")
Back to Journals » Patient Preference and Adherence » Volume 13
Engaging patients and informal caregivers to improve safety and facilitate person- and family-centered care during transitions from hospital to home – a qualitative descriptive study
Authors Backman C , Cho-Young D
Received 10 January 2019
Accepted for publication 5 March 2019
Published 26 April 2019 Volume 2019:13 Pages 617—626
DOI https://doi.org/10.2147/PPA.S201054
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Chantal Backman,1–3 Danielle Cho-Young1
1School of Nursing, Faculty of Health Sciences, University of Ottawa, Ottawa, ON, Canada; 2Ottawa Hospital Research Institute, Ottawa, ON, Canada; 3Bruyère Research Institute, Ottawa, ON, Canada
Purpose: The purpose was to describe patients and informal caregivers’ perspectives on how to improve and monitor care during transitions from hospital to home as part of a larger research study to prioritize the components that most influence the development of successful care transition interventions.
Methods: We conducted a qualitative descriptive study between July and August 2016, during which time semi-structured telephone interviews (n=8) were completed with patients and informal caregivers across select Canadian provinces. Interviews were audio-recorded, transcribed and thematically analyzed.
Results: Main themes included: the need for effective communication between providers and patients and informal caregivers; the need for improving key aspects of the discharge process; and increasing patients and informal caregivers involvement in care practices. Participants also provided suggestions on how to best monitor care transitions.
Conclusion: This study highlighted the following strategies with patients and informal caregivers: focus on effective communication regarding important information; provide appropriate resources; and increase involvement. Future research is needed to incorporate the input from patients and informal caregivers into the design and implementation of care transition interventions.
Keywords: care transitions, patient engagement, patient safety, person- and family-centered care
Background
Care transitions are described as the transfer of a patient between different settings and health care providers during the course of an acute or chronic illness.1 Care transitions are significant as they can often lead to fragmented care, decreased quality of care, and an increase in adverse events.2–5 These “vulnerable exchange points” may also contribute to high rates of health services and health care costs,6 which is often the case since care transitions from hospital to home continue to be poorly managed and pose a high risk for harm.2–5 Challenges associated with care transitions are complex and thus require a multifaceted approach and coordinated care to improve quality and health outcomes.7,8 Ensuring a high level of person- and family-centered care (PFCC) is one particularly important aspect for improving quality and health outcomes during care transitions.9–11
Person- and-family-centered care (PFCC) focuses on the unique individual as a “whole person” and not just their illness or disease.12 The components of person- and family-centered care include holistic care, collaborative care, and responsive care.13 This approach to care encompasses the individual’s own experience of health, family, culture and community.14 It focuses on improving the autonomy of the individual to make healthcare decisions and to improve their overall healthcare experience.12
In the last decade, there have been major strides toward person- and family-centered care at all levels of the health system including a multitude of provincially funded initiatives as well as provincial legislation.12 Central to person- and family-centered care is the engagement of patients and their informal caregivers.15 Patient engagement can range from consultation, to involvement, all the way up to partnership and shared leadership.15 Engaging patients and informal caregivers is crucial to improving the health and experiences of patients, specifically during these “vulnerable exchange points.” The purpose of this study was to describe patients’ and informal caregivers’ perspectives on how to improve and monitor care during transitions from hospital to home as part of a larger research study to prioritize the components that most influence the development of successful care transition interventions.16
Methods
Research design and methodology
A qualitative descriptive study17 was conducted using semi-structured telephone interviews. We chose to conduct interviews over the telephone because we were seeking input from patients and informal caregivers across the country. Ethics approval including the verbal consent process was obtained from the University of Ottawa Research Ethics Board. We used the Standards for Reporting Qualitative Research (SRQR) checklist when writing the report on our study findings.18
Research team
The research team has expertise on care transitions (CB) and qualitative research methods (CB, DCY). The primary researcher (CB) is an affiliate investigator at the Ottawa Hospital Research Institute and at Bruyère Research Institute. Two patient partners (KKB and LH) helped with the design and pilot of the interview guide.
Sampling and recruitment
Using convenience sampling, patients and informal caregivers were contacted by email through the Patients for Patient Safety Canada members list, and were asked to participate in a semi-structured telephone interview. Patients for Patient Safety Canada is a national patient-led program of the Canadian Patient Safety Institute with an aim to help improve patient safety.19 Three reminder recruitment emails were sent at approximately 3-week intervals. Patient and informal caregivers interested in participating were instructed to contact the research assistant (JR).
The inclusion criteria were individuals: 65 years or older, admitted and discharged from the hospital to home with the last 90 days, able to communicate in English, and not cognitively impaired. Family members who were at least 18 years of age or older were also invited.
Data collection tools and methods
Following pilot testing of the interview guide, a trained research assistant (JR) conducted 45 to 60- minute audio-recorded semi-structured telephone interviews with patients and informal caregivers (Appendix A: Semi-structured telephone interview questions). The research assistant (JR) arranged a time that was most convenient for the telephone interview. Prior to the start of the interview, the research assistant read the information sheet, and obtained verbal consent. Participants were informed of the researcher’s research background and professional affiliation, and noted that the purpose of the interview was to engage in a general discussion and obtain their perspective on how care transitions could be improved.
Data analysis
A thematic analysis19 was used to extract key themes from all the transcripts. Two researchers (CB and DCY) independently reviewed and coded each transcript. The individual analyses were then collectively reviewed by the team members, looking for similarities between the transcripts and using an iterative process until consensus was obtained on the coding (code book) and the core themes were determined.20 Themes were derived from the data with ATLAS.ti software21 used to manage the qualitative data and support the thematic analysis. Researchers (CB and DCY) kept a journal to record any personal thoughts and information related to the data analysis. Participants were not provided final transcripts for comment or asked to provide feedback on the findings.
Results
A total of eight (n=8) study participants were recruited between July and August 2016. Nine individuals (n=9) were interested in participating, however one individual was excluded (n=1) because they did not meet all of the inclusion criteria. The characteristics of the participants are found in Table 1.
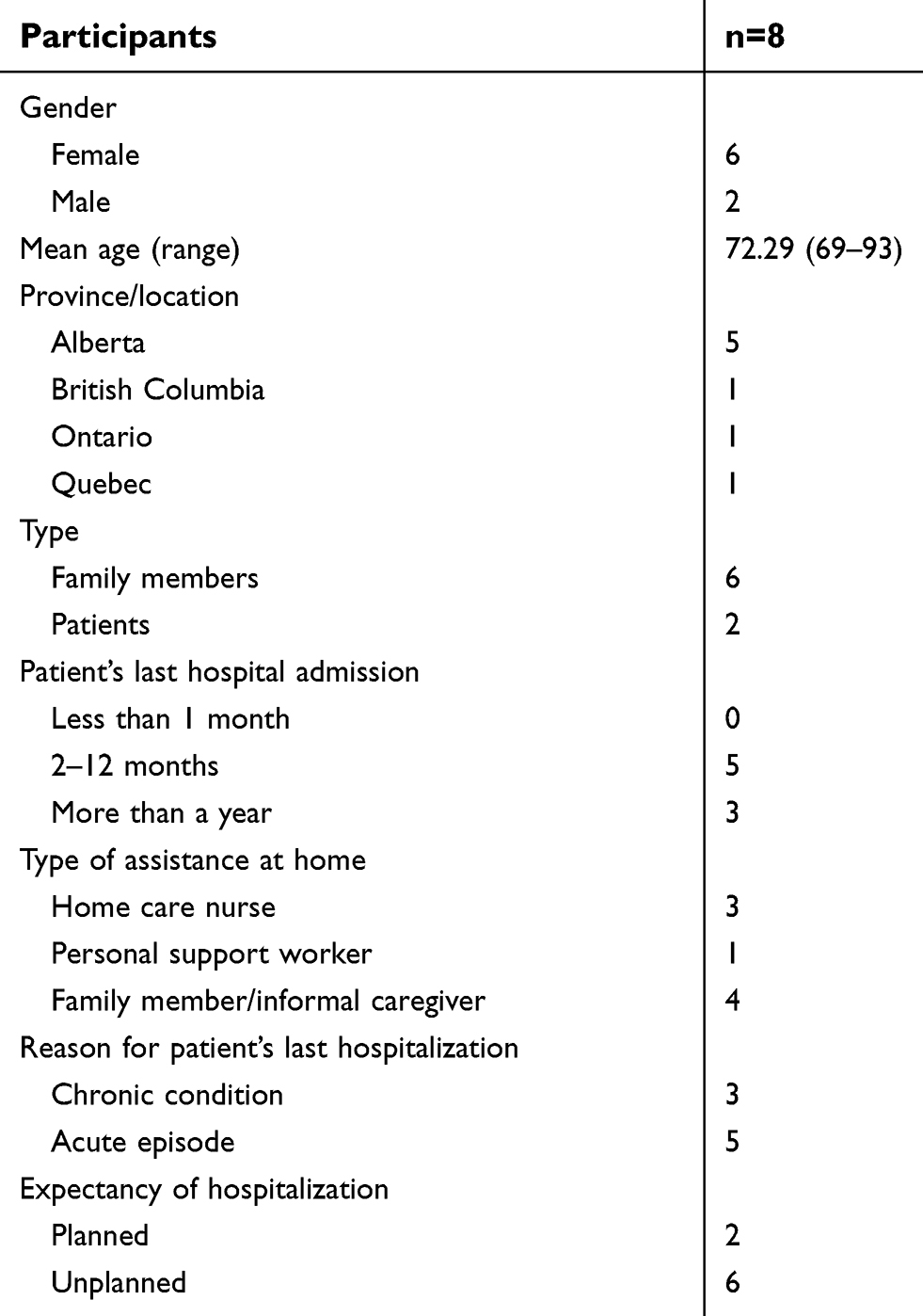 | Table 1 Participant characteristics |
Patients and their informal caregivers described their perceptions of various aspects related to care transitions from hospital to home. The main themes that emerged included: 1) the need for effective communication between providers and patients/informal caregivers, 2) the need for improving key aspects of the discharge process, 3) increasing patient and family involvement and 4) suggestions on how to best monitor care transitions.
Theme 1: need for effective communication between providers and patients/informal caregivers
Under this theme, participants described examples of successful communication between health care providers and patients and their informal caregivers and also described their experiences with lack of effective communication. Participants also made suggestions to improve communication between providers across health care sectors.
Successful communication between health care providers and patients and their informal caregivers
Participants explained that it was easy to communicate to the health care providers and that the health care providers were supportive during the discharge planning process. Participants felt that the discharge planning process was well communicated, with one of those commenting on the inclusivity of the process, Caregiver 3 explained that:
“…there was a meeting with the physician in charge of that ward, the nurse that was the care nurse on the ward, and somebody from the homecare organization and, the two of us. And that meeting was in a special room. It was totally open and free with any sort of questions being asked and being answered. It was a very good meeting. I was also clear on what was going to happen after that because of that meeting…”
Several participants also commented on their experiences with supportive health care providers, either prior to discharge or once at home. Caregiver 6 said:
“The infection specialist gave me his home phone number even and said, you know, if you get any more trouble, get on the phone. Which I did once.”
Caregiver 5 also commented,
“…at least [at] the pharmacy… there was a wonderful staff lady who whenever he had any issues or any questions about his medicine or not feeling all right, he would call her and she would help him and she would also want to talk to the family, i.e., his wife, and if his adult children were near around them.”
Despite these positive experiences, some participants also noted poor communication between health care providers and patients/informal caregivers, specifically between one level of care to another.
Poor communication between health care providers and patients/informal caregivers
Participants expressed their concerns with the lack of information received as they transitioned from one setting to another. For example, Caregiver 4 said:
“The patient- and family-centered care in an acute care facility…, you know, was excellent. But the connection into the next level of care not so excellent.”
Furthermore, participants also noted limited communication with regards to making referrals to other health care providers and follow-up appointments. Caregiver 6 explained:
“There was no follow-up or anything. It was just, you know, we fixed you, out you go. You’ve got a GP. You’ve got your specialists.”
Suggested recommendations to improve communication between providers across health care sectors
Participants described the need for a better approach to communicate the care needs between the hospital and home care providers. Patient 7 recommended:
“They [health care providers] should be in contact with the community to let them know the person is going and what they’re going to need. They should be asking the patient if they’re by themselves, if they have food in the fridge, if they’re able to make food. If they can get up by themselves at night without falling. If they have a urinal if it’s a man. If they need a bar on the bed to help them get up or a pole. If the shower is safe, if they have a bath mat.”
Caregiver 2 emphasized the importance of arranging a follow-up appointment prior to discharge from hospital.
Other suggestions included a scheduled discharge conference call or an electronic communication with the community home care agency or family physician. For example, Caregiver 1 suggested that:
“her change in medication, the new prescription, should have been transmitted directly to her community pharmacy and her GP. As well as given to her, but it should have been transmitted… I’m going to use the word electronically, and you decide whether that’s by fax, by email, or whatever, but should have been transmitted directly to the pharmacy and her GP, both of whom were known to the people doing the discharge.”
Theme 2: need for improving key aspects of the discharge process
Participants felt that the coordination of care at discharge was not very flexible and that it was not very patient and family centered. Participants described the need to improve some aspects of the discharge process. This included the lack of notice of discharge date, the paucity of patient/family teaching, gaps in follow-up care, and limited accessibility to community resources.
Lack of notice of discharge date
Some participants did not receive appropriate notice about the discharge date and time. For example, Caregiver 6 described:
“…I went to visit her in the morning and she was so relieved that I got there because she was being discharged. Like she had been discharged. I mean she was still in her bed, but, you know, she was waiting for me to come and pick her up to take her home.”
Paucity of patient/family teaching
Participants described examples of lack of adequate patient and family teaching. Specifically, a participant commented on diabetes management education. Caregiver 6 described that he was not aware of the potential complications after his family member was discharged, which was detrimental to the patient’s overall outcome:
“But if they’d just explained what the potential complications of urinary tract infections are, and what symptoms to look out for, and how urgent it is to get people back into hospital, you know, I would have reacted much faster simply because I would have known what was a probable cause of her symptoms and how desperately urgent it is to get them treated straight away to improve your chances of survival.”
Another participant, Caregiver 2 also described her experience with poor teaching,
“she didn’t know if she [patient] was supposed to be taking medication or not, as an example. There was relatively short notice for her departure. So, you know, they [my family] live an hour from there and I live an hour from there and it was sort of just scrambling to get there and she [patient] just called. I’m done. I can go.”
Another gap was the lack of specific instructions at discharge. For example, Caregiver 3 described how he only learnt about taking care of his wife’s condition after discharge:
“Well I found that mostly out of the internet.” “…I think we know what we need to know. You don’t know what you don’t know.”
Gaps in follow-up care
Participants described gaps in their follow-up care. Specifically, Patient 8 described an administrative error that occurred during the referral process:
“I had one physician who said he would, you know, put through a referral…and then that never really happened so that kind of left a few loose ends hanging two weeks later when we kind of wondered why we never got a call back.”
Caregiver 6 described an example of information that was missed during the discharge process:
“The issue was, you know, lacking the education to know that if certain symptoms demonstrated themselves, that where to go and how urgent it was.”
Another participant commented on the lack of discussion around follow-up care and support once discharged. Patient 7 explained:
“…so I was sent home and there was no one at home because my husband was also in the hospital. And fortunately, my daughter came to the rescue. We were glad she was available and able to do that, but nobody asked if she was.”
Accessibility to resources
One participant was denied access to home care resources since there was already some support from a family member. Caregiver 6 explained the shortage of resources available for patients once discharged:
“they said they just didn’t have the resources to help people, that they were overstretched just in terms of helping people alone at home to cope and so, you know, they couldn’t help me.”
Patient 7 noted the long wait time before her husband, who was also a patient in this instance, could gain access to physiotherapy in the community:
“My husband… I thought that I had everything organized for him..he was supposed to have physio and that wasn’t even ordered at that time, at the time of his discharge. And he’s slid back considerably.”
Suggested recommendations to improve key aspects of the discharge process
Participants suggested that resources be organized and that all discharge information be provided while the patients are still in the hospital. Patient 7 recommended:
“I think that the homecare should… visit you in the hospital. And it should be all set up before you go home. There shouldn’t be any surprises. The physio appointment should be made in the hospital so that you know when you’re next going for physio. And all the equipment be ordered and in place or picked up.”
Another participant, Patient 8 emphazised that all the discharge information should be provided:
“I think if you have any questions. I think if you have any symptoms that you are concerned about, that you know, are out of the ordinary. I think also when is that patient’s next appointment with a physician or a healthcare professional because I think a lot of times people are discharged and they don’t know when to see a GP or they don’t know if they need to. Not that they all need to, but I think it’s important to have…let them know a date. Kind of like what’s the next step to kind of their recovery process.”
Participants also suggested the importance of written information to help supplement the verbal instructions. Caregiver 1 described the lack of written information as one of the biggest problems:
“…if you’re going to change someone’s diet, you should leave some documentation with them, and rather than saying… and this was sort of the immediate change… and rather than saying do you understand or do you accept what I’m telling you, you should say what do you understand, because in my brother-in-law’s case, he was a very proud man, and when someone asked him do you understand, the only thing he’s going to say is yes. He’s never going to say no, I don’t understand, because… and he understood the language but he didn’t understand the meaning in the words.”..“Documentation is probably the biggest problem that I see as it relates to discharge.”
Caregiver 2 also explained the need for more written information:
“I would say, you know, communication in terms of more information about when she comes home, what to look for, not just a verbal, you know, they provided her with a verbal, you know, look for this, look for that, but there was nobody there with her. So, you know, hearing her say something when she’s sick, she might not remember it all. So, you know, I would say some kind of written documentation.”
Another participant, Patient 8 explained:
“Like I really think like any handout they can give, a phone number, like especially if there… you know like in 24 hours if you have any major questions.”
Theme 3: increasing patient and family involvement
Some family members showed their active involvement in the care of their loved one throughout their transition. In all of these cases this was demonstrated through their extensive knowledge about the patient’s health condition(s), and in some instances where they acted as advocates for the patient. Participants also commented on negative aspects of their own and/or family member’s care transition, and the need to increase patient and family involvement.
Family as an advocate for the patient
One family member described that his wife was experiencing abnormal symptoms, and questioned a diagnosis based on his baseline knowledge of the patient’s condition. This example not only demonstrated his expertise on the patient’s baseline condition(s) but is also an example of a family member using their leadership skills and acting as an advocate for the patient.
Caregiver 6:
“…but I did question it and I actually wrote down her symptoms on paper for the doctors, and I did point out that until sort of late August she was as sharp as a razor mentally and it seemed to me from what I knew about dementia that it seemed to be a very rapid onset because normally, although I do understand now because I’ve researched this since she died, that sometimes Alzheimer’s can come on very quickly, but it’s normally a very slow process.”
Caregiver 3 also commented that:
“you have to get to know how the system works and you have to get to know what is available.”
Family presence
Patient 8 described the importance of family presence, and involvement in the discussions:
“Like myself, either my husband or a family member is present for any important teaching or important information.”
Caregiver 2 said:
“The second set of ears is a really big key to safe transitions.”
Lack of patient and family involvement
Participants also commented on the lack of patient and family involvement. Caregiver 1 described:
“… she [patient] has problems and they discharged her on her own without asking for a family member to be part of the discharge process.” “I think there needs to be more emphasis, for lack of a better word, on their family [patient family] being involved with them [patient] so as to ensure that what they are told is followed, for lack of a better word.”
Another participant, Caregiver 4 said:
“The family weren’t even allowed to, you know, assist in the decision…” and described that “…as those patients get older, you know, the family…the involvement of the family should be greater not less. So the communication to the family GP that serves those care facilities, you know, needs to be bumped up a little bit.” “And I, you know, where patients want the family to be involved and want the communication back to the family, there’s got to be a way to do that. You know, I don’t know whether it’s email or if the physicians are really, you know, can’t make those follow-up phone calls but just to be available to informal caregivers so that everyone’s on the same page. My husband always has to chase the physician down and that’s not always easy.”
Theme 4: suggestions on how to best monitor care transitions
Participants made suggestions on how to monitor care transitions whether they are successful or not. This included identifying a central person to facilitate the transitions, and the development of a detailed discharge protocol with a follow-up survey.
Identifying a central person to facilitate the transitions
Participants highlighted the need for one central person to be their designated contact, to ensure that they have all the required discharge information.
Caregiver 6 explained:
“there is no gatekeeper to ensure that when somebody is discharged from hospital all the steps that should be done to ensure a smooth transition are made. So several people, doctors, nurses, [home care staff], who can discharge somebody and they do discharge people, without knowing whether all these things have been done properly. And that horrifies me. And I’m sure that’s what happened to the lady I mentioned, that, you know, somebody discharged her without informing all these other bodies that were supposed to coordinate her home care. But, you know, I mean that should…obviously should never happen. There has to be one person who says either everything’s been done to ensure a smooth transition, or I’m not discharging this patient until it is done.”
Caregiver 4 proposed:
“… a care coordinator, you know, could be the hub of, you know, when…what the experience is going to be like, a central point of, you know, questions, concerns for patient and family while they’re there. As well as someone in that follow-up, you know, package that she should have gone home with would have been the contact information for that person once you’re back in your own [home]…”
Another participant, Caregiver 6 suggested monitoring the success of the transition by having a provider follow-up with each patient:
“the only way you find out if there’s something wrong with the transition is when the patient comes back, you know, either to the general practitioner or specialists, you know, as I did, as we did, with [wife] on a number of occasions.” or “the only way you could do that systematically I suppose is have some sort of social worker to just check up and see how you’re getting on.”
Caregiver 6 also suggested the need for a central person to meet the patients’ specific needs:
“…different patients have different needs. Some patients need…their appointments with whoever they need in follow-up after they’ve been discharged have been made for them and you know, for transportation to be arranged and, you know, a whole bunch of stuff but in our case, of course, we didn’t need that because I could just put her [patient] in the car and take her to whoever and I knew, you know, who her doctors were and so, you know, it varies from patient to patient but for sure I think there needs to be some sort of gatekeeper to make sure patients aren’t discharged before they’ve got adequate arrangements, whatever those arrangements are for them individually.”
A detailed discharged protocol with a follow-up survey
Participants also suggested how to monitor if the transition went well or not. Caregiver 5 proposed a discharge protocol:
that there is need for… a structured program like this pharmacy lady called [my brother] .. The moment the patient is discharged and all that, there is a [protocol in place]…that starts immediately. That today patient number 123 is going home. So every week, like the clinic was calling my brother for his upcoming appointment, they would call and they would find out. If everything is going well, that’s fantastic too, right. But if everything is not going well, it’ll be caught in time.
Another participant suggested a checklist with a follow-up survey. For example, Patient 7 proposed that a provider:
“Phone them and ask them. Or give them an evaluation to fill out” or “…with a follow-up. I mean lots of companies give you a follow-up to see if their service is adequate. Or again, they send them a survey to fill out, a brief survey. They could have a checklist for when patients go home that you can mark off all these things that they’re done.”
Patient 8 recommended that patients should have a follow-up from a discharge team:
“the nurse comes in the first 24 hours and I think if there was something wrong, we could…we could talk to that nurse and then they can relate back to our physician, relate it back to the discharging unit.” or “…the health care professionals need to have at least maybe a phone call follow-up or a number that the patient can call if they have any questions or concerns.” “It’s hard if they’re not… like if they’re not in a system, like a home care system. If they’re just a patient in, that’s been discharged. It’s kind of hard. But maybe if there was a way that you might ensure that you have the patient information, like contact numbers before you left the hospital and maybe if there was a follow-up team or a discharge team that made that quick phone call the next day to see. That could be a possibility in a perfect world.”
Discussion
The overall goal of the study was to obtain input from patients and informal caregivers on how to improve safety and facilitate person- and family-centered care during transitions from hospital to home. Engaging patients and their informal caregivers is an important strategy for examining care transitions practices in order to facilitate the development of innovative solutions for safer care transitions between hospital and home.
In this study, patients and informal caregivers described what was important to them during the transition between hospital and home. This included providing appropriate communication between providers and patients/informal caregivers, providing discharge teaching, and access to adequate resources needs, and empowering patients and informal caregivers in their care during the transition from hospital to home. Participants also noted the importance of a central person or a strong support system to help during this crucial phase. Person- and family-centered care requires a true partnership between the individual, their family and health care providers.12 A therapeutic relationship between these individuals helps achieve continuity of care (ie partnerships with the same health care providers) and shared decision-making.12 In addition, fostering effective communication, collaboration and respectful care that reflects the individual’s unique values, beliefs, culture, circumstances and changing health states are important.12 Furthermore, appropriate resources and support for caregivers22,23 as well as meaningful engagement of patients and informal caregivers during the transition24–26 are needed to improve safety and person- and family-centered care during the transition between hospital and home. In this study, patients and informal caregivers expressed that many of these aspects are needed in order for them to feel better prepared for discharge, and better equipped to manage their health condition(s) at home.
Findings are consistent with other research studies27–32 that have explored patient and family perspectives on care transitions and have suggested several approaches or strategies to improve care transitions. An initial strategy would be to focus on effective communications between providers and patients/informal caregivers. A second approach would be the provision of appropriate teaching and community resources. There is also a need to develop better methods for involving patients and informal caregivers and to create a strong support system that allows patients to safely move from hospital to home. These patients and informal caregivers’ perspectives were incorporated into the first round of a larger Delphi study aimed at identify the value statements that are perceived by health care decision-makers, patients and informal caregivers to best signify safe person- and family-centered care during transitions from hospital to home.16
Strengths and limitations
A primary limitation of this study was the small sample size and convenience sampling. We were limited in recruiting patients and informal caregivers from one organization (Patients for Patient Safety Canada19). With this convenience sampling, we may have missed some important perspectives from individuals who are not as actively involved in the healthcare system. However, key themes emerged from the interviews that are worth investigating further. Another limitation is that participants were self-selected; therefore, it is possible that some important factors were not identified in this study. That said, the results are broadly aligned with the findings of other researchers in this area.25,28–32
Conclusion
This study provided insight on patients and informal caregivers’ perceptions to improve and monitor care during transitions from hospital to home. Strategies to improve care transitions should focus on more effective communication to patients and informal caregivers regarding important information, providing them with appropriate resources, and increasing their involvement while they transition from hospital to home. Future research is needed to incorporate the input from patients and informal caregivers into the design and implementation of care transition interventions.
Ethics approval
Ethical approval was obtained from the University of Ottawa Research Ethics Board.
Provenance and peer review
This paper was not commissioned and was externally peer reviewed.
Data sharing statement
No additional data are available.
Acknowledgments
We would like to thank Janice Rudderham (JR) for her assistance in conducting the telephone interviews. We would also like to thank our two patient partners on the study team: Katharina Kovacs Burns (KKB) and Linda Hughes (LH) for their valuable contributions. This study was supported by a grant from the Canadian Patient Safety Institute, Accreditation Canada, the Canadian Home Care Association (CHCA), Patients for Patient Safety Canada (PFPSC), Patients Canada, and the Registered Nurses’ Association of Ontario (RNAO).
Author contributions
Both authors contributed toward data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Coleman EA. Falling through the cracks: challenges and opportunities for improving transitional care for persons with continuous complex care needs. J Am Geriatr Soc. 2003;51(4):549–555.
2. McMurray J, Hicks E, Johnson H, Elliott J, Byrne K, Stolee P. Trying to find information is like hating yourself every day: the collision of electronic information systems in transition with patients in transition. Health Informatics J. 2013;19(3):218–232. doi:10.1177/1460458212467547
3. Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138(3):161–167.
4. Kripalani S, LeFevre F, Phillips CO, Williams MV, Basaviah P, Baker DW. Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297(8):831–841. doi:10.1001/jama.297.8.831
5. Laugaland K, Aase K, Barach P. Interventions to improve patient safety in transitional care–a review of the evidence. Work. 2012;41(Supplement 1):2915–2924. doi:10.3233/WOR-2012-0544-2915
6. Naylor MD, Aiken LH, Kurtzman ET, Olds DM, Hirschman KB. The importance of transitional care in achieving health reform. Health Aff. 2011;30(4):746–754. doi:10.1377/hlthaff.2011.0041
7.
8. McDonald KM, Sundaram V, Bravata DM, et al. Care coordination. Closing Qual Gap. 2007;7:1–210.
9. Rhodes KV. Completing the play or dropping the ball? The case for comprehensive patient-centered discharge planning. JAMA Intern Med. 2013;173(18):1723–1724. pmid:23959515. doi:10.1001/jamainternmed.2013.2512
10. Cawthon C, Walia S, Osborn CY, Niesner KJ, Schnipper JL, Kripalani S. Improving care transitions: the patient perspective. J Health Commun. 2012;17(suppl3):312–324. pmid:23030579. doi:10.1080/10810730.2012.712619
11. Backman C, Chartrand J, Dingwall O, Shea B. Effectiveness of person- and family-centered care transition interventions: A systematic review protocol. BMC Syst Rev. 2017;6:158. doi:10.1186/s13643-017-0554-z
12.
13. Sidani S, Fox M. Patient-centered care: clarification of its specific elements to facilitate interprofessional care. J Interprof Care. 2014;28(2):134–141. doi:10.3109/13561820.2013.862519
14.
15. Carman KL, Dardess P, Maurer M, et al. Patient and family engagement: a framework for understanding the elements and developing interventions and policies. Health Aff. 2013;32(2):223–231. doi:10.1377/hlthaff.2012.1133
16. Backman C, Johnston S, Oelke ND, et al. Safe and effective person- and family-centered care practices during transitions from hospital to home—A web-based Delphi technique. PLoS One. 2019;14(1):e0211024. doi:10.1371/journal.pone.0211024
17. Sandelowski M. Focus on research methods-whatever happened to qualitative description? Res Nurs Health. 2000;23(4):334–340.
18. O’Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for reporting qualitative research: a synthesis of recommendations. Acad Med. 2014;89(9):1245–1251. doi:10.1097/ACM.0000000000000388
19.
20. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
21. Muhr T. ATLAS. Ti 8.0 [Version 8:]. Berlin, Germany: ATLAS. ti Scientific Software Development GmbH; 2018.
22. Schumacher K, Beck CA, Marren JM. Family caregivers: caring for older adults, working with their families. Am J Nurs. 2006;106(8):40–49.
23. Bauer M, Fitzgerald L, Haesler E, Manfrin M. Hospital discharge planning for frail older people and their family. Are we delivering best practice? A review of the evidence. J Clin Nurs. 2009;18(18):2539–2546. doi:10.1111/j.1365-2702.2008.02685.x
24.
25. Backman C, Stacey D, Crick M, Cho-Young D, Marck PB. Use of participatory visual narrative methods to explore older adults’ experiences of managing multiple chronic conditions during care transitions. BMC Health Serv Res. 2018;18:482. doi:10.1186/s12913-018-3292-6
26. Levine C, Halper D, Peist A, Gould DA. Bridging troubled waters: family caregivers, transitions, and long-term care. Health Aff. 2010;29(1):116–124. doi:10.1377/hlthaff.2009.0520
27. Allen J, Hutchinson A, Brown R, Livingston PM. Quality care outcomes following transitional care interventions for older people from hospital to home: a systematic review. BMC Health Serv Res. 2014;14:1–27. doi:10.1186/1472-6963-14-1
28. Allen J, Hutchinson AM, Brown R, Livingston PM, Experience U. Care integration in transitional care for older people from hospital to home. Qual Health Res. 2017;27(1):24–36. doi:10.1177/1049732316658267
29. Allen J, Hutchinson AM, Brown R, Livingston PM. User experience and care for older people transitioning from hospital to home: patients’ and carers’ perspectives. Health Expect. 2018;21(2):518–527. doi:10.1111/hex.12646
30. Hesselink G, Flink M, Olsson M, et al. Are patients discharged with care? A qualitative study of perceptions and experiences of patients, family members and care providers. BMJ Qual Saf. 2012;21:i39–i49. doi:10.1136/bmjqs-2012-001165
31. Flink M, Ekstedt M. Planning for the discharge, not for patient self-management at home - an observational and interview study of hospital discharge. Int J Integr Care. 2017;17(6):1. doi:10.5334/ijic.3003
32. Sims-Gould J, Stott-Eveneshen S, Fleig L, McAllister M, Ashe MC. Patient perspectives on engagement in recovery after hip fracture: a qualitative study. J Aging Res. 2017;2017:2171865. doi:10.1155/2017/2171865
Supplementary material
Appendix A. Semi-structured phone interview questions
CONTEXT QUESTIONS
- When was your (or your family member’s) last hospital admission?
- How often have you (or your family member) been hospitalized in the last 12 months?
- Do you have someone who helps you at home? What do they help you with? (Prompts: home care nurse, personal support worker, family member/informal caregiver, other)
- What was the reason for your (or your family member’s) last hospital admission? (Chronic condition, Acute episode); Was this planned or unplanned?
MAIN QUESTIONS
(Prompts: Who could help (specific health care provider or role) and how? When could they have helped (before you left, after you left, etc.)
For example:
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.