")
Back to Journals » Clinical and Experimental Gastroenterology » Volume 12
Eosinophilic esophagitis incidence in New Zealand: high but not increasing
Authors Weerasekera K, Sim D, Coughlan F, Inns S
Received 21 May 2019
Accepted for publication 16 July 2019
Published 31 July 2019 Volume 2019:12 Pages 367—374
DOI https://doi.org/10.2147/CEG.S216126
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Andreas M. Kaiser
Kavindu Weerasekera,1 Dalice Sim,2 Finbarr Coughlan,3 Stephen Inns1
1Department of Medicine, University of Otago, Wellington, New Zealand; 2Department of Public Health, University of Otago, Wellington, New Zealand; 3Department of Pathology, Capital & Coast District Health Board, Wellington, New Zealand
Background and aim: Eosinophilic esophagitis (EoE) is an immune-mediated inflammatory condition of the esophagus. Recent literature has shown an increasing incidence of the disease. However, no epidemiological data exist regarding New Zealand rates of EoE. The disease is associated with atopy, and New Zealand’s high rate of atopic disease means the disease may be important in our population. We carried out a retrospective study to describe the incidence of EoE in the Wellington region of New Zealand, as well as key histological and clinical factors associated with the disease.
Method: A search was made of laboratory and endoscopic databases in the Wellington region to identify all diagnosed cases in the five years between January 1, 2011, and December 31, 2015. Case notes were examined to determine the key demographic and clinical parameters in the cases. Incidence rates were calculated for each year, and the effects of age group and sex on the incidence rates were analyzed.
Result: We found 152 cases of EoE in the Wellington region with an annual incidence of 6.95 per 100,000 person/years. We found no evidence of a significant difference in incidence rates by year in our study population. There was a significantly lower incidence rate in those aged <16 compared to those aged ≥16 (RR=0.26). Males had a higher incidence rate than females with an estimated rate ratio of 2.45 (p<0.05).
Conclusion: Our results are in contrast to previous reports of increasing incidence rates and may reflect a leveling off of incidence. Further research is needed to determine whether the low incidence in our pediatric age group is due to ascertainment bias or due to a real difference in the epidemiology of EoE in NZ compared to other countries.
Keywords: eosinophilic esophagitis, incidence, epidemiology
Introduction
Eosinophilic esophagitis (EoE) is an immune-mediated inflammatory condition of the esophagus that causes difficulty with swallowing (dysphagia).1 Over time, EoE can cause the esophagus to narrow, which can result in a food bolus becoming stuck or impacted within the esophagus requiring endoscopic removal.2,3
First identified in 1989, it was previously thought to be a rare disease but is now recognized as being relatively common. A recent meta-analysis found a pooled incidence rate of 3.7 per 100,000 persons per year.4 Several studies also report increasing incidence rates of EoE.5–12 However, no epidemiological data exist regarding New Zealand rates of EoE. EoE is associated with allergy.13,14 Some studies show that around 38–66% of patients with EoE have some kind of an allergic condition.3,8,15,16 New Zealand’s high rate of atopic disease suggests this disease might be important in our population.17,18
EoE is difficult to diagnose as its symptoms overlap with that of the more common condition gastroesophageal reflux disease (GORD).19 Hence, to diagnose EoE, patients must exhibit both clinical and endoscopic features as well as pathological features. Typical clinical features are dysphagia, throat/chest/abdominal pain, nausea and vomiting. Endoscopy commonly reveals ridging and furrowing of the esophagus as well as fragility of the esophageal epithelium, white plaques on the epithelial surface and sometimes strictures of the esophagus. The hallmark pathological feature is eosinophilic infiltrate in an esophageal biopsy amounting to more than 15 eosinophils per high power field (hpf).20 Studies show that EoE is more common in Caucasian males and affects both adults and children.4,20
EoE is a relatively new disease, and consensus guidelines for its diagnosis were first written in 2011.20 As a result, it has been unclear whether reports of increasing incidence rates reflect a true increase due to external factors or are simply due to an increased awareness and recognition of EoE.6,7,11,12
We carried out a retrospective, population-based study to describe the epidemiology of EoE in the Wellington region of New Zealand over the 5 years, from January 1, 2011, through to December 31, 2015. All cases of EoE were identified by examining endoscopic and pathological databases in the region.
Materials and methods
This study had ethical approval from the University of Otago Human Ethics Committee.
Population
The regional population of Wellington was 471,315 in the 2013 census.21 This ranked Wellington as the third most populated region in New Zealand after Auckland and Canterbury, respectively. As of the 2013 census, 11.1% of the population of New Zealand resided in Wellington, and of this 77% were of European descent. The remainder comprised of Māori (13%), Asian (10.5%), Pacific Island (8%) and people of other ethnicities (3.3%). In this study, where a person reported more than one ethnic group, they were counted in each applicable group. In the Wellington region, 13.2% of people are aged over 65 years, whilst 19.5% are under the age of 15 years.
The residents in the Wellington region, defined by the boundaries of the Capital and Coast District Health Board (CCDHB) and the Hutt Valley District Health Board (HVDHB), were chosen as the target population. CCDHB is based in Wellington and covers an area from Wellington up to Waikanae along the Kapiti Coast. HVDHB is based in Lower Hutt and covers an area including Upper Hutt, Wainuiomata and Eastbourne.
Most New Zealanders use the public health system; however, around 30% have private hospital cover.22 Therefore, patients attending these clinics and hospitals were identified also.
Case definition
Following the 2011 consensus guidelines for the diagnosis of EoE, cases for the period from January 1, 2011, to December 31, 2015, were identified through esophageal biopsy specimens containing ≥15 intraepithelial eosinophils per hpf in a patient with symptoms of esophageal dysfunction, dysphagia, food bolus impaction, esophageal/chest/abdominal pain, vomiting and/or an endoscopic appearance suggestive of EoE (ringed/corrugated esophagus, linear furrows, strictures, white surface exudates and crepe paper esophagus).
Case finding and clinical information
Potential cases of EoE were identified by searching regional endoscopy and histology databases both at the public hospitals, private hospitals and in the private laboratory. The histology laboratory databases were searched for the term “eosinophil”, except one database which provided the facility for a SNOMED search for patients that had their biopsy categorized under the code T62 (esophagus), M47150 (eosinophilic inflammation) or T62 M40000 (inflammation). For DHB patients, clinical data were obtained from a centralized data repository used to store patient information and hospital records. This repository was also used to ensure that there were no biopsy reports with an eosinophil count of ≥15/hpf prior to 2011. For patients in the private setting, clinical information was sought from the caring clinician. Pathology reports from private hospitals were stored in a central database which were used to identify potential patients with EoE. Permission was obtained from each of the four private centers (Boulcott clinic, Bowen hospital, Southern Cross hospital and Wakefield hospital) before the caring clinician was approached to obtain the endoscopy report.
All biopsies that were reported as being “diagnostic of” or “consistent with” a diagnosis of EoE (ie, without an exact eosinophil count) were reanalyzed by a pathologist (FC) to ensure an eosinophil count of ≥15/hpf. Histological features evident in the biopsy, number and location of biopsies taken as well as the eosinophil count in each location was also collected.
To verify a new diagnosis of EoE, all endoscopy reports prior to the diagnostic endoscopy were reviewed in order to ensure a diagnosis had not been made outside of the study period. Every patient in NZ is assigned a unique NHI (National Health Index) number, and this was used to ensure that no patients were included more than once in the study. All data accessed were anonymized.
Statistical analysis
Crude incidence rates were calculated by dividing the number of new cases of EoE by the annual mid-year population of the predefined Wellington Region during the study period from 2011 to 2016 (not inclusive). Population sizes for each respective year were obtained from Statistics NZ.
The clinical data were described using proportions for categorical variables and means and SDs for continuous variables using SPSS Statistics for Windows, Version 24.0. Armonk, NY: IBM Corp. A Poisson regression model was used to analyze the effects of age group, sex and year on the incidence rates.
Results
Baseline characteristics
During the 5-year period from January 1, 2011, to December 31, 2015, we found a total of 152 new cases of EoE in the Wellington region. The demographics of those diagnosed with EoE are shown in Table 1.
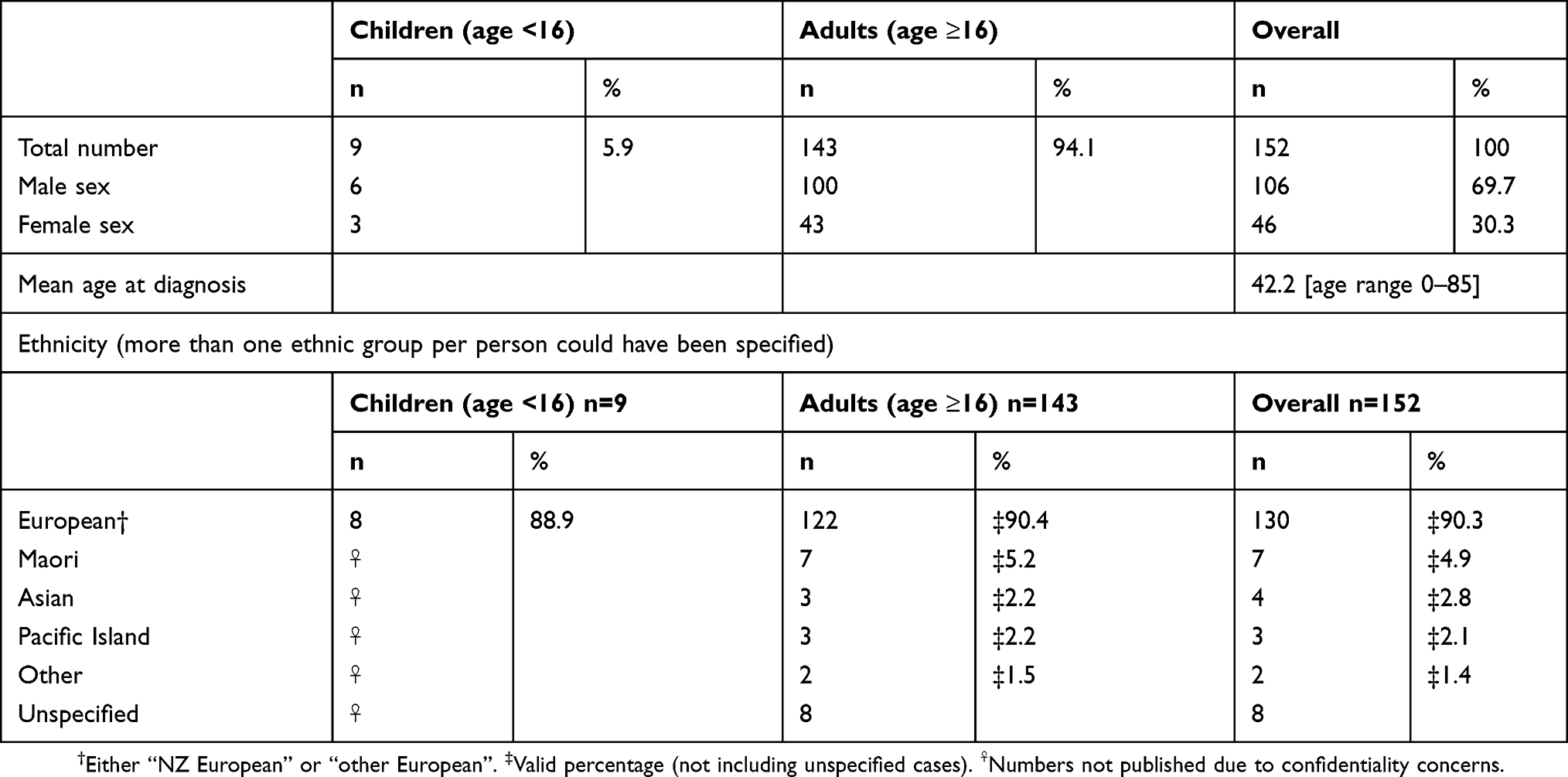 |
Table 1 Characteristics of patients with eosinophilic esophagitis |
Dysphagia and food bolus impaction were the two most common indications for an endoscopy as shown in Table 2. More than half of the pediatric patients’ indication for endoscopy was either abdominal/chest pain or nausea/vomiting.
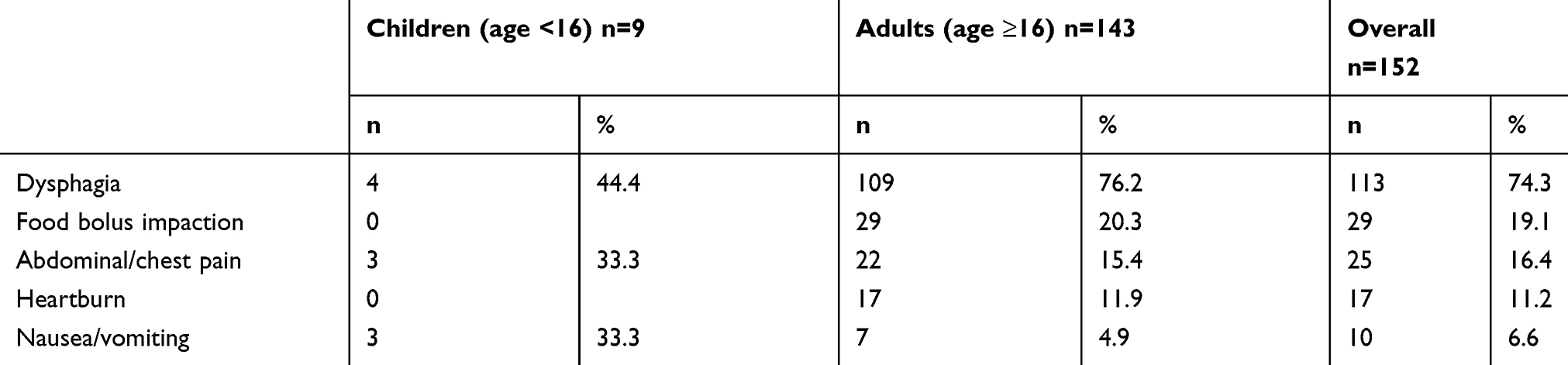 |
Table 2 Indication for endoscopy (patients could present with >1 indication) |
The most common endoscopic feature was a ringed/corrugated esophagus, and this was followed by the appearance of furrows in the esophagus. Endoscopic features were not mentioned in the endoscopy report in 48 (31.6%) cases as shown in Table 3. This rate was similar between both groups. Basal cell hyperplasia and elongated vascular papillae were the most common histologic features – refer to Table 4.
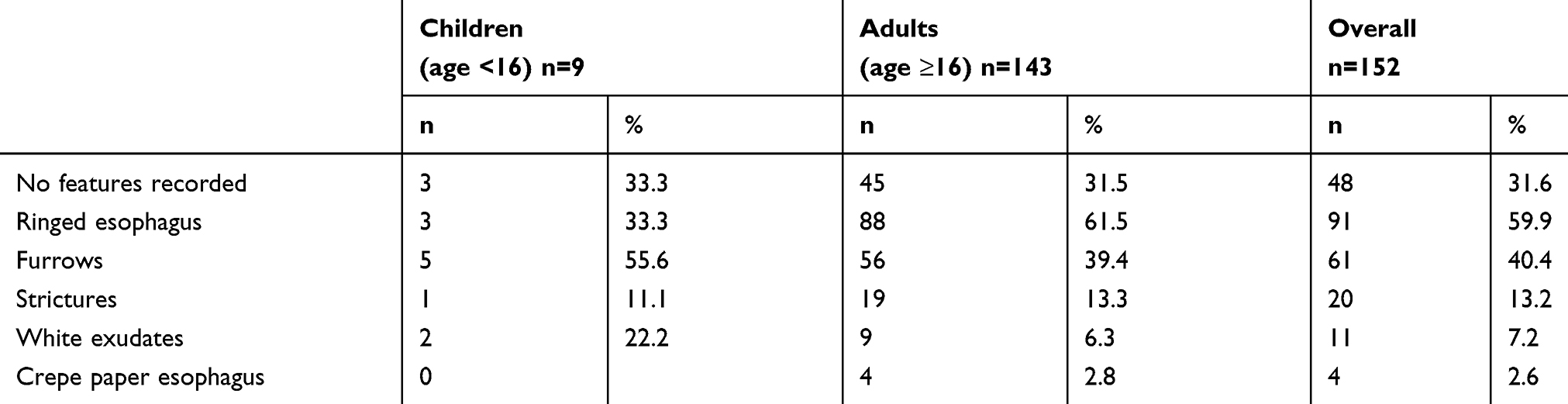 |
Table 3 Endoscopic features recorded in endoscopy report (>1 endoscopic feature could be present on endoscopy) |
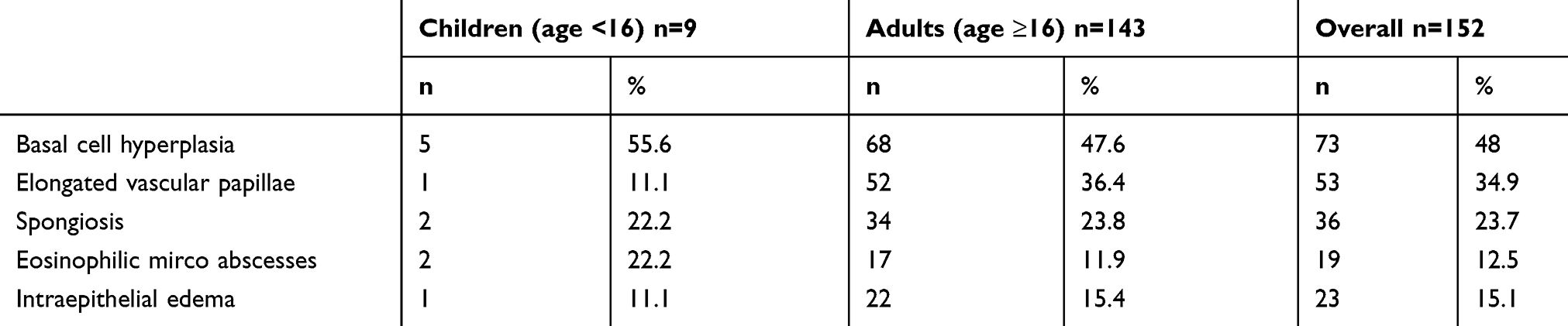 |
Table 4 Histologic features recorded in the biopsy report (>1 histological feature could be present on the biopsy report) |
The median number of locations biopsied during an endoscopy (be it upper, middle or lower esophagus) was 2 (range 1–3). This was the same for children and adults. Biopsies were taken from only one location in 76 patients (50%), from two locations in 67 patients (44.1%) and from three locations in 9 patients (5.9%). The median number of biopsies taken from any one location was 3. The location of the biopsy in which a histological diagnosis was made from is highlighted in Table 5.
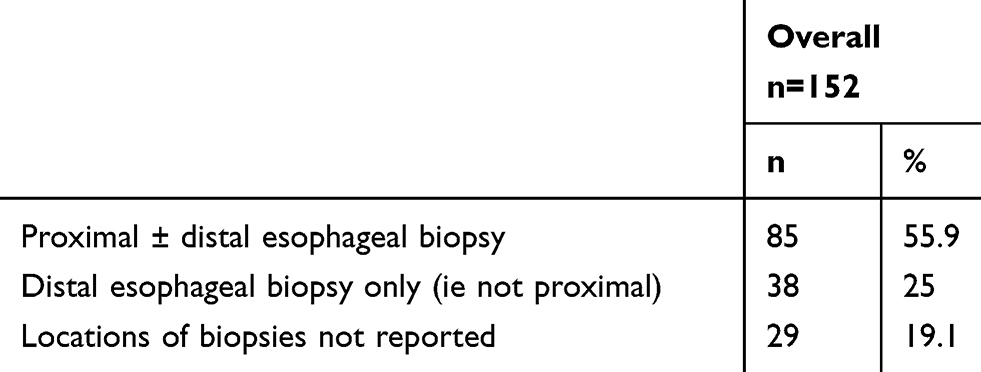 |
Table 5 Location of the biopsy in which a histological diagnosis was made |
The median peak eosinophil count totaled across all biopsies was 40 (ranged from 15 to 105). For the younger age group, the median was 40 (range 20–80). For those 16+, the median was 35 (range 15 to 105).
Incidence
The average annual incidence rate was 6.95 (95% CI 5.91, 8.12) per 100,000 persons. The incidence was highest in 2012 where there was a total of 38 cases of EoE with an incidence of 8.74 per 100,000 persons. Incidence rates for each year including incidence rates for both age groups are shown in Table 6. The average annual incidence for those <16 was 2.12 (95% CI 1.03, 3.89) per 100,000 persons compared to 8.11 (95% CI 6.86, 9.53) per 100,000 persons in those aged ≥16.
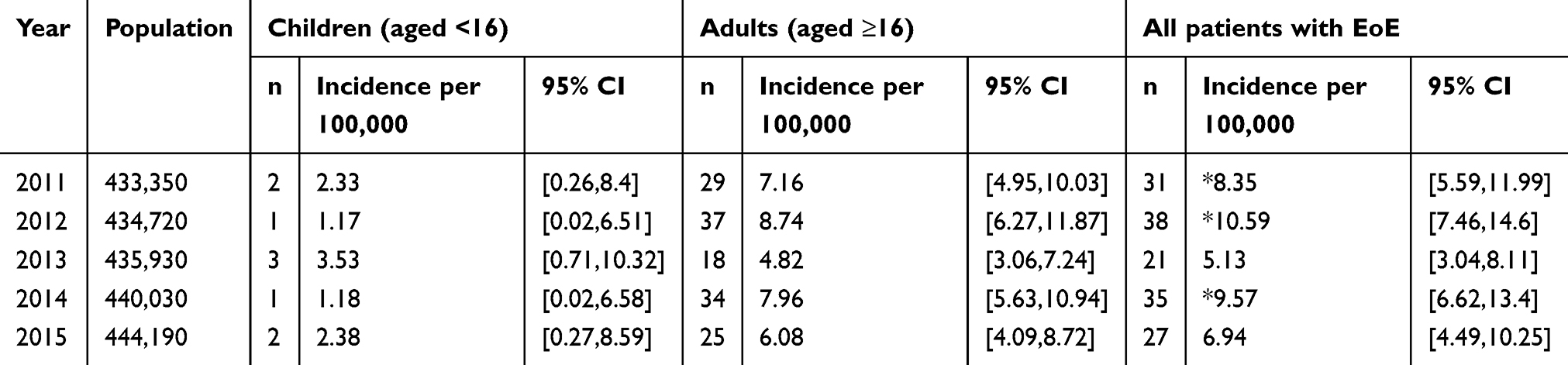 |
Table 6 The incidence rates (per 100,000 person years, 95% CI) by year and age group |
To investigate whether there was a significant difference in incidence rates by year and age group, we fit a Poisson regression model with year and age group (two groups, <16 and ≥16) as predictors of the number of cases. The model was statistically significant (likelihood ratio X2=29.169, 4 df, p=<0.0005). Year was not significant (X2=5.907, 4df, p=0.206), but age group was (X2=15.296, 2 df, p<0.0005).
On this basis of our calculations, we concluded that:
- There was no evidence of a significant difference in the overall incidence rates by year in this population. There was also no significant difference in the overall incidence rates by year in both age groups (<16: X2=1.454, 4df, p=0.835, ≥16: X2=7.854, 4df, p=0.097).
- There was a significantly lower incidence rate in those aged <16 compared to those aged ≥16 (RR (young/old) =0.26 (0.13,0.49); X2=15.269, 1df, p=0.002).
- There was a statistically significant difference in incidence rates by sex where males had a significantly higher incidence rate than females with an estimated rate ratio of 2.45 (95% CI (1.74, 3.49)).
Discussion
This study is the first to describe the incidence of EoE in a New Zealand population. We found a total of 152 cases of EoE in the Wellington region with an average annual incidence rate of 6.95 (95% CI 5.91, 8.12) cases per 100,000 persons over the last 5 years. A recent prospective observational study was conducted in Dunedin, New Zealand,23 but it only looked at the incidence and features of EoE in patients who presented with dysphagia. That study demonstrated that EoE was a common cause of dysphagia with an incidence of 14.1% in those having an esophageal biopsy. However, there are no New Zealand studies which look at the population incidence of EoE.
A recent meta-analysis of EoE incidence in North America and Europe by Arias et al reported a pooled incidence of 3.7 (95% CI 1.7, 6.5) per 100,000 persons/year.4 A higher pooled incidence rate of 5.4 per 100,000 persons/year was reported in North America compared to 1.7 per 100,000 persons/year in Europe.4 When compared with these pooled incidence rates, we report a higher incidence rate of EoE in New Zealand with an average annual incidence rate of 6.95 per 100,000 persons.
Whether the increase in incidence reported by recent studies6–12 is due to a true increase or because of increased awareness of EoE is not clear. A study performed in Denmark11 found a 19.5-fold rate increase in the incidence of EoE compared to a 1.9-fold rate increase in biopsies performed. The authors concluded that, given the rate of incidence was far greater than that of biopsy utilization, the increases in the incidence of EoE were not solely due to increased biopsy practices. Other studies have found that the increase in the use of biopsies was equal to the increase in the incidence rate of EoE and concluded that this may be due to increased awareness of the disease.5,6
In comparison to these studies, we found no evidence of a significant difference in incidence rates over a 5-year period in our population. Criteria for the diagnosis of EoE were originally released by the American Gastroenterological Association in 200724 and subsequently, the revised consensus guidelines were released in 2011.20 As a result, to focus on the more recent trends in EoE diagnosis, we only looked at cases that were diagnosed in the last 5 years. It is plausible that by the time these guidelines came into effect, there was enough awareness among gastroenterologists to identify most, if not all, of the cases of EoE. As such, it is possible that the rates of EoE are no longer increasing in our population and may have in fact reached a plateau. Van Rhijn et al7 predicted that a stable incidence rate may emerge over time, and as such our results provide some evidence to support that hypothesis.
Endoscopic features of EoE were reported in 68.4% of our cases. This is comparatively higher when compared to past studies, which showed that around half of the study population had a normal esophagus during upper endoscopy.5,15 The authors of these studies proposed that it may be worthwhile routinely collecting biopsy specimens from patients during an upper endoscopy, even when no outward features of EoE are present. It is possible the high rate of endoscopic features in our population reflects a lower relative rate of biopsy in patients without endoscopic features. This could potentially have resulted in underestimation of the incidence of EoE in our population.
In our study, we found that our pediatric group (aged <16 years) had a very low incidence rate compared to other studies.4 From a total of 152 cases, only 9 were pediatric cases. It is difficult to hypothesize why this may be. It was interesting to note, however, that the main presenting complaint in two-thirds of this group (aged <16) was abdominal pain or nausea and vomiting. A study by Prasad et al5 found that only 9% of the pediatric cases showed any features of EoE on endoscopy. In our study, the presence of endoscopic features of EoE on endoscopy was comparable between both groups. It may be that pediatric cases presenting for upper endoscopy are often not biopsied in New Zealand, and as such, it is possible that EoE is being underdiagnosed in this age group. It is also possible that this may be due to differences in practice between pediatricians. The results of this study are largely generalizable to the rest of the NZ population, but further research from other regions in NZ would be useful to explore this issue further.
There are some limitations to this study. A longer study period would allow us to more confidently describe trends in the incidence of EoE and may be warranted in future studies.
Further limitations are present given the retrospective design of our study. We were unable to exclude cases of proton pump inhibitor responsive EoE (PPI-REE). History of PPI use was unable to be reliably determined in all patients, so this information was not recorded. One of the criteria in the 2011 consensus guidelines was to exclude PPI-REE as they considered it a separate clinical entity to EoE.20 However, there is mounting evidence which supports the argument that PPI-REE is a continuum of EoE and not a separate clinical entity of its own.25 Past diagnostic guidelines reflected the assumption that PPIs only exert acid-suppressive effects, and as such only GORD or PPI-REE would respond to therapy.1 However, studies have shown that EoE patients may derive value from PPI due to their proposed anti-inflammatory properties.26 Goyal et al1 have postulated that PPIs should be considered as a management option for EoE instead of a diagnostic screen.
Similarly, due to the retrospective nature of our study, we were unable to definitively exclude GORD in our population. In the Wellington region, pH studies are not routinely carried out to confirm cases of GORD. We are confident most cases of GORD were excluded in our study by requiring a biopsy containing ≥15 eosinophils/hpf to diagnose EoE. A previous study found that <2% of GORD patients had an eosinophil count of ≥15 per hpf.27
The study was further limited as we could not standardize the collection and reporting of the data from the endoscopy and biopsy reports. This introduces the potential for information bias. Ideally, an EoE endoscopic reference score28 would have been used as some endoscopic features may not have been reported by the endoscopist. Ideally, more than one esophageal biopsy specimen would have been collected from multiple locations (ie, the upper, middle and lower esophagus) to assist the confident diagnosis of EoE. Unfortunately, this could not be standardized due to the retrospective nature of our study. The biopsy reports were accessed retrospectively in most patients so this meant that the reporting of biopsy specimens could not be standardized; hence, some features may have easily been overlooked or not reported. A strength of our study was that we rigorously cross-checked both endoscopy and biopsy databases to ensure that we did not miss any patients diagnosed with EoE in the Wellington region.
In conclusion, we found 152 cases of EoE in the Wellington region with an average annual incidence of 6.95 per 100,000 persons. We found no evidence of a significant difference in incidence rates by year in our study population. This is in contrast to previous reports of increasing incidence rates and may reflect a leveling off of incidence. Although historically EoE has been considered a disease of young male adults, we found that our pediatric patient group had a very low incidence rate. Further research prospectively examining the incidence of EoE in this group would be useful in determining whether this is due to ascertainment bias or is a real difference in the epidemiology of EoE in NZ compared to other countries.
Abbreviations
EoE, eosinophilic esophagitis; hpf, high-power field; CCDHB, Capital and Coast District Health Board; HVDHB, Hutt Valley District Health Board; SNOMED, systematically organized computer processable collection of medical terms providing codes, terms, synonyms and definitions used in clinical documentation and reporting; NHI, National Health Index; PPI-REE, proton pump inhibitor responsive EoE; GORD, gastro-esophageal reflux disease; PPI, proton pump inhibitors.
Acknowledgments
Many thanks to the Department of Medicine, University of Otago, Wellington, for sponsoring this study. We would also like to extend our thanks to our pathologists Dr Diane Kenwright & Dr Rupa Maitra, CCDHB, HVDHB and Acurity Health Group Ltd for their support. This study was funded in part by the Department of Medicine at the University of Otago Wellington.
Disclosure
The authors have no competing interests to declare in this work.
References
1. Goyal A, Cheng E. Recent discoveries and emerging therapeutics in eosinophilic esophagitis. World J Gastrointest Pharmacol Ther. 2016;7:21. doi:10.4292/wjgpt.v7.i1.21
2. Dellon ES, Kim HP, Sperry SLW, Rybnicek DA, Woosley JT, Shaheen NJ. A phenotypic analysis shows that eosinophilic esophagitis is a progressive fibrostenotic disease. Gastrointest Endosc. 2014;79:577–585.e4. doi:10.1016/j.gie.2013.10.027
3. Schoepfer AM, Safroneeva E, Bussmann C, et al. Delay in diagnosis of eosinophilic esophagitis increases risk for stricture formation in a time-dependent manner. Gastroenterology. 2013;145:1230–1236.e2. doi:10.1053/j.gastro.2013.08.015
4. Arias A, Pérez-Martínez I, Tenías JM, Lucendo AJ. Systematic review with meta-analysis: the incidence and prevalence of eosinophilic oesophagitis in children and adults in population-based studies. Aliment Pharmacol Ther. 2016;43:3–15. doi:10.1111/apt.13441
5. Prasad GA, Alexander JA, Schleck CD, et al. Epidemiology of Eosinophilic Esophagitis Over Three Decades in Olmsted County, Minnesota. Clin Gastroenterol Hepatol. 2009;7:1055–1061. doi:10.1016/j.cgh.2009.06.023
6. Syed AAN, Andrews CN, Shaffer E, Urbanski SJ, Beck P, Storr M. The rising incidence of eosinophilic oesophagitis is associated with increasing biopsy rates: a population-based study. Aliment Pharmacol Ther. 2012;36:950–958. doi:10.1111/apt.12053
7. Van Rhijn BD, Verheij J, Smout AJPM, Bredenoord AJ. Rapidly increasing incidence of eosinophilic esophagitis in a large cohort. Neurogastroenterol Motil. 2013;25:47–e5. doi:10.1111/nmo.12009
8. Giriens B, Yan P, Safroneeva E, et al. Escalating incidence of eosinophilic esophagitis in Canton of Vaud, Switzerland, 1993–2013: a population-based study. Allergy Eur J Allergy Clin Immunol. 2015;70:1633–1639. doi:10.1111/all.12733
9. Liacouras CA, Spergel JM, Ruchelli E, et al. Eosinophilic esophagitis: a 10-year experience in 381 children. Clin Gastroenterol Hepatol. 2005;3:1198–1206. doi:10.1016/S1542-3565(05)00885-2
10. Maradey-Romero C, Prakash R, Lewis S, Perzynski A, Fass R. The 2011–2014 prevalence of eosinophilic oesophagitis in the elderly amongst 10 million patients in the United States. Aliment Pharmacol Ther. 2015;41:1016–1022. doi:10.1111/apt.13171
11. Dellon ES, Erichsen R, Baron JA, et al. The increasing incidence and prevalence of eosinophilic oesophagitis outpaces changes in endoscopic and biopsy practice: national population-based estimates from Denmark. Aliment Pharmacol Ther. 2015;41:662–670. doi:10.1111/apt.13129
12. Warners MJ, de Rooij W, van Rhijn BD, et al. Incidence of eosinophilic esophagitis in the Netherlands continues to rise: 20-year results from a nationwide pathology database. Neurogastroenterol Motil. 2018;30:e13165. doi:10.1111/nmo.13165
13. Spergel JM. An allergist’s perspective to the evaluation of Eosinophilic Esophagitis. Best Pract Res Clin Gastroenterol. 2015;29:771–781. doi:10.1016/j.bpg.2015.06.011
14. González-Cervera J, Arias Á, Redondo-González O, Cano-Mollinedo MM, Terreehorst I, Lucendo AJ. Association between atopic manifestations and eosinophilic esophagitis: a systematic review and meta-analysis. Ann Allergy Asthma Immunol. 2017;118:582–590.e2. doi:10.1016/j.anai.2017.02.006
15. Altun R, Akbas E, Yildirim AE, Öcal S, Korkmaz M, Selcuk H. Frequency of eosinophilic esophagitis in patients with esophageal symptoms: a single-center Turkish experience. Dis Esophagus. 2013;26:776–781. doi:10.1111/j.1442-2050.2012.01395.x
16. Krupp NL, Sehra S, Slaven JE, Kaplan MH, Gupta S, Tepper RS. Increased prevalence of airway reactivity in children with eosinophilic esophagitis. Pediatr Pulmonol. 2016;51:478–483. doi:10.1002/ppul.23327
17. Asher MI, Montefort S, Björkstén B, et al. Worldwide time trends in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC Phases One and Three repeat multicountry cross-sectional surveys. Lancet. 2006;368:733–743. doi:10.1016/S0140-6736(06)69283-0
18. Pearce N, Aït-Khaled N, Beasley R, et al. Worldwide trends in the prevalence of asthma symptoms: Phase III of the International Study of Asthma and Allergies in Childhood (ISAAC). Thorax. 2007;62:758–766. doi:10.1136/thx.2006.070169
19. Inns SJ, Wyeth JW, Lamont D, Stace NH. Eosinophilic oesophagitis: an emerging important cause for undiagnosed dysphagia. N Z Med J. 2006;119(1230):77–83.
20. Liacouras CA, Furuta GT, Hirano I, et al. Eosinophilic esophagitis: updated consensus recommendations for children and adults. J Allergy Clin Immunol. 2011;128:3–20.e6. doi:10.1016/j.jaci.2011.02.040
21. Statistics New Zealand. Census Population and Dwelling Tables - Regional. Wellington, New Zealand; Statistics New Zealand; 2013.
22. Health Funds Association of New Zealand. Annu Rev. Health Funds Association of New Zealand Inc; 2017. Available from: https://docs.wixstatic.com/ugd/606d2f_f5c089160a0d46bea1a8d98d4b3efabb.pdf.
23. Alexander Murray I, Joyce S, Palmer J, Lau M, Schultz M. Incidence and features of eosinophilic esophagitis in dysphagia: a prospective observational study. Scand J Gastroenterol. 2016;51:257–262. doi:10.3109/00365521.2015.1093166
24. Furuta GT, Liacouras CA, Collins MH, et al. Eosinophilic esophagitis in children and adults: a systematic review and consensus recommendations for diagnosis and treatment. Gastroenterology. 2007;133:1342–1363. doi:10.1053/j.gastro.2007.08.017
25. Molina-Infante J, Bredenoord AJ, Cheng E, et al. Proton pump inhibitor-responsive oesophageal eosinophilia: an entity challenging current diagnostic criteria for eosinophilic oesophagitis. Gut. 2016;65:524–531. doi:10.1136/gutjnl-2015-310991
26. Cheng E, Souza RF, Spechler SJ. Eosinophilic esophagitis: interactions with gastroesophageal reflux disease. Gastroenterol Clin North Am. 2014;43:243–256. doi:10.1016/j.gtc.2014.02.004
27. Fiocca R, Mastracci L, Engström C, et al. Long-term outcome of microscopic esophagitis in chronic gerd patients treated with esomeprazole or laparoscopic antireflux surgery in the lotus trial. Am J Gastroenterol. 2010;105:1015–1023. doi:10.1038/ajg.2009.631
28. Hirano I, Moy N, Heckman MG, Thomas CS, Gonsalves N, Achem SR. Endoscopic assessment of the oesophageal features of eosinophilic oesophagitis: validation of a novel classification and grading system. Gut. 2013;62:489–495. doi:10.1136/gutjnl-2011-301817
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.