")
Back to Journals » Clinical Epidemiology » Volume 13
Estimation of Risk of Death Attributable to Acute Gastroenteritis Not Caused by Clostridioides difficile Infection Among Hospitalized Adults in England
Authors Alexandridou M, Cattaert T, Verstraeten T
Received 11 December 2020
Accepted for publication 18 March 2021
Published 23 April 2021 Volume 2021:13 Pages 309—315
DOI https://doi.org/10.2147/CLEP.S296516
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Vera Ehrenstein
Maria Alexandridou, Tom Cattaert, Thomas Verstraeten
P95 Pharmacovigilance and Epidemiology Services, Leuven, Belgium
Correspondence: Thomas Verstraeten Email [email protected]
Introduction: The role of an infectious agent may be unclear as the primary cause of death. Furthermore, many infections go undiagnosed, particularly if identification does not affect treatment. To circumvent the limitations of individual death attribution, a population-level assessment of the role of infectious acute gastroenteritis (AGE) was performed.
Methods: Using the Clinical Practice Research Datalink and the Office for National Statistics – Mortality Statistics, covering 16 million patients in the UK, we conducted a matched case–control study to estimate the odds of having AGE not due to Clostridioides difficile infection (CDI) diagnosed in the month before death among hospitalized adults in England. To estimate the number of deaths, we first estimated the attributable fraction (AF). The population attributable fraction (PAF) was then derived by multiplying AF with the proportion of AGE hospitalizations among all hospitalizations. Finally, by multiplying the PAF with the number of deaths, the number of deaths attributable to AGE not caused by CDI among hospitalized patients was estimated.
Results: The odds of having AGE not caused by CDI was 4.6 times higher among fatal compared to non-fatal hospitalizations. The overall PAF was 1.7% for AGE not caused by CDI. The overall number of deaths attributable to AGE not caused by CDI among adults in England is estimated to be 5000 annually.
Discussion: Approximately 5000 of the 276,000 deaths that occur annually among hospitalized adults in England can be attributed to AGE not caused by CDI, which is higher than previously estimated.
Keywords: acute gastroenteritis, CPRD, England, population attributable fraction
Introduction
Acute gastroenteritis (AGE) is an important cause of morbidity across all ages worldwide. It is estimated that in the UK approximately 17 million cases of AGE and 1 million general practitioner (GP) consultations for AGE occur per year.1 And in the United States, the number of AGE cases was estimated at 179 million in 2010,2 and 274 million cases per year between 2005 and 2014, although a decrease was seen over time in this study.3 Acute gastroenteritis can be caused by a range of viruses, bacteria, parasites, and fungi;4 however, in most cases the pathogen causing AGE goes unidentified due to lack of testing.5
The Global Burden of Disease study estimated that diarrhea was a leading cause of death, with 1.7 million deaths in 2016.6 Clostridioides difficile is one of the more frequently identified pathogens causing AGE, in particular in hospitalized patients,5 possibly because of recognized risk factors in patients, including recent antibiotic use, hospitalization, or advanced age, that may prompt testing.7 C. difficile infection (CDI) is the most frequently identified healthcare-associated infection in high-income countries including the United States7 and is also an important cause of mortality. In 2004 the age-standardized mortality rate for CDI was 17 per million population, or 89 deaths, in Finland,8 and 24 per million population, or nearly 7000 deaths, in the United States.9 Death rates for AGE due to infectious pathogens other than Clostridioides difficile are not well defined. Some studies have assessed a limited number of other causes such norovirus and Salmonella.10,11
It is recognized that infections as proximal causes of death are underestimated.12 Mortality statistics rely on the use of death certificates as a primary data source,12 and hence, on the assessor’s judgement and perception of the importance of the different processes that may have led to death. Death certificate data generally emphasize the burden of chronic disease; however, a clear majority of deaths occur during hospitalizations for reasons quite different from the reported underlying cause of death.12 Death due to an infectious agent in particular is often not put forward as the primary cause.13 A study from the United States estimates that from 17-to-19% of inpatient deaths attributed to heart disease, cancer and stroke by death certificates, actually occur during hospitalization for infectious causes.12 The same study also suggests that hospital records for patients who died during an inpatient hospitalization “paint distinct and complementary impressions about mortality”.
To assess the role of AGE as a cause of death in hospitalized adult patients, we performed a matched case–control study, using routinely collected medical datasets.
Methods
Data Sources
We analyzed data from the Clinical Practice Research Datalink (CPRD), linked to data from the Hospital Episode Statistics Admitted Patient Care (HES APC) and the Office for National Statistics – Mortality Statistics (ONS, https://www.ons.gov.uk) databases. The CPRD is a primary healthcare database containing anonymized medical records for over 16 million patients attending 691 general practitioners (GPs) in the UK (release January 2016). The HES APC database contains records of all hospital admissions in England.
Study Design
As we anticipated that infectious AGE episodes are more likely to be diagnosed in hospitalized patients than non-hospitalized patients, we expected an important diagnostic bias to occur in a study that would include all deaths, irrespective of hospitalization. Moreover, given that the majority of deaths (60%) in the UK occur in hospitalized patients,14 we limited the study to these patients.
We conducted a matched case–control study. We considered as cases all adults who died within 30 days of discharge, between January 1st, 2006 and December 31st, 2014. The date of death served as index date. Using risk-set sampling, each case was matched to one control selected from hospitalized adults who did not decease within 30 days after discharge. Matching occurred 1:1 on gender, year of birth, calendar time of the index date, and Charlson’s comorbidity score 30 days before cases’ death (index date). The Charlson’s comorbidity score is a method of categorizing patients based on the presence of categories of comorbidities. Each comorbidity category has an associated weight (from 1 to 6), based on the adjusted risk of mortality or resource use, and the sum of all the weights results in a single comorbidity score for a patient, with a higher score predicting a higher likelihood of mortality or higher resource use. Cases and controls were matched on their exact Charlson’s comorbidity scores. The predictive value of the Charlson’s comorbidity score for mortality was recently shown in the Finnish National Care Register for Health Care (HILMO), which is comparable to the HES database.15
Exposure
An AGE episode was defined as a series of at least one AGE event (ICD-10 codes A00.0-A09.9, excluding A06.4-A06.7, and K52.8-K52.9, and their Read code counterparts, see Supplemental Table 1), with the lag time between successive events not exceeding 14 days. Hence, a recurrence with a lag time of more than 14 days was considered as a new AGE episode. The episode index date was the date of the first AGE event of the AGE episode. AGE episodes were classified as primary care-only or requiring hospitalization based on the level of care required over the course of the episode. Any episode containing at least one AGE event from HES Inpatient was classified as requiring hospitalization. An AGE caused by CDI was identified as an AGE with the code A04.7 (for Read code counterparts, see Supplemental Table 2). For the timing of exposure ascertainment relative to the index date, a period of 30 days was chosen, as a rather standard time to look at the immediate effect of a relatively short-lived infectious disease, in analogy to 30-day mortality.16 AGE will usually be limited to a few days in healthy persons but can be prolonged in frail individuals and thus contribute to death beyond its acute stage.
Inclusion Criteria
Cases and controls were eligible for inclusion if: 1) they had been registered in the CPRD database for at least 6 months; 2) their GP practice had been classified as “up to standard” for at least 6 months; and 3) subjects were eligible for HES linkage. To include all deaths, ONS and HES were combined, as both report deaths regardless of cause of death.
Ethics
The study protocol was approved by the MHRA Independent Scientific Advisory Committee [ISAC protocol. 16_063R]. Study-specific patient informed consent was not required. The CPRD has been granted Multiple Research Ethics Committee approval (05/MRE04/87) to undertake purely observational studies, with external data linkages including HES and ONS mortality data. The work of CPRD is also covered by NIGB–ECC approval ECC 5-05 (a) 2012.
Analysis
The association between death and diagnosis in the preceding 30 days of AGE not caused by CDI (AGE-nonCDI) was estimated with odds ratio (OR) using a conditional logistic regression model (not adjusting for other variables). To estimate the number of deaths due to AGE-nonCDI among adults in England, we first estimated the attributable fraction (AF) under the rare disease assumption, using the formula AF = (OR-1)/OR. The population attributable fraction (PAF) was then derived by multiplying the AF with the proportion of AGE-nonCDI hospitalizations among all hospitalizations. Finally, by multiplying the PAF with the number of deaths among hospitalized adults in England,14,17 the absolute number of deaths attributable to AGE-nonCDI among hospitalized patients was estimated. In addition, we performed the same exercise for AGE caused by CDI. As we believe CDI is a well identified cause of death and likely to be accurately diagnosed and recorded in death registers, we compared the estimates for AGE caused by CDI using our methodology to the reported numbers as a positive control. All analyses were stratified by age, with the age categories 18–64 years, 65–74 years, 75–84 years and 85+ years, using a category for younger adults (18–64 years) in line with prior analyses of mortality due to infectious causes, and more granular age groups for the elderly.
Results
Population Description
Between January 2006 and December 2014, the CPRD and ONS databases included 212,399 death records for adults. Using the hospitalization data, we could match 35,219 deaths (cases) to an identical number of controls who survived and were hospitalized in the same period. The number of deaths varied by age group: 2163 in the age group 18–64 years; 4,313 in the age group 65–74 years; 11,813 in the age group 75–84 years; and 16,930 in the age group 85+ years (Table 1).
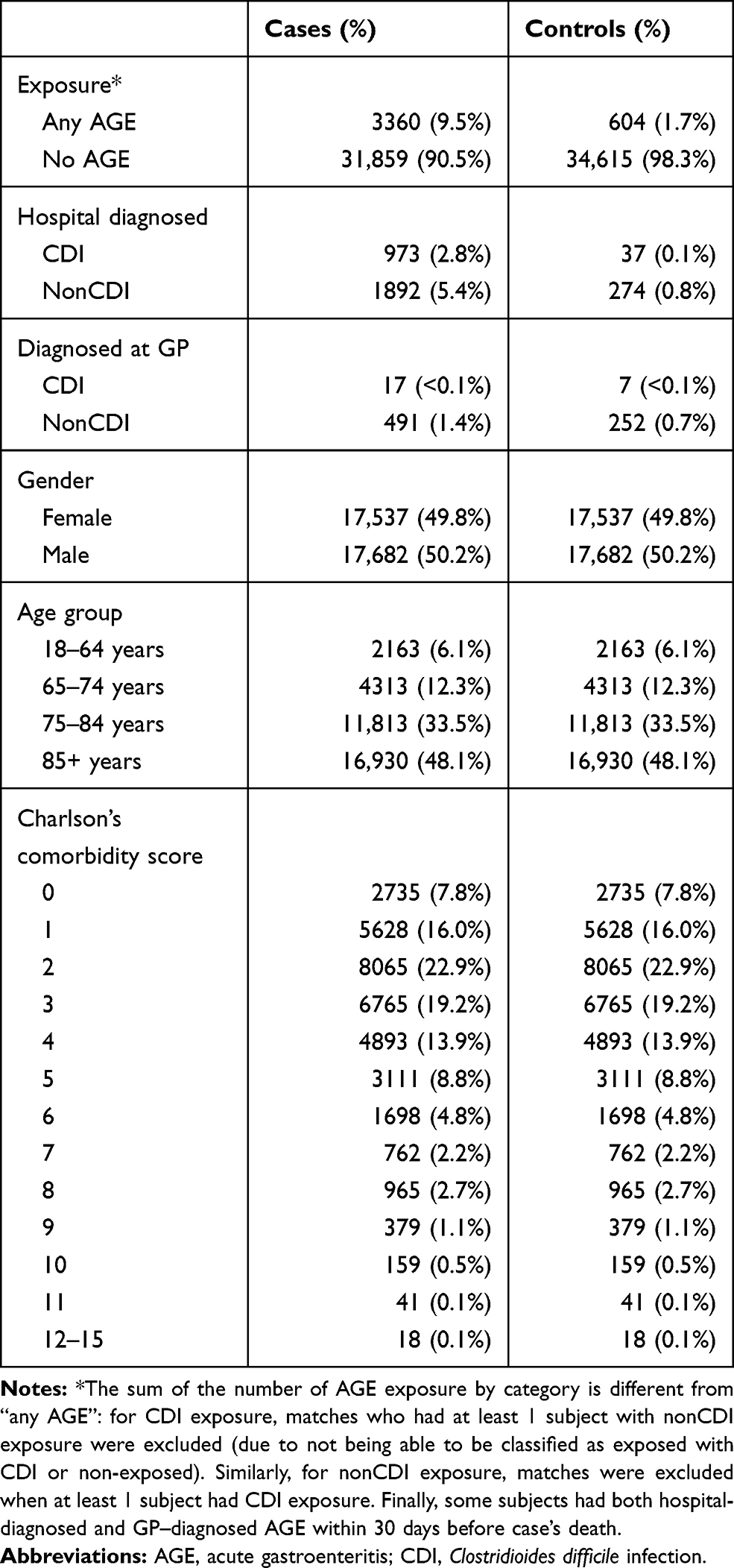 |
Table 1 Summary of AGE Diagnosis, Age Category, Gender and Charlson’s Comorbidity Score of Cases and Controls |
Diagnosis of AGE-NonCDI in Patients Who Died versus Those Who Survived
A total of 3360 cases (9.5%) and 604 controls (1.7%) had an AGE diagnosis in the 30 days before the index date. The majority of AGE episodes were diagnosed in hospital (3176 out of 3964 subjects, or 80.1%). The estimated odds ratios (OR) of having an AGE episode not caused by CDI in the 30 days prior to dying, among the hospitalized patients was 4.6 (95% CI: 4.2–5.1) across all age groups (Figure 1). The OR was higher when the episode was diagnosed in hospital (OR 7.2, 95% CI: 6.4–8.3) than when diagnosed by the GP (OR 2.0: 95% CI 1.7–2.3). The OR for a hospital-diagnosed episode of AGE-nonCDI in patients who died versus survived, was significantly lower in patients aged 18–64 years than in older patients. This trend was not observed when the episode was GP-diagnosed.
 |
Figure 1 The odds ratios of mortality in hospitalized patients following non-C. difficile AGE diagnoses by age group. Abbreviations: AGE, acute gastroenteritis; GP, general practitioner; OR, odds ratio. |
Number of Deaths Attributable to AGE-NonCDI
The overall PAF was 1.7% for any AGE-nonCDI. The highest PAF was observed in the 85+ years age group, where the PAF was 2.6% for any AGE-nonCDI (Table 2). The overall number of deaths attributable to AGE-nonCDI in adults was estimated at 5000 annually, with nearly half (2423, 48.5%) occurring in the 85+ years age group.
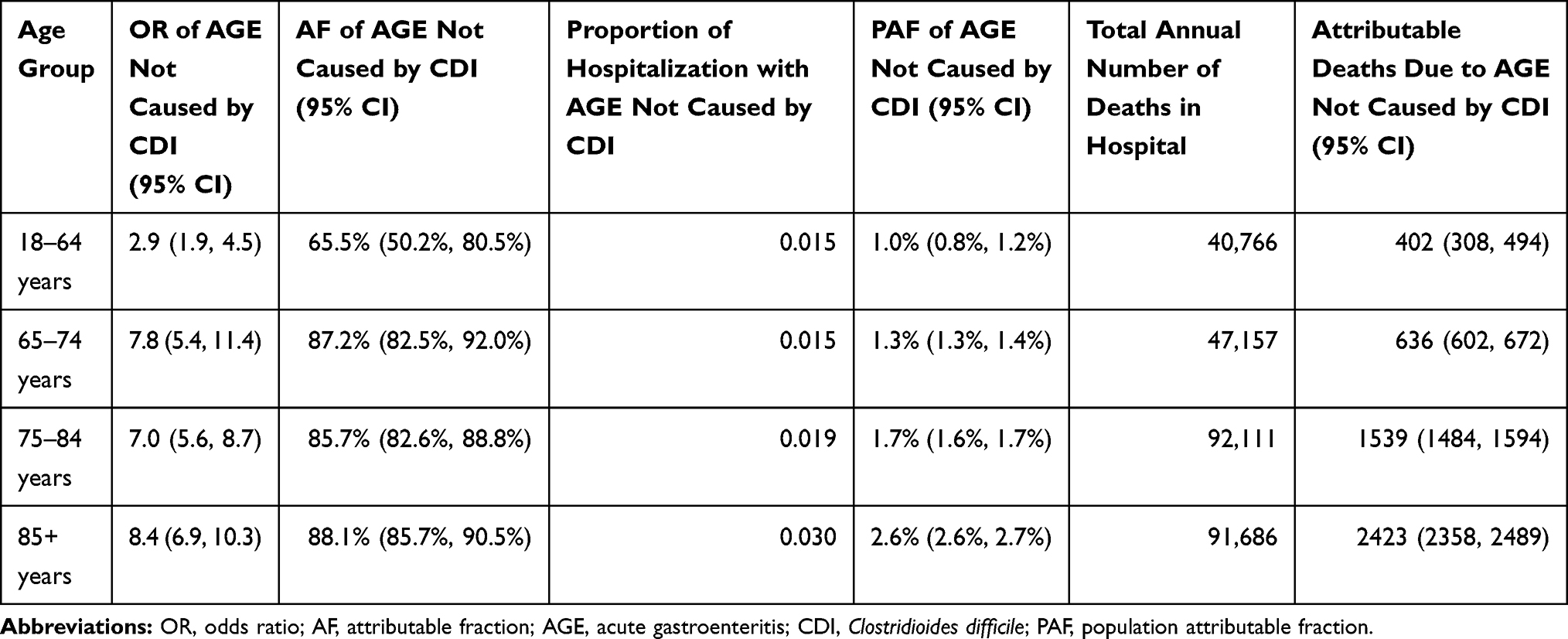 |
Table 2 Estimates of Odds Ratio, Attributable Fraction, Proportion of Hospitalization with AGE Excluding CDI, Population Attributable Fraction, Annual Deaths in Hospital and Attributable Deaths, Due to AGE Not Caused by CDI |
Number of Deaths Attributable to CDI
For AGE caused by CDI, the PAF was 0.14%. The highest PAF, 0.6%, was observed in the 85+ years age group. The overall number of deaths attributable to CDI in adults was estimated at 856 annually. Of these, 566 (66%) occurred in the 85+ years age group.
Discussion
This study aimed to better define the role of AGE in all-cause mortality in hospitalized adults by estimating the odds of having AGE diagnosed in the month before death. Using linked routine datasets, we estimated that every year 5000 deaths in England may be attributable to AGE not caused by CDI, and 856 deaths to CDI. This suggests that AGE caused by pathogens other than C. difficile may contribute to 6-times more deaths than CDI in hospitalized adults in England. Our data also suggest that using death certificates to estimate mortality attribution may significantly underestimate deaths due to AGE. In a study using death certificates (the Office of National Statistics), Harris et al estimated that in England and Wales 400 deaths/year in persons 65+ years were attributable to AGE other than CDI.10 In comparison, we found that AGE other than CDI contributed to 4598 deaths in persons 65+ years.
Norovirus is an important cause of AGE other than CDI. Harris et al estimated, using death certificates, that annually 80 people aged 65+ years in England and Wales die of norovirus-attributable AGE.10 We recently conducted a study using the CPRD and HES databases and a similar methodological approach to model the role of norovirus in AGE in England,5,18 estimating that norovirus caused 11.3% of all AGE hospitalizations.5,18 Applying age-specific rates, we estimated that approximately 565 of the nonCDI deaths in England might be related to norovirus, of which 460 occur in aged 65+ years. This confirms that the number of pathogen-specific AGE deaths are highly underreported, and that linked nationwide datasets can be used to better understand the role of specific pathogens as the causes of death.
Our study has some potential limitations. We did not have access to the actual causes of death in our analyses, but we believe this did not affect our final estimates of the attributable number of deaths. Knowledge of the causes of death would have allowed us to exclude deaths obviously unrelated to AGE. This would likely have led to higher ORs and PAFs. Combined with a lower number of deaths we believe this would in turn have resulted in similar estimates as what we achieved ignoring the causes of death. We cannot exclude that some residual bias may still be present in our estimates of the OR, despite the matching on gender, age, and Charlson’s comorbidity score. This may result in an overestimation of the AGE attributable deaths. When we applied the same approach to AGE caused by CDI, using CDI-specific AGE codes, we estimated 856 deaths to occur annually due to CDI, well below the official estimate of 1899.19 This suggests that our approach did not result in an overestimation of the AGE attributable deaths overall. The relatively low estimate we obtained for deaths due to CDI may also indicate that CDI was under ascertained in the CPRD/HES datasets, leading to an overestimate of the importance of AGE not due to CDI. In our dataset, 26% of AGE was coded as being caused by CDI. As this is higher than the 13% estimate from Sweden,20 and 20% estimate in the Netherlands,21 we believe that such under-ascertainment of CDI is unlikely to have happened. We could not differentiate between community-acquired and hospital-acquired AGE cases as we did not have access to the exact date of the AGE diagnosis. The relatively higher ORs for cases diagnosed at the hospital may be driven by hospital-acquired infections. Finally, as we restricted our analysis to hospitalized adults our study does not account for deaths due to AGE that may have occurred outside the hospital setting, especially for AGEs with an acute onset.
In conclusion, our analyses suggest that the number of deaths among hospitalized adults in England attributable to AGE-nonCDI is higher than previously estimated. Further studies, including microbiological confirmation of AGE among hospitalized patients may be needed to confirm our findings and the role of the different pathogens.
Acknowledgments
The authors would like to thank Anita van den Biggelaar (P95) for editorial assistance and Marc Baay (P95) for publication management. Preliminary results of this paper have been presented at the Vaccines for Enteric Diseases conference, 2017, in Faro, Portugal and at the International Conference of Pharmaco-epidemiology, Montreal, Canada, 2017. The proceedings of the latter meeting were published in Pharmacoepidemiol Drug Saf 2017, 26;S2:1053–8569, https://onlinelibrary.wiley.com/toc/10991557/2017/26/S2.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This study was supported by a grant from the Flemish region government, Belgium, through the Agency for Innovation through Science and Technology (IWT, grant 150274).
Disclosure
MA declares no conflict of interest. TC and TV have received consulting fees from pharmaceutical companies, unrelated to this work. The authors report no other conflicts of interest in this work.
References
1. Tam CC, Rodrigues LC, Viviani L, et al. Longitudinal study of infectious intestinal disease in the UK (IID2 study): incidence in the community and presenting to general practice. Gut. 2012;61(1):69–77. doi:10.1136/gut.2011.238386
2. Hall AJ, Wikswo ME, Manikonda K, Roberts VA, Yoder JS, Gould LH. Acute gastroenteritis surveillance through the National Outbreak Reporting System, United States. Emerg Infect Dis. 2013;19(8):1305–1309. doi:10.3201/eid1908.130482
3. Kim HS, Rotundo L, Nasereddin T, et al. Time trends and predictors of acute gastroenteritis in the United States: results from national health and nutrition examination survey 2005–2014. J Clin Gastroenterol. 2017;51(8):693–700. doi:10.1097/MCG.0000000000000907
4. Troeger C, Forouzanfar M, Rao PC, et al. Estimates of global, regional, and national morbidity, mortality, and aetiologies of diarrhoeal diseases: a systematic analysis for the global burden of disease study 2015. Lancet Infect Dis. 2017;17(9):909–948. doi:10.1016/S1473-3099(17)30276-1
5. Verstraeten T, Cattaert T, Harris J, Lopman B, Tam CC, Ferreira G. Estimating the burden of medically attended norovirus gastroenteritis: modeling linked primary care and hospitalization datasets. J Infect Dis. 2017;216(8):957–965. doi:10.1093/infdis/jix410
6. GBD 2016 Causes of Death Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: a systematic analysis for the global burden of disease study 2016. Lancet. 2017;390(10100):1151–1210.
7. Guh AY, Kutty PK. Clostridioides difficile infection. Ann Intern Med. 2018;169(7):Itc49–itc64. doi:10.7326/AITC201810020
8. Lyytikainen O, Turunen H, Sund R, et al. Hospitalizations and deaths associated with Clostridium difficile infection, Finland, 1996–2004. Emerg Infect Dis. 2009;15(5):761–765. doi:10.3201/eid1505.081154
9. Redelings MD, Sorvillo F, Mascola L. Increase in Clostridium difficile-related mortality rates, United States, 1999–2004. Emerg Infect Dis. 2007;13(9):1417–1419. doi:10.3201/eid1309.061116
10. Harris JP, Edmunds WJ, Pebody R, Brown DW, Lopman BA. Deaths from norovirus among the elderly, England and Wales. Emerg Infect Dis. 2008;14(10):1546–1552. doi:10.3201/eid1410.080188
11. Gibney KB, O’Toole J, Sinclair M, Leder K. Disease burden of selected gastrointestinal pathogens in Australia, 2010. Int J Infect Dis. 2014;28:176–185. doi:10.1016/j.ijid.2014.08.006
12. Govindan S, Shapiro L, Langa KM, Iwashyna TJ. Death certificates underestimate infections as proximal causes of death in the U.S. PLoS One. 2014;9(5):e97714. doi:10.1371/journal.pone.0097714
13. Scallan E, Hoekstra RM, Angulo FJ, et al. Foodborne illness acquired in the United States–major pathogens. Emerg Infect Dis. 2011;17(1):7–15. doi:10.3201/eid1701.P11101
14. Whalley L Report from the steering group for the national review of the hospital standardised mortality ratio, 2010. From the National Health Service, UK.
15. Pylvalainen J, Talala K, Murtola T, et al. Charlson comorbidity index based on hospital episode statistics performs adequately in predicting mortality, but its discriminative ability diminishes over time. Clin Epidemiol. 2019;11:923–932. doi:10.2147/CLEP.S218697
16. Atamna A, Elis A, Gilady E, Gitter-Azulay L, Bishara J. How obesity impacts outcomes of infectious diseases. Eur J Clin Microbiol Infect Dis. 2017;36(3):585–591. doi:10.1007/s10096-016-2835-1
17. Campbell MJ, Jacques RM, Fotheringham J, Maheswaran R, Nicholl J. Developing a summary hospital mortality index: retrospective analysis in English hospitals over five years. BMJ. 2012;344:e1001. doi:10.1136/bmj.e1001
18. Burke RM, Shih SM, Yen C, et al. Burden of severe norovirus disease in Taiwan, 2003–2013. Clin Infect Dis. 2018;67(9):1373–1378. doi:10.1093/cid/ciy298
19. Public Health England. Thirty-day all-cause fatality subsequent to MRSA, MSSA, and E. coli bacteraemia and C. difficile infection. London, UK; 2017.
20. Svenungsson B, Lagergren A, Ekwall E, et al. Enteropathogens in adult patients with diarrhea and healthy control subjects: a 1-year prospective study in a Swedish clinic for infectious diseases. Clin Infect Dis. 2000;30(5):770–778. doi:10.1086/313770
21. Friesema IH, De Boer RF, Duizer E, et al. Aetiology of acute gastroenteritis in adults requiring hospitalization in The Netherlands. Epidemiol Infect. 2012;140(10):1780–1786. doi:10.1017/S0950268811002652
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.