")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 10
Ethical and legal framework and regulation for off-label use: European perspective
Received 18 March 2014
Accepted for publication 4 May 2014
Published 12 July 2014 Volume 2014:10 Pages 537—546
DOI https://doi.org/10.2147/TCRM.S40232
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Christian Lenk,1 Gunnar Duttge2
1Institute for History, Theory and Ethics of Medicine, Ulm University, Ulm, Germany; 2Center for Medical Law, Göttingen University, Göttingen, Germany
Abstract: For more than 20 years the off-label use of drugs has been an essential part of the ethical and legal considerations regarding the international regulation of drug licensing. Despite a number of regulatory initiatives in the European Union, there seems to remain a largely unsatisfactory situation following a number of critical descriptions and statements from actors in the field. The present article gives an overview of the ethical and legal framework and developments in European countries and identifies existing problems and possible pathways for solutions in this important regulatory area. In addition to the presentation of the ethical and legal foundations, some attention is given to criticisms from medical practitioners to the current handling of off-label drug use. The review also focuses on the situation confronted by patients and physicians when off-label prescriptions are necessary. Through legal descriptions from a number of countries, possible solutions for future discussion of European health care policy are selected and explained.
Keywords: ethics, law, Europe, health care policy
Introduction
Developing the adequate conceptual definition of the phenomenon of off-label drug use shows a close connection to drug law because off-label use means use outside of the originally tested and licensed indication. The realization of license depends on national drug laws, which are derived from the relevant European directives and regulations. Too extensive an off-label area could be seen as a sign or symptom of a regulatory system which is overly rigid. In an ideal drug regulation framework, important applications in medical practice should not fall into the area of off-label use. What applications are licensed depends also on the historical developments in specific countries; for example, the Federal Republic of Germany simply had no drug law before the thalidomide scandal in the years 1961 and 1962.1 The first German drug law came into force in 1961, and there was no mandate for the authorization of drugs until the German Drug Law of 1976.1 Therefore, before this date there were, by definition, no off-label drug uses.1
For our purposes, we follow the European Medicines Agency’s (EMA) definition of off-label use from the guideline on good pharmacovigilance practices, which is as follows:
Situations where a medicinal product is intentionally used for a medical purpose not in accordance with the authorized product information. Off-label use includes use in nonauthorized paediatric age categories. Unless specifically requested, it does not include use outside the EU in an indication authorized in that territory which is not authorized in the EU.2
This definition presupposes that the off-label use takes place in a conscience manner (intentionally), and that the use of the drug deviates from the foreseen area of application or age group, and that it is locally bound to the countries of the EU. The last criterion means that the product information in the EU is decisive, and that other possible fields of application in other countries are of no significance from the regulatory point of view. The discussion of the definition of off-label use of drugs is described in a publication by Neubert et al,3 where it is also mentioned (from the EMA’s point of view) that drugs which already received European marketing authorization will in general be “off-label”; drugs without such an authorization will be “unlicensed”, and the use of drugs which are “contraindicated” will be considered “off-label”.3 As in other regions, manufacturers are not allowed to market a drug’s off-label use in European countries.
Off-label use in Europe: incidence in particular patient groups
Concerning the factual degree of off-label use in European countries, a number of studies focused on different patient groups. Perhaps most publications in this area of research in the last 15 years have focused on off-label use in children and adolescents. In a French study in the Paris region, Chalumeau et al4 examined the prescriptions of 95 office-based pediatricians for 1 single day for patients under 15 years. They found that from the 2,522 prescriptions from this day, which were administered to 989 patients, 33% were used unlicensed and 29% off-label. Five hundred and fifty, or 56%, of the children on this day received at least one off-label prescription. For pediatric outpatients in Germany, Bücheler et al5 examined 1.74 million prescriptions from the first quarter of the year 1999 for children and adolescents from 0 to 16 years. Altogether, 13.2% of these prescriptions were off-label, with strongly increased levels of off-label use for single medical areas. For example, 78.6% of the drugs topically used in eyes and ears and 57.9% of the dermatological drugs were used off-label, according to the findings of this study.
Another field of research addressed off-label use in palliative care. In 2013, Culshaw et al6 conducted an online survey in the UK with selected doctors, nurses, and pharmacists in the area of palliative medicine on the communication of the approval status of drugs. Only one-sixth, or 15%, of the respondents reported that their institutions regularly inform the patients on the off-label use of drugs, and 22% of the doctors stated that they never “draw (the patient’s) attention to the license” in case of prescribing a drug which is routinely used off-label.
In psychiatry, Martin-Latry et al7 conducted a study on off-label prescriptions of psychotropic drugs among hospitalized patients in France. They also examined prescriptions from 1 day (in March 2005), in this case from a state psychiatric hospital. They found that the 75 patients on four hospital wards received 261 prescriptions altogether, from which 39.8% were off-label. The highest rate of off-label drugs were found in the case of anticonvulsants, with 97% of the prescribed drugs. The studies show not only the sometimes surprisingly high rates of off-label use for vulnerable patient populations, but also an uncertain handling of knowledge regarding patients and off-label use of drugs.
Ethical considerations concerning the authorization of drugs
On the one hand, the existing legal framework and regulations are of huge importance for the concrete work of physicians and the actual medical supply to patients. On the other hand, there exist a number of overarching ethical aims and considerations which can give some orientation towards a convincing regulation of drug licensing. Such considerations are, among others, the safety of patients and a smooth organization of drug testing; the benefit of new, effective, and safe drugs for specific patient groups as well as the overall population; the particular responsibility of physicians and health care professionals using and prescribing drugs; and questions of justice and equity regarding the access of patients to safe and effective drugs. To fully understand the implications of the phenomenon of off-label use, one has also to take into account that it allows physicians to use existing drugs in an innovative way, when evidence exists, although a formal authorization did not take place. In some cases, the off-label use of drugs also allows the supply of adequate medicines to vulnerable patient populations (in the case of orphan or rare diseases). Additionally, Liang and Mackey8 recommend, from a US perspective, “(…) appropriate off-label promotion and information sharing for orphan diseases, by promoting and expanding the systematic collection of and access to data, (…)”.
Despite individual inequalities of social status, education, age, and health, it is an important ethical demand that all citizens and all patient groups should have access to sufficiently tested and safe drugs, which went through a systematic and structured process of licensing. It is known that some patient groups, for example children, regularly fall outside these “normal” processes and pose a formidable challenge for the regulation of drug licensing. Therefore, an effective ethical and legal framework has to be built that can accomplish these important demands. Additionally, in the legal area, questions of concrete criteria for drug licensing, of liability, and of possible damages to patients due to risky and/or unlicensed drugs or off-label drug use as well as compensation claims from patients play an important role.
Political aims and statements from the European Union
The EU developed the most intensive activities concerning the off-label use of drugs in the area of children and adolescents. According to official statements of the European Commission, around 21% of European citizens fall into these groups, which means that the question of adequate drug supply in pediatrics concerns more than 100 million persons in the EU’s member states alone.9 The commission estimates that more than 50% of medicines used in practice were not tested for the specific age group before the coming into force of the Orphan Regulation.10 As the decisive reason for political intervention, the commission points to “the associated nonnegligible risks of inefficacy or adverse reactions”.9 Therefore, it is the official aim of the European Commission that most drugs should be specifically authorized for the respective treatment with adequate forms and formulations. Similar to other political actors, the commission took not a strategy of rigid and compelling legal regulations, but a system of “incentives” to steer the actors in the field into the desired direction. Two of these incentives are 1) “a six-month extension to the Supplementary Protection Certificate” and 2) “in respect of orphan medicines, (…) an extra two years of market exclusivity added to the existing ten years awarded under the EU’s Orphan Regulation”.9 Pharmaceutical companies can therefore realize a strengthened protection of their patents and intellectual property in exchange for an extension of the study population and documentation for children and adolescents. In large part, this idea and program followed the Orphan Drug Act in the US; more comprehensive discussion of this regulatory issue can be found in a report by Lenk.11
The European Commission also sees a fundamental “change of culture” in pharmaceutical enterprises as “undertakings now consider paediatric development to be an integral part of the overall development of a product”.9 However, this presupposed cultural change is currently not backed up by data because, as the authors of the commission report must acknowledge, the registrations in the EudraCT database show no increase in the number of pediatric trials. Therefore, it is questionable at present whether the mere strategy of incentives does effectively target the existing problem.
The physician’s perspective: the example of oncology
The difference between on-label and off-label drug use also has some important implications for the physician who prescribes the drugs. In the following discussion, we will focus on the field of oncology, which can be seen as a special case in off-label use because some cancer drugs that are effective for one indication can also be used for other cancer forms. In this context, the position paper of the European Society for Medical Oncology (ESMO) describes a number of ethical issues; for example, the ESMO bylaws demand “to promote equal access to optimal cancer care of all cancer patients.”12 From the ethical point of view, this is a demand for justice in health care and a safeguard to avoid unjustified disadvantages and unnecessary harm for specific patient groups. However, the position paper suggests that due to the status of approval of a specific drug, a patient group that can be treated with a licensed drug will be treated better and in a more homogeneous way in comparison with a group where only off-label drugs are available, independent from the drug’s actual effectiveness for the treatment of the respective disease entity. There are clinical practice guidelines which recommend the off-label use of drugs (where evidence for the effectiveness of the treatment exists), but this is perceived by the ESMO as “outside existing regulatory boundaries, [in a sense] ‘against’ the law […].”12 Although this is not the case in the literal sense, and the off-label use of drugs is not illegal; indeed, there are some important differences in comparison with licensed drugs. From the ESMO’s point of view, this culminates in a particular responsibility of the treating physician:
In fact, by prescribing a drug off-label, the physician is asked to take a special responsibility. Formally, he is prescribing something which the regulatory body has not stated is safe and effective. Therefore, he/she may be called to respond for any problem arising from the use of the drug as if he/she had done something outside the state of the art. Often this is not the case, but the burden of the proof rests on the physician. In any case, the responsibility can be administrative, and third payers may claim that the prescription was not allowed, so that the physician may even be called to reimburse personally or be threatened to do so.12
Therefore, the prescription of off-label drugs contains a double danger for treating physicians: firstly, they can well come into a position where they must show that the treatment in itself was not in violation of professional duties. And secondly, even when the treatment was successful and, in comparison with other possible treatments, in the patient’s best interest, they could be accused that their decision was wrong due to administrative reasons and the insurance will not pay for it. Therefore, a complex ethical and legal situation might develop, with the potential outcome being that the original aim – the patient’s safe and effective treatment – cannot be achieved. The authors suggest the compilation of a list of “selected, evidence-based, off-label uses of anticancer drugs”12 to enable physicians to provide a safe and effective supply for patients despite the absence of licensed drugs. This could be a reasonable bridge in the absence of licensed drugs in a specific medical field until a sufficient amount of those drugs are on hand. As stated in the ESMO position paper, “A powerful solution would be that the EU regulatory body might facilitate the production of compendia of anticancer drugs, enlisting those off-label uses judged to be legitimate.”12 This would not solve the whole problem at once, but it would at least clarify the situation and improve the physician’s position (particularly regarding the question of medical liability) when confronted with the described paradoxes of off-label drug use.
Knowledge and perspective of patients and parents
The discussion of the off-label use of drugs is mainly led by experts, pharmacologists, and physicians. Patients and patient representatives seldom take part in this predominantly technical matter. From an ethical point of view, this is unsatisfying because those persons concerned should have knowledge regarding a drug’s status of authorization. In case of treatment alternatives, where one drug is off-label and the other drug is licensed, but from the physician’s point of view both alternatives are equivalent, the patient’s knowledge and decision on this question is of special importance. Therefore, the question has to be posed, what do patients know of off-label use of drugs? A number of publications show that experts perceive off-label treatment as a safety problem,13 but how would patients evaluate this situation? And when the experts’ point of view is that off-label use is different from a treatment with a licensed drug, does the ethical demand of “informed consent” not imply that patients should also be informed about a drug’s off-label status? At this point, ethical and legal considerations regarding the information of patients intertwine with empirical questions concerning the existing knowledge of patients.
In 2009, we initiated a study to determine what patients in a medical setting know about the off-label use of drugs.14 We wanted to find out what parents knew about the drugs used in treating their children’s chronic renal disease at two German university hospital outpatient care units. As a control group, parents of healthy children from a local soccer club were invited to participate in the study. One presupposition at the start of the project was that parents of chronically ill children would have, in general, a great interest to be informed about the safety and status of the drugs used. This idea was affirmed in the study. However, it was also shown that the existing interest in drug safety stood in stark contrast to the actual knowledge regarding the off-label use of drugs. Knowledge of the phenomenon of off-label use was generally poor among the participating parents. Roughly one third (28%) of the parents of healthy children knew that children sometimes receive drugs which are not tested and licensed for the actual patient or age group and/or indication. Surprisingly, this number was only slightly increased to 35% of parents of the chronically ill children knowing this fact. Not all parents were satisfied with this situation, leading to a considerable amount of parents who refused the off-label treatment altogether (parents of healthy children: 20%; parents of chronically ill children: 9%) or accepted it only “when there is no other possibility” (parents of healthy children: 72%; parents of chronically ill children: 51%).14 Our findings regarding a lack of information may also demonstrate an existing concern on the side of health care professionals: patients or their parents would, as a consequence of adequate information, eventually refuse a possible off-label treatment.
Interestingly, this finding corresponds with a demand in another context; in a study on off-label prescriptions for antipsychotic drugs, the authors showed that to a considerable extent (around one third), and for a specific drug, ziprasidone (Geodon, Pfizer, Inc., New York, NY, USA), children received an off-label prescription despite the existence of licensed drugs for their disease entity, and although it was their first prescription of an off-label drug.11,15 The authors therefore appeal for the implementation of “fail first and prior authorization policies”, ie, to initially treat children and adolescents with an authorized drug, and only change to an off-label drug prescription if this medication shows no treatment success. This could avoid inappropriate prescriptions and minimize treatment risks for the pediatric population.
Legal considerations
The legal discussion in Europe regarding the off-label use of drugs mainly aims at the increased risks for patient safety of medicinal products which are used without indication (this is also the understanding of the view of the EMA16 in its concept paper on conduct of pharmacovigilance for medicines used by children “not licensed for such use”) or otherwise deviating from the technical information (eg, in terms of dosage, the dosage form, the consideration of contraindications, etc).1,17 Because there is, at most, a gradual but no qualitative difference in medicinal products which have not yet received regulatory approval, by an expanded understanding of the concept, also the so-called “off-license” or “unlicensed use” (section 67 of the British “good practice in prescribing and managing medicines and devices”, entered into force on March 25, 2013), is included. If the medical product is provided for “humanitarian reasons to a group of patients suffering from a debilitating and chronic or serious illness or whose disease is considered to be life-threatening” (Article 83, subsection 2 of the EU regulation number 726/2004), it is regarded as a special form, the so called “compassionate use.”
The basic problem is easy to illustrate: on the one hand, drugs (such as any form of medical treatment) shall guarantee the highest possible level of safety and effectiveness in order to alleviate the suffering of patients and not to increase it. On the other hand, there are sometimes no precisely fitting drugs for a concrete case or the existing spectrum of drugs is soon exhausted without providing adequate help to the patient. In this situation, the treating physician is trapped in a difficult dilemma: because of his professional duties, he does not want to leave the patient without a cure (and is sometimes even not allowed to if he wants to avoid an omission offence). But if the physician wants to administer not sufficiently proven medicinal products, they assume all the risks, which the regulatory drug approval process as well as medical malpractice law (focused on the medical “standard”) should normally prevent for the patients’ protection.
Pharmaceutical law
It was essentially the thalidomide scandal which, in Germany as well as in other European countries, sustainably caused the implementation of a tight net of rules for preventive controls of the production and marketing of pharmaceuticals. In contrast to general product liability, which compensates damages in retrospect, adverse drug effects should preferably be discovered and averted before the first damage. The central element of the legal assurance is the requirement of an official authorization or approval (eg, section 21 AMG [German medical law]), see also Article 6, section 1 of the EU directive 2001/83/EC), which is only granted if the drug has been tested analytically (chemically, physically, biologically) as well as toxicologically and pharmacologically (also on humans). In Germany, the disregard of this rule leads (if intended) to a criminal penalty or, in case of negligence, to administrative fines (section 96, number 5, 97 subsection 1 AMG). However, this is only the case if the drug has been delivered in a way that provided the patient power of disposal over the drug (“placing on the market”, see section 4 subsection 17 AMG). The immediate off-label use of the drug by the patient, however, does not constitute a “discharge” in this sense, because the lack of authorization does not limit the medical treatment decision but only the abstract marketability of the drug.18 The same applies to the medical prescription; if the prescription is obtained for a medicinal product that is liable for registration but still has no authorization, criminal liability of the prescribing physician for incitement or complicity in the illicit placing on the market would certainly be possible if the discharge does not correspond with the rules of compassionate use. When the (currently clinical tested) drug is provided for free, and a severe or life-threatening disease cannot be treated satisfactorily by an authorized medicinal product, there is an exception of the authorization requirement according to section 21, section 2, number 6 AMG.
As in Germany, other European countries have partially omitted special statutory regulations for off-label use (as in the UK, but here the UK General Medical Council’s professional legal guidelines require the conviction of the prescribing physician of the efficiency and safety of off-label use and the existence of sufficient evidence or experience for this).19 In contrast, some countries adopted special statutory regulations, thus we can find in Article 9 of the Swiss federal law on medicinal products and medical devices the possibility for a temporary regulatory exemption for the delivery of nonapproved drugs if they shall be used against life-threatening diseases, a great therapeutic benefit can be expected while respecting the health protection, and if there is no comparable medicinal product available. Additionally, (according to Article 26, Swiss Federal Law) physicians always must consider the recognized rules of medical and pharmaceutical sciences if they want to prescribe and dispense such a drug. This means, that a medical specialist has in any case to prove the medical indication on the basis of a careful diagnosis. A think-tank consisting of Swissmedic, the hospital pharmacists, and representatives of the cantons solidified the medical and pharmaceutical care duties in a work report.20 In case of following these rules, the off-label use is permitted exceptionally by law, regardless of the authorization requirement existing by itself.21
In the wake of a recent medicinal product scandal, France has created a more restrictive version of such an “authorities solution”: for off-label drug delivery, the law number 2011-2012 from December 29, 2011 and the regulation to “temporary recommendations for use” (TRU) (regulation number 2012-743, TRU) demand the permission from an expert committee, Agence Nationale de Sécurité du Médicament et des Produits de Santé (ANSM), which is limited to 3 years. This permission includes the contractual commitment to scientific observation and evaluation.22 A TRU can be granted according to the following criteria: quality of the scientific evidence, general safety of the drug, and severity and commonness of the disease. The pharmaceutical company has to ensure the course of monitoring, the compliance with the operating demands, and the collection and assessment of information, which must be passed on to the ANSM. Equally, the company has to inform the ANSM if there is a violation of the foreseen procedure. If there are any emerging health risks, the ANSM can modify, suspend, or even cancel the TRU (for more information on this issue, see the ANSM principles for TRU23). However, most European states do not have a formal or legal preventive control and can therefore only name the material conditions for an off-label use by law or case-law (eg, Article 3, subsection 2 of the Italian law 94/98 (Legge di Bella); Spanish law 41/2002 and royal decree 1015/2009, section 8, subsection 1, number 2 Austrian AMG; and section 6 of the guidelines on the economic prescription of medicines and medical aids).24–26 In addition to the absence of an on-label indication, the patient has to be informed about the special character of the off-label treatment and a reasonable prospect of success must be given (according to the Italian law 244/2007 [Legge Finanziaria 2008] at least based on a Phase II study). In some cases, there is additionally an abstract-general limitation that the respective disease has to be life-threatening or leads to a severe health hazard (section 8, subsection 1, number 2 Austrian AMG) (For an overview, Table 1).
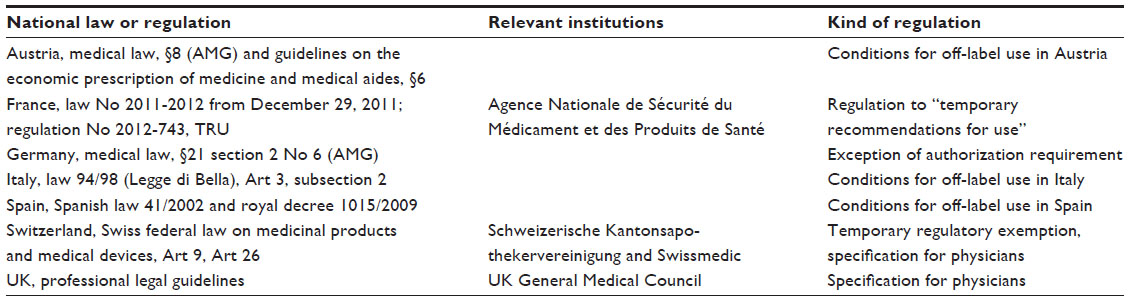 | Table 1 Overview of national regulation for off-label use in selected European countries |
Tort law
Common principles of medical jurisprudence demand that, in order to avoid a liability or even criminal punishment, any deviation from medical standards (the “recognized and backed up status of medical sciences”27 (section 839 BGB Rn 6, German Civil Code) has to follow special preconditions. Firstly, there has to be a compelling reason for choosing a less secure method, and secondly, additional security measures are necessary which can compensate an increased treatment risk. Consistently, the German Federal Court judged as follows:
The choice of therapy is primarily in the physician’s responsibility […]; not always the physician has to choose the safest therapeutic way. However, a larger risk must be justified in the specific circumstances of the case or in a more favorable healing prognosis […]; and the physician must proceed more carefully, the more a mistake can affect the patient. (Translation by the authors).28
To avoid prosecution for medical malpractice, the intension of a very “careful physician” has to be demonstrated. If a drug is used in the case of a disease for which it is not sufficiently tested, an increased level of caution (especially regarding the dose) and monitoring must be shown to be aware of warning signals and to be able to react immediately. However, the lack of approval does not automatically mean a departure from the “standard.” This standard can also be met in the case of an off-label use when there is sufficient practical proof.17 In this case, the nonuse of the drug can lead to liability, and even to a criminal punishment for assault by omission (OLG Köln NJW-RR 1991, 186;18 the verdict claims in individual cases a duty for off-label treatment even beyond the foreseen standard treatment: BGH NJW 1991, 1543).18
If for this purpose an unapproved drug with unknown risks is used, it has further consequences regarding the patient’s information from the perspective of the physician (see also Article 3, subsection 2 of the Charter of Fundamental Rights of the European Union): the patient has to be adequately informed about the lack of authorization and the possible existence of unknown risks. Only under these circumstances does the patient have the possibility to estimate whether they want to be treated with a conventional (tested/approved) drug or the new preparation, which gives them the chance of a better result, but at the same time, bears the danger of unknown risks.28 The patient must be made aware of the existing alternative to make an “informed” decision. In general, “The more […] it is intended to deviate from the generally accepted practice […], the more thoroughly the patient must be informed – there is a close correlation between the choice of method and the obligation to inform.”29 The physician also has a duty to inform the patient when the health insurance provider could refuse reimbursement of costs, as well as the level of costs due to the off-label status of a treatment (so-called economic information; see section 630c, subsection 3, sentence 1 German Civil Code; for Switzerland BGE 130 V 532; for Austria26). Notwithstanding increased preventive and protective measures, if the health of the sufficiently informed patient is damaged due to an off-label drug use, only the pharmaceutical manufacturer can be sued. However, the liability risk in section 84 AMG (German drug law) is only relevant when there is a “proper use” of the drug, as it results from the labeling, package leaflet, and expert information. By including contraindications, warnings, and especially by defining the areas of application, the manufacturer can limit the intended use and can nearly release itself from liability.17,18 However, a different situation occurs when in the meantime the drug has become part of a scientifically recognized therapy practice with the manufacturer’s knowledge.30 Consequently, the manufacturer would then also be liable for such use of the drug. However, an occasional off-label use that has not yet become a general therapy does not establish recognition of the manufacturer’s liability. In those cases, compensation could only be collected from an existing clinical trial insurance when it covers a drug’s off-label-use.31
The law of health insurance
The off-label application of medicinal products is usually done outside the framework of clinical studies; therefore, normally, no trial insurance exists. The practical recognition of an off-label use in medical practice depends on its financial sustainability. For patients with a private health insurance (in the German or other “two-tier” insurance systems), it is not difficult because “well-founded off-label prescriptions” can be easily included in the insurance. According to the German Federal Court, there is a legitimate interest for patients to use drugs not belonging to so-called conventional medicine, which have proven to be promising in practice for the benefit of patients. Due to this rationale, the older science clauses in German Law (“no obligation for treatments scientifically not generally recognized …”) were declared as legally invalid (BGHZ 123, 83; 152, 262).32,33 The situation is more complex in the context of the German public health care insurance: here, the Federal Social Court in Germany made strict requirements for proof of efficacy of drugs that are administered off-label. First, there has to be serious disease, which is life-threatening or strongly affects the patient’s health-related quality of life. Additionally, there exists no other possible therapy, and there must be a “reasonable expectation”, based on the available data, that the product in question is the key to successful treatment (curative or palliative). This “reasonable expectation” is only given when either the extension of the authorization has already been applied for and the results of a controlled Phase III clinical trial demonstrate clinically relevant efficacy, or if there are findings which were recovered and published out of the authorization process, leading to a professional consensus on the likelihood of benefit with acceptable risks.34
By providing much lower requirements for a proof of efficacy, the so-called “Nicholas decision” of the German Federal Constitutional Court changed the legal situation clearly in favor of the patient.35 According to this decision, circumstantial evidence is sufficient to show a not very unlikely prospect of cure or a significant positive effect on the disease process, and when the serious indications exist for the judgment of a conscientious physician (BVerfGE 115). This judgment has now been brought into law (German Federal Constitution Court section 2, subsection 1a German Social Security Code, Book V). Additionally, the German Federal Social Court has adapted its jurisdiction considerably and extended this patient-friendly legal situation to treatment circumstances having urgent necessity beyond a life-threatening illness or disease.36,37 Today, in addition to the requirement of an acute need for treatment, and in order that unlicensed medicines may not be prescribed at the expense of the statutory health insurance, it is necessary that 1) the pharmaceutical legislation is not violated, 2) a general and specific risk-benefit analysis was made, and 3) sufficient documentation is guaranteed and the insured person has agreed after receiving specific treatment information. The German legislator has created section 35c German Social Security Code, Book V for authorizing the establishment of expert groups, who are called to provide scientific reviews in order to give a broader scientific basis to assumptions of benefits. But it is rather doubtful whether this instrument can adequately fulfil the complexity of the diverse issues of a necessary off-label-use.1
The dilemma between desired security and necessary flexibility is also evident in other European countries: In October 2012, the British National Institute for Health and Clinical Excellences38 published the first “evidence summaries” for the unlicensed or off-label use of drugs; however, these summaries are not legally binding. Their task is to reduce the existing information gaps.39 In Austria, only those drugs named in a “positive list” are covered (similar to the demands made by the ESMO), but the key criterion is not the regulatory drug approval, but the predicted benefits and ongoing treatment need.17,26,27 The courts did not restrict the practice of off-label use to life-threatening or otherwise serious diseases. In this approach, there is also no necessity for a scientifically valid study to demonstrate a drug’s effectiveness. It is sufficient for the drug to be seen as promising by a specialized medical assessment (Oberster Gerichtsh of Österreichs [Austria High Court] decision March 26, 1996 and April 29, 2003).40,41 In Switzerland, the requirements are higher: according to the controversial “Pompe disease” judgment by the Swiss Federal Court, cost coverage beyond the drugs recorded on a so-called “list of specialties” is possible if there is a scientifically proven “high therapeutic value” for cases of life-threatening or chronic disease, and even then only in cases where a “reasonable cost-benefit ratio” exists. The limitation of necessary life-supporting therapy for reasons of the cost-effectiveness requirement has triggered a very controversial discussion across borders and stimulated conversation in Germany.42,43
Conclusion
The overview in the present article shows a range of activities within the European Commission and within single European countries as well. On the European level, the setting of economic and patent incentives, especially in the case of pediatric drugs, was the decisive approach. However, a convincing proof of this strategy could not, according to official EU documents, be furnished at the present time. This leads to the question of whether a more direct and active approach should be chosen to fulfil the ethical and legal demand of safe and tested drugs for all patient groups. Our review of national discussions and regulations in Austria, France, Germany, Spain, the UK, and Switzerland shows consistently that the off-label use of drugs poses in all countries a problem in the medical supply to patients. However, the different countries took different paths to handle the problem and to moderate its negative effects. Due to the dependency of a country’s off-label situation on the national drug regulation (a drug may have a different authorization status in different countries) it is necessary for the different countries to find a national solution, especially in the areas of pharmaceutical law and health insurance law. Our overview shows that there are mainly two kinds of solutions which can be implemented as an interim arrangement. Firstly, a consensus list of accepted off-label uses, backed up by scientific evidence, would at least partly relieve the work of physicians in the field. Such a list could also be administered by the EMA with scientific support from the different European member states. The second solution, as practiced in France, is the evaluation and approval of specific off-label uses by an official expert group. Both solutions would have, from our point of view, the effect of helping physicians handle the ethical and legal paradoxes associated with the off-label use of drugs. At the same time, this would probably lead to a more safe and homogeneous medical supply for the concerned patients. For European citizens, a harmonized approach would presumably be of even greater value. Therefore, a discussion should be initiated at the European level to address which measures could be adopted to realize a direct improvement of the current off-label drug use situation.
Disclosure
The authors report no conflicts of interest in this work.
References
Klein B, Arzneimittelrechtliche Betrachtungen des Off-Label-Use, [Observations from pharmaceutical legislation on the off-label use of drugs]. Hamburg 2009. | |
European Medicines Agency (EMA) 2013: Guideline on good pharmacovigilance practices (GVP) Annex I - Definitions (Rev 2). EMA/876333/2011 Rev 2*. | |
Neubert A, Wonga I, Bonifazi A et al. Defining off-label and unlicensed use of medicines for children: Results of a Delphi survey. Pharmacological Research. 2008;316–322. | |
Chalumeau M, Tréluyer JM, Salanave B, et al. Off label and unlicensed drug use among French office based paediatricians. Arch Dis Child. 2000;83(6):502–505. | |
Bücheler R, Meisner C, Kalchthaler B, et al. [“Off-label” prescribing of drugs in the ambulatory care of children and adolescents]. Dtsch Med Wochenschr. 2002;127(48):2551–2557. German. | |
Culshaw J, Kendall D, Wilcock A. Off-label prescribing in palliative care: a survey of independent prescribers. Palliat Med. 2013;27(4):314–319. | |
Martin-Latry K, Ricard C, Verdoux H. A one-day survey of characteristics of off-label hospital prescription of psychotropic drugs. Pharmacopsychiatry. 2007;40(3):116–120. | |
Liang BA, Mackey T. Health care policy. Reforming off-label promotion to enhance orphan disease treatment. Science. 2010;327(5963):273–274. | |
European Commission. Better Medicines for Children: From Concept to Reality. Brussels: European Commission; 2013. Available from: ec.europa.eu/health/ files/paediatrics/2013_com443/paediatric_report-com(2013)443_en.pdf. Accessed April 15, 2104. | |
Regulation [EC] number 141/2000 of the European Parliament and the Council of December 16, 1999 on orphan medicinal products. | |
Lenk C. Off-label drug use in paediatrics: a world-wide problem. Curr Drug Targets. 2012;13(7):878–884. | |
Casali PG; Executive Committee of ESMO. The off-label use of drugs in oncology: a position paper by the European Society for Medical Oncology (ESMO). Ann Oncol. 2007;18(12):1923–1925. | |
Hoppu K. Paediatric clinical pharmacology: at the beginning of a new era. Eur J Clin Pharmacol. 2008;64(2):201–205. | |
Lenk C, Koch P, Zappel H, Wiesemann C. Off-label, off-limits? Parental awareness and attitudes towards off-label use in paediatrics. Eur J Pediatr. 2009;168(12):1473–1478. | |
Penfold RB, Kelleher KJ, Wang W, Stange B, Pajer K. Pediatric uptake of a newly available antipsychotic medication. Pediatrics. 2010;125(3):475–482. | |
European Agency for the Evaluation of Medicinal Products. Concept Paper on Conduct of Pharmacovigilance for Medicines Used by Children. London: European Agency for the Evaluation of Medicinal Products; 2002. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2009/09/WC500003765.pdf. Accessed April 15, 2014. | |
Rückeshäuser P, Off-Label-Use: Die rechtlichen Probleme des zulassungsüberschreitenden Einsatzes von Arzneimitteln, [The legal problems of drug application beyond the licensed use]. Hamburg. 2011. German. | |
Müller H. Die Rechtsproblematik des Off-Label-Use, [The legal problem of off-label drug use]. Berlin: LIT-Verlag; 2009; 1991, 186. German. | |
Plate V. The Impact of Off-Label, Compassionate and Unlicensed Use on Health Care Laws in Preselected Countries [dissertation]. 2009; Bonn: Universität Bonn. Available from: http://hss.ulb.uni-bonn.de/2009/1936/1936.pdf. Accessed April 15, 2014. | |
Schweizerische Kantonsapothekervereinigung und Swissmedic. Ausführungen der Schweizerischen Kantonsapothekervereinigung und der Swissmedic betreffend des Einsatzes von Arzneimitteln im Sinne des off label use. [Remarks concerning the application of pharmaceutical in the sense of off-label use]. Basel: Schweizerische Kantonsapothekervereinigung und Swissmedic; 2006. Available from: http://www.gesundheitsdienste.bs.ch/print/hmw_offf-label-use_schlusspapier_06-07-24d1.pdf. Accessed April 15, 2014. German. | |
Widmer S. Off-label-use in der Schweiz: heilmittelrechtliche Zulässigkeit und Kostenübernahme. [Off-label use in Switzerland: legitimacy according to pharmaceutical law and reimbursement] [webpage on the Internet]. Zeitschrift für Recht und Gesundheit; 2013. Available from: https://hill.swisslex.ch/JournalPortal.mvc/AssetDetail?assetGuid=8d84b61f-e45c-4820-b48f-8f8083a14225. Accessed April 15, 2014. German. | |
Emmerich J, Dumarcet N, Lorence A. France’s new framework for regulating off-label drug use. N Engl J Med. 2012;367(14):1279–1281. | |
Agence Nationale de Sécurité du Médicament. Temporary Recommendations for Use: Principles and Information on the Methods Used by the ANSM for Establishment and Implementation. Saint Denis: Agence Nationale de Sécurité du Médicament; 2012. Available from: http://ansm.sante.fr/var/ansm_site/storage/original/application/e8daacd4d465d71e95a6333d8af9b461.pdf. Accessed May 1, 2014. | |
Guidi B, Nocco L. The debate concerning the off-label prescriptions of drugs: a comparison between Italian and US law. Op J. 2011;1(1):45. | |
Molyneux CG, Bogaert P. The need for informed consent in off-label use in the EU. Scrip Regulatory Affairs. 2010:13–16. | |
Sieb M, Strasser S. Rechtliche Situation von Off-Label Use bis Heilversuch [Legal situation from off-label use to individual attempt for cure]. Wiener Klinisches Magazin. 2009;12(6):20–24. German. | |
Greiner HP. Kommentierung des Arzthaftungsrechts (§ 823 BGB), [Commentary on medical liability law]. In: Spickhoff A, editor. Medizinrecht Kommentar [Medical Law. Commentary]. München: Beck; 2011. | |
Bundesgerichtshof [BGH, German Federal Court], Urteil vom 22.5.2007 – VI ZR 35/06 – BGHZ 172, 254. | |
Grupp K. Rechtliche Probleme alternativer Behandlungsmethoden, [Legal problems of alternative treatment methods]. Medizinrecht. 1992;10(4):256–263. German. | |
Schwee M. Die Zulassungsüberschreitende Verordnung von Fertigarzneimitteln (Off-Label-Use), [The prescription of proprietary medicinal products beyond the licensed use]. Frankfurt am Main: Lang; 2008. German. | |
Deutsch E, Spickhoff A. Medizinrecht [Medical Law]. 6th ed. Berlin/Heidelberg: Springer; 2008. German. | |
Bundesgerichtshof [BGH, German Federal Court], Urteil vom 23.9.1993 – VI ZR 135/92 – BGHZ 123, 83. | |
Bundesgerichtshof [BGH, German Federal Court], Urteil vom 30.10.2002 – VI ZR 60/01 – BGHZ 152, 262. | |
Bundessozialgericht [BSG, German Federal Social Court], Urteil vom 19.3.2002 – B 1 KR 37/00 R – BSGE 89, 184. | |
Bundesverfassungsgericht [BVG, German Federal Constitution Court], Beschluss vom 6.12.2005 – 1 BvR 347/98 – BverfGE 115, 25. | |
Bundessozialgericht [BSG, German Federal Social Court], Urteil vom 4.4.2006 – B 1 KR 7/05 – BSGE 96, 170. | |
Bundessozialgericht [BSG, German Federal Social Court], Urteil vom 5.5.2009 – B 1 KR 15/08 – Neue Zeitschrift für Sozialrecht 2010, 392. | |
Evidence summaries: unlicensed/off-label medicines [webpage on the Internet]. London: National Institute for Health and Care Excellence [updated May 6, 2014]. Available from: http://www.nice.org.uk/mpc/evidencesummariesunlicensedofflabelmedicines/home.jsp. Accessed April 15, 2014. | |
Shkopiak T. Unlicensed and Off-label Use of Medicines in the UK – A Balancing Act. London: Taylor Wessing LLP; 2012. Available from: http://www.taylorwessing.com/fileadmin/files/docs/InFocus_Unlicensed-and-off-label-use-of-medicines-in-the-UK.pdf. Accessed April 15, 2014. | |
Oberster Gerichtshof Österreichs [Austria High Court], Beschluss vom 26.3.1996 – 10 Obs 52/96 – SZ 69/80. | |
Oberster Gerichtshof Österreichs [Austria High Court], Beschluss vom 29.4.2003 – 10 Obs 409/02y – RIS Nr. | |
Duttge G, Zimmermann-Acklin M, Gerecht sorgen. Verständigungsprozesse über den Einsatz knapper Ressourcen bei Patienten am Lebensende [Just care. Agreement processes on the use of scarce resources in the case of patients at the end of life]. Universitätsverlag Göttingen; 2013. German. | |
Huster S, Das “Morbus-Pompe”-Urteil des Schweizerischen Bundesgerichts (MedR 2012, 324) – eine Diskussion aus rechtlicher, sozialmedizinischer und Medizinethischer Sicht [The “Morbus-Pompe-Verdict” of the Swiss Federal Court – Remarks from the German Law’s point of view]. Medizinrecht. 2012;30(5):289–291. German. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.