")
Back to Journals » Infection and Drug Resistance » Volume 15
Epidemiological Trend of RSV Infection Before and During COVID-19 Pandemic: A Three-Year Consecutive Study in China
Authors Qiu W, Zheng C, Huang S , Zhang Y, Chen Z
Received 1 September 2022
Accepted for publication 18 November 2022
Published 28 November 2022 Volume 2022:15 Pages 6829—6837
DOI https://doi.org/10.2147/IDR.S388231
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Weiling Qiu, Chen Zheng, Shumin Huang, Yuanyuan Zhang, Zhimin Chen
Department of Pulmonology, Children’s Hospital, Zhejiang University School of Medicine, National Clinical Research Center for Child Health, National Children’s Regional Medical Center, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Zhimin Chen, Department of Pulmonology, Children’s Hospital, Zhejiang University School of Medicine, National Clinical Research Center for Child Health, National Children’s Regional Medical Center, No. 3333, Binsheng Road, Binjiang District, Hangzhou, Zhejiang, 310052, People’s Republic of China, Tel +86-571-88873731, Fax +86-571-86658672, Email [email protected]
Objective: This study aimed to explore the epidemiological trend and clinical characteristics of respiratory syncytial virus (RSV) infection among inpatient children with lower respiratory tract infection (LRTI) before and during the coronavirus disease 2019 (COVID-19) pandemic.
Methods: A retrospective study of inpatients with LRTI was conducted at the Department of Pulmonology, The Children’s Hospital, Zhejiang University School of Medicine (Hangzhou, China) from January 2019 to December 2021. All respiratory specimens were tested for common respiratory pathogens. The clinical data in children with RSV-induced LRTI in the past three years were collected and analyzed.
Results: A total of 11,290 patients were enrolled, and RSV positive cases were 402 (7.6%), 288 (9.6%), 415 (13.8%) in 2019, 2020, 2021, respectively, with a significant statistical difference of the RSV positive rate among the three groups (p < 0.001). Most patients were under 2-year old, especially under 1-year old, and the median age of patients was 4 months, 5 months, 6 months in 2019, 2020, 2021, respectively, with a tendency to increase in age. In terms of the seasonal distribution, most patients of LRTI with RSV infection were admitted in winter, while in 2021 compared with in 2019, the cases significantly reduced in winter and increased in autumn. From 2019 to 2021, there was an increase in autumn trend year by year.
Conclusion: RSV infection was still an important cause of hospitalization in children with LRTI after the outbreak of COVID-19, and its proportion increased gradually. LRTI caused by RSV is still more common in infants under 1-year old, but there is a trend of increasing in older children. What deserves the attention of pediatricians and Center for Disease Control is that the incidence of RSV infection continues to rise in autumn, and the difference in seasonal distribution is narrowed.
Keywords: respiratory syncytial virus, RSV, COVID-19, lower respiratory tract infection, non-pharmaceutical interventions
Introduction
Acute respiratory infections are common among children worldwide. Lower respiratory tract infection (LRTI) caused by respiratory syncytial virus (RSV) is the main cause of hospitalization in children under 1 year of age and causes approximately 200,000 deaths among children aged less than five years, which mostly happened in resource-constrained countries.1 While COVID-19 pandemic has drastically changed the epidemiology of other viral respiratory infections, including RSV.2,3 Worldwide, the autumn and winter RSV epidemics have virtually disappeared in 2020, and in some countries in the Southern Hemisphere like South Africa or Australia, the RSV season has moved to spring, marking an unprecedented phenomenon.3
In China, the government has enforced comprehensive and stringent non-pharmaceutical interventions (NPIs) since the pandemic, such as social distancing, enhanced hand hygiene, mask-wearing, working from home and school closures, to reduce the transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) at the early stage of the epidemic.4 In most cities of China, NPIs were strictly implemented in the first half of 2020. For example, in Hangzhou, working from home, school closings and public cultural or entertainment venue closures had been implemented for several months. It was not until 2021 that interventions to close schools and other public places throughout the whole society were canceled, but the “relaxed NPIs” including physical distancing and mask-wearing were still mandatory in public places. If SARS-CoV-2 positive cases occur, the certain area would be designated as a high-risk area, where stringent NPIs would be implemented. Up to now, the relaxed NPIs and NPIs in high-risk areas are still being implemented, which may become normalized during the pandemic. These interventions were quite different from those in many other countries, which might have a significant impact on the epidemiology of other respiratory viruses in both children and adults. Therefore, it is necessary to understand whether the epidemiological trend of RSV infection in China is different from that in other countries after the outbreak of COVID-19 pandemic.
Understanding the epidemiological trend of RSV is of great significance to the health of young children as it is the main pathogen of LRTI in infants. Recently, some studies have focused on the trend of respiratory viruses during the pandemic period in China,5,6 but they are mainly based on laboratory results and lack of analysis of consecutive years of clinical data. In this study, we reported and discussed the transmission pattern and clinical characteristics of RSV among inpatient children with LRTI in Hangzhou, before and after the outbreak of COVID‐19. We focused primarily on the comparison of clinical data for three consecutive years, with the aim to investigate the long-term effects of the China’s epidemic prevention and control measures on the epidemiology of RSV among inpatient children with LRTI.
Materials and Methods
Study Design
To explore the epidemiological trend of RSV among inpatient children with LRTI before and during the COVID-19 pandemic, all patients who met the criteria were continuously recruited at the Children’s Hospital of Zhejiang University School of Medicine from January 1, 2019 to December 31, 2021. The inclusion criteria were as follows: (1) patients more than 28 days and under 18 years old; (2) diagnosed with LRTI, presenting with fever and lower respiratory tract symptoms, such as tachypnea, nonproductive cough, wheeze, and increased breath sound,7 as well as one of the conditions for signs of LRTI (rales or wheezes) or chest imaging findings (bronchitis or pneumonia) to be met, including the diagnosis of pneumonia, bronchitis, bronchiolitis and prolonged pneumonia; (3) Admission to respiratory ward during 1 January 2019 to 31 December 2021. We excluded children with underlying diseases, such as congenital heart disease, immune deficiency, and chronic lung disease. Respiratory pathogens of all enrolled patients were analyzed. Among them, the clinical data of RSV positive children, including age, gender, length of stay (LOS), season distribution, co-infected pathogens and diagnosis were comprehensively analyzed to evaluate the impact of the pandemic on them.
Measurement
Respiratory specimens (pharyngeal swabs or nasopharyngeal aspirates) were collected from all of the enrolled inpatients with LRTI by trained staff following standard operating procedures. The specimens were tested by direct immunofluorescence (DIF) test for seven respiratory viruses, including RSV, influenza virus A (Flu A), influenza virus B (Flu B), adenovirus (ADV), Para-influenza virus 1 (PIV-1), Parainfluenza virus 2 (PIV-2), Para-influenza virus 3 (PIV-3), by Polymerase chain reaction (PCR) for Mycoplasma pneumonia (MP), Chlamydia trachomatis (CT), and by bacteria culture for bacteria. If RSV was detected, the patient was considered positive for RSV and was enrolled for further analysis. Meanwhile, the co-infection was evaluated according to the test results of other pathogens.
According to the year of admission, we defined three groups: 2019, 2020 and 2021. 2019 is considered the “pre-COVID-19” period, without nationwide NPIs; 2020 and 2021 are the “post- COVID-19” period, including “COVID-19 pandemic” period, when stringent NPIs or relaxed NPIs were implemented. Under the current COVID-19 prevention measures in China, there is no clear boundary between the “COVID-19 pandemic” period and the “post-COVID-19” period, but the observation study for three consecutive years can reflect the trend of RSV infection after the outbreak of COVID-19.
Data Processing and Statistical Analyses
Categorical variables were expressed as numbers (%). The ages and length of stay (LOS) of the patients were expressed as medians and interquartile ranges (IQR), as they were not normally distributed. χ2 tests and rank‐sum tests were used when making comparisons among respective groups. A p value below 0.05 was considered to indicate a statistically significant difference. We performed statistical analysis with SPSS version 24.0.
Results
Overall
During the whole study period, a total of 11,290 patients who met the inclusion criteria were enrolled, including 5271 in 2019, 3006 in 2020, and 3013 in 2021. RSV positive cases were 402 (7.6%), 288 (9.6%), 415 (13.8%) in 2019, 2020, 2021, respectively, with a significant statistical difference of the RSV positive rate among the three groups (p < 0.001). The characteristics of LRTI with RSV infection in 2019 to 2021 are shown in Table 1. The patients in 2021 (median age: 6 months) were older than those in 2019 (median age: 4 months). There was no difference in gender and in LOS among patients in three groups. In terms of diagnosis, bronchopneumonia accounted for the largest proportion, followed by bronchiolitis in all three years. In the assessment of disease severity, the proportion of severe pneumonia in 2019, 2020 and 2021 was 23.5%, 28.1% and 14.9%, respectively, with a statistically different between 2020 and 2021. The cases of co-infection with other pathogens were 96 (23.9%), 42 (14.6%) and 45 (10.8%) in 2019, 2020 and 2021, respectively. From 2019 to 2021, the co-infection rate gradually decreased. From the specific pathogen of co-infection, bacterial infection was the most common, especially Streptococcus pneumoniae, Moraxella catarrhalis, Staphylococcus aureus, Haemophilus influenzae, Escherichia coli, and Pseudomonas aeruginosa. In addition, other co-infected bacteria included Enterobacter aerogenes, Pseudomonas aeruginosa and Raoul ornithinolytica in 2019, Acinetobacter baumannii and Klebsiella acidogenes in 2020, and Streptococcus intermedius, Enterobacter cloacae, and Serratia marcescens in 2021. The incidence of co-infections with other respiratory viruses was the lowest in 2021. The incidence of co-infections with viruses decreased year by year and with a statistical difference. Co-infection with ADV and MP was significantly lower in 2021 than in 2019. Age stratification and seasonal distribution were described in detail below.
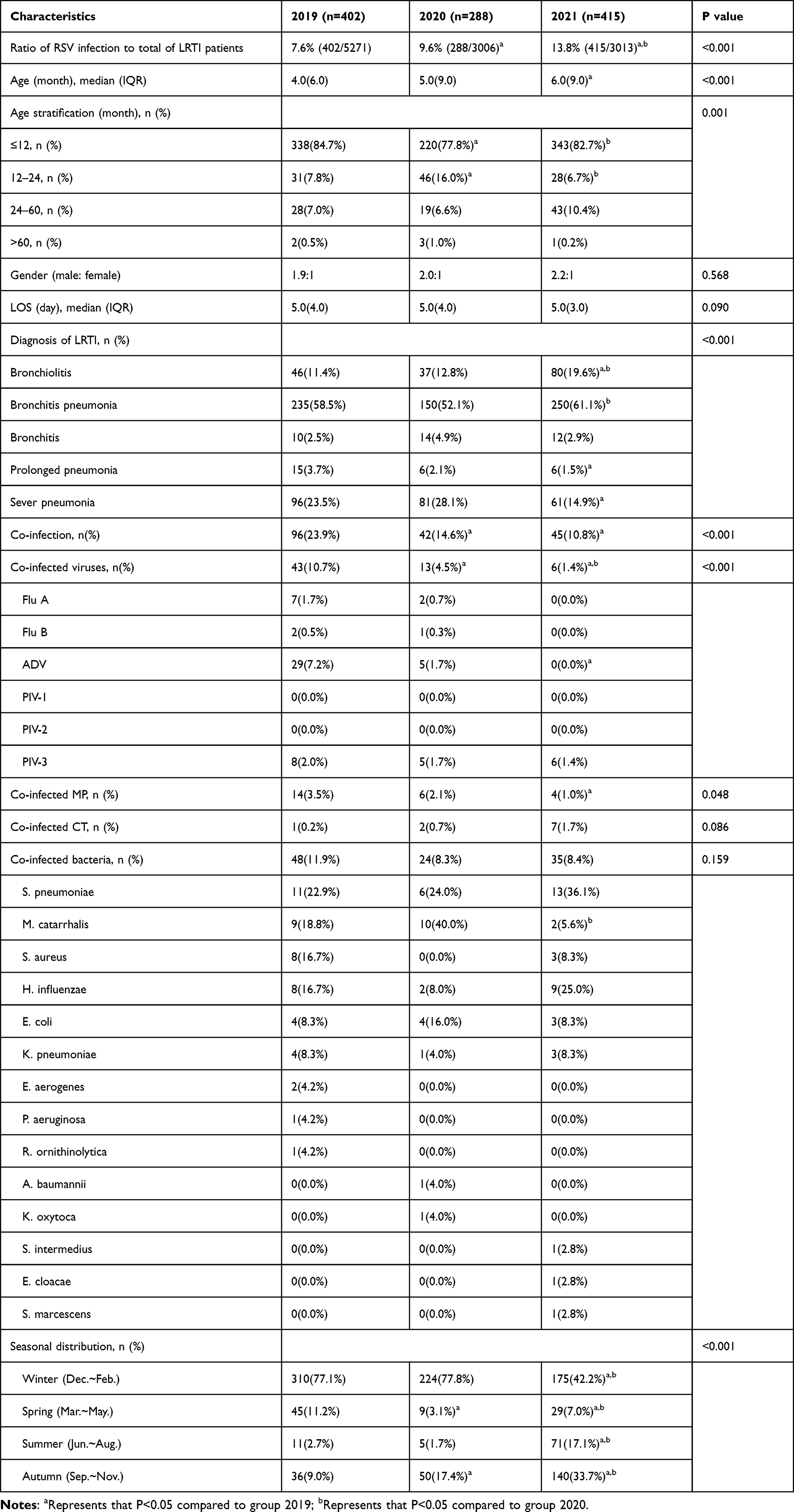 |
Table 1 Characteristics of LRTI with RSV Infection in 2019 to 2021 |
Age Stratification
All patients were divided into 5 grades according to their age, which were ≤12 months, 12–24 months, 24–60 months and >60 months. Most patients were under 2 years old, especially under 1-year old, accounting for 77.8%–84.7%. In 2020, compared with the other two groups, the number of patients <12 months was less, and the number of patients aged from 12 to 24 months was more, with a statistical difference. There were more children aged 24–60 months in 2021, and the proportion was even higher than that of children aged 12–24 months (Figure 1).
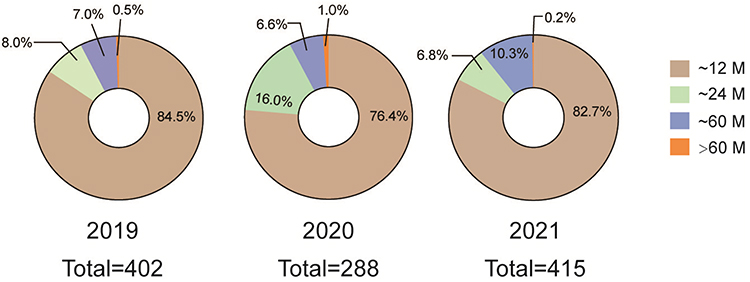 |
Figure 1 Proportion of different age groups in RSV positive children in 2019, 2020 and 2021. |
Seasonal Distribution
We defined December to February as winter, March to May as spring, June to August as summer, and September to November as autumn. Depending on when the patients were admitted, they were divided into 4 admission periods, winter, spring, summer and autumn. It showed that the incidence was highest in winter, while in 2021 compared with the other two groups, it was significantly reduced, with a statistical difference. Instead, in 2021, there was an increase of the incidence in autumn, almost equal to that in winter. The number of patients in spring was the lowest in 2020 and the largest in 2019, with statistical differences between every two groups. In summer, the number of cases in 2021 was the largest, which was significantly higher than the other two groups, with a statistical difference. It is worth noting that from 2019 to 2021, there was an increasing trend in autumn year by year (Figure 2).
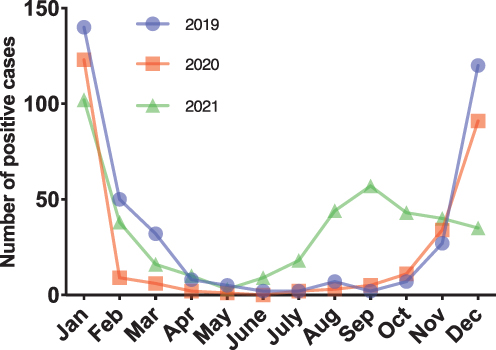 |
Figure 2 Proportion of RSV positive children in different seasons in 2019, 2020 and 2021 and the total cases of each year. |
Based on the distribution of cases in every month, RSV is the respiratory virus with a seasonal distribution pattern with more positive cases in the winter months, before the COVID-19 pandemic. In 2019, RSV detection declined sharply since February and remained at low levels until the autumn (October) and then increased steadily. The positive cases of September to November 2020 were even higher than that in 2019. In 2021, the seasonal distribution trend is significantly different from the previous two years, before entering the winter peak period, an obvious peak period in September was seen (Figure 3).
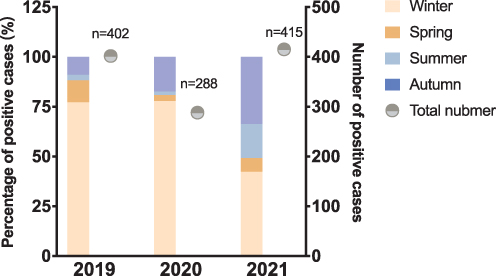 |
Figure 3 The monthly distribution of RSV positive cases in 2019, 2020 and 2021. |
Discussion
The present study promotes our understanding of epidemic trend and clinical characteristics of RSV infection before and after COVID-19 pandemic, and the three consecutive years of clinical data also presented the epidemic trend under different prevention and control interventions. Epidemic prevention measures vary in different countries and regions, and our results showed the prevalence of RSV in southeast China before and after the pandemic.
Mitigation of the COVID-19 pandemic has necessitated extraordinary changes to community behavior at a population level and affected the transmission of endemic respiratory pathogens.8 Reports from around the world have revealed up to a 98% reduction in RSV cases during the pandemic.3,9 It is reasonable to hypothesize that the restrictive measures adopted to reduce SARS-CoV-2 diffusion had an impact on other respiratory viruses with similar routes of infection. The major interventions at a global level were NPIs, such as stay-at-home orders, social distancing, hand hygiene and mandatory face masks. All of these interventions contribute to reduce RSV transmission through droplets and contact through dirty hands and fomites.10 Specifically, hand washing reduces the virus’ capability to infect the host, disrupting the viral envelope, face masks block RSV transmission through droplets, and social distancing reduces the chances to have contact with infected people.11 Besides, during the severe period of COVID-19, people’s visit to hospitals for emergencies and face-to-face outpatient clinic visits were delayed, and most patients did not want to present to hospitals due to mild clinical issues. These also explain the phenomenon of sharp decline in RSV cases in February 2020 and the highest proportion of severe pneumonia in 2020 found in our study. The resurgence of RSV infection after the pandemic has raised a concern.2,12 An Australian study suggested that COVID-19 public health measures were associated with suppression of the 2020 southern hemisphere respiratory syncytial virus (RSV) season, and an unseasonal resurgence of RSV infections was observed after the relaxation of interventions.12 It was likely driven by a buildup in population susceptibility coupled with relaxed community behaviors.
Since early 2020, Hangzhou has always asked to maintain social distances, hand hygiene and wearing masks. Once a SARS-CoV-2 positive case is found, local areas are required to work from home, and close the school. However, from the results of the present study, the RSV infection rate did not decrease due to NPIs. Instead, it has increased year by year. It should be pointed out that there were 40% fewer illnesses evaluated in 2020 and 2021 compared to 2019, which may be related to the stricter admission criteria for patients under the pandemic situation and the NPIs taken under the pandemic. However, the increased RSV infection proportion in children with LRTI indicated that children with RSV infection had a higher need for hospitalization.
Based on the comparison of three consecutive years of data, the clinical characteristics of RSV infection were different before and during the pandemic. RSV infections mainly occurred in children under 1-year old, and we observed a modest increase in the median age of children (6 vs 4 months). It is worth noting that the percentage of children aged 2 to 5 years in 2021 was slightly increased compared with previous years, which is consistent with some previous findings. Saravanos et al observed a paradoxical increase in the frequency of RSV infections in children aged 2 to 4 years in 2020 compared with previous years, and they believed that a lower threshold for respiratory virus testing in the context of the COVID-19 pandemic likely contributed to the increases in RSV-related disease and older age distribution.12 Children with respiratory symptoms get increased testing during the pandemic, and whether the increase of RSV infection in older children is a trend after COVID-19 pandemic is worthy of further study.
We found decreased proportion of severe pneumonia in children of post-COVID-19 period (in 2021) compared with pre-COVID-19 period (in 2019). Recently published studies from Europe and Australia provide further evidence that the delayed RSV epidemic was no more severe than previous seasons based on an examination of clinical outcomes, including length of stay and intensive care requirement.12–14 However, the proportion of severe pneumonia in our study was higher in 2020, which may be related to stricter admission criteria during the severe period of the pandemic. Ongoing research is needed to understand the impact of disrupted RSV transmission on disease severity in different settings and over time.
Our study analyzed the combined pathogens of LRTI caused by RSV but did not separately analyze the trend of other respiratory viruses before and during the pandemic. The co-infection rate of Flu, ADV, PIV and MP with RSV decreased in post-COVID-2019 period, especially ADV and MP, with a statistical difference. Similar to the result as our study, some studies analyzed the epidemiological trend of common respiratory viruses indicated that compared with RSV, the suppression of Flu virus was more obvious during the pandemic.5,12 It is suggested that the transmission dynamics of Flu and RSV may be different. Influenza virus circulation may be more sensitive to COVID-19–related public health measures, in particular global travel restrictions, than RSV.8 From our research, it should be considered that Flu, ADV and MP might be more sensitive to social health measures than RSV. It should be noted that in the three consecutive years before and after the pandemic, many RSV positive children were co-infected with bacteria, which may be related to the fact that most children with RSV infection were young and were prone to secondary bacterial infection. It also suggested that social health measures might have little effect on bacterial infections.
RSV circulation may not be as sensitive to COVID-19 related public health measures, in particular global travel restrictions, as other respiratory virus, and the reasons deserve further investigation. The studies in Australia observed a striking predominance of RSV-A in 2020, and it likely continued to circulate at low levels in the population during COVID-19 restrictions.12,15 It has been reported that a localized inflammatory response could be induced after infection with the Flu, while circulation of the Flu in 2020 was suppressed.16,17 Therefore, it can be explained that RSV could be the predominant respiratory virus and should be monitored more diligently in children in the future.
From Figure 3, RSV-positive cases was suppressed in the spring of 2020, when the most restrictive NPIs were enforced, and recovered by autumn, when the relaxed-NPIs were still sustained, indicating that the relaxed-NPIs were ineffective in inhibiting RSV transmission. The positive cases increased in autumn every year, and a peak of incidence occurred in the autumn of 2021, reflecting the changes in the peak season of RSV after the pandemic, which needs to attract the attention of pediatricians. At present, there were few studies on RSV for more than three consecutive years after the outbreak, and it is not sure whether it will become another peak of RSV in autumn in China. However, from the present study, we can see that the seasonal difference of RSV infection is gradually narrowing.
Strengths of our study include use of a large sample of database for three consecutive years, combined with clinical data, and stratified by age and disease severity to compare the trends of RSV before and after the pandemic. A limitation of the study is that stricter admission criteria during the outbreak may create selection bias. Second, it is a single-center study, and it would be more convincing if the data were from different centers. In addition, RSV typing was absent and we failed to explore the mechanism of changes in clinical characteristics and epidemic trend of RSV infection after the epidemic, which was limited by our laboratory testing methods and the fact that the study was a retrospective study.
Conclusion
In conclusion, RSV infection was still an important cause of hospitalization in children with LRTI after the outbreak of COVID-19, and its proportion increased gradually. LRTI caused by RSV was still more common in infants under 1-year old, but there is a trend of increasing in older children. It is worth noting that the incidence of RSV infection increased continuously in autumn, and the seasonal distribution difference narrowed. COVID-19-related public health measures taken in China may continue to have an impact on the circulation of RSV, and our study may suggest future epidemics. It should emphasize the need for robust RSV surveillance to support policy decisions and research related to RSV prophylaxis, future vaccines, and non-pharmaceutical prevention strategies considering the important position of RSV in infantile LRTI.
Abbreviations
RSV, respiratory syncytial virus; LRTI, lower respiratory tract infection; COVID-19, coronavirus disease 2019; MP, Mycoplasma pneumonia; CT, Chlamydia trachomatis; NPIs, non-pharmaceutical interventions; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; DIF, direct immunofluorescence; Flu A, influenza virus A; Flu B, influenza virus B; ADV, adenovirus; PIV-1, Para-influenza virus 1; PIV-2, Para-influenza virus 2; PIV-3, Para-influenza virus 3; PCR, Polymerase chain reaction; LOS, length of stay; IQR, interquartile ranges.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Statements
This study was approved by Medical Ethics Committee of affiliated hospital of The Children’s Hospital, Zhejiang University School of Medicine in accordance with the Declaration of Helsinki (2021-IRB-325). The application for excepting informed consent was approved as the clinical data was retrospectively studied. The informed consent was waived due to the retrospective and anonymous nature of this study. We declare that the privacy of the participants was covered and the data was maintained with confidentiality throughout the study.
Acknowledgments
The authors thank the National Natural Science Foundation of China, Zhejiang Provincial Natural Science Foundation of China, Grant from the Key Program of the Independent Design Project of National Clinical Research Center for Child Health and Zhejiang Provincial Key R & D Projects for sponsoring the study and the participating children and their parents. The funding body had no role in the design of the study, the collection, analysis, and interpretation of data, or in writing the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Zhejiang Provincial Natural Science Foundation of China (LY22H100007), the Grant from the Key Program of the Independent Design Project of National Clinical Research Center for Child Health (G20B0003), Zhejiang Provincial Key R & D Projects (No. 2020C03062).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nair H, Nokes DJ, Gessner BD, et al. Global burden of acute lower respiratory infections due to respiratory syncytial virus in young children: a systematic review and meta-analysis. Lancet. 2010;375(9725):1545–1555. doi:10.1016/S0140-6736(10)60206-1
2. Agha R, Avner JR. Delayed seasonal RSV surge observed during the COVID-19 pandemic. Pediatrics. 2021;148(3):e2021052089. doi:10.1542/peds.2021-052089
3. Yeoh DK, Foley DA, Minney-Smith CA, et al. Impact of coronavirus disease 2019 public health measures on detections of influenza and respiratory syncytial virus in children during the 2020 Australian winter. Clin Infect Dis. 2021;72(12):2199–2202. doi:10.1093/cid/ciaa1475
4. Pan A, Liu L, Wang C, et al. Association of public health interventions with the epidemiology of the COVID-19 outbreak in Wuhan, China. JAMA. 2020;323(19):1915–1923. doi:10.1001/jama
5. Ye Q, Wang DJ. Epidemiological changes of common respiratory viruses in children during the COVID-19 pandemic. J Med Virol. 2022;94(5):1990–1997. doi:10.1002/jmv.27570
6. Liu PC, Xu MH, Lu LJ, et al. The changing pattern of common respiratory and enteric viruses among outpatient children in Shanghai, China: two years of the COVID-19 pandemic. J Med Virol. 2022;94(10):4696–4703. doi:10.1002/jmv.27896
7. Pabbaraju K, Wong S, Tokaryk KL, et al. Comparison of the Luminex xTAG respiratory viral panel with xTAG respiratory viral panel fast for diagnosis of respiratory virus infections. J Clin Microbiol. 2011;49(5):1738–1744. doi:10.1128/JCM.02090-10
8. Sullivan SG, Carlson S, Cheng AC, et al. Where has all the influenza gone? The impact of COVID-19 on the circulation of influenza and other respiratory viruses. Euro Surveill. 2020;25(47):2001847. doi:10.2807/1560-7917.ES.2020.25.47.2001847
9. Brusselen DV, Troeyer KD, Haar ET, et al. Bronchiolitis in COVID-19 times: a nearly absent disease? Eur J Pediatr. 2021;180(6):1969–1973. doi:10.1007/s00431-021-03968-6
10. Piedimonte G, Perez MK. Respiratory syncytial virus infection and bronchiolitis. Pediatr Rev. 2014;35(12):519–530. doi:10.1542/pir.35-12-519
11. Britton PN, Hu N, Saravanos G, et al. COVID-19 public health measures and respiratory syncytial virus. Lancet Child Adolesc Health. 2020;4(11):e42–e43. doi:10.1016/S2352-4642(20)30307-2
12. Saravanos GL, Hu N, Homaira N, et al. RSV epidemiology in Australia before and during COVID-19. Pediatrics. 2022;149(2):e2021053537. doi:10.1542/peds.2021-053537
13. Fourgeaud J, Toubiana J, Chappuy H, et al. Impact of public health measures on the post-COVID-19 respiratory syncytial virus epidemics in France. Eur J Clin Microbiol Infect Dis. 2021;40(11):2389–2395. doi:10.1007/s10096-021-04323-1
14. Foley DA, Phuong LK, Peplinski J, et al. Examining the interseasonal resurgence of respiratory syncytial virus in Western Australia. Arch Dis Child. 2022;107(3):e7. doi:10.1136/archdischild-2021-322507
15. Eden J-S, Sikazwe C, Xie R, et al. Off-season RSV epidemics in Australia after easing of COVID-19 restrictions. Nat Commun. 2022;13(1):2884. doi:10.1038/s41467-022-30485-3
16. Nickbakhsh S, Mair C, Matthews L, et al. Virus-virus interactions impact the population dynamics of influenza and the common cold. Proc Natl Acad Sci USA. 2019;116(52):27142–27150. doi:10.1073/pnas.1911083116
17. Chan KF, Carolan LA, Korenkov D, et al. Investigating viral inter- ference between influenza A virus and human respiratory syncytial virus in a ferret model of infection. J Infect Dis. 2018;218(3):406–417. doi:10.1093/infdis/jiy184
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.