")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 16
Enhancement of Adherence to Therapeutic and Lifestyle Recommendations Among Hemodialysis Patients: An Umbrella Review of Interventional Strategies
Authors Zhianfar L, Nadrian H , Shaghaghi A
Received 26 November 2019
Accepted for publication 21 March 2020
Published 6 April 2020 Volume 2020:16 Pages 233—243
DOI https://doi.org/10.2147/TCRM.S240125
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Leila Zhianfar,1 Haidar Nadrian,2 Abdolreza Shaghaghi1
1Health Education & Promotion Department, Faculty of Health, Tabriz University of Medical Sciences, Tabriz, Iran; 2Social Determinants of Health Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
Correspondence: Abdolreza Shaghaghi
Health Education & Promotion Department, Faculty of Health, Tabriz University of Medical Sciences, Golgasht Ave., Tabriz, Iran
Tel +98 41 33376227
Email [email protected]
Objective: To systematically retrieve and condense the best possible evidence on the successful interventions that targeted enhancement of therapeutic and lifestyle recommendations adherence in hemodialysis patients (HDPs).
Design: An umbrella review of interventional studies.
Data Sources: A comprehensive search of the Cochrane Database of Systematic Reviews, Ovid, PubMed, Scopus, EMBASE and Web of science databases to identify relevant publications in 2000– 2018 (June) timeframe.
Study Selection: Two reviewers independently applied inclusion criteria to select potential systematic reviews assessing the successful interventions that targeted enhancement of therapeutic and lifestyle recommendations adherence in HDPs. Data were summarized for information about the first author(s)’ names, year of publication, type(s) of the intervention and output variables, main findings and also the applied quality appraisal tools in the retrieved research evidence.
Data Extraction: Eligible studies were selected and data were extracted independently by two reviewers. The Joanna Briggs Institute (JBI)’s critical appraisal tool for systematic reviews was used to assess the quality of the identified publications, and discrepancies were resolved by consensus with a third reviewer.
Data Synthesis: Thirteen systematic reviews (12 solely systematic reviews and 1 systematic review with meta-analyses) were eligible to be enrolled in the study. The range of interventions that had been reported to boost therapeutic and lifestyle recommendations adherence in HDPs’ included psycho-educational programs, physical activity enhancement initiatives, information technology (IT)-based interventions and aromatherapy. Depression, diet biomarkers and interdialytic weight gain (IDWG) were among the myriad of output variables that had been measured as proxies to assess impacts of the implemented interventions. Psycho-educational interventions were among the prevalent initiatives to boost therapeutic and lifestyle recommendations adherence among the HDPs.
Conclusion: This umbrella review revealed that various intervention approaches and strategies can be used for HDPs’ better therapeutic and lifestyle recommendations adherence with considerable methodological heterogeneity. The pinpointed research evidence is also supporting application of multifaceted interventional modalities to reach an improved acquiescence form the patients’ side and their families. Further studies are recommended to address the interactions across various interventions in discordant socio-cultural contexts.
Keywords: hemodialysis, intervention, adherence, psychosocial, cognitive, exercise
Introduction
More than 2 million patients are undergoing hemodialysis worldwide as a result of mostly life-style related chronic conditions that cause kidney failure including type 2 diabetes, hypertension and Atherosclerotic Reno Vascular Disease (ARVD).1 Hemodialysis is one of the life-supporting renal replacement therapies (RRT) for patients suffering from an absence of effective kidney function or kidney failure to remove wastes and extra fluid and also balance important minerals such as potassium, sodium, and calcium in the patients’ blood. HDPs require blood dialysis for 4 h, 3 times a week as a standard protocol to remove toxic waste metabolites in their blood. The procedure could pose restrictions in patients’ everyday life, e.g., limitations in fluid and food intake which in turn could exacerbate their vulnerability to other health conditions such as hampered intestinal transit and its consequent complications.
The patients inevitably should have numerous alterations and adjustments in the daily life routines to fit into the rhythm of the dialysis sessions. Considering the required dietary change (restriction in salt, phosphorus, potassium, and fluid contents of diet) and plenty of medications HDPs should take, non-adherence to the prescribed dietary change and medications are common among the patients.2–4 Successful management of chronic conditions require immense impetus from the patients' side, their families and also care givers.5 Dietary and medication non-adherence in HDPs could cause serious negative consequences including poor health outcomes and increased morbidity and mortality.6 Several precipitating factors were suggested to affect medical advice adherence including HDPs’ educational level and health literacy, their socio-economic status, presence of multiple co-morbidities,7 complexities of the medication regimen and inadequate education of the HDPs about the prescribed life-style change or medicines.8–10
To empower patients with chronic disorders several educational interventions were designed and implemented throughout the world to enhance the patients’ knowledge or psychological preparedness for maintaining the recommended changes or adherence to prescribed medications.11–13 The experiences were similarly successful in changing the HDPs’ beliefs, their health-related behaviors and improving adherence to the recommended diet and medications.12,13
Due to heterogeneity of the studies and presentation of their results, this umbrella review was conducted according to the recommended protocol of Joanna Briggs Institute (JBI)14 to retrieve and condense the best possible evidence on the successful interventions that targeted the HDPs’ therapeutic regimens of adherence improvement.
Materials and Methods
Literature Search
A comprehensive search of the Cochrane Database of Systematic Reviews, Ovid, PubMed, Scopus, EMBASE and Web of science databases was carried out to identify relevant publications in the 2000–2018 (June) timeframe. A conclusive combination of keywords related to three main headings of hemodialysis, intervention and adherence (as listed in Appendix 1) was utilized to retrieve the congruous publications.
The title and abstract screenings were performed independently by the two members of the research team (LZH, ASH) to reduce probability of identification/selection bias and all discrepancies were discussed and adjudicated by the senior author (ASH). Full texts of the supposedly admissible research reports were obtained and assessed for relevance against the pre-determined inclusion/exclusion criteria and any disagreements were mitigated by a third reviewer (HN).
Eligibility Criteria and Data Extraction
All systematic reviews with or without meta-analyses that examined effectiveness of the conducted interventions to enhance therapeutic and lifestyle recommendations adherence with definite health outcomes in diet, dialysis, fluid restriction and medications dimensions as proxy measures to clinical outcomes and QOL in HDPs were eligible to be included in this study. A broad range of psycho-educational interventions or their combinations individual or group-based interventions, interdisciplinary versus multidisciplinary Interventions and also information technology (IT) assisted interventions were considered for inclusion.
Those reviews that have been conducted on pediatric patients (<18y); the reviews that assessed impacts of pharmacological interventions; non-English publications; narrative literature reviews; studies on only Peritoneal Dialysis (PD); reviews of qualitative studies and reviews of economic evaluation studies were all excluded in this study. A complete list of retrieved publications is provided in Table 1.
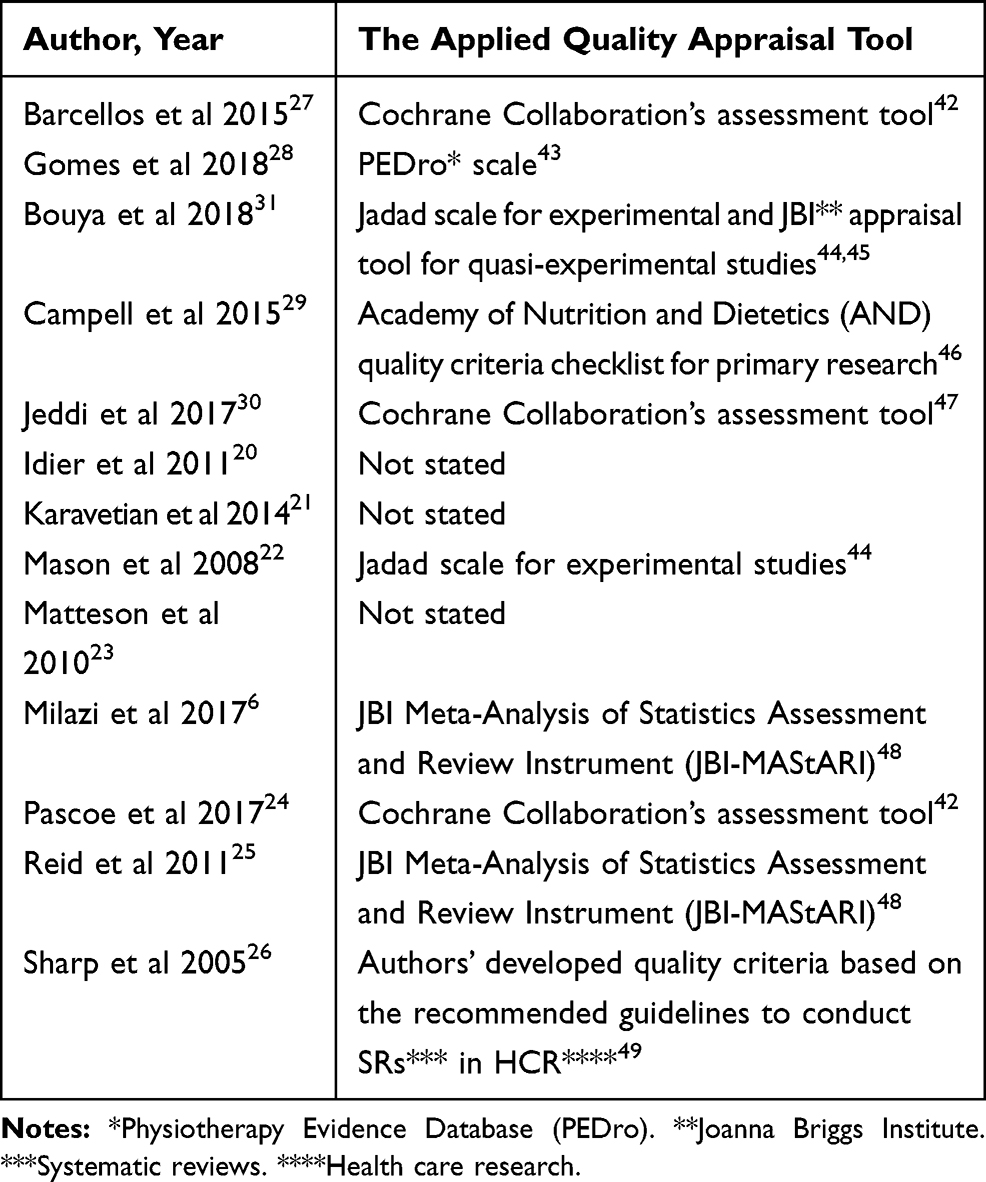 |
Table 1 The Utilized Quality Appraisal Tools in the Retrieved Systematic Reviews of Interventions to Enhance Therapeutic and Lifestyle Recommendations Adherence Among Hemodialysis Patients. |
Information about the first author(s)’ name and family name in the identified publications, year of publication, type(s) of the intervention, number of the included studies, the number of participants, main findings and also quality of the research evidence (using the JBI checklist for systematic reviews)15 were extracted independently by the two members of the research team (LZH and ASH) and any disagreement was resolved by consensus.
Quality of the Systematic Reviews
The methodological quality appraisal of the identified relevant publications was performed by the two authors (LZH, ASH) based on the JBI15 critical appraisal tool for systematic reviews and discrepancies were resolved by consensus with a third reviewer (HN). The reviews that had all 11 criteria of the JBI checklist15 were categorized as publications with high quality, those that had criteria of the 1–3 and concurrently criteria of the 5–8 in addition to at least one of the criteria of 9–11 from the JBI checklist were classified as having admissible quality group. Those publications that lacked the specified quality criteria of this study were excluded. But considering the JBI’s broader view of what constitutes research evidence for practice, and its developed unique levels of evidence and grades of recommendation,16 all included publications with high and admissible quality will be categorized in the “strong” level of evidence. The selected reports based on the ranking, however, must be looked upon as the likely best available evidence, and should not be used as a definitive measure of the best available evidence.16
Statistical Analysis of the Systematic Reviews or Meta-Analyses
Data synthesis of the retrieved systematic reviews of therapeutic and lifestyle intervention strategies will involve comparison of the outcomes, aggregation and categorization of the qualitative evidence on the basis of similarity in the implemented interventions and their contrastive outcomes. The intended statistical data pooling procedure for the quantitative outcome measures will include calculation of the Higgins I2 statistic17 for testing the retrieved studies’ findings for heterogeneity. Based on the test results a fixed or random effect model will be employed to estimate the interventions’ effect size using the professional version of the Comprehensive Meta-Analysis (CMA) software.18
Results
Literature Review
The primary search of the literature retrieved 727 publications. After removing duplicates in overlapped databases, non-relevant and incompatible reports (based on the inclusion/exclusion criteria) 45 publications remained for further scrutiny and after their full-text screening only 13 study reports were identified as having the intended eligibility criteria, including 12 solely systematic reviews and 1 systematic review with meta-analyses. The utilized quality appraisal tools in the retrieved systematic reviews were tabulated in Table 1. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram19 was used to summarize process of the studies selection (Figure 1).
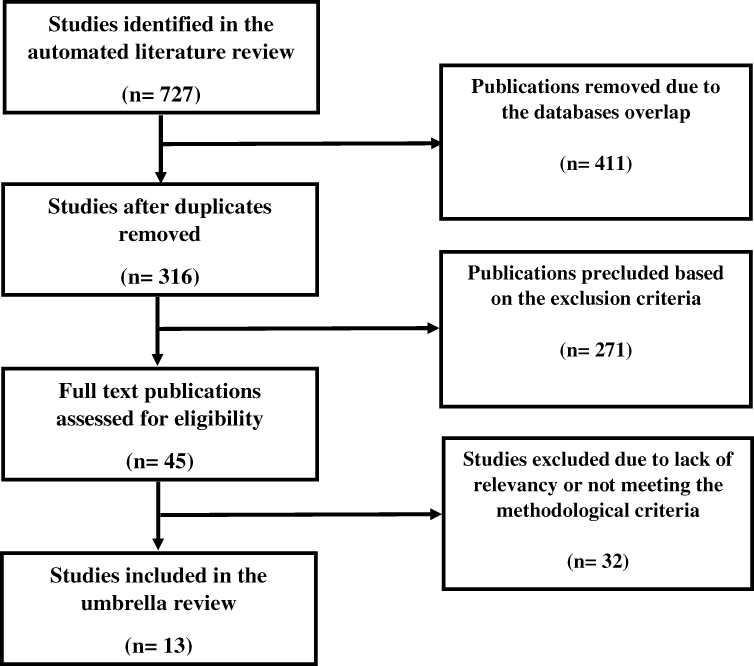 |
Figure 1 The PRISMA flow diagram of the publications screening process in the umbrella review of interventional studies* to enhance therapeutic and lifestyle recommendations adherence among hemodialysis patients. Notes: * The identified publications in the literature review included: Cochrane Database of Systematic Reviews (n= 66), OVID (n= 135), PubMed (n= 120), Scopus (n= 96), EMBASE (n= 161) and Web of Science (n= 149). |
Findings from Systematic Review with/Without Meta-Analysis
The range of interventions that had been reported in this group of systematic reviews to boost therapeutic and lifestyle recommendations adherence in the hemodialysis patients included psycho-educational (in 8 publications),6,20-26 physical activity enhancement (in 2 systematic reviews27,28 with recommended home and HD center-based aerobic, resistance and low-intensity strength training before or during HD sessions, home-based cycling and walking, stretching, Hatha yoga exercise in the included studies of the systematic review conducted by Barcellos et al27 and intradialytic exercise training in the systematic review of the Gomes Neto et al),28 IT platform-based intervention (in 2 studies)29,30 and aromatherapy in another systematic review study.31 None of the included publications had all the 11 quality criteria of the JBI checklist.15 Four study reports20,23,27,29 had only 8 quality criteria, 4 other studies21,24-26 had 9 quality criteria and 5 publications6,22,28,30,31 had 10 quality criteria of the checklist that were categorized in the “likely best available evidence” group of studies.16 The retrieved research evidence about the effectiveness of the different interventions to reinforce therapeutic and lifestyle recommendations adherence among HDPs was tabulated in Table 2. Objectives of the included studies, types of the applied interventions and the outcome measures that have been utilized to assess the mediatory impacts of the implemented interventional initiatives on diet, spectrum of the dialysis behavior, fluid restriction and prescribed medications adherence as proxy dimensions of an improved clinical outcome and QOL in HDPs were summarized in Table 3.
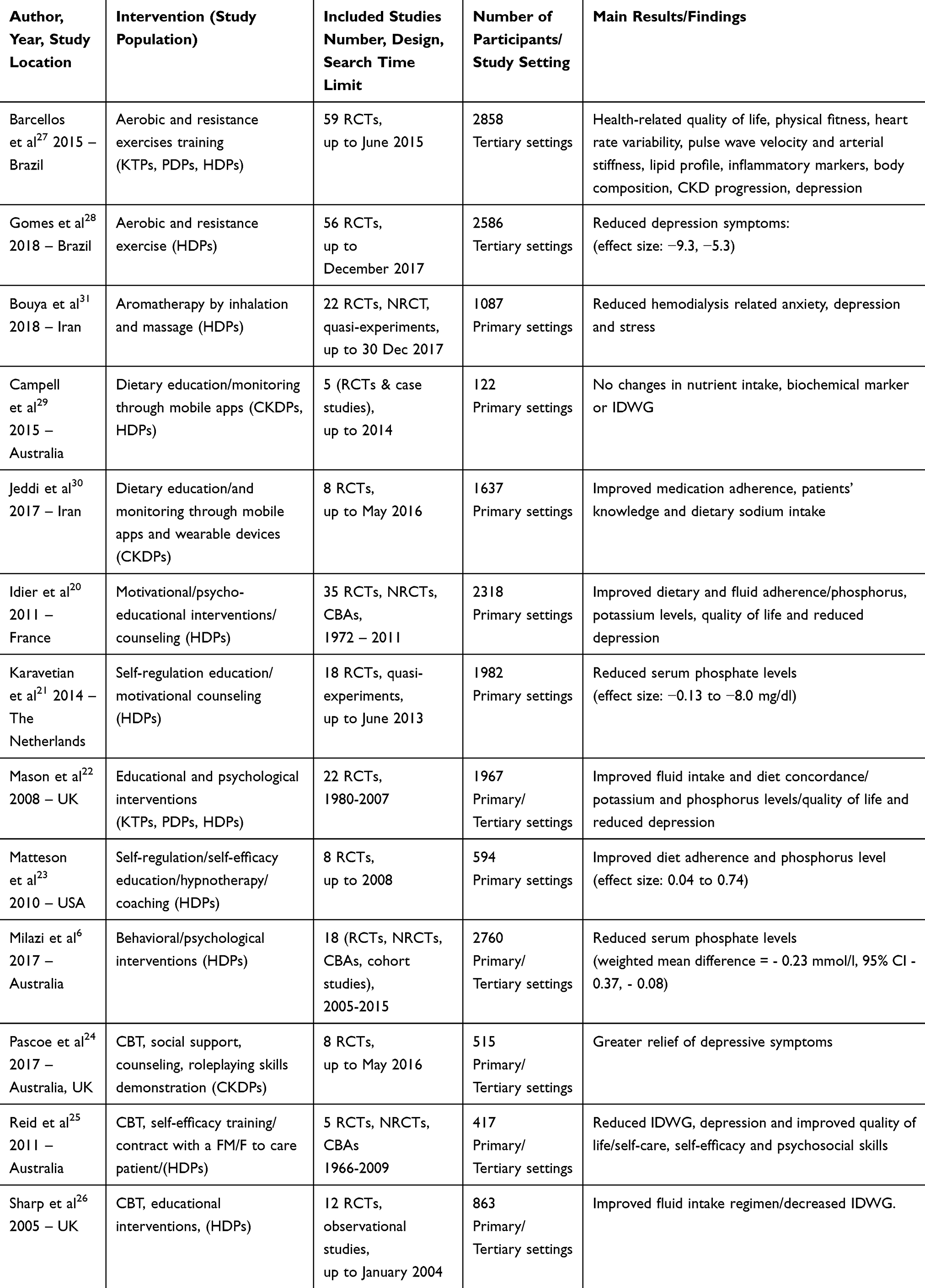 |
Table 2 List of the Retrieved Publications that Reported Interventions to Enhance Therapeutic and Lifestyle Recommendations Adherence Among Hemodialysis Patients. |
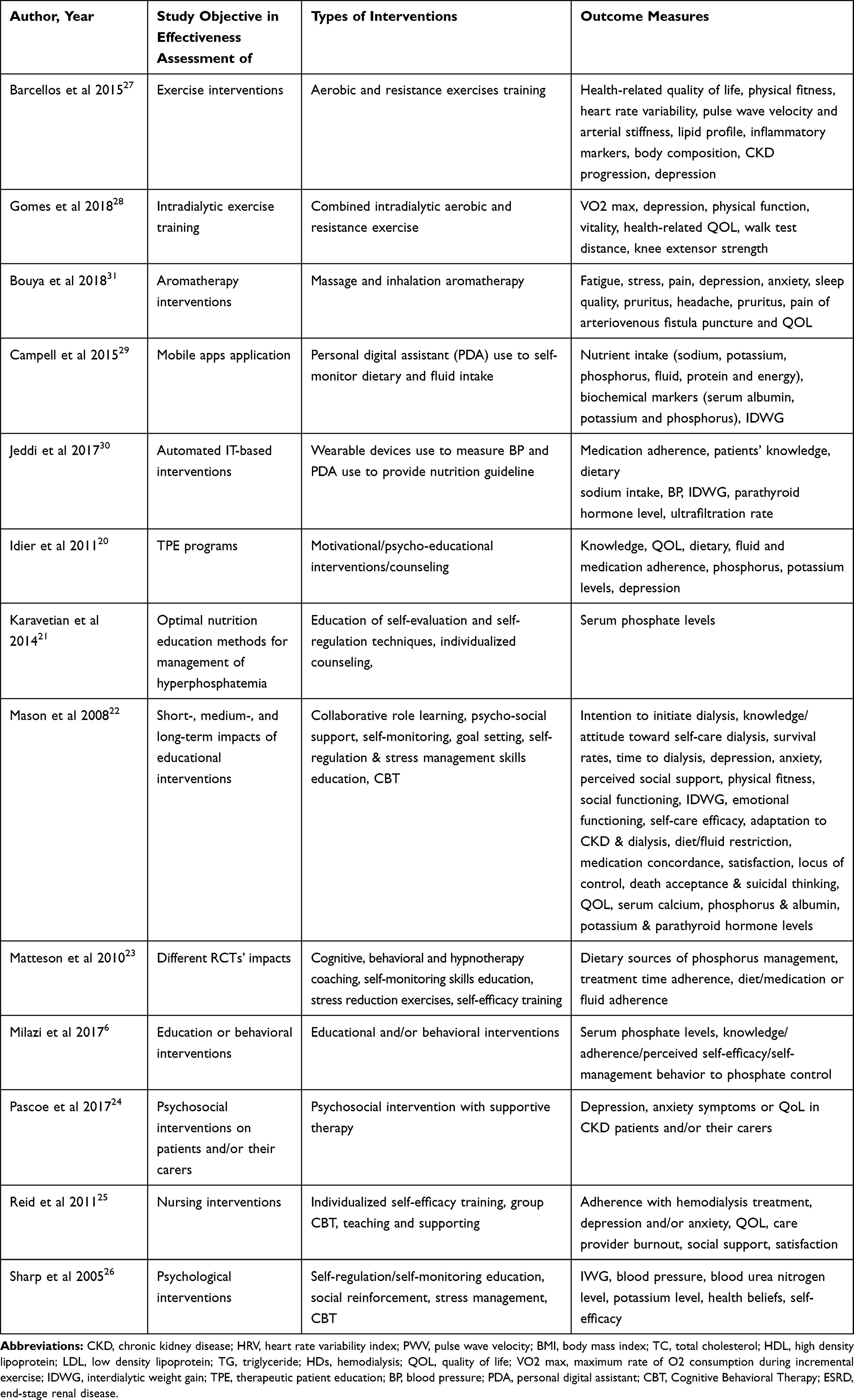 |
Table 3 The Objectives, Types of Interventions and Outcome Measures in the Retrieved Systematic Reviews of Interventions to Enhance Therapeutic and Lifestyle Recommendations Adherence Among Hemodialysis Patients. |
The Reported Achievement(s) in the Psycho-Educational Interventions
The various intervention approaches identified in the studies are as follows: educational interventions6,20,24 to enhance patients’ knowledge, self-care and self-management skills based on the constructs of the behavioral cognitive theory,18,21-26 trans-theoretical model of change,26 self-regulation model19,21 and social cognitive theory20 as well as the psychosocial interventions including counseling,20,22 application of motivational techniques20,21 and social support23,25 as explained in the self-efficacy theory.22,25 The findings revealed that dietary/fluid intake adherence and important biomarkers level (i.e., phosphorus or potassium levels etc.) in line with other clinical feature (i.e., IDWG) and most importantly the perceived quality of life could be improved by the successful implementation of the psycho-educational interventions. For instance in the study by Matteson et al23 the baseline adherence to the therapeutic regimens of adherence was reported to be improved from 33% to 54.1%. A significant reduction in the serum phosphorus level was reported in the study by Karavetian et al (variation of reduction was from 0.3 mg/dl to 1.6 mg/dl).21 Meta-analysis of the eight RCTs for serum phosphate control was also pinpointed the mean reduction of −0.23 mmol/l in the study of Milazi et al.6
The Reported Achievement(s) in the Physical Activity Improvement Interventions
Combined aerobic and resistance exercise (both during dialysis and in separate sessions) were suggested in the identified publications to alleviate the depression symptoms in the HDPs and in consequence meliorate the health-related quality of life.27,28 Depression scores of the HDPs were assessed in four RCTs (using the Beck Depression Inventory [BDI]), in three of them aerobic exercises and in one study aerobic plus resistance exercises were endorsed. The cumulative findings of the studies revealed that aerobic exercises could reduce depression scores of the HD patients by 30–40% and application of combined aerobic and resistance exercises may reduce significantly the depression symptoms (−7.3; 95% CI −9.3, −5.3; N = 88).
The Reported Achievement(s) in the Information Technology-Based Interventions
The IT-based interventions refer to use of Internet, local area networks (LANs) and mobile devices (personal digital assistants [PDAs], smartphones etc.) in delivery of disease-related services or information due to their noticeable feasibility of application and efficiency in embracing positive outcomes. The study by Campbell et al29 found that installation of dietary mobile applications on PDAs for dietary improvement and sending information about sound dietary habits for HD patients indicated no significant improvement in the nutrients intake. However, in the other IT-based intervention30 that used smartphones/PDAs, wearable devices, computerized systems and multiple digital components for providing information and counseling about positive and protective behaviors for HDPs, remarkable improvements in 75% of the clinical outcomes (e.g., IDWG, ultrafiltration rate, BP) and 86% of the process of care or outcomes (e.g., medication adherence, dietary sodium intake, etc., as the proxies to clinical outcomes) were observed.
The Reported Achievement(s) in the Aromatherapy Interventions
The systematic review conducted by Bouya et al31 suggested that aromatherapy could reduce some of the prevalent complaints of the HDPs, including anxiety, stress, depression, etc. According to the reported findings of the included studies inhalation of the essences of lavender and damask rose oils could reduce the severity of depression in HDPs.
Discussion
No gold standard intervention was identified in this umbrella review for boosting adherence to therapeutic regimens in the HDPs. Four main categories of interventions were reported (psycho-educational, physical activity, IT-based and aromatherapy interventions) to have direct effects on therapeutic and hygiene–dietary regimens adherence of HDPs and reduction of their complaints and also indirect effect on their conformity with the prescribed medication or lifestyle recommendations.
Psycho-educational interventions were among the most prevalent suggested interventions to reinforce adherence to the therapeutic and other lifestyle recommendations in HDPs.6,20,26 Based on the retrieved scientific literature proper application of cognitive/behavioral strategies in planning interventional programs for HDPs could target the patients’ abilities for better management of their health conditions with extrusive bio–psychological outcomes. The psycho-educational approach that was employed in the conducted studies is compatible with the World Health Organization (WHO)’s recommended Therapeutic Patient Education (TPE) program.32 The TPE was aimed to help patients in acquiring and maintaining the skills they need in management of their life with a chronic disease in the best possible way. The recommended constituents of the TPE include: 1) Presence of a psychologist in a multidisciplinary team that consists different professions, i.e., nurse, dietician, pharmacist or physician for the patients’ skills development to achieve better adherence; 2) Merging collective and individual oriented practices to obtain more beneficial effects compared to application of single approach; 3) Combination of biological/clinical outcomes (objective measure) and psychosocial criteria (subjective measure) in evaluation of interventions that target therapeutic and lifestyle recommendations adherence’s improvement; and 4) Continuous follow up of not only the short-term effects but also the medium- and long-term effects of the interventions, since some of the achievements might be at risk with time.32
Self-management capacity of the HDPs could enable these patients to take better care of themselves and enable knowledgeable decision-making about their well-being.33
The psychological status of patients (e.g., mild or severe depression) with chronic conditions was also suggested to exert negative impact on their therapeutic regimens adherence and illness behavior.34–36 Empirical research evidence exists to suggest the importance of physical exercise as a non-pharmacological means of reducing depressive symptoms among healthy and non-healthy individuals.37,38
Supervised exercising has been suggested to improve exercise capacity, muscular strength, and QOL in HDPs and reduce their depression symptoms.37–40 The main un-answered question that requires further scrutiny however is to find feasible strategies for encouragement of depressed HDPs to participate in physical exercise programs.
The use of IT-based technologies to help dietary self-monitoring of HDPs, and therefore to improve IDWG and dietary biomarkers, were recommended based on the findings of two systematic reviews.27,28 Technology use may help health care providers (HCPs) to encourage better dietary adherence for instance by sending a daily dietary short message (SMS) to HDPs. Access to smartphone applications could help HCPs when monitoring HDPs’ self-management behaviors and skills. The current pace of worldwide digital technology expansion prompts further investment on planning IT-based interventions for improved therapeutic adherence among patients with chronic diseases.
The small sample sizes in the study29 caused statistically insignificant variations in medication adherence or biomarkers of better self-management when IT-based interventions were applied. Further studies are needed with larger sample sizes to examine the beneficial effects of IT-based interventions in relation to other types of interventions in different subgroups of HDPs with diverse age structure, socio-economic background, and literacy level.
Aromatherapy as an alternative approach to ameliorate the HDPs’ complaints was assessed in another systematic review.31 Regarding the direct and indirect effects of the anxiety, stress and depression on HDPs’ health and willingness to adhere to the prescribed medications, application of the aromatherapy could be considered as a complimentary intervention. The procedure is inexpensive and its application is feasible in many countries. The main methodological limitation in the study of aromatherapy for improved therapeutic regimens adherence was the variety of aromas and their varied dose of application that makes accurate assessment of the procedure application on the other HDPs cumbersome. Overall safety and effectiveness of the applied aromas is also required to be assessed in future studies.
Blended patient-centered education and psychosocial support strategy was suggested to better improve all dimensions of the therapeutic and lifestyle recommendations adherence in terms of prescribed medications, diet, dialysis and fluid restriction as proxy measures of the dialysis clinical outcome and perceived quality of life (QOL) according to the endorsed new quality paradigm41 of care provision for HDPs.
Limitations of the Umbrella Review
This review has a number of methodological limitations, therefore the results must be interpreted with caution due to the inconsistent methodological quality of the included studies. First, because of the observed heterogeneity mainly in the intervention protocols, outcome measures and study designs of the included studies, it was not rational nor ingenious to quantitatively pool their findings in a meta-analysis. Validities of the quantitatively reported outputs in the included systematic reviews for calculation of point estimates were circumscribed due to the applied different investigative designs and intervention protocols with high susceptibility of bias. So the research team preferred to give an augmented summary of findings. Second, the inherent variation in the included studies’ design might cast (RCT, pre-post intervention etc.) prominent imprecision on the findings. Small studies’ effects, probable measurement, selection, detection and attrition biases in the retrieved research and logistic or methodological limitations in control of these potential biases are other limitations of this study. Last, despite efforts being made to identify all relevant publications, the probability of selection bias due to limiting the conducted search outputs to publications that have been written in English language, for instance (language bias), not considering search for grey literature or hand searching (publication bias) and also paucity of key terms used to search the literature (searching bias) should not be ruled out completely.
Conclusion
This umbrella review indicated that various intervention approaches and strategies can be used for HDPs' better therapeutic and lifestyle recommendation adherence with considerable methodological heterogeneity. The pinpointed research evidence also supports the application of multifaceted interventional modalities to reach an improved acquiescence from the patients and their families. Further studies are recommended to address the interactions across various interventions in discordant socio-cultural contexts. Explicit explanations of intervention protocols and sticking to standard reporting protocols in future research would help the understanding of the contextual appropriateness of different interventions and their outputs in terms of HDPs’ better therapeutic and lifestyle recommendations adherence.
Ethics and Informed Consent Statements
This article was prepared based on the findings of a research project that had been conducted for partial fulfilment of the requirements to obtain a PhD degree by the first author (LZH). This study was approved by the Medical Ethics Board of Trustees (MEBoT) (approval number: IR.TBZMED.REC.1397.425) affiliated to the Tabriz University of Medical Sciences.
Funding
This research was supported partially by Tabriz University of Medical Sciences (grant number: 5-D-193090- 1397-06-10).
Disclosure
Professor Abdolreza Shaghaghi reports grants from Tabriz University of Medical Sciences, outside the submitted work. The authors report no conflicts of interest in conducting this review and reporting its findings.
References
1. Liyanage T, Ninomiya T, Jha V, et al. Worldwide access to treatment for end-stage kidney disease: a systematic review. Lancet. 2015;385(9981):1975–1982. doi:10.1016/S0140-6736(14)61601-9
2. Bleyer AJ, Hylander B, Sudo H, et al. An international study of patient compliance with hemodialysis. JAMA. 1999;281(13):1211–1213. doi:10.1001/jama.281.13.1211
3. Hecking E, Bragg-Gresham JL, Rayner HC, et al. Haemodialysis prescription, adherence and nutritional indicators in five European countries: results from the Dialysis Outcomes and Practice Patterns Study (DOPPS). Nephrol Dial Transplant. 2004;19(1):100–107. doi:10.1093/ndt/gfg418
4. Saran R, Bragg-Gresham JL, Rayner HC, et al. Nonadherence in hemodialysis: associations with mortality, hospitalization, and practice patterns in the DOPPS. Kidney Int. 2003;64(1):254–262. doi:10.1046/j.1523-1755.2003.00064.x
5. Curtin RB, Mapes DL. Health care management strategies of long-term dialysis survivors. Nephrol Nurs J. 2001;28(4):385–394.
6. Milazi M, Bonner A, Douglas C. Effectiveness of educational or behavioral interventions on adherence to phosphate control in adults receiving hemodialysis: a systematic review. JBI Database System Rev Implement Rep. 2017;15(4):971–1010. doi:10.11124/JBISRIR-2017-003360
7. Collinson A, McMullan M, Tse WY, et al. Managing serum phosphate in haemodialysis patients: time for an innovative approach? Eur J Clin Nutr. 2014;68(3):392–396. doi:10.1038/ejcn.2013.283
8. San Miguel S, Curtale M, Knagge D, et al. Improving patient understanding of phosphate binders: a bony challenge. Ren Soc Aust J. 2009;5(3):119–125.
9. Sandlin K, Bennett PN, Ockerby C, et al. The impact of nurse-led education on haemodialysis patients’ phosphate binder medication adherence. J Ren Care. 2013;39(1):12–18. doi:10.1111/j.1755-6686.2013.00343.x
10. Rifkin DE, Laws MB, Rao M, et al. Medication adherence behavior and priorities among older adults with CKD: a semistructured interview study. Am J Kidney Dis. 2010;56(3):439–446. doi:10.1053/j.ajkd.2010.04.021
11. Lorig KR, Sobel DS, Stewart AL, et al. Evidence suggesting that a chronic disease self-management program can improve health status while reducing hospitalization: a randomized trial. Med Care. 1999;37(1):5–14. doi:10.1097/00005650-199901000-00003
12. Shi YX, Fan XY, Han HJ, et al. Effectiveness of a nurse-led intensive educational programme on chronic kidney failure patients with hyperphosphataemia: randomised controlled trial. J Clin Nurs. 2013;22(7–8):1189–1197. doi:10.1111/jocn.12159
13. Van Camp YP, Huybrechts SA, Van Rompaey B, et al. Nurse-led education and counselling to enhance adherence to phosphate binders. J Clin Nurs. 2012;21(9–10):1304–1313. doi:10.1111/j.1365-2702.2011.03967.x
14. Aromataris E, Fernandez R, Godfrey C, et al. Methodology for JBI Umbrella Reviews. Joanna Briggs Institute Reviewers’ Manual: 2014 Edition. Australia: The Joanna Briggs Institute; 2014:1–34.
15. The Joanna Briggs Institute. Critical appraisal tools for use in JBI systematic reviews: checklist for systematic reviews and research syntheses. 2017. Available from: https://joannabriggs.org/sites/default/files/2019-05/JBI_Critical_Appraisal-Checklist_for_Systematic_Reviews2017_0.pdf.
16. The Joanna Briggs Institute Levels of Evidence and Grades of Recommendation Working Party. Supporting Document for the Joanna Briggs Institute Levels of Evidence and Grades of Recommendation. The Joanna Briggs Institute; 2014. Available from https://joannabriggs.org/sites/default/files/2019-05/JBI%20Levels%20of%20Evidence%20Supporting%20Documents-v2.pdf.
17. Borenstein M, Hedges LV, Higgins JPT, et al. Introduction to Meta-Analysis. Chichester (UK): Wiley; 2009. doi:10.1002/9780470743386
18. Borenstein M, Hedges LV, Higgins JPT, et al. Comprehensive Meta-Analysis Version 3. Englewood, NJ (USA): Biostat; 2013.
19. Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. doi:10.1371/journal.pmed.1000097
20. Idier L, Untas A, Koleck M, et al. Assessment and effects of therapeutic patient education for patients in hemodialysis: a systematic review. Int J Nurs Stud. 2011;48(12):1570–1586. doi:10.1016/j.ijnurstu.2011.08.006
21. Karavetian M, de Vries N, Rizk R, et al. Dietary educational interventions for management of hyperphosphatemia in hemodialysis patients: a systematic review and meta-analysis. Nutr Rev. 2014;72(7):471–482. doi:10.1111/nure.12115
22. Mason J, Khunti K, Stone M, et al. Educational interventions in kidney disease care: a systematic review of randomized trials. Am J Kidney Dis. 2008;51(6):933–951. doi:10.1053/j.ajkd.2008.01.024
23. Matteson ML, Russell C. Interventions to improve hemodialysis adherence: a systematic review of randomized-controlled trials. Hemodial Int. 2010;14(4):370–382. doi:10.1111/j.1542-4758.2010.00462.x
24. Pascoe MC, Thompson DR, Castle DJ, et al. Psychosocial interventions for depressive and anxiety symptoms in individuals with chronic kidney disease: systematic review and meta-analysis. Front Psychol. 2017;8:992. doi:10.3389/fpsyg.2017.00992
25. Reid C, Hall J, Boys J, et al. Self management of haemodialysis for end stage enal disease: a systematic review. JBI Libr Syst Rev. 2011;9(3):69–103. doi:10.11124/01938924-201109030-00001
26. Sharp J, Wild MR, Gumley AI. A systematic review of psychological interventions for the treatment of nonadherence to fluid-intake restrictions in people receiving hemodialysis. Am J Kidney Dis. 2005;45(1):15–27. doi:10.1053/j.ajkd.2004.09.010
27. Barcellos FC, Santos IS, Umpierre D, et al. Effects of exercise in the whole spectrum of chronic kidney disease: a systematic review. Clin Kidney J. 2015;8(6):753–765. doi:10.1093/ckj/sfv099
28. Gomes Neto M, de Lacerda FFR, Lopes AA, et al. Intradialytic exercise training modalities on physical functioning and health-related quality of life in patients undergoing maintenance hemodialysis: systematic review and meta-analysis. Clin Rehabil. 2018;32(9):1189–1202. doi:10.1177/0269215518760380
29. Campbell J, Porter J. Dietary mobile apps and their effect on nutritional indicators in chronic renal disease: a systematic review. Nephrology (Carlton). 2015;20(10):744–751. doi:10.1111/nep.12500
30. Jeddi FR, Nabovati E, Amirazodi S. Features and effects of information technology-based interventions to improve self-management in chronic kidney disease patients: a systematic review of the literature. J Med Syst. 2017;41(11):170. doi:10.1007/s10916-017-0820-6
31. Bouya S, Ahmadidarehsima S, Badakhsh M, et al. Effect of aromatherapy interventions on hemodialysis complications: a systematic review. Complement Ther Clin Pract. 2018;32:130–138. doi:10.1016/j.ctcp.2018.06.008
32. World |Health Organization. Therapeutic Patient Education: Continuing Education Programmes for Health Care Providers in the Field of Prevention of Chronic Diseases: Report of a WHO Working Group. Copenhagen: World Health Organization: Regional Office for Europe; 1998. Availabe from: https://apps.who.int/iris/handle/10665/108151.
33. Richard CJ. Self-care management in adults undergoing hemodialysis. Nephrol Nurs J. 2006;33(4):
34. Fava GA, Cosci F, Sonino N. Current psychosomatic practice. Psychother Psychosom. 2017;86(1):13–30. doi:10.1159/000448856
35. Pu J, Jiang ZH, Wu W, et al. Efficacy and safety of intradialytic exercise in haemodialysis patients: a systematic review and meta-analysis. BMJ Open. 2019;9(1):e020633. doi:10.1136/bmjopen-2017-020633
36. Rhee SY, Song JK, Hong SC, et al. Intradialytic exercise improves physical function and reduces intradialytic hypotension and depression in hemodialysis patients. Korean J Intern Med. 2019;34(3):588–598. doi:10.3904/kjim.2017.020
37. Catalan-Matamoros D, Gomez-Conesa A, Stubbs B, et al. Exercise improves depressive symptoms in older adults: an umbrella review of systematic reviews and meta-analyses. Psychiatry Res. 2016;244:202–209. doi:10.1016/j.psychres.2016.07.028
38. Baggetta R, D’Arrigo G, Torino C, et al. Effect of a home based, low intensity, physical exercise program in older adults dialysis patients: a secondary analysis of the EXCITE trial. BMC Geriatr. 2018;18:248. doi:10.1186/s12877-018-0938-5
39. Groussard C, Rouchon-Isnard M, Coutard C, et al. Beneficial effects of an intradialytic cycling training program in patients with end-stage kidney disease. Appl Physiol Nutr Metab. 2015;40(6):550–556. doi:10.1139/apnm-2014-0357
40. Chen JL, Godfrey S, Ng TT, et al. Effect of intradialytic, low-intensity strength training on functional capacity in adult haemodialysis patients: a randomized pilot trial. Nephrol Dial Transplant. 2010;25(6):1936–1943. doi:10.1093/ndt/gfp739
41. Nissenson AR. Improving outcomes for ESRD patients: shifting the quality paradigm. Clin J Am Soc Nephrol. 2014;9(2):430–434. doi:10.2215/CJN.05980613
42. Verhagen AP, de Vet HCW, de Bie RA, et al. The Delphi list: a criteria list for quality assessment of randomized clinical trials for conducting systematic reviews developed by Delphi consensus. J Clin Epidemiol. 1998;51(12):1235–1241. doi:10.1016/S0895-4356(98)00131-0
43. Maher CG, Sherrington C, Herbert RD, et al. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. 2003;83(8):713–721. doi:10.1093/ptj/83.8.713
44. Jadad AR, Moore RA, Carroll D, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Contr Clin Trials. 1996;17(1):1–12. doi:10.1016/0197-2456(95)00134-4
45. Tufanaru C, Munn Z, Aromataris E, Campbell J, Hopp L. Chapter 3: systematic reviews of effectiveness. In: Aromataris E, Munn Z, editors. Joanna Briggs Institute Reviewer’s Manual. The Joanna Briggs Institute; 2017. Available from: https://reviewersmanual.joannabriggs.org/.
46. Academy of Nutrition and Dietetics. Evidence Analysis Manual: Steps in the Academy Evidence Analysis Process. Chicago, USA: Academy of Nutrition and Dietetics; 2012.
47. Higgins JPT, Green S (Eds.). Cochrane handbook for systematic reviews of interventions version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from: www.handbook.cochrane.org.
48. The Joanna Briggs Institute (JBI). Joanna Briggs Institute Reviewers’ Manual: 2014 Edition/Supplement. Australia: The University of Adelaide; 2014. Available from: https://nursing.lsuhsc.edu/JBI/docs/ReviewersManuals/Mixed-Methods.pdf.
49. Khan KS, Kunz R, Kleijnen J, Antes G. Systematic Reviews to Support Evidence-Based Medicine: How to Review and Apply Findings of Healthcare Research. UK, Royal Society of Medicine: Oxford; 2003.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.