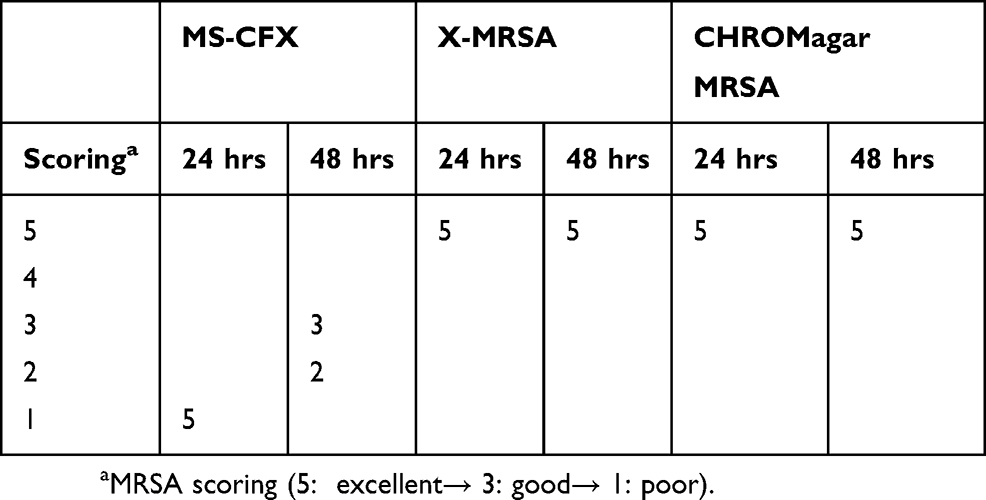 | Table 2 Evaluation of SCV-MRSA score of 5 stocked strains on each agar plate |
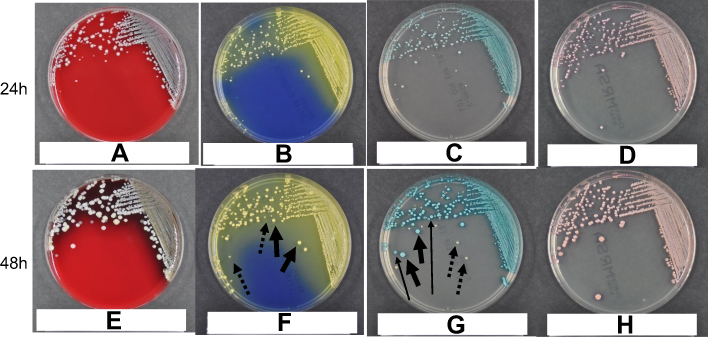
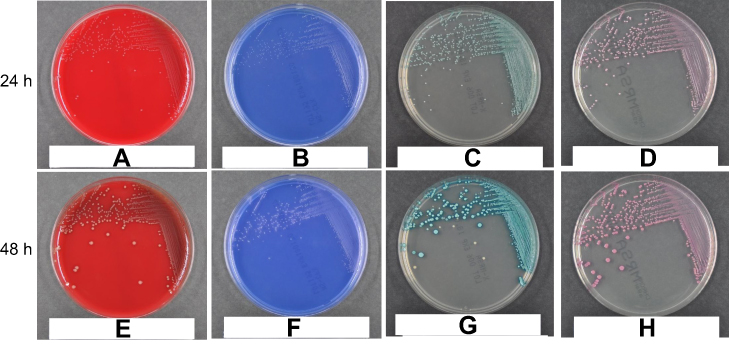 | Figure 1 Identification of SCV-MRSA from stocks after 24 (A–D) and 48 (E–H) hours of growth (respectively) on sheep agar plates (A and E), MS-CFX (B and F), X-MRSA (C and G), and CHROMagar (D and H). The results obtained with the SCV-3 strain (as shown in this figure) were representative of the results obtained with all five stocked SCV-MRSA strains. SCV-MRSA colonies were detected more easily on X-MRSA and CHROMagar plates than on MS-CFX plates. The regular sheep agar plates yielded colonies of sizes similar to those seen on X-MRSA and CHROMagar plates, but sheep agar did not permit distinction between regular- and SCV-MRSA. |
Detection of SCV-MRSA from clinical isolates using MS-CFX, X-MRSA, and chromagar plates
Most clinical isolates of SCV-MRSA were detected readily on X-MRSA plates. These clinical isolates also were detected readily on CHROMagar and MS-CFX, although some of these SCV-MRSA were not as easily observed after 48 hrs on CHROMagar and MS-CFX compared to X-MRSA at the same time point; notably, at 48 hrs on X-MRSA, these isolates showed growth exceeding grade 4 in all cases (Table 3).
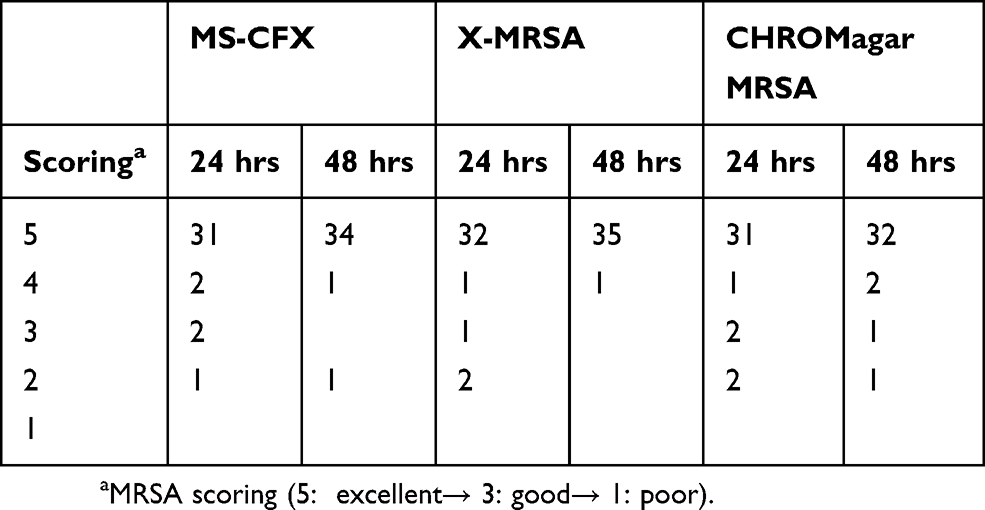 | Table 3 Evaluation of MRSA score of SCV-MRSA clinically isolated from 36 patients on each agar plate |
Representative SCV-MRSA detected in cases among 36 clinical swabs from the patients are shown in Figure 2. Case 4 corresponded to an 80-year-old male patient with rheumatoid arthritis; slow-growing colonies of SCV-MRSA from the sputum of this case were detected readily on X-MRSA, and we could distinguish SCV-from regular-MRSA and from Corynebacterium species based on colony size and color, respectively, after 48 hrs of culturing (Figure 2G). However, we were unable to distinguish between SCV-MRSA and the other similar bacterium, such as regular-MRSA and Corynebacterium species, when growing on CHROMagar plates for either 24 or 48 hrs (Figure 2D and H). SCV-MRSA colonies also might be detectable on MS-CFS plates at 48 hrs, but we observed only regular-MRSA and Corynebacterium species from this case when grown on this medium (Figure 2F). On sheep agar plates, over-growth and growth of contaminant colonies were observed at both 24 and 48 hrs (Figure 2A and E).
 | Figure 2 Identification of SCV-MRSA from clinical specimens of Patient 4 after 24 (A–D) and 48 (E–H) hours of growth on sheep agar plates (A and E), MS-CFX (B and F), X-MRSA (C and G), and CHROMagar (D and H). This SCV-MRSA strain was cultured from the sputum of an 80-year-old male. Thin and long arrows indicate the SCV-MRSA colonies. Thick arrows indicate regular-MRSA colonies, which were bigger and clearer than those of SCV-MRSA. Dotted arrows indicate colonies of Corynebacterium species; which were of similar size but whiter than those of SCV-MRSA. Such colonies were detected more readily on X-MRSA plates at 48 hrs than on the other three plate types at 24 or 48 hrs. |
Discussion
SCV-MRSA emerge as MRSA variants that persist in patients for months or years in a dormant metabolic state, sometimes appearing as fatal pathogens, as demonstrated by the isolation of SCV-MRSA not only from the sputum of CF patients, but also from bloodstream, urine, and pus of intraabdominal abscess.3–5 SCV-MRSA are defined based on their ability to grow on sheep blood agar as tiny, nonpigmented, and nonhemolytic colonies that show decreased metabolic activity.3 Such variants can be cultured only in the presence of distinct growth factors, including thymidine; therefore, MRSA-specific plates that can detect not only regular MRSA, but also SCV-MRSA, are necessary.
Recently, we have been employing several versions of MRSA-specific solid media, including MS-CFX, X-MRSA, and CHROMagar plates. In the present study, we evaluated and compared the SCV-MRSA detection efficiencies of these three plate types.7–9 Among the three types, X-MRSA plates showed very good detection ability, although CHROMagar also showed similar detection rates for stocked SCV-MRSA compared with MS-CFX plates. X-MRSA plates provided better detection of SCV-MRSA from clinical samples than did either CHROMagar or MS-CFX plates; this detection included that of isolates from the sputum of immunocompromised patients. These results suggested that there were some differences among the MRSA-specific plates in terms of SCV-MRSA detection, and that X-MRSA detected SCV-MRSA better than did the other two MRSA-specific plates. The use of these MRSA-specific plates, in addition to standard sheep agar plates, is expected to prevent the misdetection and/or delayed detection of SCV-MRSA.
The use of chromogenic media recently has become an important method for the rapid identification of microorganisms in clinical samples: these media permit the detection of the production of key microbial enzymes as diagnostic markers for pathogens by incorporating chromogenic substrates into a solid-agar-based matrix.7–9 In contrast to conventional culture media, chromogenic media allow direct colony-color-based identification of the pathogen in primary culture. This identification reduces the need for subculturing for further biochemical testing and genetic analysis (eg, PCR and Next-Generation Sequencing).12–17 These biochemical and genetic analyses are accurate and consistent, but the techniques typically are expensive and time-consuming, and may be still difficult to distinguish SCV- and regular-MRSA: Thus, direct colony-color-based identification of the pathogen from primary culture reduces the cost and time required for bacterial characterization.
However, recommended incubation times are usually 24 hrs, not 48 hrs; two days of culturing can result in overgrowth of MRSA and other contaminating bacteria, making it difficult to distinguish the MRSA colonies. Our data suggest that 48 hrs culturing might be better than 24 hrs incubation for detecting SCV-MRSA, consistent with the results of previous reports.7,8 Further studies in both basic and clinical microbiology will be needed to address the extension of incubation time with MRSA to permit the efficient detection of SCV-MRSA.
In conclusion, we compared the efficiency of SCV-MRSA detection on three types of MRSA-specific solid media. We tested both stocked SCV-MRSA strains and isolates from primary clinical samples, and found that X-MRSA plates might be better than MS-CFX and CHROMagar plates for SCV-MRSA detection. Extending the incubation time (from 24 to 48 hrs) also might be needed to facilitate SCV-MRSA detection.
Acknowledgments
This work was supported by a Grant-in-Aid for Scientific Research (17K09623 to MS) from the Japanese Society for the Promotion of Science.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Song JH, Hseuh PR, Chung DR, et al. Spread of methicillin-resistant Staphylococcus aureus between the community and the hospitals in Asian countries: an ANSORP study. J Antimicrob Chemother. 2011;66:1061–1069. doi:10.1093/jac/dkr024
2. Isobe M, Uejima E, Seki M, et al. Methicillin-resistant Staphylococcus aureus bacteremia at a university hospital in Japan. J Infect Chemother. 2012;18:841–848. doi:10.1007/s10156-012-0423-6
3. Proctor RA, von Eiff C, Kahl BC, et al. Small colony variants: a pathogenic form of bacteria that facilitates persistent and recurrent infections. Nat Rev Microbiol. 2006;4:295–305. doi:10.1038/nrmicro1384
4. Besier S, Zander J, Siegel E, et al. Thymidine-dependent Staphylococcus aureus small-colony variants: human pathogens that are relevant not only in cases of cystic fibrosis lung disease. J Clin Microbiol. 2008;46:3829–3832. doi:10.1128/JCM.01440-08
5. Besier S, Zander J, Kahl BC, Kraiczy P, Brade V, Wichelhaus TA. The thymidine-dependent small-colony-variant phenotype is associated with hypermutability and antibiotic resistance in clinical Staphylococcus aureus isolates. Antimicrob Agents Chemother. 2008;52:2183–2189. doi:10.1128/AAC.01395-07
6. Kriegeskorte A, Lorè NI, Bragonzi A, et al. Thymidine-dependent staphylococcus aureus small-colony variants are induced by Trimethoprim-Sulfamethoxazole (SXT) and have increased fitness during SXT challenge. Antimicrob Agents Chemother. 2015;59:7265–7272. doi:10.1128/AAC.00742-15
7. Malhotra-Kumar S, Abrahantes JC, Sabiiti W, et al. Evaluation of chromogenic media for detection of methicillin-resistant Staphylococcus aureus. J Clin Microbiol. 2010;48:1040–1046. doi:10.1128/JCM.01745-09
8. Peterson JF, Dionisio AA, Riebe KM, et al. Alternative use for spectra MRSA chromogenic agar in detection of methicillin-resistant Staphylococcus aureus from positive blood cultures. J Clin Microbio. 2010;48:2265–2267. doi:10.1128/JCM.00674-10
9. Verkade E, Elberts S, Verhulst C, Kluytmans J. Performance of Oxoid Brilliance MRSA medium for detection of methicillin-resistant Staphylococcus aureus: an in vitro study. Eur J Clin Microbiol Infect Dis. 2009;28:1443–1446. doi:10.1007/s10096-009-0802-9
10. Hariu M, Watanabe Y, Oikawa N, Seki M. Usefulness of matrix-assisted laser desorption ionization time-of-flight mass spectrometry to identify pathogens, including polymicrobial samples, directly from blood culture broths. Infect Drug Resist. 2017;10:115–120. doi:10.2147/IDR.S132931
11. Hariu M, Watanabe Y, Oikawa N, Manaka T, Seki M. Evaluation of blood culture broths with lysis buffer to directly identify specific pathogens by matrix-assisted laser desorption/ionization time-of-flight mass spectrometry methods. Infect Drug Resist. 2018;11:1573–1579. doi:10.2147/IDR.S169197
12. Seki M, Takahashi H, Yamamoto N, et al. Polymerase chain reaction-based active surveillance of MRSA in emergency department patients. Infect Drug Resist. 2015;14:113–118. doi:10.2147/IDR.S80123
13. Takahashi H, Seki M, Yamamoto N, et al. Validation of a phage-open reading frame typing kit for rapid identification of methicillin-resistant Staphylococcus aureus (MRSA) transmission in a tertiary hospital. Infect Drug Resist. 2015;14:107–111.
14. Bischof LJ, Lapsley L, Fontecchio K, et al. Comparison of chromogenic media to BD GeneOhm methicillin-resistant Staphylococcus aureus (MRSA) PCR for detection of MRSA in nasal swabs. J Clin Microbiol. 2009;47:2281–2283. doi:10.1128/JCM.02256-08
15. Seki M, Gotoh K, Nakamura S, et al. Fatal sepsis caused by an unusual Klebsiella species that was misidentified by an automated identification system. J Med Microbiol. 2013;62:801–803. doi:10.1099/jmm.0.051334-0
16. Seki M, Yoshida H, Gotoh K, et al. Severe respiratory failure due to co-infection with human metapneumovirus and Streptococcus pneumoniae. Respir Med Case Rep. 2014;15:13–15.
17. Seki M, Ohno H, Gotoh K, et al. Allergic bronchopulmonary mycosis due to co-infection with Aspergillus fumigatus and Schizophyllum commune. IDCases. 2014;1:5–8. doi:10.1016/j.idcr.2014.01.001
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.