")
Back to Journals » Infection and Drug Resistance » Volume 15
Environmental Monitoring of Parvovirus B19 in the Kidney Transplantation Ward of a Chinese Teaching Hospital
Authors Wang F, Zhan Q, Yu SP, Feng HT, Hu P, Zhong ZF, Qu TT
Received 2 February 2022
Accepted for publication 26 March 2022
Published 18 April 2022 Volume 2022:15 Pages 1903—1910
DOI https://doi.org/10.2147/IDR.S356174
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Fang Wang,1,* Qing Zhan,1,* Shi-Ping Yu,2 Hai-Ting Feng,1 Ping Hu,2 Zi-Feng Zhong,1 Ting-Ting Qu1,3
1Infection Control Department, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, 310003, People’s Republic of China; 2Kidney Disease Center, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, 310003, People’s Republic of China; 3State Key Laboratory for Diagnosis and Treatment of Infectious Diseases, National Clinical Research Center for Infectious Diseases, Collaborative Innovation Center for Diagnosis and Treatment of Infectious Diseases, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, 310003, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ting-Ting Qu; Zi-Feng Zhong, Email [email protected]; [email protected]
Purpose: Parvovirus B19 (B19V) infection is a viral threat after kidney transplantation. It is mainly transmitted by close-contact inhalation of aerosolized viral particles. The risk of nosocomial spread of B19V in the transplantation ward is quite high. This study aimed to evaluate the quality of routine disinfection and the effectiveness of isolation measures in the wards of B19V-infected kidney transplant recipients.
Patients and Methods: Throat swab samples of 19 kidney transplant recipients admitted to the isolation ward and three healthcare workers (HCWs) were collected for viral DNA detection. Routine disinfection procedures were performed twice a day in general and B19V isolation wards. Environmental surface and air samples were collected for viral DNA detection before and after disinfection.
Results: A total of four patients were diagnosed with B19V infection and transferred to the B19V isolation ward, of which only two had positive throat swab samples. The other 15 patients and all HCWs tested negative for B19V. A total of 88 environmental surface and air samples were collected. Eight of the environmental samples collected in the B19V isolation ward before disinfection tested positive for B19V, while one sample tested positive after disinfection. In the general wards, all environmental samples collected before disinfection tested negative for B19V. All 24 samples collected from ambient air, whether in B19V isolation or general wards, before or after disinfection, tested negative for B19V.
Conclusion: Existing methods of routine or terminal disinfection for air and object surfaces were effective in eliminating B19V from object surfaces and ambient air in the isolation and general wards. Material surfaces that are exposed to high frequency and easily contaminated by blood, body fluids, and indoor air were the focus of cleaning and disinfection. Nosocomial cross-infection of other immunocompromised patients and HCWs can be avoided if appropriate prevention and control measures are taken.
Keywords: parvovirus B19, B19V, kidney transplantation ward, isolation, disinfection
Introduction
Parvovirus B19 (B19V), a member of the large Parvoviridae family and Erythroparvovirus genus, is a small, non-enveloped, single-stranded DNA (ssDNA) virus that infects only humans.1 It is a common community-acquired respiratory pathogen without ethnic, socioeconomic, gender, age, or geographic boundaries.2 Infectivity is temperature-dependent, with the infection being most frequent in the winter and spring.3 B19V is mainly transmitted in close contact by the inhalation of viral particles in aerosol (ie, respiratory spread transmission).4 Transmission may also occur through blood-donor transfusion and transplantation, mostly during the viremia that precedes the seroconversion period, as well as vertically, from mother to fetus.5 B19V is typically acquired during childhood, and at lower rates throughout adulthood, such that between 70% and 85% of adults show serologic evidence of past infection. Infection with B19V causes several clinical syndromes (fifth disease, transient aplastic crisis, pure red cell aplasia, hydrops fetalis, glomerulopathy, and anemia in end-stage kidney disease) and may contribute to other illnesses.6 Transient aplastic crisis because of B19V infection is of particular concern in patients with either decreased red blood cell production or increased turnover.4
Owing to their immunosuppressed status, kidney transplant recipients are particularly prone to acquire B19V infection, and it is a new viral threat in post-kidney transplantation.7 One of the most serious common diseases in immunosuppressed allograft recipients is B19V-associated pure red cell aplasia (PVB19-PRCA).8 Specific antiviral drugs or therapy are not available to treat B19V infection, and there is no effective vaccine for prevention. The treatment approach for infection depends on host factors such as immune status, underlying conditions, and manifestations of infection. Intravenous immunoglobulins (IVIG) and a reduction of immunosuppression make up the cornerstone of therapeutic management of B19V infection post-kidney transplantation.9,10 Patients with transient aplastic crisis may need supportive therapy with blood transfusions until the neutralizing antibody response can clear the virus and hematopoiesis is restored.11 B19V infection can persist and relapse frequently in individuals with compromised immune systems, which may affect patient prognosis and increase treatment costs.4
Due to the relative ease of spread of the virus among both hospital staff and patients, the risk of nosocomial spread of the disease, acquired from close contact or environmental surfaces, is quite high, with reported attack rates of 50%.12,13 Control measures such as prompt disinfection, hand hygiene, ward closure, and B19V education are likely crucial for containing transmission.14 To avoid the contagion, standard and droplet precautions and isolation should be implemented. Although many cases of B19V infection in kidney transplant recipients have been reported, in the last few decades there have been few relevant evaluations concerning environmental monitoring for B19V during their hospitalization.15–17 In order to identify potential risk factors for B19V infection, and ensure effective isolation of infected patients and a safe living environment for other patients with compromised immune systems after transplantation, we performed a thorough environmental surveillance, including air and surface sampling; meanwhile, we continued to sample the respiratory tract of medical staff and patients to evaluate the quality of routine disinfection and effectiveness of isolation measures in the wards of B19V-infected kidney transplant recipients.
Materials and Methods
Study Design
This study was conducted in the protective isolation ward for kidney transplantation. After kidney transplantation, patients were admitted to this ward and would transfer to the general ward or discharged directly after their condition stabilized in 1–2 weeks. There were three beds in each ward and one public restroom. The patients were appropriately restricted to activities inside the ward. Patients diagnosed with B19V infection were immediately isolated in the same room, with a bed spacing of ≥1.1 m. The floor plan of the ward is shown in Figure 1. A special buffer zone was set up in this ward, where the staff would change to special shoes, work clothes, surgical caps, surgical masks, and an isolation gown before entering the ward. The staff strictly performed hand hygiene before and after contact, treatment, or care of patients; in addition, gloves were worn when necessary.
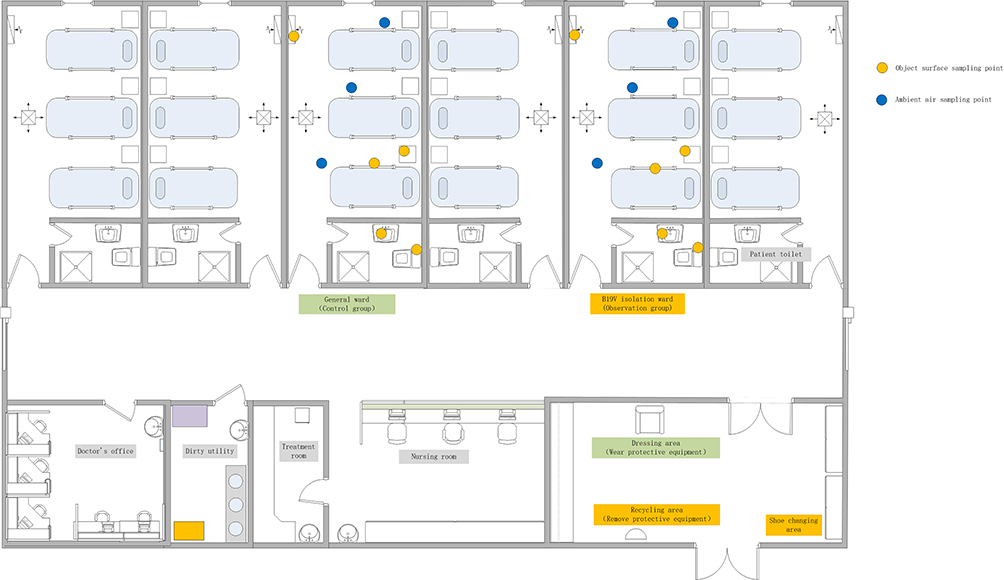 |
Figure 1 The floor plan of the kidney transplantation ward. |
The B19V epidemic season was selected as the research time, and the B19V isolation ward where the infected patients were located, and the adjacent ward managed by the same medical care group were selected as the research objects. From June 1, 2020 to June 29, 2020, a total of 19 patients were admitted to our study area, of which 15 were free from B19V infection and were transferred to general wards. Four patients tested positive for B19V about one week after transplantation, confirmed at two different times, and were moved to the B19V isolation ward. The time in the hospital of the four confirmed B19V-positive patients was slightly longer than that of the 15 B19V-negative patients in the general ward. It was confirmed that every two patients were received the same donor and were non-living transplant recipients. All donors were tested for B19V DNA, and one donor was positive. Daily diagnosis and treatment and the normal entry and exit of patients were not affected during the study period.
Disinfection
The entire ward was cleaned and disinfected twice a day by using disposable dry towels or clean floor towels soaked with 500 mg/L of chlorine-containing disinfectant to wipe or mop the surface of objects and the floor and waiting for 30 min. Routine cleaning and disinfecting of B19V isolation wards were done after all other wards. The medical equipment utilized was wiped after each use with Gama Clinell universal wipes containing 0.765–0.935% active ingredient. Any place suspected of being polluted or with visible pollution, including bed railings, bedside tables, furniture, door handles, floors or other articles, were completely cleaned and disinfected at any time. Continuously running plasma air disinfection machines were used for air disinfection in B19V isolation wards. The return air filter of the air purification device was cleaned weekly and at the end of the terminal disinfection.
After a patient was discharged or transferred, terminal disinfection of the bed unit was performed in the general ward and the B19V isolation ward. The concentration of chlorine disinfectant was increased to 2000 mg/L for the terminal disinfection in the isolation ward; after 30 min of disinfection the ward was wiped with clean water and a mobile ultraviolet lamp was used for air disinfection for more than 1 hour before ventilation.
Collection of Environmental and Air Samples for Detection
A virus sampling tube and accompanying swab (yocon®, Beijing, China) were used to collect throat swab samples from patients with confirmed B19V, patients in the general wards of the same medical care group, and the medical staff. The sampling sites are marked in Figure 1; the blue dots represent environmental surface sampling sites and the yellow dots represent air sampling sites. Surfaces deemed to be high-contact sites were sampled using swabs wetted with universal transport medium (UTM). Environmental surface sampling was performed on the high-frequency contact surfaces, including bed rails, bedside tables, toilet washbasins, and the flush button of the toilet bowl in the patient’s hospital room, and the return air outlet surface of the air purification device. The surface and throat swab samples were placed in UTM containing Hanks’ balanced salt solution, amino acids, glycerin, and other ingredients as described by Moore et al, pending inspection.18 Three air sampling sites were selected and marked with yellow dots as seen in Figure 1. A nutrient agar medium with a diameter of 9 cm was used to collect air samples by the sedimentation method.19 This agar medium containing the air samples was transferred to a 15 mL centrifuge tube, 4 mL of double-distilled water (ddH20) was added, and the agar was dissolved in a 37°C water bath for 10 min, pending inspection.
DNA Extraction and Real-Time Quantitative Reverse Transcription-PCR
Genomic DNA (gDNA) was extracted from the samples by heat treatment according to the manufacturer’s instructions. Commercial human parvovirus B19 real-time polymerase chain reaction (PCR) kit (LiferiverTM, Shanghai ZJ Bio-Tech Co., Ltd.) was used for the detection and quantification of B19V DNA in the samples. The lowest detection limit for this test was 1×103 copies/mL and the linear range of detection ranged from 2×103 to 1×108 copies/mL. A sample with a viral load corresponding to ≥1 × 103 copies/mL was considered to be positive.
Results
Throughout the study period four patients with confirmed B19V were hospitalized and lived in the B19V isolation ward at two different times. It was confirmed that every two patients were received the same donor and were non-living transplant recipients. One donor was positive for B19V DNA at screening. The remaining 15 patients lived in general wards with shorter hospital stays. Twenty-two respiratory samples of patients and medical staff were collected. Among the four patients with confirmed B19V, two respiratory throat swab samples tested positive for B19V but the detection value of the remaining two did not reach the positive threshold. All throat swab samples from three medical staff involved in the study and the 15 patients in the general wards tested negative for B19V (Table 1).
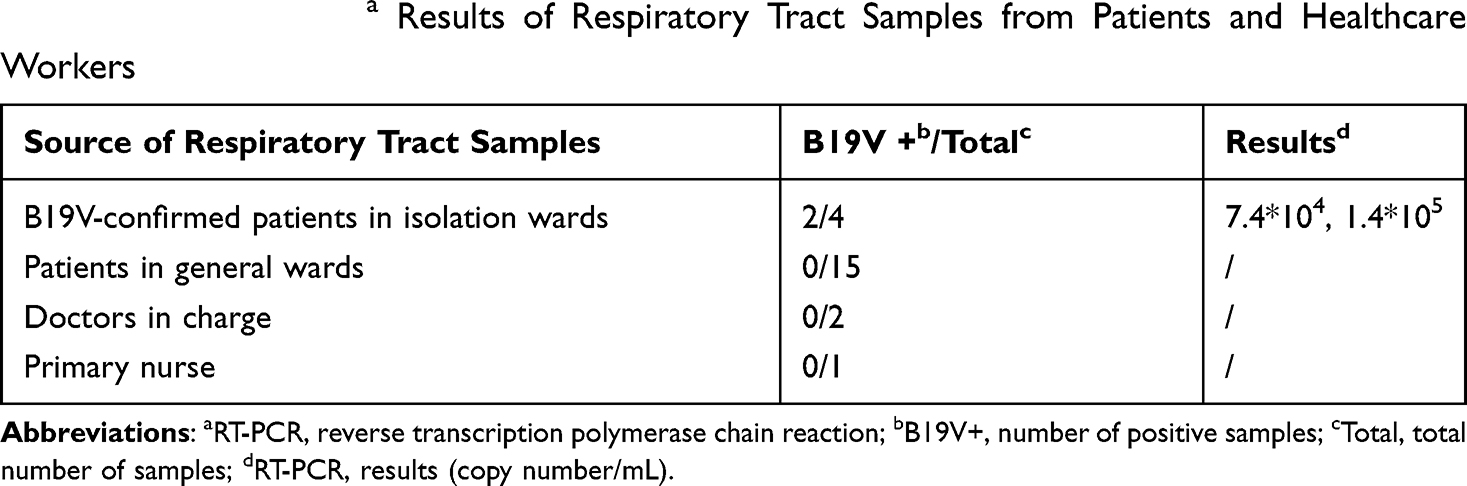 |
Table 1 B19V RT-PCRa Results of Respiratory Tract Samples from Patients and Healthcare Workers |
The sampling sites with high-frequency contact were sampled before and after disinfection and are marked in Figure 1. A total of 88 environmental surface and air samples were collected, including 44 from the B19V isolation ward and 44 from the non-isolation ward. Among all the samples, 22 samples came from the wards before disinfection, including 16 from environmental material surfaces and 6 from the air. After disinfection, samples were collected at three different time periods (3 h, 5 h, and 14 h after disinfection), for a total of 48 environmental surface samples and 18 air samples (Table 2).
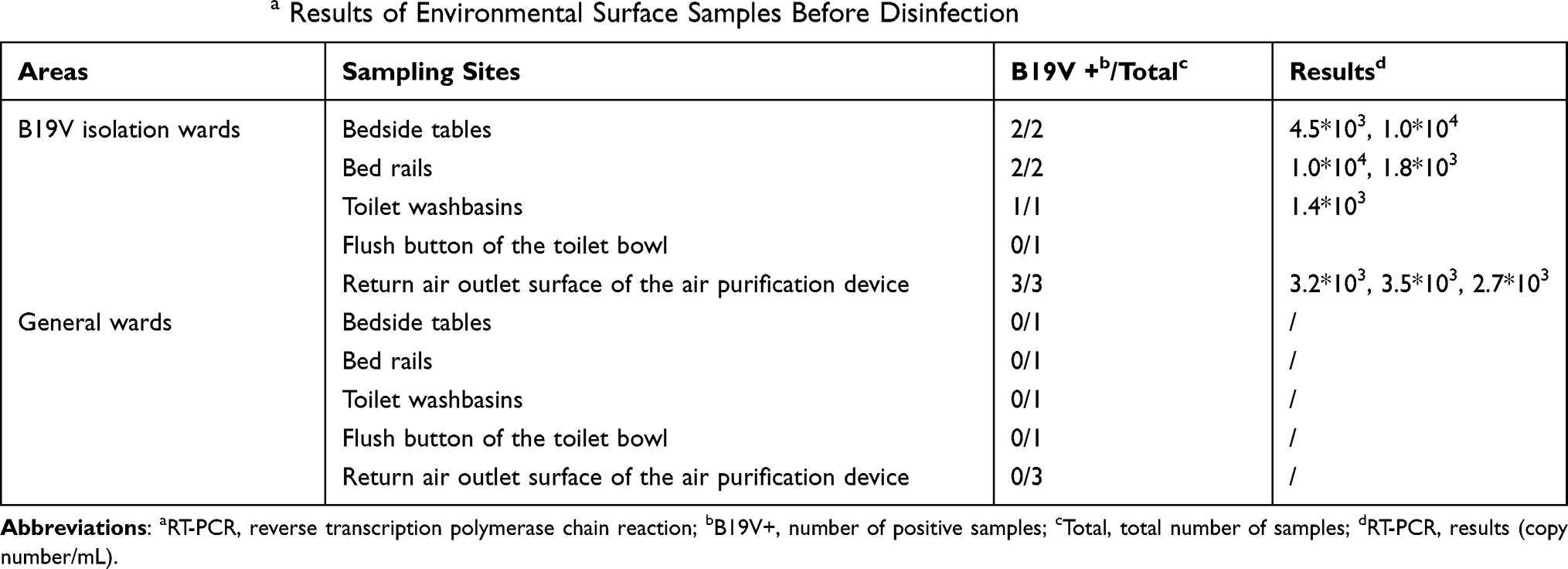 |
Table 2 B19V RT-PCRa Results of Environmental Surface Samples Before Disinfection |
Seven of the environmental material surface samples tested negative for B19V before disinfection in the general ward. Eight of the environmental samples tested positive for B19V before disinfection in the B19V isolation ward, and originated from the bed bar, bedside table, toilet washbasin, and the return air outlet of the air purification and disinfection device; meanwhile, one sample from the flush button of the toilet bowl tested negative (Table 2). After disinfection, one sample from an environmental material surface tested positive for B19V in the isolation ward, originating from the washbasin of the patient’s bathroom 3 h after disinfection, while the remaining 47 samples tested negative (Table 3). We confirmed that a B19V confirmed patient spit out mouthwash into the disinfected washbasin and failed to rinse it in time. The difference in the number of B19V positive surface samples detected before and after disinfection in B19V isolation wards was statistically significant (p<0.01). Air sampling sites are marked with yellow dots in Figure 1 and three locations were selected. A total of 24 samples were collected, including 12 in the general ward and 12 in the B19V isolation ward. Each ward included 3 samples before disinfection and 9 after disinfection. All 24 samples collected from ambient air, tested negative for B19V (Table 4).
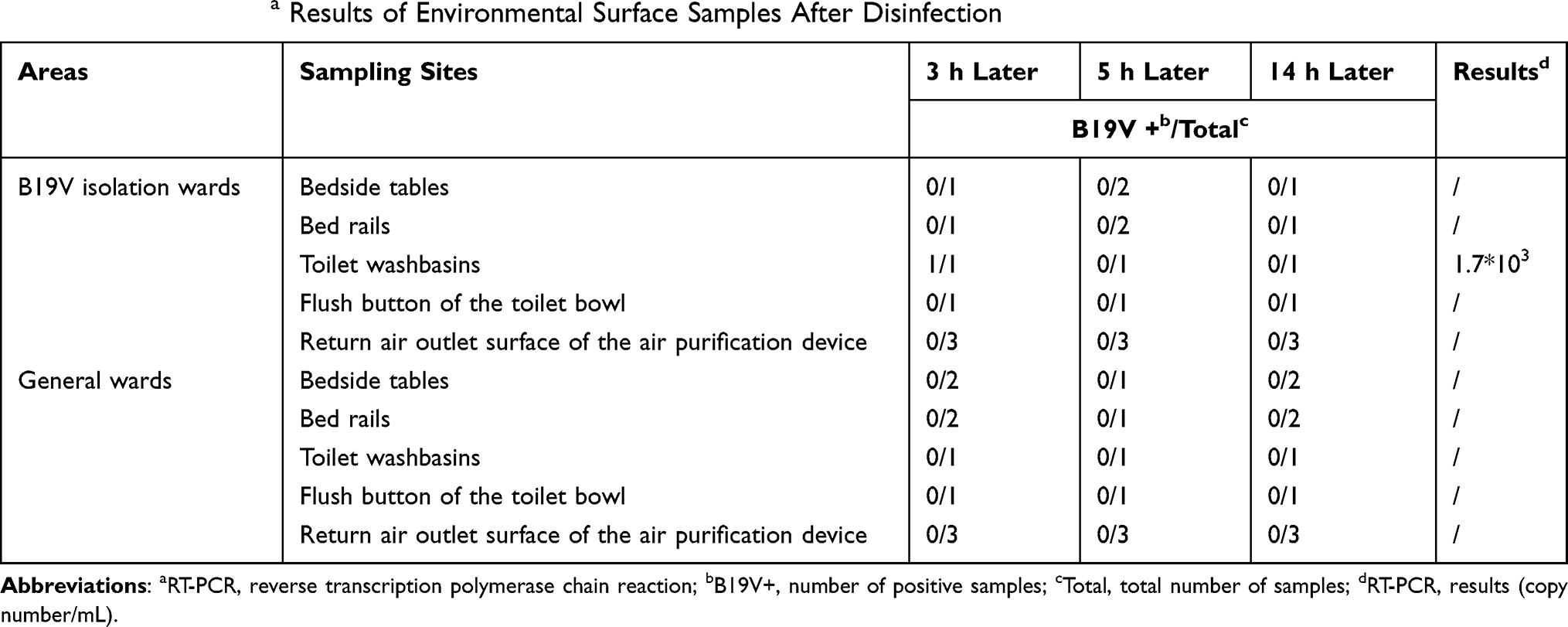 |
Table 3 B19V RT-PCRa Results of Environmental Surface Samples After Disinfection |
 |
Table 4 B19V RT-PCRa Results of Ambient Air Samples Before and After Disinfection |
Discussion
B19V infection is common worldwide, showing regional epidemiological differences with generally over one-half of the adult population having been exposed.4 The first case of B19V infection in a kidney transplant recipient (KTR) was reported in 1986.15 Among solid-organ transplant recipients, most seronegative KTRs of B19V-positive organs became infected within 1 month, and could develop persistent refractory anemia with reticulocytopenia, which posed a potentially serious threat to the allograft and recipient survival.20 This is similar to our research, in which most kidney transplant patients became infected with B19V within 1 week. In cases where the donor had low-level B19 DNAemia, the recipients were less likely to have obvious clinical manifestations, and the B19V could be quickly cleared even if the recipient was infected; however, high levels of B19 DNAemia may lead to graft failure.21,22 Previous studies at our hospital also showed that higher B19V viral loads in recipients within 7 days after transplantation were positively correlated with donor-derived B19V infection in deceased-donor kidney transplantation.23
Nonenveloped viruses of the Parvoviruses family can resist harsh environmental conditions, surviving on surfaces for long periods with the possibility of being transmitted to susceptible hosts. Parvoviruses are also tolerant to several mild disinfectants but sensitive to halogens, such as chlorine-releasing agents, which are often used for decontamination of ward floors and facility surfaces due to their broad spectrum of activity.24,25 According to some studies, parvoviruses can cause nosocomial cross-infection directly through contact with respiratory droplets or contaminated surfaces, and the parvovirus attack rates among patients or HCWs might not be as low as once thought.12,13,26 Therefore, strict implementation of isolation measures, personal protection, and environmental cleaning and disinfection is crucial.27
In our study, among the four isolated patients with B19V confirmed with blood samples by the laboratory, only two tested positive for B19V through throat swab samples; meanwhile, the detection value of the remaining two patients did not reach the positive threshold. Patients can cause B19V positivity in the surrounding environment through the respiratory tract and daily contact. There was B19V contamination on the high-frequency contact surfaces of the B19V isolation ward before disinfection, such as bed rails, bedside tables, toilets, sinks, and the return air outlet surface of the air purification device; even without visible contamination they were all positively detected. This result also confirms that isolation in a single room or isolation of the same disease is necessary, otherwise transmission of B19V and cross infection among other patients after transplantation and HCWs could occur through the contaminated environment. We believe that it is very important to increase patient health education to improve hand hygiene and reduce environmental pollution via the respiratory tract and daily contact. Additionally, high-frequency contact surfaces and surfaces that are easily contaminated by blood and body fluids should be the focus of daily surface cleaning and disinfection, while effective terminal disinfection can avoid persistent infections in newly admitted patients. This study shows that the positive detection of B19V DNA on environmental surfaces can be reduced by correct disinfection.
Considering the stimulating effect of chlorine-containing disinfectants on the respiratory tract, a concentration of 500 mg/L was used for routine disinfection at 6 am and 3 pm every day. The concentration of chlorine disinfectant was increased to 2000 mg/L during the terminal disinfection in the B19V isolation ward. In our results, all surface samples collected in the B19V isolation ward after disinfection were negative except for the washbasin, which tested positive for B19V. We confirmed that a B19V-positive patient vomited mouthwash into the disinfected washbasin and failed to rinse it in time. We communicated with patients and told them to wash the basin with running water immediately after each dumping of contaminated liquid, and there were no B19V positive samples detected after this improvement. Similarly, patients admitted to the ward after terminal disinfection did not develop B19V infection, indicating that the cleaning and disinfection methods used were effective. The frequency of cleaning and disinfection should be increased for the surface of objects easily contaminated by blood and body fluids. Before disinfection, B19V in the air did not reach the positive threshold mainly due to the single unit laminar air flow system in all isolation wards. However, the return air outlet surface of the air purification device was positive for B19V DNA detection before disinfection, which indicates that B19V could be attached to the environmental surfaces through air transmission. B19V is between 23 and 28 nm in size and thus a laminar flow system cannot completely purify the air, requiring plasma air disinfection machines running continuously.4,28
In addition, we implemented various disinfection and isolation measures for infected patients. Healthcare workers and cleaning staff wore full personal protective equipment (PPE) when entering and leaving the isolation ward, properly put on and took off PPE, and increased hand hygiene compliance per “My five moments for hand hygiene”.29 Although the staff responsible for the diagnosis, treatment, care, and sanitation of the isolation and general wards were the same group, their respiratory tract samples and all environmental and air samples from the general ward tested negative. These results indicate that nosocomial cross-infection can be avoided if appropriate prevention and control measures are taken.
There are several limitations to this study. First, the positive samples were not cultured to prove their viability and infectivity. Second, the source of B19V infection in patients after kidney transplantation was not very clear. Among the four isolated patients with confirmed B19V in this study, it was confirmed that every two patients were received the same donor and were non-living transplant recipients. One donor screened positive for B19V DNA detection. Therefore, screening for B19V is recommended for kidney transplant donors with a long history of hospitalization, especially in the intensive care unit, who may have low immunity, as well as implementation of early isolation observation and monitoring of such recipients. However, to the best of our knowledge, this is the first study to examine the environmental hygienic monitoring of parvovirus B19 in a kidney transplantation ward of a general hospital, although there have been many reports of hospital outbreaks of B19V.12,30,31 Our study provides an important evidence-based basis and reference value for providing targeted disinfection guidance and avoiding parvovirus cross-infection for immunosuppressed patients undergoing kidney transplantation.
In conclusion, existing methods of routine or terminal disinfection for air and object surfaces are effective. Material surfaces that are exposed to high frequency and easily contaminated by blood and body fluids and indoor air should be the focus of cleaning and disinfection. Ensuring adequate frequency of cleaning and disinfection every day and disinfection at any time is also very important to control pollution. Nosocomial cross-infection of other immunocompromised patients and staff can be avoided if appropriate prevention and control measures are taken.
Ethical Approval and Consent to Participate
Written informed consent was obtained from all the patients involved in this study. All kidneys were donated voluntarily with written informed consent during the upfront diagnosis and treatment process, which was carried out in accordance with the Istanbul Declaration. This study was approved by the local ethics committees of the First Affiliated Hospital, College of Medicine, Zhejiang University.
Acknowledgments
The authors would like to thank all medical staff in the kidney transplantation ward (Kidney Disease Center, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, China) for their excellent technical support and kindly suggestions.
Author Contributions
FW, SY, HF, PH collected samples and performed laboratory measurements. FW and QZ collated and analyzed the data. FW and QZ drafted the article. TQ and ZZ made substantial contributions to the study’s conception and design and made a critical revision to the article. All the authors read and approved the final version of the manuscript. All authors contributed to data analysis, drafting, or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This work was supported by A Project Supported by the Scientific Research Fund of the Zhejiang Provincial Education Department (Y202146838).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cotmore SF, Agbandje-McKenna M, Canuti M, et al. ICTV virus taxonomy profile: parvoviridae. J Gen Virol. 2019;100(3):367–368. doi:10.1099/jgv.0.001212
2. Cnc Garcia R, Leon LA. Human parvovirus B19: a review of clinical and epidemiological aspects in Brazil. Future Microbiol. 2021;16(1):37–50. doi:10.2217/fmb-2020-0123
3. Mage V, Lipsker D, Barbarot S, et al. Different patterns of skin manifestations associated with parvovirus B19 primary infection in adults. J Am Acad Dermatol. 2014;71(1):62–69. doi:10.1016/j.jaad.2014.02.044
4. Qiu J, Söderlund-Venermo M, Young NS. Human parvoviruses. Clin Microbiol Rev. 2017;30(1):43–113. doi:10.1128/CMR.00040-16
5. Gallinella G. The clinical use of parvovirus B19 assays: recent advances. Expert Rev Mol Diagn. 2018;18(9):821–832. doi:10.1080/14737159.2018.1503537
6. de Jong EP, Walther FJ, Kroes AC, Oepkes D. Parvovirus B19 infection in pregnancy: new insights and management. Prenat Diagn. 2011;31(5):419–425. doi:10.1002/pd.2714
7. Bentata Y. Parvovirus B19 in kidney transplantation: key points and essential pitfalls to know. Infect Dis. 2021;53(6):404–408. doi:10.1080/23744235.2021.1893379
8. Zolnourian ZR, Curran MD, Rima BK, Coyle PV, O’Neill HJ, Middleton D. Parvovirus B19 in kidney transplant patients. Transplantation. 2000;69(10):2198–2202. doi:10.1097/00007890-200005270-00043
9. Eid AJ, Chen SF; AST Infectious Diseases Community of Practice. Human parvovirus B19 in solid organ transplantation. Am J Transplant. 2013;13(Suppl 4):201–205. doi:10.1111/ajt.12111
10. Mouthon L, Guillevin L, Tellier Z. Intravenous immunoglobulins in autoimmune- or parvovirus B19-mediated pure red-cell aplasia. Autoimmun Rev. 2005;4(5):264–269. doi:10.1016/j.autrev.2004.10.004
11. Bonvicini F, Mirasoli M, Gallinella G, Zerbini M, Musiani M, Roda A. PNA-based probe for quantitative chemiluminescent in situ hybridisation imaging of cellular parvovirus B19 replication kinetics. Analyst. 2007;132(6):519–523. doi:10.1039/b701664f
12. Lara-Medrano R, Martínez-Reséndez MF, Garza-González E, Medina-Torres AG, Camacho-Ortiz A. Outbreak of parvovirus B19 infection among anesthesiology and surgical fellows. Am J Infect Control. 2016;44(9):1069–1070. doi:10.1016/j.ajic.2015.12.004
13. Miyamoto K, Ogami M, Takahashi Y, et al. Outbreak of human parvovirus B19 in hospital workers. J Hosp Infect. 2000;45(3):238–241. doi:10.1053/jhin.2000.0771
14. Siegel JD, Rhinehart E, Jackson M, et al.; for the Healthcare Infection Control Practices Advisory Committee. 2007 guideline for isolation precautions: preventing transmission of infectious agents in healthcare settings. Available from: https://www.cdc.gov/infectioncontrol/guidelines/isolation/index.html.
15. Neild G, Anderson M, Hawes S, Colvin BT. Parvovirus infection after renal transplant. Lancet. 1986;2(8517):1226–1227. doi:10.1016/S0140-6736(86)92245-2
16. Azzi A, Zakrzewska K, Bertoni E, Guidi S, Salvadori M. Persistent parvovirus B19 infections with different clinical outcomes in renal transplant recipients: diagnostic relevance of polymerase chain reaction (PCR) and of quantification of B19 DNA in sera. Clin Microbiol Infect. 1996;2(2):105–108. doi:10.1111/j.1469-0691.1996.tb00214.x
17. Egbuna O, Zand MS, Arbini A, Menegus M, Taylor J. A cluster of parvovirus B19 infections in renal transplant recipients: a prospective case series and review of the literature. Am J Transplant. 2006;6(1):225–231. doi:10.1111/j.1600-6143.2005.01139.x
18. Moore G, Rickard H, Stevenson D, et al. Detection of SARS-CoV-2 within the healthcare environment: a multi-centre study conducted during the first wave of the COVID-19 outbreak in England. J Hosp Infect. 2021;108:189–196. doi:10.1016/j.jhin.2020.11.024
19. Chamseddine A, Soudani N, Kanafani Z, et al. Detection of influenza virus in air samples of patient rooms. J Hosp Infect. 2021;108:33–42. doi:10.1016/j.jhin.2020.10.020
20. Yu Y, Bao R, Lyu J, Wu J, Chen J, Peng W. Foscarnet therapy for pure red cell aplasia related to human parvovirus B19 infection in kidney transplant recipients: a preliminary exploration. Infect Drug Resist. 2021;14:2911–2923. doi:10.2147/IDR.S321936
21. Koppelman MH, Cuypers HT, Emrich T, Zaaijer HL. Quantitative real-time detection of parvovirus B19 DNA in plasma. Transfusion. 2004;44(1):97–103. doi:10.1046/j.0041-1132.2004.00610.x
22. Eid AJ, Brown RA, Patel R, Razonable RR. Parvovirus B19 infection after transplantation: a review of 98 cases. Clin Infect Dis. 2006;43(1):40–48. doi:10.1086/504812
23. Yu Y, Wei C, Lyu J, et al. Donor-derived human parvovirus B19 infection in kidney transplantation. Front Cell Infect Microbiol. 2021;11:753970. doi:10.3389/fcimb.2021.753970
24. Cavalli A, Marinaro M, Desario C, Corrente M, Camero M, Buonavoglia C. In vitro virucidal activity of sodium hypochlorite against canine parvovirus type 2. Epidemiol Infect. 2018;146(15):2010–2013. doi:10.1017/S0950268818002431
25. Eterpi M, McDonnell G, Thomas V. Disinfection efficacy against parvoviruses compared with reference viruses. J Hosp Infect. 2009;73(1):64–70. doi:10.1016/j.jhin.2009.05.016
26. Sungkate S, Phongsamart W, Rungmaitree S, et al. Human parvovirus B19 nosocomial outbreak in healthcare personnel in a paediatric ward at a national tertiary referral centre in Thailand. J Hosp Infect. 2017;96(2):163–167. doi:10.1016/j.jhin.2017.03.014
27. Naides S. Infection control measures for human parvovirus B19 in the hospital setting. Infect Control Hosp Epidemiol. 1989;10(7):326–329. doi:10.2307/30146476
28. Centers for Disease Control and Prevention. Guidelines for environmental infection control in health-care facilities: recommendations of CDC and the Healthcare Infection Control Practices Advisory Committee (HICPAC). MMWR. 2003;52(RR–10):1–48.
29. World Health Organization. Guidelines on hand hygiene in health care. Available from: https://www.who.int/infection-prevention/publications/hand-hygiene-2009/en/.
30. Alves ADR, Langella BB, Barbosa JR, et al. High prevalence of parvovirus B19 infection in patients with chronic kidney disease under hemodialysis: a multicenter study. Int J Infect Dis. 2020;100:350–356. doi:10.1016/j.ijid.2020.09.010
31. Sharif A, Aghakhani A, Velayati AA, et al. Frequency and genotype of human parvovirus B19 among Iranian hemodialysis and peritoneal dialysis patients. Intervirology. 2016;59(3):179–185. doi:10.1159/000455124
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.