")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Employment-Related Factors of Forensic Psychiatric Outpatients with Psychotic Disorders
Authors Takeda K, Sugawara N , Yamada Y , Nagata T, Kashiwagi H, Kono T, Hirabayashi N , Okada T
Received 27 August 2019
Accepted for publication 12 November 2019
Published 2 December 2019 Volume 2019:15 Pages 3341—3350
DOI https://doi.org/10.2147/NDT.S228916
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Taro Kishi
Koji Takeda,1,2 Norio Sugawara,3 Yuji Yamada,1 Takako Nagata,1 Hiroko Kashiwagi,1 Toshiaki Kono,4 Naotsugu Hirabayashi,1 Takayuki Okada2
1Department of Psychiatry, National Center of Neurology and Psychiatry Hospital, Kodaira, Tokyo 187-8551, Japan; 2Section of Psychiatry and Behavioral Sciences, Graduate School of Medical and Dental Sciences, Tokyo Medical and Dental University, Tokyo 113-8510, Japan; 3Department of Psychiatry, Dokkyo Medical University School of Medicine, Tochigi 321-0843, Japan; 4Department of Community Mental Health and Law, National Institute of Mental Health, National Center of Neurology and Psychiatry, Kodaira, Tokyo 187-8553, Japan
Correspondence: Koji Takeda
Department of Psychiatry, National Center of Neurology and Psychiatry Hospital, 4-1-1 Ogawa-Higashi, Kodaira, Tokyo 187-8551, Japan
Tel +81 42 341 2711
Fax +81 42 344 6745
Email [email protected]
Purpose: Employment is important for forensic psychiatric patients with psychotic disorders, in terms of reduction in symptoms, improving the quality of life, and preventing re-offenses. However, few detailed studies on employment status in such patients exist. We aimed to determine the employment rate among forensic psychiatric outpatients with psychotic disorders and identify the factors associated with employment.
Patients and methods: The study population comprised 406 patients with psychotic disorders who completed a forensic outpatient treatment order, were aged discharge from a forensic psychiatric ward and provided written informed consent. Psychotic disorders were defined as psychiatric disorders classified into F2 in the International Statistical Classification of Diseases and Related Health Problems, 10th edition. Demographic data were collected from the medical records of the inpatient treatment period. Prognostic data during the outpatient treatment order period was provided by the reintegration coordinators responsible for coordinating the patients’ social environment during this period. Exploratory univariate and multivariable logistic regression analyses identified the factors associated with employment.
Results: The mean age at discharge was 44.4±10.8 years. The mean follow-up period was 2.69±1.01 years. There were 4.6 times more men (n=334) than women (n=72). During the outpatient treatment order period, 56 of 406 participants achieved employment (13.8%). Participants who committed serious crime, including homicide, arson, robbery, and sexual assault, had a lower employment rate compared to participants who committed bodily injury crimes (multivariable odds ratio, 0.421; 95% confidence interval, 0.220–0.807). History of substance use and living with family after discharge from a forensic psychiatric ward positively contributed to employment.
Conclusion: The employment rate among forensic psychiatric outpatients with psychotic disorders was low and was similar to that reported in previous studies on general psychiatric patients with schizophrenia. Furthermore, serious criminal behavior negatively impacted employment.
Keywords: criminal behavior, schizophrenia, work, job, mentally disordered offenders
Introduction
Despite the fact that most people with mental disorders want to work,1–3 on average, people with mental disorders have high rates of unemployment.4–6 The employment rate among patients with psychiatric diseases depends on the type of psychiatric disease.5 For example, most studies on patients with bipolar disorder have reported employment rates of 40–60%.7 A recent large study of mood disorders in Denmark also reported that the unemployment rates of bipolar cases or depression cases were 62% and 53% at age 30, respectively.8 The employment rate among patients with schizophrenia is also lower than that of the general population,1,5,9–12 ranging from 4% to 50.4%,13 with most studies reporting a rate between 10–20%.11,14 The severity of negative symptoms,15,16 cognitive dysfunction,17 early onset age and duration of illness,15 higher rate of early relapse,18 older age,16,17 and lower education,16 have all been reported to be negatively associated with employment outcomes.13,19 Work history is positively associated with employment rate.14 It has also been suggested that the availability of vocational services and welfare benefits may contribute to variations in employment rate between countries.9
Patients believe that meaningful employment aids in avoiding illness and psychosis, motivates them to recover from relapse, and increases feelings of being a part of the community.20 Furthermore, another qualitative study has suggested that employment is a protective factor for preventing relapse in patients with schizophrenia.21 A review of employment for patients with schizophrenia suggested a possible influence on clinical benefits such as reduction in symptoms and hospitalizations.14 Employment is also related to the positive health-related quality of life (QOL) and self-esteem in patients with schizophrenia.13,14,22
The United States Bureau of Justice Statistics reported that 67.8% of released prisoners in 2005 were arrested within three years of release.23 In the United States, the Second Chance Act authorized federal grants to government agencies and nonprofit organizations to provide reentry services, including employment assistance, supporting correction and supervision practices that aimed to reduce recidivism.24 This has improved the outcomes in those returning from state and federal prisons, local jails, and juvenile facilities.25 In fact, eleven states have experienced impressive declines (7–28%) in the return-to-prison rate since the time of the most recent peak recidivism for each state.25 A study conducted in India also reported that employment reduced recidivism.26 In the United Kingdom, offenders with employment at some point in the year after being released from custody were significantly less likely to re-offend than were offenders without employment.27 Another United Kingdom study reported that forensic occupational therapy practices contribute to reducing the reoffending risk.28 Furthermore, another study reported that job quality is associated with reduced criminal behaviors in high-risk released prisoners.29
Forensic psychiatric outpatients with psychotic disorders have two issues to address: the presence of a psychotic disorder and a history of criminal behavior. Consequently, improving the employment status of forensic psychiatric patients with psychotic disorders is important, as it aids in the reduction of symptoms or re-hospitalization, prevents re-offenses, and improves the QOL. However, gaining jobs is difficult for offenders with mental illnesses. A study of offenders with mental illness (n=97) showed 74.5% of the offenders were unemployed at intake and only one individual gained a job at the end of the twelve-month program.30 Only a few studies have evaluated the employment rate among forensic psychiatric outpatients after discharge from a forensic psychiatric ward.31,32 Although over half of the patients who were discharged from inpatient forensic services to a forensic community team in New Zealand achieved some degree of paid employment, the rate of full-time employment was only 12%.31 Similarly, the rate of stable employment in patients discharged from a medium security unit in the United Kingdom was 14.5%.32
On July 15, 2005, the Medical Treatment and Supervision Act (MTSA) became effective in Japan. The MTSA is the first law to render forensic mental health services mandatory for psychiatric patients judged as having diminished responsibility, including insanity, at the time of committing a crime.33 The MTSA is responsible for implementing forensic outpatient treatment orders, the duration of which is generally three years, but may be up to five years. Detailed information about the MTSA has been provided in previous domestic studies.34–37
In the Japanese legal system, individuals with personality disorders are rarely considered to have diminished responsibility. Furthermore, to receive services under the MTSA, the possibility of treatment for the psychiatric disease must exist, which is chiefly determined by the availability of an effective psychiatric drug therapy. Thus, patients with psychiatric diseases that lack an effective psychiatric drug therapy, such as dementia, intellectual disabilities, and pervasive developmental disorders, rarely receive a treatment order under the MTSA. For these reasons, patients with psychotic disorders account for approximately 80% of all forensic psychiatric inpatients.38 Consequently, the forensic psychiatric services under the MTSA have been mainly established with psychotic disorders in mind.
The aim of the present study was to determine the employment rate among forensic psychiatric outpatients with psychotic disorders who were discharged from forensic psychiatric wards. We also aimed to determine the factors associated with employment. We hypothesized that the employment rate would be low and that the seriousness of the criminal behavior leading to the treatment order under the MTSA would contribute to unemployment.
Patients and Methods
Study Design
This was a cohort study designed and conducted in collaboration with the reintegration coordinators of the Ministry of Justice and 29 forensic psychiatric wards throughout Japan. The reintegration coordinators were responsible for coordinating the social environment of the forensic outpatients during the MTSA treatment order period. The details of the study methods have been previously described.39 Participants were recruited from the 29 forensic psychiatric wards. After receiving written informed consent from the participants, their demographic data was collected from the medical records of the inpatient treatment period at each forensic psychiatric ward. Additionally, the reintegration coordinators completed questionnaires regarding the prognosis of the participants on July 15, every year during the outpatient treatment order period. The follow-up period was from the time of discharge from the forensic psychiatric wards to finishing the outpatient treatment order. During follow-up period, cases of death (Appendix 2) and dropout were finished at that time and included in the statistical analysis.
Research collaborators at each forensic psychiatric ward combined the demographic and prognosis data and submitted the dataset to the National Center of Neurology and Psychiatry Hospital, every year. We then analyzed the dataset.
Participants
Participants included patients who were mandated to receive an outpatient treatment order under the MTSA at the time of discharging from forensic psychiatric wards between July 15, 2005 and July 15, 2018. A total of 966 patients provided written informed consent to participate in this study. However, patients rarely work soon after discharge from forensic psychiatric care, as a focus on becoming comfortable with community life is preferred during the early stage of the MTSA outpatient treatment order. Thus, we decided to evaluate the highest form of employment achieved during the outpatient treatment order. As a result, we only included participants who completed their outpatient treatment order before July 15, 2018. Considering the typical working age, patients aged over 65 years at discharge from a forensic psychiatric ward were excluded. Additionally, as we focused on patients with psychotic disorders in this study, we excluded patients with other psychiatric disorders. After applying these inclusion and exclusion criteria, 406 patients remained (Figure 1).
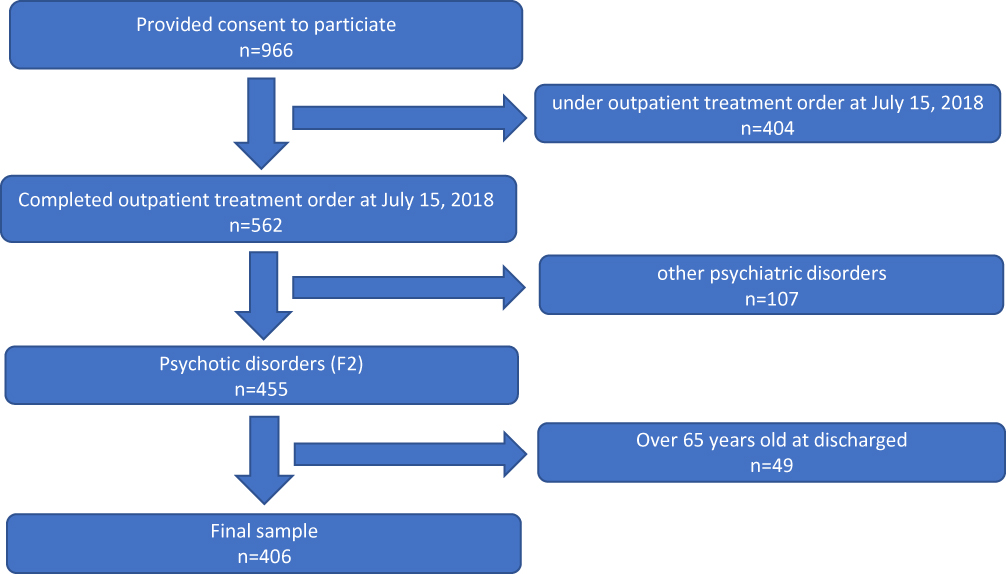 |
Figure 1 Patient selection flowchart. |
Although the observation period is different, according to a protection statistics survey from the Ministry of Justice, 2086 patients, including those with or without inpatient treatment order history, finished a forensic outpatient treatment order under the MTSA in Japan between July 15, 2005 and December 31, 2018.40 Considering the ratio of patients with direct and indirect outpatient treatment orders (23% vs. 77%),40 and the proportion of psychotic disorders (80%),41 approximately 1300 patients in Japan fit the inclusion criteria of this study. Thus, we estimated that this study included almost 30–35% of all patients in Japan who fit the inclusion criteria.
Approval of conducting this study was granted by the Ethics Committee of the National Center of Neurology and Psychiatry in accordance with the Declaration of Helsinki. Further, this study complied with the Ethical Guidelines for Medical and Health Research Involving Human Subjects, which was established by the Ministry of Education, Culture, Sports, Science and Technology, and the Ministry of Health, Labour, and Welfare in Japan.
Measures
The collected demographic data included age, sex, primary psychiatric diagnosis (based on the International Statistical Classification of Diseases and Related Health Problems, 10th version [ICD-10]), criminal behaviors leading to the MTSA treatment order (bodily injury, homicide, arson, robbery, and sexual assaults), and substance use problems (including alcohol) before admission to a forensic psychiatric ward. We defined psychotic disorders as psychiatric disorders classified as F2 in the ICD-10.
We collected data on employment status (employed or unemployed, full-time or part-time, and supported or unsupported); residence type at discharge from a forensic psychiatric ward (living with family, alone, in a welfare facility, or in a general psychiatric hospital). Employment was defined as working full-time or part-time, and supported or unsupported, but excluded welfare work.
Statistical Analysis
The student’s t test was used to compare continuous variables, including age and the follow-up duration, between patients who achieved and did not achieve employment. The Fisher’s exact test was used to compare categorical variables, including sex, history of substance use problems, type of criminal behavior, and residence type at discharge.
Exploratory univariate and multivariate logistic regression analyses were performed to determine the factors associated with employment in patients with psychotic disorders. Employment status was the dependent variable. We classified employment status into two categories, employed and unemployed, in the univariate and multivariate logistic regression analyses. The independent variables comprised age, sex, history of substance use problems, type of criminal behavior, and residence type at discharge. Age and gender were adjusted to control for possible inter-relationships between the factors in the multivariate analysis. As the degree of bodily injury inflicted by forensic inpatients varies from light to serious, the social stigma for forensic patients also varies. On the other hand, other types of criminal behaviors that are subject to the forensic treatment order under the MTSA are typically serious and create strong social stigmas for forensic psychiatric patients. Thus, we classified criminal behaviors into two categories, bodily injury and other serious crimes subject to the MTSA, in the univariate and multivariate analysis from the viewpoint of the difference in strength of social stigma.
P values <0.05 were considered statistically significant. All analyses were performed using SPSS version 24.0 (IBM Corp., Armonk, NY).
Results
During the forensic outpatient treatment order period, 56 of 406 participants achieved employment (Table 1). The mean follow-up period was 2.69±1.01 years. Overall, the mean age at discharge from the forensic psychiatric ward was 44.8±10.8 years and was significantly younger in those who achieved employment than in those who did not achieve unemployment (39.4±9.9 years vs 45.2±10.8 years, p<0.001). Men accounted for 82.3% of the study population (334/406). There was no significant difference in sex between patients who achieved and did not achieve employment. Substance use problems before admission to the forensic psychiatric ward were identified in 116 participants (28.6%) and those who achieved employment were more likely to have a history of substance use problem than were those who did not achieve employment. The most common type of criminal behavior was bodily injury (36.2%), followed by homicide (32.3%). The proportion of bodily injury criminal behavior was significantly higher in those who achieved employment (51.8%) than in those who did not achieve employment (33.5%) (p=0.001). The most common type of residence at discharge was a welfare facility (34.7%). Patients who achieved employment were more likely to live with family at discharge than were those who did not achieve employment (48.2% vs 24.3%, p=0.001); those who did not achieve employment were more likely to live in a welfare facility or be admitted to a general psychiatric hospital.
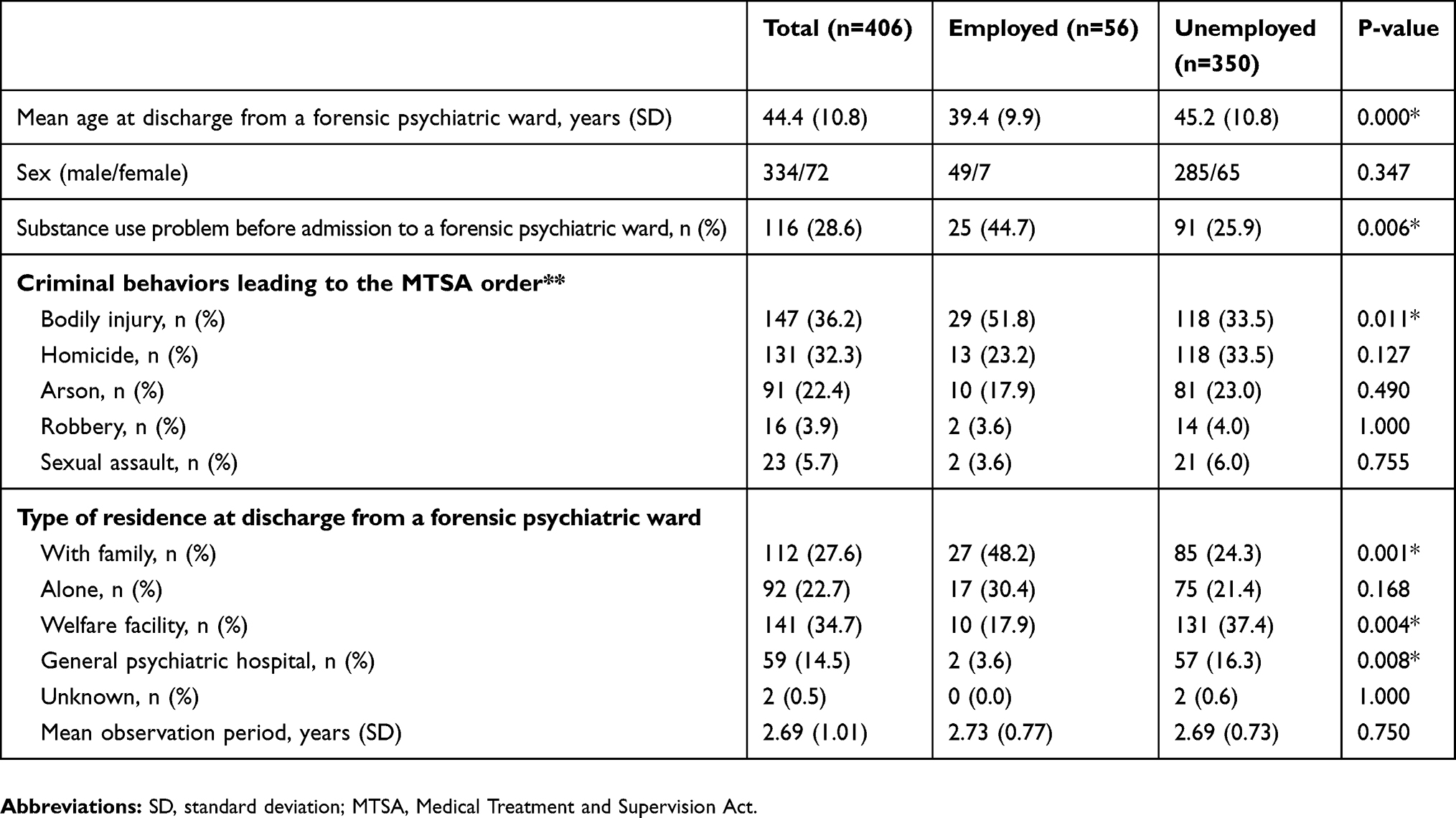 |
Table 1 Comparison Between Patients Who Achieved and Did Not Achieve Employment |
Table 2 shows the highest form of achieved employment during the MTSA outpatient treatment order. Part-time work was the highest form of achieved employment in over half of the employed patients, and 39.3% achieved full-time employment. Support service for employment was provided in 13 of 22 full-time employees (59.1%).
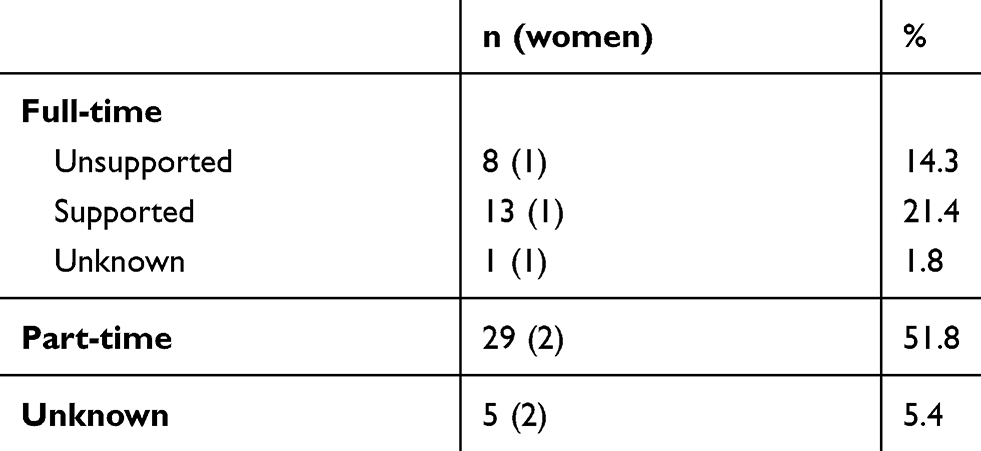 |
Table 2 Highest Form of Achieved Employment Among Patients with Psychotic Disorders (N=56) |
The multivariate logistic regression analysis showed that older age was significantly and negatively associated with employment (odds ratio [OR], 0.947; 95% confidence interval [95% CI], 0.917–0.978) (Table 3). The presence of a substance use problem before admission to the forensic psychiatric ward was significantly and positively associated with employment in the multivariate analysis (OR, 3.191; 95% CI, 1.623–6.275). Furthermore, the employment rate was significantly lower among those who committed a serious crime than among those who inflicted bodily injury (OR, 0.421; 95% CI, 0.220–0.807). Additionally, the employment rate was significantly lower among those living in a welfare facility (OR, 0.185; 95% CI, 0.078–0.437) or a general psychiatric hospital at discharge (OR, 0.121; 95% CI, 0.026–0.552) than among those living at home at discharge.
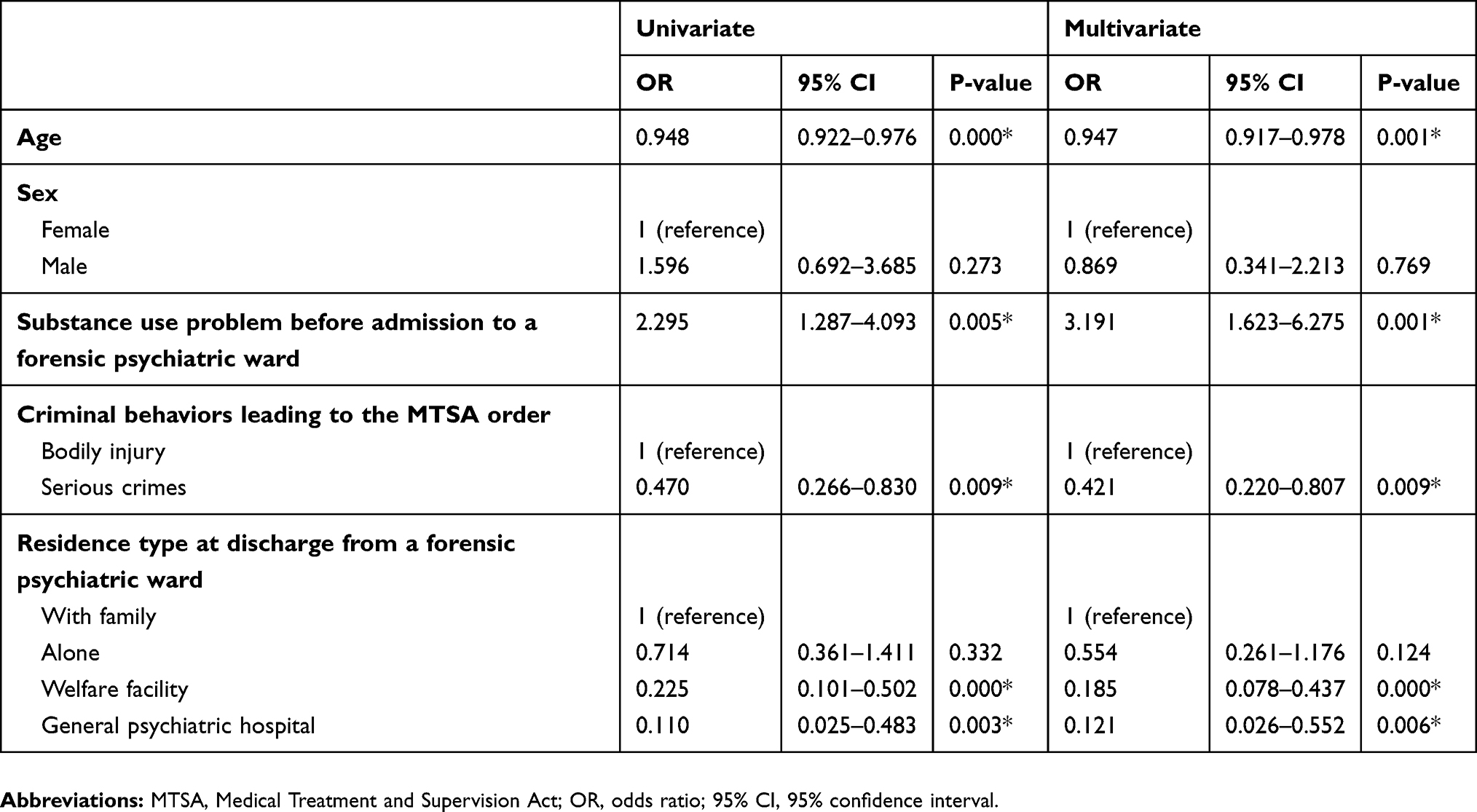 |
Table 3 Results of the Univariate and Multivariate Logistic Regression Analyses of the Factors Associated with Employment |
Discussion
This study aimed to identify the employment rate among forensic psychiatric outpatients with psychotic disorders who were discharged from forensic psychiatric wards and determine the factors related with employment. The results showed that the employment rate among forensic psychiatric outpatients with psychotic disorders is low. As expected, the employment rate was lower in those who committed serious criminal behaviors than in those who inflicted bodily injury. The employment rate of our sample was higher in those living with family than in those living in a welfare facility or a general psychiatric hospital at discharge from the forensic psychiatric ward.
The Statistics Bureau in the Ministry of Internal Affairs and Communications reported the employment rate of Japanese general population (aged 15–64 years) as 76.8%.42 The employment rate of general schizophrenia patients was 22.6% in Japan.43 As expected, the employment rate in our sample (13.8%) was significantly lower than that of the general population,42 and relatively low compared to that of general schizophrenia patients in Japan.43 The employment rate in our sample was almost the same as previous overseas studies on patients with schizophrenia (which varies considerably).13
As the highest form of achieved employment status was part-time in over half of the employed patients in present study, full-time employment rate of our study (5.4%) was lower than that of the previous forensic outpatients study in New Zealand.31 The employment rate of our study was similar to the stable employment rate in patients discharged from a medium security unit in the United Kingdom.32 However, we evaluated the employment rate regardless of the employment period; therefore, patients who worked only a few days were included in the employed group in the present study. Thus, the stable employment rate of our participants is likely to be considerably lower than 13.8%.
No previous studies have reported on the relationship between the type of criminal behavior and employment after discharge from a forensic psychiatric ward. Consistent with our hypothesis, committing a serious crime (including homicide, arson, robbery, and sexual offenses) was significantly associated with a lower employment rate than that for inflicting bodily injury. We supposed that the stigma of criminal behaviors may contribute to difficulty in job attainment. A previous study showed that a criminal record presents a major barrier to employment.44 The criminal behaviors of forensic psychiatric patients who receive a treatment order under the MTSA are not recorded in their criminal record. However, their committing serious crimes are often reported in newspapers, television news shows, and websites; the names of patients are occasionally provided. Thus, residents in their community come to know of their serious criminal behaviors through these media. The MTSA aims to reintegrate forensic psychiatric patients into their community; almost all patients return to their original community, in which they committed a crime, after discharge from the forensic psychiatric ward. Patients may struggle to find a job because of the stigma of serious criminal behaviors.
A previous study of released prisoners suggested that familial ties are associated with higher job attainment and less recidivism.45 Furthermore, a previous study of forensic psychiatric outpatients who were discharged from a medium security unit in the United Kingdom reported that stable employment was often provided by family members.32 Living with family was associated with a higher employment rate in the present study. Those who live with family may have stronger familial ties than those who do not live with family after discharge. The positive relationship between the employment rate and living with family may indicate a positive relationship between job attainment and familial ties, or providing jobs by family members as reported in previous forensic studies.32,45 Family support is related with higher psychiatric medication usage,46 and the absence of a familial caregiver is negatively associated with poor outcomes such as a high rate of homelessness and lower survival rate.47 Thus, it is probable that those who live with their family may receive beneficial support and encouragement from familial members, which may build an environment suitable for working.
As expected, older age was negatively associated with employment, which is consistent with previous studies of general patients with psychotic disorders.13 Worldwide, including Japan, men are generally more likely to work than are women.48 A previous study of general patients with schizophrenia also reported that being male is an independent positive predictor of employment.16 On the other hand, a recent study of patients with first-episode schizophrenia-spectrum disorders reported that females who receive standard care services have better employment outcomes than men.18 There was no sex difference in employment in the present study. Further research on this topic is needed, as our sample size, which included a small number of women, might have been insufficient to identify a sex difference. Additionally, it has been reported that the harmful use of alcohol is a predictor of employment loss.15 However, a history of a substance use problem was found to be a positive factor for employment in the present study after adjusting for age and gender. We were unable to interpret this result logically. Further detailed research is needed regarding the relationship between substance use history and employment in forensic psychiatric patients with psychotic disorders.
Several challenges must be met to improve the employment status in forensic psychiatric patients with psychotic disorders. First, reducing the stigma of a history of criminal behavior is important. Consequently, attempts to avoid mentioning the patient’s criminal behavior in the news and in search engines may be effective. We previously reported a low recidivism rate in forensic outpatients during the outpatient treatment order under the MTSA;49 thus, disseminating this finding and the MTSA system to the general population to may be also important to improve negative feeling towards patients from residents of their community. Second, there are few vocational programs in forensic psychiatric wards, and a specialized direct mediation system from forensic psychiatric wards to employment does not exist. Forensic psychiatric outpatients under the MTSA use the same social welfare services as general psychiatric patients, even though they have more severe problems, including dealing with the stigma of criminal behaviors, and extended periods of isolation from society (Appendix 1). A review of specific work skills programs for offenders with mental disorders reported program participants are more likely to receive paid employment.50 The establishment of employment support services specializing in forensic psychiatric patients may be effective in improving the employment status of forensic psychiatric patients with psychotic disorders. Japanese traditional vocational services are mainly designed with an emphasis on gradual training for employment based on Diathesis-stress model. Thus, severe mental disorders tend to be recommended to gradually step up from vocational facilities for people with disabilities; the same is true in forensic psychiatric patients with psychotic disorders (Appendix 1). It is well known that Individual Placement and Support (IPS) is an effective approach to improve the employment status of patients with severe mental disorders.4 Randomized controlled trials in Japan have also showed that IPS groups have a significantly higher employment rate than groups that use traditional vocational services.51,52 We should consider introducing IPS for forensic psychiatric outpatients in Japan.
Strengths
This study was conducted through collaboration with 29 of 33 established urban and local forensic psychiatric wards in Japan. Thus, the present study is one of the largest to report on the employment status of forensic psychiatric outpatients discharged from forensic psychiatric wards in Japan.
Limitations
The present study has several limitations. First, for ethical reasons, we only included patients who consented to participate; thus, we do not know the employment status of patients who did not consent to participate in our study. However, we were able to compare demographic data between the study participants and all inpatients who were mandated to inpatient treatment under the MTSA in Japan,41 even though the observation period differed. No major differences were found regarding age, sex, and type of criminal behavior leading to the MTSA treatment order. Therefore, we believe that our sample is generally representative of forensic psychiatric patients with psychotic disorders.
Second, the follow-up period was shorter in the present study than in previous studies of forensic outpatients, as the period of the forensic outpatient treatment order under the MTSA is typically three years and is at most five years. Thus, we were unable to evaluate long-term employment status after discharge from a forensic psychiatric ward. Further study is needed to evaluate changes in employment status after completing a forensic outpatient treatment order.
Third, we were unable to collect adequate information about the employment period and salary. Thus, it was difficult to classify the employment as stable or unstable, and as competitive or not. Further research is needed to describe the employment status in more detail.
Fourth, we could not collect data on several factors previously reported as associated with employment in studies of general patients with psychotic disorders (e.g. negative and cognitive symptoms, previous employment history, onset age, and education). Further research is needed to evaluate the influence of these factors on employment in forensic psychiatric patients with psychotic disorders.
Conclusion
Our study demonstrated that the employment rate among forensic psychiatric outpatients with psychotic disorders was low, and around the same as those reported in previous studies on general psychiatric patients with schizophrenia. However, this result must be treated with some caution, as the competitive or stable employment rate of our participants is likely to be considerably lower than 13.8%. Additionally, the seriousness of the criminal behavior leading to the MTSA order was negatively associated with employment.
Abbreviations
MTSA, Medical Treatment and Supervision Act; QOL, quality of life; ICD-10, International Statistical Classification of Diseases and Related Health Problems, 10th version; OR, odds ratio; 95% CI, 95% confidence interval; SD, standard deviation.
Acknowledgments
We sincerely thank the Rehabilitation Bureau of the Ministry of Justice and reintegration coordinators throughout Japan. We are also deeply grateful to members of the research group for their cooperation with the forensic psychiatric wards.
Disclosure
TK reports grants from The Ministry of Health, Labour and Welfare, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Mueser KT, Salyers MP, Mueser PR. A prospective analysis of work in schizophrenia. Schizophr Bull. 2001;27:281–296. doi:10.1093/oxfordjournals.schbul.a006874
2. McQuilken M, Zahniser JH, Novak J. The work project survey: consumer perspectives on work. J Vocat Rehabil. 2003;18:59–68.
3. Poremski D, Hwang SW. Willingness of housing first participants to consider supported-employment services. Psychiatr Serv. 2016;67(6):667–670. doi:10.1176/appi.ps.201500140
4. Kinoshita Y, Furukawa TA, Omori IM, et al. Supported employment for adults with severe mental illness. Cochrane Database Syst Rev. 2013:CD008297. doi:10.1002/14651858.CD008297.pub2.
5. Hakulinen C, Elovainio M, Arffman M, et al. Mental disorders and long-term labour market outcomes: nationwide cohort study of 2 055 720 individuals. Acta Psychiatr Scand. 2019;140:371–381. doi:10.1111/acps.v140.4
6. Organisation for Economic Co-operation and Development. Mental health and work. Available from: http://www.oecd.org/health/mental-health-and-work.htm.
7. Marwaha S, Durrani A, Singh S. Employment outcomes in people with bipolar disorder: a systematic review. Acta Psychiatr Scand. 2013;128(3):179–193. doi:10.1111/acps.2013.128.issue-3
8. Hakulinen C, Musliner KL, Agerbo E. Bipolar disorder and depression in early adulthood and long‐term employment, income, and educational attainment: A nationwide cohort study of 2,390,127 individuals. Depress Anxiety. 2019;36:1080–1088. doi:10.1002/da.v36.11
9. Marwaha S, Johnson S, Bebbington P, et al. Rates and correlates of employment in people with schizophrenia in the UK, France and Germany. Br J Psychiatry. 2007;191:30–37. doi:10.1192/bjp.bp.105.020982
10. Thornicroft G, Tansella M, Becker T, et al. The personal impact of schizophrenia in Europe. Schizophr Res. 2004;69(2–3):125–132. doi:10.1016/S0920-9964(03)00191-9
11. Fleischhacker WW, Arango C, Arteel P, et al. Schizophrenia—time to commit to policy change. Schizophr Bull. 2014;40(Suppl 3):S165–S194. doi:10.1093/schbul/sbu006
12. Hakulinen C, McGrath JJ, Timmerman A, et al. The association between early‑onset schizophrenia with employment, income, education, and cohabitation status: nationwide study with 35 years of follow‑up. Soc Psychiatry Psychiatr Epidemiol. 2019;54:1343–1351. doi:10.1007/s00127-019-01756-0
13. Bouwmans C, de Sonneville C, Mulder CL, Hakkaart-van Roijen L. Employment and the associated impact on quality of life in people diagnosed with schizophrenia. Neuropsychiatr Dis Treat. 2015;11:2125–2142. doi:10.2147/NDT.S83546
14. Marwaha S, Johnson S. Schizophrenia and employment - a review. Soc Psychiatry Psychiatr Epidemiol. 2004;39(5):337–349. doi:10.1007/s00127-004-0762-4
15. Marwaha S, Johnson S, Bebbington PE, et al. Predictors of employment status change over 2 years in people with schizophrenia living in Europe. Epidemiol Psichiatr Soc. 2009;18(4):344–351. doi:10.1017/S1121189X00000324
16. Üçok A, Gorwood P, Karadayı G; EGOFORS. Employment and its relationship with functionality and quality of life in patients with schizophrenia: EGOFORS Study. Eur Psychiatry. 2012;27(6):422–425. doi:10.1016/j.eurpsy.2011.01.014
17. Hofer A, Bodner T, Kaufmann A, et al. Symptomatic remission and neurocognitive functioning in patients with schizophrenia. Psychol Med. 2011;41(10):2131–2139. doi:10.1017/S0033291711000353
18. Chan SKW, Pang HH, Yan KK, et al. 10-year employment patterns of patients with first-episode schizophrenia-spectrum disorders: comparison of early intervention and standard care services. Br J Psychiatry. 2019;9:1–7. doi:10.1192/bjp.2019.161
19. Tsang HWH, Leung AY, Chung RCK. Review on vocational predictors: a systematic review of predictors of vocational outcomes among individuals with schizophrenia: an update since 1998. Aust N Z J Psychiatry. 2010;44(6):495–504.
20. Gunnmo P, Bergman HF. What do individuals with schizophrenia need to increase their well-being. Int J Qual Stud Health Well-Being. 2011;6(1). doi:10.3402/qhw.v6i1.5412
21. Sariah AE, Outwater AH, Malima KI. Risk and protective factors for relapse among individuals with schizophrenia: a qualitative study in Dar es Salaam, Tanzania. BMC Psychiatry. 2014;14:240. doi:10.1186/s12888-014-0240-9
22. Luciano A, Bond GR, Drake RE. Does employment alter the course and outcome of schizophrenia and other severe mental illnesses? A systematic review of longitudinal research. Schizophr Res. 2014;159:312–321. doi:10.1016/j.schres.2014.09.010
23. Durose MR, Cooper AD, Snyder HN. Recidivism of prisoners released in 30 states in 2005: patterns from 2005 to 2010. BJS Statisticians; 2014. Available from: https://www.bjs.gov/content/pub/pdf/rprts05p0510.pdf.
24. National Reentry Resource Center [homepage on the Internet]. About the National Reentry Resource Center. Available from: https://csgjusticecenter.org/nrrc/about.
25. Justice Center, The Council of State Governments; The National Reentry Resource Center. Reducing recidivism: states deliver results; 2018. Available from: https://csgjusticecenter.org/wp-content/uploads/2018/11/StatesDeliverResults-2018.pdf.
26. Manikandan S, Latha S. Employment reduces recidivism: an overview of employment based rehabilitation in India. Indian Soc Sci J. 2017;6(2):1–8
27. Ministry of Justice. Analysis of the impact of employment on re-offending following release from custody, using propensity score matching; 2013. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/217412/impact-employment-reoffending.pdf.
28. Connell C. Forensic occupational therapy to reduce risk of reoffending: a survey of practice in the United Kingdom. J Forens Psychiatry Psychol. 2016;27:907–928. doi:10.1080/14789949.2016.1237535
29. Uggen C. Ex-Offenders and the conformist alternative: a job quality model of work and crime. Soc Probl. 1999;46(1):127–151. doi:10.2307/3097165
30. Sneed Z, Koch DS, Estes H. Employment and psychosocial outcomes for offenders with mental illness. Int J Psychosocial Rehab. 2006;10(2):103–112.
31. Simpson AI, Jones RM, Evans C, McKenna B. Outcome of patients rehabilitated through a New Zealand forensic psychiatry service: a 7.5 year retrospective study. Behav Sci Law. 2006;24(6):833–843. doi:10.1002/bsl.740
32. Davies S, Clarke M, Hollin C, Duggan C. Long-term outcomes after discharge from medium secure care: a cause for concern. Br J Psychiatry. 2007;191:70–74. doi:10.1192/bjp.bp.106.029215
33. The Medical Treatment and Supervision Act of 2003, Pub. L. No. 110 of 2003 [in Japanese]; 2005. Available from: https://elaws.e-gov.go.jp/search/elawsSearch/elaws_search/lsg0500/detail?lawId=415AC0000000110.
34. Ando K, Soshi T, Nakazawa K, Noda T, Okada T. Risk factors for problematic behaviors among forensic outpatients under the medical treatment and supervision act in Japan. Front Psychiatry. 2016;7:144. doi:10.3389/fpsyt.2016.00144
35. Fujii C, Fukuda Y, Ando K, Kikuchi A, Okada T. Development of forensic mental health services in Japan: working towards the reintegration of offenders with mental disorders. Int J Ment Health Syst. 2014;8:21. doi:10.1186/1752-4458-8-21
36. Nakatani Y. Challenges in interfacing between forensic and general mental health: a Japanese perspective. Int J Law Psychiatry. 2012;35(5–6):406–411. doi:10.1016/j.ijlp.2012.09.021
37. Nakatani Y, Kojimoto M, Matsubara S, Takayanagi I. New legislation for offenders with mental disorders in Japan. Int J Law Psychiatry. 2010;33(1):7–12. doi:10.1016/j.ijlp.2009.10.005
38. Ministry of Health, Labour and Welfare. State of patients who have been ordered inpatient order under the MTSA [in Japanese]. Available from: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/hukushi_kaigo/shougaishahukushi/sinsin/nyuin.html.
39. Takeda K, Sugawara N, Matsuda T, et al. Mortality and suicide rates in patients discharged from forensic psychiatric wards in Japan. Compr Psychiatry. 2019;95:152131. doi:10.1016/j.comppsych.2019.152131
40. Ministry of Justice. Protection statistics survey. Available from: http://www.moj.go.jp/housei/toukei/toukei_ichiran_hogo.html.
41. Kono T. Monitoring report for designated forensic psychiatric institutions [in Japanese]. In Okada T, editor. Report for the Medical Treatment and Supervision Act [Internet]. Tokyo: Department of Forensic Psychiatry, National Institute of Mental Health, National Center of Neurology and Psychiatry; 2017:7–28. Available from: https://www.ncnp.go.jp/nimh/chiiki/documents/04-01.pdf.
42. Statistics Bureau, Ministry of Internal Affairs and Communications. Labor force survey. Available from: https://www.stat.go.jp/data/roudou/sokuhou/nen/ft/pdf/index1.pdf.
43. Ministry of Health, Labour and Welfare. Report on the survey of employment conditions in people with psychiatric disorders. Available from: http://www.nivr.jeed.or.jp/download/houkoku/houkoku95.pdf.
44. Pager D. The mark of a criminal record. Am J Sociol. 2003;108(5):937–975. doi:10.1086/374403
45. Berg MT, Huebner BM. Reentry and the ties that bind: an examination of social ties, employment, and recidivism. Justice Q. 2011;28(2):382–410. doi:10.1080/07418825.2010.498383
46. Garcia JIR, Chang CL, Young JS, et al. Family support predicts psychiatric medication usage among Mexican American individuals with schizophrenia. Soc Psychiatry Psychiatr Epidemiol. 2006;41:624–631. doi:10.1007/s00127-006-0069-8
47. Ran MS, Chui CHK, Wong IYL. Family caregivers and outcome of people with schizophrenia in rural China: 14-year follow-up study. Soc Psychiatry Psychiatr Epidemiol. 2016;51:513–520. doi:10.1007/s00127-015-1169-0
48. International Labour Organization. Gender gap in labour force participation rates; 2018. Available from: https://www.ilo.org/infostories/en-GB/Stories/Employment/barriers-women#global-gap/labour-force.
49. Takeda K, Nagata T, Sugawara N, et al. Recidivism and suicide rate of patients discharged from forensic psychiatric wards in Japan. In:
50. Talbot EC, Völlm B, Khalifa N. Effectiveness of work skills programmes for offenders with mental disorders: a systematic review. Crim Behav Ment Health. 2017;27(1):40–58. doi:10.1002/cbm.v27.1
51. Yamaguchi S, Sato S, Horio N, et al. Cost-effectiveness of cognitive remediation and supported employment for people with mental illness: a randomized controlled trial. Psychol Med. 2017;47:53–65. doi:10.1017/S0033291716002063
52. Oshima I, Sono T, Bond G, et al. A randomized controlled trial of individual placement and support in Japan. Psychiatr Rehabil J. 2014;37(2):137–143. doi:10.1037/prj0000085
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.