")
Back to Journals » Clinical Epidemiology » Volume 12
Epidemiology of Venous Thromboembolism After Second Cancer
Authors Gade IL , Severinsen MT , Kragholm KH , Kristensen SR, Torp-Pedersen C , Riddersholm SJ
Received 31 January 2020
Accepted for publication 14 March 2020
Published 8 April 2020 Volume 2020:12 Pages 377—386
DOI https://doi.org/10.2147/CLEP.S247823
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Henrik Sørensen
Inger Lise Gade,1,2 Marianne Tang Severinsen,2,3 Kristian Hay Kragholm,4,5 Søren Risom Kristensen,1,3 Christian Torp-Pedersen,3,5,6 Signe Juul Riddersholm7
1Department of Clinical Biochemistry, Aalborg University Hospital, Aalborg, Denmark; 2Department of Hematology and Clinical Cancer Research Center, Aalborg University Hospital, Aalborg, Denmark; 3Department of Clinical Medicine, Aalborg University, Aalborg, Denmark; 4Department of Cardiology, North Denmark Regional Hospital, Hjørring, Denmark; 5Unit of Clinical Biostatistics, Aalborg University Hospital, Aalborg, Denmark; 6Department of Cardiology and Clinical Investigation, North Zealand Hospital, Hillerød, Denmark; 7Department of Medicine, Randers Regional Hospital, Randers, Denmark
Correspondence: Inger Lise Gade
Department of Hematology, Aalborg University Hospital, Mølleparkvej 4, Aalborg 9000, Denmark
Tel +45 61656584
Email [email protected]
Background: Venous thromboembolism (VTE) is a serious, yet preventable, complication in cancer. Some patients are diagnosed with a second cancer; however, little is known about the epidemiology of VTE in this population.
Methods: From Danish national healthcare registries, we studied all patients diagnosed with a first breast, prostate, lung, or colorectal cancer from 1995 to 2015. We estimated incidence rates (IRs) of VTE according to the timing of the diagnosis of a second cancer. We controlled for confounder variables in Poisson regression models.
Results: In total, 309,077 patients with a first breast, prostate, lung, or colorectal cancer were included in the study. A second cancer was diagnosed in 20,090 (6.5%) of these patients. In total, 11,908 VTEs were observed in the study period, 786 of these occurred after a diagnosis of second cancer. Second cancer types such as pancreas and stomach cancer were associated with fivefold higher IRs of VTE compared with second cancer types such as breast and prostate cancer. The IR of VTE was highest within the first 6 months after the second cancer was diagnosed (IR 40.5 per 1000 person-years, 95% CI 36.3– 42.2) with no differences based on how long since the first cancer it was diagnosed.
Conclusion: The epidemiology of VTE after a second cancer is similar to the epidemiology of VTE after a first cancer with higher rates within the first months after aggressive second cancer types.
Keywords: venous thromboembolism, second cancer, epidemiology, incidence, cancer
Introduction
Venous thromboembolism (VTE) is a frequent complication of cancer that leads to mental and physical morbidity and results in high mortality rates.1–5 Cancer survival rates have continuously increased due to accelerated diagnostic work-up and successively refined cancer treatments.6,7 Despite these improvements for cancer patients, little is known about their long-term risk of VTE. This growing group of patients, however, represents a considerable proportion patients with VTE, and some of these patients develop a second cancer.8–12 The epidemiology of VTE in cancer patients who develop a second cancer has not been previously described.
The aim of this study was to investigate the epidemiology of VTE among patients diagnosed with a second cancer. We used data from Danish nationwide healthcare registers where diagnoses, procedures, and information about reimbursed medicine are prospectively registered at an individual level. This provides unique opportunities for epidemiological research.13–15
Our hypothesis was that cancer patients who develop a second cancer had a higher risk of VTE than patients with only one cancer. We investigated the risk of VTE based on the timing of the second cancer diagnosis in the subset of the general population diagnosed with a first breast, prostate, lung, or colorectal cancer between 1995 and 2015 from the Danish National Cancer Registry, the Danish National Patient Registry (DNPR), and the Danish National Prescription Registry. Estimates of VTE risk were calculated separately for the following periods after the first and second cancer diagnosis: 0–6 months, 6–12 months, 1–2 years and >2 years.
Methods
Setting
There are approximately 5.5 million people in the Danish population. The Danish Civil Registration system keeps track of the Danish residents’ vital status and movement within the Danish border and abroad. This is possible by assigning a unique civil personal registration (CPR) number to all Danish residents at birth or at the time of immigration. The unique CPR number enables linking of information from all Danish registries and cradle-to-grave follow-up at an individual level.14
Danish residents have income-independent access to universal healthcare. The Danish healthcare system is tax-funded based on individual contacts registered with the CPR number. Hospital admissions, diagnoses, surgeries, and therapies for each contact have been recorded in the DNPR since 1977. Until 1994, the International Classification of Diseases codes—8th edition (ICD-8 codes)—were used for classification of the diagnoses. From 1994 onwards, the ICD-10 classification has been used in the DNPR. Surgeries are registered in the DNPR by the Nordic Medico Statistical Committee (NOMESCO)16 classification. Since 1995, contacts to outpatient clinics and emergency departments have also been prospectively registered in the DNPR. More than 99% of all contacts to the Danish healthcare system are captured in the DNPR.13,17
Study Population
We included all Danish residents diagnosed with a first primary breast, prostate, lung, or colorectal cancer between 1995 and 2015. Since 1987, the registration of new cancer cases plus certain tumor-like and benign lesions in the Danish National Cancer Registry has been mandatory by law and linked to the DNPR. The Danish National Cancer Registry captures more than 95% of all new cancer cases, and 93% of the diagnoses are verified by microscopy.15,18 Study patients were identified in the Danish National Cancer Registry by the ICD-10 codes C34.0–34.9 for lung cancer, C61.0–61.9 for prostate cancer, C50.0–50.9 for breast cancer, and C18.0–21.9 for colorectal cancer. The last available date of cancer registration was December 31, 2015.
Exposure
Second cancer was identified by the combination of the procedure code AZCA1 in the DNPR, which is used for new malignant diseases not fully registered previously in the Danish National Cancer Registry, and an ICD-10 code within the C00-97 group in the Danish National Cancer Registry. If the second registration was within the same ICD-10 group as the first cancer, we considered the patient as having progression/relapse of the first cancer and did not classify patients as having developed a second cancer. Carcinoma in situ, non-melanoma skin cancer, and benign tumors were excluded. Second cancers were classified as either very high VTE-risk, high VTE-risk, or intermediate/low VTE-risk based on published risk assessment models for prediction of VTE in cancer patients (Supplementary Table 1).19,20
Outcome and Confounders
Outcome was VTE after a first diagnosis of breast, prostate, lung or colorectal cancer. The VTEs were identified by linkage to the DNPR (ICD-10 I26, I80.0-I80.9). Last date for follow-up of VTE was December 31, 2017. Due to the low positive predictive value of VTE diagnosis codes from emergency departments,21 we excluded events that were not subsequently coded in a ward or an outpatient clinic.
VTEs preceding the first cancer diagnosis were identified by the ICD-8 codes 450 and 451 in addition to the aforementioned ICD-10 codes for VTE in the DNPR. Information about anticoagulation medication was retrieved from the Danish National Prescription Registry, in which the type of medicine is registered with the World Health Organization’s Anatomical Therapeutic Chemical codes along with dose, pack size and date of reimbursement.22 We used the Anatomical Therapeutic Chemical codes B01AA03, B01AE07, B01AF02, B01AF01, B01AB10, B01AB04, and B01AB05 to identify anticoagulation treatment. If patients were hospitalized and had a period of anticoagulation treatment, they were considered “anticoagulated” during the hospitalization. Information about hospitalization admission and discharge dates was retrieved from the DNPR.
Lower extremity fractures (ICD-10 codes T02, S72, S82, S92) and arthroplasties including surgical revisions (NOMESCO codes NFB, NFC, NGB and NGC) after the first cancer diagnosis were identified in the DNPR.
Study Design and Statistics
Study entry was the date of diagnosis of one of the studied first cancer types, patients were followed until whichever of the following came first: death, VTE, emigration, or administrative censoring (ie, last follow-up for cancer was December 31, 2015). The patients who were diagnosed with a second cancer during follow-up shifted to contribute with person-time at risk of VTE in the group with a second cancer from the date of the second cancer diagnosis onwards. One day of observation time was given in cases where cancer and VTE were diagnosed on the same date.
Estimates of absolute risk of VTE were measured using incidence rates (IRs) of VTE expressed as events per 1000 person-years (p-y) and associated 95% confidence intervals (CIs). We calculated IRs of VTE in patients with only one cancer and in patients diagnosed with a second cancer. We calculated IRs of VTE for second cancers diagnosed within the following four periods: 0–6 months, 6–12 months, 1–2 years and >2 years after the first cancer. We calculated IR’s of VTE by increasing time since diagnosis of first and second cancer, respectively. Additionally, we calculated IRs of VTE according to the second cancers’ VTE risk category.
Incidence rate ratios (IRRs) of VTE were estimated using Poisson regression models, including pre-determined time-dependent covariates. Covariates included the second cancer VTE risk group, time since first cancer diagnosis, calendar period, and time since second cancer diagnosis. We defined the following risk periods after the first and possibly second cancer diagnosis: 0–6 months, 6–12 months, 1–2 years and >2 years. Patients who received anticoagulant medication in the study period changed from “not on anticoagulation medication” to “on anticoagulation medication” on the date of first reimbursed prescription, and changed back to “not on anticoagulation medication” status on the date of calculated last anticoagulation medicine dose. Regarding the covariates fractures and arthroplasties, we defined the 90 days following the diagnosis/operation day as the exposed time in accordance with the definition of transient risk factors by the International Society of Thrombosis and Haemostasis.23 Age was included as a categorical time-dependent variable, and sex and a history of VTE before study entry were included as dichotomous variables.
In a sensitivity analysis, we excluded patients with a history of VTE before study entry.
Ethics
Neither ethical approval nor informed consent is not required for studies based on Danish register data if conducted for the sole purpose of statistics and scientific research. The study was approved by the data responsible institute (Region Hovedstaden – Approval number P-2019-348) in accordance with the General Data Protection Regulation.
Results
Patient Characteristics
A total of 309,077 patients were diagnosed with either a first breast (n = 86,632), prostate (n = 64,381), lung (n = 77,791), or colorectal cancer (n = 80,275) from 1995 to 2015 (Supplementary Figure 1). The median age at study entry was 70.0 years (25th–75th percentile, 60.2–76.9) and 52% were women (Table 1). In 10,689 of the study patients, a VTE was registered before the first cancer diagnosis; however, 988 of these VTEs were solely coded in an emergency department. Thus, in total, 9701 study patients were diagnosed with a VTE prior to the first cancer diagnosis (519 concurrent pulmonary embolism and deep vein thrombosis, 2559 pulmonary embolisms and 6623 deep vein thromboses). Median time from the previous VTE to first cancer diagnosis was 6.7 years (25th–75th percentile 2.0–14.3 years). The median follow-up time was 2.4 years (25th–75th percentile, 0.6–6.5 years).
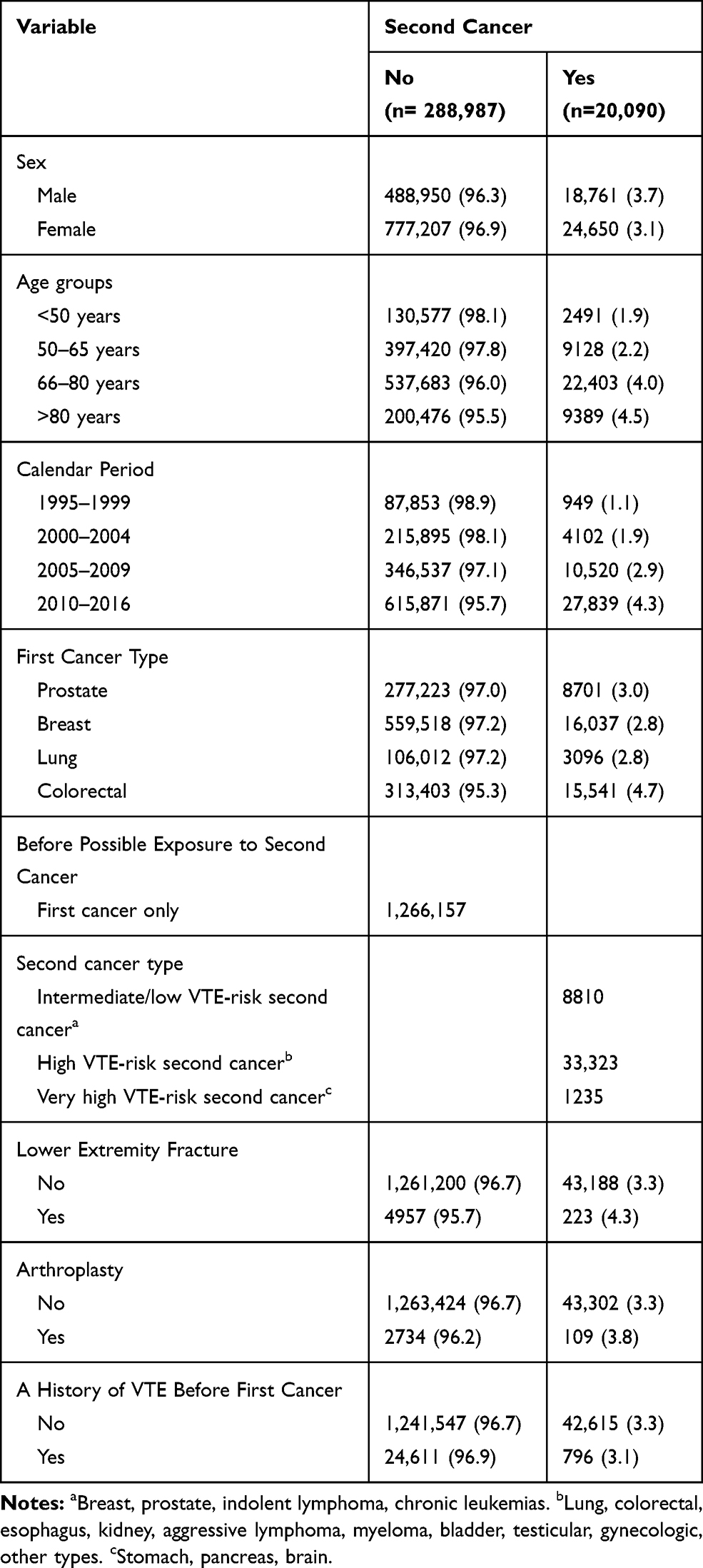 |
Table 1 Patient Characteristics According Exposure to Second Cancer in the Study Period, Person-Years (%) |
Exposure
A second cancer was diagnosed in 6.5% (20,090) of the study patients, most frequently after a first colorectal or prostate cancer (Table 2). Seven percent (1431) of the second cancers were classified as very high VTE-risk cancer types, 77.6% (15,592) as high VTE-risk second cancers, and 15.3% (3067) as intermediate/low VTE-risk cancers. The proportion of intermediate/low VTE-risk second cancers was lower in patients with a first prostate and breast cancer than in patients with a first lung or colorectal cancer because the vast majority of intermediate/low VTE-risk second cancers were either prostate or breast cancer.
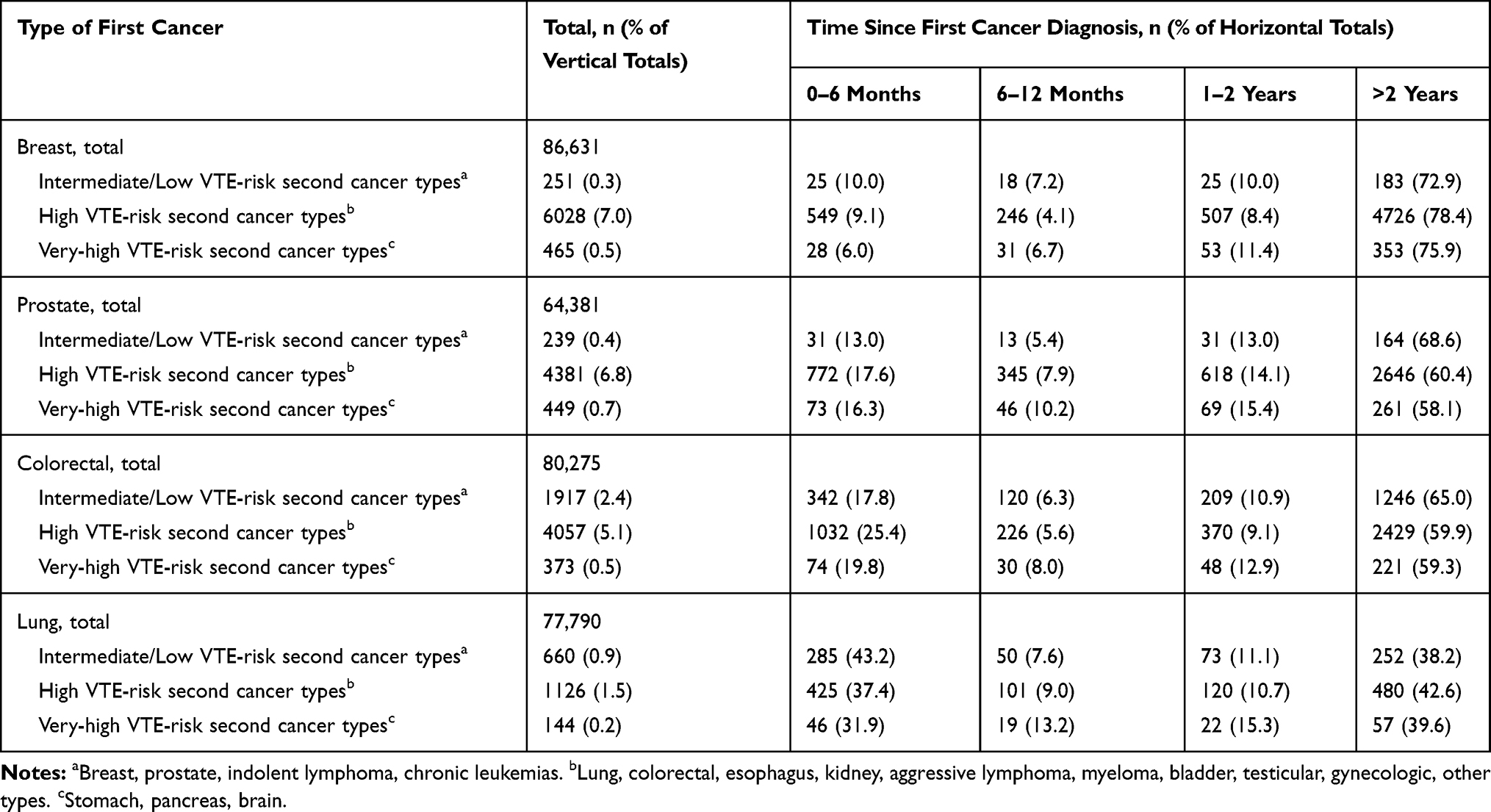 |
Table 2 Distribution of Very-High VTE Risk, High VTE Risk and Intermediate/Low VTE Risk Second Cancers by Type of First Cancer and Time Since Diagnosis Hereof, n (% of Total) |
Outcome
A total of 11,918 VTEs were observed after study entry following exclusion of 1152 VTEs that were coded solely in an emergency department. Ten patients emigrated after a first cancer diagnosis and were years later diagnosed with a VTE after returning to Denmark. These 10 events were not included in the analysis because we did not have data concerning possible second cancer development during their emigration period. Thus, 11,908 VTEs remained in our study (393 concurrent pulmonary embolism and deep vein thrombosis, 5526 pulmonary embolisms and 5989 deep vein thromboses) (Supplementary Figure 1). Twelve percent (1400) of the VTEs occurred in patients with a history of VTE before study entry. For further details, see supplemental results. The overall IR of VTE in the study was 9.1 per 1000 p-y (95% CI, 8.9–9.3).
First Cancer and VTE in Unexposed Patients
The overall IR of VTE among patients without a second cancer was 8.9 per 1000 p-y (95% CI, 8.8–9.1); however, there were large variations based on the type of first cancer and time since it was diagnosed. Please see supplemental results for detailed description (Table 3, Figure 1).
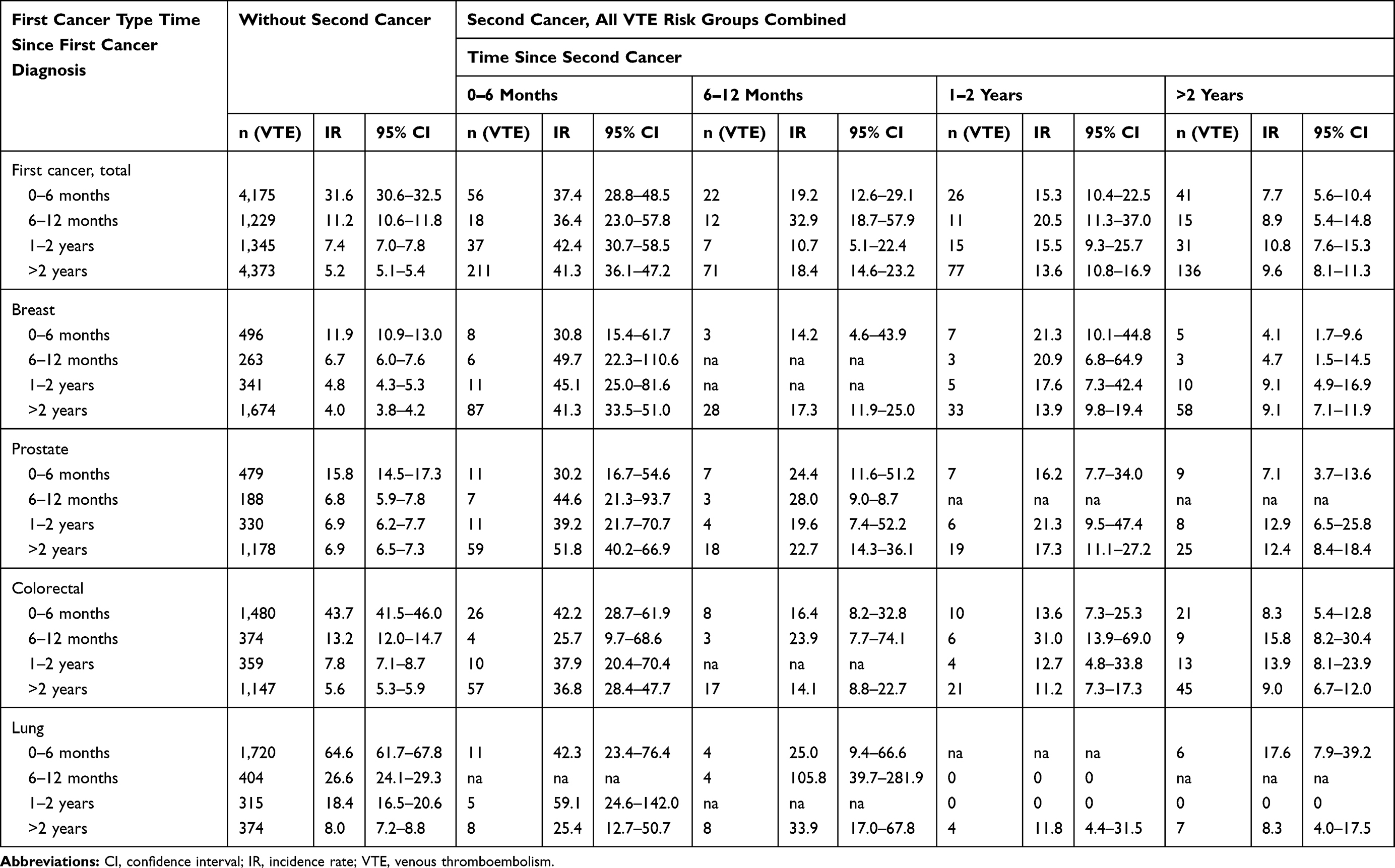 |
Table 3 Incidence Rates (per 1000 p-y) of VTE by Increasing Time Since First/Second Cancer Diagnosis According to When Patients Were Diagnosed with the Second Cancer |
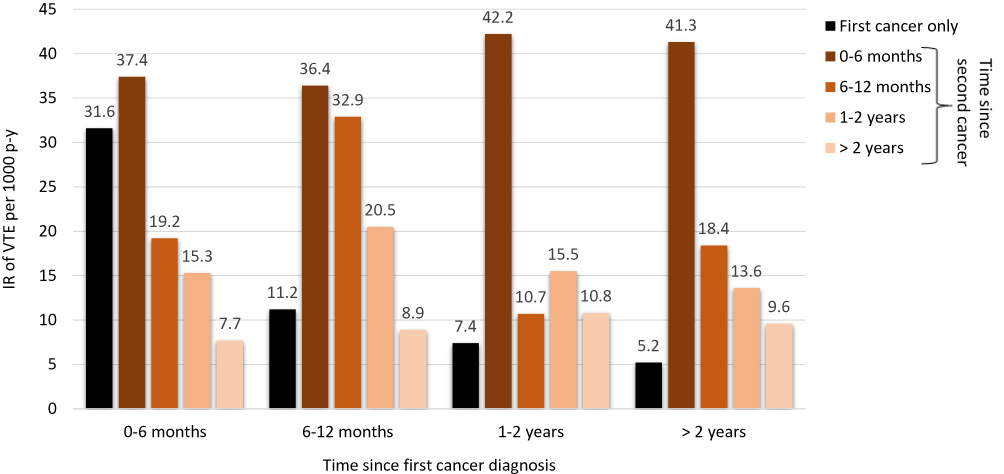 |
Figure 1 Incidence rates of VTE by time since first cancer according to time since second cancer, if exposed in the period. |
Second Cancer and VTE
The overall IR of VTE in patients after diagnosis of a second cancer was 20.9 per 1000 p-y (95% CI, 19.4–22.3); however, there was considerable variation based on time since diagnosis and the type of the second cancer.
The IRs of VTE were markedly higher for very high VTE-risk second cancer types than high - and intermediate/low VTE-risk second cancers (Figure 2, Supplementary Table 2). Very high VTE-risk second cancer was associated with a 5-fold higher risk of VTE than an intermediate/low VTE-risk second cancer in multivariate analysis accounting for: type of and time since first cancer diagnosis; time since second cancer diagnosis; and patient-related factors such as age, sex, anticoagulation treatment, previous VTE, arthroplasties and fractures (Figure 3).
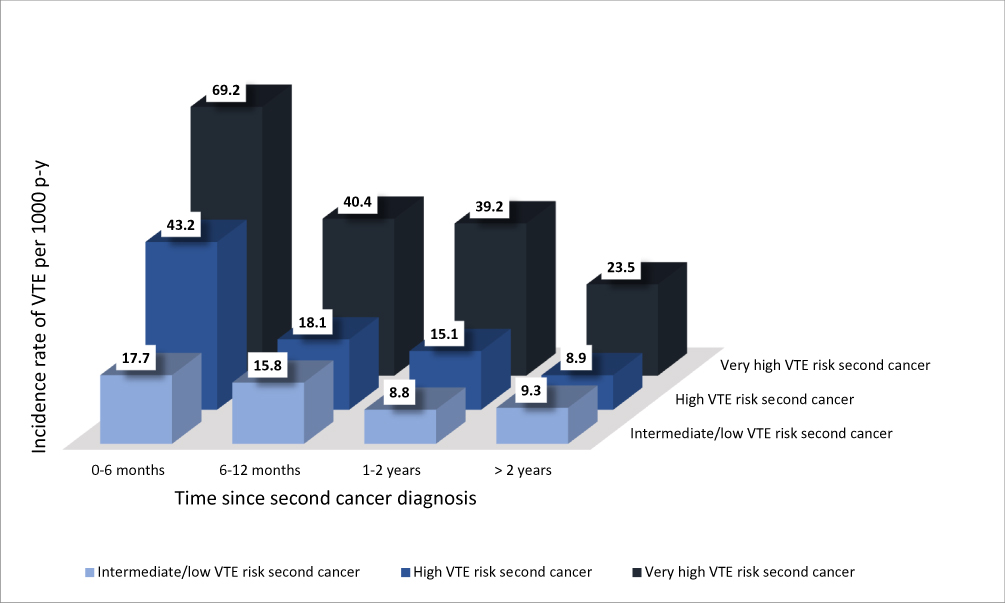 |
Figure 2 Incidence rates of VTE by time since second cancer diagnosis for each of the three second cancer VTE-risk groups. |
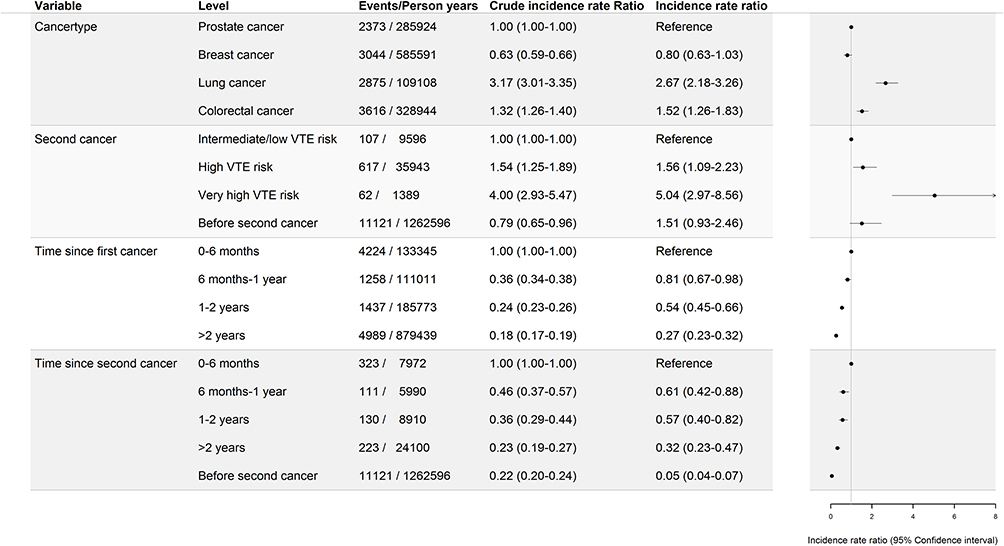 |
Figure 3 Crude and adjusted incidence rate ratios (IRR) of VTE, adjusted estimates are depicted in the forest plot. |
The IR of VTE was highest within the first 6 months after a second cancer diagnosis. We observed similar 0–6 month IR’s for second cancers diagnosed within the first six months after the first cancer diagnosis and second cancers diagnosed later after the first cancer (Figure 1, Table 3). The impact of a second cancer on the risk of VTE declined with time since the second cancer diagnosis. This association was confirmed by the multivariate analysis where the IRR of VTE more than two years after the second cancer diagnosis was 0.32 (95% CI, 0.23–0.47) compared with the first 0–6 months after the second cancer diagnosis (Figure 3). Please see supplemental results for further description.
The impact of a second cancer on the IR of VTE was more pronounced in patients with a first intermediate/low VTE-risk cancer type (ie a first prostate or breast cancer) than in patients with a first high VTE-risk cancer type (ie a first lung and colorectal cancer). In patients with a first prostate or breast cancer, second cancer lead to markedly higher IRs of VTE than in patients with only prostate or breast cancer regardless of the timing of diagnosis of the second cancer (Table 3). Contrarily, similar 0–6 month IRs of VTE was observed for patients with only lung or colorectal cancer and those who were diagnosed with a second cancer within the first six months after the lung cancer diagnosis. For those with a first lung cancer even if diagnosed with high/very high VTE-risk second cancer types (0–6 month IR of VTE: 55.0, 95% CI, 27.5–110.0). If a second cancer was diagnosed more than one year after a first lung or colorectal cancer diagnosis; however, the IR was higher than in patients free of second cancer (Table 3).
The impact of a second cancer on the risk of VTE in cancer patients was surpassed by exposure to lower extremity fractures (IRR of VTE in exposed period compared with unexposed 12.3, 95% CI, 9.7–15.6), arthroplasties (IRR of VTE in exposed period compared with unexposed 13.8, 95% CI, 10.2–18.5), and a history of VTE (IRR of VTE in patients with a history of VTE compared with no VTE before first cancer 10.8, 95% CI 9.4–12.5) in the multivariate analysis (Supplementary Figure 2).
Exclusion of patients with a history of VTE did not alter the observed associations. The IRs of VTE were generally marginally lower in the sensitivity analysis than in the primary analysis. Largest difference was seen in the IR of VTE within 0–6 months after a first lung cancer diagnosis (primary analysis: IR in unexposed patients 65.6, 95% CI, 61.7–67.8; sensitivity analysis: IR in unexposed patients 54.3, 95% CI, 52.5–57.2) (Table 3 and Supplementary Table 3). Similarly, the association with second cancer remained in the sensitivity analysis after adjustment for confounder variables; IRR of VTE in very high VTE-risk second cancer compared with unexposed patients was 4.66 (95% CI, 2.71–8.04) (Supplementary Figure 3).
Discussion
This nationwide study on VTE among 309,077 patients diagnosed with a first breast, prostate, lung, or colorectal cancer in the period between 1995 and 2015 had two key findings. First, the impact of a second cancer on the IR of VTE was dependent on the type of second cancer and the time since second cancer diagnosis. The association was strongest for very high VTE-risk second cancer types such as pancreatic and stomach cancers within the first months after the second cancer diagnosis. Second, the impact of a second cancer on the IR of VTE was dependent on the type of patient’s first cancer and timing of the second cancers diagnosis. A second cancer did not markedly alter the risk of VTE for patients with a newly diagnosed high VTE-risk first cancer type, while second cancers diagnosed later or in patients with even newly diagnosed low VTE-risk first cancers was associated with markedly higher IRs of VTE.
Our observations concerning second cancer and cancer associated VTE are first in class. The associations with type and time since second cancer diagnosis and risk of VTE observed in this study are, however, a spitting image of well-known effects of type of and time since first cancer and VTE.24–30 Development of second cancer is associated with increased risk of VTE recurrence.31,32 We found that exposure to a second cancer also increases the risk of a first incident VTE in cancer patients, which is new and important information for both clinicians and researchers within the field of cancer associated thrombosis, obvious as it might seem. Our paper for the first time confirms what is possibly already presumed as common sense or biological plausible based on knowledge of the pathophysiology of cancer-associated VTE.
Based on our observations in this study, we propose that clinicians should consider thromboprophylaxis for patients who are diagnosed with a second cancer in the same way that thromboprophylaxis is considered for first cancer cases. In addition, we suggest that cancer patients who undergo arthroplasty, get a lower extremity fracture and those with a history of VTE before the cancer diagnosis undergo careful evaluation of the benefit of prophylactic anticoagulant treatment, as they are at a particularly higher risk of VTE than cancer patients without these risk factors. Cancer is generally considered a high-risk factor in guidelines for the prophylaxis of surgical thrombosis.33,34
We found a markedly higher risk of VTE as long as 6 months after both first and second cancer diagnoses in a multivariate analysis. Is has been estimated that 70% of all VTEs are hospital acquired.35 In a recent Australian study, Stubbs et al found that the risk of hospital-acquired VTE was markedly higher for cancer patients than cancer-free patients.36 Four weeks of postoperative thromboprophylaxis is currently recommended for both open - and laparoscopic cancer surgery in the Danish guidelines, that are based on international guidelines.37–39 The Australian data showed that the risk of hospital acquired VTE while still hospitalized was indeed higher for surgical patients than for medical patients. Interestingly, the risk of VTE was markedly higher for at least 90 days after hospital discharge for medical patients compared with surgical patients.36 Current Danish guidelines suggest in-hospital thromboprophylaxis for immobilized, hospitalized medically ill cancer patients. Future research should aim at identifying subgroups of medically ill, hospitalized cancer patients who might benefit from thromboprophylaxis after discharge.
In our study design, we took advantage of the opportunities provided by high-quality person-time data from the Danish national healthcare registries, including all follow-up data. Invalid VTE diagnoses were excluded before data analysis, exposures, and relevant confounder variables were allowed to vary over time. Despite these advantages, our study has important limitations to bear in mind. First, we did not include information about chemotherapy, as this information is not validated for all cancer types. In a previous study concerning VTE in chronic lymphocytic leukemia patients, we observed an apparent under-reporting of traditional chemotherapy and antibody-based regimens for this patient group.40
Some of the very-high VTE-risk second cancers were diagnosed in close timely relation to the first cancer and, in some of these cases, a VTE may have been registered before the second cancer was diagnosed. This would draw our observations towards the null-hypothesis of no differences in VTE occurrence in patients who develop a second cancer and those who do not and, hence, underestimate the impact of a second cancer on the risk of VTE. The reported increased IRs of VTE in patients diagnosed with a second cancer in our study are thus conservative estimates of the impact of development of a second cancer on the risk of VTE.
Future studies on cancer-associated VTE, both short- and long-term, should address possible second cancers, as they are frequent after some cancer types and can have a significant effect on the risk of VTE. The impact of a second cancer on the risk of cancer-associated VTE needs investigation, as prevention strategies could be appropriate for certain groups. The results from this study, however, need confirmation in other cohorts including other types of first cancers.
In conclusion, we examined the epidemiology of cancer-associated VTE with regards to diagnoses of a second cancer. Patients diagnosed with a second cancer had higher IRs of VTE in general. The IR of VTE was highest in very high/high VTE-risk second cancer types within the first six months after the second cancer diagnosis.
Author Contributions
I. L. Gade conceived the idea of the study. I. L. Gade and S. J. Riddersholm are responsible for the study design, data managing and analysis, interpretation of the results and they wrote the first draft and revised it. M. T. Severinsen, K. H. Kragholm, and S. R. Kristensen contributed to the study design, interpretation of results, reviewed and commented on the manuscript. S. R. Kristensen contributed to the study design, interpretation of results and reviewed and commented the manuscript. C. Torp-Pedersen provided access to the study data, contributed to the study design, interpretation of results and reviewed and commented on the manuscript. All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
Christian Torp-Pedersen reports grants from Bayer and Novo Nordisk outside the submitted work. The authors received no funding for the study and have no other disclosures to report.
References
1. Timp JF, Braekkan SK, Versteeg HH, Cannegieter SC. Epidemiology of cancer-associated venous thrombosis. Blood. 2013;122(10):1712–1723. doi:10.1182/blood-2013-04-460121
2. Parpia S, Julian JA, Thabane L, Lee AY, Rickles FR, Levine MN. Competing events in patients with malignant disease who are at risk for recurrent venous thromboembolism. Contemp Clin Trials. 2011;32(6):829–833. doi:10.1016/j.cct.2011.07.005
3. Sørensen HT, Mellemkjær L, Olsen J, Baron JA. Prognosis of cancers associated with venous thromboembolism. N Engl J Med. 2000;343(25):1846–1850. doi:10.1056/NEJM200012213432504
4. Noble S, Prout H, Nelson A. Patients’ Experiences of LIving with CANcer-associated thrombosis: the PELICAN study. Patient Prefer Adherence. 2015;9:337–345. doi:10.2147/PPA.S79373
5. Farge D, Cajfinger F, Falvo N, et al. Quality of life in cancer patients undergoing anticoagulant treatment with LMWH for venous thromboembolism: the QUAVITEC study on behalf of the Groupe Francophone Thrombose et Cancer (GFTC). Oncotarget. 2018;9(43):26990–26999. doi:10.18632/oncotarget.25454
6. De AR, Sant M, Coleman MP, et al. Cancer survival in Europe 1999–2007 by country and age: results of EUROCARE–5-a population-based study. Lancet Oncol. 2014;15(1):23–34.
7. Allemani C, Matsuda T, Di Carlo V, et al. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet (London, England). 2018;391(10125):1023–1075. doi:10.1016/S0140-6736(17)33326-3
8. Van HM, Adolfsson J, Garmo H, et al. Risk of thromboembolic diseases in men with prostate cancer: results from the population-based PCBaSe Sweden. Lancet Oncol. 2010;11(5):450–458.
9. Brand JS, Hedayati E, Bhoo-Pathy N, et al. Time-dependent risk and predictors of venous thromboembolism in breast cancer patients: a population-based cohort study. Cancer. 2017;123:468–475
10. Walker AJ, West J, Card TR, Crooks C, Kirwan CC, Grainge MJ. When are breast cancer patients at highest risk of venous thromboembolism: a cohort study using English healthcare data. Blood. 2015.
11. Walker AJ, West J, Card TR, Humes DJ, Grainge MJ. Variation in the risk of venous thromboembolism in people with colorectal cancer: a population-based cohort study from England. J Thromb Haemost. 2014;12(5):641–649. doi:10.1111/jth.12533
12. Gade IL, Brækkan SK, Næss IA, et al. Long-term incidence of venous thromboembolism in cancer: the Scandinavian thrombosis and cancer cohort. Th Open. 2018;02(02):e131–e138. doi:10.1055/s-0038-1641678
13. Schmidt M, Schmidt SA, Sandegaard JL, Ehrenstein V, Pedersen L, Sorensen HT. The Danish National Patient Registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449–490. doi:10.2147/CLEP.S91125
14. Pedersen CB. The Danish Civil Registration System. Scand J Public Health. 2011;39(7_suppl):22–25. doi:10.1177/1403494810387965
15. Storm HH, Michelsen EV, Clemmensen IH, Pihl J. The Danish Cancer Registry–history, content, quality and use. Dan Med Bull. 1997;44(5):535–539.
16. Nordic Centre for Classifications in Health Care. NOMESCO Classification of Surgical Procedures. Oslo; 2010. Available from: https://norden.diva-portal.org/smash/get/diva2:970547/FULLTEXT01.pdf. Accessed March 30, 2019.
17. Andersen TF, Madsen M, Jørgensen J, Mellemkjoer L, Olsen JH. The Danish National Hospital Register. A valuable source of data for modern health sciences. Dan Med Bull. 1999;46(3):263–268.
18. The Danish National Heatlh Authority (Sundhedsstyrrelsen). Det Moderne Cancerregister - Metode Og Kvalitet [The modern cancer register - methods and quality]. Copenhagen; 2009. Available from: https://sundhedsdatastyrelsen.dk/da/registre-og-services/om-de-nationale-sundhedsregistre/sygedomme-laegemidler-og-behandlinger/cancerregisteret. Accessed March 30, 2019 Danish.
19. Khorana AA, Kuderer NM, Culakova E, Lyman GH, Francis CW. Development and validation of a predictive model for chemotherapy-associated thrombosis. Blood. 2008;111(10):4902–4907. doi:10.1182/blood-2007-10-116327
20. Pabinger I, van Es N, Heinze G, et al. A clinical prediction model for cancer-associated venous thromboembolism: a development and validation study in two independent prospective cohorts. Lancet Haematol. 2018;5(7):e289. doi:10.1016/S2352-3026(18)30063-2
21. Severinsen MT, Kristensen SR, Overvad K, Dethlefsen C, Tjonneland A, Johnsen SP. Venous thromboembolism discharge diagnoses in the Danish National Patient Registry should be used with caution. J Clin Epidemiol. 2010;63(2):223–228. doi:10.1016/j.jclinepi.2009.03.018
22. Kildemoes HW, Sørensen HT, Hallas J. The Danish National Prescription Registry. Scand J Public Health. 2011;39(7):38–41. doi:10.1177/1403494810394717
23. Kearon C, Ageno W, Cannegieter SC, et al. Categorization of patients as having provoked or unprovoked venous thromboembolism: guidance from the SSC of ISTH. J Thromb Haemost. 2016;14(7):1480–1483. doi:10.1111/jth.13336
24. Cohen A, Katholing A, Rietbrock S, Bamber L, Martinez C. Epidemiology of first and recurrent venous thromboembolism in patients with active cancer. A population-based cohort study. Thromb Haemost. 2017;117(1):57–65. doi:10.1160/TH15-08-0686
25. Walker AJ, Card TR, West J, Crooks C, Grainge MJ. Incidence of venous thromboembolism in patients with cancer - a cohort study using linked United Kingdom databases. Eur J Cancer. 2013;49(6):1404–1413. doi:10.1016/j.ejca.2012.10.021
26. Horsted F, West J, Grainge MJ. Risk of venous thromboembolism in patients with cancer: a systematic review and meta-analysis. PLoS Med. 2012;9(7):e1001275. doi:10.1371/journal.pmed.1001275
27. Cronin-Fenton D, Sondergaard F, Pedersen LA, et al. Hospitalisation for venous thromboembolism in cancer patients and the general population: a population-based cohort study in Denmark, 1997–2006. Br J Cancer. 2010;103(7):947–953. doi:10.1038/sj.bjc.6605883
28. Chew HK, Wun T, Harvey D, Zhou H, White RH. Incidence of venous thromboembolism and its effect on survival among patients with common cancers. Arch Intern Med. 2006;166(4):458–464. doi:10.1001/archinte.166.4.458
29. Martinez C, Cohen AT, Bamber L, Rietbrock S. Epidemiology of first and recurrent venous thromboembolism: a population-based cohort study in patients without active cancer. Thromb Haemost. 2014;112(2):255–263. doi:10.1160/TH13-09-0793
30. Blix K, Gran OV, Severinsen MT, et al. Impact of time since diagnosis and mortality rate on cancer‐associated venous thromboembolism: the Scandinavian Thrombosis and Cancer (STAC) cohort. J Thromb Haemost. 2018;16(7):1327–1355. doi:10.1111/jth.14130
31. Heit JA, Lahr BD, Ashrani AA, Petterson TM, Bailey KR. Predictors of venous thromboembolism recurrence, adjusted for treatments and interim exposures: a population-based case-cohort study. Thromb Res. 2015;136(2):298–307. doi:10.1016/j.thromres.2015.06.030
32. Chee CE, Ashrani AA, Marks RS, et al. Predictors of venous thromboembolism recurrence and bleeding among active cancer patients: a population-based cohort study. Blood. 2014;123(25):3972–3978. doi:10.1182/blood-2014-01-549733
33. Samama CM, Afshari A, Force EVGT. European guidelines on perioperative venous thromboembolism prophylaxis. Eur J Anaesthesiol. 2017;35(2):1.
34. Gould M, Garcia D, Wren S, et al. Prevention of VTE in nonorthopedic surgical patients: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e227S–e277S. doi:10.1378/chest.11-2297
35. Cohen AT, Agnelli G, Anderson FA, et al. Venous thromboembolism (VTE) in Europe. The number of VTE events and associated morbidity and mortality. Thromb Haemost. 2007;98(4):756–764. doi:10.1160/TH07-03-0212
36. Stubbs JM, Assareh H, Curnow J, Hitos K, Achat HM. Incidence of in-hospital and post-discharge diagnosed hospital-associated venous thromboembolism using linked administrative data. Intern Med J. 2018;48:157–165.
37. Lyman GH, Bohlke K, Khorana AA, et al. Venous thromboembolism prophylaxis and treatment in patients with cancer: American Society of Clinical Oncology Clinical Practice Guideline Update 2014. J Clin Oncol. 2015;33(6):654–656. doi:10.1200/JCO.2014.59.7351
38. Mandala M, Falanga A, Roila F, Group EGW. Management of venous thromboembolism (VTE) in cancer patients: ESMO Clinical Practice Guidelines. Ann Oncol. 2011;22(Suppl 6):vi85–vi92. doi:10.1093/annonc/mdr392
39. Watson HG, Keeling DM, Laffan M, Tait RC, Makris M; for Standards in Haematology BC. Guideline on aspects of cancer-related venous thrombosis. Br J Haematol. 2015;170(5):640–648. doi:10.1111/bjh.13556
40. Gade IL, Riddersholm SJ, Christiansen I, et al. Venous thromboembolism in chronic lymphocytic leukemia: a Danish nationwide cohort study. Blood Adv. 2018;2(21):3025–3034. doi:10.1182/bloodadvances.2018023895
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.