")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 13
Erosive Adenomatosis of the Nipple: A Clinical Diagnostic Challenge
Authors Ying S, Fang H, Qiao J
Received 29 April 2020
Accepted for publication 30 July 2020
Published 19 August 2020 Volume 2020:13 Pages 587—590
DOI https://doi.org/10.2147/CCID.S260534
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Shuni Ying, Hong Fang, Jianjun Qiao
Department of Dermatology, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Jianjun Qiao
Department of Dermatology, The First Affiliated Hospital, Zhejiang University School of Medicine, No. 79, Qingchun Road, Hangzhou 310003, Zhejiang Province, People’s Republic of China
Tel +86-571-87236340
Fax +86-571-87236628
Email [email protected]
Abstract: Erosive adenomatosis of the nipple (EAN) is a rare benign neoplasm of the nipple. The entity is generally characterized by erosion, serous discharge (serous and/or sanguineous), nodularity, swelling, itching and erythema of the nipple. It may be confused with mammary Paget’s disease of the nipple and obtain over-treatment. We reported a patient with typical clinical and histopathological features. Clinicians should consider EAN as one of the differential diagnosis in patients with erosions on the nipple.
Keywords: breast neoplasm, adenoma, erosive adenomatosis of the nipple, histopathology, surgical excision
Case Description
A 25-year-old woman presented with a 1-year history of erosion on the left nipple. The lesion was asymptomatic. One month ago, this erosion occurred with exudation and crust on the surface. Physical examination revealed that the left nipple skin was slightly raised, and a 0.5 cm × 0.5 cm nodule with infiltration. The surface of the lesion was rough and thickened with clear border, the texture was firm without tenderness (Figure 1). The patient denied family history of breast cancer or exposure towards oestrogen. On the physical examination, no palpable masses were detected in the breast. Lymphadenopathy was absent. In breast ultrasound imaging studies, the nodule presented with similar tissue density with normal breast tissue, and without sign of dilated duct.
 |
Figure 1 Photograph of the lesion on the left nipple. Erosion and crust on the left nipple. |
A biopsy obtained from the left nipple revealed papillomatous hyperplasia of the epidermis, and well-circumscribed glands in the dermis. The glands were composed of monolayer columnar epithelial cells with papillomatous hyperplasia in the lumina (Figure 2A and B). The luminal epithelia of the glands were positive for epithelial membrane antigen and cytokeratin five-sixths staining (Figure 2C), which confirmed the proliferation of usual ductal epithelium cells. Smooth muscle actin (Figure 2D) and p63 demonstrated that there were myoepithelial cells surrounding the luminal epithelial cells (Figure 2E). In the stroma, there were diffuse sparse infiltrates composed of lymphocytes and plasma cells. The patient underwent wedge resection of the nipple, no recurrence was found after 6 months of surgery.
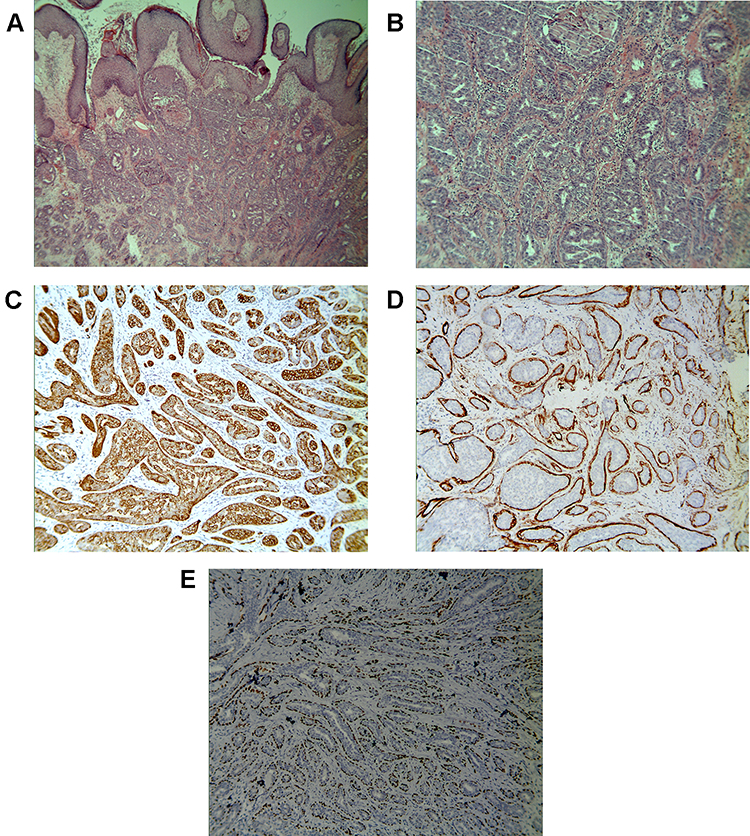 |
Figure 2 (A and B) Histopathology reveals ductal differentiation. (Hematoxylin-eosin stain, Original magnification×40 (A); Original magnification×200 (B)). The luminal epithelial cells were positive for (C) CK5/6 stain. (Immunohistochemistry, original magnification×100). The out-layer myoepithelial cells were positive for (D) SMA and (E) p63 stains. (Immunohistochemistry, original magnification×100). |
Discussion
Erosive adenomatosis of the nipple (EAN) is a rare benign neoplasm of the nipple first described by Jones in 1955.1–3 EAN occurs in middle-aged women, typically in fourth and fifth decades of life, and extremely less in men and children.1,4 The tumor is usually unilateral and asymptomatic, and the common clinical symptoms are erosion, serous discharge (serous and/or sanguineous), nodularity, swelling, itching and erythema of the nipple.1,2,4 Physical examination often reveals an irregular ulcer on the nipple without breast lump or lymphadenopathy.1,4
The major histopathology of EAN is characterized by a proliferation of lactiferous ducts, and gland-like structures in the stroma with clear border.1,4 In the ducts, two types of epithelial cells consisted by luminal epithelial and myoepithelial cells can be found,1,5 this is important to distinguish EAN from invasive breast carcinoma.6 Tumor may grow into the epidermis and replace squamous epithelium, or push the papillomatous lesion to the surface of the nipple, which make it look like an erosion or ulceration.1 Cytologic examinations including aspiration cytology, imprint cytology and brush cytology can help distinguish benign tumor and malignant tumor.1 On scrape smears, EAN is composed of regular epithelial cells, without necrosis and mitotic figures.1,5
Clinically, EAN should be differentiated with mammary Paget’s disease of the nipple, nipple eczema, chronic contact dermatitis, primary syphilis, lactiferous duct ectasia, herpes simplex virus infection, impetigo, and cutaneous malignant neoplasms.1,2,6
Mammary Paget’s disease is more prevalent in women after menopause, usually after the sixth decade of life.7,8 It often presents as a unilateral lesion with eczematoid erythematous plaques, ulceration, and destruction involving nipple and areola.2,3,7 Paget’s disease can be analyzed with scrape smears, cutaneous fine needle aspiration biopsy, and incisional biopsy.8 Epidermal with Paget’s cells, which have clear and abundant cytoplasm and stained by anti-c-erbB-2 antibody, can be found.3 Nipple eczema presents as itching erythematous scaly papules or plaques with indefinite edge affecting bilateral nipples2,5 with an intermittent history.2 Skin biopsy is characterized by spongiotic dermatitis with lymphocytic infiltration in the superficial dermis.9 Primary syphilis is a main cause of genital ulcer disease caused by treponema pallidum, which can penetrate epidermis or mucosal epithelium through tiny wounds after sexual exposure.2,9 Primary syphilis may present in extragenital regions including the lips, oral mucosa, tongue, conjunctiva,10 chin, neck, anus, arms, abdomen, and nipple–areola.11 The chancres are painless ulcerations in the nipple-areola region10 and associate with regional lymphadenopathy.2 Serological tests can differentiate it from EAN.
A simple complete excision of tumor can get excellent prognosis.1,12 Some limited forms of complete surgical excision can be considered when EAN remains in the nipple stroma, including wedge resection technique, Mohs micrographic surgery and nipple splitting enucleation technique, which can remove the tumor completely and preserve this important area both cosmetically and psychologically.1,5,12 Cryotherapy may be chosen to preserve as much intact nipple tissue as possible for women of childbearing age who need to breastfeed.13 And it is necessary for patients to have regular breast follow-up with annual breast physical examination and mammography to prevent the local recurrence and development of breast cancer.1
EAN is a rare benign neoplasm of the nipple caused by adenomatous proliferation of lactiferous ducts. EAN is easily misdiagnosed as nipple erosion, especially Paget’s disease of the breast, which is difficult to diagnose on mammography, ultrasound, or MRI. Histology is the gold standard of diagnosis. Compared with the normal mammary tissue, EAN presents with benign hyperplasia of lactiferous ducts and the disorganized growth of two types of epithelial cells. The main treatment method is surgical resection, patients can obtain a good prognosis after a simple complete excision of the lesion. For women of childbearing age who need to retain intact nipples, a tissue sparing surgical technique like Mohs surgery or cryotherapy can be considered if the tumor does not invade the dermal papilla and epidermal layer. However, regardless of the treatments, regular follow-up is recommended as the entity has a risk of developing into a malignancy.
Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. Institutional approval is not required for this case study.
Acknowledgments
We thank the patient’s permission to publish this information. This work was supported by the Zhejiang Medical and Health Science and Technology Project (2020KY558, to JQ).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Spohn GP, Trotter SC, Tozbikian G, Povoski SP. Nipple adenoma in a female patient presenting with persistent erythema of the right nipple skin: case report, review of the literature, clinical implications, and relevancy to health care providers who evaluate and treat patients with dermatologic conditions of the breast skin. BMC Dermatol. 2016;16(1):4. doi:10.1186/s12895-016-0041-6
2. Qiao J, Zhou S, Fang H. An ulcer on the nipple. BMJ. 2018;360:j5850. doi:10.1136/bmj.j5850
3. Ooi PS, Draman N, Yusoff SSM, Zain WZW, Ganasagaran D, Chua HH. Mammary Paget’s disease of the nipple: relatively common but still unknown to many. Korean J Fam Med. 2019;40(4):269–272. doi:10.4082/kjfm.17.0143
4. Gu X, Wang G, Wu R, Jia H. Erosive adenomatosis of the nipple in a man. Indian J Dermatol Venereol Leprol. 2015;81(1):68–70. doi:10.4103/0378-6323.148581
5. Lee HJ, Chung KY. Erosive adenomatosis of the nipple: conservation of nipple by Mohs micrographic surgery. J Am Acad Dermatol. 2002;47(4):578–580. doi:10.1067/mjd.2002.122752
6. Alhayo ST, Edirimanne S. Clinically challenging case of nipple adenoma. Breast J. 2018;24(6):1084–1085. doi:10.1111/tbj.13089
7. Lopes Filho LL, Lopes IMRS, Lopes LRS, Enokihara MMSS, Michalany AO, Matsunaga N. Mammary and extramammary Paget’s disease. An Bras Dermatol. 2015;90(2):225–231. doi:10.1590/abd1806-4841.20153189
8. Raivoherivony ZI, Feron J, Klijanienko J. The utility of nipple scraping in the diagnosis of Paget disease of the breast. Diagn Cytopathol. 2019;47(3):249–250. doi:10.1002/dc.24033
9. Liu X-K, Li J. Erosive patches on bilateral nipples. JAMA Dermatol. 2018;154(6):719–720. doi:10.1001/jamadermatol.2017.5640
10. Fukuda H, Takahashi M, Kato K, Oharaseki T, Mukai H. Multiple primary syphilis on the lip, nipple-areola and penis: an immunohistochemical examination of Treponema pallidum localization using an anti-T. pallidum antibody. J Dermatol. 2015;42(5):515–517. doi:10.1111/1346-8138.12818
11. Menet E, Vabres P, Brecheteau P, et al. Pigmented Paget’s disease of the male nipple. Ann Dermatol Venereol. 2001;128(5):649–652.
12. Brankov N, Nino T, Hsiang D, Zeineh L. Utilizing Mohs surgery for tissue preservation in erosive adenomatosis of the nipple. Dermatol Surg. 2016;42(5):684–686. doi:10.1097/DSS.0000000000000677
13. Pasquali P, Freites-Martinez A, Fortuño A. Nipple adenoma: new images and cryosurgery treatment. Breast J. 2016;22(5):584–585. doi:10.1111/tbj.12636
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.