")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 17
Evaluating the Prognostic Role of Monocytopenia in Chemotherapy-Induced Febrile Neutropenia Patients Treated with Granulocyte Colony-Stimulating Factor
Authors Alshari O , Al Zu’bi YO, Al Sharie AH, Wafai FH, Aleshawi AJ, Atawneh FH, Obeidat HA, Daoud MN, Khrais MZ, Albals D, Tubaishat F
Received 5 May 2021
Accepted for publication 21 July 2021
Published 7 September 2021 Volume 2021:17 Pages 963—973
DOI https://doi.org/10.2147/TCRM.S318370
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Osama Alshari,1 Yazan O Al Zu’bi,2 Ahmed H Al Sharie,2 Farouk H Wafai,2 Abdelwahab J Aleshawi,2 Farah H Atawneh,3 Hasan A Obeidat,2 Majd N Daoud,2 Mohammad Z Khrais,4 Dima Albals,5 Faize Tubaishat6
1Division of Oncology, Department of Internal Medicine, Faculty of Medicine, Jordan University of Science & Technology, Irbid, Jordan; 2Faculty of Medicine, Jordan University of Science & Technology, Irbid, Jordan; 3Department of Medical Laboratory Sciences, Faculty of Applied Medical Sciences, Jordan University of Science and Technology, Irbid, Jordan; 4Department of Internal Medicine, King Hussein Cancer Foundation and Center, Amman, Jordan; 5Department of Medicinal Chemistry and Pharmacognosy, Faculty of Pharmacy, Yarmouk University, Irbid, Jordan; 6Division of Oncology, Department of Internal Medicine, Al Bashir Hospital, Amman, Jordan
Correspondence: Osama Alshari
Division of Oncology, Department of Internal Medicine, Faculty of Medicine, University of Science & Technology, P. O. Box: 3030, Irbid, 22110, Jordan
Email [email protected]
Objective: Chemotherapy-induced febrile neutropenia is a common and serious oncological emergency which carries a substantial mortality and morbidity. The main objective of this study is to evaluate the usage of absolute monocyte count (AMC) at presentation as a prognostic factor for patients with chemotherapy-induced febrile neutropenia who were subsequently treated with granulocyte colony-stimulating factor (G-CSF).
Study Design: The electronic medical records of our center were used retrospectively to identify patients diagnosed with unprecedented chemotherapy-induced febrile neutropenia treated with G-CSF between January 2010 to December 2020 and diagnosed with solid and hematological malignancies. Patient’s demographics, disease characteristics and laboratory investigations were extracted. Disease progression measures were statistically compared between the study groups in the short-term period of follow-up (six days) including absolute neutrophil count (ANC), ANC difference compared to the baseline readings, hospitalization period, and mortality.
Results: A total of 80 patients were identified and categorized into two groups namely monocytopenia (n = 34) and non-monocytopenia (n = 46) with an AMC cutoff point of 0.1× 109 cells/L. The monocytopenia group exhibited a worse prognosis with lower ANC values and slower improvement illustrated by the low ANC difference values at all follow up points (P-value ≤ 0.05) apart from day 5. A statistically significant lower hospitalization period was also observed in the non-monocytopenia group (P-value = 0.006). Linear regression analysis evaluated the association between AMC values at admission and ANC values at admission along with subsequent days of follow up which were found to be statistically significant (P-value ≤ 0.05). Receiver operating characteristic curves suggest a satisfactory predictability of ANC changes by AMC values at admission, days1, 2, 3, 4 and 6.
Conclusion: Monocytopenia holds a worse prognosis in chemotherapy-induced febrile neutropenia patients treated with G-CSF. In addition, AMC values at presentation represents a potential risk factor that can predict short-term changes regarding ANC measures.
Keywords: febrile neutropenia, granulocyte colony-stimulating factor, G-CSF, chemotherapy, absolute monocyte count, monocytopenia, absolute neutrophil count
Introduction
Febrile Neutropenia is a major and critical complication of chemotherapy provided for cancer patients, ensuring a tremendous impact on healthcare resources and patients’ outcomes.1 Neutropenia is defined by the American Society of Clinical Oncology (ASCO) and Infectious Diseases Society of America (IDSA) joint guideline as an absolute neutrophil count (ANC) of less than 1000 cells/µL. Moreover, fever in neutropenic patients has been defined as a single oral temperature of ≥ 38.3°C or a temperature of ≥ 38.0°C persisting over 1 hour.2 A consistent definition is also provided by the European Society for Medical Oncology (ESMO) clinical practice guidelines, in which febrile neutropenia is defined as an oral temperature of more than 38.3°C or two consecutive readings of more than 38.0°C for two hours and an ANC of less than 0.5 × 109/L or expected to fall below it.3
Various pathophysiological pathways have been hypothesized previously to determine the probable cause of fever in neutropenic patients. To begin with, it has been regarded to the cytokines release by the immune cells and stromal cells in response to microorganisms and molecular motifs.4 Furthermore, a reduction in anti-inflammatory molecules such as interleukin-10 (IL-10), antimicrobial peptides such as interleukin-1 (IL-1) receptor antagonists would prevent the physiological feedback inhibition of inflammation, intensifying the damage.4 An elevation in uric acid levels may have a role as well, amplifying the response of innate immune cells to microbial stimulation by elevating the proinflammatory cytokines; tumor necrosis factor-alpha (TNF-α) and interleukin-1 alpha (IL-1α).5 A vast amount of evidence regards fever to be a consequence of infection since patients are at a higher risk, albeit the lack of microbiological evidence in certain cases.6 Fever of unidentified origin was observed in almost 40% of neutropenic patients.7 A potential reason behind such phenomena can be justified by the release of danger-associated molecular patterns (DAMPs) because of mucosal barrier injury due to the cytotoxic effects of chemotherapeutic agents, which along with the pathogen-associated molecular patterns (PAMPs) eventually results in a substantial inflammatory response provoking fever.4
The consequences of febrile neutropenia remain a source of concern that cannot be disregarded with major complications effecting the patient’s treatment outcomes, cost, morbidity, and mortality, yet, variations exist due to the cancer type and stage, its treatment, and patient’s demographics.20 The economic burden is considerable with the costs going from $16,000 to $19,000 for the extraordinary greater part of patients being hospitalized, in which they require a prolonged hospitalization care period, which might end with the patient’s death.8,9 Additionally, febrile neutropenia patients are 50% more likely to have an infection with 20% of the patients having bacteremia. The most common sights infected being the lungs, the gastrointestinal tract, and the skin.22 The most common pathogens isolated were gram negative organisms Escherichia coli, Pseudomonas aeruginosa and Klebsiella pneumoniae. However, the trend is changing with the predominance of gram-positive organisms such as methicillin-resistant Staphylococcus aureus (MRSA), as well as a rise of fungal infections, in particular Candida.10 Therefore, the cornerstone of treatment for febrile neutropenic patients are antibiotics. Low risk patients are indicated oral antibiotics with fluoroquinolone as a primary treatment, which can be given in an outpatient setting even though patients should be cautiously chosen with attentive monitoring for any emergency if one occurs. In comparison, high risk patients are admitted with an intravenous (IV) antibiotics treatment plan including antipseudomonal beta-lactam agents.1 It is recommended that all patients are continued on antibiotics until the patient is afebrile for at least 48 hours with an ANC exceeding 500 cells/mm3.1,11 Nonetheless, if the patient does not improve, antimicrobial coverage ought to be expanded to cover resistant gram negative, gram positive, anaerobic microorganisms, and fungi.11
Notwithstanding anti-microbials, colony stimulating factors might be an essential part of a treatment plan. Evidence from existing literature has proven the favorable effects of colony stimulating factors in reducing the hospitalization and IV antibiotics administration periods.12 Even though G-CSF does not reduce mortality in chemotherapy induced febrile neutropenia, it has been found that G-CSF added to antibiotics reduces the hospitalization period, antibiotic use, fever, neutropenia, and recovery of the neutrophils number duration.13,14 Since a growing body of research suggests that the clinical course of neutropenic patients could be predicted by the usage of monocyte measures as monocyte percentage (MP) and absolute monocyte count (AMC). In this work, we hypothesized and tested the idea suggesting that the AMC could predict the clinical responsiveness of G-CSF therapy in febrile neutropenia patients without any age, gender, chemotherapy regimen or malignancy restrictions.
Patients and Methods
Patients and Data Collection
The aim of this study is to evaluate the utilization of AMC at presentation as a prognostic factor for patients with chemotherapy-induced febrile neutropenia and subsequently treated with G-CSF. Data was collected from King Abdullah University Hospital (KAUH), a tertiary care center located in Ar Ramtha, Jordan. We retrospectively identified patients diagnosed with chemotherapy-induced febrile neutropenia for the first time and treated with G-CSF according to the current hospital guidelines between January 2010 to December 2020. The hospital electronic medical records were used to extract the following data including demographics, type of malignancy (solid tumors versus hematological malignancies), distant metastasis, bone marrow involvement, chemotherapeutic regimens and its current cycle, temperature at admission, clinical presentation, comorbidities, blood culture results, number of febrile neutropenia attacks, hospitalization period and mortality. Complete blood count (CBC) and the white blood cells (WBC) differential were also extracted at different time intervals representing the short-term progression or improvement after admission and treatment with G-CSF including day 1 to 6. After day 6, a minority of patients possessed a laboratory follow up results impairing the statistical judgment due to low statistical power, hence they were excluded from the analysis.
A total of 80 patients were enrolled. Exclusion criteria included patients missing key data such as CBC and WBC differential at presentation with no follow up laboratory results, patients did not get G-CSF therapy, non-malignant cases which developed febrile neutropenia including Chediak-Higashi syndrome, aplastic anemia, acquired immunodeficiency syndrome (AIDS), neutropenia, cyclical neutropenia, alcoholic liver cirrhosis and a severe malnutrition case. The first attack was only included in the analysis for patients who developed multiple febrile neutropenia attacks, to eliminate the personalized response bias. Patients were then categorized based on AMC values into two groups namely monocytopenia group (n = 34) and a non-monocytopenia group (n = 46) with a cutoff point of 0.1×109 cells/L as previously described.15–19 ANC and ANC differences at each follow up interval compared to ANC at admission were calculated. This study was conducted in accordance with the declaration of Helsinki, applying all the current regulations for retrospective studies in KAUH. Patient’s consent was waived as data was used in aggregate anonymously.
Statistical Analysis
Statistical analysis was performed using the IBM SPSS statistical package for Windows v.26 (Armonk, NY, USA). Data was expressed as frequency (percentage) for nominal data, mean ± standard deviation of the mean (SD) for normally distributed continuous variables or median (Interquartile range) for non-normally distributed continuous variables. Normality was tested using Shapiro–Wilk test. Statistical significance between the study groups regarding the previously mentioned parameters was determined using Chi-square test or Fisher’s exact test, likelihood ratio accordingly, for categorical variables and Mann–Whitney U-test for non-normally distributed continuous variables and independent t-test for normally distributed continuous variables. P ≤ 0.05 was considered statistically significant.
A simple linear regression was used to assess the direction and strength of the relationship between the AMC at admission and the ANC at admission and different time intervals of follow up (day 1–6). The data was transformed using the natural logarithm (ln) since the data was skewed to the right. The sensitivity and specificity of AMC values as a predictor variable for the ANC change at different time intervals was assessed using the receiver operating characteristic (ROC) curves. The ANC change at different time intervals was dichotomized into a binary system (1 for an increase and 0 for a decrease or no-change compared to reported admission ANC value) as previously described.20 ROC parameters were calculated including the area under the curve (AUC) and the cut-off point which indicates the point of the maximum sensitivity and specificity. The Kaplan–Meier analysis was used to calculate the probability of a second attack and the probability of survival as a function of time. Second attack and death were coded a value of 1. While patients who lived or did not develop a second attack during the period of data collection were assigned as 0. Statistical significance between Kaplan–Meier curves were tested using the Log rank test. Graphs were generated using GraphPad Prism 8 (San Diego, CA, USA).
Results
A total of 80 patients were enrolled in the analysis, ranging in age from 1 to 78 years-old, who were admitted to the hospital for a febrile neutropenia attack (47.5% males and 52.5% females). According to the AMC values at admission, patients were divided into two subgroups; 34 patients (42.5%) were included in the monocytopenia group, while the non-monocytopenia group included 46 patients (57.5%). According to the type of malignancy 36 patients (45%) had a hematological malignancy in which Hodgkin’s lymphoma, non-Hodgkin’s lymphoma and diffuse large B-cell lymphoma were the highest three occurring malignancies, on the other hand, breast cancer, neuroblastoma and Ewing’s sarcoma were the most occurring solid malignancies (55%, n = 44). Of the 80 patients included, 12 had a bone marrow involvement, in addition to 17 patients (21.3%) who had a distant metastasis. Patient’s chemotherapy regimens varied, with R-CHOP (15%), ABVD (6.3%), AC (6.3%), VCD (5%), and ICE (5%) being the most used protocols (Supplementary data, Table S1), with a median of 3.00 (3.00) prior cycles of treatment. Additionally, most patients presented with fever solely in both monocytopenia (61.8%, n = 21) and non-monocytopenia (54.3%, n = 25) groups, succeeded by fever with cough (12.5%, n = 10) and fever with general weakness (7.5%, n = 6) respectively. At the time of admission, the patients’s temperatures ranged between 38°C and 41°C. Principally, patients were free of any co-morbidity, apart from 21 patients who had one or more co-morbidities, with diabetes mellitus and hypertension being the dominant observations. In 10 patients, there was an obvious indication of a microbiologically defined infection, with five having a positive blood culture, four having a positive urine culture, and only one having a positive sputum culture (Supplementary data, Table S2). No statistically significant difference was observed amidst demographics and baseline characteristics, apart from gender (P-value = 0.049) when comparing the mentioned subgroups (Table 1).
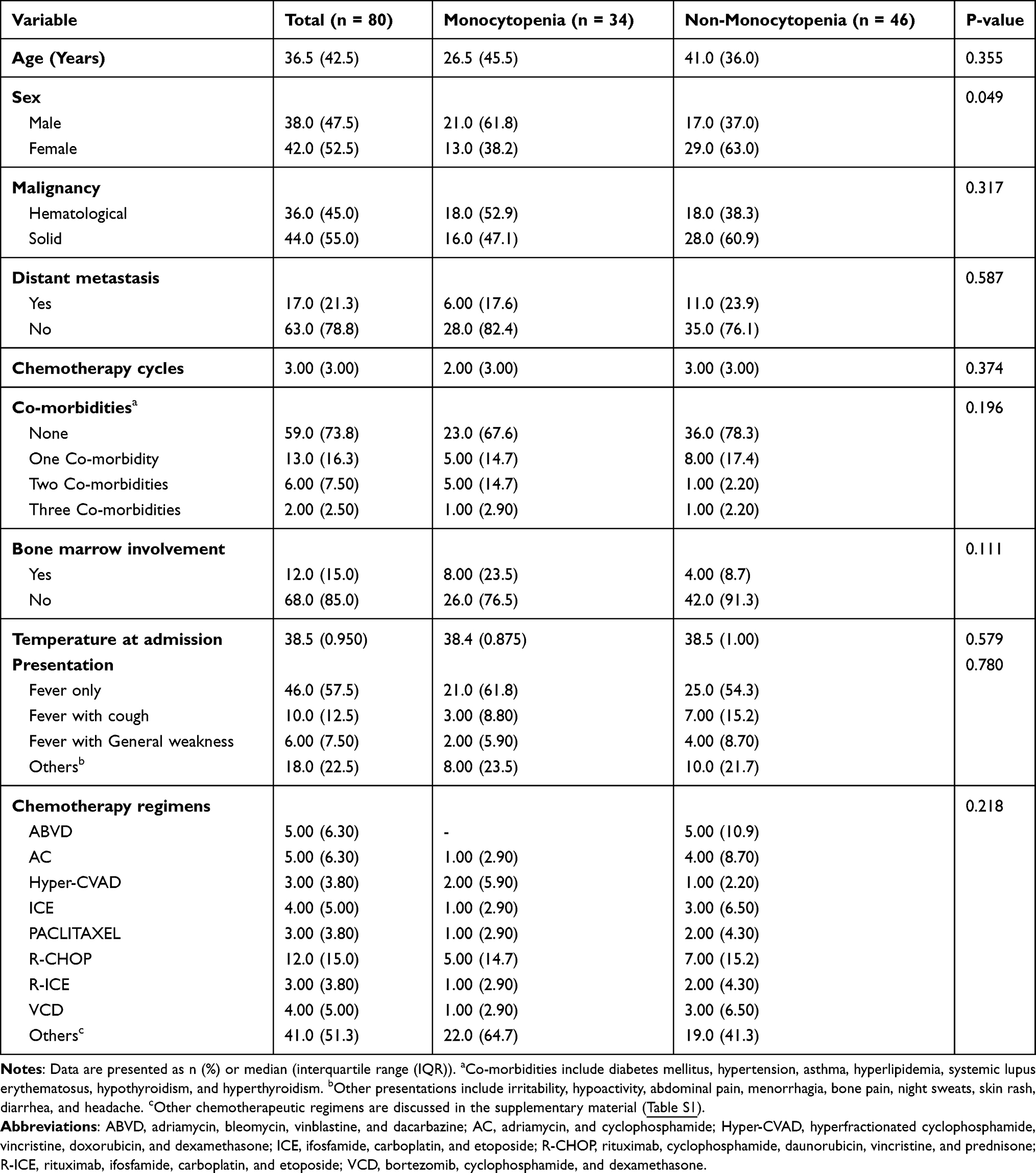 |
Table 1 Patient’s Demographics, Malignancy Characteristics and Chemotherapy Regimens of the Selected Population |
The CBC parameters alongside the WBC differential values were obtained at admission and at different follow up time intervals up to 6 days following the attack. Statistical significance was calculated between the study groups regarding the previously mentioned parameters (Supplementary data, Table S3–S9). At admission, no significance was highlighted between both groups except for baseline WBCs count (P-value < 0.001), red cell distribution width (RDW) (P-value = 0.026), platelets count (P-value = 0.016), lymphocytes (P-value < 0.001) and basophils (P-value = 0.041). WBCs count illustrated a significant difference at all the observational readings apart from day five, in which the non-monocytopenia group exhibited a better prognosis presented by a higher WBCs count at follow ups. The same trend was also seen in the neutrophil’s percentage and ANC values, emphasizing the importance of monocytopenia in determining the improvement degree of febrile neutropenia patients after G-CSF therapy. The statistically significant difference observed regarding other CBC parameters and WBC differential values at different follow ups will not be discussed since they are totally not germane. But such analysis was performed to explore the possible concurrent significant variables that could be optimized and utilized as predictive measures for future work as in the case of lymphocyte percentage. Additional measures including liver and kidney function tests were also shown for both groups (Supplementary data, Table S10 and S11).
The main prognostic outcomes included in the analysis were WBCs count, neutrophils percentage, ANC, ANC difference at different follow up time intervals, and the hospitalization period. ANC difference represent the degree of improvement calculated by the mathematical difference in ANC at a specific follow up point compared to the baseline reading. Albeit the lack of significance identified in neutrophils percentage and ANC at admission, they have showed to be significant at all the follow up intervals as illustrated in Table 2. Figure 1 illustrates a visual representation of the ANC values at admission and different follow up intervals regarding the monocytopenia and non-monocytopenia groups, which shows a preferred prognostic path displayed by the non-monocytopenia group with a curve up shift to a higher ANC values, thus a better response to G-CSF treatment. ANC difference was also significant at all the follow up observations. Initially, on day one (P-value = 0.006) and subsequently progressing through the consecutive days, day two (P-value < 0.001), day three (P-value < 0.001), day four (P-value = 0.001), and day six (P-value = 0.019), except day five with P-value of 0.056. The hospitalization period of patients within the monocytopenia group was 6.0 (2.25) which was higher compared to the non-monocytopenia group which was 5.0 (3.00) (P-value = 0.006).
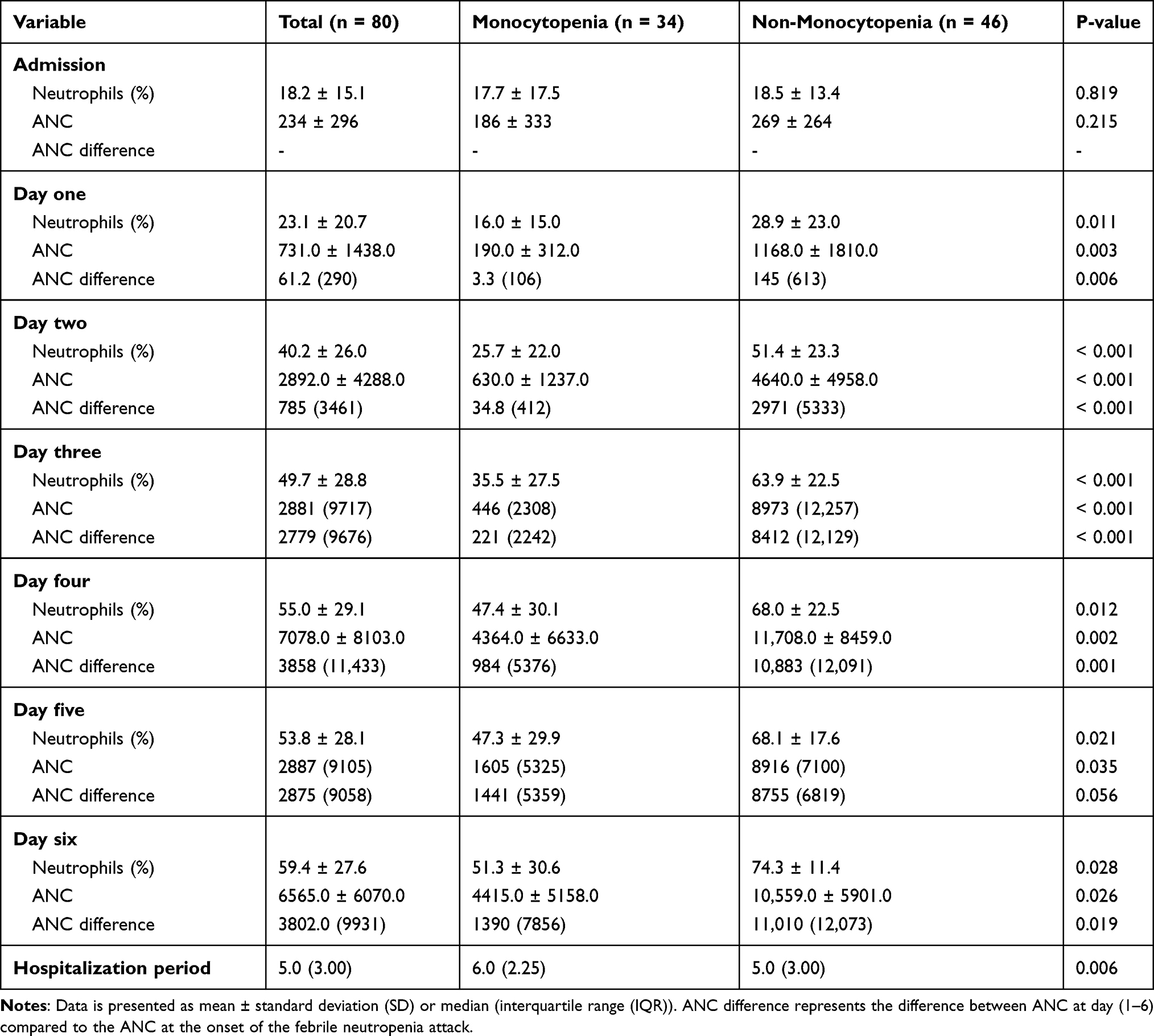 |
Table 2 Neutrophil Percentage, Absolute Neutrophil Count, and Absolute Neutrophil Count Difference at Several Days Following the Febrile Neutropenia Attack Treated with G-CSF |
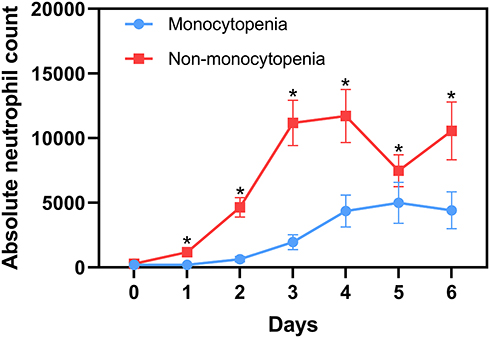 |
Figure 1 The short-term progression of patients with chemotherapy-induced febrile neutropenia (n=80) and subsequently treated with G-CSF illustrated by the daily change in ANC values. Patients were categorized into two groups namely monocytopenia (n=34) and non-monocytopenia (n=46) groups with a cutoff point of 0.1×109 cells/L. Data points are presented as mean ± standard error of the mean (SEM). *P-value ≤ 0.05. |
As a result of the different hospitalization periods, 67 patients were tested on the first day of follow up, 78 in the second, 64 on the third, 46 on the fourth, 32 on the fifth, and only 20 on the sixth day out of the 80 patients included in the present study which subsequently conducted a CBC test on the day of admission. To evaluate the relationship between AMC values at admission and ANC at different time intervals, linear regression analysis was utilized to further examine this relationship, since ANC difference at different time intervals exhibited a significant difference between monocytopenia and non-monocytopenia groups. The AMC values at admission were found to have a significantly positive relationship with ANC levels at various time intervals (Figure 2). A significant linear equation was found for day one (F (1,65) = 43.943, P-value < 0.001, R2 = 0.403) (β =0.736, P-value < 0.001), day two (F (1,76) = 112.744, P-value < 0.001, R2 = 0.597) (β =1.049, P-value < 0.001), day three (F (1,62) = 60.157, P-value < 0.001, R2 = 0.492) (β =0.964, P-value < 0.001), day four (F (1,44) = 21.441, P-value < 0.001, R2 = 0.328) (β =0.786, P-value < 0.001), day five (F (1,30) = 7.909, P-value = 0.009, R2 = 0.209) (β =0.511, P-value = 0.009) and finally, day six (F (1,18) = 12.969, P-value = 0.002, R2 = 0.647) (β =0.799, P-value = 0.002).
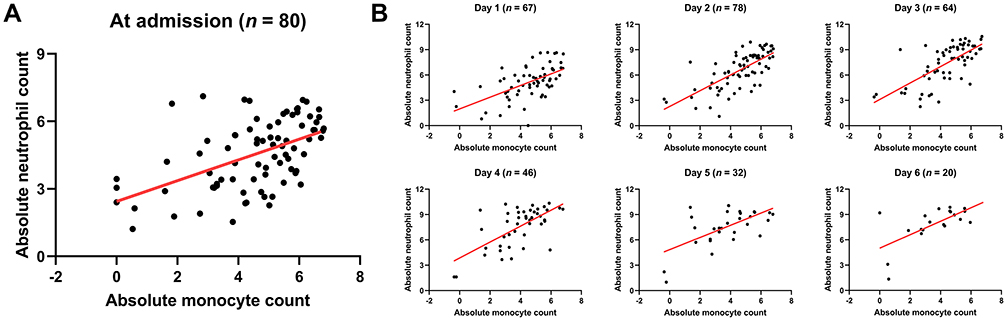 |
Figure 2 Linear regression analysis evaluated the association between AMC values at admission and ANC values at admission (A) and subsequent follow up days (B). AMC and ANC values were transformed using the natural logarithm (ln). |
ROC analysis was used to evaluate the predictive role of AMC at admission regarding the ANC improvement after G-CSF therapy at different time intervals (Figure 3). A cutoff value of 107 for ANC difference at day one yielded a sensitivity of 63.6% and a specificity of 65.2%, with an AUC of 0.625. At the second day, a cutoff value of 103 for ANC difference yielded a sensitivity of 61.9% and a specificity of 73.3%, with an AUC of 0.705. At the third day, a cutoff value of 67.0 yielded a sensitivity of 64.3% and a specificity of 87.5%, with an AUC of 0.752. At the fourth day, a cutoff value of 17.4 yielded a sensitivity of 80.5% and a specificity of 60.0%, with an AUC of 0.634. At the fifth day, a cutoff value of 17.4 yielded a sensitivity of 67.9% and a specificity of 50.0%, with an AUC of 0.518. Finally, at the sixth day, a cutoff value of 3.2 yielded a sensitivity of 89.5% and a specificity of 100%, with an AUC of 0.895.
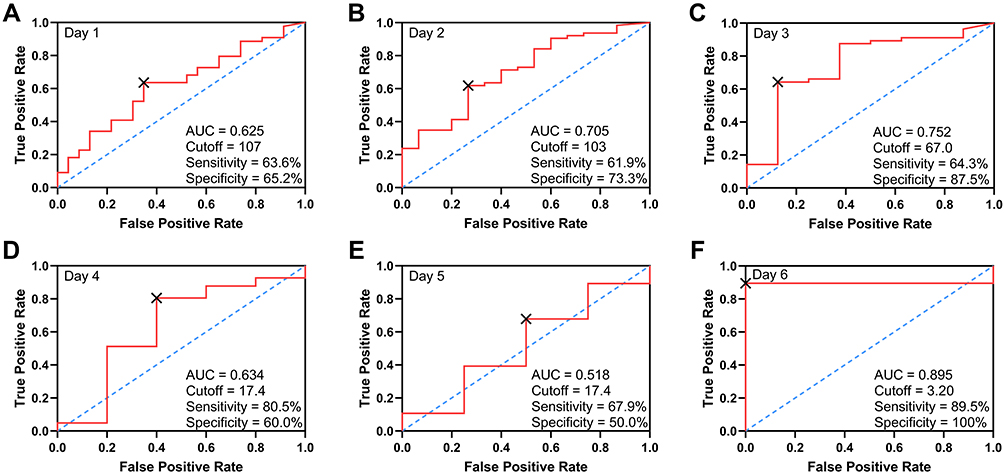 |
Figure 3 Receiver operating characteristic (ROC) curves of the AMC values at admission for prediction of ANC changes at day 1 to 6 (A-F). |
Kaplan–Meier estimator was used to assess the role of monocytopenia at the first attack in the recurrence probability of a second febrile neutropenia incidence. A total of 32 patients developed a second attack during the retrospective study period with 16 patients in each group. The Log rank test revealed no statistically significant difference between the monocytopenia and non- monocytopenia groups with P-value of 0.297 (Figure 4A). The same analysis was also applied to patients’s mortality rates. In which 19 deaths in both groups, 8 in the non-monocytopenia group and 11 in the monocytopenia group with no statistically significant difference (P-value = 0.198) as presented in Figure 4B.
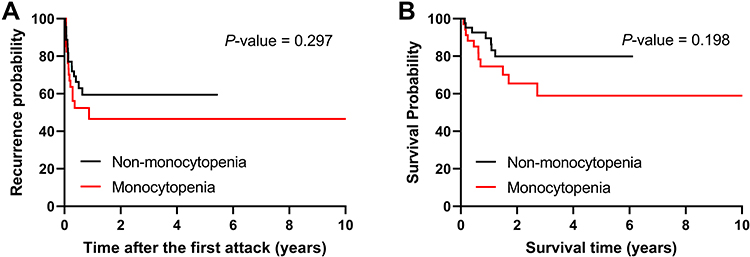 |
Figure 4 Kaplan–Meier curves to assess the role of monocytopenia in determining the recurrence (A) and survival (B) probability. |
Discussion
Chemotherapy-induced febrile neutropenia is a common and serious oncological emergency which develops in about 1% of patients undergoing a chemotherapeutic regimen and can reach up to 18% in the case of myelosuppressive agents’ usage.21–23 Certain patients have been identified to have a greater risk of developing febrile neutropenia, the components effecting such probability are treatment protocols, type of malignancy, and patient’s demographics and characteristics.24 Age has been identified as one of the risk factors for patients with non-Hodgkin lymphoma, in which it was noteworthy in patients older than 65 years.25–27 Female sex has been perceived as a potential risk factor in small-cell lung cancer patients who were more likely to be hospitalized, nevertheless sex was not identified as a significant risk factor in most studies.27,28 Multiple comorbidities have also been recognized as risk factors of developing febrile neutropenia including cardiovascular and renal diseases. All things considered, the number of comorbidities present concurrently with a malignancy type contribute to the hospitalization and mortality in neutropenic hospitalized patients.24 Certain chemotherapeutic agents are more prescient in inducing neutropenia including anthracyclines, vinorelbine, alkylators, taxanes, gemcitabine and topoisomerase inhibitors. In addition to the history of previous chemotherapy cycles and admission of three or more agents, notwithstanding the tumor type and stage.24 Genetic related risk factors including TP53 R72P and MDM2 SNP309, GSTM1 and UGTIA1 genotypes in patients treated by the FEC (fluorouracil + epirubicin + cyclophosphamide), FOLFOX (fluorouracil + oxaliplatin) and IROX (irinotecan + oxaliplatin) chemotherapy protocols respectively.29,30
As a result of the wide variation of risk factors, multiple risk indices have been developed including the Multinational Association for Supportive Care in Cancer (MASCC) and the Clinical Index of Stable Febrile Neutropenia (CISNE) guiding the clinical decision process. The MASCC index, which is now being widely used, was developed to identify patients with a lower risk of developing serious complications having a score of more than or equal to 21.1,31 Those patients are eligible for oral antibiotics treatment in the outpatient setting if being stable after 24 hours of monitoring.16 On the other hand, the CISNE index is a promising prognostic tool which divides patients into three categories depending on six variables including low (0 points), intermediate (1–2 points), and high risk (3 points or more) patients for predicting critical complications in patients with solid tumors and stable episodes of febrile neutropenia.32 More recent evidence reveals that CISNE index can be more accurate and predictive than the MASCC score.33,34
A growing body of literature has been devoted to study the correlation between monocytes measures and neutropenia in several clinical settings. In a retrospective clinical study conducted by Moriyama et al, the utilization of monocyte nadir has been investigated as a clinical indicator for neutrophil nadir in patients with lung cancer who developed chemotherapy induced neutropenia. A strong correlation between ANC nadir and AMC nadir has been observed, which potentiates the role of AMC nadir in the prediction of ANC nadir and its timing.35 In another similar study, Shimanuki et al have investigated the use of pre-treatment hematological laboratory parameters to construct a prediction model for chemotherapy induced febrile neutropenia in patients with head and neck squamous cell carcinoma. The model has revealed that AMC values less than 370cells/ mm3 are a good predictor for TPF (Docetaxel, cisplatin, and fluorouracil) regimen induced febrile neutropenia.36 Sato et al have studied the use of pre-treatment monocytes percentage in the prediction of docetaxel monotherapy induced neutropenia in patients suffering from several types of malignancies. The study has demonstrated an inverse correlation between monocytes percentage and neutrophil count decrease in G-CSF administration and non‑treated groups.37 Adding to this, Ouyang et al have demonstrated that monocytes and neutrophils count change possess the same time-wise trend in patients who developed chemotherapy induced neutropenia. In the same study, monocytes nadir occurred before neutrophil nadir with an inverse correlation between neutrophil decrease value and monocyte baseline percentage.38 Furthermore, a baseline monocyte count less than 150 cells per µL has been established as a bad prognostic variable in chemotherapy induced febrile neutropenia patients along with chemotherapeutic protocol, underlying malignancy, body surface area of less than or equal to 2 m2 and bone marrow involvement.39 In a retrospective study conducted among 62 patients with chemotherapy-induced febrile neutropenia, AMC and MP were evaluated for their short-term prognostic role regarding ANC changes, which revealed that MP can predict ANC changes with a cutoff point of 6.5% elucidating a sensitivity and specificity of 80 and 88.6% respectively and an AUC value of 0.908.20 Finally, multiple reports suggests that monocyte measures could have a predictive role in the clinical prognostic parameters of chemotherapy-induced febrile neutropenia.40,41
The exact pathophysiological mechanism that links AMC to ANC in the case of febrile neutropenia is not well understood or studied, which indicates the need to explore the cellular and molecular interactions in such clinical setting. The counter effects neutrophils and monocytes exhibit could be explained by hematopoiesis since they share a common progenitor namely “granulocyte-monocyte progenitor”. The differentiation route of neutrophils depends on the expression of C/EBP-ε and Gfi-1 followed GATA-1 down expression, while C/EBP-α and PU.1 induce monocyte and macrophage generation.42 In addition, human adherent monocytes have experimentally illustrated a synthetic capability of hematopoiesis modulators such as G-CSF and GM-CSF.43 G-CSF is the main granulopoietic cytokine involved in neutrophil production and mobilization, it increases the survival of neutrophils, influences its function in infection sites and sensitize them to chemotactic factors.44,45 On the other hand, GM-CSF mediates neutrophil progenitor’s proliferation and growth, other functionalities include its effect on mature neutrophils and the synergistic role with growth factors it exhibits.46,47 Monocytes even cause G-CSF driven mobilization of hematopoietic stem cells.44 So clinically speaking, a high monocyte count could result in partially higher concentration of these mediators leading to neutrophil production which could prevent neutropenia. G-CSF affects a variety of cellular pathways and modulates the secretory cytokine profile.48 These actions could influence monocytes to mediate granulopoiesis since they express the G-CSF receptor.49 Adding to this, G-CSF has been proven experimentally to modulate monocyte cytokine secretion.50,51 The exact mechanism of action should be subjected to further studies since such clinical observation has the potential to furnish a new insight in the fields of immunology and molecular biology along with its clinical applications.
Conclusion
In the current work, we represent a comprehensive analysis evaluating AMC values as a prognostic variable in determining ANC changes following G-CSF therapy in febrile neutropenia patients. A retrospective search throughout the electronic system of KAUH was performed representing a 10-year single center data of febrile neutropenia cases. Based on the current analysis, AMC values hold a prognostic entity regarding ANC changes in chemotherapy-induced febrile neutropenia without any restriction to patients’ demographics and characteristics following G-CSF treatment. The findings emphasize the role of AMC in notifying emergency doctors and oncology specialist toward high-risk febrile neutropenia patients and can predict the responsiveness of G-CSF therapy. The main limitation in this study is its retrospective nature with moderate sample size. The first attack of each patient was included, and the rest were omitted to eliminate the factor of response bias, which necessitate the need for additional analysis of recurrent attacks with their compatibility to the first one. Although AMC values could predict ANC changes to a certain degree, it did not exhibit any statistically significant difference in determining the morality and recurrence probability paths according to Kaplan-Meier analysis. Further studies are needed to increase the sample size and to specify the target population regarding the type of malignancy and chemotherapy protocol utilized. Future work should be also directed toward a more specific and sensitive risk prediction indices for chemotherapy-induced febrile neutropenia following G-CSF therapy.
Ethical Approval
The study was approved by the institutional review board committee in King Abdullah University Hospital (KAUH). This study was conducted in accordance with the declaration of Helsinki, applying all the current regulations for retrospective studies in KAUH. Patient consents were waived as data was used in aggregate anonymously.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest for this work.
References
1. Lucas AJ, Olin JL, Coleman MD. Management and preventive measures for febrile neutropenia. P & T. 2018;43(4):228–232.
2. Taplitz RA, Kennedy EB, Bow EJ, et al. Outpatient management of fever and neutropenia in adults treated for malignancy: American society of clinical oncology and infectious diseases society of America clinical practice guideline update. J Clin Oncol. 2018;36(14):1443–1453. doi:10.1200/JCO.2017.77.6211
3. Klastersky J, de Naurois J, Rolston K, et al. Management of febrile neutropaenia: ESMO clinical practice guidelines†. Ann Oncol. 2016;27:v111–v118. doi:10.1093/annonc/mdw325
4. van der Velden WJFM, Herbers AHE, Netea MG, et al. Mucosal barrier injury, fever and infection in neutropenic patients with cancer: introducing the paradigm febrile mucositis. Br J Haematol. 2014;167(4):441–452. doi:10.1111/bjh.13113
5. Netea MG, Kullberg BJ, Blok WL, et al. The role of hyperuricemia in the increased cytokine production after lipopolysaccharide challenge in neutropenic mice. Blood. 1997;89(2):577–582. doi:10.1182/blood.V89.2.577
6. Schwartzberg LS. Neutropenia: etiology and pathogenesis. Clin Cornerstone. 2006;8:S5–S11. doi:10.1016/S1098-3597(06)80053-0
7. Pagano L, Caira M, Nosari A, et al. Etiology of febrile episodes in patients with acute myeloid leukemia: results from the hema e-chart registry. Arch Intern Med. 2011;171(16):1502–1503. doi:10.1001/archinternmed.2011.374
8. Weycker D, Li X, Edelsberg J, et al. Risk and consequences of chemotherapy-induced febrile neutropenia in patients with metastatic solid tumors. J Oncol Pract. 2015;11(1):47–54.
9. Weycker D, Barron R, Kartashov A, et al. Incidence, treatment, and consequences of chemotherapy-induced febrile neutropenia in the inpatient and outpatient settings. J Oncol Pharm Pract. 2014;20(3):190–198. doi:10.1177/1078155213492450
10. Kanamaru A, Tatsumi Y. Microbiological data for patients with febrile neutropenia. Clin Infect Dis. 2004;39(Supplement_1):S7–S10. doi:10.1086/383042
11. Freifeld AG, Bow EJ, Sepkowitz KA, et al. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the Infectious Diseases Society of America. Clin Infect Dis. 2011;52(4):e56–e93.
12. Clark OA, Lyman GH, Castro AA, et al. Colony-stimulating factors for chemotherapy-induced febrile neutropenia: a meta-analysis of randomized controlled trials. J Clin Oncol. 2005;23(18):4198–4214. doi:10.1200/JCO.2005.05.645
13. Clark OAC, Lyman GH, Castro AA, et al. Colony-stimulating factors for chemotherapy-induced febrile neutropenia: a meta-analysis of randomized controlled trials. J Clin Oncol.. 2005;23(18):4198–4214.
14. Mhaskar R, Clark OA, Lyman G, et al. Colony‐stimulating factors for chemotherapy‐induced febrile neutropenia. Cochrane Database Syst Rev. 2014;10.
15. Brito-Zerón P, Soria N, Muñoz S, et al. Prevalence and clinical relevance of autoimmune neutropenia in patients with primary Sjögren’s syndrome. Semin Arthritis Rheum. 2009;38(5):389–395. doi:10.1016/j.semarthrit.2008.01.014
16. Stewart DJ, Bodey GP. Infections in hairy cell leukemia (leukemic reticuloendotheliosis). Cancer. 1981;47(4):801–805. doi:10.1002/1097-0142(19810215)47:4<801::AID-CNCR2820470428>3.0.CO;2-6
17. Ogimi C, Krantz EM, Golob JL, et al. Antibiotic exposure prior to respiratory viral infection is associated with progression to lower respiratory tract disease in allogeneic hematopoietic cell transplant recipients. Biol Blood Marrow Transplant. 2018;24(11):2293–2301. doi:10.1016/j.bbmt.2018.05.016
18. Gui C, Cheng Z, Cecil E, et al. Low peripheral blood leukocyte counts during radiation therapy for head and neck cancer predict distant relapse and dysphagia. Int J Radiat Oncol Biol Phys. 2019;105(1):E421. doi:10.1016/j.ijrobp.2019.06.1530
19. Georgiadou SP, Sampsonas FL, Rice D, et al. Open-lung biopsy in patients with undiagnosed lung lesions referred at a tertiary cancer center is safe and reveals noncancerous, noninfectious entities as the most common diagnoses. Eur J Clin Microbiol Infect Dis. 2013;32(1):101–105. doi:10.1007/s10096-012-1720-9
20. Zheng B, Huang Z, Huang Y, et al. Predictive value of monocytes and lymphocytes for short-term neutrophil changes in chemotherapy-induced severe neutropenia in solid tumors. Supportive Care Cancer. 2020;28(3):1289–1294. doi:10.1007/s00520-019-04946-3
21. Freifeld AG, Bow EJ, Sepkowitz KA, et al. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the infectious diseases society of America. Clin Infect Dis. 2011;52(4):e56–e93.
22. Adelberg DE, Bishop MR. Emergencies related to cancer chemotherapy and hematopoietic stem cell transplantation. Emerg Med Clin North Am. 2009;27(2):311–331. doi:10.1016/j.emc.2009.01.005
23. Zheng B, Toarta C, Cheng W, et al. Accuracy of the Multinational Association of Supportive Care in Cancer (MASCC) and Clinical Index of Stable Febrile Neutropenia (CISNE) scores for predicting serious complications in adult patients with febrile neutropenia: a systematic review and meta-analysis. Crit Rev Oncol Hematol. 2020;149:102922.
24. Lyman GH, Abella E, Pettengell R. Risk factors for febrile neutropenia among patients with cancer receiving chemotherapy: a systematic review. Crit Rev Oncol Hematol. 2014;90(3):190–199. doi:10.1016/j.critrevonc.2013.12.006
25. Pettengell R, Bosly A, Szucs TD, et al. Multivariate analysis of febrile neutropenia occurrence in patients with non-Hodgkin lymphoma: data from the INC-EU Prospective Observational European Neutropenia Study. Br J Haematol. 2009;144(5):677–685. doi:10.1111/j.1365-2141.2008.07514.x
26. Lyman GH, Morrison VA, Dale DC, et al. Risk of febrile neutropenia among patients with intermediate-grade non-Hodgkin’s lymphoma receiving CHOP chemotherapy. Leuk Lymphoma. 2003;44(12):2069–2076. doi:10.1080/1042819031000119262
27. Lyman GH, Delgado DJ. Risk and timing of hospitalization for febrile neutropenia in patients receiving CHOP, CHOP-R, or CNOP chemotherapy for intermediate-grade non-Hodgkin lymphoma. Cancer. 2003;98(11):2402–2409. doi:10.1002/cncr.11827
28. Crawford J, Glaspy JA, Stoller RG, et al. Final results of a placebo-controlled study of filgrastim in small-cell lung cancer: exploration of risk factors for febrile neutropenia. Support Cancer Ther. 2005;3(1):36–46. doi:10.3816/SCT.2005.n.023
29. Okishiro M, Kim SJ, Tsunashima R, et al. MDM2 SNP309 and TP53 R72P associated with severe and febrile neutropenia in breast cancer patients treated with 5-FU/epirubicin/cyclophosphamide. Breast Cancer Res Treat. 2012;132(3):947–953. doi:10.1007/s10549-011-1637-5
30. McLeod HL, Sargent DJ, Marsh S, et al. Pharmacogenetic predictors of adverse events and response to chemotherapy in metastatic colorectal cancer: results from north American gastrointestinal intergroup trial N9741. J Clin Oncol. 2010;28(20):3227–3233.
31. Klastersky J, Paesmans M, Rubenstein EB, et al. The multinational association for supportive care in cancer risk index: a multinational scoring system for identifying low-risk febrile neutropenic cancer patients. J Clin Oncol. 2000;18(16):3038–3051.
32. Carmona-Bayonas A, Gómez J, González-Billalabeitia E, et al. Prognostic evaluation of febrile neutropenia in apparently stable adult cancer patients. Br J Cancer. 2011;105(5):612–617. doi:10.1038/bjc.2011.284
33. Carmona-Bayonas A, Jiménez-Fonseca P, Virizuela Echaburu J, et al. Prediction of serious complications in patients with seemingly stable febrile neutropenia: validation of the clinical index of stable febrile neutropenia in a prospective cohort of patients from the FINITE study. J Clin Oncol. 2015;33(5):465–471.
34. Coyne CJ, Le V, Brennan JJ, et al. Application of the MASCC and CISNE risk-stratification scores to identify low-risk febrile neutropenic patients in the emergency department. Ann Emerg Med. 2017;69(6):755–764. doi:10.1016/j.annemergmed.2016.11.007
35. Moriyama Y, Horita N, Kudo M, et al. Monocyte nadir is a possible indicator for neutrophil nadir during lung cancer chemotherapy. Clin Respir J. 2017;11(4):453–458. doi:10.1111/crj.12358
36. Shimanuki M, Imanishi Y, Sato Y, et al. Pretreatment monocyte counts and neutrophil counts predict the risk for febrile neutropenia in patients undergoing TPF chemotherapy for head and neck squamous cell carcinoma. Oncotarget. 2018;9(27):18970–18984. doi:10.18632/oncotarget.24863
37. Sato I, Nakaya N, Shimasaki T, Nakajima H, Motoo Y. Prediction of docetaxel monotherapy-induced neutropenia based on the monocyte percentage. Oncol Lett. 2012;3(4):860–864.
38. Ouyang W, Liu Y, Deng D, et al. The change in peripheral blood monocyte count: a predictor to make the management of chemotherapy-induced neutropenia. J Cancer Res Ther. 2018;14(Supplement):S565–s570. doi:10.4103/0973-1482.177502
39. Moreau M, Klastersky J, Schwarzbold A, et al. A general chemotherapy myelotoxicity score to predict febrile neutropenia in hematological malignancies. Ann Oncol. 2009;20(3):513–519. doi:10.1093/annonc/mdn655
40. Fonseca PJ, Carmona-Bayonas A, García IM, et al. A nomogram for predicting complications in patients with solid tumours and seemingly stable febrile neutropenia. Br J Cancer. 2016;114(11):1191–1198. doi:10.1038/bjc.2016.118
41. Oguz A, Karadeniz C, Ckitak EC, et al. Which one is a risk factor for chemotherapy-induced febrile neutropenia in childhood solid tumors: early lymphopenia or monocytopenia? Pediatr Hematol Oncol. 2006;23(2):143–151. doi:10.1080/08880010500457673
42. Lawrence SM, Corriden R, Nizet V. The ontogeny of a neutrophil: mechanisms of granulopoiesis and homeostasis. Microbiol Mol Biol Rev. 2018;82(1):e00057–17. doi:10.1128/MMBR.00057-17
43. Sallerfors B, Olofsson T. Granulocyte-macrophage colony-stimulating factor (GM-CSF) and granulocyte colony-stimulating factor (G-CSF) secretion by adherent monocytes measured by quantitative immunoassays. Eur J Haematol. 1992;49(4):199–207. doi:10.1111/j.1600-0609.1992.tb00047.x
44. Bendall LJ, Bradstock KF. G-CSF: from granulopoietic stimulant to bone marrow stem cell mobilizing agent. Cytokine Growth Factor Rev. 2014;25(4):355–367. doi:10.1016/j.cytogfr.2014.07.011
45. Castellani S, D’Oria S, Diana A, et al. G-CSF and GM-CSF modify neutrophil functions at concentrations found in cystic fibrosis. Sci Rep. 2019;9(1):12937. doi:10.1038/s41598-019-49419-z
46. Bober LA, Grace MJ, Pugliese-Sivo C, et al. The effect of GM-CSF and G-CSF on human neutrophil function. Immunopharmacology. 1995;29(2):111–119. doi:10.1016/0162-3109(94)00050-P
47. Fossati G, Mazzucchelli I, Gritti D, et al. In vitro effects of GM-CSF on mature peripheral blood neutrophils. Int J Mol Med. 1998;1(6):943–951.
48. Rutella S, Zavala F, Danese S, et al. Granulocyte colony-stimulating factor: a novel mediator of T cell tolerance. J Immunol. 2005;175(11):7085–7091. doi:10.4049/jimmunol.175.11.7085
49. Christopher MJ, Rao M, Liu F, et al. Expression of the G-CSF receptor in monocytic cells is sufficient to mediate hematopoietic progenitor mobilization by G-CSF in mice. J Exp Med. 2011;208(2):251–260. doi:10.1084/jem.20101700
50. Saito M, Kiyokawa N, Taguchi T, et al. Granulocyte colony-stimulating factor directly affects human monocytes and modulates cytokine secretion. Exp Hematol. 2002;30(10):1115–1123. doi:10.1016/S0301-472X(02)00889-5
51. Cheng DE, Chang W-A, Hung J-Y, et al. Involvement of IL‑10 and granulocyte colony‑stimulating factor in the fate of monocytes controlled by galectin‑1. Mol Med Rep. 2014;10(5):2389–2394. doi:10.3892/mmr.2014.2573
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.