")
Back to Journals » International Journal of General Medicine » Volume 14
Endoscopic Retrograde Appendicography: An Alternative Diagnostic Method for Acute Appendicitis
Authors Liu Z , Ma X, Ullah S , Song J, Kong L, Li D, Pan C, Liu B
Received 25 August 2021
Accepted for publication 1 October 2021
Published 21 October 2021 Volume 2021:14 Pages 7043—7049
DOI https://doi.org/10.2147/IJGM.S336040
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Zhenzhen Liu,1 Xiao Ma,2 Saif Ullah,1 Jitao Song,2 Lingjian Kong,1 Deliang Li,1 Chao Pan,2 Bingrong Liu1
1Department of Gastroenterology, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, People’s Republic of China; 2Department of Gastroenterology, The Second Affiliated Hospital of Harbin Medical University, Harbin, People’s Republic of China
Correspondence: Bingrong Liu
Department of Gastroenterology, The First Affiliated Hospital of Zhengzhou University, No. 1 Eastern Jianshe Road, Zhengzhou, 450052, People’s Republic of China
Tel/Fax +86-15713815559
Email [email protected]
Purpose: To evaluate the role of endoscopic retrograde appendicography for the diagnosis of acute appendicitis.
Patients and Methods: We retrospectively analyzed 33 patients (20 men and 13 women, average age 44± 18 years) with suspected acute appendicitis between December 2016 and November 2018. Endoscopic direct-vision imaging or fluoroscopic endoscopic retrograde appendicography was performed to separate suspected acute appendicitis from actual acute appendicitis. The success rate, complications, and recurrence rate were recorded.
Results: Acute appendicitis was ruled out by normal endoscopic retrograde appendicography in 8 (24%) and confirmed in 23 patients (70%). In 2 patients (6%), appendiceal orifice cannulation failed. Colonoscopic findings in acute appendicitis were mucosal hyperemia and edema of appendiceal orifice (83%), outpouring of pus from the appendiceal orifice (74%), and swollen cecal mucosa (61%). Appendicograpic findings were either normal or in acute disease showed diffuse luminal dilation (diameter: 0.8± 0.4 mm), partial stenosis (43%), stiffness or inflexibility (87%) and filling defects (22%). There were no complications during or after follow-up for a median of 13 months (IQR: 9– 24 months).
Conclusion: Endoscopic retrograde appendicography appears to be a reliable and safe method to confirm or exclude the diagnosis of acute appendicitis and prevent unnecessary appendectomy.
Keywords: acute appendicitis, endoscopic retrograde appendicography, diagnosis, appendicography
Introduction
Acute appendicitis (AA) is one of the most common causes of acute abdominal pain. The incidence ranges from 6.7% to 8.6%.1 Currently, appendectomy is the first-line treatment for uncomplicated and complicated appendicitis.2–7 However, the clinical diagnosis of AA is often challenging and involves a synthesis of clinical, laboratory, and radiological findings, improved by using clinical scoring systems that involve physical examination findings and inflammatory markers. Many simple and user-friendly scoring systems such as Alvarado score, appendicitis inflammatory response score have been used as a structured algorithm in order to aid in predicting the risk of AA3 The rate of false positive diagnoses of acute appendicitis still remains in spite of a lower negative appendectomy rate following the introduction of new imaging techniques such as multidetector enhanced computed tomography (CT) or ultrasonography (US). Graff et al’ reported that the rate of false-positive diagnoses of acute appendicitis ranged from 4.7% to 19.5% (average 10.5%), which was variable among hospitals,4 and the reported negative appendectomy rate is as high as 36%.5 While false positive tests to negative appendectomy, false negative diagnoses may result in delayed management and complications of the disease. A more accurate diagnostic method is needed especially when the initial diagnostic approach is not definitive.
Colonoscopy has been recognized as an alternative approach to diagnose acute appendicitis, with 100% sensitivity and 99% specificity.8 General colonoscopy can observe mucosal morphology and discriminate inflammation performance. Colonoscopy may be useful in the diagnosis of appendicitis when the clinical presentation is atypical for appendicitis and/or imaging studies are nondiagnostic.8
Inspired by endoscopic retrograde cholangiopancreatography (ERCP), Liu et al developed a new minimally invasive approach to treat AA called endoscopic retrograde appendicitis therapy (ERAT).9 First step of ERAT is endoscopic retrograde appendicography (ERA) which is to diagnose appendicitis. The direct fluoroscopy method visually revealed the condition of the inner appendiceal orifice and aided into the accurate diagnosis, and treatment of suspected acute appendicitis.10–12 The aim of this study was to systematically evaluate the efficacy of ERA in the diagnosis of acute appendicitis.
Patients and Methods
Patients
Consecutive patients with suspected acute uncomplicated appendicitis were offered ERA and ERAT at the Second Affiliated Hospital of Harbin Medical University (a tertiary care center in China) between December 2016 and November 2018. The inclusion criteria included: 1) patients with suspected acute appendicitis diagnosed by abdominal CT or US. The CT scan or US criteria of the radiographic diagnosis of appendicitis were the presence of an inflammatory reaction or fecal stone on CT (CT scan showing an appendix larger than 15 mm with thickened or irregular walls is suspected of neoplasia), 2) suspected appendicitis was diagnosed by clinical symptoms and signs (eg an Alvarado score ≥5), 3) for patients such as pregnant women, children, and couples planning for conception who rejected CT, the diagnosis was confirmed by colonoscopy based on the findings of edema at the opening of the appendix or pus flowing out of the appendix cavity, and 4) patients with a strong desire to preserve the appendix and some special patients who cannot tolerate surgical treatment. Exclusion criteria included: 1) patients with a clear diagnosis of acute complicated appendicitis (such as perforated appendicitis or periappendiceal abscess) confirmed by non-enhanced CT (16-detector-row) or US, 2) patients with suspected appendiceal tumors for those endoscopic results showed an involuted, mass-like protrusion, mucus or polyp-like tissue at the opening of the appendix.
The study was performed according to the principles of the Declaration of Helsinki, and was approved by the Institutional Review Board of the Second Affiliated Hospital of the Harbin Medical University. The written informed consent was obtained from the patients before the study.
Description of Technique
Preparation for ERAT includes bowel preparation using either 2L polyethylene glycol electrolyte solution or low-pressure cleansing enemas (300–500 mL per enema) given five times. For patients with mild or moderate symptoms, oral prep was given 4–6 hours before the procedure. For clinically severe cases or patients with anorexic or nauseous/vomiting low-pressure cleansing enemas (300–500 mL per enema) were given approximately 30 minutes prior to endoscopy so as not to delay treatment of appendicitis.
All the ERAT procedures were performed as described by Liu et al in 2012.9 Briefly, ERA involves a colonoscope (CF-H260 or GIF-Q260J, Olympus, Japan) with an attached transparent cap. After finding Gerlach’s valve in the cecum, the colonoscope was positioned close to the appendiceal orifice. Gerlach’s valve was pushed aside using the transparent cap so that the tip of a catheter (OE-104-2225DL, EndoFlex, Germany) could be wedged into the appendiceal orifice. A 0.035 inch guide wire (BostonScientific, US) was then inserted into the appendiceal lumen over the catheter and placed deep into the lumen under fluoroscopic guidance. Decompression of the appendiceal lumen was achieved by suction using a syringe (5 mL) attached to the catheter. A soluble contrast agent was then infused to fill the appendix while being monitored by fluoroscopy to check the location, length, shape, content and flexibility of the appendix.
The reference standard for confirming acute appendicitis was defined as symptom resolution after successful ERAT with subjects remaining recurrence-free during follow-up. Patients without appendicitis included those for whom another disease was diagnosed or who uneventfully recovered after corresponding treatment based on the current guidelines.
Outcomes and Follow-Up
The primary outcome measures were the performance characteristics (sensitivity, specificity, positive and negative predict values) of ERA in the patients with suspected acute appendicitis. The diagnosis of acute appendicitis was made when the endoscopic retrograde appendicography features of the patient matched (1), (2) or (3) as shown in Table 1.
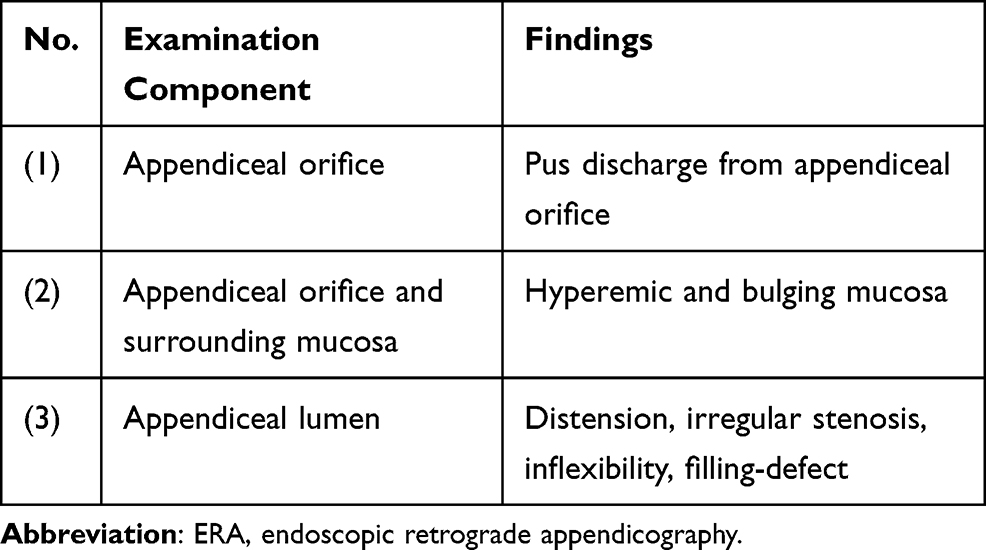 |
Table 1 The Positive Findings of ERA for the Diagnosis of Acute Appendicitis |
The secondary outcome measures included complications, appendiceal cannulation rate, colonoscopy and endoscopic retrograde appendicography findings and the accuracy of CT and US.
Telephone follow-up was conducted to assess for recurrent symptoms and long-term complications until the end of the study period. If any symptoms were present, such as abdominal pain, fever or other digestive symptoms, the patient was recommended to return for further examination, laboratory tests and US or CT, as necessary.
Statistical Analyses
Results were expressed as mean ± standard deviation (SD) or median (interquartile range, IQR). Quantitative variables were compared between the two groups using the t-test or the Mann–Whitney U-test, as appropriate. Categorical variables were compared between the two groups using the Fisher’s exact test. A two-tailed P value <0.05 was considered to be statistically significant. Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS) version 23.0 for Windows.
Results
The 33 consecutive patients (20 men and 13 women, average age 44±18 years) were enrolled. Patients’ baseline characteristics are shown in Table 2. In patients with clinically suspected acute appendicitis, the median of Alvarado scores was 7 (IQR: 5.5–8). According to clinical symptoms, signs, laboratory examination, imaging findings (US or CT), treatment results and prognosis, acute appendicitis was confirmed in 25 patients (76%) and ruled out in 8 patients (24%).
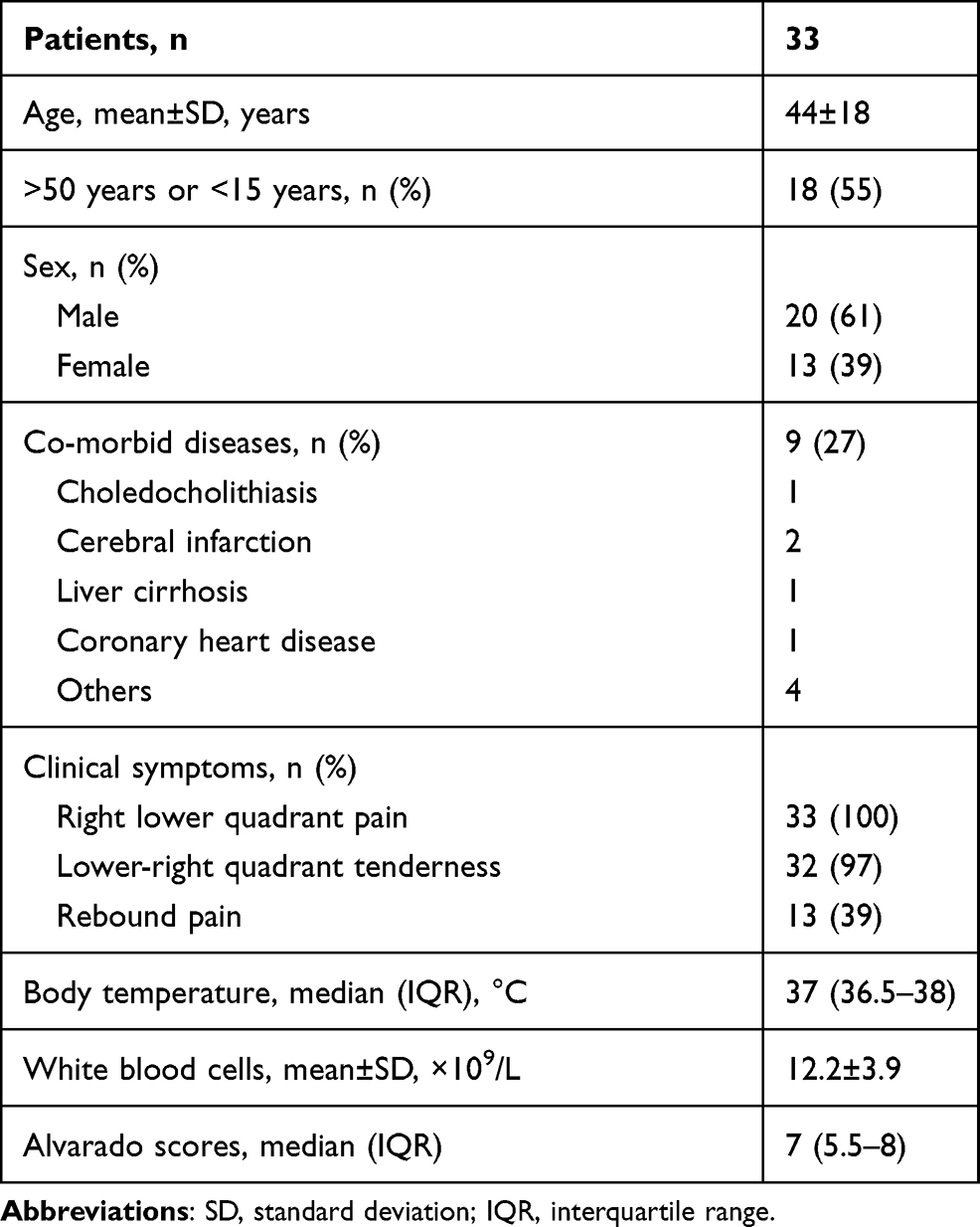 |
Table 2 Basic Characteristics of Study Patients |
Thirty-one patients (94%) successfully underwent endoscopic ERA, including 23 patients with acute appendicitis and 8 patients without acute appendicitis. Two (6%) had failed cannulation of the appendiceal orifice due to blockage by fecaliths. In the 23 patients with acute appendicitis (Table 3), colonoscopic findings showed mucosal hyperemia and edema of appendiceal orifice (83%) (Figure 1A and B), swollen mucosa of cecum (61%) and discharge of pus from appendiceal orifice (74%) (Figure 1C). Appendicography showed intraluminal filling defect sign (22%) (Figure 1D), lumen distension (median 0.7 cm; IQR = 0.4–1.0cm), partial stenosis (43%) (Figure 1E), and inflexibility or stiffness (87%). The median luminal diameter of the appendix in patients without acute appendicitis was significantly less than the patients with acute appendicitis (0.3 cm vs 0.7 cm, p = 0.004) although the luminal length was not significant difference (6.7 ± 2.3 cm vs 6.5 ± 1.6 cm, p = 0.802). Figure 1F shows a normal appendix.
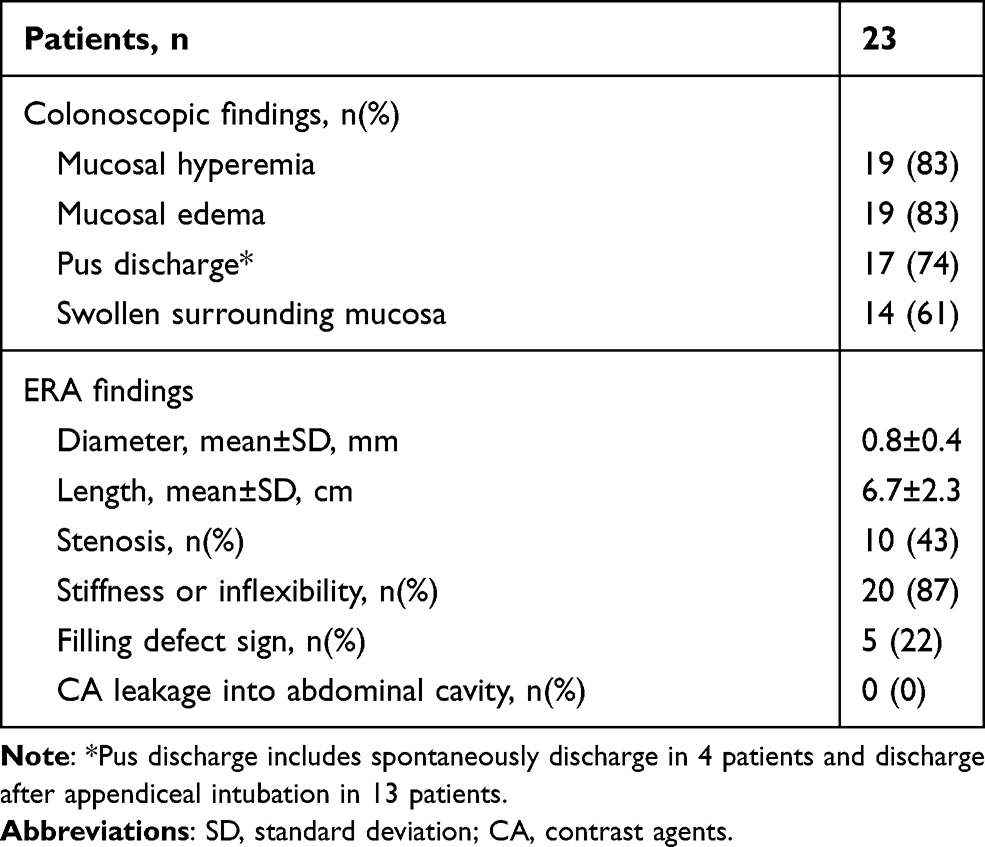 |
Table 3 Colonoscopic and Radiological Findings of Patients with Acute Appendicitis That Underwent ERA |
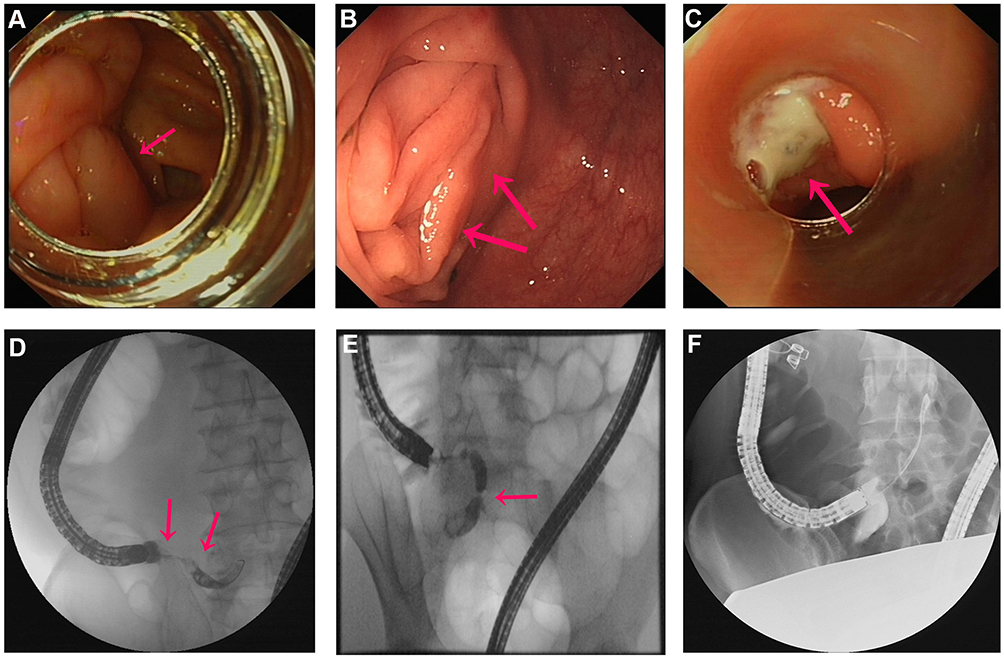 |
Figure 1 The colonoscopic and radiological findings during ERA. (A and B) Hyperemic and bulging mucosa around the appendiceal orifice. (C) Pus discharge from the appendiceal orifice. (D) Intraluminal filling-defect sign. (E) Luminal distension and stenosis. (F) Normal appendix. |
The ERAT technique requires direct endoscopic imaging or fluoroscopic endoscopic retrograde appendicography to separate suspected acute appendicitis from actual acute appendicitis. For patients with appendicitis, the ERAT procedure is performed to relieve the appendiceal lumen obstruction. All the patients with confirmed acute appendicitis by ERA recovered uneventfully. The diagnosis of acute appendicitis in the 2 patients in whom the appendiceal orifice could not be cannulated was confirmed on the basis of appendectomy and histology. We included these 2 failure cases in the equivocal ERA results. During follow-up (median: 13 months; IQR: 9–24 months), 2 (8%) of the patients with acute appendicitis subsequently underwent appendectomy for recurrent abdominal pain and were histologically diagnosed with acute appendicitis.
The diagnoses of the 8 patients without acute appendicitis are shown in Table 4. All 8 patients uneventfully recovered after corresponding treatment and no recurrences occurred during follow-up. One attempted ERA had failed because the appendiceal orifice was blocked by a malignant tumor. We also included the patient with carcinoma in the equivocal negative results. Overall, in 8 patients (24%) acute appendicitis was definitely ruled out through endoscopic retrograde appendicography.
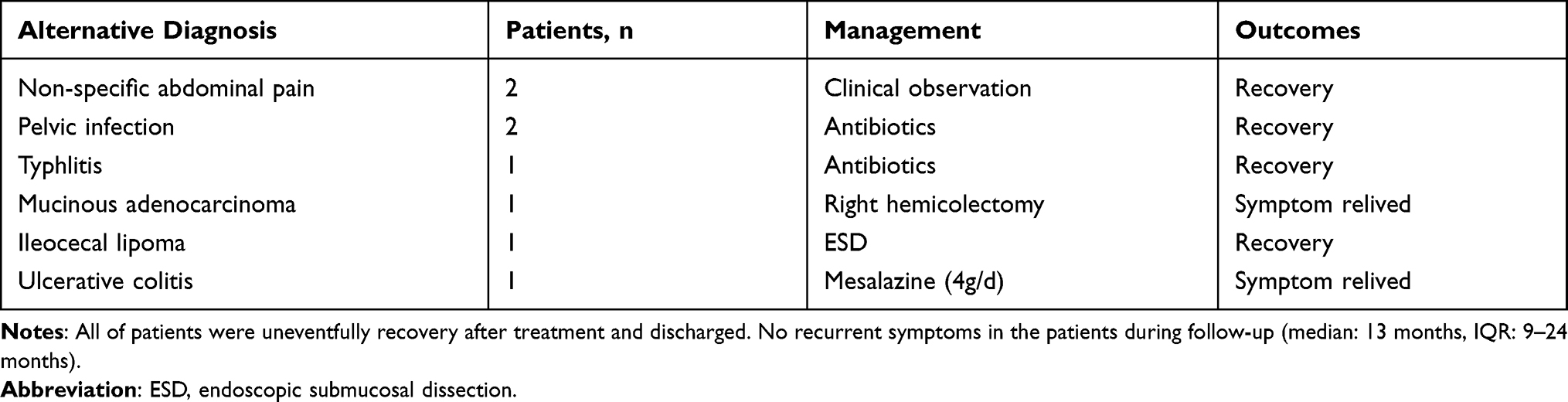 |
Table 4 Alternative Diagnosis of Patients Without Acute Appendicitis |
Overall, endoscopic retrograde appendicography was correctly diagnosed in 23 patients with acute appendicitis and ruled it out in 8 cases; 2 cases had equivocal results due to failure appendix cannulation. If the equivocal results were included, the sensitivity and specificity of ERA were 92% and 100%, respectively. The positive predict value and negative predict value of endoscopic retrograde appendicography were 100% and 80%, respectively. Furthermore, there were no complications during a median follow-up period of 13 months (IQR: 9–24 months).
Comparison with CT and Ultrasound
In the study, CT scans were performed in 24 patients and US in 17 before endoscopic retrograde appendicography; both CT scan and US were performed in 7 patients. With CT scans, 2 patients (8%) were misdiagnosed and 8 patients (33%) had equivocal results. Two patients (12%) were incorrectly diagnosed and 2 other patients (12%) had equivocal results using ultrasound. Even if the equivocal results of CT and US were excluded from the calculations, the sensitivity and specificity of CT was 88% and 75%, respectively. The sensitivity and specificity of US was 73% and 50%, respectively. The sensitivity and specificity of the endoscopic retrograde appendicography results were 100% and 100%, respectively (when equivocal results were included, 92% and 100%, respectively) (Table 5). Overall, 8 patients (24%) were prevented from having unnecessary surgery.
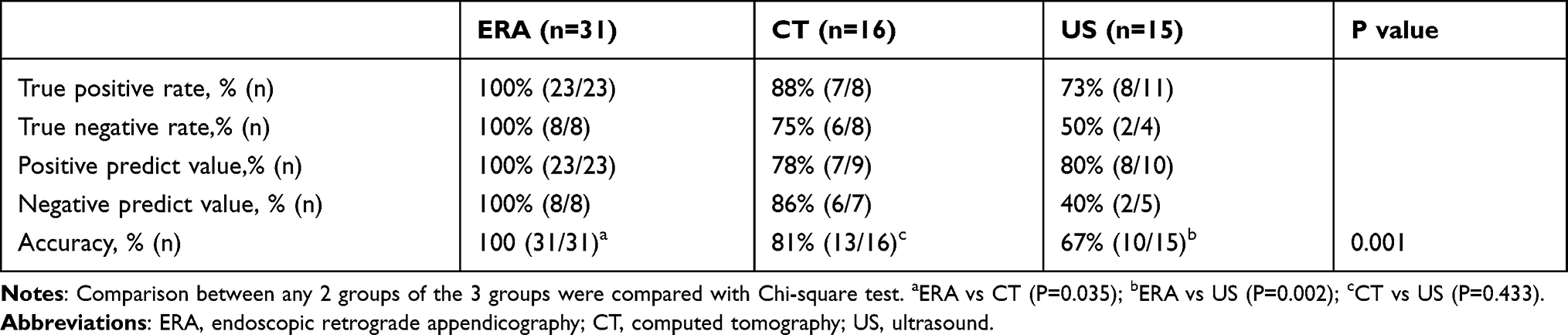 |
Table 5 Comparison of ERA, CT and US |
Discussion
Acute appendicitis is one of the most common causes of acute abdominal pain. Although the classical symptoms of acute appendicitis is periumbilical pain migrating to the right lower quadrant, the presentation is rarely typical and diagnostic errors are common resulting in either negative appendectomies or appendiceal perforations. This study systematically investigated the efficacy of ERA in the diagnosis of acute appendicitis and showed a high diagnostic yield in patients with acute abdominal pain.
Previous studies have reported colonoscopy as a useful diagnostic method of acute appendicitis in the patients with atypical presentation of abdominal pain or with non-diagnostic imaging studies.8,13 Chang et al described the colonoscopic features of acute appendicitis, including hyperemia and bulging at the appendiceal orifice area with surrounding mucosal edema and drainage of pus from the appendiceal orifice. Our study confirms the value of these features. However, some patients with acute appendicitis did not have any of these colonoscopic features. In our study, although there were 17 patients (74%) with pus discharge from the appendiceal orifice, only 4 (24%) had spontaneous pus discharge. In 13 patients (76%) pus discharge only occurred after successful cannulation of appendiceal orifice. Moreover, one patient presented with normal mucosa around the area of appendiceal orifice which is consistent with the fact that in some patients the inflammatory changes may affect only the distal appendix.14 Thus, colonoscopy alone is unable to reliably predict which patients have an abnormal appendiceal lumen. In contrast, appendicography combined with colonoscopy allowed acquisition of clear images of both appendiceal orifice and lumen for providing more accurate diagnosis.
The advantage of ERA over traditional barium enema lies in higher success rate of filling appendix. The diagnosis of acute appendicitis by barium enema is mainly based on non-filling of the full appendix.15 However, 15% to 23% of normal appendices fail to fill16,17 such that failed filling of the appendix is not a reliable sign for acute appendicitis.18 On the contrary, with a remarkable success (94%) of filled appendix, ERA easily identified the presence of lumen dilatation, partial stenosis, lack of flexibility and intraluminal filling-defects and thus can reliably confirm the diagnosis of acute appendicitis.
ERA advantages over CT or US are that it provides radiological imaging of appendix with more objectivity, irrespective of shape and position of appendix within abdominal cavity. Although some studies have reported high sensitivity and specificity of CT and US, some fecal stones cannot be found by imaging examination. Spyglass which is now being used for ERAT can directly view the appendix cavity and carry out targeted treatment, just as it is applied in biliary tract. Wilson et al described the equivocal rates of CT (28%) and US (75%),19 which is consistent with the result of CT (33%) in the present study. However, the equivocal rate of US (12%) was lower than the previous study, maybe due to the small sample size. US is more operator dependent, relying both on the US technician and the interpretation by the radiologist. Even though CT is more objective, the diagnostic accuracy is also limited by technical and interpretative pitfalls due to the shape and position of appendix inside the abdomen.20 Actually, clinicians have reported potential negative appendectomy rates of 21.4% due to CT.3 Another reason for relative lower accuracy of CT and US in our study is that many cases underwent endoscopic retrograde appendicography because of equivocal results of CT scan or US. In addition, some patients (pregnant women, children, and couples planning for conception, etc.) are not suitable for radiation and/or they do not wish to undergo X-ray or other radiological examination. However, CT exposes the patient to more ionizing radiation than radiography and is associated with a risk of radiation-induced cancer. ERA does not require radiological examination, and if there is a mechanical obstruction of appendicitis such as fecal stones can be successfully treated by Spyglass-assisted ERAT laser lithotripsy.
Another advantage of ERA compared to CT or US lies in differential diagnosis of abdominal pain mimicking acute appendicitis. During the procedure, the endoscopist can visualize the entire colon or appendix and make histological diagnosis by biopsy. In the present study, endoscopic retrograde appendicography identified 2 patients with pelvic infection, and 4 patients with typhlitis, mucinous adenocarcinoma, ileocecal lipoma or ulcerative colitis. However, further study is necessary to obtain a full comparison of the diagnostic accuracy of endoscopic retrograde appendicography, CT and US.
Previous studies have also reported that the patients with an atypical presentation were diagnosed as acute appendicitis using colonoscope.21,22 However, colonoscopy was not widely used for diagnosis of acute appendicitis, because the conventional wisdom is that colonoscope may aggravate abdominal pain and induce complications. However, there were no complications in this study. In contrast, the results showed that ERA can be safely performed on the patients with suspected acute uncomplicated appendicitis.
ERAT (including ERA) procedure can be performed in the outpatient department. Initially, we admitted patients after undergoing ERAT as this was a preliminary study with a limited sample size. A large prospective controlled randomized trial is necessary to provide more valuable information for clinical implication of endoscopic retrograde appendicography. However, with the development of colonoscopic technology, we believe this method will become the most reliable method of diagnosis for acute appendicitis in the future. ERAT can be used to diagnose and also to treat appendicitis. Its advantages include no damage on the body, organ retention, no postoperative pain, early food intake, quick recovery, fewer postoperative complications, and shorter hospital stay. So, in our opinion ERAT could be a first choice for acute uncomplicated appendicitis therapy, but it should not replace surgical appendectomy. However, most of the patients avoid surgical resection and have good results with ERAT.
In conclusion, our study suggests that ERA can accurately diagnosis and exclude acute appendicitis. ERA provides the physicians with clear images of both appendiceal orifice and lumen which might help in reducing the rate of negative appendectomies, and more importantly can preserve the normal appendix. However, further studies are needed to compare the efficacy of ERA with other radiological examinations before the recommendations are made.
Acknowledgments
We express our gratitude to Professor David Y. Graham, Professor of Medicine, Molecular virology and Microbiology, Baylor college of Medicine for his encouragement and assistance in revising the manuscript.
Funding
The research team fund of the first affiliated hospital of Zhengzhou University. Outstanding foreign scientist studio project of Henan province [No.GZS2020006]. Henan province higher education institutions key scientific research project plan [No.20A320081].
Disclosure
All authors report no conflicts of interest in this work.
References
1. Addiss DG, Shaffer N, Fowler BS, Tauxe RV. The epidemiology of appendicitis and appendectomy in the United States. Am J Epidemiol. 1990;132(5):910–925. doi:10.1093/oxfordjournals.aje.a115734
2. Ferris M, Quan S, Kaplan BS, et al. The global incidence of appendicitis: a systematic review of population-based studies. Ann Surg. 2017;266(2):237–241. doi:10.1097/SLA.0000000000002188
3. Di Saverio S, Podda M, De Simone B, et al. Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines. World J Emerg Surg. 2020;15(1):27. doi:10.1186/s13017-020-00306-3
4. Graff L, Russell J, Seashore J, Tate J, Elwell A, Prete M. False-negative and false-positive errors in abdominal pain evaluation: failure to diagnose acute appendicitis and unnecessary surgery. Acad Emerg Med. 2000;7(11):1244–1255. doi:10.1111/j.1553-2712.2000.tb00470.x
5. Allaway MGR, Eslick GD, Cox MR. The unacceptable morbidity of negative laparoscopic appendicectomy. World J Surg. 2019;43(2):405–414. doi:10.1007/s00268-018-4784-6
6. Isaksson K, Montgomery A, Moberg AC, Andersson R, Tingstedt B. Long-term follow-up for adhesive small bowel obstruction after open versus laparoscopic surgery for suspected appendicitis. Ann Surg. 2014;259(6):1173–1177. doi:10.1097/SLA.0000000000000322
7. Guller U, Hervey S, Purves H, et al. Laparoscopic versus open appendectomy: outcomes comparison based on a large administrative database. Ann Surg. 2004;239(1):43–52. doi:10.1097/01.sla.0000103071.35986.c1
8. Chang HS, Yang SK, Myung SJ, et al. The role of colonoscopy in the diagnosis of appendicitis in patients with atypical presentations. Gastrointest Endosc. 2002;56(3):343–348. doi:10.1016/S0016-5107(02)70036-9
9. Liu BR, Song JT, Han FY, Li H, Yin JB. Endoscopic retrograde appendicitis therapy: a pilot minimally invasive technique (with videos). Gastrointest Endosc. 2012;76(4):862–866. doi:10.1016/j.gie.2012.05.029
10. Liu BR, Ma X, Feng J, et al. Endoscopic retrograde appendicitis therapy (ERAT): a multicenter retrospective study in China. Surg Endosc. 2015;29(4):905–909. doi:10.1007/s00464-014-3750-0
11. Li Y, Mi C, Li W, She J. Diagnosis of acute appendicitis by Endoscopic Retrograde Appendicitis Therapy (ERAT): combination of colonoscopy and endoscopic retrograde appendicography. Dig Dis Sci. 2016;61(11):3285–3291. doi:10.1007/s10620-016-4245-8
12. Kang J, Zhang W, Zeng L, et al. The modified endoscopic retrograde appendicitis therapy versus antibiotic therapy alone for acute uncomplicated appendicitis in children. Surg Endosc. 2020. doi:10.1007/s00464-020-08129-8
13. Simsek Z, Altinbas A, Uskudar O, Han U. Role of colonoscopy in the diagnosis of acute appendicitis. Dig Endosc. 2012;24(1):50. doi:10.1111/j.1443-1661.2010.01102.x
14. Carr NJ. The pathology of acute appendicitis. Ann Diagn Pathol. 2000;4(1):46–58. doi:10.1016/S1092-9134(00)90011-X
15. Smith DE, Kirchmer NA, Stewart DR. Use of the barium enema in the diagnosis of acute appendicitis and its complications. Am J Surg. 1979;138(6):829–834. doi:10.1016/0002-9610(79)90306-4
16. Brenner DJ, Hall EJ. Computed tomography – an increasing source of radiation exposure. N Engl J Med. 2007;357(22):2277–2284. doi:10.1056/NEJMra072149
17. Sakover RP, Del Fava RL. Frequency of visualization of the normal appendix with the barium enema examination. Am J Roentgenol. 1974;121(2):312–317. doi:10.2214/ajr.121.2.312
18. Terasawa T, Blackmore CC, Bent S, Kohlwes RJ. Systematic review: computed tomography and ultrasonography to detect acute appendicitis in adults and adolescents. Ann Intern Med. 2004;141(7):537–546. doi:10.7326/0003-4819-141-7-200410050-00011
19. Rao PM. Technical and interpretative pitfalls of appendiceal CT imaging. AJR Am J Roentgenol. 1998;171(2):419–425. doi:10.2214/ajr.171.2.9694467
20. Ujiki MB, Murayama KM, Cribbins AJ, et al. CT scan in the management of acute appendicitis. J Surg Res. 2002;105(2):119–122. doi:10.1006/jsre.2002.6407
21. Zimmer V, Raedle J. Endoscopic view of appendicitis. Mayo Clin Proc. 2008;83(6):622. doi:10.1016/S0025-6196(11)60886-0
22. Minocha A. An endoscopic view of appendicitis. N Engl J Med. 1998;339(20):1481. doi:10.1056/NEJM199811123392015
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.