")
Back to Journals » Advances in Medical Education and Practice » Volume 5
Empathy levels among health professional students: a cross-sectional study at two universities in Australia
Authors Williams B , Brown T, McKenna L , Boyle M, Palermo C, Nestel D, Brightwell R, McCall L, Russo V
Received 14 November 2013
Accepted for publication 22 January 2014
Published 3 May 2014 Volume 2014:5 Pages 107—113
DOI https://doi.org/10.2147/AMEP.S57569
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Brett Williams,1 Ted Brown,2 Lisa McKenna,3 Malcolm J Boyle,1 Claire Palermo,4 Debra Nestel,5 Richard Brightwell,6 Louise McCall,7 Verity Russo1
1Department of Community Emergency Health and Paramedic Practice, 2Department of Occupational Therapy, 3School of Nursing and Midwifery, 4Department of Nutrition and Dietetics, 5School of Rural Medicine, Monash University, Melbourne, VIC, 6School of Medical Sciences, Edith Cowan University, Perth, WA, 7Faculty of Medicine, Nursing and Health Sciences, Monash University, Melbourne, VIC, Australia
Background: Empathy is paramount in the health care setting, optimizing communication and rapport with patients. Recent empirical evidence suggests that empathy is associated with improved clinical outcomes. Therefore, given the importance of empathy in the health care setting, gaining a better understanding of students' attitudes and self-reported empathy is important. The objective of this study was to examine self-reported empathy levels of students enrolled in different health disciplines from two large Australian universities.
Materials and methods: A total of 1,111 students from two different universities enrolled in eight different health professions were administered the Jefferson Scale of Physician Empathy – Health Profession Students version, a 20-item 7-point Likert scale questionnaire to evaluate self-reported empathy levels.
Results: A total of 1,111 students participated in this study. The majority of participants were from Monash University (n=771), with 340 students from Edith Cowan University. No statistically significant differences were found between universities: Monash University (mean 110.1, standard deviation [SD] 11.8); Edith Cowan University (mean 109.2, SD 13.3, P=0.306). The mean female empathy score (mean 110.8, SD 11.7) was significantly higher than the mean male score (mean 105.3, SD 13.5; P<0.0001; d=0.44). Paramedic students had significantly lower empathy scores (mean 106.3, SD 12.73) than all other participants except nursing students (P<0.0001).
Conclusion: Results relating to sex are reflective of previous studies. There is some discrepancy in results relating to empathy and its incline/decline as students progress through a program. Further study is warranted to explore why there are variations in empathy levels in students of different health disciplines.
Keywords: empathy, health care professions
A Letter to the Editor has been received and published for this article.
Introduction
Empathy is the ability to “stand in the shoes of another”: to consider a situation from someone else’s point of view and thereby gain a greater understanding into their perspective.1 Despite being considered an enigmatic concept,2 empathy is almost universally valued by the “helping” professions.3 In the context of health care specifically, Hojat et al define empathy as “a predominantly cognitive attribute that involves an understanding of the patient’s experiences, concerns, and perspectives, combined with a capacity to communicate this understanding and an intention to help”.4 It is thought to be manifested consciously, and is nonjudgmental.5 In contrast, sympathy lacks a cognitive element.6 Instead, it relates more to emotion and the development of feelings for a patient,7,8 as does pity. Sympathy is considered an affective response, which could interfere in the objectivity required in medical assessment and treatment.9
In the health care setting, empathy is paramount10 and is widely recognized as a key component to effective communication,9 establishing rapport,11,12 and achieving optimal outcomes in patient care.1 It is suggested that empathy improves patient satisfaction,8,13,14 increases patient engagement15 and motivation,12 improves compliance with treatment,14–16 and lowers the rates of patient litigation.17–19 Similarly, it is suggested that higher empathy levels contribute to more accurate diagnoses.15 Most recently, it was found that higher empathy levels in physicians were associated with improved clinical outcomes.4,20 The outcomes of these studies are significant. Not only could this optimize patient care and management, but it has the capacity to reduce financial demands on the health care system. It may be that an empathetic approach may result in a shorter treatment period or reduced demand on resources.
The literature on empathy reports that females are generally more empathetic than males,1,6,9,15,21,22 and that often empathy declines as a student progresses through their course of study.9,15,23 As a cognitive attribute, there are grounds to assume that empathy can be taught. It has been suggested that effective educational programs might facilitate and improve empathetic skills.24 Similarly, a recent study found that 81% of students felt “better prepared” after empathy-based training.2 Hojat et al is of the opinion that empathy is “neither a highly stable personality trait, nor a state that can be changed without effort”.7,8 He suggests that empathy is rooted in evolutionary, genetic, developmental, experiential, situational, and educational ground, and its deficit can be improved.7,8
The universities involved in this study – Monash University and Edith Cowan University – have well-established medical and health care professional programs, and describe empathy as an institutional graduate attribute. Students involved in this study included those in 3-year (ie, nursing), 4-year (ie, physiotherapy), and 5-year (ie, medicine) degree programs. Given the importance of empathy in the health care setting, gaining a better understanding of students’ attitudes and self-reported empathy is important both in terms of curriculum consistency and also whether empathy levels differ by year of study and health care professions. The objective of this study was to examine self-reported empathy levels of students enrolled in different health disciplines from two large Australian universities.
Materials and methods
Participants
This was a cross-sectional study using a paper-based questionnaire. Students were enrolled at either Monash University or Edith Cowan University and enrolled in the following health care programs: paramedics (the term “paramedic” in Australia refers to a highly trained clinician and autonomous health professional who works with an emergency out-of-hospital ambulance service. Paramedics have all formally completed an undergraduate or postgraduate paramedic degree). Midwifery, nursing, paramedic/nursing, occupational therapy, physiotherapy, medicine, or nutrition and dietetics. Participants were in either the first, second, third, or fourth year of their program. Inclusion criteria for the study were being enrolled in one of the above programs and consenting to take part in the study. Approval was obtained from Monash University and Edith Cowan University human ethics committees prior to the commencement of the study.
Instrumentation
The Jefferson Scale of Physician Empathy – Health Profession Students (JSPE-HPS) version (adapted from Hojat et al)25 was administered to students to examine self-reported empathy levels. The JSPE-HPS version is reworded so it is specific to health care providers generally, not just physicians. Designed as a 20-item 7-point Likert scale (1= strongly disagree, 7= strongly agree), the JSPE-HPS version is designed to be completed without time constraints. Ten of the items are positively worded, while the other ten are negatively worded. The possible score range is 20–140: the higher the mean score, the higher the self-reported empathy level. There is evidence to support the reliability and validity of the JSPE, including the HPS version.8,26 A short demographic questionnaire was also included.
Procedures
Participants were advised of the project and its aims following a lecture during the academic schedule in April 2012. Participants were provided with an explanatory statement and were informed that participation was voluntary. The questionnaire took students approximately 10 minutes to complete, and consent was implied by its completion and submission.
Data analysis
SPSS (IBM, Armonk, NY, USA) was used for data storage, tabulation, and the generation of descriptive and inferential statistics. Descriptive statistics means and standard deviations (SDs) were used to summarize the demographic data. Independent-sample Student’s t -tests and one-way analyses of variance, including post hoc tests, were used to compare the differences between health care professions, age-groups, sex, year of study, and university. All tests were two-tailed, with the results considered statistically significant if the P-value was <0.05; effect sizes (d) were also calculated for quantifying the differences between mean scores.
Results
Demographic results
The majority of participants were from Monash University (n=771, 96.4%), with 340 (30.6%) students from Edith Cowan University. The majority of students were female (n=907, 81.6%), and just under half (46.6%, n=518) were in the 20- to 24-year age bracket. One in four students (n=440, 39.6%) were in the first year of their course. The majority of participants were midwifery students (n=349, 31.4%), 247 (22.2%) were nursing students, and 184 (16.6%) were paramedic students.
Dimensionality of the JSPE-HPS version
While the JSPE has well-established construct validity, dimensionality, and reliability, the same level of widespread psychometric examination of the JSPE-HPS version has not yet been examined. In a recent paper by Williams et al,26 the authors performed a confirmatory factor analysis using 330 paramedic students, and found that a two-factor 17-item JSPE-HPS version produced a better model fit. In another study by Fjortoft et al,27 the research team used exploratory factor analysis to achieve scale parsimony with a two-factor 20-item structure. Therefore, given the underexamination of the JSPE-HPS version, an exploratory factor analysis was undertaken to further appraise the construct validity and dimensionality.
A factor analysis with oblimin rotation was performed to understand the dimensionality of the JSPE-HPS version better, using Kaiser’s criteria28 (an eigenvalue greater than 1.25 was used),29 cumulative, scree test,30 and percentage of variance extracted,31 and only retaining items if coefficients were equal to or greater than 0.30.32 Results from the factor analysis demonstrated a three-factor solution, with one item being deleted (see Table 1). This result accounted for 39.38% of the total explained variance.
There were ten items that loaded on subscale 1 (perspective taking), with item loadings ranging from 0.65 to 0.40 and explaining 23.03% of the variance. The top item within the factor was, “Health care providers’ understanding of the emotional status of the patients, as well as that of their families, is one important component of the health care provider–patient relationship”.
There were three items that loaded on subscale 2 (patient perceptions), with item loadings ranging from 0.79 to 0.40 and explaining 9.32% of the variance. The top item within the factor was, “Because people are different, it is difficult to see things from patients’ perspectives”. There were six items that loaded on subscale 3 (compassionate care), with item loadings ranging from −0.74 to −0.44 and explaining 7.02% of the variance. The top item within the factor was, “Attentiveness to patients’ personal experiences does not influence treatment outcomes”.
Item 18 – “Health care providers should not allow themselves to be influenced by strong personal bonds between patients and their family members” – failed to meet the factor-extraction criteria and was not retained in further analyses. Two items cross-loaded: item 14 (“I believe that emotion has no place in the treatment of medical illness”) and item 11 (“Patients’ illnesses can be cured only by targeted treatment; therefore, health care providers’ emotional ties with their patients do not have a significant influence in treatment outcomes”.
Item-level results
A number of items produced high mean scores: “Patients feel better when their health care providers understand their feelings” (mean 6.31, SD 1.02), while the item, “I believe that empathy is an important factor in patients’ treatment” produced a mean score of 6.07 (SD 1.05). The item, “Because people are different, it is difficult to see things from patients’ perspectives” yielded a mean of 4.43 (SD 1.57). Full item-level results can be seen in Table 1.
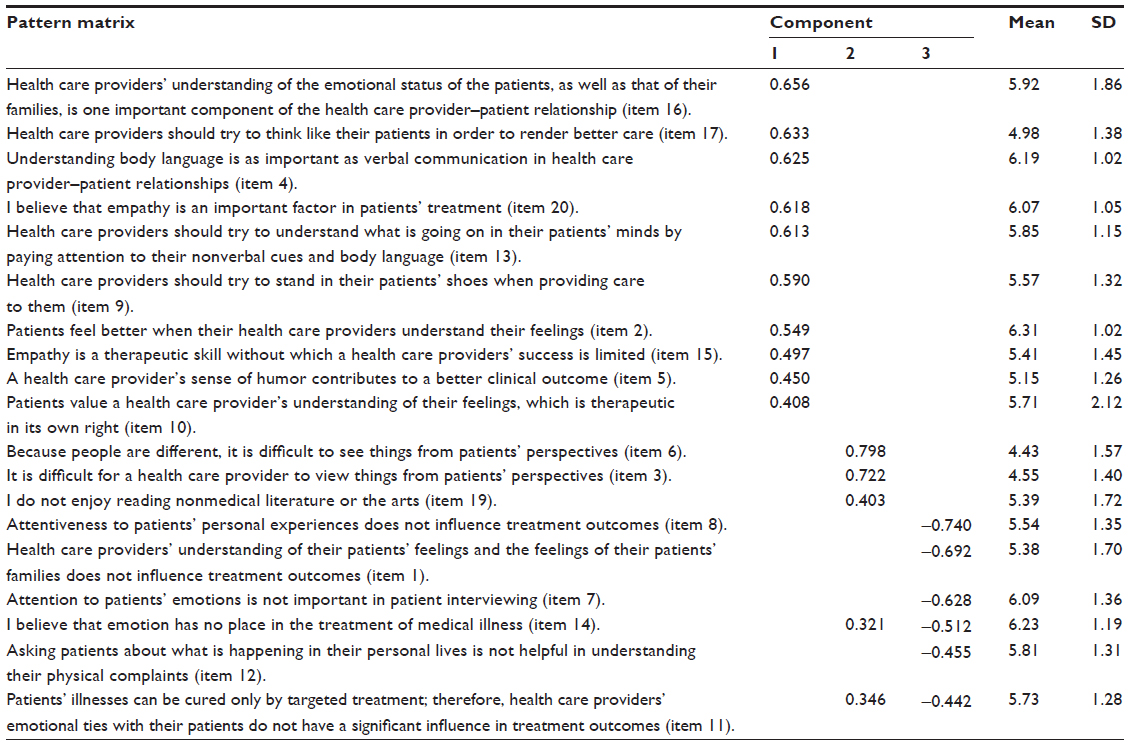 | Table 1 Factor analysis (oblimin rotation) and mean scores of Jefferson Scale of Physician Empathy – Health Profession Students version |
Jefferson empathy mean score comparisons
No statistically significant differences in overall empathy mean scores were found between participants from either university: Monash University, mean 110.1, SD 11.8; Edith Cowan University, mean 109.2, SD 13.3; P=0.306. The mean female empathy score (110.8, SD 11.7) was significantly higher than the mean male score (105.3, SD 13.5, P<0.0001; d=0.44). Paramedic students had significantly lower empathy scores (mean 106.3, SD 12.73) than all other participants except nursing students (P<0.0001). The full distribution of results can be seen in Table 2.
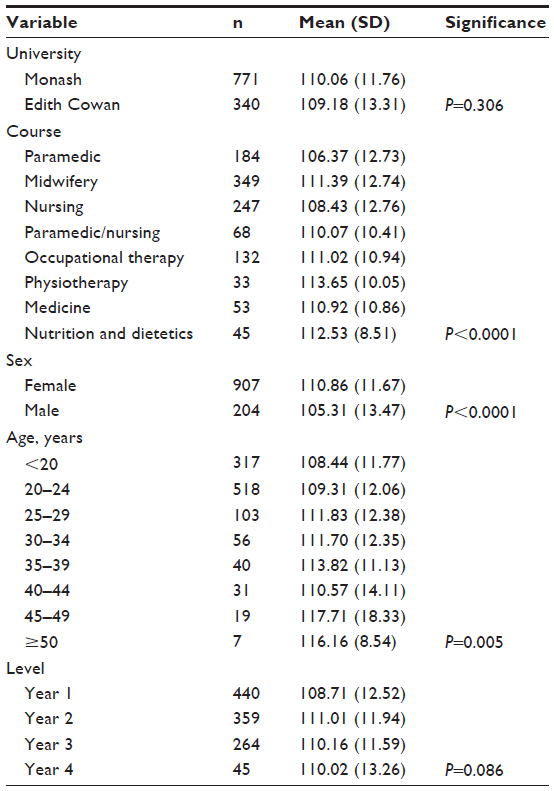 | Table 2 Jefferson Scale of Physician Empathy – Health Profession Students version mean comparison scores across different variables |
Empathy scores increased from the first year to second year of study (P=0.012; d=0.18) but no significant change in later years was observed. Analysis of empathy scores across year of study and health professions was also undertaken. This revealed a general trend of empathy scores declining from first to final year across the majority of professions, although this was not statistically significant (Table 3). Students in the 25- to 29-year age bracket self-reported higher empathy scores than those <20 years of age (P=0.015; d= 0.28), as did students in the 35- to 39-year age bracket (P=0.009; d=0.46).
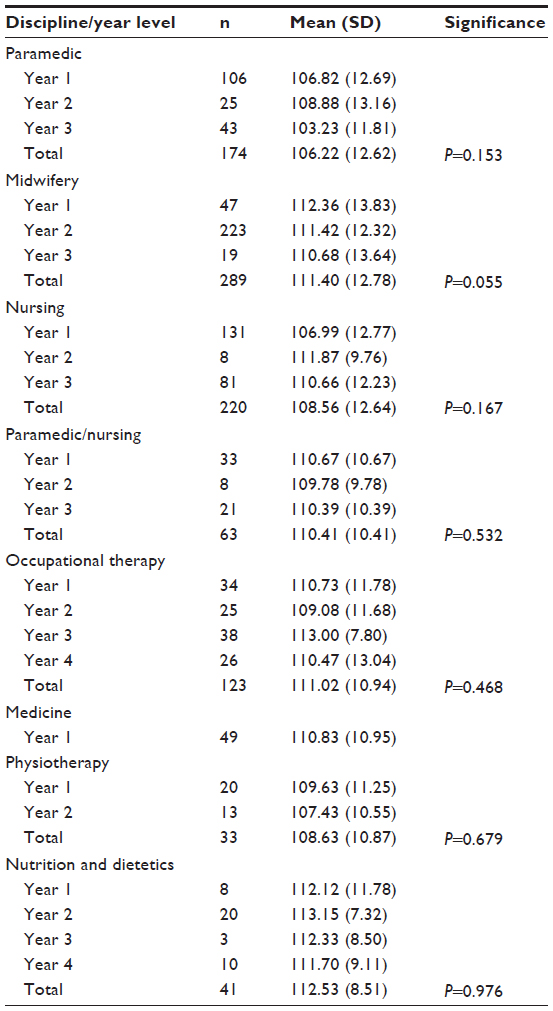 | Table 3 Jefferson Scale of Physician Empathy – Health Profession Students version level mean comparison scores across different health professions |
The internal consistency of the JSPE-HPS version was measured using Cronbach’s α-coefficient. In this study, the JSPE-HPS demonstrated good reliability – α=0.78. The value of 0.78 is well above the accepted benchmark value of 0.70 required for adequate internal consistency, particularly for new measures, such as the JSPE-HPS version.33
Discussion
This study examined empathy levels in students from different health disciplines. It was found that paramedic students had statistically lower empathy results than all other health professions except nursing students. We speculate the reason for this is the similarities between their roles and skill sets in Australia. Females had higher empathy scores than males, empathy scores increased from the first year to the second year of study, but did not significantly increase/decrease after this, and there were significant differences between certain age-groups. These cross-sectional findings provide important information in attempting to better understand undergraduate students’ self-reported empathy in Australia.
Few studies have examined variations in empathy levels among multiple health care providers, such as in our study.21 A recent paper by Boyle et al34 found no significant difference in empathy levels in Australian undergraduate students enrolled in paramedics, nursing, midwifery, occupational therapy, physiotherapy, and health sciences. Nunes et al15 looked at empathy levels in students enrolled in dentistry, pharmacy, medicine, veterinary medicine, and nursing, and found that nursing students and dental students had higher empathy scores than all other participants.15
However, a number of studies have considered one specific cohort of students. Sherman and Cramer looked at empathy levels among dental students, and found that first-year students had higher empathy levels than students in later years.9 Ward et al conducted a longitudinal study involving 214 nursing students, and found that empathy levels declined in students who were exposed to more patient encounters.35 This was also found by Ward et al.22 McKenna et al also looked at empathy levels in nursing students, and found that there were no significant differences in empathy relating to age, sex, or year of study,42 quite similar to the results found in our research.
Due to the growing emphasis on interprofessional collaboration within health care systems21 and the recent finding that empathy is associated with positive clinical outcomes,4,20 it is important to consider and examine empathy levels across health disciplines. These data from our study provide important baseline information from which educational activities can be tailored toward health care professions.
It would be of interest to ascertain why paramedic students reported the lowest empathy levels among the eight professions. Other studies have also shown low empathy scores among paramedic students.36,37 As out-of-hospital emergency workers, paramedics are regularly exposed to pain and suffering in often-unpredictable situations and environments.9 Often, they are the first health care providers to a scene, in which case they are normally the first to assess, treat, and manage the patient to hospital. In these critical situations, paramedics must be able to set limits; they need to manage both the situation and their own reactions.38 It may be that in order to do both, empathy levels are compromised.39 Similarly, lower empathy scores among paramedic students may be related to the unpredictable and dangerous nature of their job, although this might be better answered using qualitative methodologies. Alternatively, one could hypothesize that people drawn to paramedics as a career are by nature less empathetic. Empathy, it is suggested, has a genetic root (in addition to several others).8 This may potentially add strength to this suggestion.
Differences in courses and teaching may also have contributed to the variations noted. Physiotherapy students, whose mean empathy score was higher than all other health disciplines examined, may be exposed to more empathy-based education and training. Alternatively, they may be privy to a different kind of training or teachers who themselves are more empathetic in nature, which may impact student empathy levels. This is worth further examination using curricula benchmarking to better assess the levels of empathy education and assessment in undergraduate programs. Given the evidence that empathy is amenable to change7 and is therefore worth teaching,8,24,40 it is worth assessing whether empathy-related subjects and programs within health-discipline courses can be improved.
Positive associations have been found between agreeableness, openness to experience, and empathy.41 With this knowledge, it is worth considering if certain personalities (who are more agreeable or open to experience) are drawn to certain professions; it may be that these traits are more prolific in physiotherapy students and nutrition and dietetic students than paramedic students, for example.
As noted in several previous studies1,6,9,15,21,22 females were found to have higher empathy levels than males. This finding was reiterated in this study, adding more data to the body of knowledge. Explanations for these results are worth considering. Similarly, the traditional and evolutionary role of women as caregivers may also explain noted variations in empathy levels between males and females, as may the possibility that perhaps females are more perceptive to emotions, or that males take a more rational rather than emotive approach.9
While some recent studies suggest that empathy levels decline as a student progresses through a program,15,35 this study found that empathy levels increased from the first year to the second year of study and did not significantly change after this. It would be worth exploring the innumerable factors that may contribute to these results, such as experiences during student placements and mentoring during study.
Similarly, there is some evidence to suggest that older students have higher empathy levels than younger students.15,21 These findings are supported in this study, with significant differences noted between students <20 years old and students between the ages of 25–29 and 35–39 years; and between students 20–24, 35–39, and 45–49 years old. It has been suggested that increased life experience increases empathy levels.22 Experiences of love and loss, pain and regret, and suffering and loneliness may enable a person to consider the effect of these experiences on others.
Limitations
A number of limitations of this study exist. Firstly, self-reported measures, such as the JSPE-HPS version, have respondent bias and in no way reflect what might occur in actual clinical practice. Secondly, convenience sampling, while easier to recruit participants for, limits the capacity to control for nonrespondent bias. Thirdly, given the cross-sectional nature of this study, we were unable to control for clinical placement experience or the level of empathy training or assessment. We would encourage further work in this area to undertake formal curricula alignment and course mapping of empathy pedagogy and assessment to better gauge the level of significance across different variables.
Other recommendations for future research include longitudinally based designs that monitor empathy levels at each year of students’ health care program; ideally, this design should also include postqualification measurement. Further psychometric work is required examining the JSPE-HPS version; results from this study highlight a poor total explained variance suggestive of other latent variables.
Conclusion
A variation in empathy levels is recognized between students of different health care disciplines. There is a significant difference between paramedic students and all other participants, except nursing students. It is worth investigating why this may be. Further study of the teaching of empathy would also be of value. Results regarding sex and empathy levels are reflective of previous studies.
Acknowledgments
We would like to acknowledge the Office for Learning and Teaching, who provided funding for this project to take place. We would also like to thank the students who completed the questionnaire.
Disclosure
The authors report no conflicts of interest in this work.
References
Kataoka HU, Koide N, Ochi K, Hojat M, Gonnella JS. Measurement of empathy among Japanese medical students: psychometrics and score differences by gender and level of medical education. Acad Med. 2009;84(9):1192–1197. | |
Regehr C, Goldberg G, Hughes J. Exposure to human tragedy, empathy, and trauma in ambulance paramedics. Am J Orthopsychiatry. 2002;72(4):505–513. | |
Williams CA. Empathy and burnout in male and female helping professionals. Res Nurs Health. 1989;12(3):169–178. | |
Hojat M, Louis DZ, Markham FW, Wender R, Rabinowitz C, Gonnella JS. Physicians’ empathy and clinical outcomes for diabetic patients. Acad Med. 2011;86(3):359–364. | |
Forsyth GL. Analysis of the concept of empathy: illustration of one approach. ANS Adv Nurs Sci. 1980;2(2):33–42. | |
Suh D, Hong J, Lee D, Gonnella J, Hojat M. The Jefferson Scale of Physician Empathy: a preliminary psychometric study and group comparisons in Korean physicians. Med Teach. 2012;34(6):e464–e468. | |
Hojat M, Louis DZ, Maio V, Gonnella JS. Empathy and health care quality. Am J Med Qual. 2013;28(1):6–7. | |
Hojat M. Empathy in Patient Care: Antecedents, Development, Measurement and Outcomes. New York: Springer; 2007. | |
Sherman JJ, Cramer A. Measurement of changes in empathy during dental school. J Dent Educ. 2005;69(3):338–345. | |
Gosselink MJ, Witteveen T. Growth in empathy during clinical exchange. Clin Teach. 2012;9(3):188–189. | |
Brown T, Williams B, Boyle M, et al. Levels of empathy in undergraduate occupational therapy students. Occup Ther Int. 2010;17(3):135–141. | |
Squier RW. A model of empathic understanding and adherence to treatment regimens in practitioner-patient relationships. Soc Sci Med. 1990;30(3):325–339. | |
Bertakis KD, Putnam SM, Roter D. The relationship of physician medical interview style to patient satisfaction. J Fam Pract. 1991;32(2):175–181. | |
Zachariae R, Pedersen CG, Jensen AB, Ehrnrooth E, Rossen PB, von der Maase H. Association of perceived physician communication style with patient satisfaction, distress, cancer-related self-efficacy, and perceived control over the disease. Br J Cancer. 2003;88(5):658–665. | |
Nunes P, Williams S, Sa B, Stevenson K. A study of empathy decline in students from five health disciplines during their first year of training. Int J Med Educ. 2011;2:12–17. | |
DiMatteo MR, Sherbourne CD, Hays RD, et al. Physicians’ characteristics influence patients’ adherence to medical treatment: results from the Medical Outcomes Study. Health Psychol. 1993;12(2):93–102. | |
Moore PJ, Adler NE, Robertson PA. Medical malpractice: the effect of doctor-patient relations on medical patient perceptions and malpractice intentions. West J Med. 2000;173(4):244–250. | |
Levinson W, Roter DL, Mullooly JP, Dull VT, Frankel RM. Physician-patient communication. The relationship with malpractice claims among primary care physicians and surgeons. JAMA. 1997;277(7):553–559. | |
Beckman HB, Markakis KM, Suchman AL, Frankel RM. The doctor-patient relationship and malpractice. Lessons from plaintiff depositions. Arch Intern Med. 1994;154(12):1365–1370. | |
Del Canale S, Louis DZ, Maio V, et al. The relationship between physician empathy and disease complications: an empirical study of primary care physicians and their diabetic patients in Parma, Italy. Acad Med. 2012;87(9):1243–1249. | |
Fields S, Mahan P, Tillman P, Harris J, Maxwell K, Hojat M. Measuring empathy in healthcare profession students using the Jefferson Scale of Physician Empathy: health provider – student version. J Interprof Care. 2011;25(4):287–293. | |
Ward J, Schaal M, Sullivan J, Bowen ME, Erdmann JB, Hojat M. Reliability and validity of the Jefferson Scale of Empathy in undergraduate nursing students. J Nurs Meas. 2009;17(1):73–88. | |
Hojat M, Mangione S, Nasca TJ, et al. An empirical study of decline in empathy in medical school. Med Educ. 2004;38(9):934–941. | |
Ozcan CT, Oflaz F, Bakir B. The effect of a structured empathy course on the students of a medical and a nursing school. Int Nurs Rev. 2012;59(4):532–538. | |
Hojat M, Mangione S, et al. (2001). The Jefferson Scale of Physician Empathy: Development and Preliminary Psychometric Data. Educational and Psychological Measurement. 61(2):349–365. | |
Williams B, Brown T, Boyle M, Dousek S. Psychometric testing of the Jefferson Scale of Empathy Health Profession Students’ version with Australian paramedic students. Nurs Health Sci. 2013;15(1):45–50. | |
Fjortoft N, Van Winkle LJ, Hojat M. Measuring empathy in pharmacy students. Am J Pharm Educ. 2011;75(6):109. | |
Kaiser HF. The application of electronic computers to factor analysis. Educ Psychol Meas. 1960;20:141–151. | |
Henson RK, Roberts JK. Use of exploratory factor analysis in published research: common errors and some comment on improved practice. Educ Psychol Meas. 2006;66(3):393–416. | |
Cattell RB. The scree test for the number of factors. Multivariate Behav Res. 1966;1(2):245–276. | |
Horn JL. A rationale and test for the number of factors in factor analysis. Psychometrika. 1965;30(2):179–185. | |
Pett MA, Lackey NR, Sullivan JJ. Making Sense of Factor Analysis: The Use of Factor Analysis for Instrument Development in Health Care Research. Thousand Oaks (CA): Sage; 2003. | |
deVaus DA. Surveys in Social Research. 3rd ed. Sydney: Allen and Unwin; 1991. | |
Boyle M, Williams B, Brown T, McKenna L, Molloy L, Lewis B. Attitudes towards patients by undergraduate health students. Proceedings of The 4th International Multi-Conference on Society, Cybernetics and Informatics: IMSCI 2010; Orlando, Florida, USA. 2010. | |
Ward J, Cody J, Schaal M, Hojat M. The empathy enigma: an empirical study of decline in empathy among undergraduate nursing students. J Prof Nurs. 2012;28(1):34–40. | |
Williams B, Boyle M, Brightwell R, et al. Paramedic empathy levels: results from seven universities. Int J Emerg Serv. 2012;1(2):111–121. | |
Williams B, Boyle M, Earl T. Measurement of empathy levels in undergraduate paramedic students. Prehosp Disaster Med. 2013;28(2):145–149. | |
Wahlin U, Wieslander I, Fridlund B. Loving care in the ambulance service. Intensive Crit Care Nurs. 1995;11(6):306–313. | |
Grevin F. Posttraumatic stress disorder, ego defense mechanisms, and empathy among urban paramedics. Psychol Rep. 1996;79(2):483–495. | |
Winefield HR, Chur-Hansen A. Evaluating the outcome of communication skill teaching for entry-level medical students: does knowledge of empathy increase? Med Educ. 2000;34(2):90–94. | |
Magalhães E, Costa P, Costa MJ. Empathy of medical students and personality: evidence from the Five-Factor Model. Med Teach. 2012;34(10):807–812. | |
McKenna L, Boyle M, Brown T, et al. Levels of empathy in undergraduate midwifery students: an Australian cross-sectional study. Women Birth. 2012;24(2):80–84. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.