")
Back to Journals » Medical Devices: Evidence and Research » Volume 15
Evaluating Filtering Facepiece Respirator Wearing-Comfort of Lebanese Red Cross Healthcare Providers
Authors Kheir O , Watts R, Verlinden J, Jacoby A, Smedts S, Vleugels J, Verwulgen S
Received 10 March 2022
Accepted for publication 13 May 2022
Published 2 June 2022 Volume 2022:15 Pages 153—161
DOI https://doi.org/10.2147/MDER.S362198
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Omar Kheir, Regan Watts, Jouke Verlinden, Alexis Jacoby, Sam Smedts, Jochen Vleugels, Stijn Verwulgen
Product Development, University of Antwerp, Antwerp, Belgium
Correspondence: Omar Kheir, Email [email protected]
Introduction: The COVID-19 pandemic significantly increased the usage of various types of face masks. In addition, it triggered the rapid manufacture of new production lines of masks to cope with the unprecedented demand to overcome worldwide shortages. Such masks, which were previously used mostly by the health care personnel, became a daily necessity to the greater mainstream population. This rapid and sudden increase in their usage and the fact that new masks’ innovations are progressively emerging to meet the growing global shortage requires an ongoing analysis on the factors associated with the fit and comfort while using these masks.
Methods: This paper presents the first translation and validation of the R-COMFI questionnaire to evaluate the comfort of a newly developed filtering face-piece respirator by the research team at the University of Antwerp. The questionnaire, which consists of 3 sections: Discomfort, General wearing experience, and Function, was translated from English to Arabic and involved 43 participants in the Lebanese Red Cross healthcare field based in Lebanon.
Results: The results showed discomfort factors that are mostly related to breathability and sweating caused by mask usage. Additionally, the results revealed that female respondents found the mask significantly less comfortable than male respondents (p-value with the two-tailed test is 0.0319), which confirmed that future validations should consider the concerns of both genders, and validated the R-COMFI translation exercise detailed in this paper.
Discussion: The contribution of this paper can be pinned down into three findings. The first finding is related to the discomfort issues. The second finding highlighted a significant difference in comfort experience between females and males. The last finding is the translation validation of the R-COMFI instrument, which confirmed that the questionnaire can be applied among wider geographical locations.
Keywords: respirator masks, R-COMFI, user comfort, breathability, demographic, gender
Introduction
Healthcare workers are frequently required to wear filtering facepiece respirators (FFRs), such as N95, KN95 and FFP respirators, during their shifts for their personal protection. FFRs are designed to prevent the wearer from inhaling small airborne particles.1 They must meet filtration requirements and fit tightly to the wearer’s face to limit facial seal leakage as per the requirements of the National Institute for Occupational Safety and Health (NIOSH) in the United States.2 Medical masks, however, often referred to as surgical masks, are intended to block microorganism transmission from the wearer to the patient. However, with their loose fit to the face, they do not provide reliable respiratory prevention against to inhalation of small airborne particles as much as they prevent hand-to-face contact and facial contact with large droplets and sprays.3
To be fully effective, properly fitting FFRs must be worn correctly for the entire duration of exposures in accordance with relevant national regulatory agencies, such as the regulation of the Occupational Safety and Health Administration (OSHA) in the United States.4 Nevertheless, previous research studies have reported insufficient compliance among health care personnel (HCP) with the recommendations of respiratory protection, including wearing several forms of personal protective equipment.5 This lack of adherence, which is a major challenge to the health care system,6 has been investigated by several former studies that could not precisely identify the hinderance.7 However, discomfort when wearing respirators by HCP has been frequently reported and is supported by the literature,8 but provides insufficient evidence to determine whether this directly causes non-adherence to the related guidelines, which enforce the proper use of respirators. Moreover, HCP have reported that many FFRs used in the US health care service have suboptimal tolerability,9 hence possibly cause a negative influence on the willingness of HCP to wear FFRs during patient care. Therefore, a wider research in this context, especially if it tackles the evaluation mechanism, can help explore adherence barriers and accordingly support the design requirements and the respective comfort evaluation procedures of future respirators.
The characteristics of FFRs that are requested by HCP while providing health care services include improved comfort, improved straps, less interference with breathing, and proper facial-fit despite the presence of facial hair.10 For this to be investigated scientifically and to be able to validate these factors pertaining to any FFR, researchers from the US Department of Veterans Affairs (VA) established a questionnaire instrument, which is referred to as “the Respirator Comfort, Wearing, Experience, and Function Instrument (R-COMFI)”.11 It is a novel questionnaire instrument used to establish the comfort and tolerability experienced by the HCP while wearing fit-tested FFRs. This questionnaire-based comfort evaluation mechanism has been widely used as it can be applied to measure the comfort factors related to any developed FFR to ensure it is convenient and meets the end-user comfort expectations.
This paper will examine an R-COMFI study performed on an FFR, that was manufactured by the Antwerp Design Factor (ADF) following the SARS-CoV-2 pandemic,12 and evaluated after being utilized by members of the Lebanese Red Cross (LRC) in Lebanon, to address the relevant R-COMFI comfort factors and the R-COMFI evaluation process. This study particularly aims to collect data from participants in a relatively new geographical location where similar studies have not been frequently conducted, as the case in Europe and the United States.
The questionnaire planning, preparation, and results are based on the data collected in Lebanon, and considerations with adopting the R-COMFI questionnaire are discussed toward the end of this paper.
Methods and Materials
Following the explosion of around 2750 metric tons of ammonium nitrate stored in the port of Beirut, which is located in the center of the Lebanese capital, on August 4, 2020,13 the University of Antwerp (UA) and the Antwerp Design Factory (ADF) initiated a donation of 2000 FFRs to be utilized by the HCP at the Lebanese Red Cross (LRC), after approaching and assessing the needs of the local NGOs in Lebanon. These FFRs were shipped on August 31, 2020, through one of the European Union’s humanitarian air-bridge flights that took place post the unfortunate incident. They were transferred by LRC from Beirut airport to LRC North Lebanon branch, as demonstrated in Figure 1, to be utilized by their designated HCP team against COVID-19.
 |
Figure 1 Picture highlighting the boxes of the Poly 2+ masks, with the user manual provided in Arabic, and their transfer to LRC’s northern branch. |
These respirators are novel, as they are based on an e-PTFE membrane filter material, as opposed to conventional respirator materials, which are based on melt-blown fibers. These respirators are shown in Figure 2. ADF also visually describes in a YouTube video all materials, components, processing, and production steps used in the respirators.14
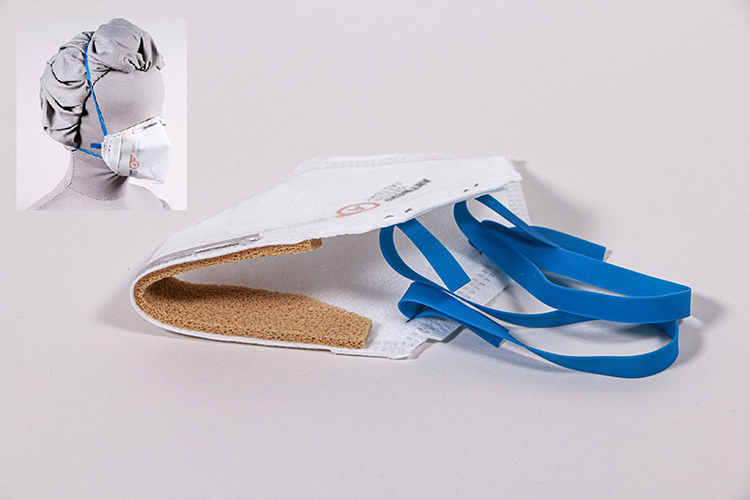 |
Figure 2 Picture of the ADF Poly 2+ masks. |
These respirator masks were certified by the Belgian alternative testing protocol (ATP) for FFP2/FFP3, which was a temporary national pandemic certification for FFP2/FFP3 respirators used during the start of the COVID-19 pandemic.15 As well as having Belgian certification, the comfort of these masks was studied, and design improvements were identified and implemented.16 The first author, based in Beirut, conducted the local research and coordinated with the LRC teams all issues related to requirements, logistics and the utilization of this donation with the support and close synchronization of the local research team in Antwerp.
Among the boxes of the donated FFRs were user manuals for these FFRs, which were provided in Arabic to ensure they are comprehensible for the native speakers, and which were translated and then translated back according to the “translation/back-translation” method,17 followed with translation evaluation by a committee of expert bilinguals and translators. The manual highlights in clear sentences with supporting visuals the steps to examine, use, and dispose the respirator, considering that too many people still do not know how to correctly use, reuse, and dispose masks.18 This user manual was divided into three sections: user instructions, fit test, and removal instructions. The local researcher, who is a native Arabic speaker, has tested the final Arabic version of these user manuals with five LRC members to validate the translation prior to the dispatch of the donation from Antwerp to the LRC team in Beirut.
The evaluation process of these FFRs, which was completed by 43 LRC frontliners, was derived from the R-COMFI questionnaire, which is divided into three sections: Comfort (10 issues to rate), General wearing experience (6 issues to rate) and Function (5 issues to rate). Of the 43 participants, 41 were within the same age group, aged between 21 and 34 years. The local researcher, and in coordination with the supervising professionals at UA, decided however to add an open-ended question for participants to compare their experience with the subject FFR versus any previously used FFRs that are commercially available. Also, a small set of demographic questions were added at the end of the questionnaire to further support the analysis, especially since the local researcher observed that females wearing a “hijab” or veil as part of their daily practice encounter more wearing discomfort than males. The questionnaire was additionally translated from English to Arabic and then from Arabic to English according to the “translation/back-translation” method,17 and with the presence of two bilinguals participating in this research, the local researcher and linguistic institute affiliated with the University of Antwerp (UA). A few translated words were adjusted to ensure they better fit the targeted context behind a specific question, while considering the adopted translation process and most importantly the feedback of the participating bilinguals. The translated questionnaire was subsequently validated with one LRC member, who acted as a formal LRC focal point for this exercise, to ensure that there was no misunderstanding by the potential LRC participants. This focal person was informed that he will not participate in the questionnaire being in a managerial position and therefore is not a frontline caregiver.
The inquiry started with a brief description on the purpose behind this rating exercise aiming at evaluating the comfort of the utilized respirators for research purposes. A statement of consent was then presented highlighting that by completing this survey, participants are aware of the objective of this survey and willing to participate in the research in case they decide to continue with the survey. The note also stated that the research follows the guidelines outlined in the Declaration of Helsinki and that the approval of the Independent Ethics Advisory Committee for Research in the Social and Humane Sciences (EA SHW), founded by the Executive Council of the University of Antwerp on 03.07.2012, has been obtained. The actual questionnaire consisted of three sets of ordinal scaled questions derived from the R-COMFI questionnaire, followed with one additional open-ended question and two demographic multiple-choice questions. In line with the original R-COMFI questionnaire, the first two sets of questions used three-point Likert scale while the third one used four-point Likert scale.
To minimize risks due to physical contact in the context of COVID-19 measures, the questionnaire was published online using a questionnaire tool “QuestionPro”. The online approach was positively received by the LRC team, considering the benefits of online questionnaires such as convenience when compared to paper-based.19 Several rounds of testing of the online tool were performed to confirm content validity as per the content validity indexes.20 In that process, the established online questionnaire was tested by three content experts, each of whom was an LRC HCP with previous experience in FFRs in the patient care setting, yet none had used the subject FFRs. The questionnaire was reviewed and finalized once a universal agreement among the experts was achieved. After a three-week period of testing and utilizing the FFRs while the LRC team members on duty, the online questionnaire link was shared with the LRC focal point who in turn cascaded it with the selected LRC team members that have used the FFRs from the Antwerp Design Factory using their adopted communication channel.
After several rounds of follow-up with the LRC focal person to ensure as many of the relevant LRC personnel complete the survey, the data was exported from the questionnaire tool. The data were subsequently grouped in line with the R-COMFI questionnaire in order to identify the factors of discomfort per category and entry of the questionnaire. Following this, the data were divided among the two genders, and median ratings for each group was calculated in order to compare the experience between female and male participants.
Because participants answered a series of questions about discomfort, general wearing experience, and function using Likert-type response options, in which each response was weighted equally, R-COMFI scores were obtained for the three subscales and summed for a total score for female, male, and total participants in line with the conversion adopted by Warndorff et al.16 For the discomfort and general wearing experience subscales, possible responses included “none of the time” (zero points), “some of the time” (one point) or “all of the time” (two points). For the function subscale, possible responses included “strongly disagree” (zero points), “disagree” (one point), “agree” (two points) or “strongly agree” (three points). The range of possible scores was zero to 20, zero to 12, and zero to 15 for the discomfort, general wearing experience, and function subscales, respectively. The total maximum R-COMFI score was 47, where lower score reflects better tolerability of the FFR.
The Likert scale ratings were used to identify the rating trends among the question groups and across both genders to describe the comfort rating of the respirator overall and between genders respectively. The R-COMFI score rating was then compared with t-test to highlight the comfort rating among genders and support the validity of the translation exercise.
Results
Out of the total 46 LRC participants, 43 participants completed the questionnaire (26 females and 17 males). Accordingly, the responses were grouped for each comfort issue across the three sections of the R-COMFI questionnaire. Table 1 shows the results pertaining to the three sections of the R-COMFI questionnaire on “Discomfort”, “General Wearing Experience” and “Function”.
 |
Table 1 Questionnaire Results for the 43 Respondents Regarding “Discomfort”, “General Wearing Experience” and “Function” |
In the first section of the R-COMFI questionnaire on “Discomfort”, the participants mostly highlighted discomfort issues that are related to facial heat or warmth, sweat or moisture buildup, and lack of fresh air.
In the second section of the R-COMFI questionnaire on “General Wearing Experience”, the participants indicated that they have mostly encountered comfort issues related to loss of energy, tiredness or fatigue, shortness of breath, and difficulty of breathing.
In the third section of the R-COMFI questionnaire on “Function”, the responses mostly demonstrated comfort issues related to difficulty in communicating to others and difficulty of hearing others.
For the open-ended questions, few participants provided comments to emphasize on issues that were already highlighted within the questionnaire, mostly related to breathability and tightness of the straps. Therefore, this section of the questionnaire was excluded during the analysis as it did not present additional valuable information.
When the questionnaire data was divided into the separate responses’ ratings for females and males, it was noticed that the female respondents found the mask less comfortable than the male respondents. Figure 3 illustrates the variance of the average question rating among each gender across most of the 21 questions of the questionnaire. This is based on comparing the mean Likert scale rating for every question per gender, while noting again that the range of possible scores varies for each section as described previously, and visually highlighting the variance between the responses of both groups. The standard error bars, resembling the variability of data to indicate the error or uncertainty in reported measurement and to represents one standard deviation of uncertainty, that top every Likert scale mean shows that while even considering a margin of error, the highlighted variance per question stands.
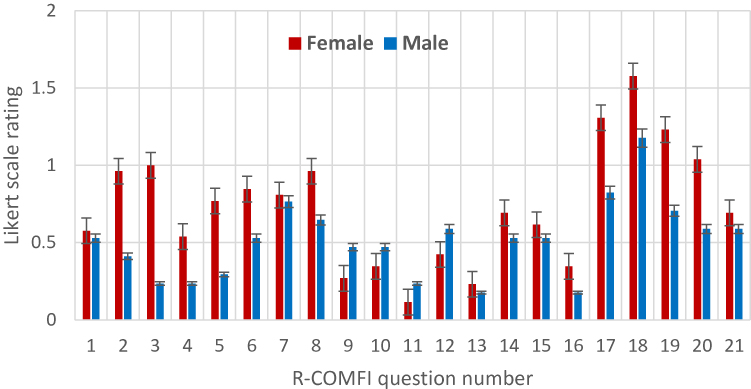 |
Figure 3 Bar chart diagram showing the averaged Likert scale rating with standard error, per each of the R-COMFI 21 questions, for female and male participants. |
Additionally, when comparing the calculated R-COMFI scores for the male and female participants, the results showed a clear variance. Table 2 groups the scoring of each gender along with scoring of all participants combined across the “Discomfort and General wearing experience questions”, “Mask functionality questions”, and the “Mean of all questions combined”. This disparity is illustrated through the mean R-COMFI score of all questions for the male group being 10.71 while for the female group is 15.35, indicating that female participants experienced the FFR to be less tolerable than their male counterparts.
 |
Table 2 R-COMFI Scoring per Questions Groups and Total Scoring Across Genders |
Discussion
While the R-COMFI questionnaire does not include demographic questions and does not make the distinction between including female and male, the results in this study demonstrate a significant difference between genders. In addition to the graphical rating differences represented in Figure 3, the R-COMFI score for the male and female participants was 10.71 and 15.35, respectively, with standard deviation equal to 3.28 of the mean R-COMFI male vs female scoring, and while noting again that lower score reflected better tolerability. To explore these results, t-tests were conducted and accordingly p-values were calculated for the female versus male question-rating means, as illustrated in Table 3. This table indicates that with the confidence interval, α, set at 0.05, the p-value with the two-tailed test is 0.0319 or 3.19%. Having the p-value lower than 5% in this instance, we reject the null hypothesis that there is no significant difference between genders. This confirms that there is a statistical difference between genders for discomfort, general wearing and function and confirms that the female participants found the masks less comforting than male participants.
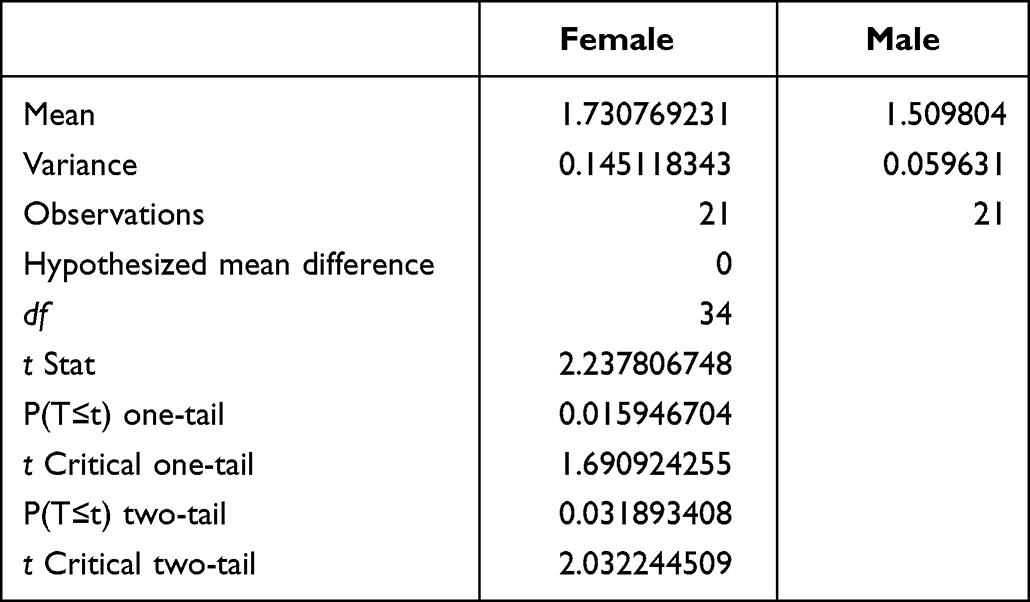 |
Table 3 Extracted t-test: Two Sample Assuming Unequal Variances, Which Reveals a Statistical Difference Between Genders for Discomfort, General Wearing and Function, Indicating p-value with the Two-Tailed Test is 0.0319 at a Significance Level of α = 0.05 |
Therefore, further studies with R-COMFI should pay attention to gender. For example, if this were neglected, and the study were to include only males or only females, the data would not be representative of the experience of the broad population. Having fair gender representation could also address specific gender sensory attributes in the design of new respirator devices. Previous studies in this domain also indicated that gender differences were observed for the variables reflecting physiological and facial comfort effect.21 This same study has confirmed that gender influences the rating of respirators since women more often rate temperature and sweat as more uncomfortable than men.
Additionally, the results achieved especially in Figure 3 and Table 2 can be seen against the validation of the R-COMFI translation since each gender has specific sensory perceptions, especially as Lebanese or Arab men typically have facial hair and women typically wear hijabs/veils, a cultural trend, which is particular to Middle Eastern countries.
Conclusion
This study discusses the process of applying the R-COMFI questionnaire on a newly manufactured filtering facepiece respirator (FFR). It is intended to evaluate the comfort issues of these FFRs in addition to discussing the use of the R-COMFI instrument in order to present possible enhancements that can be applied in future FFRs comfort evaluation studies in geographical regions beyond Europe or the United States, as more knowledge may help remove barriers to the challenge of adherence of correct use of personal protective equipment in the healthcare sector, and can lead to the development of new respirator designs that are more comfortable and tolerable.
The contribution of this paper can be pinned down into three findings. The first one is related to the discomfort issues that the LRC participants encountered while using the evaluated FFRs, which were mainly related to breathability and shortness of breath. The second finding highlighted a significant difference in comfort experience between females and males, which indicates the importance of even gender distributions in future FFRs comfort studies, were the goal to have effective (re-)design of future FFRs. The last contribution is the translation validation of the R-COMFI instrument, which confirmed that the questionnaire can be applied among wider geographical locations without having language burden, providing a proper translation method is used. The findings presented can support the respirators’ comfort evaluation process in order to overcome adherence barriers to the proper utilization of respirators among healthcare personnel and properly reflect design requirements on the basis of gender for the development of future respirator device.
Acknowledgments
This study was possible with the great support of the various teams and leadership of the Lebanese Red Cross and the generosity of the respirators’ donors, who swiftly initiated a donation to support the unfortunate incident that occurred in Beirut on August 4, 2020, and everyone who facilitated this humanitarian initiative.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Janssen L, Ettinger H, Graham S, Shaffer R, Zhuang Z. The use of respirators to reduce inhalation of airborne biological agents. J Occup Environ Hyg. 2013;10(8):D97–D103. doi:10.1080/15459624.2013.799964
2. The National Institute for Occupational Safety and Health. USA: NIOSH-Approved Particulate Filtering Facepiece Respirators; 2021. Available from: https://www.cdc.gov/niosh/npptl/topics/respirators/disp_part/default.html.
3. Lipp A, Edwards P. Disposable surgical face masks for preventing surgical wound infection in clean surgery. The Cochrane Library website; 2016. Available from: http://www.cochranelibrary.com/.
4. Occupational Safety and Health Administration. USA. OSHA- Directives - Directive Number; 2019. Avialable from: https://www.osha.gov/enforcement/directives/directivenumber/CPL.
5. Nichol K, McGeer A, Bigelow P, et al. Behind the mask: determinants of nurse’s adherence to facial protective equipment. Am J Infect Control. 2013;41(1):8–13. doi:10.1016/j.ajic.2011.12.018
6. Yassi A, Moore D, FitzGerald JM, et al. Research gaps in protecting healthcare workers from SARS and other respiratory pathogens: an interdisciplinary, multi-stakeholder, evidence based approach. J Occup Environ Med. 2005;47(1):41–50. doi:10.1097/01.jom.0000150207.18085.41
7. LaVela S, Kostovich C, Locatelli S, et al. Development and initial validation of the respirator comfort, wearing experience, and function instrument [R-COMFI]. J Occup Environ Hyg. 2016;14(2):135–147.
8. Shenal B, Radonovich L, Cheng J, Hodgson M, Bender B. Discomfort and exertion associated with prolonged wear of respiratory protection in a healthcare setting. J Occup Environ Hyg. 2012;9(1):59–64. doi:10.1080/15459624.2012.635133
9. Gosch M, Shaffer R, Eagan A, Roberge R, Davey V, Radonovich L. B95: a new respirator for health care personnel. Am J Infect Control. 2013;41(12):1224–1230. doi:10.1016/j.ajic.2013.03.293
10. Locatelli S, LaVela S, Gosch M. Health care workers’ reported discomfort while wearing filtering face-piece respirators. Workplace Health Saf. 2014;62(9):362–368. doi:10.3928/21650799-20140804-03
11. LaVela S, Kostovich C, Locatelli S, Gosch M, Eagan A, Radonovich L. Development and initial validation of the Respirator Comfort, Wearing Experience, and Function Instrument [R-COMFI]. J Occup Environ Hyg. 2017;14(2):135–147. doi:10.1080/15459624.2016.1237025
12. Vanhooydonck A, Van Goethem S, Van Loon J, et al. Case study into the successful emergency production and certification of a filtering facepiece respirator for Belgian hospitals during the COVID-19 pandemic. J Manuf Syst. 2021;60:876–892. doi:10.1016/j.jmsy.2021.03.016
13. CNN.com. USA. Beirut explosion rocks Lebanon’s capital city; 2020. Available from: https://edition.cnn.com/middleeast/live-news/lebanon-beirut-explosion-live-updates-dle-intl/index.html.
14. ADF - ONCORONA - Poly2+ production. Youtube; 2021. Available from: https://www.youtube.com/watch?v=OtJp-KJcaiI.
15. Belgian Federal Public Service Economy. Conditions with which the supply of mouth masks FFP2 and FFP3 must meet in order to be released; 2020. Available from: https://economie.fgov.be/nl/themas/ondernemingen/coronavirus/mondmaskers-enfilters/coronavirus-conformiteitseisen.
16. Warndorff V, Huysmans S, Dirx W, et al. Heuristic evaluation of respirator masks: incorporating NIOSH respirator mask comfort surveying in the product design process. In: Rebelo F, editor. Advances in Ergonomics in Design. AHFE. Lecture Notes in Networks and Systems. Vol. 261. Cham: Springer; 2021.
17. Brislin RW. Back-translation for cross-cultural research. J Cross Cult Psychol. 1970;1(3):185–216. doi:10.1177/135910457000100301
18. Scalvenzi M, Villani A, Ruggiero A. Community knowledge about the use, reuse, disinfection and disposal of masks and filtering facepiece respirators: results of a study conducted in a dermatology clinic at the University of Naples in Italy. J Community Health. 2021;46:786–793. doi:10.1007/s10900-020-00952-3
19. Roberts L, Allen P. Exploring ethical issues associated with using online questionnaires in educational research. Edu Res Eval. 2015;21(2):95–108. doi:10.1080/13803611.2015.1024421
20. Polit DF, Beck CT. The content validity index: are you sure you know what’s being reported? Critique and recommendations. Res Nurs Health. 2006;29(5):489–497. doi:10.1002/nur.20147
21. Harber P, Santiago S, Wu S, Bansal S, Liu Y, Yun D. Subjective response to respirator type: effect of disease status and gender. J Occup Environ Med. 2010;52(2):150–154. doi:10.1097/JOM.0b013e3181cfcf09
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.