")
Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 11
Enthesitis-related arthritis: current perspectives
Authors Mistry RR, Patro P, Agarwal V , Misra DP
Received 9 September 2018
Accepted for publication 19 December 2018
Published 25 January 2019 Volume 2019:11 Pages 19—31
DOI https://doi.org/10.2147/OARRR.S163677
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Chuan-Ju Liu
Rutviz Rajendra Mistry,1 Pallavi Patro,2 Vikas Agarwal,1 Durga Prasanna Misra1
1Department of Clinical Immunology, Sanjay Gandhi Postgraduate Institute of Medical Sciences (SGPGIMS), Lucknow, India; 2Department of Pharmacology, Sriram Chandra Bhanja (SCB) Medical College, Cuttack, India
Abstract: In this narrative review, we overview the recent literature on enthesitis-related arthritis (ERA). For the purpose of our review, we searched Scopus for recent articles on this subject from 2013 onward, including some classic older articles for perspective. ERA is a juvenile idiopathic arthritis (JIA) subtype more common in males, associated in a majority with human leucocyte antigen B27. Such children generally present with asymmetric oligoarthritis or polyarthritis, predominantly of lower limb joints, associated with enthesitis or sacroiliitis. While diagnosis remains clinical, ultrasound is being increasingly used to detect subclinical enthesitis and for guiding entheseal site injections. Spine MRI can help detect sacroiliitis, inflammatory spinal changes, and pelvic sites of enthesitis in such patients. The recent juvenile spondyloarthropathy disease activity index recognizes the key clinical features of ERA, viz enthesitis and inflammatory back pain, which other disease activity indices used in JIA did not include. Management includes NSAIDs with physical therapy. Conventional disease-modifying agents like sulfasalazine and methotrexate may be used to minimize duration of NSAID use and in those with high inflammatory burden. In patients refractory to these drugs, biologics such as antitumor necrosis factor alpha agents have proven useful, based on evidences from randomized controlled trials and retrospective registry analyses. Factors predicting a poorer outcome in such children include hip or ankle involvement or restricted spinal mobility. Considering that children with ERA have overall poorer long-term outcomes than other subtypes of JIA, there is a need to further optimize therapeutic strategies for such patients.
Keywords: enthesitis-related arthritis, juvenile spondyloarthropathy, diagnosis, management, exercise, anti-TNF
Introduction
Juvenile idiopathic arthritis (JIA) is a form of inflammatory arthritis affecting children. Currently accepted classification criteria proposed by the International League Against Rheumatism (ILAR) in 2001, published in 2004, for JIA require age of onset by 16 years, with different categories based on the predominant clinical and laboratory manifestations.1 The various categories described were as follows. Systemic subtype was defined as arthritis of at least one joint, with daily fever of at least 2 weeks duration, with one of the following – transient, evanescent rash, lymphadenopathy, hepatomegaly or splenomegaly, or serositis (excluding those with psoriatic arthritis, enthesitis-related arthritis [ERA], features of spondyloarthropathy, or rheumatoid factor [RF)] positivity). Oligoarthritis subtype was defined as involvement of one to four joints in the first 6 months, persistent if similar number of joints remains involved or extended if five or more joints are involved later on, excluding those with systemic JIA, psoriatic arthritis, ERA, features of spondyloarthropathy, or RF positivity. Polyarticular JIA involves five or more joints in first 6 months, further qualified as RF negative or positive (if RF is demonstrable twice 3 months apart), excluding those with systemic JIA, psoriatic arthritis, ERA, or features of spondyloarthropathy. Psoriatic arthritis was defined as the presence of either arthritis with psoriasis or arthritis along with two of the following three features: dactylitis, nail changes, and family history of psoriasis in a first-degree relative, excluding those with systemic JIA, ERA, features of spondyloarthropathy, or RF positivity. ERA, which is the topic of interest of our review, is defined in the subsequent paragraph. Undifferentiated arthritis either does not fit into any of these above categories or could be classified under two or more of them.1
One such subtype of JIA is ERA, which may be considered as the pediatric counterpart of adult spondyloarthropathies2 (hence often referred to as juvenile spondyloarthropathy), albeit with certain significant differences. In a child with JIA, ERA requires the presence of arthritis along with enthesitis or the presence of either arthritis or enthesitis along with any of the two following features: uveitis, onset in a male child ≥6 years of age, presence of human leucocyte antigen B27 (HLA-B27), presence of either inflammatory low back ache or clinically elicitable tenderness on palpating the sacroiliac joints, or family history of an HLA-B27-associated disease such as spondyloarthropathy (adult or juvenile), reactive arthritis, inflammatory bowel disease (IBD) along with sacroiliac joint involvement, or acute anterior uveitis in a first-degree relative. In addition, the child should not have systemic-onset JIA or juvenile psoriatic arthritis and should be negative for IgM RF at least twice over 3 months to fulfill ERA classification criteria.1 In this narrative review, we shall discuss the pathogenesis, clinical features, diagnosis, and treatment of ERA, with a focus on the recent literature in this field.
Search strategy
We utilized a search strategy based on previously published guidelines.3 We searched the database Scopus (which automatically includes all the available information on MEDLINE) on 20 February 2018 to identify published literature on ERA, utilizing the search term “Enthesitis-related arthritis” to search titles, abstracts, and keywords, limiting our search for articles published from 2013 onward. We could identify 258 such articles, which we then further screened to identify articles relevant to our narrative review. In addition to this, further landmark articles in this area were identified by cross-searching the reference lists of the above articles or based on the authors’ personal knowledge. Inclusion of some older articles was essential to provide an appropriate context to the topic; however, we have taken care to include as recent literature as we could in most instances.
Pathogenesis
A large proportion of the understanding of the pathogenesis of ERA has been derived from adult spondyloarthropathies. Nearly three-fourth of patients with ERA have the presence of HLA-B27 antigen, encoded by the HLA-B27 gene.4 HLA-B27 is a class I HLA molecule involved in antigen processing and presentation. It has been proposed that HLA-B27 drives the pathogenesis of spondyloarthropathy or ERA by three mechanisms, presentation of an as-of-yet unidentified arthritogenic peptide that causes lymphocyte activation, dimerization on surface of antigen-presenting cells causing CD4 T lymphocyte activation, or induction of endoplasmic reticulum stress resulting in secretion of cytokines IL-23 and IL-17, further also causing activation of T-helper 17 (Th17) cells.5 Other HLA associations that are associated with increased risk of ERA include DRB1:01, DQA1:01:01, and DQB1:05, whereas the HLA alleles DRB1:07 and DRB1:02:01 confer protection against ERA.6 With respect to non-HLA associations, endoplasmic reticulum resident aminopeptidases (ERAP1 and ERAP2) are another molecule involved in antigen processing and presentation, and polymorphisms in ERAP1 and ERAP2 genes also predispose to spondyloarthritis.5,7 Polymorphisms in ERAP1 predispose to ERA, so also do polymorphisms in IL-12A, which encodes the receptor for IL-12, a key cytokine driving Th1 cell differentiation.6
Animal models enhance the understanding of disease pathogenesis. With regard to spondyloarthritis or ERA, the HLA-B27 transgenic rat model mimics the clinical features of peripheral joint arthritis, axial involvement with sacroiliitis, enthesitis, bowel wall inflammation, as well as skin lesions mimicking psoriasis and nail dystrophy. Another animal model of these diseases is mice with mutations in zeta-associated protein 70 (ZAP70), also called SKG mice. ZAP70 is a molecule that plays a role in signal transduction in T lymphocytes, and in SKG mice, thymic selection for autoreactive T lymphocytes in abnormal, resulting in peripheral arthritis. When such mice are administered beta-glucan, a normal component of fungal cell wall, intraperitoneally, they also develop features of sacroiliitis, enthesitis, dactylitis, and skin lesions akin to psoriasis, mimicking the phenotype of spondyloarthritis.8
Innate immune cells play a role in the disease processes in ERA. Macrophages have been demonstrated to infiltrate the synovial lining of affected joints of patients with spondyloarthritis.9 Macrophages produce inflammatory cytokines like tumor necrosis factor alpha (TNFα), and blocking this cytokine helps improve arthritis and enthesitis in these children.10 A proportion of patients with spondyloarthritis or ERA also have clinically evident or subclinical bowel wall inflammation, and this is believed to be driven by innate immune cells such as gamma delta T cells or innate lymphoid cells type 3, as well as by Th17 cells, involving cytokines such as IL-17 and IL-23. A skewing toward T helper 1 cells has been demonstrated in the synovial fluid of patients with JIA.11 Although the classical understanding of spondyloarthritis has not emphasized the role of B lymphocytes in spondyloarthritis, recent literature suggests that autoantibodies to CD74 [a receptor for macrophage migration inhibitory factor (MIF)] may be present in the sera of patients with spondyloarthritis,12 and another recent study showed that MIF interacts with monocytes to promote secretion of TNFα as well as stimulate osteoclast activation driving the synovitis of spondyloarthritis.13 The pathogenesis of enthesitis in spondyloarthritis or ERA is driven by different factors. Mechanical stress stimulates stromal cells at the entheseal sites and promotes enthesitis.14 Also, the direct action of IL-23 on the entheseal sites drives this process further.15 Recent literature has emphasized on the role of alterations in the gut microbiome in spondyloarthritis, and in children with ERA, the gut microbiome is relatively less diverse and demonstrates altered tryptophan metabolism.16,17 However, attempts at altering the gut microbiome by means of probiotics have not been shown to be beneficial to reduce disease activity in children with ERA.18
Clinical features
The different subtypes of JIA differ in their prevalence depending on ethnicity. Worldwide, as well as in series from Europe and North America, oligoarticular JIA is the commonest subtype described.19,20 However, in Asian populations, including series from India,21 China,22 and Taiwan,23 systemic-onset JIA and ERA are the commonest described subtypes. Recent series of patients with ERA have been summarized in Table 1,22–28 utilizing the ILAR classification criteria.1 Those children with an oligoarticular presentation before the age of 6 years are more likely to be female and lack features of enthesitis or inflammatory back pain, therefore, are classifiable as oligoarticular JIA. On the contrary, ERA is more common in males above the age of 6 years, and such children often have enthesitis, with or without sacroiliitis, and a greater propensity for hip joint involvement.1,20
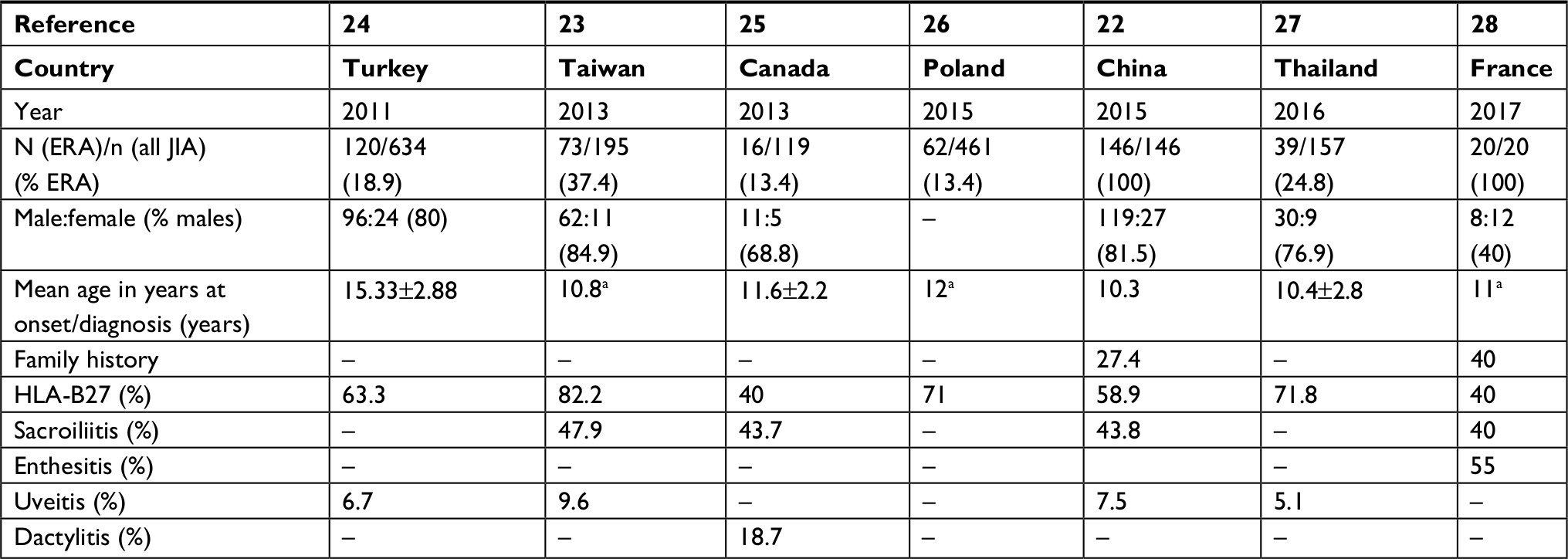 | Table 1 Recently published series of patients with ERA detailing their clinical characteristics Note: aMedian. Abbreviations: ERA, enthesitis-related arthritis; F, female; HLA-B27, human leukocyte antigen B27; JIA, juvenile idiopathic arthritis; M, male. |
Enthesitis
Enthesitis refers to the inflammation at or surrounding the site of attachment of ligaments or tendons to bone. Enthesitis is the characteristic clinical finding in ERA and may even be the presenting feature. Greater than half of patients with ERA may have enthesitis, and this feature is present only in ERA or juvenile psoriatic arthritis, but generally not in the other categories of JIA.28 The various entheseal sites that can be involved and are commonly assessed are the plantar fascia (either at the site of insertion to the calcaneus or the metatarsal heads), the Achilles tendon, the superior and inferior portions of the patella (generally at 2, 6, and 10 o’clock positions), the tibial tuberosity, the greater trochanter, the ischial tuberosity, the anterior and superior iliac spines, the iliac crest, costochondral junctions, spinous processes of the cervical, thoracic or lumbar spines, sites of insertion of the rotator cuff, or medial and lateral epicondyles of the elbow.29 The prevalence of entheseal sites was assessed in an inception cohort of 32 patients with ERA, wherein the inferior pole of the patella and the plantar fascia at the site of insertion to calcaneum were the most commonly involved sites, in about a half of such patients. Another finding of this study revealed that most commonly, the involvement of entheseal sites was symmetrical.30 While clinically evident enthesitis is more common in ERA or the spondyloarthropathy spectrum of diseases, subclinical enthesitis detected by advanced imaging techniques such as MRI may also be found in other forms of inflammatory arthritis such as rheumatoid arthritis.9 Different scoring systems for enthesitis, such as the Leeds enthesitis index and others, have been described in literature;29 however, their use is predominantly in clinical studies rather than in routine patient care in a busy outpatient clinic. It was interesting to note a recent paper which revealed that the number of entheseal sites involved in patients with ERA tended to go hand in hand with the number of joints involved as well.31
Arthritis
Classically, the pattern of joint involvement in ERA is an asymmetric oligoarthritis or polyarthritis affecting predominantly large joints, especially in the lower limbs. Axial involvement in the form of sacroiliac joint, hip or shoulder involvement, is characteristic.24 As a consequence, early in the course of the disease, such children may be erroneously classified as oligoarticular JIA; however, enthesitis and axial involvement help differentiate ERA from oligoarticular JIA.20 Whereas knee joints can be involved in about half of patients with ERA, hip joint is involved in about a third.22,23 Lack of early treatment may predispose these children to develop deformities of the affected joints.23 Table 222,23,25 summarizes the pattern of joint involvement in ERA from different studies.
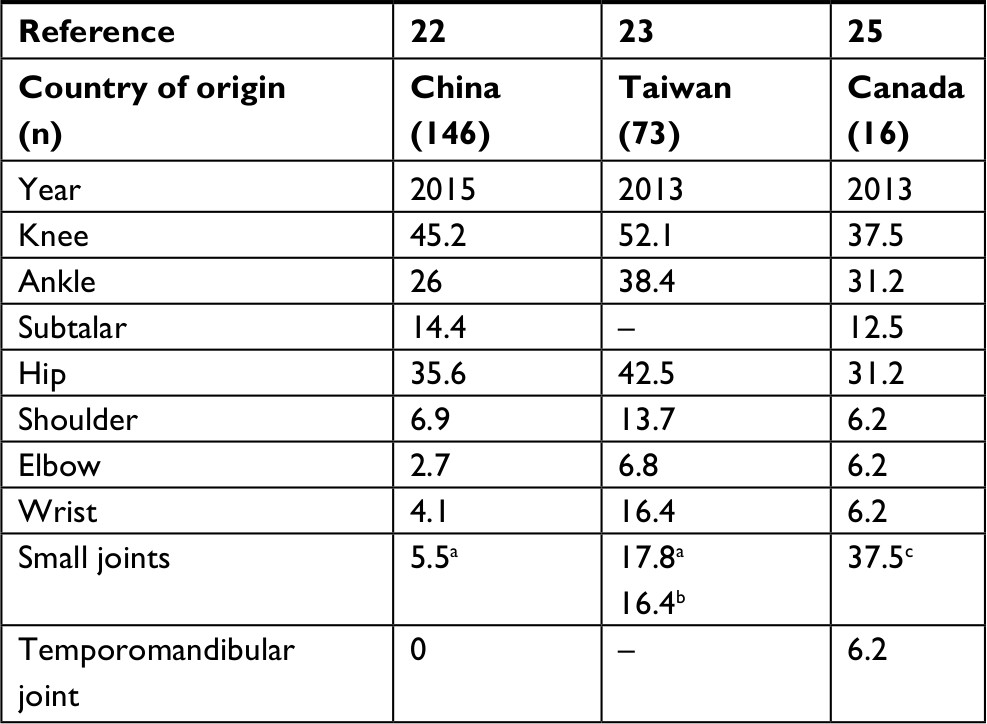 | Table 2 Frequency of involvement of individual joints (percentage) in different cohorts of enthesitis-related arthritis Note: aSmall joints of hand; bsmall joints of feet; csmall joints of hand or feet. |
Axial involvement is a characteristic feature of ERA. Involvement of the sacroiliac joints may be seen in up to a third of children with ERA; however, it may be clinically inapparent in about a fifth of such children, demonstrable only by imaging techniques such as MRI. Those children with hip arthritis are more likely to also have additional sacroiliac joint involvement.32 The shoulder joints may be involved in about a tenth of such patients.22,23
Extra-articular features
Systemic symptoms in the form of fever may be a prominent presenting manifestation in about a third of children with ERA, and such patients tend to have more active arthritis at presentation.22 Uveitis is a characteristic feature of ERA, seen in about a fifth of such children.33 Uveitis associated with JIA may be acute (ie, acute onset, generally resolving in a short time period), recurrent (episodes recur after >3 months of each other), or chronic (persistent uveitis, which recurs within 3 months of stopping therapy).34 Certain disease characteristics are associated with a higher risk of developing uveitis, such as earlier age of onset, female gender, antinuclear antibody (ANA) positivity, and subtypes of oligoarticular JIA, juvenile psoriatic arthritis, or undifferentiated arthritis for chronic anterior uveitis. On the contrary, male gender with ERA subtype, especially in the presence of HLA-B27, predisposes toward a higher risk of acute anterior uveitis.34 Considering that chronic uveitis in JIA can be asymptomatic until vision loss occurs, it is essential to screen in a protocolized manner for the same, especially in younger females with oligoarticular JIA who are ANA positive.34 Management of uveitis in children is initially with topical corticosteroid drops, which if required for >3 months, or if ineffective, form an indication for disease-modifying antirheumatic drug (DMARD) therapy. Methotrexate is the first-line DMARD in such a case, followed by anti-TNFα targeted agents, ie, adalimumab, infliximab, or golimumab, with other biologics such as abatacept, tocilizumab, and rituximab intended for use in refractory cases. Of note, etanercept has not shown efficacy in uveitis and may actually increase the risk of new onset of uveitis.35 Gut inflammation is another common extra-articular feature in such children. In a study including eight children with ERA who had some gastrointestinal symptoms, biopsies from the colon, small bowel, stomach, or esophagus revealed nonspecific inflammatory changes in five of eight children.36 In another study of four children with ERA who had elevated fecal calprotectin levels suggesting the presence of gut inflammation, of whom only one was symptomatic, MRI of the abdomen revealed the presence of IBD in three children.37
Considering the significant inflammatory burden in such children, another concern in such children remains the risk of developing premature atherosclerosis resulting in increased predisposition toward cardiovascular events. Studies have demonstrated increased subclinical atherosclerosis in the form of increased carotid intima-media thickness and aortic stiffness along with endothelial dysfunction in such children.38 However, a cohort of 211 patients with JIA followed up over >29 years did not reveal an increased occurrence of cardiovascular events in such patients when compared with the general population.39
Diagnosis
ERA remains a clinical diagnosis, whenever a child with peripheral arthritis has enthesitis or axial involvement in the form of inflammatory low backache or clinical sacroiliitis, especially in a male child. The differential diagnosis of presentation with peripheral oligoarthritis in a child should entail consideration of other differential diagnoses. If monoarthritis is the predominant presentation, then septic arthritis merits consideration, with an urgent joint aspiration and microbiological analysis of synovial fluid mandatory. Recent history of gastrointestinal or urinary infection, especially if microbiologically proven, followed by a history of oligoarthritis with enthesitis should merit consideration of reactive arthritis. Viral infections like rubella, parvovirus, and dengue can cause acute onset, generally short-lasting inflammatory arthritis in children, whereas chikungunya virus infection can cause persistent arthritis. Hematological neoplasias can present with joint pains, worse at nights, often without much swelling; therefore, it is essential to look at the peripheral blood picture and consider doing a bone marrow examination to look for childhood leukemias if there is any suggestion of low platelets or leukopenia. In a male child with mono- or oligoarthritis following trauma, hemarthrosis resulting from underlying hemophilia must be considered. Rare synovial tumors such as pigmented villonodular synovitis can also present with oligoarthritis, especially of the lower limb joints, and can be diagnosed by MRI, confirmed by synovial biopsy. Differentiation from other subtypes of JIA has been discussed previously.40–42
In many instances, however, the presentation may be early during the course of illness,43 such as involvement of joints in an oligoarticular fashion without clinically apparent enthesitis or sacroiliitis. Keeping in mind such instances, it is important to discuss investigation modalities for the diagnosis of early disease or clinically inapparent disease. In a study involving 40 patients with JIA (including five with ERA), it was demonstrated that the use of ultrasound to detect synovitis was more sensitive (45%) than a clinical examination alone (sensitivity 34%).43 In another study of 19 children with JIA (only one had ERA), clinical examination to diagnose synovitis of the ankle and knee joints only has a sensitivity of 64% while retaining a reasonable specificity of 86%. Interestingly, of those children who had clinically inapparent synovitis detectable only on ultrasound, nearly a fifth developed clinical synovitis in the involved joint within 6 months.44 Another study of 30 children with ERA revealed clinical enthesitis in only half, but ultrasonographic enthesitis in 83% children.45 Ultrasonography of the entheseal sites has been shown to be superior (interrater and intrarater reliability nearly 80%) compared with the use of dolorimetry (interrater reliability about 50%).46 Another concern while objectively assessing the presence of enthesitis is the normal entheseal thickness in children, which a study of healthy children revealed to be directly proportional to the weight of the child, with the ability to detect differences in entheseal thickness in between the two sides at the superior patellar tendon insertion, inferior patellar tendon insertion at the tibial tuberosity, or Achilles insertion beyond 28%, 26%, or 18%.47 The recent definition of enthesitis in spondyloarthropathy by the Outcome Measures in Rheumatology (OMERACT) group have helped clinicians standardize their practice, with the requirement of entheseal site tendon thickening, erosion, enthesophyte, irregularity, power Doppler signal within 2 mm of insertion of tendon to bone, or calcifications at the entheseal site to make a diagnosis of ultrasonographic enthesitis.48 In this vein, it must be reiterated that the present accepted practice for the diagnosis of arthritis and enthesitis in children remains clinical assessment, with ultrasound only playing an adjunctive role in this process. The present classification criteria for ERA do not mention the use of imaging modalities,1 and these may require to be addressed in a future revision of these criteria.
Another important modality to assess disease extent in ERA is the use of MRI, especially to detect the presence of sacroiliitis. This is generally defined as either the presence of erosions or synovial thickening in the lower, synovial portion of the sacroiliac joint, or the presence of associated bone marrow edema around the sacroiliac joint, which can then be graded for its intensity and the depth at which this is present.49 Recent literature suggests that noncontrast MRI of the sacroiliac joints using fluid-sensitive sequences has similar sensitivity and specificity to contrast-enhanced MRI in children.50 In a study on 58 pediatric patients with ERA, the review of the MRI of the pelvic region done at the time of diagnosis revealed the presence of sacroiliitis in nearly four-fifth of such children, whereas other abnormalities in the lumbar spine were present in nearly two-thirds, the most common being synovitis of the apophyseal joint.51 In another cohort of 50 children with juvenile-onset spondyloarthropathy, MRI evidence of sacroiliitis was evident in about two-thirds, despite being clinically inapparent in about 40% of such patients. In about a third of such children with sacroiliitis, synovial enhancement was demonstrable even in the absence of marrow edema. Nearly four-fifth of such children had associated hip arthritis, whereas two-fifth had pelvic enthesitis on MRI.52 Another study retrospectively evaluated MRI films of 143 patients with JIA, of whom 58 had ERA. It was interesting to note that pelvic enthesitis was present in nearly a fifth of patients with ERA (ie, having clinically apparent peripheral enthesitis), while nearly a seventh of the remaining children with JIA also had pelvic enthesitis on MRI. An additional seven children could have been more appropriately classified as ERA had pelvic enthesitis been sought on MRI, and in the presence of pelvic enthesitis, about three-fourth of children had sacroiliitis.53 Recent literature suggests the utility of a sacroiliac inflammation scoring system initially developed for use on adults with spondyloarthritis by the Spondyloarthritis Research Consortium of Canada (SPARCC), in children with juvenile spondyloarthropathy, with good intraclass correlation coefficient of nearly 80%, and an ability to differentiate those children with elevated serum C-reactive protein from those without.54 In spite of the above literature, it is still unclear whether every child with ERA should be screened for the presence of sacroiliitis or inflammatory disease in the lumbar spine by MRI. Indeed, in another recent study of 20 children with ERA, the presence of either buttock pain or clinically evident abnormalities on lumbar spine examination was associated with positive predictive value of 75% for the presence of sacroiliitis on MRI, and the absence of both these had negative predictive value of 83% for MRI sacroiliitis, suggesting that a clinical evaluation is sufficient in such patients to suspect sacroiliitis.28 While the use of plain radiography of the sacroiliac joints is a useful modality for detecting sacroiliitis in adults, the same does not hold true in children. This was emphasized in a recent study analyzing 60 pairs of MRI and plain radiographs in children with juvenile spondyloarthritis, wherein the sensitivity of X-ray compared with MRI varied from 25% to 78% and specificity varied from 60% to 92%, with significant interobserver variability for most parameters of plain radiographs.55 Positron emission tomography computerized tomography using 18-fluorodeoxyglucose to identify sites of increased metabolic activity, and thereby, inflammation, is yet another technique to assess the extent of disease in ERA. However, its practical utility is limited due to lack of widespread availability, significant radiation exposure, and high costs.56
Disease assessment and outcomes
Initial attempts to devise disease activity indices for children with JIA had resulted in the Juvenile Arthritis Disease Activity Score (JADAS), which assessed four parameters, physician global assessment, patient global assessment, inflammatory marker [erythrocyte sedimentation rate (ESR)], and active joint count.57,58 However, the utility of this particular tool in ERA was limited due to lack of assessment of enthesitis, which is a major cause of morbidity in such children.59 Subsequent outcome measures devised in children with ERA were the Juvenile Arthritis Parent Assessment Index (JAPAI) and the Juvenile Arthritis Child Assessment Index (JACAI), both of which were composite indices assessing four parameters, ie, pain, physical function, quality of life, and global well-being assessment of either the parent or the child, and these were found to be valid indices overall for JIA.60 Another core set of criteria for assessing improvement in clinical trials in children with JIA are the American College of Rheumatology (ACR) pediatric response criteria, which assess improvement across six domains, physician global assessment, patient or parent global assessment, functional status, inflammatory marker (ESR), number of joints with active arthritis, and the number of joints whose mobility is restricted. ACR Pedi 30, 50, 70, 90, and 100 criteria have been proposed, each of which requires the absence of worsening in more than one domain by 30%, along with improvement in at least three out of the six domains by 30%, 50%, 70%, 90%, and 100%, respectively.58 The accurate assessment of disease activity in ERA by these criteria is limited by the lack of recognition of enthesitis, a key component and major cause of disability in ERA.61 A recent development of note in this area was the development of the juvenile spondyloarthropathy disease activity index, which was the first validated index for use exclusively in children with ERA, and recognized the key components of this disease, viz enthesitis, sacroiliitis, inflammatory low back ache with early morning stiffness lasting at least 15 minutes, and restricted lumbar flexion. This index could segregate active from inactive disease, as well as demonstrated responsiveness to change.62
It must be noted that the ACR recommendations for the management of JIA do not separately prognosticate different ILAR classes of JIA, but rather do so on the basis of involved joints. For those with sacroiliitis, the presence of radiographic damage, either erosions or narrowing of the joint space, is a marker of poor prognosis. For those with peripheral arthritis of four or less joints, the presence of certain axial features (cervical spine or hip involvement) or peripheral features (ankle or wrist arthritis, along with either persistent or marked elevation of acute phase reactants), along with radiographic joint damage are poor prognostic factors. Similarly, for those with involvement of five or more joints, the presence of either cervical spine or hip joint arthritis, seropositivity for RF or anti-citrullinated peptide antibodies, or radiographic joint damage portend a poorer prognosis.10 Few studies have exclusively assessed outcomes in children with ERA. It has been suggested that the presence of ERA is associated with worse long-term outcomes than either the presence of oligoarticular or polyarticular JIA, when followed up for >15 years. Over a longer term, only two-fifth of children attained remission, whereas nearly a third developed clinically evident sacroiliitis and three-fourth developed restricted spinal mobility. Such children had lesser degree of physical functioning and poorer overall physical health, along with greater pain scores than their other disease counterparts. Male sex, ankle arthritis, presence of hip arthritis, and persistent elevation of ESR were markers of a poorer long-term prognosis.63 This was confirmed in another study of 398 patients with JIA (nearly a fourth of whom had ERA), wherein the presence of either ERA or oligoarticular disease was associated with greater amount of body pain, worse quality of life, and greater impairment of physical functioning.59 Another study of 118 patients with juvenile-onset spondyloarthropathy followed up over 4 years revealed that only a fourth could attain drug-free remission, and greater than half continued to have active disease. About a third of those with active peripheral arthritis at initial presentation had persistent arthritis after 4 years, whereas the same was true for nearly a half of patients with inflammatory low back pain at presentation.64 A study from Portugal assessed 426 patients with JIA who had transitioned into adulthood and found that nearly 95% of those who had ERA could be classified as adult spondyloarthropathy. Interestingly, about a third of patients with persistent oligoarticular disease could also be classified as having adult spondyloarthritis.65 Although HLA-B27 is associated with ERA, a study of >305 children with JIA (of whom only a tenth had ERA) revealed that the presence of HLA-B27 predisposed children of both sexes to develop inflammatory low back ache and also predisposed male children to develop more small joint arthritis in the feet and enthesitis.66
Management
Initial management of patients with ERA is with administration of NSAID, often sequentially if one particular NSAID does not work.67 There are limited data in adult spondyloarthropathy that suggests that the continuous use of NSAIDs may potentially retard spinal radiographic progression;68 however, such evidence is sparse in ERA. The risk of subclinical renal injury even with a short course of NSAIDs in young subjects with otherwise normal renal functions should always be kept in mind while prescribing NSAIDs to such patients.69
Sulfasalazine is a DMARD commonly used in such patients. Classically, sulfasalazine is used in patients with active peripheral arthritis in spite of NSAID use. Since bowel wall inflammation may be an antecedent event in patients with ERA and spondyloarthritis, the potential action of sulfasalazine on the gut wall and its permeability may underlie its effectiveness in this group of diseases.70 Few studies have systematically studied the effectiveness of sulfasalazine in juvenile spondyloarthropathy or ERA. In a randomized double-blind placebo controlled trial of 33 children with juvenile spondyloarthritis (16 treated with placebo and 17 with sulfasalazine, at a dose of 2 g/day if weight was >30 kg, or 30–60 mg/kg/day if weight was <30 kg) over 26 weeks, the significant differences were better overall improvement as assessed by the physician as well as the patient in those receiving sulfasalazine than placebo.71 Another older study predating the ILAR classification criteria (thereby did not separately describe ERA) studied the safety and efficacy of sulfasalazine in 32 children with either oligoarticular or polyarticular involvement compared with 29 on placebo over 24 weeks and demonstrated that while sulfasalazine was effective in improving the severity of joint inflammation, about a third had poor tolerability.72 On a longer term follow-up of nearly 9 years, those children treated in this trail with sulfasalazine had better long-term outcomes than those on placebo.73 Although studies on the use of methotrexate in ERA are sparse, the ACR recommendations for the management of JIA suggest the use of methotrexate as an early agent for peripheral arthritis in JIA10,74
For those patients with ERA who fail to respond to conventional DMARDs, biologic DMARDs (bDMARDs) are the treatment of choice. Anti-TNF agents are the first choice of bDMARD, and the evidences for the effectiveness of their utility in ERA are drawn from a few prospective clinical trials (summarized in Table 3)75–80 and mostly retrospective or registry-based data (Table 4).81–86 Overall, these drugs help to improve arthritis and enthesitis, as well as patient/parent and physician global assessment, and quality of life scores. Most of the studies in this regard have used either etanercept or adalimumab in these children, including two randomized controlled trials on these drugs, which demonstrated beneficial effects compared with placebo in reducing disease activity as well as the frequency of relapses.76,77 The major concern with the use of anti-TNF agents is the risk of reactivation of latent tuberculosis infection, especially in Asian countries where tuberculosis is endemic.67 Other significant concerns remain the higher risk of uveitis or IBD in children receiving etanercept, although the risk remains low. A recent retrospective study reported the effectiveness of ustekinumab (a blocker of the common p40 subunit of the IL-12 and IL-23 receptor, thereby interrupting the activation of both Th1 and Th17 cells) in arthritis, enthesitis, and sacroiliitis in four out of five children with refractory ERA treated over 1–12 months, with no specific adverse safety signals. Overall, compared with other subtypes of JIA, the literature on the management of ERA is sparse, probably due to its relative rarity except in Asian populations.86 Literature on the use of other bDMARDs specifically in the subtype of ERA is sparse.87
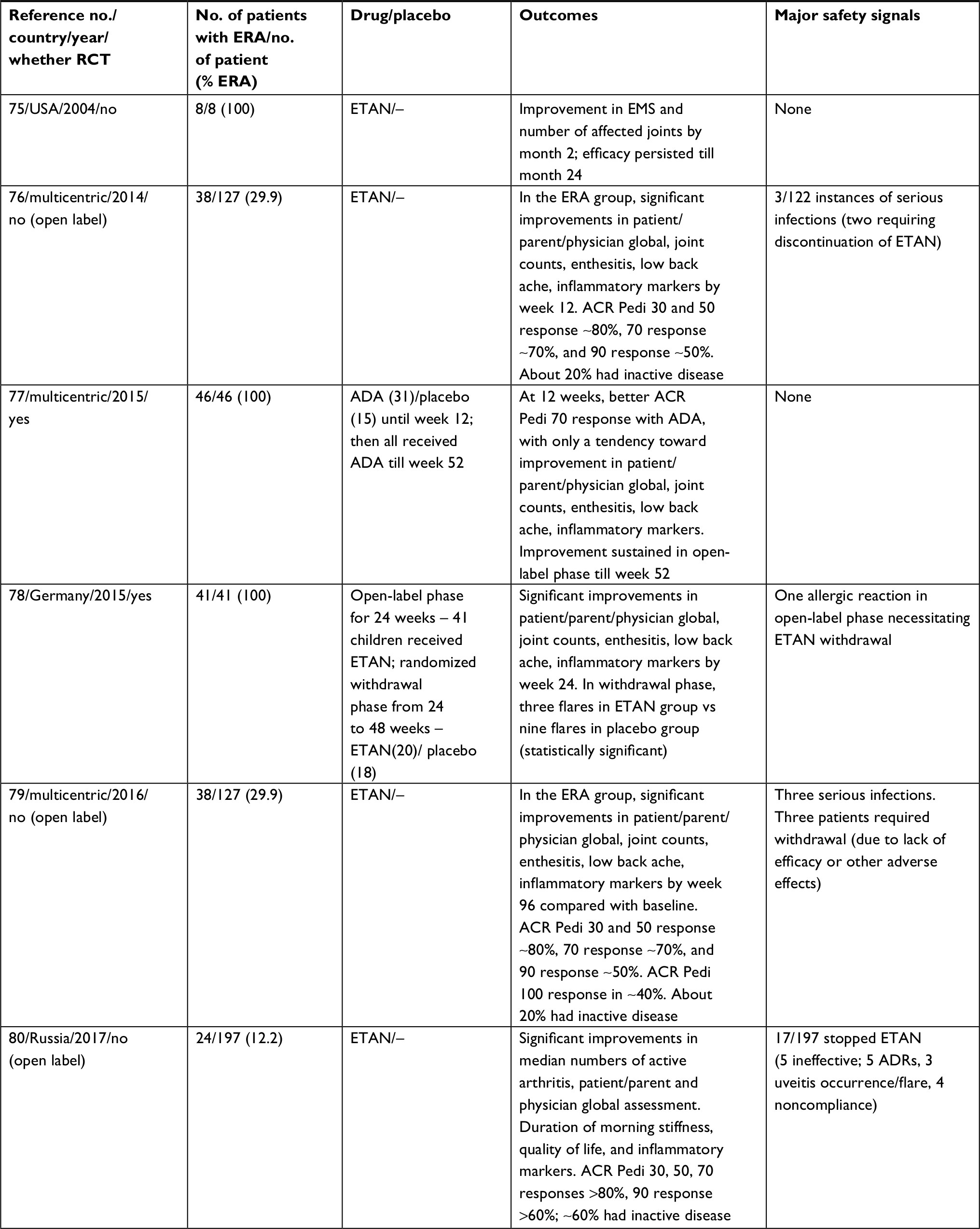 | Table 3 Summary of prospective studies on the use of biologic DMARDs in patients with ERA Abbreviations: ACR Pedi 30, 50, 70, 90, and 100, American College of Rheumatology Pediatric 30, 50, 70, 90, and 100 Response; ADA, adalimumab; ADRs, adverse drug reactions; DMARDs, disease-modifying antirheumatic drugs; EMS, early morning stiffness; ERA, enthesitis-related arthritis; ETAN, etanercept; RCT, randomized controlled trial. |
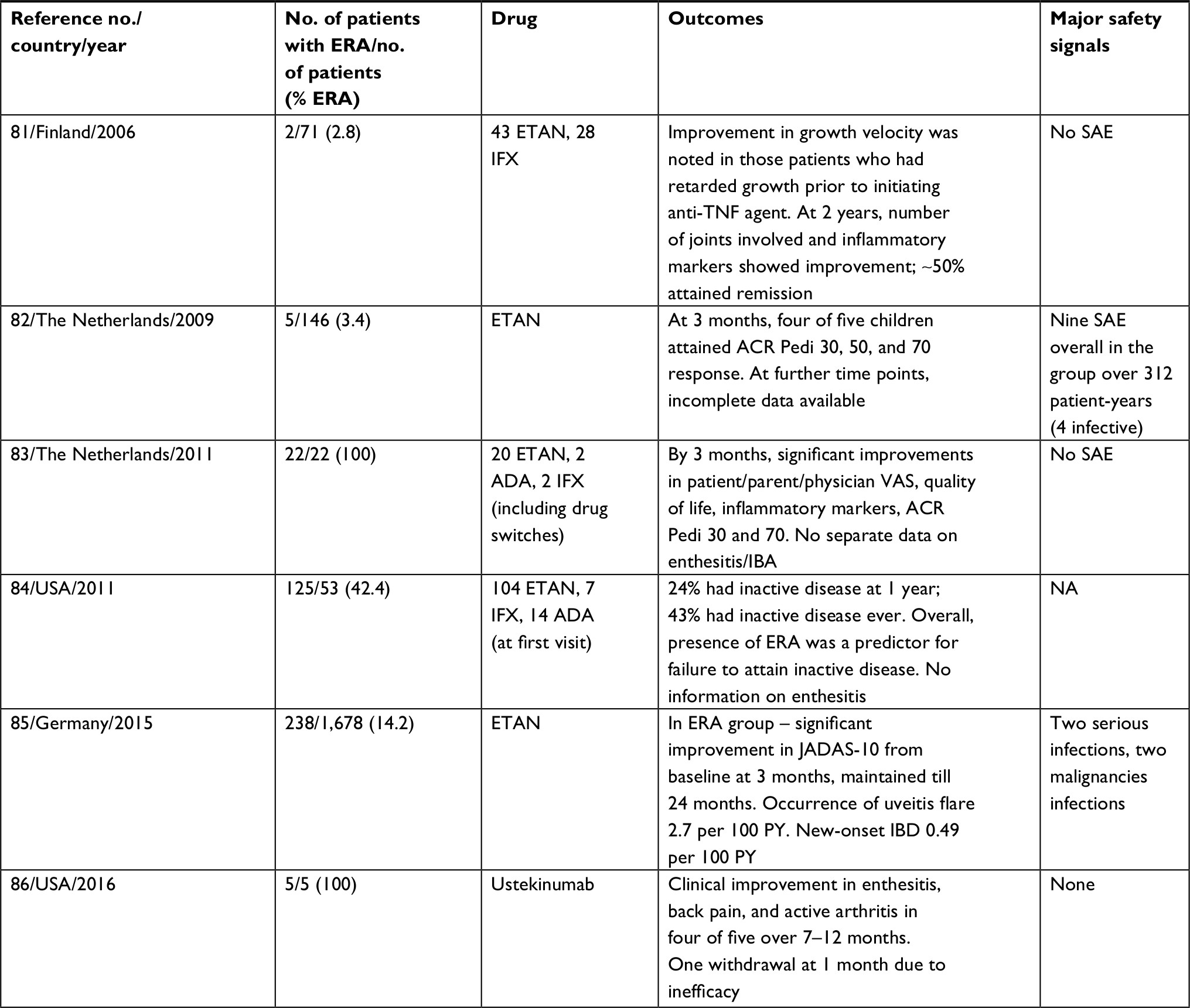 | Table 4 Summary of retrospective/registry-based studies on biological DMARDs in ERA Abbreviations: ACR Pedi 30, 50, 70, 90, and 100, American College of Rheumatology Pediatric 30, 50, 70, 90, and 100 Response; ADA, adalimumab; DMARDs, disease-modifying antirheumatic drugs; ERA, enthesitis-related arthritis; ETAN, etanercept; IBA, inflammatory backache; IBD, inflammatory bowel disease; IFX, infliximab; JADAS-10, Juvenile Arthritis Disease Activity Score 10; NA, not available; SAE, serious adverse events; PY, patient years; TNF, tumor necrosis factor. |
Exercises form an important adjunct to the therapy of ERA. For those with axial involvement, regular exercises to stretch and maintain the flexibility of the spine are essential in an attempt to preserve spinal mobility. Since the end result of long-term untreated spondyloarthritis/ERA affecting the spine is a flexed posture, such exercises logically emphasize spinal extension. A proportion of patients with more advanced disease may not be able to perform spinal extension; instead, they may be advised to at least lie prone on a hard bed for at least an hour every day.88 Additional aerobic exercises to the conventionally prescribed physiotherapy may not be of much benefit.89 Apart from spinal disease, exercise also forms a critical adjunct to the management of inflamed joints, wherein passive movements are encouraged in the presence of active arthritis in an attempt to maintain the range of motion and prevent contractures, whereas active muscle strengthening exercises should be done after the acute phase of joint inflammation has settled down.90 Limited evidence suggests that aquatic exercise (such as swimming) may help patients with spondyloarthritis.91,92 Similarly, in the management of enthesitis, cold application may help in the acute phase. With respect to Achilles tendinitis, the use of a high-heel shoe may help keep the inflamed Achilles insertion in a relaxed state.93 For plantar fasciitis, the use of a soft sole, as well as heel stretching exercises may help.94
ACR recommendations for the management of JIA have discussed the treatment strategies based on the number of joints involved and the presence or absence of systemic features. The recommendations for oligoarticular involvement (four or less joints) propose initial management with NSAIDs or intra-articular glucocorticoid injections. Only in the presence of either high disease activity or poor prognostic factors (discussed previously), they recommend the use of methotrexate or leflunomide. Should disease activity continue to be moderate to high in the presence of poor prognostic factors, a switch to anti-TNFα agents (anti-TNF) is recommended at 3 months, whereas if the disease remains highly active at 6 months after initiating methotrexate or leflunomide, irrespective of prognostic factors, a switch to anti-TNF agents is recommended. In case of polyarticular involvement, upfront use of methotrexate or leflunomide is recommended with adjunct use of either intra-articular injections of corticosteroids or NSAIDs, with similar strategy for the use of anti-TNF agent after reassessment at 3 or 6 months as for oligoarticular involvement. Should the disease continue to be moderately to highly active at 4 months after treatment with anti-TNF agent, then either another of the anti-TNF agents or abatacept may be tried in such children. The only statement specifically related to ERA from these guidelines was that in children with ERA, irrespective of the presence or absence of poor prognostic factors, those children continuing to have moderately to highly active disease after initial trial of intra-articular corticosteroids or NSAID should be commenced on sulfasalazine. No specific mention of the use of leflunomide has been made for ERA.10,74
Most of our patients are from a lower socioeconomic background and cannot afford bDMARDs, and there is a lack of government support for such costly therapies.67 Our personal preference for patients with ERA with purely axial disease is to initiate NSAIDs at baseline and assess further improvements after also advising concomitant physical therapy. Once the patient shows clinical improvement, we attempt reducing the dose of NSAID initially, and if possible, stop it altogether while continuing physical therapy. Should an attempt to reduce the dose of NSAID or to stop NSAID not be successful, or monotherapy with NSAID not be successful, we generally add a conventional DMARD, preferably sulfasalazine, since in our experience this helps even in patients with pure axial disease. For those with peripheral arthritis alone, or with both axial and peripheral arthritis, we generally add a conventional DMARD, either sulfasalazine or methotrexate, along with NSAID from the beginning itself, in an attempt to minimize the duration of daily, full-dose NSAID exposure.
Conclusion
While ERA is relatively uncommon in Caucasian series, it remains one of the commonest forms of JIA seen in Asia. Enthesitis and axial involvement along with oligo- or polyarthritis predominantly of the lower limb joints are characteristic features. Uveitis and IBD are common accompaniments. Initial management is with NSAIDs and physical therapy with intra-articular corticosteroids if there is oligoarthritis, with a preference to add sulfasalazine to minimize eventual NSAID use. If conventional DMARDs fail, then anti-TNF agents are the drug of choice, always keeping in mind their associated costs and infection risks. Ankle and hip involvement as well as positivity for HLA-B27 portend a poorer long-term prognosis in such children.
Author contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Petty RE, Southwood TR, Manners P, et al. International league of associations for rheumatology classification of juvenile idiopathic arthritis: second revision, Edmonton, 2001. J Rheumatol. 2004;31(2):390–392. | ||
Sieper J, Rudwaleit M, Baraliakos X, et al. The Assessment of SpondyloArthritis international Society (ASAS) handbook: a guide to assess spondyloarthritis. Ann Rheum Dis. 2009;68(Suppl 2):ii1–ii44. | ||
Gasparyan AY, Ayvazyan L, Blackmore H, Kitas GD. Writing a narrative biomedical review: considerations for authors, peer reviewers, and editors. Rheumatol Int. 2011;31(11):1409–1417. | ||
Żuber Z, Turowska-Heydel D, Sobczyk M, Chudek J. Prevalence of HLA-B27 antigen in patients with juvenile idiopathic arthritis. Reumatologia. 2015;53(3):125–130. | ||
Chen B, Li J, He C, et al. Role of HLA-B27 in the pathogenesis of ankylosing spondylitis (Review). Mol Med Rep. 2017;15(4):1943–1951. | ||
Hersh AO, Prahalad S. Genetics of juvenile idiopathic arthritis. Rheum Dis Clin North Am. 2017;43(3):435–448. | ||
Kenna TJ, Robinson PC, Haroon N. Endoplasmic reticulum aminopeptidases in the pathogenesis of ankylosing spondylitis. Rheumatology. 2015;54(9):1549–1556. | ||
Breban M, Araujo LM, Chiocchia G. Editorial: animal models of spondyloarthritis: do they faithfully mirror human disease? Arthritis Rheumatol. 2014;66(7):1689–1692. | ||
Paramarta JE, van der Leij C, Gofita I, et al. Peripheral joint inflammation in early onset spondyloarthritis is not specifically related to enthesitis. Ann Rheum Dis. 2014;73(4):735–740. | ||
Beukelman T, Patkar NM, Saag KG, et al. 2011 American College of Rheumatology recommendations for the treatment of juvenile idiopathic arthritis: initiation and safety monitoring of therapeutic agents for the treatment of arthritis and systemic features. Arthritis Care Res. 2011;63(4):465–482. | ||
Scola MP, Thompson SD, Brunner HI, et al. Interferon-gamma:interleukin 4 ratios and associated type 1 cytokine expression in juvenile rheumatoid arthritis synovial tissue. J Rheumatol. 2002;29(2):369–378. | ||
Baerlecken NT, Nothdorft S, Stummvoll GH, et al. Autoantibodies against CD74 in spondyloarthritis. Ann Rheum Dis. 2014;73(6):1211–1214. | ||
Ranganathan V, Ciccia F, Zeng F, et al. Macrophage migration inhibitory factor induces inflammation and predicts spinal progression in ankylosing spondylitis. Arthritis Rheumatol. 2017;69(9):1796–1806. | ||
Jacques P, Lambrecht S, Verheugen E, et al. Proof of concept: enthesitis and new bone formation in spondyloarthritis are driven by mechanical strain and stromal cells. Ann Rheum Dis. 2014;73(2):437–445. | ||
Sherlock JP, Joyce-Shaikh B, Turner SP, et al. IL-23 induces spondyloarthropathy by acting on ROR-γt+ CD3+CD4-CD8- entheseal resident T cells. Nat Med. 2012;18(7):1069–1076. | ||
Stoll ML, Weiss PF, Weiss JE, et al. Age and fecal microbial strain-specific differences in patients with spondyloarthritis. Arthritis Res Ther. 2018;20(1):14. | ||
Stoll ML, Kumar R, Lefkowitz EJ, Cron RQ, Morrow CD, Barnes S. Fecal metabolomics in pediatric spondyloarthritis implicate decreased metabolic diversity and altered tryptophan metabolism as pathogenic factors. Genes Immun. 2016;17(7):400–405. | ||
Shukla A, Gaur P, Aggarwal A. Effect of probiotics on clinical and immune parameters in enthesitis-related arthritis category of juvenile idiopathic arthritis. Clin Exp Immunol. 2016;185(3):301–308. | ||
Giancane G, Consolaro A, Lanni S, Davì S, Schiappapietra B, Ravelli A. Juvenile idiopathic arthritis: diagnosis and treatment. Rheumatol Ther. 2016;3(2):187–207. | ||
Barut K, Adrovic A, Şahin S, Kasapçopur Ö. Juvenile idiopathic arthritis. Balkan Med J. 2017;34(2):90–101. | ||
Kunjir V, Venugopalan A, Chopra A. Profile of Indian patients with juvenile onset chronic inflammatory joint disease using the ILAR classification criteria for JIA: a community-based cohort study. J Rheumatol. 2010;37(8):1756–1762. | ||
Guo R, Cao L, Kong X, et al. Fever as an initial manifestation of enthesitis-related arthritis subtype of juvenile idiopathic arthritis: retrospective study. PLoS One. 2015;10(6):e0128979. | ||
Shen CC, Yeh KW, Ou LS, Yao TC, Chen LC, Huang JL. Clinical features of children with juvenile idiopathic arthritis using the ILAR classification criteria: a community-based cohort study in Taiwan. J Microbiol Immunol Infect. 2013;46(4):288–294. | ||
Demirkaya E, Ozen S, Bilginer Y, et al. The distribution of juvenile idiopathic arthritis in the eastern Mediterranean: results from the registry of the Turkish Paediatric Rheumatology Association. Clin Exp Rheumatol. 2011;29(1):111–116. | ||
Butbul Aviel Y, Tyrrell P, Schneider R, et al. Juvenile Psoriatic Arthritis (JPsA): juvenile arthritis with psoriasis? Pediatr Rheumatol Online J. 2013;11(1):11. | ||
Żuber Z, Kania U, Król-Zdechlikiewicz A, et al. Analysis of clinical symptoms and laboratory profiles in children with juvenile idiopathic arthritis in Malopolska region (Poland) in the years 2007-2010. Open Access Maced J Med Sci. 2014;2(1):56–61. | ||
Vilaiyuk S, Soponkanaporn S, Jaovisidha S, Benjaponpitak S, Manuyakorn W. A retrospective study on 158 Thai patients with juvenile idiopathic arthritis followed in a single center over a 15-year period. Int J Rheum Dis. 2016;19(12):1342–1350. | ||
Bou Antoun M, Adamsbaum C, Semerano L, Koné-Paut I, Rossi-Semerano L. Clinical predictors of magnetic resonance imaging-detected sacroiliitis in children with enthesitis related arthritis. Joint Bone Spine. 2017;84(6):699–702. | ||
Ramanathan A, Srinivasalu H, Colbert RA. Update on juvenile spondyloarthritis. Rheum Dis Clin North Am. 2013;39(4):767–788. | ||
Weiss PF, Klink AJ, Behrens EM, et al. Enthesitis in an inception cohort of enthesitis-related arthritis. Arthritis Care Res. 2011;63(9):1307–1312. | ||
Rumsey DG, Guzman J, Rosenberg AM, et al. Characteristics and course of enthesitis in a juvenile idiopathic arthritis inception Cohort. Arthritis Care Res. 2018;70(2):303–308. | ||
Stoll ML, Bhore R, Dempsey-Robertson M, Punaro M. Spondyloarthritis in a pediatric population: risk factors for sacroiliitis. J Rheumatol. 2010;37(11):2402–2408. | ||
Heiligenhaus A, Minden K, Föll D, Pleyer U. Uveitis in juvenile idiopathic arthritis. Dtsch Arztebl Int. 2015;112(6):92–100. | ||
Sen ES, Ramanan AV. Juvenile idiopathic arthritis-associated uveitis. Best Pract Res Clin Rheumatol. 2017;31(4):517–534. | ||
Constantin T, Foeldvari I, Anton J, et al. Consensus-based recommendations for the management of uveitis associated with juvenile idiopathic arthritis: the SHARE initiative. Ann Rheum Dis. 2018;77(8):1107–1117. | ||
Pichler J, Ong C, Shah N, et al. Histopathological features of gastrointestinal mucosal biopsies in children with juvenile idiopathic arthritis. Pediatr Res. 2016;79(6):895–901. | ||
Stoll ML, Patel AS, Punaro M, Dempsey-Robertson M. MR enterography to evaluate sub-clinical intestinal inflammation in children with spondyloarthritis. Pediatr Rheumatol Online J. 2012;10(1):6. | ||
del Giudice E, Dilillo A, Tromba L, et al. Aortic, carotid intima-media thickness and flow-mediated dilation as markers of early atherosclerosis in a cohort of pediatric patients with rheumatic diseases. Clin Rheumatol. 2018;37(6):1675–1682. | ||
Anderson JH, Anderson KR, Aulie HA, et al. Juvenile idiopathic arthritis and future risk for cardiovascular disease: a multicenter study. Scand J Rheumatol. 2016;45(4):299–303. | ||
Kim KH, Kim DS. Juvenile idiopathic arthritis: diagnosis and differential diagnosis. Korean J Pediatr. 2010;53(11):931–935. | ||
Malleson PN. Management of childhood arthritis. Part 1: Acute arthritis. Arch Dis Child. 1997;76(5):460–462. | ||
Dhochak N, Kabra SK, Lodha R. Dengue and chikungunya infections in children: Guest Editor: Bhim S. Pandhi. Indian J Pediatr. Epub 2018 Dec 4. | ||
Darwish AF, Ismael FM, Ell-Laban A, Hamed A, Kader MA, Osman A. Implementation of musculoskeletal ultrasonography in detection of early juvenile idiopathic arthritis. Eur J Radiol Open. 2016;3:264–271. | ||
Janow GL, Panghaal V, Trinh A, Badger D, Levin TL, Ilowite NT. Detection of active disease in juvenile idiopathic arthritis: sensitivity and specificity of the physical examination vs ultrasound. J Rheumatol. 2011;38(12):2671–2674. | ||
Shenoy S, Aggarwal A. Sonologic enthesitis in children with enthesitis-related arthritis. Clin Exp Rheumatol. 2016;34(1):143–147. | ||
Weiss PF, Chauvin NA, Klink AJ, et al. Detection of enthesitis in children with enthesitis-related arthritis: dolorimetry compared with ultrasonography. Arthritis Rheumatol. 2014;66(1):218–227. | ||
Lin C, Diab M, Milojevic D. Grey-scale ultrasound findings of lower extremity entheses in healthy children. Pediatric Rheumatology. 2015;13(1). | ||
Terslev L, Naredo E, Iagnocco A, et al. Defining enthesitis in spondyloarthritis by ultrasound: results of a Delphi process and of a reliability reading exercise. Arthritis Care Res. 2014;66(5):741–748. | ||
Weiss PF, Maksymowych WP, Lambert RG, et al. Feasibility and reliability of the spondyloarthritis research consortium of Canada sacroiliac joint inflammation score in children. Arthritis Res Ther. 2018;20(1):56. | ||
Weiss PF, Xiao R, Biko DM, Johnson AM, Chauvin NA. Detection of inflammatory sacroiliitis in children with magnetic resonance imaging: is gadolinium contrast enhancement necessary? Arthritis Rheumatol. 2015;67(8):2250–2256. | ||
Vendhan K, Sen D, Fisher C, Ioannou Y, Hall-Craggs MA. Inflammatory changes of the lumbar spine in children and adolescents with enthesitis-related arthritis: magnetic resonance imaging findings. Arthritis Care Res. 2014;66(1):40–46. | ||
Lin C, MacKenzie JD, Courtier JL, Gu JT, Milojevic D. Magnetic resonance imaging findings in juvenile spondyloarthropathy and effects of treatment observed on subsequent imaging. Pediatr Rheumatol Online J. 2014;12(1):25. | ||
Herregods N, Dehoorne J, Pattyn E, et al. Diagnostic value of pelvic enthesitis on MRI of the sacroiliac joints in enthesitis related arthritis. Pediatr Rheumatol Online J. 2015;13(1):46. | ||
Rumsey DG, Guzman J, Rosenberg AM, et al. Characteristics and course of enthesitis in a juvenile idiopathic arthritis inception cohort. Arthritis Care Res. 2018;70(2):303–308. | ||
Weiss PF, Xiao R, Brandon TG, et al. Radiographs in screening for sacroiliitis in children: what is the value? Arthritis Res Ther. 2018;20(1):141. | ||
Inoue N, Mizuta M, Shimizu M. Clinical usefulness of 18F-fluorodeoxyglucose positron emission tomography for enthesitis-related arthritis diagnosis. J Rheumatol. 2016;43(7):1434–1435. | ||
Consolaro A, Ruperto N, Bazso A, et al. Development and validation of a composite disease activity score for juvenile idiopathic arthritis. Arthritis Rheum. 2009;61(5):658–666. | ||
Consolaro A, Giancane G, Schiappapietra B, et al. Clinical outcome measures in juvenile idiopathic arthritis. Pediatr Rheumatol Online J. 2016;14(1):23. | ||
Taxter AJ, Wileyto EP, Behrens EM, Weiss PF. Patient-reported outcomes across categories of juvenile idiopathic arthritis. J Rheumatol. 2015;42(10):1914–1921. | ||
Consolaro A, Ruperto N, Pistorio A, et al. Development and initial validation of composite parent- and child-centered disease assessment indices for juvenile idiopathic arthritis. Arthritis Care Res. 2011;63(9):1262–1270. | ||
Oen K, Duffy CM, Tse SML, et al. Early outcomes and improvement of patients with juvenile idiopathic arthritis enrolled in a Canadian multicenter inception cohort. Arthritis Care Res. 2010;62(4):527–536. | ||
Weiss PF, Colbert RA, Xiao R, et al. Development and retrospective validation of the juvenile spondyloarthritis disease activity index. Arthritis Care Res. 2014;66(12):1775–1782. | ||
Flatø B, Hoffmann-Vold AM, Reiff A, Førre Ø, Lien G, Vinje O. Long-term outcome and prognostic factors in enthesitis-related arthritis: a case-control study. Arthritis Rheum. 2006;54(11):3573–3582. | ||
Weiß A, Minden K, Listing J, Foeldvari I, Sieper J, Rudwaleit M. Course of patients with juvenile spondyloarthritis during 4 years of observation, juvenile part of GESPIC. RMD Open. 2017;3(1):e000366. | ||
Oliveira-Ramos F, Eusébio M, M Martins F, et al. Juvenile idiopathic arthritis in adulthood: fulfilment of classification criteria for adult rheumatic diseases, long-term outcomes and predictors of inactive disease, functional status and damage. RMD Open. 2016;2(2):e000304. | ||
Berntson L, Damgård M, Andersson-Gäre B, et al. HLA-B27 predicts a more extended disease with increasing age at onset in boys with juvenile idiopathic arthritis. J Rheumatol. 2008;35(10):2055–2061. | ||
Misra DP, Sharma A, Agarwal V. Rheumatology science and practice in India. Rheumatol Int. 2018;38(9):1587–1600. | ||
Wanders A, Heijde D, Landewé R, et al. Nonsteroidal antiinflammatory drugs reduce radiographic progression in patients with ankylosing spondylitis: a randomized clinical trial. Arthritis Rheum. 2005;52(6):1756–1765. | ||
Shukla A, Rai MK, Prasad N, Agarwal V. Short-term non-steroid anti-inflammatory drug use in spondyloarthritis patients induces subclinical acute kidney injury: biomarkers study. Nephron. 2017;135(4):277–286. | ||
Mielants H, Veys EM, Cuvelier C, De Vos M. Course of gut inflammation in spondyloarthropathies and therapeutic consequences. Baillières Clin Rheumatol. 1996;10(1):147–164. | ||
Burgos-Vargas R, Vázquez-Mellado J, Pacheco-Tena C, Hernández-Garduño A, Goycochea-Robles MV. A 26 week randomised, double blind, placebo controlled exploratory study of sulfasalazine in juvenile onset spondyloarthropathies. Ann Rheum Dis. 2002;61(10):941–942. | ||
Van Rossum MA, Fiselier TJ, Franssen MJ, et al. Sulfasalazine in the treatment of juvenile chronic arthritis: a randomized, double-blind, placebo-controlled, multicenter study. Dutch Juvenile Chronic Arthritis Study Group. Arthritis Rheum. 1998;41(5):808–816. | ||
Van Rossum MA, Van Soesbergen RM, Boers M, et al. Long-term outcome of juvenile idiopathic arthritis following a placebo-controlled trial: sustained benefits of early sulfasalazine treatment. Ann Rheum Dis. 2007;66(11):1518–1524. | ||
Ringold S, Weiss PF, Beukelman T, et al. 2013 Update of the 2011 American College of Rheumatology Recommendations for the treatment of juvenile idiopathic arthritis: recommendations for the medical therapy of children with systemic juvenile idiopathic arthritis and tuberculosis screening among children receiving biologic medications. Arthritis Rheum. 2013;65(10):2499–2512. | ||
Henrickson M, Reiff A. Prolonged efficacy of etanercept in refractory enthesitis-related arthritis. J Rheumatol. 2004;31(10):2055–2061. | ||
Horneff G, Burgos-Vargas R, Constantin T, et al. Efficacy and safety of open-label etanercept on extended oligoarticular juvenile idiopathic arthritis, enthesitis-related arthritis and psoriatic arthritis: part 1 (week 12) of the CLIPPER study. Ann Rheum Dis. 2014;73(6):1114–1122. | ||
Burgos-Vargas R, Tse SML, Horneff G, et al. A randomized, double-blind, placebo-controlled multicenter study of adalimumab in pediatric patients with enthesitis-related arthritis. Arthritis Care Res. 2015;67(11):1503–1512. | ||
Horneff G, Foeldvari I, Minden K, et al. Efficacy and safety of etanercept in patients with the enthesitis-related arthritis category of juvenile idiopathic arthritis: results from a phase III randomized, double-blind study. Arthritis Rheumatol. 2015;67(8):2240–2249. | ||
Constantin T, Foeldvari I, Vojinovic J, et al. Two-year efficacy and safety of etanercept in pediatric patients with extended oligoarthritis, enthesitis-related arthritis, or psoriatic arthritis. J Rheumatol. 2016;43(4):816–824. | ||
Alexeeva EI, Namazova-Baranova LS, Bzarova TM, et al. Predictors of the response to etanercept in patients with juvenile idiopathic arthritis without systemic manifestations within 12 months: results of an open-label, prospective study conducted at the national scientific and practical center of children’s health, Russia. Pediatr Rheumatol Online J. 2017;15(1):51. | ||
Tynjälä P, Lahdenne P, Vähäsalo P, Kautiainen H, Honkanen V. Impact of anti-TNF treatment on growth in severe juvenile idiopathic arthritis. Ann Rheum Dis. 2006;65(8):1044–1049. | ||
Prince FH, Twilt M, Ten Cate R, et al. Long-term follow-up on effectiveness and safety of etanercept in juvenile idiopathic arthritis: the Dutch national register. Ann Rheum Dis. 2009;68(5):635–641. | ||
Otten MH, Prince FH, Twilt M, et al. Tumor necrosis factor-blocking agents for children with enthesitis-related arthritis--data from the Dutch arthritis and biologicals in children register, 1999-2010. J Rheumatol. 2011;38(10):2258–2263. | ||
Donnithorne KJ, Cron RQ, Beukelman T. Attainment of inactive disease status following initiation of TNF-α inhibitor therapy for juvenile idiopathic arthritis: enthesitis-related arthritis predicts persistent active disease. J Rheumatol. 2011;38(12):2675–2681. | ||
Windschall D, Müller T, Becker I, Horneff G. Safety and efficacy of etanercept in children with the JIA categories extended oligoarthritis, enthesitis-related arthritis and psoriasis arthritis. Clin Rheumatol. 2015;34(1):61–69. | ||
Mannion ML, McAllister L, Cron RQ, Stoll ML. Ustekinumab as a therapeutic option for children with refractory enthesitis-related arthritis. J Clin Rheumatol. 2016;22(5):282–284. | ||
Davies R, Gaynor D, Hyrich KL, Pain CE. Efficacy of biologic therapy across individual juvenile idiopathic arthritis subtypes: a systematic review. Semin Arthritis Rheum. 2017;46(5):584–593. | ||
Ozgocmen S, Akgul O, Altay Z, et al. Expert opinion and key recommendations for the physical therapy and rehabilitation of patients with ankylosing spondylitis. Int J Rheum Dis. 2012;15(3):229–238. | ||
Verhoeven F, Guillot X, Prati C, et al. Aerobic exercise for axial spondyloarthritis--its effects on disease activity and function as compared to standard physiotherapy: a systematic review and meta-analysis. Int J Rheum Dis. Epub 2018 Sep 5. | ||
Musumeci G. Effects of exercise on physical limitations and fatigue in rheumatic diseases. World J Orthop. 2015;6(10):762–769. | ||
Fernández García R, Sánchez Sánchez Ldec, López Rodríguez Mdelm, Sánchez Granados G. [Effects of an exercise and relaxation aquatic program in patients with spondyloarthritis: a randomized trial]. Medicina Clínica. 2015;145(9):380–384. Spanish. | ||
Ribeiro F, Leite M, Silva F, Sousa O. [Physical exercise in the treatment of Ankylosing Spondylitis: a systematic review]. Acta Reumatol Port. 2007;32(2):129–137. Portuguese. | ||
Wilson F, Walshe M, O’Dwyer T, Bennett K, Mockler D, Bleakley C. Exercise, orthoses and splinting for treating Achilles tendinopathy: a systematic review with meta-analysis. Br J Sports Med. 2018;52(24):1564–1574. | ||
Thompson JV, Saini SS, Reb CW, Daniel JN. Diagnosis and management of plantar fasciitis. J Am Osteopath Assoc. 2014;114(12):900–906. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.