")
Back to Journals » International Journal of General Medicine » Volume 12
Engagement of Jordanian Physicians in Continuous Professional Development: Current Practices, Motivation, and Barriers
Authors Younes NA, AbuAlRub R, Alshraideh H, Abu-Helalah MA, Alhamss S, Qanno' O
Received 24 September 2019
Accepted for publication 20 November 2019
Published 24 December 2019 Volume 2019:12 Pages 475—483
DOI https://doi.org/10.2147/IJGM.S232248
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Nidal A Younes,1 Raeda AbuAlRub,2 Hussam Alshraideh,3,4 Munir A Abu-Helalah,5 Sohaib Alhamss,1 Omar Qanno’1
1Department of Surgery, Faculty of Medicine, University of Jordan, Amman, Jordan; 2Department of Community and Mental Health, Faculty of Nursing, Jordan University of Science and Technology, Irbid, Jordan; 3Industrial Engineering Department, Faculty of Engineering, Jordan University of Science and Technology, Irbid, Jordan; 4Industrial Engineering Department, American University of Sharjah, Sharjah, UAE; 5Department of Public Health, Faculty of Medicine, Mutah University, Alkarak, Jordan
Correspondence: Nidal A Younes Email [email protected]
Background: Mandatory relicense of all physicians in Jordan went into effect at the beginning of May 2018. The bylaw states that all physicians should engage in Continuing Professional Development (CPD) in order to upgrade their knowledge and maintain competency as a prerequisite to renew their license every 5 years. The characteristics of effective CPD are different from one country to another. Jordan has decided to link CPD to mandatory relicense; however, no research has been done to identify the factors that influence CPD offerings, needs, practices, experiences, and effectiveness in the healthcare sector in Jordan. This paper reviews the history of CPD and CME, and the different options to upgrade and improve the competence of physicians. It explores the current practices, motivation, and barriers for physicians to get engaged in CPD activities in Jordan.
Purpose: The purpose of this research was to provide a better understanding of the state of CPD in the healthcare sector in Jordan with a view to informing the development of Jordan’s first CPD framework. The findings of this research will provide policymakers with baseline information concerning current CPD practices, experiences, and attitudes of physicians towards CPD, and enablers and contributors to effective CPD in Jordan.
Methods: Stratified clustered self-selected participants that represented physicians working at all healthcare sectors in Jordan were used in this study. A structured pre-tested self-reported questionnaire was used to collect the data. A total of 457 physicians were included in the sample according to one-proportion sample size calculation method, and they were distributed among the healthcare sectors based on their shared proportions.
Conclusion: Despite considerable evidence supporting the role of CPD in maintaining competency of physicians, participating in CPD activities in Jordan is compromised by lack of mandatory laws and barriers related to staff shortage, heavy workload, limited funds, lack of time, and cost. Personal interests and career progression are the top motivators for CPD. Most Jordanian physicians are interested in CPD activities related to health/medical informatics and enhancing their skills in evidence-informed practice. We recommend that future interventions and health policy directions should be informed by these findings in order to optimize uptake of CPD programs in Jordan.
Keywords: continuing professional development, continuing medical education, CPD, CME, accreditation, re-license, Jordan
Introduction
The continuum of medical education in Jordan includes three distinct periods of learning: undergraduate, graduate and postgraduate (professional development). Each phase is characterized by transitions: basic to clinical, undergraduate to graduate (residency), and residency to postgraduate (practice).
It is widely accepted around the world that lifelong learning should be the main objective of medical education, it starts from medical schools and gets reinforced through the period of specialization during residency and fellowship programs up to final retirement days.1
Rapid explosion of medical knowledge and technology over the past decades has meant that it is increasingly challenging for practicing physicians to keep up with these advances as well as sustain and fine-tune and refresh the foundation knowledge acquired during their years of training. Research has shown that as time goes during years of practice, the clinical skills of physicians do decline.1,2 In addition, physicians are not reliable when it comes to diagnosing their own learning requirements.3 Taking a systematic approach to lifelong learning and regarding it as a foundational skill will benefit physicians as they transition from one stage to the other, and their practices evolve from being novice to becoming expert.4
Methodology
Research Purpose
The purpose of this research was to provide a better understanding of the state of CPD in the healthcare sector in Jordan with a view to informing the development of Jordan’s first CPD framework. The findings of this research will provide policymakers with baseline information concerning current CPD practices, experiences, and attitudes of physicians towards CPD, and enablers and contributors to effective CPD in Jordan.
Sample and Setting
Stratified clustered self-selected participants that represented physicians working at all healthcare sectors were used in this study. Physicians were clustered based on health sector and governorate. Healthcare sectors included in the study were the Jordanian Ministry of Health (MOH), the Jordanian Royal Medical Services (JRMS), University hospitals, private hospitals, and the United Nations for Relief and Works Agency (UNRWA). For analysis purposes, participants from UNRWA were merged with the participants from the private sector as their sample size was very small to be included in a separate group. Three governorates within Jordan: Irbid, Amman, and Al-Karak were used in the study. These governorates were chosen as they represent a good representative geographic cross section of Jordan: Irbid is in the North, Amman in the center and Al-Karak is further south. In addition, Al-Karak is rural while Amman and Irbid are urban centers. These areas were also chosen as each contains a reasonable mix of different health service providers.
Within a healthcare facility, physicians were asked to participate in the study. Given their participation approval, they have been asked to on-spot self-respond to the questionnaire. Completed questionnaires were collected directly once physicians were done with the answers. A total of 457 physicians were included in the sample according to one proportion sample size calculation method, and they were distributed among the healthcare sectors based on their share proportions.
Data Collection Tools
A structured pre-tested self-reported questionnaire adapted from previous studies (Alsharif & Al-Khaldi, 2001; Bower et al, 2008; Elshami et al, 2016; Shah et al, 2017)5–8 was used to collect the data. The questionnaire consisted of ten sections as follows:
- Section I: Demographic data;
- Section II: Current involvement in CPD activities
- Section III: Motivations to participate in CPD;
- Section IV: Attitudes towards CPD;
- Section V: Perceived benefits and impact of current CPD participation;
- Section VI: Perceived barriers to CPD participation;
- Section VII: CPD providers;
- Section VIII: Preferences for CPD design by activity type;
- Section IX: Views on the necessity of CPD; and
- Section X: CPD topic interests.
The questionnaire was validated by the Human Resources for Health 2030 (HRH2030) Research Advisory Group and was pilot-tested before data collection commenced.
Data Analysis
Data were analyzed using R statistical computing software (version 3.4.3). Descriptive analysis including means, frequencies and proportions was used to describe the sample, CPD needs, and perceived enablers, barriers, experiences, and attitudes of physicians towards CPD. For categorical responses, the chi-squared test was used to test for differences among healthcare sectors while ANOVA was used to test for differences for numerical responses. Binary logistic regressions combined with stepwise selection were used to identify significant predictors of involvement in research activities. A significance level of 0.05 was used throughout the analysis.
Ethical Approval Consideration
Approvals from the institutional review boards of the Jordan University of Science and Technology, the MOH, the JRMS, and targeted hospitals were granted before data collection commenced. Consent forms were obtained from all participants in the study.
Data Collection Procedures
Data collection commenced in December 2017 and was completed in April 2018. Participants were approached in their work settings through collaboration with their administrators to gain their approval to participate in the study.
Findings
Participant Demographics
This study included a total of 457 participants of which 375 (82.6%) were males and 79 (17.4%) were females. Of these participants 170 are working at the MOH, 174 are working in the private sector, 48 are from University hospitals, and 65 are working at the JRMS. Of all participants, 112 (24.5%) were from Irbid Governorate representing the Northern part of Jordan, 314 (68.7%) from Amman Governorate representing the Middle part of Jordan while 31 (6.8%) were from Al-Karak Governorate representing the Southern part of Jordan. These percentages were consistent with the reported statistics of the number of physicians working in these Governorates. Summary of participants’ demographic characteristics by healthcare sector is shown in Table 1. Participants’ average age was 34.42 years with a standard deviation of 9.45 years. An average year of experience of 8.35 years was observed for the participants with a standard deviation of 8.51 years. Participants from University hospitals had the highest average years of experience of 11.48 while participants from the JRMS had the lowest experience of 6.98 years. About 1.8% of all participants were divorces/widows while 41.6% were singles and 56.6% were married. Majority of the participants (66%) have a Bachelor degree, 15.1% have a Master’s degree, and18.9% have a PhD degree. About 46.9% of all participants are graduates from Jordan, 21.1% are graduates from other Arab countries, 24.2% are graduates from East Europe, 3.3% from West Europe, only 0.7% from USA, and the rest 3.7% are from other countries.
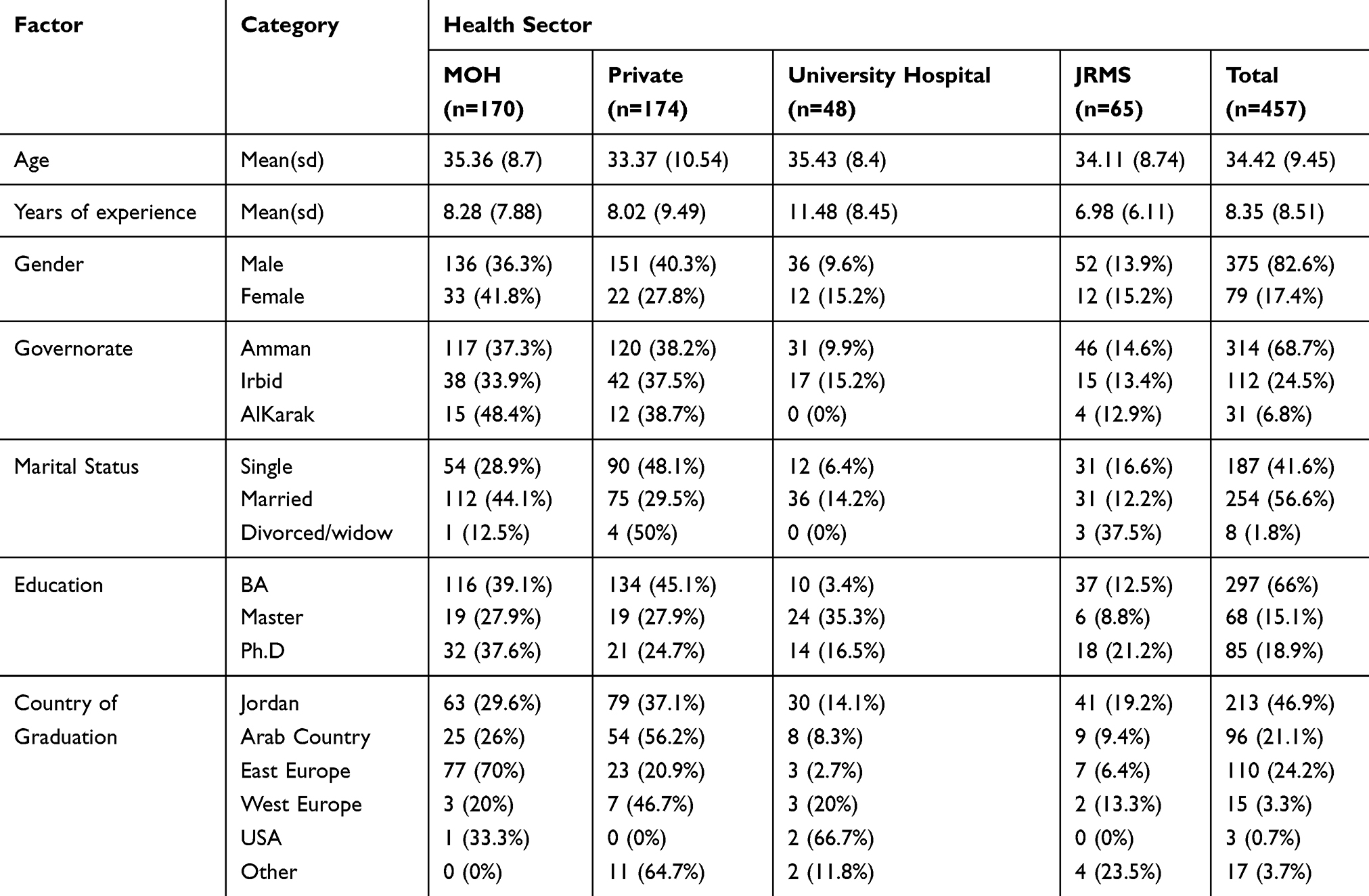 |
Table 1 Summary of Participants’ Demographic Characteristics |
Current CPD/CME Practices in Jordan
Figure 1 shows detailed summary of the current participants' activities related to CPD. As it can be seen in Figure 1, most physicians practice CPD in terms of attending conferences (80.7%), local seminars (79.8%) and training workshops (75.7%). Surprisingly, only 21.3% of all participants have published an article in the past two years and only 34.9% have participated in a research-related activity in the same period. Majority of participants know the latest guidelines related to their profession CPD (71.7%) but unfortunately, only 44.8% of all participants keep track of their CPD hours/points.
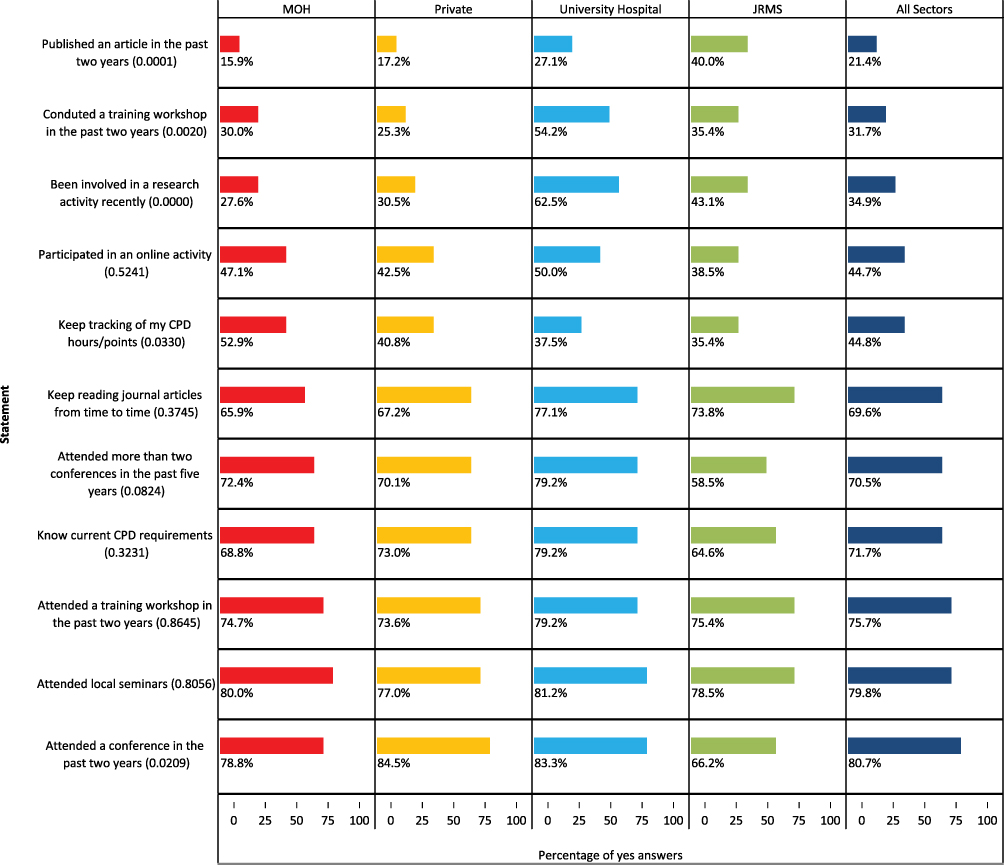 |
Figure 1 Summary of participants’ current CPD practices by health sector. Numbers in parentheses are the p-values for testing differences among participants from the different health sectors for each item. |
P-values used for testing significant differences among the participants from the different health sectors are also provided in Figure 1. These p-values indicate a significant difference in healthcare sectors in regards to publishing scientific articles and participating in research-related activities. Physicians from the JRMS had the highest participation rates in publishing research articles (40%) while physicians from University hospitals had the highest rate of being involved in research-related activities (62.5%).
Logistic regression analysis was used to identify predictors of current participation in CPD related activities. Model inputs were the demographic attributes of participants, and model outputs were the participants’ responses to each question about their current participation. Identified significant predictors of current participation in CPD related activities are provided in Table 2. Results indicate that marital status, education level, and health sector are significant predictors for both articles publishing and involvement in recent research activities. PhD holders had the highest articles publishing rate and involvement in research activities. Physicians from University hospitals had the highest involvement in research activities while those from the JRMS had the highest publication rate. Unfortunately, physicians from the private sector had the lowest publication and research involvement rates. Female participants have shown higher probability in publishing research articles than male participants. Participants with single marital status have shown lower rate of publishing articles than the married and widows/divorced participants. Regression results indicate a positive relationship between years of experience and publication of research articles, which entails that a higher probability of publication is expected for those with more experience. For involvement in research activities, divorced/widowed have shown the highest involvement probability followed by singles. Married participants have shown the lowest probability in involvement in research-related activities.
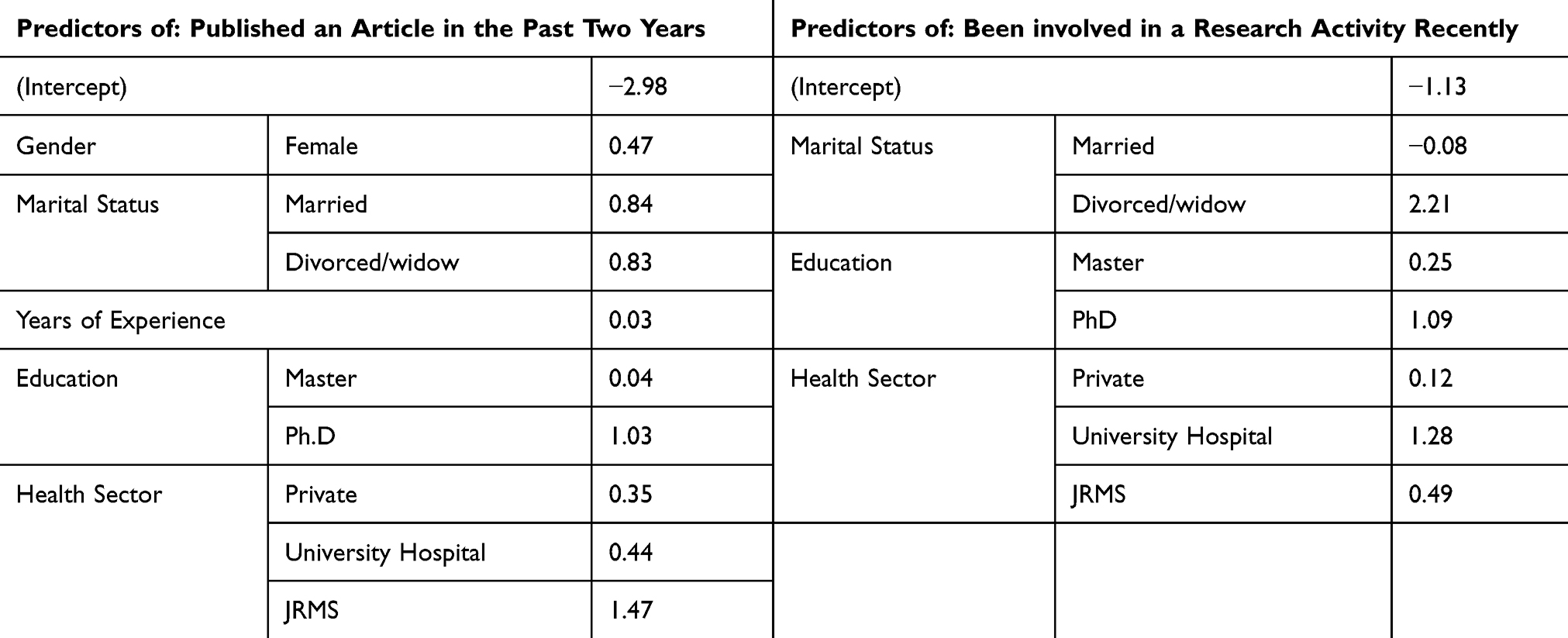 |
Table 2 Predictors of Current CPD Participation in Research Related Activities |
Motivation for CPD in Jordan
Figure 2 shows a summary of the responses for the motivations section of the questionnaire by health sector. Percentage of participants with “Strongly Agree” and “Agree” responses to the items in this section of the questionnaire are reported. As shown in this figure, generally high agreement levels have been shown by the physicians that the suggested items are motivators for their participation in CPD activities. Career progression was the topmost motivator to practice CPD among all participants with 91.2% agreement. Unfortunately, national policy and patient feedback were the lowest motivators among all with 62.2% and 71.1% agreement, respectively. Patient feedback, department/section policy, collecting CPD points and career progression had significantly different agreement levels among health sectors. Only 55.4% of JRMS participants reported that patient feedback was a motivator for their CPD participation while 75.3% of MOH participants reported this item as a motivation. Of all JRMS participants, 89.2% reported department/section policy a motivator while only 64.2% of private-sector participants reported the same. Surprisingly, all JRMS participants reported career progression was a motivator for CPD participation.
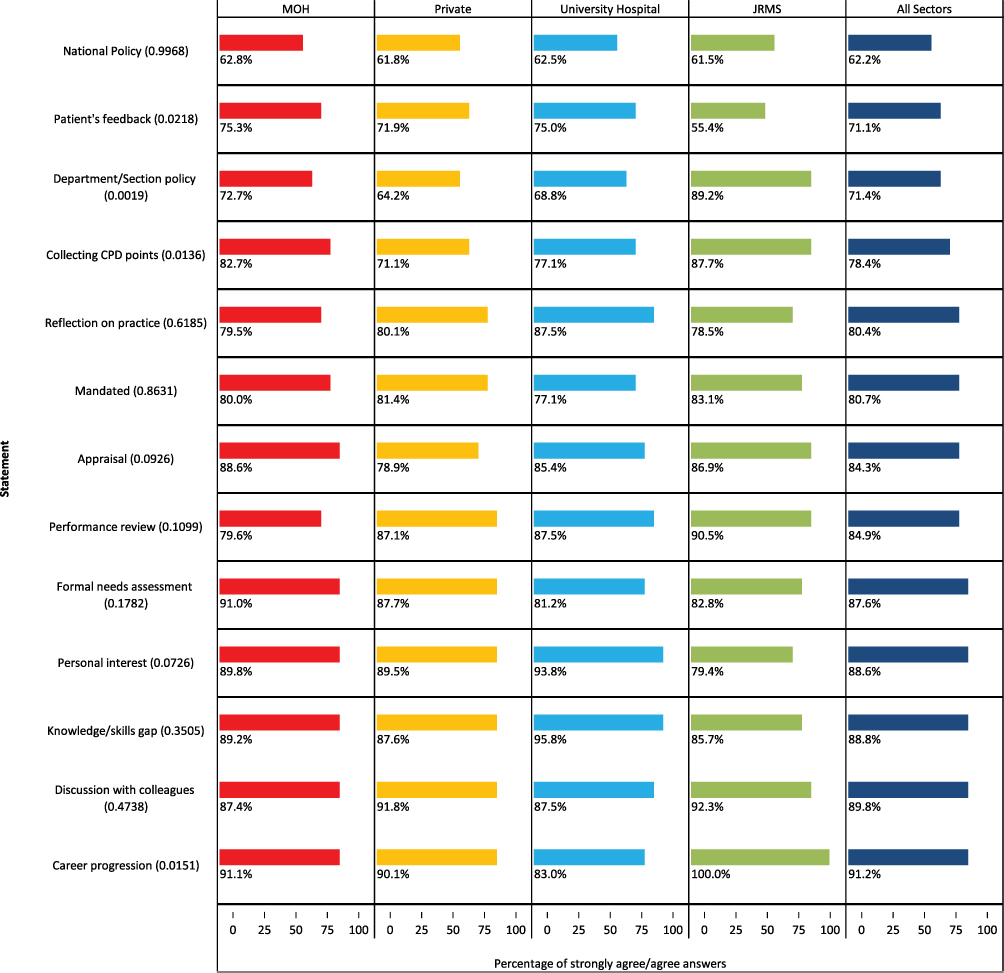 |
Figure 2 Motivators for participation in CPD activities by health sector. P-values for testing for differences among health sectors are given in parentheses. |
Barriers Towards CPD
Table 3 shows barrier significance by health sector assuming a five-point Likert scale of 1=“very low” to 5=“very high”. Results indicate that staff shortage and workload, limited funds, lack of time, event cost and lack of CPD resources were ranked as the top barriers to CPD. Table 3 shows that satisfactions with field knowledge, ability to obtain work leaves, event cost, limited funds, lack of encouragement, and lack of CPD resources have similar scores across healthcare sectors. Staff shortage and limited funds were identified as the top two most barriers to practice CPD for MOH, private sector, and university hospital participants, while staff shortage and family responsibilities were the top two most barriers for JRMS participants.
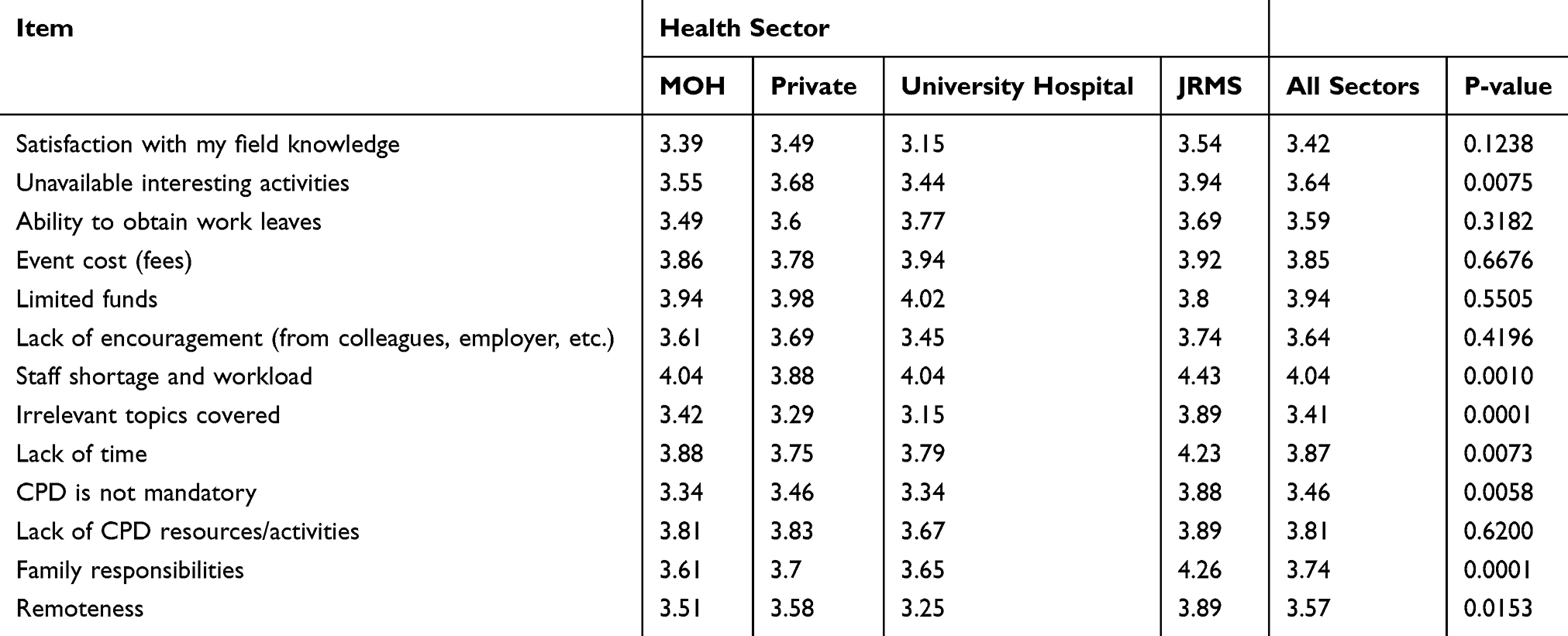 |
Table 3 Barriers to Practice CPD as Reported by the Study Participants Assuming a Five Points Likert Scale of “Very Low”=1 Through “Very High”=5 |
Discussion
Recertification or Revalidation of License
Time-limited certification in the US started in 1969 when the American Board of Family Medicine issued 7-year-limited certificates. Other American boards moved along the same lines, and by the year 2000 most American boards adopted the concept of “maintenance of certification (MOC)” programs which have included a 10 yearly, four part recertification assessments of medical knowledge, clinical competence, and communication skills.9
In 2000, the American Board of Medical Specialties (ABMS) mandated that all 24 specialty affiliate to limit board certification (BC) duration to 10 years, Subsequently, ABMS recertification programs to renew and maintain BC now require all physicians to subscribe to maintenance of certification.10 However, some physicians in the US are exempted from participating in MOC and not all of the 24 ABMS boards have the same requirements in terms of time and activities.11
The General Medical Council in the UK mandates that all the General Medical Council (GMC) physicians must revalidate their license and all specialists must undergo recertification on the specialist register of the GMC.12 The purpose of the recertification in the US and the UK is principally to ensure that doctors update their knowledge and improve their professional conduct.
The General Medical Council (GMC) of the United Kingdom in the 1990s used the term “revalidation” which was defined by the International Association of Medical Regulatory Authorities as the process by which doctors show that they are up to date and fit to practice medicine. The revalidation process in the UK commenced formally in 2012 and has become a mandatory component of medical license renewal. Revalidation in the UK requires CPD activities, participation in an annual appraisal along with a more detailed assessment every 5 years. This includes multisource feedback from multiple health practitioners as well as patients.13 The process is considered by many as being cumbersome, labor-intensive, and very costly.14,15
Walshe et al, showed while there were improvements noted in certain areas in the system of revalidation, these mostly related to identifying poor performance, and that the “one size fits all” process did not appear to create anything positive for highly performing individuals.16
Revalidation is mandatory in Canada and involves a combination of CPD including practice audit, multisource feedback, and formative assessment, aligned with the Can MEDS framework that promotes self-reflection and practice improvement. Similar systems of mandatory revalidation exist in Germany, New Zealand, and the Netherlands.17,18
In the US to be called a board-certified physician, this requires a level of training, competence, and knowledge that can only be achieved by completing a rigorous, defined, closely monitored training program approved by the Accreditation Council for Graduate Medical Education (ACGME), and then demonstrating a level of knowledge comparable to established standards by passing the initial certifying examination. Once American physicians are certified with the Board, the emphasis shifts to demonstrating lifelong professional development and the ability to deliver quality care and to continually improving that care through a process of ongoing assessment called Maintenance of Certification (MOC).9,10,19
Different specialties have different requirements, but these can vary from combinations of open book examinations, CME points, completion of a practice improvement program, and a high stakes secured examination every 10 years. Maintenance of Certification in the US remains voluntary and subject to continuing debate and is not yet mandated for registration renewal, although the registration renewal processes also differ between states. Studies from the US showed that recertification is associated with higher standards of care.20
In Australia, it is a mandatory requirement that medical practitioners are engaged in a CPD program. However, The Medical Board of Australia is considering the implementation of revalidation system for all registered medical practitioners in Australia in order to strengthen and formalize CPD, as well as to early identify doctors at risk of poor performance, as well as those already performing poorly.21
Participation in CPD activities and collecting certain number of CPD hours over 5-year cycle in Jordan have become mandatory according to the relicensure bylaw which was issued In April 2018 in order for a practitioner to renew their licensure every 5 years.
Continuing Medical Education (CME) or Continuing Professional Development (CPD)
The objective of Continuing Professional Development (CPD) and Continuing Medical Education (CME) is to keep healthcare workers up-to-date in their medical practice as part of a life learning commitment to their patients and society.
Around the world there has been a dynamic debate about the best way to enhance Good Medical Practice (GMP), such as knowledge, skills and performance, safety and quality, communication, partnership and teamwork, and whether to link GMP to recertification or relicensure, link it with CME or CPD, and whether these activities should be optional or mandatory.
The term continuous medical education CME refers to lectures, presentations, reading, and conference attendance, whereas continuous professional development CPD refers to a broader range of CME activities that allow practitioners to broaden their knowledge, expertise, and competence.22
The concept of CME has been well established since the 1970s, and in addition to didactic lectures, a broad range of educational models and training activities has been employed based on clinician practice.
For the practicing physician, standards of CME and CPD are less explicit and emerge from clinical practice guidelines, local and national standards of care, and the actions of the regulatory authorities. Furthermore; stimuli for learning at the independent practitioner level emerge from service with learning tied to patient needs and usually follow the principles of adult learning which emphasize the relevance and utility of the contents, include active and reflective strategies and connect to experience and previous knowledge. According to Bloom in his leading article in 2005, the most valuable educational methods regarding physician performance were interactive and included audit of patient data along with feedback, interactive educational seminars, academic detailing, and reminders. These forms of education were all shown to have a positive impact on both clinical performance and patient outcomes. Contrary to general belief, classic lectures and printed materials had little benefit on either clinical performance or patient outcomes whereas clinical practice guidelines and opinion leaders had modest effects.23 Cervero and, Gaines reported similar findings.24
The Relicense Bylaw in Jordan
Until recently, most physicians in Jordan continue to enjoy the trust and respect of their patients and the general public, and they do not need to revalidate their certificates, nor do they require to show evidence of continuous medical education to update their knowledge and skills, and fitness for the medical practice. However, the introduction of the relicensure bylaw has made it mandatory for all healthcare workers including physicians to engage in CPD activities and accumulate credit hours to be able to renew their license every 5 years.
Our study has shown that most physicians practice CPD in terms of attending conferences local seminars and training workshops. Surprisingly, only 21.3% of all participants have published an article in the past two years and only 34.9% have participated in a research-related activity in the same period. Majority of participants know the latest guidelines related to their profession CPD (71.7%), unfortunately, less than half (44.8%) of all participants keep track of their CPD hours/points.
We find that career progression was the topmost motivator to practice CPD among all participants with 91.2% agreement. Lack of national policy and patient feedback were the lowest motivators among all with 62.2% and 71.1% agreement, respectively. On the other hand, staff shortage and workload, limited funds, lack of time, event cost and lack of CPD resources were ranked as the top barriers to CPD activities among Jordanian physicians.
Conclusion
Despite considerable evidence supporting the role of CPD in maintaining competence of physicians, participating in CPD activities in Jordan is compromised by lack of mandatory laws and barriers related to staff shortage, heavy workload, limited funds, lack of time, and cost. Personal interests and career progression are the top motivators for CPD. Most Jordanian physicians are interested in CPD activities related to health/medical informatics and enhancing their skills in evidence-informed practice. We recommend that future interventions and health policy directions should be informed by these findings in order to optimize uptake of CPD programs in Jordan.
Acknowledgments
This research was conducted while professor Nidal Younes was on sabbatical leave from the University of Jordan, and the research was supported by The US Agency for International Development (USAID) grant.
Author Contributions
All authors contributed to data analysis, revising the article and gave the final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Teunissen PW, Dornan T. Lifelong learning at work. BMJ. 2008;336(7645):667–669. doi:10.1136/bmj.39434.601690.AD
2. Choudhry NK, Fletcher RH, Soumerai SB. Systematic review: the relationship between clinical experience and quality of health care. Ann Intern Med. 2005;142:260–273. doi:10.7326/0003-4819-142-4-200502150-00008
3. Davis DA, Mazmanian PE, Fordis M, et al. Accuracy of physician self-assessment compared with observed measures of competence: a systematic review. JAMA. 2006;296:1094–1102. doi:10.1001/jama.296.9.1094
4. Carraccio CL1, Benson BJ, Nixon LJ, et al. From the educational bench to the clinical bedside: translating the dreyfus developmental model to the learning of clinical skills. Acad Med. 2008;83(8):761. doi:10.1097/ACM.0b013e31817eb632
5. Alsharif A, Al-Khaldi Y. Attitude, practice and needs for continuing medical education among primary healthcare doctors in Asir region. J Family Community Med. 2001;8(3):37.
6. Bower E, Girard D, Wessel K, Becker T, Choi D. Barriers to innovation in continuing medical education. J Continuing Educ Health Professions. 2008;28(3):148–156. doi:10.1002/chp.176
7. Elshami W, Elamrdi A, Alyafie S, Abuzaid M. Continuing professional development in radiography: practice, attitude and barriers. Int J Med Res Health Sci. 2016;5(1):68–73. doi:10.5958/2319-5886.2016.00015.1
8. Shah M, Goyal V, Singh V, Lele J. Preferences and attitudes of physicians in India towards continuing medical education. J Eur CME. 2017;6(1):1332940. doi:10.1080/21614083.2017.1332940
9. Iglehart JK, Baron RB. Ensuring physicians’ competence – is maintenance of certification the answer? N Engl J Med. 2012;367:2543–2549. doi:10.1056/NEJMhpr1211043
10. Kempen PM. Maintenance of certification - important and to whom. J Community Hosp Intern Med Perspect. 2013;3(1):20326.
11. Sutherland K, Leatherman S. Does certification improve medical standards? BMJ. 2006;333(7565):439–441. doi:10.1136/bmj.38933.377824.802
12. Southgate L, Pringle M. Revalidation in the United Kingdom: general principles based on experience in general practice. BMJ. 1999;319:1180–1183. doi:10.1136/bmj.319.7218.1180
13. Hill JJ1, Asprey A, Richards SH, Campbell JL. Multisource feedback questionnaires in appraisal and for revalidation: a qualitative study in UK general practice. Br J Gen Pract. 2012;62(598):e314–21. doi:10.3399/bjgp12X641429
14. Hawkes N. Revalidation seems to add little to the current appraisal process. BMJ. 2012;345:e7375. doi:10.1136/bmj.e7375
15. Archer J, Regan de Bere S, Nunn S, Clark J, Corrigan O. “No one has yet properly articulated what we are trying to achieve”: a discourse analysis of interviews with revalidation policy leaders in the United Kingdom. Acad Med. 2015;90:88–93. doi:10.1097/ACM.0000000000000464
16. Walshe K, Boyd A, Bryce M, et al. Implementing medical revalidation in the united kingdom: findings about organizational changes and impacts from a survey of responsible officers. J R Soc Med. 2017;110:23–30. doi:10.1177/0141076816683556
17. Lemire F. Physician practice improvement. Can Fam Physician. 2015;61(9):816.
18. Burge S. Recertification in the medical specialties: a way forward. Clin Med. 2007;7:232–234. doi:10.7861/clinmedicine.7-3-232
19. Miles PV. Maintenance of certification: the role of the American Board of Pediatrics in improving children’s health care. Pediatr Clin North Am. 2009;56(4):987–994. doi:10.1016/j.pcl.2009.05.010
20. Sharp LK, Bashook PG, Lipsky MS, Horowitz SD, Miller SH. Specialty board certification and clinical outcomes: the missing link. Acad Med. 2002;77(6):534–542. doi:10.1097/00001888-200206000-00011
21. Pickles R. Revalidation or recertification: what does it all mean. Arch Med Health Sci. 2018;6:12–15. doi:10.4103/amhs.amhs_132_17
22. Peck C. Continuing medical education and continuing professional development: international comparisons. BMJ. 2000;320(7232):432–435. doi:10.1136/bmj.320.7232.432
23. Bloom BS. Effects of continuing medical education on improving physician clinical care and patient health: a review of systematic reviews. Int J Technol Assess Health Care. 2005;21:380–385. doi:10.1017/S026646230505049X
24. Cervero RM, Gaines JK. The impact of CME on physician performance and patient health outcomes: an updated synthesis of systematic reviews. J Contin Educ Health Prof. 2015;35:131–138. doi:10.1002/chp.21290
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.