")
Back to Journals » Infection and Drug Resistance » Volume 12
Epidemiology and molecular characterization of mcr-1 in Escherichia coli recovered from patients with bloodstream infections in Changsha, central China
Authors Zhong YM, Liu WE, Zheng ZF
Received 24 March 2019
Accepted for publication 27 June 2019
Published 12 July 2019 Volume 2019:12 Pages 2069—2076
DOI https://doi.org/10.2147/IDR.S209877
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sahil Khanna
Yi-Ming Zhong,1 Wen-En Liu,1 Zhao-Feng Zheng2
1Department of Clinical Laboratory, Xiangya Hospital, Central South University, Changsha, People’s Republic of China; 2Faculty of Laboratory Medicine, Xiangya School of Medicine, Central South University, Changsha, People’s Republic of China
Objectives: The main aim of this study was to investigate the prevalence and molecular characteristics of the mcr-1 gene in Escherichia coli isolates obtained from all patients with bloodstream infections over a year in a Chinese teaching hospital. We also assessed the susceptibility profiles of the mcr-1-positive strains and prognostic impact of this gene on the patients.
Methods: A total of 144 consecutive, non-repetitive E. coli isolates causing bloodstream infections were collected at a teaching hospital in Changsha, China from January to December 2016. The presence of the mcr-1 gene was assessed by PCR. All mcr-1-positive E coli isolates were characterized by antimicrobial susceptibility testing, multilocus sequence typing (MLST), a conjugation experiment, and plasmid replicon typing. Clinical data were obtained from medical records.
Results: The mcr-1 gene was detected in three (2.1%) of the 144 E. coli isolates. The three mcr-1-positive E. coli isolates were resistant to colistin. All three isolates showed a lower resistance to other classes of antibacterials, with all three being susceptible to carbapenems. The MLST results indicated that the three E. coli isolates were assigned to three different sequence types: ST457, ST101, and ST1413, respectively. The conjugation experiment showed that the mcr-1 gene was successfully transferred to the recipient (E. coli EC600) from two isolates, one of which possessed IncI1 replicons and the other of which carried IncHI2 and IncN replicons. The patients with bloodstream infections caused by mcr-1-positive isolates had severe underlying diseases and were cured after antibacterial treatment.
Conclusion: The prevalence of the mcr-1 gene in patients with E. coli bloodstream infection was 2.1% in Changsha, China. The mcr-1-positive E. coli isolates had varied susceptibility profiles, although all three were susceptible to carbapenems. This therapeutic window is crucial given the risk of rapid deterioration in high-incidence areas worldwide.
Keywords: E. coli, mcr-1, colistin resistance, bloodstream infection, clinical characteristics
Introduction
Multidrug-resistant Gram-negative bacteria such as carbapenem-resistant Enterobacteriaceae have led to the resurgent use of polymyxins (including polymyxin B and colistin) as “last-line” treatment options.1–3 However, the increased use of polymyxin antibacterials has been accompanied by more frequent reports of emerging polymyxin-resistant isolates around the world.1,3,4 The mechanisms of polymyxin resistance have been found to involve alterations in the PmrAB or PhoPQ two-component regulatory systems caused by chromosome-mediated mutations.1,4 Although the earliest reports of the emerging plasmid-mediated colistin resistance gene mcr-1 originated from China, subsequent studies from other countries reported similar results.1,5–7 In China, the prevalence rate of the mcr-1 gene in Enterobacteriaceae in samples from humans ranged from 0.6% among consecutive clinical infection isolates in central China to 6.2% among fecal samples of patients in southern China.8,9 Several studies have focused on clinical Escherichia coli isolates carrying the mcr-1 gene from patients with bloodstream infection.7,10,11 In a recent Chinese study, Quan et al showed that 1% of E. coli isolates causing bloodstream infections carried mcr-1.1 More worryingly, the co-presence of the mcr-1 gene with carbapenem and extended-spectrum beta-lactamase (ESBL) resistance genes has been reported in several studies,1,5,11 indicating the possibility of pan-drug resistance strains. Many plasmids, such as IncHI2 and IncI2, have been involved in the spread of mcr-1. China’s high population density makes the country vulnerable to uncontrolled spread of mcr-1-positive E. coli unless vigorous surveillance measures are implemented immediately.
The aims of this study were to investigate the prevalence and molecular characteristics of the mcr-1 gene in E. coli isolates obtained from all patients with bloodstream infection over a year in a Chinese teaching hospital. The susceptibility profiles of the mcr-1-positive strains and the prognostic impact of this gene were also assessed.
Materials and methods
Bacterial isolates
From January to December 2016, 144 consecutive, non-repetitive E. coli isolates causing bloodstream infections, one from each patient, were collected at Xiangya Hospital, a general teaching hospital affiliated with Central South University (Changsha, Hunan Province, China) that has 3500 beds and 7500–10,000 patient visits every day. Isolates were identified using the Vitek 2-system (bioMérieux, Marcy-l’Étoile, France). The mcr-1-positive control strain was provided by Prof. Jianzhong Shen, who was the first to report the mcr-1 gene. E. coli ATCC 25922 was used as a negative quality control strain.
Screening for the mcr-1 gene in clinical strains
Screening for the mcr-1 gene was performed as previously described.5 The PCR products were bidirectionally sequenced. Sequence type (ST) determination was performed according to the E. coli multilocus sequence typing (MLST) database.1 The primers used for all PCR reactions are listed in Table S1.
Clinical data collection
For the cases of bloodstream infection caused by mcr-1-positive E. coli, we reviewed the medical records and collected patient data, including data on demographic characteristics, underlying disease, clinical manifestations, treatments, and clinical outcomes. The study was approved by the Ethical Committee of Xiangya Hospital of Central South University.
Antimicrobial susceptibility testing
The minimum inhibitory concentration (MIC) of colistin for the mcr-1-positive isolates was determined using the broth microdilution method.12 The antimicrobial susceptibility of other antibacterials, including ampicillin, ceftazidime, cefepime, aztreonam, piperacillin–tazobactam, imipenem, ertapenem, gentamicin, amikacin, ciprofloxacin, and trimethoprim/sulfamethoxazole, was determined using the Vitek 2 system (bioMérieux). The results were interpreted according to the European Committee on Antimicrobial Susceptibility Testing (EUCAST) breakpoint recommendations.13
Conjugation experiment
The conjugation experiment was carried out in mixed broth cultures with rifampin-resistant E. coli EC600 as the recipient strain. Briefly, purified donor strains (mcr-1-positive strains) and recipient strains (E. coli EC600) were separately inoculated in Luria–Bertani (LB) broth at 37 °C for 4 h. A 20 µl aliquot of mixture containing 100 µl of each of the above cultures was then added onto a microporous membrane that was pre-placed on Mueller–Hinton agar. After overnight culture at 37 °C, all strains were collected and the E. coli transconjugants were then selected on the basis of growth on Mueller–Hinton agar containing colistin (2 mg/L) and rifampicin (600 mg/L).1 Transfer frequencies were calculated as the number of transconjugants obtained per recipient. The presence of mcr-1 was confirmed by PCR. The transconjugants’ colistin MIC values were also determined.
Plasmid replicon typing
Plasmid replicons were determined using the PCR-based replicon typing scheme.14
Results
Screening for the mcr-1 gene
Among the 144 E. coli strains recovered from patients with bloodstream infection, three (2.1%) were positive for the mcr-1 gene.
Antimicrobial susceptibility and molecular characteristics of mcr-1 genes
As indicated in Table 1, the mcr-1-positive E. coli strains in this study, herein designated #1, #2, and #3, all exhibited an unfavorable antimicrobial susceptibility profile in addition to exhibiting colistin resistance conferred by the mcr-1 gene. The MLST results indicated that the three isolates were assigned to three different STs: ST457, ST101, and ST1413, respectively.
 |
Table 1 Antibiotic susceptibility, ST and replicon type of the three mcr-1-positive isolates |
Strain #1 carried IncI1 replicons. Strain #2 carried IncHI2 and IncN replicons. Strain #3 was not typed (Table 1). In the conjugation experiment, the mcr-1 gene was successfully transferred to the E. coli EC600 standard recipient from strains #1 and #2, but not from strain #3. The transfer frequency of the mcr-1 gene for strains #1 and #2 was 6.4×10−6 and 2.2×10−6, respectively. The two resulting transconjugants both exhibited elevated colistin MIC values.
Clinical information on the three patients infected with mcr-1-positive isolates
The demographic and clinical characteristics of the three patients are summarized in Table 2. All three patients infected with mcr-1-positive E. coli had severe underlying diseases. Two patients were hospitalized within 3 months prior to the onset of bloodstream infection. Patient #1 was a 72-year-old woman with a history of right hemicolectomy because of colon cancer. She did not follow clinical recommendations regarding receiving postoperative chemotherapy and she was later diagnosed with colon cancer recurrence and metastasis. Patient #2 was a 10-year-old male child. He was diagnosed with acute leukemia and had undergone chemotherapy on three occasions. He was admitted to the Emergency Department due to septic shock. Patient #3 was a 47-year-old man with several underlying diseases, including coronary heart disease, type 2 diabetes mellitus, diabetic nephropathy, and stage 5 chronic kidney disease. After hemodialysis, he was admitted to hospital after developing signs of septic shock. All three patients with bloodstream infection were cured after treatment with antibacterials that they had been found to be susceptible to.
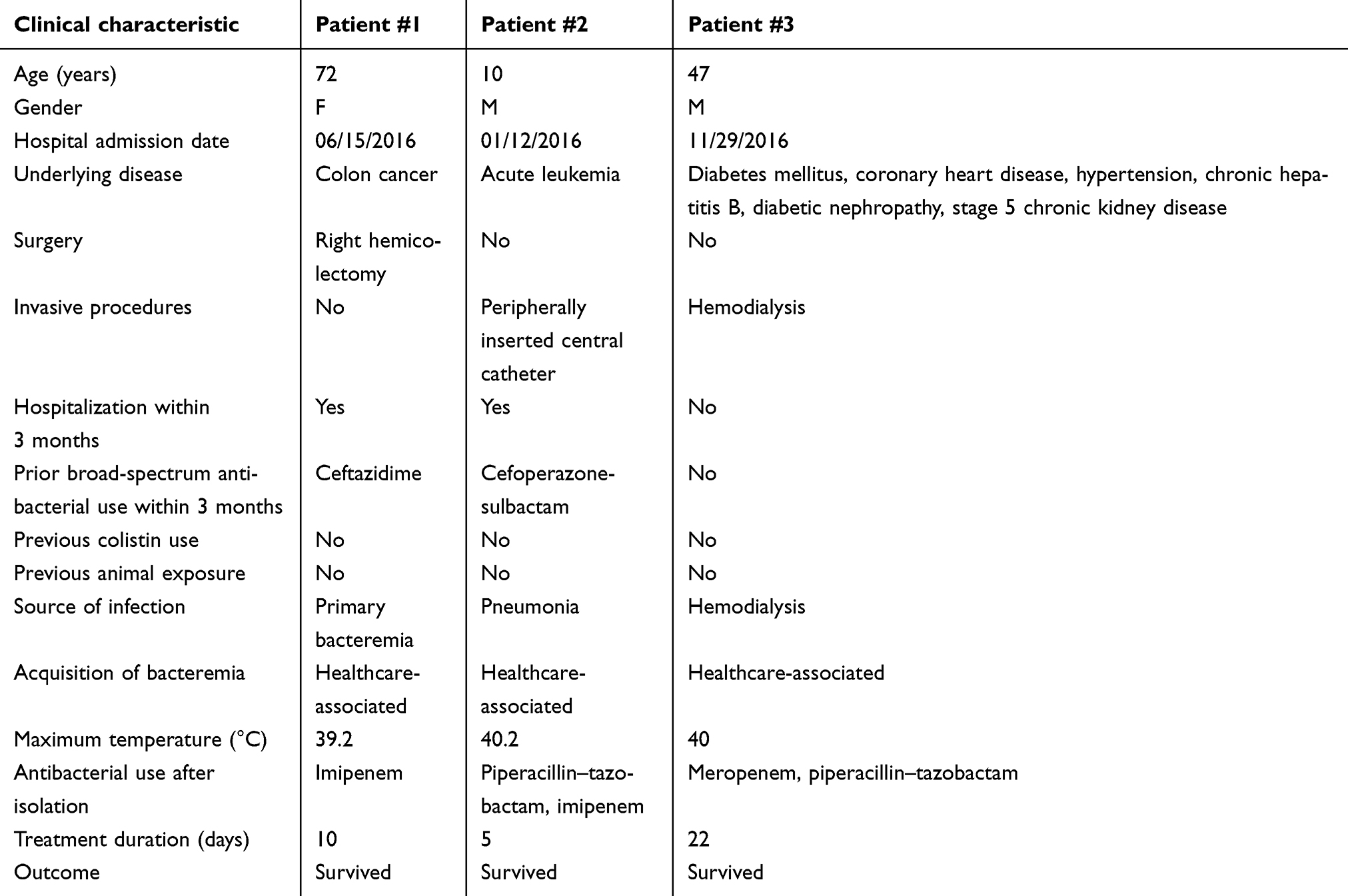 |
Table 2 Clinical characteristics of the three patients infected with mcr-1-positive isolates |
Discussion
In our study, 144 clinical E. coli isolates were collected from patients treated for bloodstream infection in a teaching hospital in China. Of these isolates, three (2.1%) carried mcr-1 genes. Our data showed that the low prevalence of the mcr-1 gene among E. coli isolates from human bloodstream infections was slightly higher than that observed (0–1%) from patients in other countries and regions,1,11,15,16 whereas Lai et al detected mcr-1 carriage in 75% of E. coli strains from pigs.11 Hence, the reservoir for mcr-1-positive E. coli seems to be larger among animals than among humans. Some studies have reported that mcr-1-positive E. coli might have a susceptibility profile that is generally favorable for antibacterials other than colistin.17,18 On the other hand, Lai et al have shown that mcr-1-positive E. coli can be highly resistant, thus suggesting that the potential for mcr-1 gene dissemination is not limited to community strains with a low baseline level of antimicrobial resistance.11 In this study, the mcr-1-positive E. coli strains #1 and #2 were resistant to cephalosporins, while all three strains were susceptible to carbapenems. This highlights the risk that the mcr-1 gene might spread even in carbapenem-susceptible E. coli isolates. This may be due to the fact that not all plasmids with the mcr-1 gene carry other genes conferring resistance to clinically relevant antibacterials such as carbapenemase.17,19 Therefore, it seems imperative that testing for colistin susceptibility should be part of the clinical routine in all microbiological laboratories in China.
A recent study involving an MLST analysis reported the extreme divergence of E coli strains carrying mcr-1 in different provinces and even in different hospitals in China.20 In the current study, the high genetic diversity among the mcr-1-positive E. coli strains #1, #2, and #3, which belonged to STs ST457, ST101, and ST1413, respectively, indicates that the isolates were unrelated. E. coli ST101 is considered as having an environmental lineage (related to water, sewage, and poultry), while many clinical isolates in multiple countries are also classified as E. coli ST101.20–22 It is also regarded as a reservoir for antibiotic resistance genes. The mcr-1-positive E. coli ST101 strains have been detected in chickens, public transportation, and one hospital in China.20,22,23 Thus, more attention should be focused on E. coli ST101 as it might promote the spread of mcr-1. In contrast, mcr-1-positive E. coli ST457 is very rare and we are the first to report ST1413 carrying mcr-1 in China.
In this study, we found that strain #1 carried one replicon (IncI1) and strain #2 carried two replicons (IncHI2 and IncN). Several studies have reported that the mcr-1 gene is primarily located on two prevalent plasmids (IncHI2 and IncI2).1,10,24–26 Consequently, these plasmids might play an important role in driving the spread of the mcr-1 gene. The conjugation experiment in this study, in which the mcr-1 gene was successfully transferred from strains #1 and #2 to the E. coli EC600 standard recipient, clearly demonstrates the potential for horizontal transfer of the mcr-1 gene. In contrast, in an experiment using the same methodology, strain #3 did not transfer the gene. This indicates that the mcr-1 gene of strain #3 might be located on a yet unknown non-conjugative plasmid. Further studies are required to elucidate and monitor the spread of the mcr-1 gene in China.
Previous reports on the epidemiology of mcr-1-positive members of the Enterobacteriaceae bacterial family have suggested a narrow variety of sources for bloodstream infection.7,17,18,27 Contrary to these findings, we have showed that mcr-1-positive E. coli might invade the bloodstream, not only from the urinary and biliary organs,7,17,18,27 but also from the respiratory tract and as primary, idiopathic infection. Some of our findings are in line with previous studies,7,17,18 however, since unhealthy patients might be vulnerable to mcr-1-positive E. coli bloodstream infection. Previous studies have established an association between infection and both kidney disease and diabetes mellitus,7,17,18 and, of the three patients in our study, two had cancer and one had diabetes mellitus. Of the three patients, two were treated with antibacterials in the 3-month period before admission to hospital. Interestingly, none of the patients received previous treatment with colistin or had close contact with farm animals. We postulate that considering the occurrence of mcr-1-positive Enterobacteriaceae in the environment, vegetables, and meat in China,28–30 the patients might have been exposed to the mcr-1 gene via these sources. Similar to previous reports,7,17,18,27 all three patients with mcr-1-positive E. coli bloodstream infection had a favorable outcome after treatment with antibacterials that they had been found to be susceptible to. However, Lai et al have reported that four patients out of ten (40%) succumbed to bloodstream infection despite being intensively treated (often with more than one antibacterial preparation).11 The inconsistent findings regarding the outcomes in these studies might be due to the small sample sizes.7,11,17,18,27
A limitation of our study is that the mcr-1-positive strains were not analyzed by whole-genome sequencing and thus further studies are required to better clarify the molecular characteristics of this resistance gene. However, this systematic investigation of all bloodstream infections caused by E. coli over a year in a Chinese hospital is noteworthy.
Conclusion
In an examination of 144 consecutive, non-repetitive, clinical samples of invasive E. coli isolates retrieved from a hospital in China over one year, we found three invasive E. coli isolates that were mcr-1-positive (2.1% of all samples). Patients, especially those with underlying diseases, may be infected with mcr-1-positive E. coli even if they have not received previous treatment with colistin. The three mcr-1-positive E. coli isolates had varied susceptibility profiles, although all three were susceptible to carbapenems. This therapeutic window is crucial given the risk of rapid deterioration in high-incidence areas of the world. We call for immediate inclusion of colistin in routine susceptibility testing in all microbiological laboratories in China.
Ethical approval
This study was approved by the Ethics Committee of the Xiangya Hospital of Central South University, and the requirement for informed consent from patients was waived because the study was retrospective and used a database that ensured confidentiality.
Acknowledgments
We thank Prof. Jianzhong Shen for offering the mcr-1-positive control strain. This work was supported by National Natural Science Foundation of China (81672066).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Quan J, Li X, Chen Y, et al. Prevalence of mcr-1 in Escherichia coli and Klebsiella pneumoniae recovered from bloodstream infections in China: a multicentre longitudinal study. Lancet Infect Dis. 2017;17(4):400–410. doi:10.1016/S1473-3099(16)30528-X
2. Long W, Yuan J, Liu J, et al. Multidrug resistant brain abscess due to Acinetobacter baumannii Ventriculitis cleared by intraventricular and intravenous tigecycline therapy: a case report and review of literature. Front Neurol. 2018;9:518. doi:10.3389/fneur.2018.00518
3. Olaitan AO, Morand S, Rolain JM. Mechanisms of polymyxin resistance: acquired and intrinsic resistance in bacteria. Front Microbiol. 2014;5:643. doi:10.3389/fmicb.2014.00643
4. Halaby T, Al Naiemi N, Kluytmans J, et al. Emergence of colistin resistance in Enterobacteriaceae after the introduction of selective digestive tract decontamination in an intensive care unit. Antimicrob Agents Chemother. 2013;57(7):3224–3229. doi:10.1128/AAC.02634-12
5. Liu YY, Wang Y, Walsh TR, et al. Emergence of plasmid-mediated colistin resistance mechanism MCR-1 in animals and human beings in China: a microbiological and molecular biological study. Lancet Infect Dis. 2016;16(2):161–168. doi:10.1016/S1473-3099(15)00424-7
6. Brennan E, Martins M, McCusker MP, et al. Multidrug-resistant Escherichia coli in bovine animals, Europe. Emerg Infect Dis. 2016;22(9):1650–1652. doi:10.3201/eid2209.160140
7. Hasman H, Hammerum AM, Hansen F, et al. Detection of mcr-1 encoding plasmid-mediated colistin-resistant Escherichia coli isolates from human bloodstream infection and imported chicken meat, Denmark 2015. Euro Surveill. 2015;20(49):30085. doi:10.2807/1560-7917.ES.2015.20.49.30085
8. Cao L, Li X, Xu Y, et al. Prevalence and molecular characteristics of mcr-1 colistin resistance in Escherichia coli: isolates of clinical infection from a Chinese University Hospital. Infect Drug Resist. 2018;11:1597–1603. doi:10.2147/IDR.S166726
9. Zhong LL, Phan HTT, Shen C, et al. High rates of human fecal carriage of mcr-1-positive multidrug-resistant Enterobacteriaceae emerge in China in association with successful plasmid families. Clin Infect Dis. 2018;66(5):676–685. doi: 10.1093/cid/cix885
10. Macesic N, Green D, Wang Z, et al. Detection of mcr-1-Carrying Escherichia coli causing bloodstream infection in a New York City Hospital: avian origins, human concerns? Open Forum Infect Dis. 2017;4(3):ofx115. doi:10.1093/ofid/ofx115
11. Lai CC, Lin YT, Lin YT, et al. Clinical characteristics of patients with bacteraemia due to the emergence of mcr-1-harbouring Enterobacteriaceae in humans and pigs in Taiwan. Int J Antimicrob Agents. 2018;52(5):651–657. doi:10.1016/j.ijantimicag.2018.08.015
12. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing: Twenty-seventh Informational Supplement M100-S27. Wayne, PA: Clinical and Laboratory Standards Institute; 2017.
13. European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters. European Committee on Antimicrobial Susceptibility Testing; 2017.Available from: http://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Breakpoint_tables/v_7.1_Breakpoint_Tables.pdf. Accessed July 05, 2019.
14. Johnson TJ, Wannemuehler YM, Johnson SJ, et al. Plasmid replicon typing of commensal and pathogenic Escherichia coli isolates. Appl Environ Microbiol. 2007;73(6):1976–1983. doi:10.1128/AEM.02171-06
15. Juhász E, Iván M, Pintér E, et al. Colistin resistance among blood culture isolates at a tertiary care centre in Hungary. J Glob Antimicrob Resist. 2017;11:167–170. doi:10.1016/j.jgar.2017.08.002
16. Nordmann P, Assouvie L, Prod’Hom G, et al. Screening of plasmid-mediated MCR-1 colistin-resistance from bacteremia. Eur J Clin Microbiol Infect Dis. 2016;35(11):1891–1892. doi:10.1007/s10096-016-2739-0
17. Corbella M, Mariani B, Ferrari C, et al. Three cases of mcr-1-positive colistin-resistant Escherichia coli bloodstream infections in Italy, August 2016 to January 2017. Euro Surveill. 2017;22(16):30517. doi:10.2807/1560-7917.ES.2017.22.16.30517
18. Nordmann P, Lienhard R, Kieffer N, et al. Plasmid-mediated colistin-resistant Escherichia coli in bacteremia in Switzerland. Clin Infect Dis. 2016;62(10):1322–1323. doi:10.1093/cid/ciw124
19. Poirel L, Jayol A, Nordmann P. Polymyxins: antibacterial activity, susceptibility testing, and resistance mechanisms encoded by plasmids or chromosomes. Clin Microbiol Rev. 2017;30(2):557–596. doi:10.1128/CMR.00064-16
20. Wang Y, Tian GB, Zhang R, et al. Prevalence, risk factors, outcomes, and molecular epidemiology of mcr-1-positive Enterobacteriaceae in patients and healthy adults from China: an epidemiological and clinical study. Lancet Infect Dis. 2017;17(4):390–399. doi:10.1016/S1473-3099(16)30527-8
21. Toleman MA, Bugert JJ, Nizam SA. Extensively drug-resistant New Delhi metallo-β-lactamase-encoding bacteria in the environment, Dhaka, Bangladesh, 2012. Emerg Infect Dis. 2015;21(6):1027–1030. doi:10.3201/eid2106.141578
22. Shen C, Feng S, Chen H, et al. Transmission of mcr-1-producing multidrug-resistant Enterobacteriaceae in public transportation in Guangzhou, China. Clin Infect Dis. 2018;67(Suppl 2):S217–S224. doi:10.1093/cid/ciy661
23. Wu C, Wang Y, Shi X, et al. Rapid rise of the ESBL and mcr-1 genes in Escherichia coli of chicken origin in China, 2008-2014. Emerg Microbes Infect. 2018;7(1):30. doi:10.1038/s41426-018-0033-1
24. Zheng B, Yu X, Xu H, et al. Complete genome sequencing and genomic characterization of two Escherichia coli strains co-producing MCR-1 and NDM-1 from bloodstream infection. Sci Rep. 2017;7(1):17885. doi:10.1038/s41598-017-18273-2
25. Mohsin J, Pál T, Petersen JE, et al. Plasmid-mediated colistin resistance gene mcr-1 in an Escherichia coli ST10 bloodstream isolate in the Sultanate of Oman. Microb Drug Resist. 2018;24(3):278–282. doi:10.1089/mdr.2017.0131
26. Xu L, Wang P, Cheng J, et al. Characterization of a novel blaNDM-5-harboring IncFII plasmid and an mcr-1-bearing IncI2 plasmid in a single Escherichia coli ST167 clinical isolate. Infect Drug Resist. 2019;12:511–519. doi:10.2147/IDR.S192998
27. Rossi F, Girardello R, Morais C, et al. Plasmid-mediated mcr-1 in carbapenem-susceptible Escherichia coli ST156 causing a blood infection: an unnoticeable spread of colistin resistance in Brazil? Clinics (Sao Paulo). 2017;72(10):642–644. doi:10.6061/clinics/2017(10)09
28. Ji X, Zheng B, Berglund B, et al. Dissemination of extended-spectrum β-lactamase-producing Escherichia coli carrying mcr-1 among multiple environmental sources in rural China and associated risk to human health. Environ Pollut. 2019;251:619–627. doi:10.1016/j.envpol.2019.05.002
29. Liu BT, Li X, Zhang Q, et al. Colistin-resistant mcr-positive Enterobacteriaceae in fresh vegetables, an increasing infectious threat in China. Int J Antimicrob Agents. 2019;54(1):89–94. doi:10.1016/j.ijantimicag.2019.04.013
30. Liu BT, Song FJ, Zou M. Characterization of highly prevalent plasmids coharboring mcr-1, oqxAB, and blaCTX-M and plasmids harboring oqxAB and blaCTX-M in Escherichia coli isolates from food-producing animals in China. Microb Drug Resist. 2019;25(1):108–119. doi:10.1089/mdr.2017.0391
Supplementary material
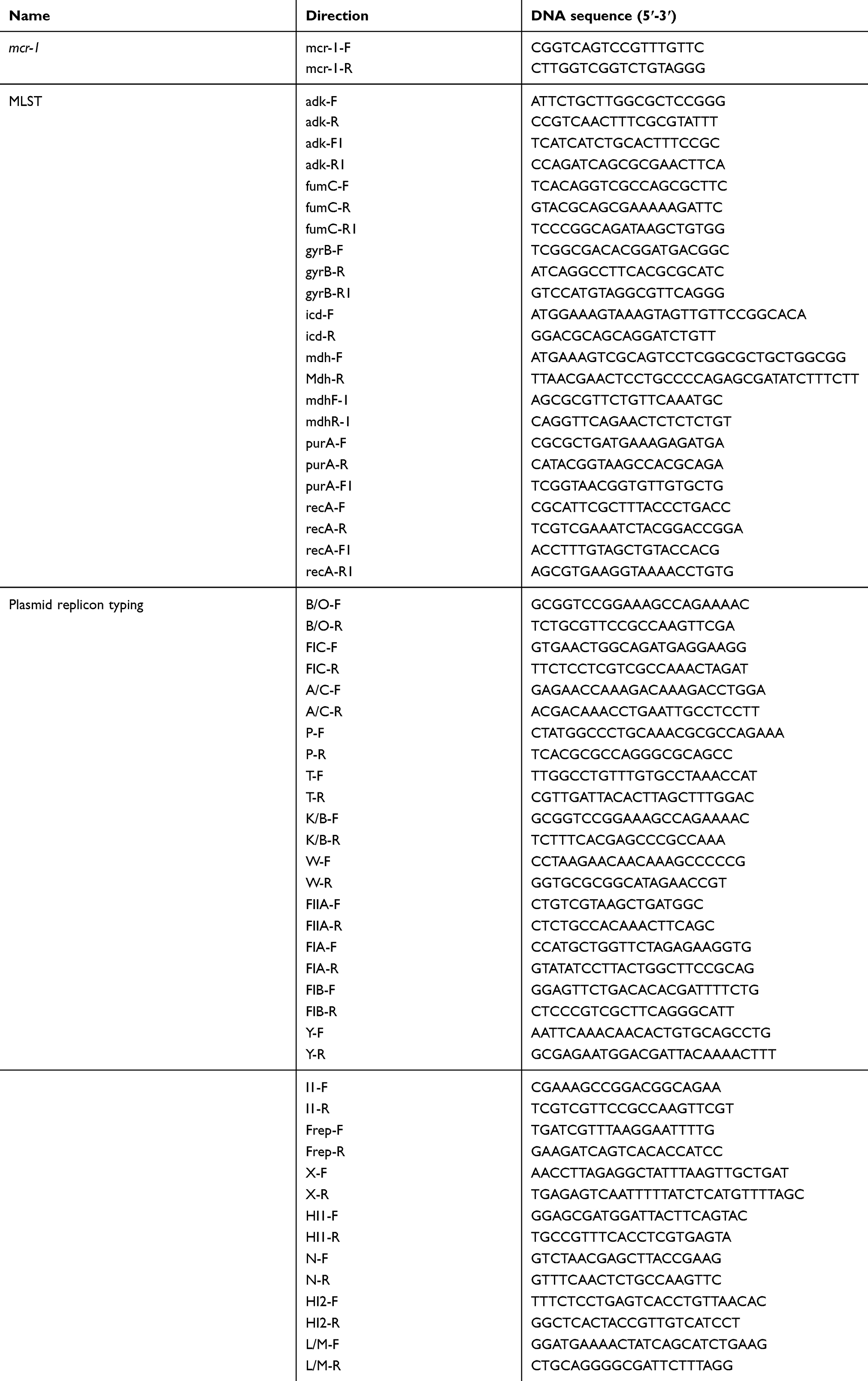 |
Table S1 The primers used for all PCR reactions in this study |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.