")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 12
Estimating the effectiveness of pulmonary rehabilitation for COPD exacerbations: reduction of hospital inpatient days during the following year
Authors Katajisto M, Laitinen T
Received 22 June 2017
Accepted for publication 13 August 2017
Published 22 September 2017 Volume 2017:12 Pages 2763—2769
DOI https://doi.org/10.2147/COPD.S144571
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Milla Katajisto,1,2 Tarja Laitinen3
1Clinical Research Unit for Pulmonary Diseases, Division of Pulmonology, Helsinki University Hospital Heart and Lung Center, 2Helsinki University, Helsinki, 3Department of Pulmonary Diseases and Clinical Allergology, Turku University Hospital, University of Turku, Turku, Finland
Aims: To study the short- and long-term results of pulmonary rehabilitation (PR) given in the Helsinki University Heart and Lung Center and to understand the hospital resources used to treat severe COPD exacerbations in the city of Helsinki.
Materials and methods: Seventy-eight inactive patients with severe COPD were recruited for a PR course; three of them did not finish the course. The course took 6–8 weeks and included 11–16 supervised exercise sessions. Using electronic medical records, we studied all COPD patients with hospital admission in the city of Helsinki in 2014, including COPD diagnosis, criteria for exacerbation, and potential exclusion/inclusion criteria for PR.
Results: Seventy-five of the patients finished the PR course and 92% of those patients showed clinically significant improvement. Their hospital days were reduced by 54% when compared to the year before. At 1 year after the course, 53% of the patients reported that they have continued with regular exercise training. In the city of Helsinki, 437 COPD patients were treated in a hospital due to exacerbation during 2014. On the basis of their electronic medical records, 57% of them would be suitable for PR. According to a rough estimate, 10%–20% hospital days could be saved annually if PR was available to all, assuming that the PR results would be as good as those shown here.
Conclusions: The study showed that in a real-world setting, PR is efficient when measured by saved hospital days in severe COPD. Half of the patients could be motivated to continue exercising on their own.
Keywords: COPD, severe exacerbation, pulmonary rehabilitation, physical inactivity, COPD health care costs
Introduction
COPD is a major health problem, but goes often unrecognized until moderate to severe disease progression.1,2 The main symptom is dyspnea, which limits the patient’s physical activity.3–6 Another feature is exacerbations, the periods of worsening dyspnea which are often associated with increasing mucus production and respiratory infections.7,8 Exercise-based pulmonary rehabilitation (PR) in randomized controlled trials has proven to reduce exacerbations, subjective dyspnea, and the need for re-hospitalization.4,9 However, meta-analysis of 20 studies (1,477 participants) showed a great variation in PR programs, including patients’ self-management. Eight of the studies involving 810 participants indicated that PR reduced hospital readmissions (pooled odds ratio 0.44, 95% confidence interval 0.21 to 0.91), but results showed significant heterogeneity compared to each other.10 Presently, the essential components of PR needed to successfully induce long-term physical activity are poorly understood.
In Finland, public health care is of high quality and equally available for all citizens. Like in the other Nordic countries, the health benefits of exercising are well understood. There are more active trainers in Finland, for example, than in Southern Europe.11 Despite this fact and the recommendations of the international and national guidelines, exercise-based PR has not yet become well-recognized standard of care of COPD.12
Standardized group PR interventions as part of the usual care in severe COPD were started at the Helsinki University Hospital Heart and Lung Center in the year 2010. In this PR approach, we had two objectives: first, to improve the patients’ physical performance, and second, to encourage the patients to find new exercise activities and continue training after the course was completed. Retrospectively, we studied whether we succeeded in these goals and were able to observe a reduction in their hospital days during the following year. We also wanted to have a better understanding of the hospital resources used to treat COPD exacerbations in the city of Helsinki (having population of 620,000) and estimate what level of reduction could be achieved if PR was equally available to patients suffering from COPD exacerbations.
Materials and methods
Patients selected for PR
All the patients were recruited from the Helsinki University Hospital Heart and Lung Center, during the years 2010–2015. Exclusion criteria for PR were dementia, alcohol or drug abuse, multimorbidity, neurological or musculoskeletal disorder, psychiatric condition, active cancer, poor communication skills or adherence to care, and unstable cardiovascular or severe peripheral vascular disease. Patients were excluded based on these reasons, only if the exercise-prohibiting disease was severe or the lack of co-operation was obvious. Smokers were not excluded. All patients were enrolled to the PR group by one pulmonary consultant (MK).
Pulmonary rehabilitation course
The PR course was structured according to the international guidelines.13 The multidisciplinary team consisted of a physiotherapist, a pulmonary nurse, a pulmonary consultant, and a nutritional therapist. After the 6-week pilot with 5 patients, the course lasted 8 weeks, and the number of supervised exercise sessions varied from 11 to 16. The 1 h and 45 min exercise session was conducted twice a week and consisted of aerobic and muscle strength training for upper and lower extremities. The participants were also advised to exercise at least once a week on their own. PR was conducted at only one location, and every visit costs 8–9€ plus the costs of transportation. If the patient was not able to use his own car or the public transportation, the taxi was reimbursed, the patients’ share being 16€ one way. When patients’ performance was tested at the end of the course and compared to the results at the beginning of the course, the change was considered clinically meaningful (minimal clinical importance difference) when walking distance in the 6-minute walking test (6MWT) improved by 35 m, the chair sit-up test by 1.7 s, or the COPD assessment test (CAT) questionnaire symptom score decreased by 2 points.14–16 The PR course also included an educational lecture by a nutritional therapist and a motivational speech by a pulmonary consultant (MK). Help with smoking cessation was offered for smokers. The patients were interviewed by a physiotherapist on their individual testing visit before the start of the group training. They answered questions about their exercise habits and performance status. At the end of the course, all the participants prepared an individual exercise plan with the help of a physiotherapist. Independent training was encouraged by the COPD nurse and physiotherapists, and help was offered to find a place to exercise after the course. The information about their activity and exercise habits at 1 year were evaluated using the electronic medical records (eMR).
To understand the hospital resources needed to treat COPD exacerbations in the city of Helsinki, we evaluated all hospital admissions with COPD (ICD10 code J44) listed among the discharge diagnoses in 2014. A single consultant in pulmonary medicine (MK) evaluated the diagnostic criteria and all hospital treatment periods for the next 12 months or until death using eMR. The diagnosis of COPD was confirmed on the basis of clinical history of the disease, smoking history, and FEV1/FVC (forced expiratory volume in 1 s/forced vital capacity) ratio <0.7 in the latest spirometry. When spirometry results were lacking, the diagnosis was confirmed by the author by consistent clinical signs and symptoms, use of COPD medication, and smoking history. The criteria for COPD exacerbation was documented dyspnea or obstructive breathing, use of short/long-acting bronchodilators, oral or intravenous corticosteroids, and possibly antibiotics during the hospital stay.
Both of these registry-based study designs were approved by the Office of the Data Protection Ombudsman, Finland, and the data gathering and analysis were performed with the permission of the Helsinki City and the Helsinki University hospitals.
Statistics
Statistical analyses were performed using SPSS, and the statistical differences between the means were tested using one-way ANOVA.
Results
Pulmonary rehabilitation group
All patients (N=78) who were enrolled in PR had severe or very severe COPD (Table 1). All of them were physically inactive. The mean 6MWT result was 328 m (SD 128), the mean chair sit-up test result was 18.7 s (SD 9.4), and the mean CAT-score was 20 (SD 6). Despite optimized medication, they had unstable disease with the tendency of frequent exacerbations. Six of them were evaluated for organ transplant. One patient left the course due to lack of motivation, and two left due to severe exacerbation. The majority (N=45, 58%) of patients were recruited during or after hospital stay due to COPD exacerbation.
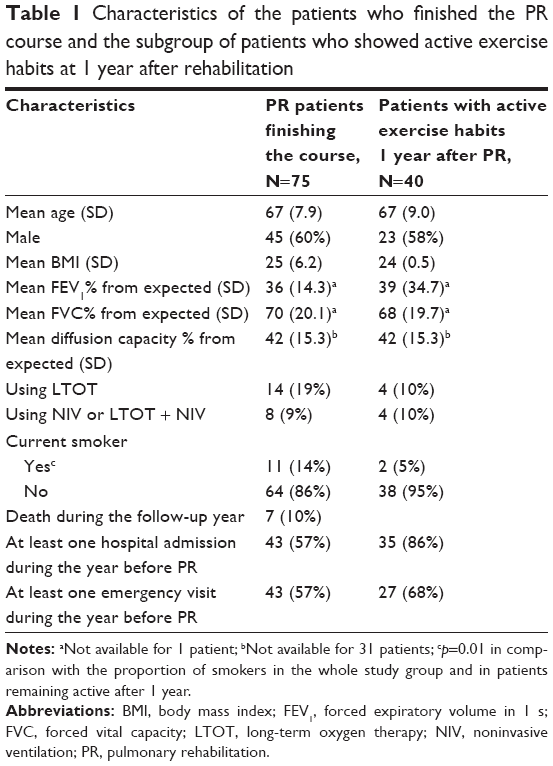 | Table 1 Characteristics of the patients who finished the PR course and the subgroup of patients who showed active exercise habits at 1 year after rehabilitation |
To study the efficacy of the PR course, we performed the 6MWT, the chair sit-up tests, and CAT-questionnaire and analyzed the symptom scores before and after the course. Sixty-nine patients (92%) were successful reaching MCID or higher in at least one measurement.
When patients were evaluated 1 year after PR, 40 (59%) of the living 68 patients reported that they had continued exercising. Of those six patients, who did not reach MCID by any of the measurements, four reported exercising regularly at 1 year. They had found new places to exercise, often senior gyms or group gymnastics. Active trainers did not differ by gender, age, body mass index (BMI), lung function, or by need of ventilation support from the patients who did not continue training. The only significant difference was the higher number of smokers among patients who did not keep their exercise habits when compared to active trainers (11/34 vs 2/40).
Hospital admissions and hospital days during the emergency visits were compared 1 year before and after the PR course, and the results showed significant reduction (Table 2). Seven patients died during the follow-up. If these patients were excluded from the analysis the result was almost the same as without their inclusion in the analysis; the trends between findings before and after remained similar and significant (8.4 hospital days before vs 3.3 days after, p=0.016). Data suggested that the best PR results were reached among women, patients under 70 years of age, and patients who remained active at 1 year, but the observed differences were not statistically significant (data not shown).
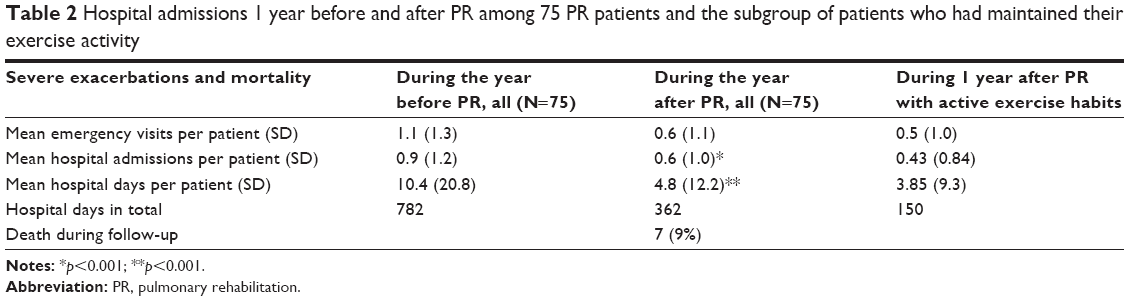 | Table 2 Hospital admissions 1 year before and after PR among 75 PR patients and the subgroup of patients who had maintained their exercise activity |
Severe COPD exacerbations in Helsinki
We identified a total of 935 patients who were discharged in the year 2014 with the diagnosis of ICD10: J44 (COPD). Of these 935 patients, we were not able to find any firm signs of COPD for 116 in their eMR. Further, 382 of them were COPD patients, but the hospitalization was due to causes other than COPD. The remaining 437 patients were verified as having COPD with acute exacerbation, and they were included in the analysis (Table 3). Starting from discharge, in total, these patients suffered 478 hospital-treated exacerbations (4,210 hospital days) during the follow-up year. Compared to the PR group, these patients were on average 7 years older. Their mean length of hospital stay was 14.0 days, the 90-day readmission rate was 27%, and the 90-day mortality rate was 12.9%. Patients in both cohorts suffered from severe airway obstruction, but death rate was significantly lower in the PR cohort (7/78=9.0% vs 157/437=36.0%, p=0.004) during the follow-up year (Table 4). Twenty-four (5%) patients died on the first admission, thus altogether 41% of the patients died during the 1-year period.
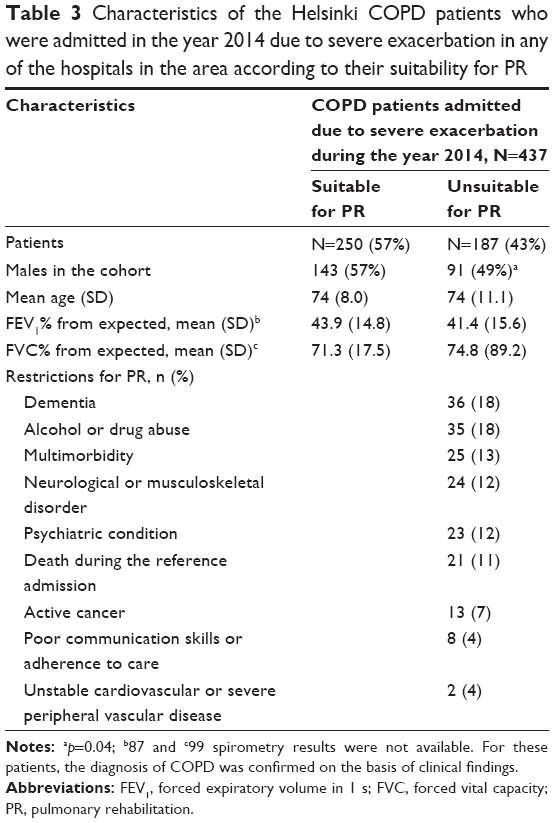 | Table 3 Characteristics of the Helsinki COPD patients who were admitted in the year 2014 due to severe exacerbation in any of the hospitals in the area according to their suitability for PR |
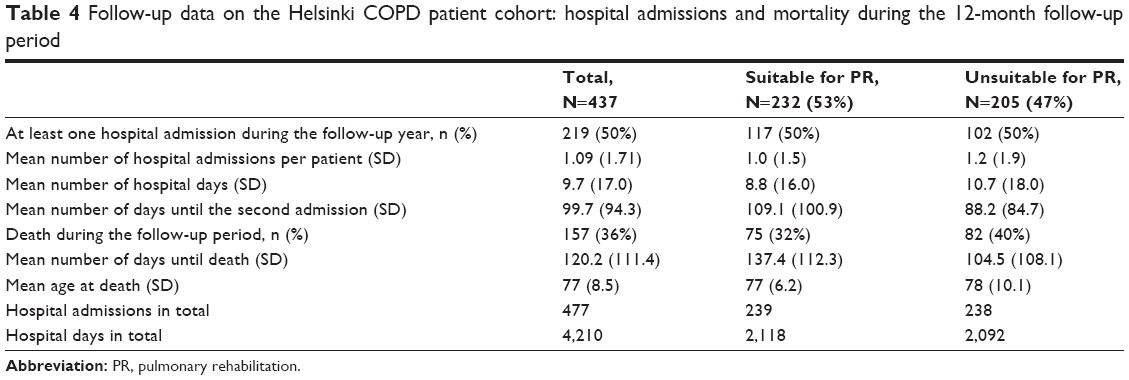 | Table 4 Follow-up data on the Helsinki COPD patient cohort: hospital admissions and mortality during the 12-month follow-up period |
We analyzed how many patients would be suitable for PR under the same criteria as used in the PR protocol. Based on the evaluation of their eMRs, 57% of the patients were shown be fit for PR (Table 3). With the exception of male gender, the suitable and unsuitable patients did not differ from each other. Table 4 shows the hospital admissions and prognosis of these patients.
In the PR group, we found a reduction of 54% in hospital days (420/782) during the year after PR compared to the year before. With similarly organized systematic PR for all COPD patients after hospital-treated exacerbation, we can roughly estimate the potential reduction of hospital days, assuming that the PR results are as good as in pulmonary clinic. Thus, patients who were not suitable for PR (47%) had 2,092 hospital days in total, and in that cohort no reduction would be achieved. Suitable patients (53%) had 2,118 hospital days. If we assume that half of the patients are adherent to PR, and the result of PR would be similar, we could achieve 10%–20% decline in hospital utilization due to severe exacerbations.
Discussion
The present study showed a significant reduction in hospital admissions among COPD patients with exacerbation, achieved with PR in a real-world setting. We showed clinically improved performance and/or reduced symptoms in 92% of patients after PR. We also showed a reduction of 54% in hospital days during the following year which was comparable to that reported before.17 Moreover, at 1 year, 59% of the patients surviving the follow-up year reported that they had continued regular training after the PR course. Their results in the reduction of severe exacerbations showed even better trends than among the rest of the patients, but the differences were not statistically significant.
To put the effectiveness of PR into context, we also analyzed the hospital resources used to treat COPD exacerbations in the city of Helsinki. Using eMRs, we carefully studied all hospital treatment periods for COPD exacerbations in 1 year and estimated the proportion of the patients suitable for PR and thus, the potential benefits of PR. Using the same inclusion and exclusion criteria as in the PR course of the Heart and Lung Center, more than half of the hospital-treated COPD patients were found suitable for PR. By using a very simplistic model, we estimated that 10%–20% of hospital days could be reduced by offering PR to all suitable patients. Severity of obstruction, age, and gender did not predict the suitability or success of continuation of training independently.
The estimate of saved hospital days should be interpreted with caution, and most probably, it might be too optimistic. In a review published in 2014, the finding was that the adherence to PR is about the same as to medication, that is, 50%.18 COPD patients’ socioeconomic status is often low, and the expenses of the pulmonary clinic’s PR course, including the rather high transportation costs (varying up to 440–640€ if taxi or invalid taxi was needed), might be a meaningful limitation for participation.19 To lower the expenses and assure the availability for everyone, the PR courses and the personalized training activities should be organized at several sites closer to the patients’ homes. The participants of the PR group of the Heart and Lung Center were obviously highly motivated to finish the course. They were also younger than patients treated for exacerbating COPD at large. However, in the PR group age, gender, or lung function did not predict the PR outcome. The high mortality among the hospital-treated COPD patients suggests that other causes such as comorbidities, poor social networks, and possibly cognitive skills most likely decrease the success rate of PR. COPD patients suffer from multimorbidity.20,21 It was not a surprise that almost half of the COPD patients’ hospital admissions were due to reasons other than exacerbations. Therefore, it is also possible that registry-based studies without access to eMRs may overestimate the burden of hospital-treated COPD exacerbations.
It has been estimated that 10,000 Finns have very severe COPD.22 Approximately 1,000 of them live in Helsinki. Our results show that almost half of them needed hospital care because of an exacerbation during 1 year. According to previous Finnish study, the average length of hospital stay decreased from 16.4 to 9.6 days during 1972–1992.23 Based on the present study, we did not find further positive development in the Helsinki area. The mortality rate of 41% in a year among the hospital-treated exacerbating COPD patients was high. The European COPD audit results from 422 hospitals in 13 countries showed that the median hospital stay was 8 vs 14 days in our study in Helsinki, the 90-day readmission rate was 35.1% vs 27.2%, and the 90-day mortality rate of 6.1% was lower than our rate of 12.9%. However, according to the European audit results, 80% of the exacerbating COPD patients were at least partly cared for by pulmonologists, compared to only 26% in Helsinki.24 The longer mean hospital stay is probably explained by the fact that, in Helsinki, patients who are unable to manage at home anymore, often have to wait in hospital wards for a place at a senior home or other assisted living accommodation.
Multiple PR studies have reported that the improvement in patients’ exercise capacity and physical activity decreased gradually during a year after PR.19,25,26 Therefore, from the first day, we concentrated on encouraging the patients to exercise independently and taught them during the supervised session that exercising is safe. We had previously learned that, due to cold winters, the patients also need an indoor exercising activity to be active year round.6 Together, the physiotherapist and participants developed a personalized training program. They also searched for suitable training facilities and, when possible, the PR participants were encouraged to continue training together. Using this approach, we could promote sustainable exercise habits to half of the patients, suggesting that this might aid in achieving better and longer lasting results. This finding was in line with a recent study in which 28 COPD patients were evaluated 1 year after 10 weeks of PR. These patients did not have any specific follow-up program, but they were given an exercise prescription to follow. Thirty-nine percent of the participants reported continuing self-directed exercising, and repeated measures confirmed not only improved functional capacity, but also improved cognitive performance and psychological well-being.27 When considering that COPD is a progressive disease, this result is even more convincing.
Conclusion
On the basis of the present results, almost 40% of the COPD patients died during the following year after severe, hospital-treated exacerbation. Therefore, a severe exacerbation should always be considered as a potentially life-threatening complication of COPD. In addition to optimizing medication, the patients should be offered help with smoking cessation, information about the benefits of exercising, and easy access to PR. From the beginning, the PR course should aim to support the development of long-lasting, personalized exercise habits for each patient. Our study also implied that offering PR after severe exacerbations may provide savings in health care expenses.
Acknowledgments
The authors would like to thank Professor Heikki Tikkanen and Dr Ari Lindqvist for their valuable advice and Chief Physician Laura Pikkarainen for her support in this study. Special thanks are given to physiotherapist Herkko Ryynänen for his excellent work with the patients and the physiotherapy unit for their cooperation. We also thank the Helsinki University Hospital Funds for financing the development of a novel treatment protocol, the Helsinki University Hospital, the Foundation of the Finnish Anti-Tuberculosis Association, the Nummela Sanatorium Foundation, and Association HES for financial support to this study.
Disclosure
The authors did not have a financial relationship with any commercial entity that has an interest in the subject of this manuscript. M Katajisto has received lecture fees from several pharmaceutical companies. Helsinki University Central Hospital has sent her to medical congresses abroad, sponsored by pharmaceutical companies. T Laitinen has been a member of the Boehringer-Ingelheim, Teva, Giesi, GlaxoSmithKline, and Astra-Zeneca Scientific Advisory Boards. She has received lecture fees, and Turku University Hospital has sent her to congresses abroad, sponsored by different pharmaceutical companies. The authors report no conflicts of interest in this work.
References
McCarthy B, Casey D, Devane D, Murphy K, Murphy E, Lacasse Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2015;(2):CD003793. | ||
Global Initiative for Chronic Obstructive Lung Disease (GOLD). Pocket guide to COPD diagnosis, management, and prevention; A Guide for Health Care Professionals; 2017 edition. Available from: http://goldcopd.org/wp-content/uploads/2016/12/wms-GOLD-2017-Pocket-Guide.pdf. Accessed February 2, 2017. | ||
Garcia-Aymerich J, Serra I, Gomez FP, et al; Phenotype and Course of COPD (PAC-COPD) Study Group. Physical activity and clinical and functional status in COPD. Chest. 2009;136(1):62–70. | ||
Garcia-Rio F, Lores V, Mediano O, et al. Daily physical activity in patients with chronic obstructive pulmonary disease is mainly associated with dynamic hyperinflation. Am J Respir Crit Care Med. 2009;180(6):506–512. | ||
Hartman JE, Boezen HM, de Greef MH, Ten Hacken NH. Physical and psychosocial factors associated with physical activity in patients with chronic obstructive pulmonary disease. Arch Phys Med Rehabil. 2013;94(12):2396–2402.e7. | ||
Katajisto M, Kupiainen H, Rantanen P, et al. Physical inactivity in COPD and increased patient perception of dyspnea. Int J Chron Obstruct Pulmon Dis. 2012;7:743–755. | ||
Schonmann M, Sievi NA, Clarenbach CF, et al. Physical activity and the frequency of acute exacerbations in patients with chronic obstructive pulmonary disease. Lung. 2015;193(1):63–70. | ||
Alahmari AD, Kowlessar BS, Patel AR, et al. Physical activity and exercise capacity in patients with moderate COPD exacerbations. Eur Respir J. 2016;48(2):340–349. | ||
Casaburi R, ZuWallack R. Pulmonary rehabilitation for management of chronic obstructive pulmonary disease. N Engl J Med. 2009;360(13):1329–1335. | ||
Puhan MA, Gimeno-Santos E, Cates CJ, Troosters T. Pulmonary rehabilitation following exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2016;12:CD005305. | ||
European Commission. Special Eurobarometer 412; Sport and physical activity [2014]. Available from: http://ec.europa.eu/health//sites/health/files/nutrition_physical_activity/docs/ebs_412_en.pdf . Accessed February 2, 2017. | ||
Kankaanranta H, Harju T, Kilpelainen M, et al. Diagnosis and pharmacotherapy of stable chronic obstructive pulmonary disease: the Finnish guidelines. Basic Clin Pharmacol Toxicol. 2015;116(4):291–307. | ||
Nici L, Donner C, Wouters E, et al. American Thoracic Society/European Respiratory Society statement on pulmonary rehabilitation. Am J Respir Crit Care Med. 2006;173(12):1390–1413. | ||
Holland AE, Nici L. The return of the minimum clinically important difference for 6-minute-walk distance in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2013;187(4):335–336. | ||
Jones SE, Kon SS, Canavan JL, et al. The five-repetition sit-to-stand test as a functional outcome measure in COPD. Thorax. 2013;68(11):1015–1020. | ||
Kon SS, Canavan JL, Jones SE, et al. Minimum clinically important difference for the COPD assessment test: a prospective analysis. Lancet Respir Med. 2014;2(3):195–203. | ||
Puhan M, Scharplatz M, Troosters T, Walters EH, Steurer J. Pulmonary rehabilitation following exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2009;(1):CD005305. | ||
Bender BG. Nonadherence in chronic obstructive pulmonary disease patients: what do we know and what should we do next? Curr Opin Pulm Med. 2014;20(2):132–137. | ||
Kanervisto M, Vasankari T, Laitinen T, Heliovaara M, Jousilahti P, Saarelainen S. Low socioeconomic status is associated with chronic obstructive airway diseases. Respir Med. 2011;105(8):1140–1146. | ||
Vilkman S, Keistinen T, Tuuponen T, Kivela SL. Survival and cause of death among elderly chronic obstructive pulmonary disease patients after first admission to hospital. Respiration. 1997;64(4):281–284. | ||
Deniz S, Sengul A, Aydemir Y, Celdir Emre J, Ozhan MH. Clinical factors and comorbidities affecting the cost of hospital-treated COPD. Int J Chron Obstruct Pulmon Dis. 2016;11:3023–3030. | ||
SOSIAALI-JA Terveysministeriön Julkaisuja. Valtakunnallinen ehkäisy-ja hoito-ohjelma 1998–2007 [National prevention and treatment program 1998–2007. Chronic bronchitis and COPD]. Finland: Publication of Social Affairs and Health; 1998; 4. Finnish. | ||
Keistinen T, Vilkman S, Tuuponen T, Kivela SL. Hospital admissions for chronic obstructive pulmonary disease in the population aged 55 years or over in Finland during 1972–1992. Public Health. 1996;110(4):257–259. | ||
Hartl S, Lopez-Campos JL, Pozo-Rodriguez F, et al. Risk of death and readmission of hospital-admitted COPD exacerbations: European COPD audit. Eur Respir J. 2016;47(1):113–121. | ||
Beauchamp MK, Evans R, Janaudis-Ferreira T, Goldstein RS, Brooks D. Systematic review of supervised exercise programs after pulmonary rehabilitation in individuals with COPD. Chest. 2013;144(4):1124–1133. | ||
Cindy Ng LW, Mackney J, Jenkins S, Hill K. Does exercise training change physical activity in people with COPD? A systematic review and meta-analysis. Chron Respir Dis. 2012;9(1):17–26. | ||
Emery CF, Shermer RL, Hauck ER, Hsiao ET, MacIntyre NR. Cognitive and psychological outcomes of exercise in a 1-year follow-up study of patients with chronic obstructive pulmonary disease. Health Psychol. 2003;22(6):598–604. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.